
Abstract
The GLOBICS—Global Consortium of Oral Health Birth Cohort Studies (OHBCS)—is a long-lasting international collaborative research group among existing OHBCS, established in response to the Lancet Series on Oral Health, which pointed out the need to shift the global oral health agenda. This study aimed to identify priority research questions from OHBCS that can be leveraged to improve children’s global oral health. A 2-phase online Delphi process sought consensus over research priorities for OHBCS. Participants were identified by mapping existing OHBCS. Fourteen research questions were grouped into 4 thematic areas. A 9-point Likert-type scale was applied. Consensus was achieved if the question had (1) at least 51% of participants scoring a research question as “high priority,” (2) an interquartile range of <2.5, and (3) a standard deviation of <1.7 or 75% of responses falling between 2 points above and below the mean score. Forty-four of 114 participants completed the Delphi survey. The 8 research priorities identified included questions about the effect of childhood dental visits on oral health throughout life (n = 2), questions related to sugar consumption and dental caries in childhood and adolescence (n = 4), infant growth and dental diseases (n = 1), and whether socioeconomic inequalities in dental caries are mitigated by fluoride exposure (n = 1). Guided by expert insight, the priorities identified for future OHBCS research should leverage a life course perspective to address knowledge gaps in children’s oral health and oral health equity.
Introduction
Like other noncommunicable diseases (NCDs), most oral diseases exhibit a prolonged latency period between exposure and observable outcomes (Crall and Forrest 2018; Wolf et al. 2021) and have a multitude of risk factors that, if persistent, will result in poor oral health, affecting people over the life span. Therefore, life course epidemiology, which examines the long-term effects of social, biological, behavioral, and psychological paths that act across the life course and generations, is crucial for understanding and preventing oral diseases (Lancet Child and Adolescent Health, 2019; Peres et al. 2020). Birth cohort studies are beneficial for this purpose, as collecting health-related behaviors and experiences as they happen mitigates potential biases, such as recall bias (Kuh et al. 2003).
Oral health birth cohort studies (OHBCS) have provided valuable insights into the development of oral diseases, including their natural history, causes, and mechanisms. These studies have revealed, for instance, links between breastfeeding and malocclusion (Peres et al. 2015; Feldens et al. 2023) and dental caries (Peres et al. 2017; van Meijeren-van Lunteren et al. 2021), the cumulative effect of sugar consumption of dental caries from childhood to young adulthood (Peres et al. 2016), the stable trajectory of dental caries over the first 4 decades of life (Broadbent et al. 2008), the early life influence of socioeconomic disadvantage on oral health later on (Ramsay et al. 2018), and the impact of life course obesity on periodontitis in adulthood (Nascimento et al. 2017; Li et al. 2023).
In 2019, a workshop was held in Bangkok, Thailand, with researchers from prominent worldwide OHBCS to discuss the challenges and opportunities related to OHBCS. The need for an International Research Agenda to optimize the existing resources available from these studies was identified (Peres et al. 2020). To address this need, the Global Consortium of OHBCS (GLOBICS), launched in 2023, has identified 120 OHBCS worldwide (Peres et al. 2022) and has begun exploring priorities for a comprehensive research agenda to prioritize and outline pertinent research questions that the OHBCSs endeavor to address.
Therefore, the present study aimed to identify research questions that could improve global children’s oral health using OHBCS data. By leveraging the insights from OHBCS studies and fostering international collaboration, researchers hope to better understand, prevent, and address oral diseases globally.
Methods
A 2-round online Delphi consensus and rating study was conducted to establish a research agenda for OHBCS. Participants were experts identified from articles in a scoping review (n = 120) of OHBCS (Peres et al. 2022). No restriction regarding the expert’s background was applied to achieve a diverse pool of researchers involved in OHBCS. Contact was made via email and LinkedIn to ensure the inclusion of 1 representative from all OHBCS. The invitation explained the purpose of the research, and the option was given for the survey to be answered by someone from the team of researchers of each OHBCS whom the expert deemed most appropriate to contribute to the study. Initially, all publications identified in the scoping review were screened, and the preliminary topics were identified. The original questions combined themes that were less consistent across the 466 papers and ideas from the initial group. Participants were also asked to suggest additional topics (open-ended questions) that they deemed appropriate for the research agenda. The open-ended questions were also scored in the subsequent round by all the participants in the study. Selected questions for round 1 were pooled into 4 thematic areas: (1) intergenerational approach to oral health, (2) relationship between oral and general health, (3) oral health care and prevention, and (4) sugar intake over the life course.
The Delphi Process
The online survey software Qualtrics CoreXM was used as the data collection platform to conduct the 2 rounds of the Delphi process. The survey forms were created and tested before being distributed to the participants, who received a unique and personalized survey link. To avoid duplication, the survey link expired after form submission.
In the first round, experts scored research questions on a Likert-type scale ranging from 1 (lowest priority) to 9 (highest priority). A further option of “I do not have an opinion” was given to the participants. In round 2, participants were shown aggregated numerical representations of how their panel had scored each research question and were asked to rescore them, taking that information into account, with the option of being able to retain their initial score assigned to each question. Each round had a 2-mo response window, with reminders sent every 2 wk.
Consensus Definition
Consensus was considered to be achieved if the research question satisfied each of the following 3 criteria, namely, (1) at least 51% of participants scoring a research question 8 or 9 (“high priority”), (2) an interquartile range of less than 2.5, and (3) a standard deviation of <1.7 or 75% of responses falling between 2 points above and below the mean score (Jünger et al. 2017).
Research questions that satisfied all 3 criteria after round 1 were directly included in the research agenda and not rerated in round 2. Questions with <40% agreement on “high priority” were excluded, and others with ≥40% agreement but not meeting all criteria were reassessed in round 2. After completion of round 1, the preliminary findings were discussed with the executive committee, and their suggestions were incorporated into designing round 2. Questions suggested by the experts in the first round were included in round 2.
The responses were analyzed using the STATA software (version 17) to calculate each research question’s mean, median, and mode and to derive the other descriptive statistics concerning each study criterion.
Ethical Considerations
This work does not meet the definition of Human Subject Research by SingHealth Centralized Institutional Review Board (CIRB), and therefore, approval from an ethical review board was not required (protocol No. 396/2023).
Results
Of the 120 OHBCS identified in the scoping review, 114 investigators were identified, 1 from each OHBCS. Of those, 49 completed round 1 (August 2022 to October 2022) and 44 participants (39% of the initial invitees; 90% of the respondents from round 1) completed round 2 (November 2022 to January 2023) (Fig. 1). The final pool of participants represented a global distribution of birth cohorts, predominantly from high-income countries (77%), with a smaller representation from middle- (21%) and low-income (2%) countries, as illustrated in Figure 2. They were experts from diverse backgrounds, such as dentists (73.6%), epidemiologists (14.3%), physicians (6.1%), microbiologists (4.1%), biomedical scientists, nutritionists, and oral health therapists (2% each) (Appendix Table 1).
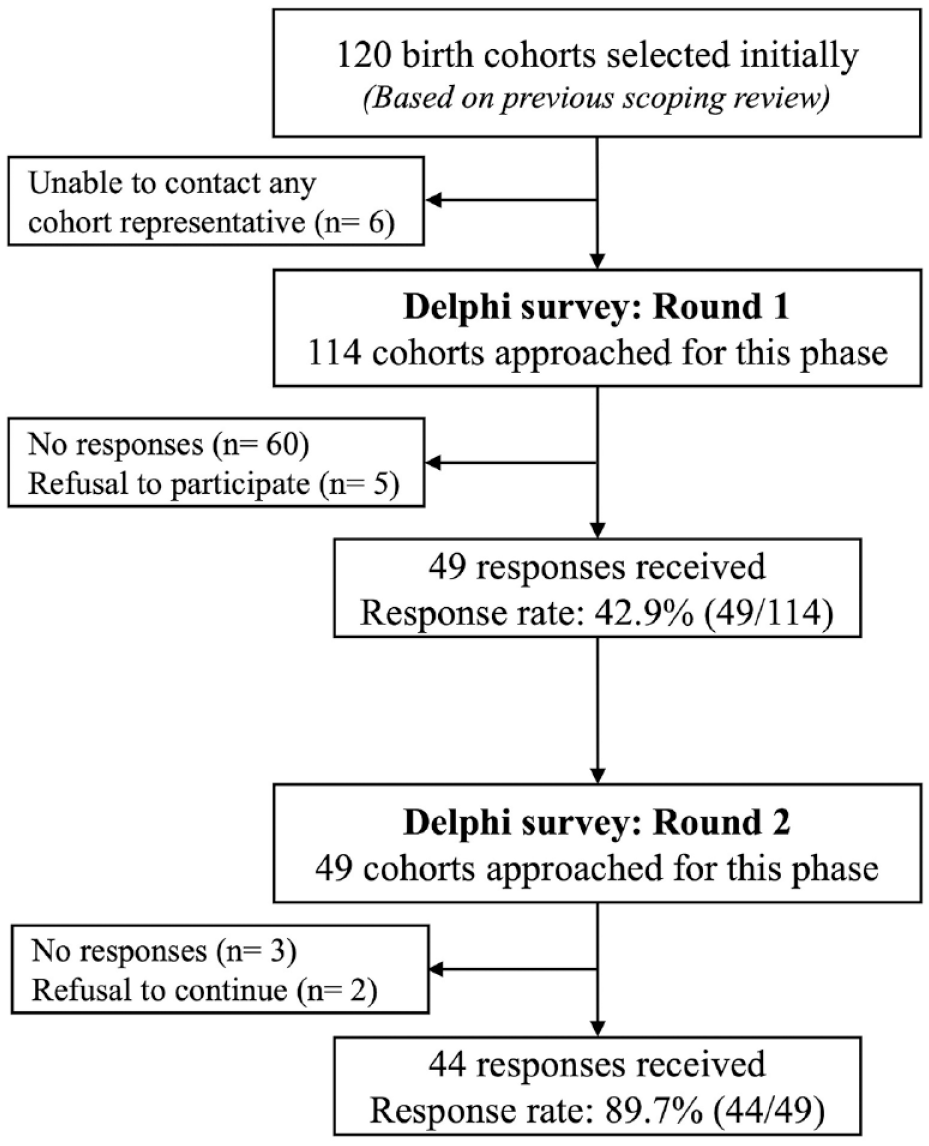
Flowchart illustrating the Delphi study design and the response rates.
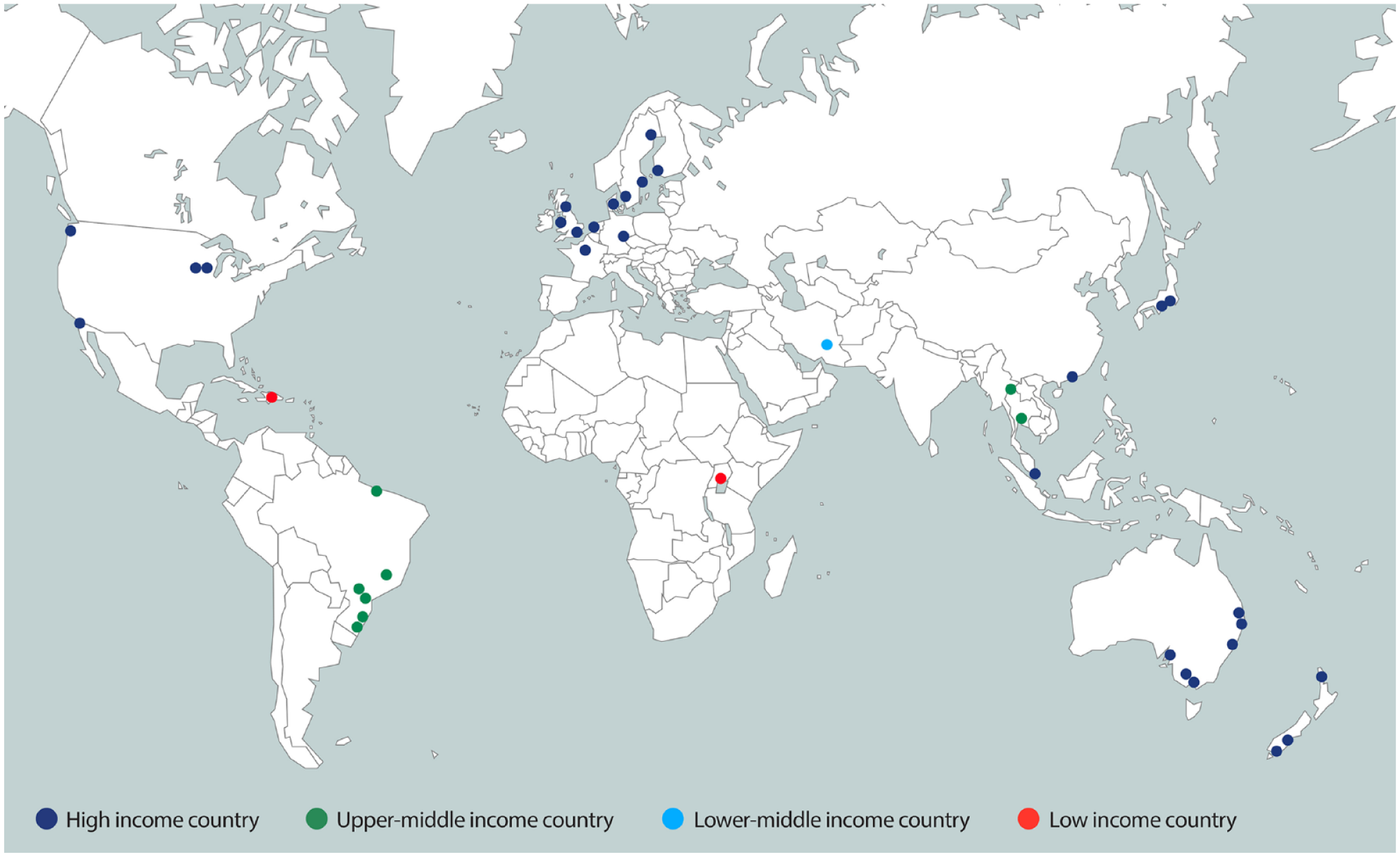
Countries of origin of Oral Health Birth Cohort Studies participating in rounds 1 and 2 of the Delphi study.
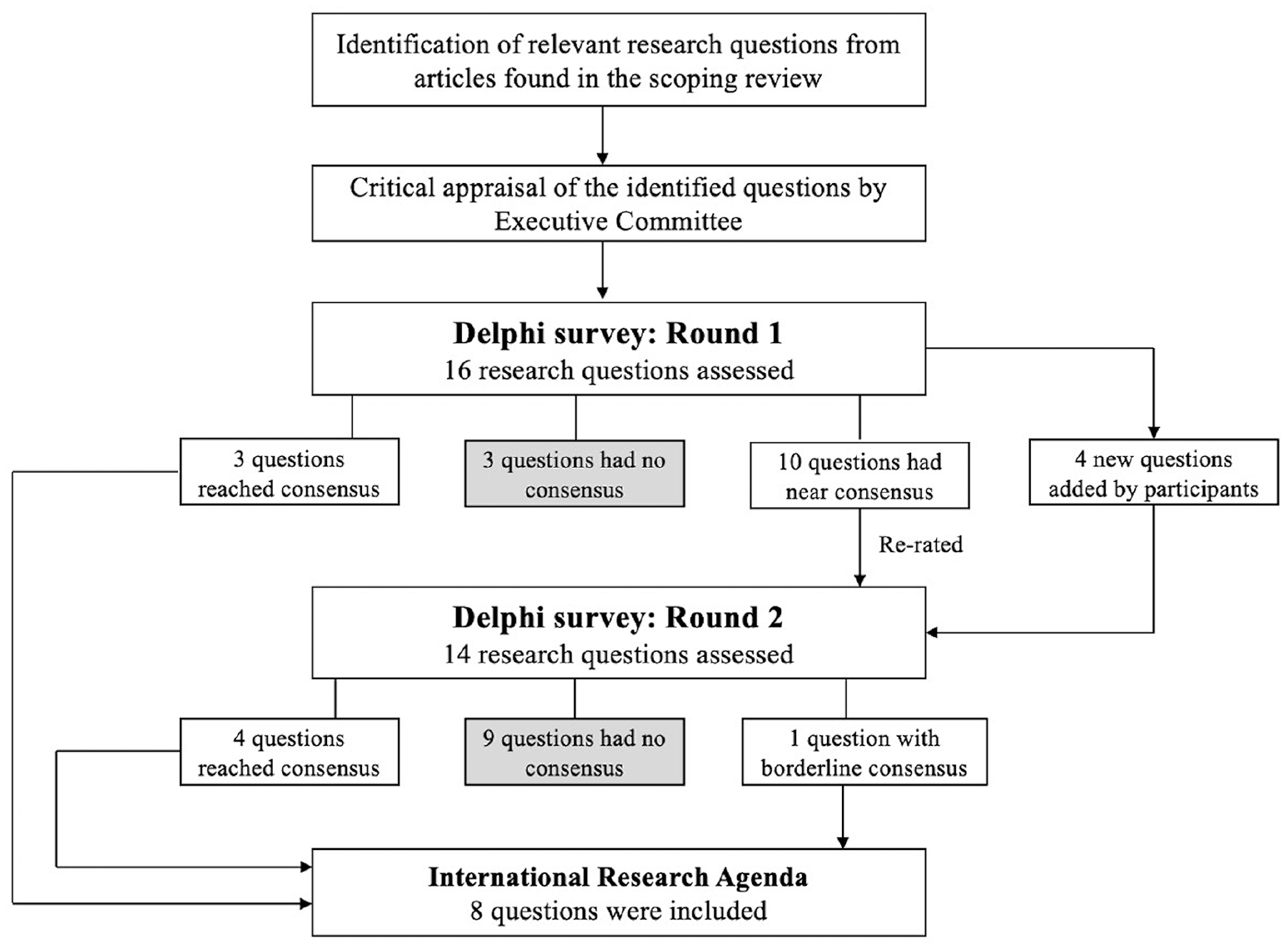
Sixteen research questions were assessed in round 1 and 14 questions in round 2. The 14 round 2 questions consisted of 10 questions that advanced from round 1 and 4 research questions added based on suggestions from participants in round 1. The final International Research Agenda comprised 7 research questions that met all 3 criteria and 1 question that reached borderline consensus (50% agreement) but fulfilled all other criteria (Fig. 3). Descriptive statistics for each research question based on each selected criterion are described in Table 1.
Questions included in the International Research Agenda.
Descriptive Statistics for the Research Questions Based on Each Selected Consensus Criteria. a
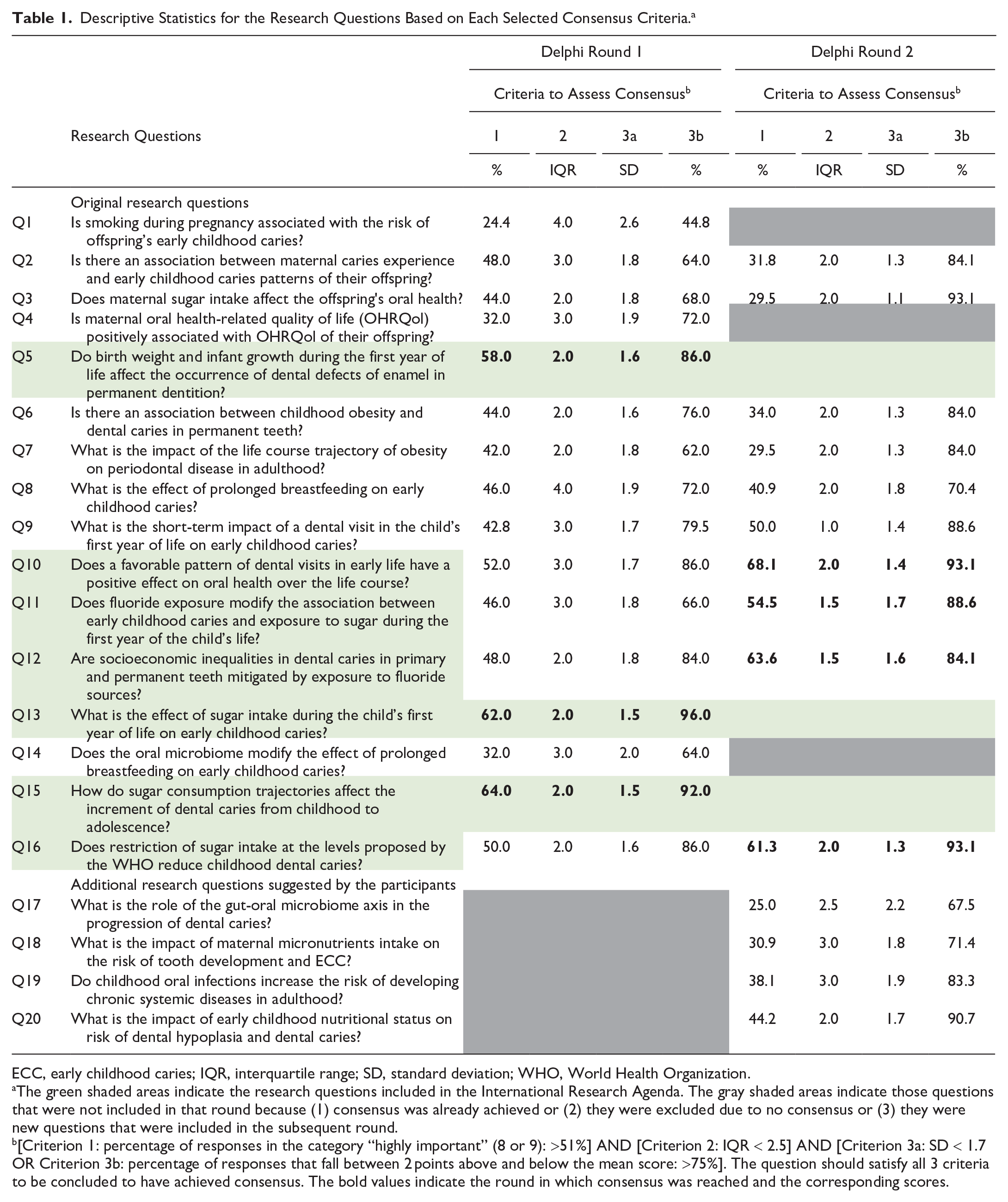
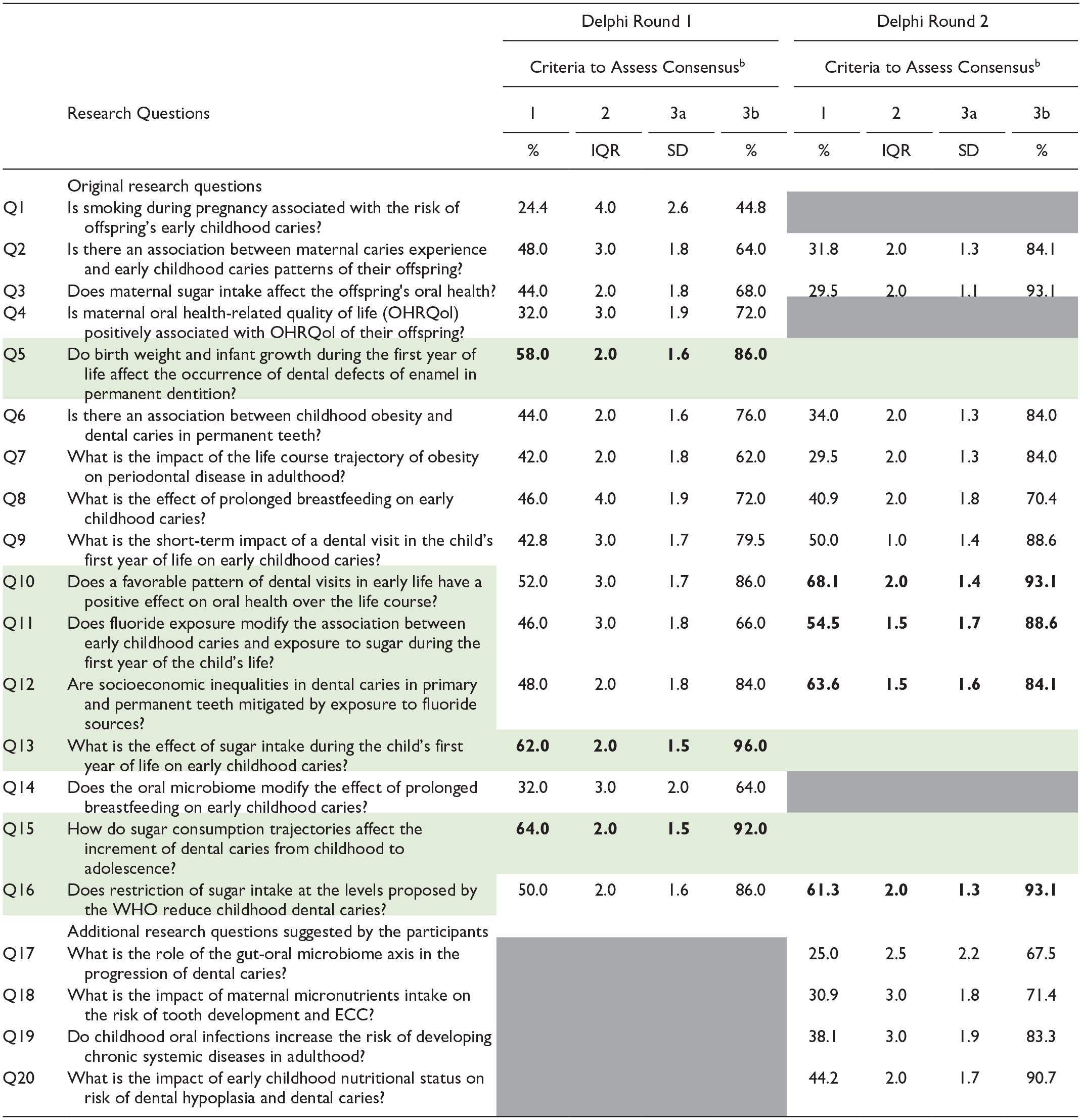
ECC, early childhood caries; IQR, interquartile range; SD, standard deviation; WHO, World Health Organization.
The green shaded areas indicate the research questions included in the International Research Agenda. The gray shaded areas indicate those questions that were not included in that round because (1) consensus was already achieved or (2) they were excluded due to no consensus or (3) they were new questions that were included in the subsequent round.
[Criterion 1: percentage of responses in the category “highly important” (8 or 9): >51%] AND [Criterion 2: IQR < 2.5] AND [Criterion 3a: SD < 1.7 OR Criterion 3b: percentage of responses that fall between 2 points above and below the mean score: >75%]. The question should satisfy all 3 criteria to be concluded to have achieved consensus. The bold values indicate the round in which consensus was reached and the corresponding scores.
Questions Included in the International Research Agenda
The final research questions included in the International Research Agenda were distributed across themes: 1 question fit into “relationship between oral and general health,” 4 into “oral health care and prevention,” and 3 into “sugar intake over the life course” (Fig. 4). While no questions from the “intergenerational approach to oral health” theme achieved consensus for inclusion, 2 questions came close to meeting the specified criteria.
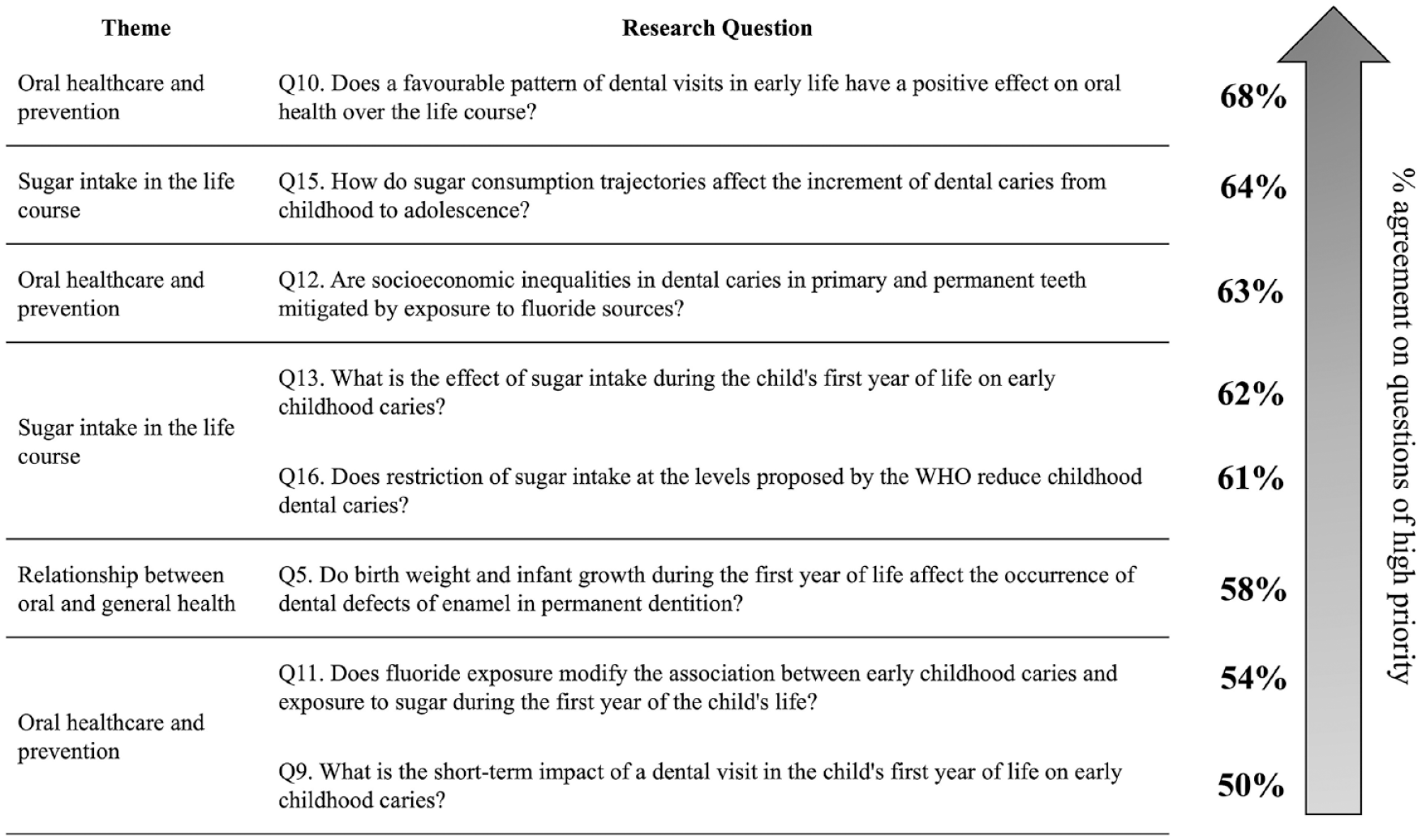
Final questions included in the International Research Agenda.
Figure 4 displays the questions included in the International Research Agenda and their respective agreement percentage. The question, “Does a favorable pattern of dental visits in early life have a positive effect on oral health throughout life?” was ranked as the top research priority, followed by questions related to sugar consumption and dental caries in childhood and adolescence, and lastly, whether exposure to fluoride sources mitigates socioeconomic inequalities in dental caries in primary and permanent teeth.
Discussion
The research agenda stemmed from our study comprised 8 priority research questions distributed across 3 proposed thematic areas: oral health care and prevention (n = 4), sugar intake in the life course (n = 3), and the relationship between general and oral health (n = 1). Half of the prioritized questions deal with a common factor in childhood morbidities and oral diseases, early sugar intake, and the need to understand better the relationship between general and oral health in children. Childhood, a critical period for the developing of life course morbidities, was present in 7 of the 8 selected questions. These priority areas reflect unanswered questions in oral health research for which OHBCS can be leveraged to inform both policy and practice.
The representation of high-income countries can influence study priorities, potentially skewing findings and recommendations toward issues relevant to those contexts while missing opportunities to address specific challenges in low-income and low-middle-income countries. Despite the representation of most OHBCS from low- and middle-income countries among the panelists, our findings shed light on the need to promote new OHBCS in these regions.
Concerns about selection bias arise as 39% of invited experts—primarily from high-income countries—participated, which could limit diversity. However, the respondent distribution mirrored the global OHBCS distribution. While only 2% of respondents were from low-income countries, they represented all existing OHBCS in these settings, with a similar pattern for middle-income countries.
The top priority was investigating whether a favorable pattern of dental visits in early life leads to positive oral health over the life course. Interestingly, another priority was aligned with this and concerned the short-term impact of the first dental visit during the first year of the child’s life. A systematic review of the effectiveness of early preventive dental visits in improving children’s oral health outcomes found weak evidence supporting the recommendation for such visits within the first year of life for preventive purposes. However, the review included only 4 studies, all of them retrospective cohort studies that analyzed public insurance claims data. Although some studies indicated mixed associations between early visits to the dentist and oral health conditions, 1 study reported no significant benefit but noted increased future preventive visits (Bhaskar et al. 2014).
Some existing research from OHBCS have described patterns of dental attendance throughout the life of individuals, particularly since childhood, with routine dental attendance typically dependent on various attributes of the population studied such as income, affordability, region, and resources available. A well-designed study investigated whether patterns of dental attendance from adolescence to adulthood were associated with better oral health and oral-health-related quality of life (OHRQoL) among adults. Although the prevalence of routine dental attendance decreased from 82% at age 15 y to 28% at age 32 y, regular dental attendees reported better oral health and OHRQoL and had fewer lost and decayed teeth (Thomson et al. 2010). The prevalence of dental attendance in the study mentioned above is considered high for age 15 y; however, this scenario does not reflect the situation children face during their first years. A few existing studies revealed that, on average, children’s first dental visit occurs after 5 y of age, with enormous inequality in visit timing. Not only do children from socially disadvantaged groups access dental care later, but when they do, the visit is more likely an emergency visit, which often includes pain and suffering (Crocombe et al. 2012). Astonishingly, the question of when a child should visit a dentist for prevention/checkup has yet to be answered. Some countries have a specific recommendation for a first dental visit focusing on counseling and prevention (Bhaskar et al. 2014). However, more robust evidence is needed to support these recommendations and examine their benefits. Also, the time of the first dental visit can modify the association between socioeconomic status (SES) and oral health. In that case, OHBCS analyses can address another open question, contributing to understanding and tackling socioeconomic inequalities in oral health (Savage et al. 2004).
The first years of a child’s life are a unique opportunity to introduce healthy behaviors and, subsequently, to improve oral and general health outcomes. When analyzing early-life dental visits, researchers should consider including behavioral aspects of oral diseases, particularly those related to dental caries and initial forms of periodontal diseases. This involves promoting health at an individual level, improving knowledge about healthy eating and oral hygiene practices, and the prompt use of preventive methods such as fluorides in arresting disease. Pediatricians and primary care providers can play an essential role in improving their patients’ oral health who have difficulty obtaining professional dental care (Pierce et al. 2002). They usually assess children in early infancy on a regular and well-accepted schedule.
The effect of trajectories of sugar consumption over time on dental caries was ranked the second research priority. Notably, 2 other questions related to sugar consumption occupied the fourth and fifth positions in importance. While the effect of sugar consumption on dental caries is unquestionable, there is a need for more reliable long-term data on how childhood sugar consumption affects dental caries over the life span. Introducing sugar before 12 mo of age is responsible for a high prevalence of caries in primary dentition (Echeverria et al. 2023). Another study observed an association between sugar introduction at 6 mo and caries in permanent molars among children aged 60 mo (Feldens et al. 2021). In a high-income country, not only early sugar introduction but also a sustained high sugar consumption trajectory during the child’s first 5 years resulted in a higher prevalence of cavities at age 5 y (Ha et al. 2023).
Trajectories of sugar consumption and dental caries in childhood and beyond have been barely investigated and revealed that the higher the sugar consumption from childhood (at 6 y of age) to young adulthood (18 y of age), the greater the dental caries increment in the same period even in the context of a fluoridated water supply and widespread use of fluoridated toothpaste (Peres et al. 2016). The scarcity of such studies underscores the importance of this topic in the consensus process. Closely examining sugar consumption trajectories during the life course could be relevant when translating research into policies such as taxation of health-deleterious foods, regulation of food labels and marketing, reformulation of foods with high sugar content, and promotion of sugar-free environments (Mozaffarian et al. 2018).
Oral diseases share the main risk factors of other NCDs—SES, sugar consumption, tobacco, any alcohol—and therefore should have a more vital place on the global NCDs agenda, with broader integration with other areas of health and more notoriety within universal health coverage commitments. In the context of OHBCS, differences across countries would help evaluate socioeconomic inequalities’ influence on oral health, considering various scenarios. In addition, the importance of aligning OHBCS with World Health Organization (WHO) recommendations on sugar intake was highlighted. The current WHO guideline recommends adults and children reduce their daily intake of free sugars to less than 10% of their total energy intake and the desirability of a further reduction to below 5% or roughly 25 g of sugars (World Health Organization 2015). Nevertheless, even smaller amounts of sugar than those recommended by the WHO have been shown to be associated with dental caries (Ladeira et al. 2024). However, determining a cutoff point below which sugar consumption is safe for caries still needs to be investigated. Pooling data from OHBCS can facilitate such investigation and help globally assess the impact of adhering to future guidelines.
The third research priority explores whether fluoride exposure can mitigate socioeconomic inequalities in dental caries. A recent systematic review identified 4 studies showing a positive impact of water fluoridation on reducing inequalities in caries among children. While water fluoridation appears to be effective in mitigating socioeconomic inequalities in dental caries, the effects of other sources of fluoride are yet to be investigated (Shen et al. 2021). On a related note, a Cochrane review found insufficient information to determine whether water fluoridation could effectively reduce inequalities in caries levels across socioeconomic status (Iheozor-Ejiofor et al. 2015); however, this finding may be due to the stringent eligibility criteria applied to this review (Rugg-Gunn et al. 2016). While no OHBCS has explored this relationship, a coordinated effort to leverage data from existing OHBCS from different socioeconomic contexts and different sources of fluoride exposures would be fundamental for establishing approaches toward reducing oral health inequalities.
Some limitations must be discussed. First, the output and recommendations from a Delphi process inherently rely on the quality of the evaluated statements. Although the proposed research questions were mainly developed based on potential gaps identified in previously published OHBCS (Peres et al. 2022), as with any Delphi process, the values, preference, and experiences of this expert panel likely contributed to their selections. While the Delphi method cannot quantify this influence, experts were encouraged to evaluate questions only within their areas of expertise. Notwithstanding the above considerations, it is essential to approach this research agenda as a synthesis of experts’ viewpoints, and any extrapolations should be made with caution. It is crucial to emphasize that when prioritizing research questions for the OHBCS agenda, no strict formula was given to prioritize research topics; the experts considered the level of existing knowledge about the research questions, their urgency to be addressed, and the strength of association between a given exposure and the outcome. The DELPHI method, therefore, allows different experts to converge on a given topic to reach a consensus. A potential advancement for OHBCS collaborations involves operationalizing the acquisition of clinical data and biological samples to facilitate the alignment of forthcoming studies. This study attracted existing OHBCS experts. A larger sample or alternative methodological approaches could also yield divergent results. However, the Delphi process’s cost-efficiency, inclusiveness, and rapid nature facilitated the involvement of a diverse panel of experts from various countries, encompassing different socioeconomic and cultural backgrounds. Lastly, different communication strategies have been adopted to engage more experts, such as institutional and personal emails and LinkedIn messages.
The strengths of the study merit emphasis. In contrast to other studies using the Delphi method—studies that typically rely on 1 (Duncan et al. 2021) or at most 2 criteria (Geist 2010) to define consensus—this study employed 3 distinct criteria. This approach, which avoids exclusive reliance on percentage agreement, can be considered both conservative and robust, ensuring the inclusion of only pertinent questions in the International Research Agenda. Moreover, it mitigates the risk of extreme discrepancies among experts by considering data distribution and variability.
This study’s findings go beyond establishing a research agenda for OHBCS. They provide valuable guidance to future OHBCS endeavors. For instance, a consensus SES index could be created based on available variables from each cohort. Furthermore, the regularity of dental visits could be harmonized according to future pooled analysis. These inquiries directly benefit clinicians and policy makers, enhancing their ability to make informed decisions based on collective evidence from numerous studies. Findings will guide GLOBICS in supporting OHBCS as a transformative force advocating global oral health (see the GLOBICS webpage https://www.ndcs.com.sg/research-innovation/NDRIS/GLOBICS/Pages/Home.aspx). Collectively, we may advance the field of OHBCS and make it significant.
Authors’ Contributions
K.G. Peres, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; A.C. Kalhan, S. Sarawagi, contributed to design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; M. Peres, contributed to conception and design, data interpretation, drafted and critically revised the manuscript; C.A. Feldens, B.W. Chaffee, A. Jardim Dornellas de Barros, A. Rugg-Gunn, contributed to design, data interpretation, drafted and critically revised the manuscript; G.G. Nascimento, contributed to conception and design, data analysis and interpretation, drafted and critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345241286869 – Supplemental material for An International Research Agenda for Oral Health Birth Cohort Studies
Supplemental material, sj-docx-1-jdr-10.1177_00220345241286869 for An International Research Agenda for Oral Health Birth Cohort Studies by K.G. Peres, A.C. Kalhan, S. Sarawagi, M.A. Peres, C.A. Feldens, B.W. Chaffee, A.J.D. Barros, A. Rugg-Gunn and G.G. Nascimento in Journal of Dental Research
Footnotes
Acknowledgements
We thank all participating experts from the OHBCS for their time and valuable contributions, including O.M. Ajetunmobi, A. Arora, A.J.D. Barros, E. Bernabe, H. Bettiol, N. Birungi, K. Boustedt, J.M. Broadbent, B.W. Chaffe, S. Hsu Chin-Ying, G. Dahllof, B.A. Darlow, S.G. Dashper, E.K. Delgado-Angulo, L.G. Do, D.R. Drake, M.E.C. Elfrink, C.A. Feldens, A. Germa, F.J. Ramos-Gomez, D. Haubek, T. Hughes, H.A. Hutchings, J.J.K. Jaakkola, I. Johansson, N.W. Johnson, S.M. Levy, T.A. Marshall, G. Maupome, K. Moriyama, K. Pattanaporn, M.S. Pearce, W. Pitiphat, H. Poureslami, W. Psoter, P. Rautava, C.C.C. Ribeiro, M.C.P. Saraiva, P.J. Schluter, W.K. Seow, M.J. Silva, N. Stormon, K. Tanaka, A. Tsang, Y. Wagner, H.M. Wong, and S. Yoshida.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Medical Research Council Singapore (PHRGOC22Jul-0021) and the Borrow Foundation (2021-2024).
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.