
Abstract
Adequate and transparent reporting is necessary for critically appraising published research. Yet, ample evidence suggests that the design, conduct, analysis, interpretation, and reporting of oral health research could be greatly improved. Accordingly, the Task Force on Design and Analysis in Oral Health Research—statisticians and trialists from academia and industry—identified the minimum information needed to report and evaluate observational studies and clinical trials in oral health: the OHStat Guidelines. Drafts were circulated to the editors of 85 oral health journals and to Task Force members and sponsors and discussed at a December 2020 workshop attended by 49 researchers. The guidelines were subsequently revised by the Task Force’s writing group. The guidelines draw heavily from the Consolidated Standards for Reporting Trials (CONSORT), Strengthening the Reporting of Observational Studies in Epidemiology (STROBE), and CONSORT harms guidelines and incorporate the SAMPL guidelines for reporting statistics, the CLIP principles for documenting images, and the GRADE indicating the quality of evidence. The guidelines also recommend reporting estimates in clinically meaningful units using confidence intervals, rather than relying on P values. In addition, OHStat introduces 7 new guidelines that concern the text itself, such as checking the congruence between abstract and text, structuring the discussion, and listing conclusions to make them more specific. OHStat does not replace other reporting guidelines; it incorporates those most relevant to dental research into a single document. Manuscripts using the OHStat guidelines will provide more information specific to oral health research.
Keywords
Introduction
Ample evidence suggests that oral health researchers would do well to improve the reporting of their studies. “Large proportions of articles contain errors in the application, analysis, interpretation, or reporting of statistics or in the design or conduct of research” (Lang and Altman 2013). Oral health clinicians cannot critically appraise the literature without adequate and transparent reporting.
Although oral health research is similar to clinical research in other fields, many dental studies have design characteristics that can confound analysis. For example, the unit of analysis can be a single tooth, multiple teeth, individual tooth sites, or a single patient. In longitudinal studies, teeth can be lost without disqualifying the participant from the study, and perhaps uniquely in human research, observational units may be added through the primary and permanent dentition process. Oral health studies sometimes incorporate within-person designs. Examples include split-mouth studies—in which patients receive all the interventions but in different portions of the dentition—or crossover studies—in which patients are randomly assigned to different sequences of interventions. These and other situations common in oral health research can make design and analysis complex.
One approach to improving reporting is the use of a checklist when preparing a manuscript (Lang and Secic 2006; Council of Science Editors 2015; Christiansen et al. 2020). In 1996, the Consolidated Standards for Reporting Trials (CONSORT) was published (Begg et al. 1996), and subsequent improvements, extensions, and elaborations have since proliferated. The EQUATOR Network website lists more than 575 checklists (University of Oxford Center for Statistics in Medicine n.d.). The aim of the Task Force writing group was to unify the guidance for observational studies and clinical trials into a single tool for oral health researchers for inclusion and dissemination within the EQUATOR network (University of Oxford Center for Statistics in Medicine n.d.).
Methods
In light of the American Statistical Association’s 2016 “Statement on P-Values” (Wasserstein and Lazar 2016) and the subsequent publication of an issue of The American Statistician devoted to “Moving to a World Beyond ‘P < 0.05’” (Wasserstein et al. 2019), several journals revised their reporting standards.(Moher 2009; Armstrong et al. 2011; Hickey et al. 2015; Hollestein and Nijsten 2015; Levesque 2015; Munafo and Wileyto 2015; Gamble et al. 2017; Curtis et al. 2018; Jones et al. 2018; Lindsey et al. 2018; Assel et al. 2019; Butcher et al. 2019; Harrington et al. 2019; Parsons et al. 2019; Kattan and Vickers 2020; Michel et al. 2020; Wilson and Falcone 2020). At the August 2019 Editorial Board meeting of The Journal of the American Dental Association, board members proposed convening a working group to improve the statistical reporting guidelines of the Journal. To support the effort, a proposal was submitted to the Task Force on Design and Analysis in Oral Health Research—a nonprofit group composed of statisticians and trialists in the public and private sectors (Task Force on Design n.d.). In November, the Task Force Board empaneled a writing group to develop a set of methodological and statistical reporting guidelines.
On December 10, 2019, the Task Force writing group began to meet online to draft new guidelines. When consensus was reached, the plan was to convene a face-to-face meeting in May 2020, but the COVID-19 pandemic made the meeting impossible. Instead, comments were solicited on draft circulated by email.
In November 2020, the Task Force writing group distributed the draft to more than 85 editors of oral health journals and to all members and sponsors of the Task Force. Subsequently, written comments were received from 12 reviewers. The December 2020 online workshop included an overview presentation (A.B.) and 3 detailed critiques by the past editor of JADA, the present editor of the Journal of Dental Research, and an internal Task Force reviewer. The comments and critiques were extensive. The Task Force brought in a consultant in scientific publications with experience in preparing reporting guidelines and the associated documents (T.A.L.). The goal was to incorporate the comments and critiques into 2 manuscripts: an overview statement that introduced the checklist (OHStat: the Oral Health Statistical reporting guidelines) and an “Explanation and Elaboration” manuscript (the “E&E paper”) that gave the background of the initiative and the rationale for including each guideline. The manuscripts were then reviewed by the writing group and approved by the Task Force in September 2021 for eventual publication in the peer-reviewed literature. In 2022, the manuscripts were submitted for review and revisions made.
The Oral Health Statistical Reporting Guidelines
The OHStat checklist is recommended for reporting key aspects of most observational studies and clinical trials in oral health. The 48 guidelines were formulated for authors, reviewers, and journal editors to improve reporting of observational studies and clinical trials (both randomized and nonrandomized trials) involving human participants evaluating an oral health–related biomedical or behavioral outcome (U.S. National Institutes of Health 2014). Many of the 48 OHStat guidelines are more focused or homogeneous, which increases the number of items but makes it easier to determine whether an individual guideline has been addressed. In contrast, the 25 CONSORT guidelines are more heterogeneous; they actually ask authors to respond to 53 questions. The same is true of the 22 Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, which ask 33 questions.
We strongly recommend that the checklist be used in conjunction with the explanation and elaboration paper (Best et al. 2024) because each item has important clarifications. Most of the major reporting guidelines and extensions are accompanied by E&E papers—for example, CONSORT for reporting randomized controlled trials (RCTs) generally (Moher et al. 2012) and HARMS for reporting adverse outcomes specifically (Junqueira et al. 2023), STROBE for observational studies (Vandenbroucke et al. 2007), STARD for diagnostic tests (Cohen et al. 2021), PRISMA for systematic reviews (Page et al. 2021), and ARRIVE for animal studies (du Sert et al. 2020). As the foundation of the OHstat guidelines, the E&E paper has several purposes:
It documents the need for better reporting of research in the oral health literature.
It expands and explains each guideline and cites supporting references.
It explains why each guideline is important.
It calls attention to aspects unique in oral health research, such as split-mouth studies and the effect of natural changes in dentition.
It addresses multiplicity in oral health measures, or the complexity that arises from measuring multiple teeth or sites in the oral cavity.
It makes the case for using modern multivariable and multivariate statistical methods.
It identifies preferred practices in both research and reporting, such as why estimates and confidence intervals are increasingly being preferred to P values for reporting results.
It presents several examples of good and poor research practices, including common errors.
It calls attention to specific problems in the literature, such as image manipulation and the insufficient reporting of harms.
It introduces new guidelines to help authors write and review their manuscripts before submittal.
It includes additional information on preparing tables, figures, and images.
It can serve as excellent overview and summary text of the key elements of oral health research.
It can be useful checklist for planning oral health research protocols.
Importantly, the guidelines identify the minimum requirements for reporting and publishing observational studies and clinical trials in oral health. Additional information may be needed to adequately report individual studies. Note that guidelines highlighted in boldface specifically apply to clinical trials but may also be applicable in observational studies (Table).
The OHStat Checklist for Reporting Oral Health Research.
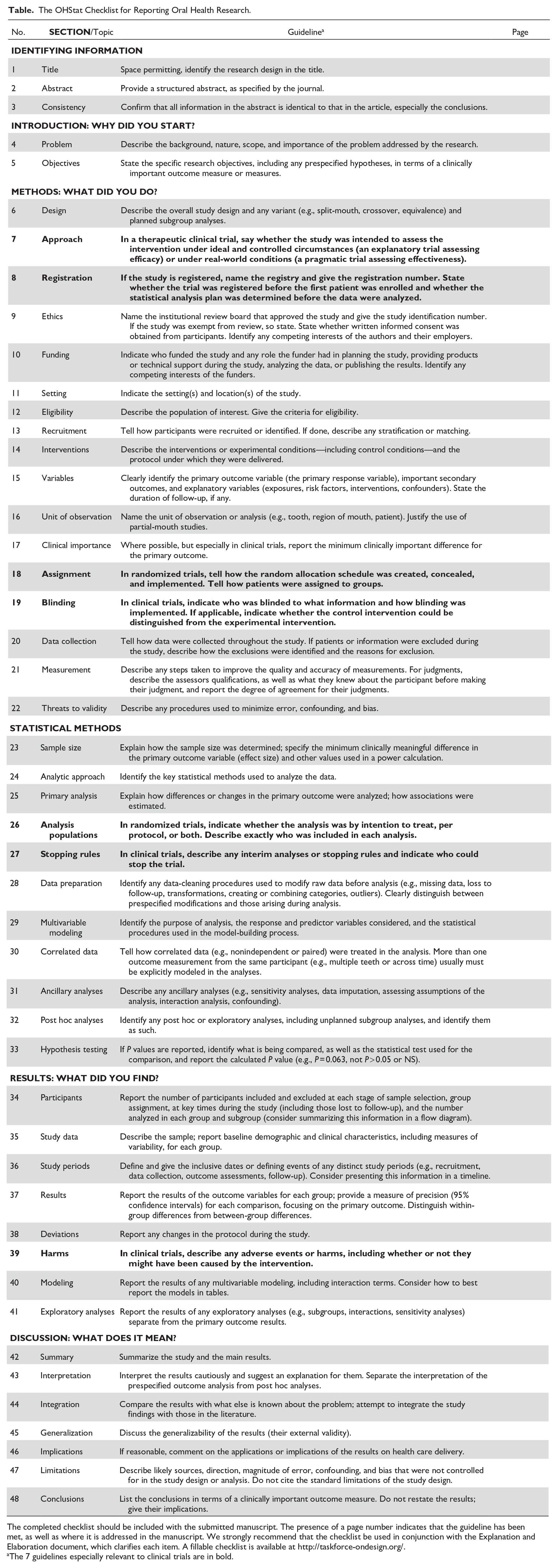
The completed checklist should be included with the submitted manuscript. The presence of a page number indicates that the guideline has been met, as well as where it is addressed in the manuscript. We strongly recommend that the checklist be used in conjunction with the Explanation and Elaboration document, which clarifies each item. A fillable checklist is available at http://taskforce-ondesign.org/.
The 7 guidelines especially relevant to clinical trials are in bold.
The checklist is intended to accompany a manuscript submitted for publication. In the right-hand column of the checklist, indicate the page number of the manuscript on which the guideline is addressed. When an item does not apply, N/A is a suitable response. In addition to helping authors and journal editors confirm that the manuscript contains the necessary information, the checklist will also help reviewers find specific information more easily.
Additional guidance for both documenting research and preparing manuscripts for publication can be found in the AMA Manual of Style and in Scientific Style and Format.
Discussion
Critical appraisal and interpretation of observational studies and clinical trials in oral health will improve with better reporting of the details that support study validity. Obviously, no checklist can address all the important factors of every research design, and articles providing all the indicated information could still be substandard. The guidelines do not ensure the quality of reporting. So, by all means, “Break any of the guidelines if it makes scientific sense to do so” (Assel et al. 2019). Accuracy and transparency are more important than trying to fit an unusual situation into a generic guideline.
The guidelines should not be used to evaluate the quality of oral health studies. The proportion of adequately addressed items is not a surrogate endpoint for study quality. Not all items are equally important, and reporting the required information is no guarantee of quality.
Limitations
The OHStat guidelines do not cover all study designs. Examples of unaddressed designs include systematic reviews and meta-analyses (Page et al. 2021), the performance characteristics of diagnostic tests (Bossuyt et al. 2015), equivalence or noninferiority studies (Piaggio et al. 2012), and comparative effectiveness studies using large databases (Ogrinc et al. 2016).
Conclusion
Evidence-based dentistry is literature-based dentistry (Lang 2010). Clinicians, authors, reviewers, and editors should take the time to learn how to accurately report and assess the validity, relevance, and implications of the published literature. The Cochrane Center is the premier site for systematic reviews in health care (The Cochrane Collaboration n.d.). Sites such as the ADA Center for Evidence-Based Dentistry (Center for Evidence-Based Medicine n.d.) and the University of Dundee Centre for Evidence-Based Dentistry (University of Dundee, School of Dentistry n.d.) make it easy to find clinical guidelines. Such guidelines are based directly on the existing evidence and on the ability to appraise that evidence through the process of critical appraisal.
Ultimately, patient care is improved when valid and useful research is planned, executed, communicated to practitioners, and widely implemented. Therefore, we also expect that the OHStat guidelines will serve as a template for updating and informing improvement in oral health research reporting.
Author Contributions
A.M. Best and T.A. Lang contributed to the conception and design of the guidelines, took the lead in organizing, drafting, and documenting the original manuscript, and incorporated comments and insights from the other authors. J.C. Gunsolley, E. Ioannidou, and B.L. Greenberg contributed to the conception of the guidelines, critically appraised each revision, and provided substantive comments and insights throughout the development process. All authors agree to be accountable for all aspects of the work and approved the final draft for publication.
Footnotes
Disclaimer
This article was written and approved by the writing group authors, who take sole responsibility for the final content. The views expressed do not represent the policies, views, or opinions of the authors’ institutions.
Task Force Writing Group
A.M. Best, Virginia Commonwealth University; B.L. Pihlstrom, University of Minnesota; D.V. Dawson, University of Iowa; B.L. Greenberg, New York Medical College; E. Ioannidou, University of Connecticut; J.C. Gunsolley, Virginia Commonwealth University; J.S. Hodges, University of Minnesota; and T.A. Lang, University of Chicago Medical Writing Program. P.B. Imrey, Cleveland Clinic and Case Western Reserve University, also provided suggested revisions and performed comprehensive reviews.
Reviews
Substantial written critiques were also provided by M. Glick, JADA Editor; N.S. Jakubovics, JDR Editor; W.M. Thomson, Community Dentistry and Oral Epidemiology Editor; B.S. Michalowicz, University of Minnesota; L.N. Borrell, Community Dentistry and Oral Epidemiology Associate Editor and City University New York; J.M. Grender and J. DiGennaro, Procter and Gamble; M.J. Hayat, Georgia State University; R. Brignardello-Petersen, McMaster University; P.B. Imrey, Cleveland Clinic and Case Western Reserve University; D. Wu, University of North Carolina; P.G. Robinson and T. Walsh, Community Dental Health Journal; and K. Divaris, University of North Carolina. Five anonymous reviewers also submitted comments and suggestions. We gratefully acknowledge their contributions; the final manuscript does not necessarily reflect either their views or the official policy of the organizations they represent.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE unified competing interest form, a copy of which is available from the corresponding author.
To encourage dissemination of the OHStat Statement, this article and the checklist is freely available on ![]() . This article has been simultaneously copublished in the Journal of Dental Research, The Journal of the American Dental Association, The Angle Orthodontist, the Journal of Oral and Maxillofacial Surgery, and the Journal of Endodontics. The articles are identical except for minor stylistic and spelling differences in keeping with each journal’s style. Any of those journal’s citations can be used when citing this article.
. This article has been simultaneously copublished in the Journal of Dental Research, The Journal of the American Dental Association, The Angle Orthodontist, the Journal of Oral and Maxillofacial Surgery, and the Journal of Endodontics. The articles are identical except for minor stylistic and spelling differences in keeping with each journal’s style. Any of those journal’s citations can be used when citing this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Task Force on Design and Analysis in Oral Health Research provided funding for the December 2020 meeting and provided support for the consultant (T.L.). A.B. received funding for travel related to the December 2020 meeting. None of the Task Force sponsors were involved in the planning, execution, or writing of the OHStat documents. Additionally, no funder helped to draft or approve of the manuscript.