
Abstract
This study aimed to compare the clinical effectiveness of resin-based fissure sealants (FS) and fluoride varnish (FV) in children at high caries risk. A practice-based split-mouth randomized clinical trial was conducted at 9 Public Dental Service (PDS) clinics in Norway. In total, 409 children age 6 to 10 y at high caries risk (d3mft > 0) meeting inclusion criteria were recruited by dentists and dental hygienists during routine examination. Eligibility criteria were 2 fully erupted first permanent molars (FPMs) in the same jaw, with sound occlusal surfaces or with initial caries. Participation was voluntary, caregivers and eligible children were informed about the study, and written parental consent was obtained. FS and FV were randomly applied on contralateral FPMs in the same jaw, with each participant serving as their own control. FS was applied at baseline and thereafter maintained according to clinicians’ conventional procedures, whereas FV was applied at baseline, 6 mo, and 12 mo. The study outcome was success, with no need for invasive treatment (caries control), while failure was defined as dentin carious lesion or restoration. Two-level mixed-effects logistic regression analysis was used to compare FS and FV groups. Of 409 recruited children, 369 (90%) children/tooth pairs were examined after 36 mo. Intention-to-treat analysis showed 94.1% adjusted predicted probability (aPP) of success (95% confidence interval [CI] 91.7 to 96.4) in the FS group and 89.6% aPP (95% CI 86.5 to 92.7) in the FV group. In the adjusted analysis, the FV group had a lower OR for success compared with the FS group (OR 0.54, 95% CI 0.24 to 0.87). In the population studied, the clinical effectiveness of FS was statistically significantly higher compared with FV but below the estimated minimal clinically important difference of 10%.
Introduction
Early measures to control caries is a key objective in dental care. Two management methods, fissure sealants (FS) and fluoride varnish (FV), specifically target the occlusal surfaces of permanent teeth and are routinely used for caries control in children because of their proven effectiveness (Ahovuo-Saloranta et al. 2016; Kashbour et al. 2020).
The placement of resin-based FS is a much more technique-sensitive and time-consuming procedure compared with FV (Kashbour et al. 2020). Moreover, the effect of FS largely relies on their retention, and it has been suggested that the durability of FS might be lower for patients with high caries risk (Splieth et al. 2010). In addition, regular monitoring is necessary for FS success (Aleksejuniene et al. 2010; Kashbour et al. 2020). By contrast, FV needs repeated applications, requiring several dental clinic visits (Norwegian Directorate of Health 2022; Wang et al. 2022).
A recent systematic review evaluated the relative effectiveness of the 2 caries control methods and concluded that few controlled trials of high scientific quality were available (Kashbour et al. 2020). The review included 4 studies, 2 performed before 2000, concluding that FS had better effect than FV but that available data were insufficient to recommend one method over the other. Moreover, the relative effectiveness of FS and FV in a practice-based setting, where clinicians follow their habitual work routines and are working under time pressure, has yet to be evaluated. It has been suggested that practice-based studies have a higher external validity than controlled trials do (Demarco et al. 2020) and thus provide a better understanding of how these treatment modalities work in dental clinics.
Norwegian national guidelines on dental care for children and adolescents recommend the use of FS as a first choice for occlusal caries management in children who are considered at risk for caries (Norwegian Directorate of Health 2022). Both FS and FV are well adopted in the Public Dental Service (PDS) in Norway, and most children at high risk in PDS receive either FS or FV on newly erupted occlusal surfaces of first permanent molars (FPMs) (Skudutyte-Rysstad et al. 2022). This provides an opportunity to assess the clinical effectiveness of these methods in real-life conditions, under time pressure and with multiple clinicians involved.
This split-mouth, practice-based randomized clinical trial aimed to compare the clinical effectiveness of FS and FV in FPMs of children at high caries risk in PDS in Norway. The null hypothesis was that there would be no difference in the clinical effectiveness of FS and FV on caries control after 36 mo when applied to occlusal surfaces of FPMs.
Methods
Trial Design and Setting
The present study was designed as a pragmatic multicenter, within-person, randomized split-mouth trial (SMT), conducted at 9 PDS clinics in 3 counties of southeastern Norway. Recruitment of children at baseline was carried out by the clinics’ dentists and dental hygienists, as part of scheduled routine examinations. Recruitment took place from February 2017 to November 2019, and the 3-y follow-up was completed in November 2022.
Participants
Children at high caries risk, defined as having a sum of decayed, missing, and filled teeth (d3mft) > 0 at enrollment, born between 2009 and 2013 (i.e., aged 6 to 10 y at the time of inclusion) were eligible to participate in the study. The inclusion criteria were 2 fully erupted FPMs in the same jaw, with sound occlusal surfaces or with initial occlusal caries, no previous restorations or FS, and no known sensitivity to FS or FV. Exclusion criteria were poor patient cooperation and communication/language barriers for obtaining consent.
Background Characteristics
Participant date of birth, sex, county of the PDS clinic, and clinician’s identification code were recorded. Caries experience at age 5 y (d3mft) was retrieved from the electronic dental record forms. Information on the use of fluoride toothpaste (no/sometimes/daily) and toothbrushing habits (never/sometimes/once daily/twice or more daily) was obtained from a parental questionnaire.
Interventions
Clinical examinations
Study participants were examined at PDS clinics. FPM occlusal surfaces were assessed clinically and radiographically using a 5-point scale routinely applied for caries registration in PDS in Norway (Amarante et al. 1998). Occlusal surfaces were registered as sound, initial caries (grades 1 to 2) or dentin caries (grades 3 to 5). Prior to the study, clinicians received information and training in the study protocol and diagnostic criteria for baseline caries assessment. Each clinic also received written instructions for participant recruitment and follow-up, participant case report forms (CRFs), and a pictorial illustration guide with caries registration criteria. Calibration of the participating clinicians was performed electronically, using 24 clinical intraoral images of the occlusal surfaces in the beginning of the study and repeated later (March and April 2019 (n = 40) and September to November 2021 (n = 25)). Weighted kappa values for interexaminer reliability for sound, initial caries, dentin caries, and sealed surfaces were 0.62 (confidence interval [CI] 0.575 to 0.662) and 0.66 (CI 0.63 to 0.69) for the first and second calibration, respectively.
Caries status was assessed at baseline and at 6, 12, 24, and 36 mo by a total of 69 clinicians at the respective clinics, among whom 36 were involved throughout the study period.
Randomization
FS and FV were randomly applied to contralateral FPMs of the same jaw at baseline, and each child served as their own control. The clinician was instructed to select a tooth and to ask the child to pick the treatment by randomly choosing 1 of 2 cards, representing either FS or FV, while the molar on the contralateral side concurrently received the other treatment. Thus, treatment allocation was a 1:1 ratio, and randomization to FS or FV was performed at a tooth level.
Methods evaluated
Clinicians were instructed to use FS and FV materials available at their clinics and to follow their conventional procedures for applying and maintaining them. FS materials and maintenance were recorded on a CRF. FS was applied at baseline and maintained/reapplied if considered necessary by the clinician. FV treatment included the application of 5% sodium fluoride (NaF) varnish (22,600 parts per million [ppm] fluoride), applied at baseline and at 6- and 12-mo follow-ups.
Outcome
The outcome was assessed based on the diagnosis of FPM occlusal surfaces at 36-mo follow-up, dichotomized as success and failure. Success was defined as no need for invasive treatment (i.e., caries control), while failure was defined as dentin carious lesion or restoration.
Sample Size
Based on the assumptions that 80% of included teeth will not develop dentin caries, that a 10% difference in dentin caries incidence between the methods constitutes a clinically meaningful/significant difference, and that the between-methods correlation is 0.3, it was estimated that 180 participants were needed at the final follow-up for the SMT, with 80% power and a 5% significance level. To compensate for an annual potential dropout rate between 20% and 25% over the 3-y follow-up, enrollment of a total of 400 participants was needed.
Approvals
The study was approved by the Regional Committee for Medical Research Ethics South-East Norway (2016/2002/REK sør-øst C) and registered at ClinicalTrials.gov (ID: NCT03315312). Participation was voluntary, caregivers and eligible children were informed about the study, and an informed, written parental consent was obtained.
Statistical Methods
Participant background characteristics and FPM occlusal surface baseline status were summarized using descriptive statistics (N, mean, standard deviation, median, and first and third quartiles) for continuous variables and number and percentage for categorical variables. Chi-squared and Mann–Whitney U tests were used to compare participants and dropouts.
Information on whether the child was examined/treated by the same clinician throughout the study period was dichotomized as “same clinician” versus “different clinician” (i.e., examined/treated by more than 1 clinician during the study).
For missing data in the independent variable (i.e., d3mft at age 5 y), multilevel multiple imputation was performed using the miceadds package in R.
The full analysis set (FAS) was defined as all patients having received both treatments at baseline and completing 36-mo follow-up. The per-protocol analysis set (PPS) included all patients who received at least 3 FV applications (i.e., baseline, 6 mo, and 12 mo).
The primary analysis was an intention-to-treat analysis (ITT) performed on FAS. Sensitivity analysis was performed using PPS. In addition, to assess the possible effect of clinics’ county, on a primary outcome, a sensitivity analysis adjusted for this measure was performed. Number needed to treat (NNT) was calculated.
The primary outcome was analyzed by a multivariate 2-level mixed-effects logistic regression model with teeth (level 1) nested within children (level 2). The model was adjusted for background characteristics (age, sex, d3mft at age 5 y, and clinician) and baseline FPM occlusal surface status.
Intracluster correlation (ICC) estimates from the adjusted model were obtained to explore the variability in the outcome variable that is attributable to differences between the clinics.
Analyses were performed with Stata SE v16 (release 16, Stata Statistical Software, College Station, TX, USA) and R Statistical Software. The results from the regression analysis were presented as crude and adjusted odds ratio (OR) with 95% CI. The significance level was set at α = 0.05.
The Consolidated Standards of Reporting Trials (CONSORT) statement for reporting within-person randomized trials was used (Pandis et al. 2017).
Results
A total of 409 children were recruited, and 369 (90%) children/tooth pairs were evaluated at the 36-mo follow-up and thus included in the FAS, whereas 330 (81%) were included in the PPS (Fig.). Of 369 pairs of teeth included in the ITT analyses, 209 were in the maxilla and 160 were in mandibula. The background characteristics of the included children are presented in Table 1. No statistically significant differences in background characteristics or FPM occlusal surface baseline status were detected between participants and dropouts, except for county (Table 1). Overall, 93% of included children reported daily use of fluoride toothpaste, 84% reported toothbrushing twice daily, and 34% were followed by the same clinician during the entire 3-y study period.
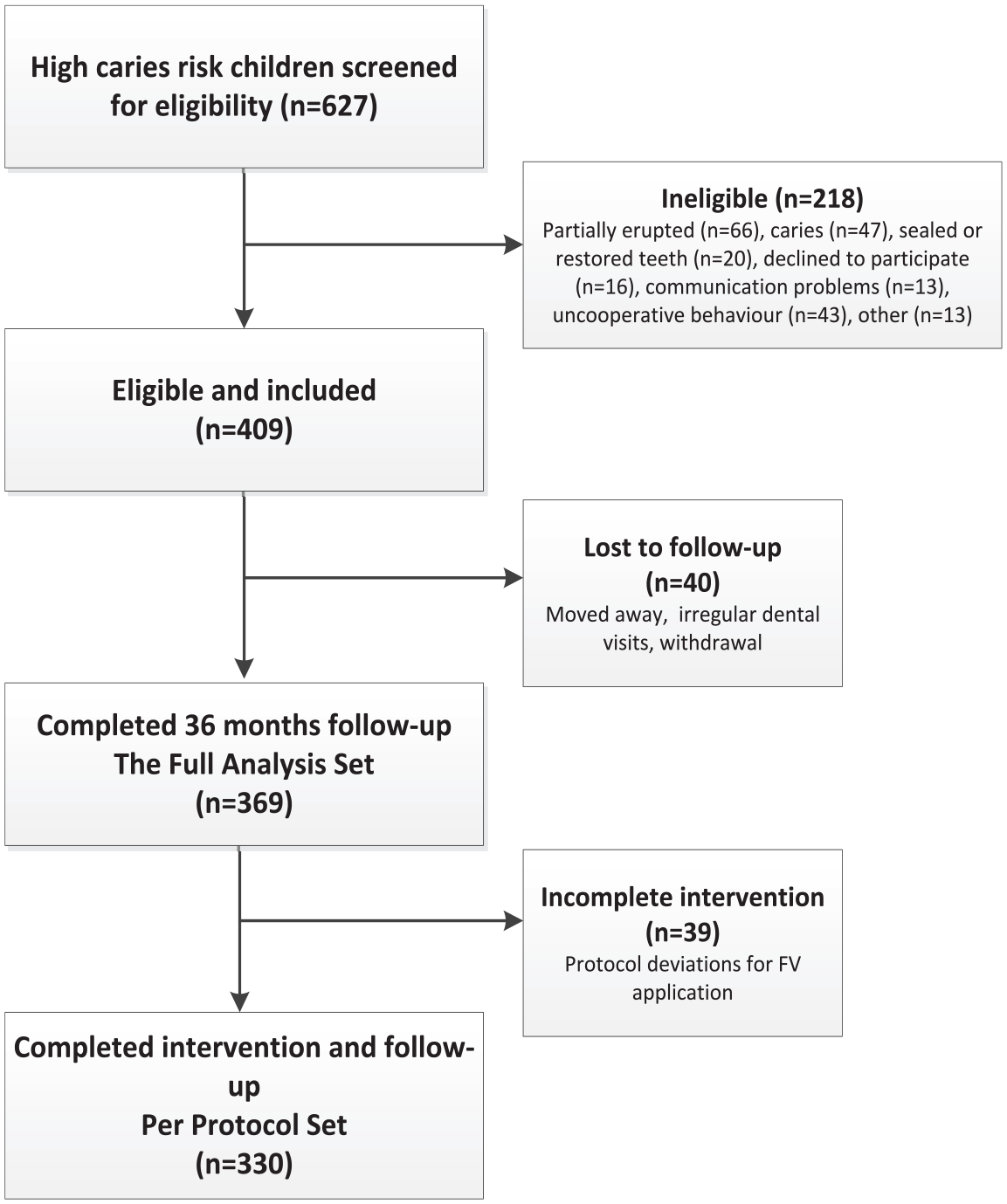
Flow chart of participants in the study.
Background Characteristics and FPM Occlusal Surface Baseline Status of Participants Who Reached 36-mo Follow-up (n = 369) and Dropouts (n = 40). a
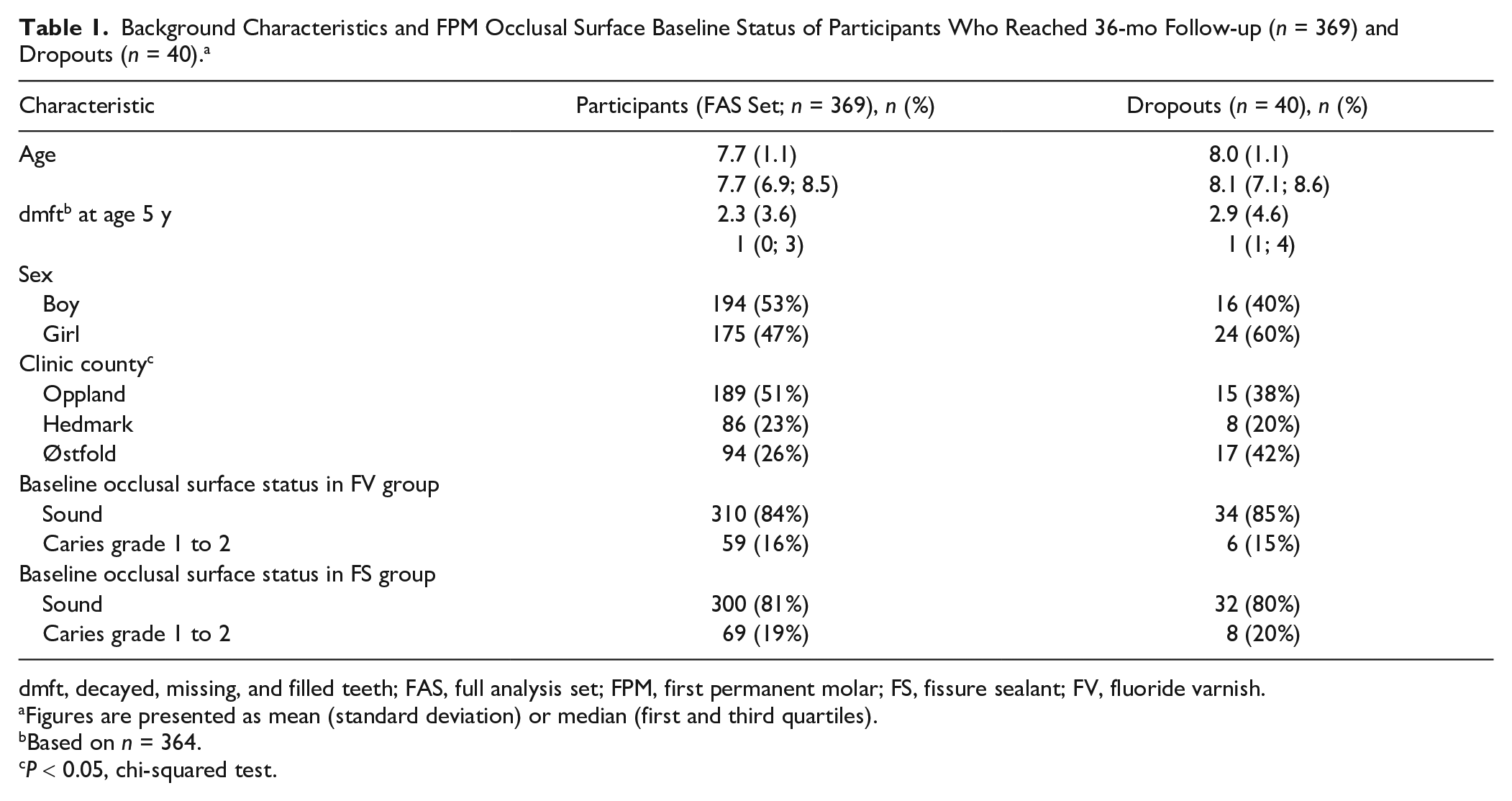
dmft, decayed, missing, and filled teeth; FAS, full analysis set; FPM, first permanent molar; FS, fissure sealant; FV, fluoride varnish.
Figures are presented as mean (standard deviation) or median (first and third quartiles).
Based on n = 364.
P < 0.05, chi-squared test.
Descriptions of the FS materials are presented in Appendix Table 1.
The ITT analysis showed 94.1% aPP of success (95% CI 91.7 to 96.4) in the FS group and 89.6% aPP (95% CI 86.5 to 92.7) in the FV group (Table 2). The NNT was 25.
Predicted Probability of Treatment Success after 36 mo Based on the Full Analysis Set, Obtained from the Multivariable 2-Level Mixed-Effects Logistic Regression Models. a

Predicted probability (aPP) of success obtained from the mixed-effects logistic regression model adjusted for background characteristics (age, sex, caries experience at age 5 y [d3mft], clinician) and baseline status of the occlusal surface of the first permanent molars.
According to the adjusted analysis, FPMs in the FV group (versus the FS group) had 54% lower odds of success (OR 0.46, 95% CI 0.24 to 0.87) (Table 3). Initial caries (caries grade 1 to 2) at baseline significantly decreased the odds for success, irrespective of method (OR 0.29, 95% CI 0.29 to 0.67).
Univariable and Multivariable 2-Level Mixed Effects Logistic Regression Models for the Success (versus Failure) of FV and FS Adjusted for Participants’ Background Characteristics and FPM Occlusal Surface Baseline Status Based on the Full Analysis Set (n = 369).
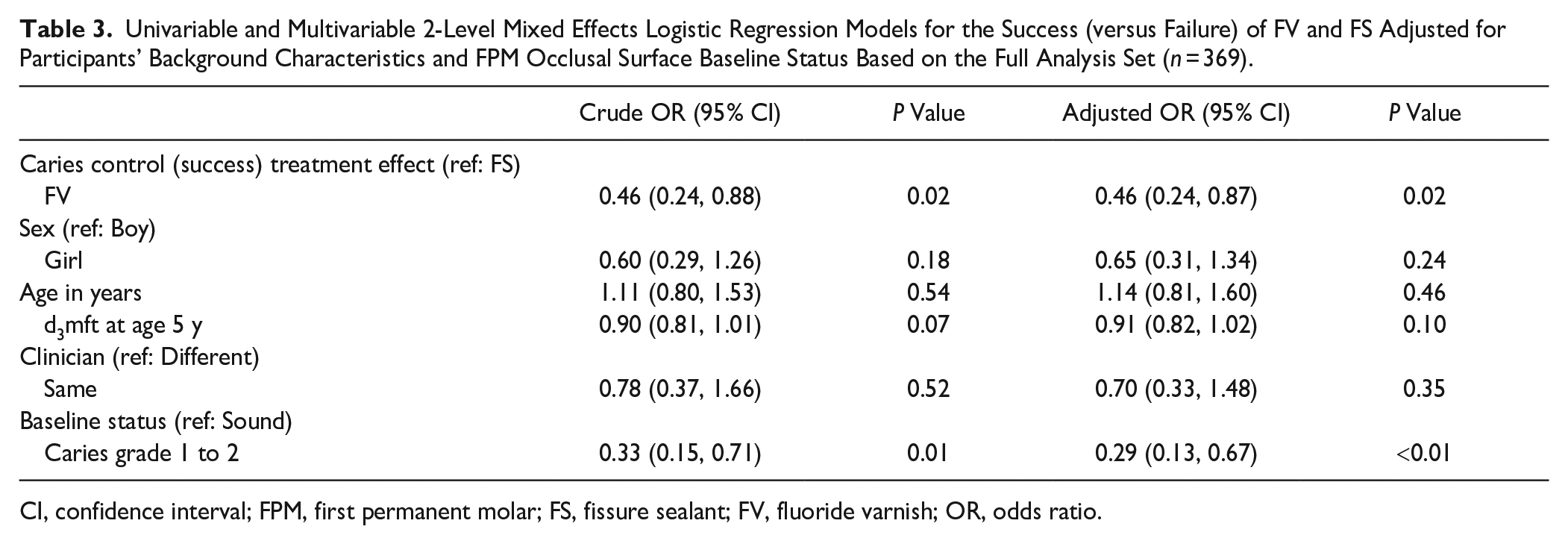
CI, confidence interval; FPM, first permanent molar; FS, fissure sealant; FV, fluoride varnish; OR, odds ratio.
Sensitivity analyses using PPS (Appendix Table 2) and sensitivity analyses of the primary outcome adjusted for clinic county (Appendix Table 3) showed consistent results. An estimate of the ICC at the clinic level of 0.048 was obtained from the adjusted model, meaning that 4.8% of the variability in the outcome (success/failure) can be attributed to differences between the clinics.
In the FS group, 34.8% of the FPMs had received FV applications over FS. Success was achieved in 95.3% of teeth with FS and in 93.9% of teeth with FV over FS.
Discussion
This practice-based clinical trial evaluated the effectiveness of routinely applied resin-based FS compared with FV for caries control on FPM occlusal surfaces of children at high caries risk in Norway. A statistically significantly better effect of FS was found, although this was below the estimated level of 10% of clinical significance. This finding was consistent in sensitivity analyses. In addition, the NNT suggests that 25 FPMs need to be treated with FS for 1 additional FPM to get a successful outcome compared with FPMs receiving FV. This suggests that FS may be more effective than FV in maintaining caries control over the 36-mo period studied. However, the NNT of 25 is a relatively high number, questioning the superior clinical effectiveness of FS compared with FV. Therefore, the null hypothesis, which suggests no difference in effectiveness between the 2 treatments, can be rejected based on statistical, but not clinical, difference. To our knowledge, this is the first study comparing the effectiveness of FS and FV in real-life conditions.
The overall results are consistent with those previously reported from randomized controlled trials (RCTs), although few RCTs have directly compared FS and FV effects in occlusal caries management. A randomized, 2-arm clinical trial in Wales by Chestnutt, Playle, et al. (2017) showed no clinically important difference in the proportion of children developing decay, regardless of receiving FS or FV. A 3-arm RCT in Spain by Bravo et al. (2005), comparing caries-preventive effects of FS and FV in children aged 6 to 8 y over a 9-y period, showed a better treatment effect for FS than for FV at both 4 and 9 y of follow-up; however, the dropout rate was high. An RCT in China by Liu et al. (2012) investigated the effectiveness of FS, FV, and silver diamine fluoride in the permanent molars of schoolchildren. Their results showed that while the prevalence of dentin caries was significantly higher in controls than in the treatment groups, caries-preventive effects did not differ significantly among the groups.
To our knowledge, only 2 SMTs comparing FS and FV have been performed to date, and none with an observation period longer than 24 mo (Raadal et al. 1984; Splieth et al. 2001). Raadal et al. (1984) studied the efficacy of sealing FPMs (intact and with initial caries) in Norwegian children at ages 6 to 9 y who received a high standard of prophylactic care. The study reported a slightly greater reduction in caries increment with sealants, concluding that FS may benefit children with medium caries experience in primary teeth, whereas for those with low caries experience (<3 to 6 dmft), fissure caries may be successfully prevented by FV application every 6 mo, consistent with the findings from the present study.
In the present study, FPMs with initial caries at baseline were more likely to develop dentin caries or be restored after 36 mo, irrespective of method. This is consistent with results from Liu et al. (2012) showing that early caries at baseline is a risk factor for dentin caries, indicating progression differences between sound surfaces and those with initial caries.
Occlusal caries lesions can present a diagnostic challenge, especially in cases in which the occlusal tooth surface has no clinically visible continuity break in the enamel or radiographic evidence of caries but in which caries is suspected due to roughness, surface opacities, or staining (Makhija et al. 2012). Despite the generally acknowledged threshold of limiting operative treatment to lesions that penetrate dentin (Baelum 2008), dentists’ ability to preoperatively detect when this penetration has occurred is suboptimal (Gordan et al. 2010). Based on questionnaire studies, the proportion of dentists in Norway who would operatively treat occlusal caries lesions confined to enamel has decreased (Kopperud et al. 2016). Nevertheless, the possibility that some teeth with questionable occlusal lesions in the FV group were opened and restored unnecessarily cannot entirely be ruled out.
Evaluating the clinical relevance of clinical research is essential to simplify the translation of knowledge into practice (Armijo-Olivo et al. 2011). Clinical trials using a pragmatic approach are scarce within dentistry (Demarco et al. 2020). A pragmatic approach to observing which method is more effective under usual conditions can be considered highly relevant for daily practice in pediatric dental care. Because we permitted delivery flexibility, FS and FV application details were clinician dependent, as instructions on how to deliver the intervention was not rigidly prescriptive in the protocol. The primary outcome was chosen based on its obvious importance from the patient’s perspective: preventing invasive treatment. Children were recruited at their regular PDS appointments, and follow-up of participants was the same as in usual care.
The annual dropout rate was lower than anticipated, with 90% of the enrolled children completing the study. This may be because all children and adolescents in Norway are followed by PDS and therefore attend the clinics regularly. Although this led to an overpowered study sample in the present study, the finding will facilitate more precise estimates for planning future trials in PDS.
Involving 9 PDS clinics from 3 different counties in the trial increased the generalizability of the results, and the 36-mo observation period was longer than most RCTs to date. Nevertheless, implementing a pragmatically oriented clinical trial at PDS clinics, where the clinicians had little or no previous clinical research experience, also presented certain challenges. Moreover, COVID-19 restrictions affected and caused some deviations from planned follow-up routines, mainly related to the number of FV applications patients received. Suboptimal protocol adherence can challenge any long-term intervention in pragmatically oriented settings (Innes 2018); nevertheless, the ITT and PPT results in the present study were consistent. Pragmatic trials are important supplements to conventional RCTs in collecting evidence applicable to real-life settings, and the present findings are generalizable to children with high caries risk in similar dental settings.
Other logistical issues were slow recruitment and a frequent need for clarification of questionable and missing CRF data. However, through continuous contact with local administrators and clinics (i.e., meetings, phone calls) as well as biannual emailed information and feedback reports, we managed to collect data with few missing values. Another possible limitation was that patients were seen by several clinicians. Because of staff turnover and division of clinic responsibilities during the study period, only 34% of children were followed by the same clinician throughout the study. Although this is common practice in PDS in Norway, it might be speculated whether this could lead to diagnostic variation or affect choice of treatment. Nevertheless, adjusting for the effect of clinicians in multivariate analyses did not change the results.
The present study used an SMT design, which is well known in dentistry, to eliminate intersubject variability and reduce number of subjects needed for the trial (Pandis et al. 2017). The limitation of SMTs is a possibility of a carryover effect; however, elevated fluoride levels after FV application are mainly local without significant crossover effects (Sköld-Larsson et al. 2000). Due to the pragmatic nature of the study, the randomization procedure was simplified, and the possibility that clinicians might have chosen a tooth with lower severity cannot be completely ruled out. Involving the child in treatment selection of the particular FPM was chosen to increase randomness and to minimize this possibility.
Preventive care is more sustainable and less costly in comparison to restorative and surgical treatment (Kashbour et al. 2020). Nevertheless, to determine whether FS or FV is most cost-effective for caries control is challenging, due to heterogeneity of settings, populations, and study designs (Neidell et al. 2016; Chestnutt, Hutchings, et al. 2017; Khouja and Smith 2018; Kashbour et al. 2020). Exploratory analysis in the present study revealed that approximately 34.8% of FPMs treated with FS received additional FV applications. This combination of FV and FS was unanticipated and would increase FS costs in general practice. Further studies are needed to assess the extent of this practice across settings.
This practice-based study compared 2 of the most frequently used methods for occlusal caries management in general practice and attempted to bridge the gap between strictly controlled trial designs and caries management in a practice-based PDS setting. The findings indicate that FS performed only marginally better than did FV did, calling into question current recommendations of using FS as a first choice for occlusal caries management in Norwegian national guidelines on dental care for children and adolescents (Norwegian Directorate of Health 2022).
Conclusion
In the population studied, the clinical effectiveness of FS was statistically significantly higher compared with FV. However, this difference was below the estimated minimal clinically important difference of 10%.
Author Contributions
M.-M. Uhlen-Strand, L. Stangvaltaite-Mouhat, I. Mdala, contributed to data analysis and interpretation, drafted and critically revised the manuscript; I. Volden Klepaker, contributed to conception, data acquisition and interpretation, critically revised the manuscript; N.J. Wang, contributed to conception, design, data acquisition, critically revised the manuscript; R. Skudutyte-Rysstad, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345241248630 – Supplemental material for Fissure Sealants or Fluoride Varnish? A Randomized Pragmatic Split-Mouth Trial
Supplemental material, sj-docx-1-jdr-10.1177_00220345241248630 for Fissure Sealants or Fluoride Varnish? A Randomized Pragmatic Split-Mouth Trial by M.-M. Uhlen-Strand, L. Stangvaltaite-Mouhat, I. Mdala, I. Volden Klepaker, N.J. Wang and R. Skudutyte-Rysstad in Journal of Dental Research
Footnotes
Acknowledgements
The authors would like to express their gratitude to Erica Ponzi, statistician at Oslo Centre for Biostatistics and Epidemiology (OCBE), for quality assurance on statistical analyses and interpretation of the results. Clinical personnel in the PDS are acknowledged for their contribution to the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.