
Abstract
Choosing hypodontia treatment requires young people and parents to consider a large amount of information, identify what is important to them, and make trade-offs between options. This study aimed to examine young people and parents’ preferences for hypodontia treatment using discrete choice experiment (DCE). This was a cross-sectional survey of young people (12–16 y) with hypodontia of any severity, at any stage of treatment, and their parents. Participants were recruited from NHS Hospitals in England and Wales. A bespoke DCE questionnaire was developed to measure preferences for 6 attributes of hypodontia treatment (waiting time, treatment time, problems during treatment, discomfort during treatment, bite, appearance). The questionnaire was completed 1) online by young people and parents, individually or together, and 2) by child–parent dyads under observation. Preferences were analyzed using regression models. In total, 204 participants (122 young people, 56 parents, 26 dyads) completed the online questionnaire and 15 child–parent dyads completed the questionnaire under observation. The most important attribute in hypodontia treatment was improvement in appearance, but significant heterogeneity was found in preferences. Four distinct groups of participants were found: group 1 (39%): severe discomfort and problems were most important; group 2 (31%): most concerned about improvement in appearance of teeth and improvement in bite; group 3 (22%): appearance 3 times more important than any other attribute; and group 4 (9%): preferences difficult to interpret. There was variation in how child–parent dyads approached decision-making, with some negotiating joint preferences, while for others, one individual dominated. Making trade-offs in DCE tasks helped some people think about treatment and identify their preferences. Appearance is an important outcome from hypodontia treatment, but preferences vary and potential risks and functional outcome are also important to some people. There is a notable level of uncertainty in decision-making, which suggests further shared decision support would be valuable.
Introduction
To date, hypodontia research has largely focused on clinical outcomes and aesthetic outcome from different treatments (Barber, Bekker, Meads, et al. 2018). Little is known about young people and parents’ preferences for dental treatment for hypodontia or the decision-making process. Establishing preferences is fundamental to informed patient choice and the delivery of person-centered care (National Institute for Health and Care Excellence [NICE] 2021). Choosing the “right” treatment requires those affected by hypodontia to consider a large amount of information, identify what is important to them, and make trade-offs between treatment options.
Discrete choice experiments (DCEs) are a stated preference method that use hypothetical scenarios to examine choice behavior. DCEs present 2 or more alternatives in choice tasks, which describe the service/treatment in terms of its constituent attributes. In each choice task, the alternatives presented have varying attribute levels. DCEs are based on utility maximization theory, which believes that when people make choices, they select the option for which they derive the most benefit (utility). It is assumed the value of an option is the weighted sum of all attributes, so people will make trade-offs that sacrifice less important attributes for gains in the attributes they perceive to be of most value (de Bekker-Grob et al. 2012). DCEs can be used to measure the relative strength of preference for different attribute levels and to understand respondents’ willingness to trade off between different attributes.
DCEs are increasingly being used in health care. A systematic review found health care DCEs were used to elicit patient preferences for services and treatments, to value health outcomes, to examine trade-offs between experience and outcomes, and to set priorities. Commonly used attributes were cost, time, risk, health care, and health status. There is increasing use of online surveys to administer the DCEs due to their ability to reach more people (Clark et al. 2014).
This research aimed to 1) use DCE to elicit young people and parents’ preferences for hypodontia treatment and 2) explore how young people and their parents make decisions individually and together and the value of trade-off tasks in decision-making.
Design
Cross-sectional using mixed methods:
Online DCE questionnaire to elicit preferences from young people with hypodontia and parents
Qualitative observation of child–parent dyads completing a DCE questionnaire, individually and together
Representatives from the target population were involved in all stages of research design and delivery. Ethical approval was granted by the North West Lancaster Ethic Research Committee (Reference 15/NW/0804).
The target population was 1) young people aged 12 to 16 y with hypodontia of any severity, at any stage of dental treatment (pretreatment, in active treatment, or completed all treatment), and 2) parents (any person with a carer role) of a child with hypodontia. Participants were recruited from NHS hospitals across England and Wales, including dental hospitals, teaching hospitals, and district general hospitals with good geographical spread.
Materials and Methods
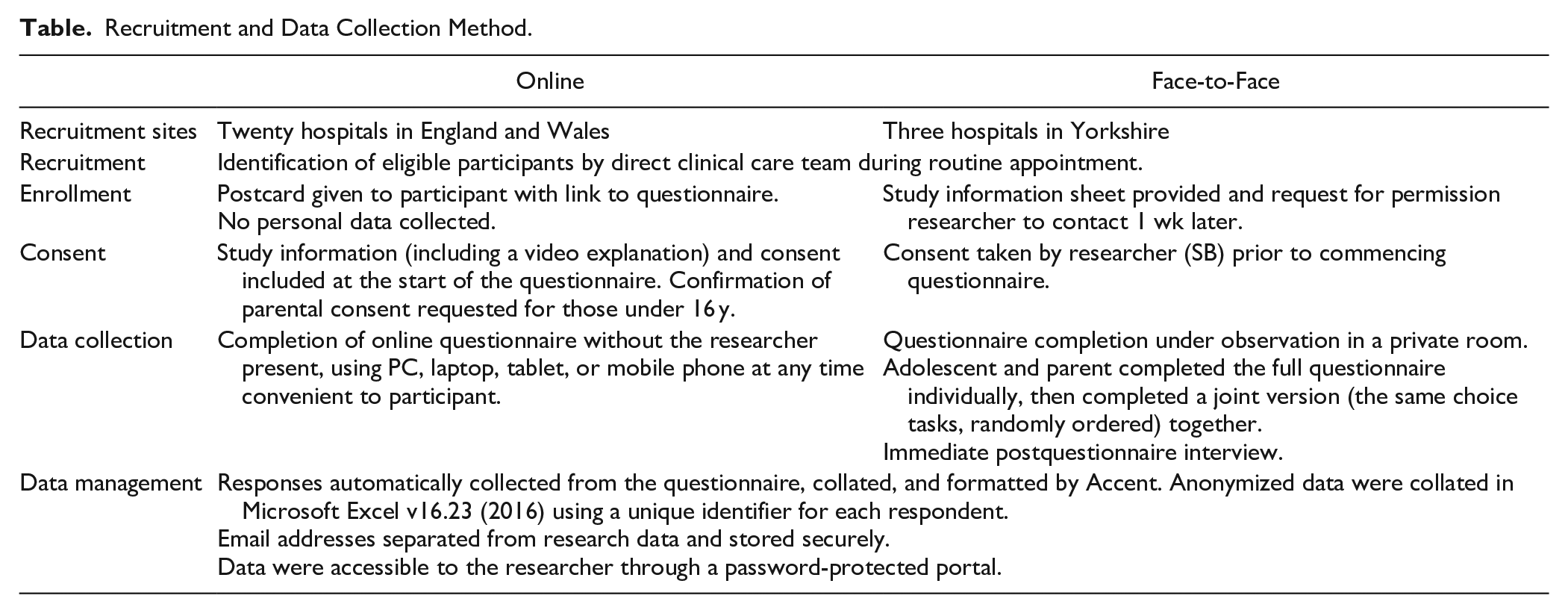
Recruitment and data collection methods are outlined in the Table 1. For the face-to-face method, a researcher (SB) passively observed completion of the questionnaire by both the adolescent and parent, individually and then again together. A short postquestionnaire interview was then conducted to explore participants’ experience of completing the DCE choice tasks. Notes were made about observed behavior and responses to interview questions, and the session was audio-recorded.
Recruitment and Data Collection Method.
DCE questionnaire development and testing followed best practice guidance (Bridges et al. 2011; Reed Johnson et al. 2013; Hauber et al. 2016), including qualitative methods (Coast et al. 2012; Vass et al. 2017). The development and testing process has been fully described (Barber, Bekker, Marti, et al. 2018) and is summarized in Appendix Table 1.
The questionnaire included the following:
Demographics: age, gender, ethnicity, number of missing teeth, stage of treatment
Seven DCE choice tasks plus 1 repeat task
Certainty in decision-making using the SURE Tool (Légaré et al. 2010), dental anxiety, and impact of hypodontia on OHRQoL (Akram et al. 2011)
DCE choice tasks contained 6 attributes, each with 2 to 3 levels (Appendix Table 2) that varied within and across each choice task. An explanation was given prior to choice tasks with a nondental example and instructions for completion. Description of attribute levels was given before and within the tasks. Paired profiles with generic labeling (treatment A/treatment B) were used. Participants were asked to read through the 2 options and then decide which they liked best. A “no treatment” option was included to reflect real life, but this was after the forced choice to prevent the optout being used to avoid difficult trade-offs (Lancsar and Louviere 2008). An example choice task is given in Figure 1. The full questionnaire is included in the Appendix.
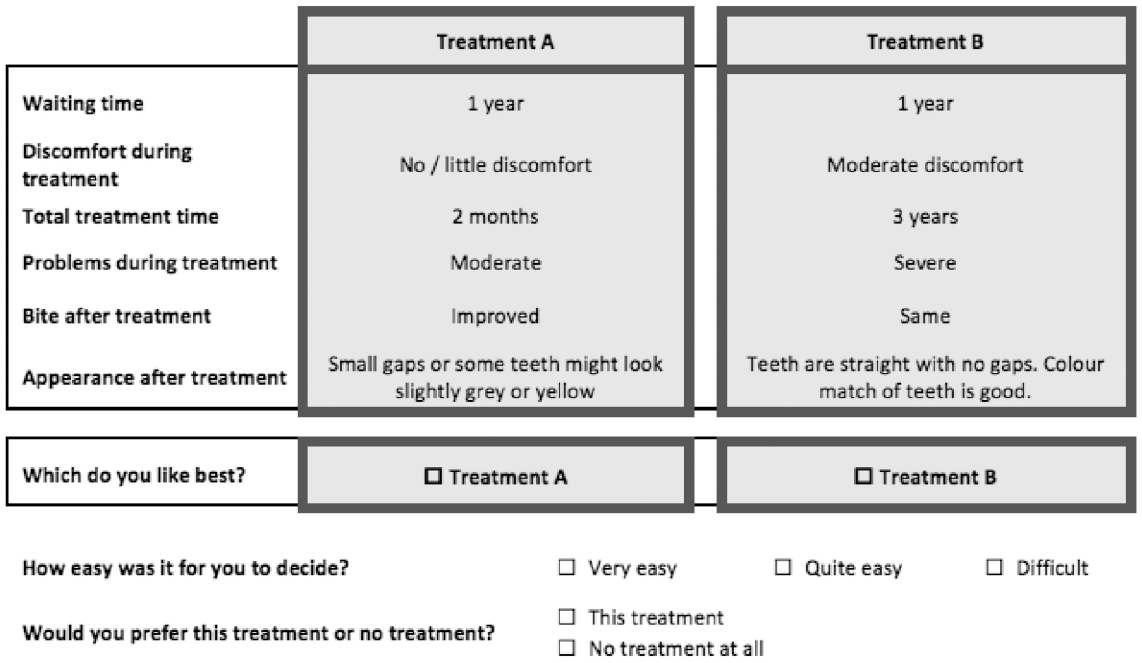
Example of a discrete choice experiment choice task.
Sample Size
For DCEs, the sample size reflects the number of observations, calculated from the number of participants and choice tasks. Using a recommended minimum sample size formula for aggregate-level full profile (Orme 2016), the estimated sample size was 80 per group.
Data Analysis
Descriptive sample characteristics
Logistic regression to examine the association between respondent characteristics and selection of “no treatment.”
Preferences were analyzed using Stata/IC v13.1 (StataCorp). The mixed logit model without correlation provided the best fit to the data using AIC/BIC (Hauber et al. 2016), so this was used to calculate preference weights (regression β-coefficients) for attribute levels.
Significant preference heterogeneity was found, so a latent class analysis was undertaken to identify distinct groups with similar preferences. Output from the latent class model included the probability for each respondent to belong to each of the groups, which was used to allocate respondents to classes and then identify whether respondent characteristics were associated with predicted class membership.
Observations and interview feedback were analyzed by reading the observation notes and reviewing audio-recordings. Notes were made about the behavior and experience of individuals and dyads, and then these were compared to identify similarities and differences. Findings were described in relation to the approach to joint preference elicitation and respondents’ perception of trade-off tasks with illustrative quotes.
Results
The online questionnaire was conducted between May and December 2018 (n = 204) and the observed questionnaire from June 2018 to January 2019 (n = 30). Due to the number of people and sites involved in recruitment, it was not feasible to record uptake to calculate response rate.
Average questionnaire completion time by respondents was 15 min. Eighteen online respondents (14 young people, 3 parents, 1 child–parent dyad) completed the questionnaire in less than 6 min, which was judged to be the minimum valid time, so these responses were removed. Sensitivity analysis indicated this had minimal effect on preference estimates. No responses suggested task nonattendance based on choosing either A or B in every task. The final sample for analysis included 216 respondents providing 1,512 observations (Appendix Fig. 1).
Sample characteristics are given in Appendix Table 3. The proportion of mild (45%), moderate (34%), and severe (21%) hypodontia is not reflective of the usual distribution of hypodontia. The sample was principally White (96%). Parents were mostly mothers (84%), and 20 parents (28%) reported having hypodontia themselves.
Self-reported certainty in decision-making suggested people were most confident about having enough advice and support but less confident about knowing risks and benefits and which are most important to them (Appendix Fig. 2). More young people reported anxiety related to hypodontia treatment (47%) than routine dental treatment (30%) (Appendix Fig. 3). The reported impact of hypodontia on OHRQoL was highest in relation to “confidence to smile” and “worry in the future,” while functional issues related to eating, speaking, and brushing were reported less frequently (Appendix Fig. 4).
Preferences for Hypodontia Treatment
The mixed logit model found all attribute levels had the expected impact on utility except moderate discomfort and moderate problems (Fig. 2). The greatest drivers of preference were suboptimal appearance and then severe problems, followed by a 5-y treatment time and severe discomfort. A segmented analysis was undertaken to examine whether preferences vary between those who are treatment naive (pretreatment, n = 69) and those with experience of treatment (in-treatment and posttreatment, n = 147) (Appendix Fig. 5). The pretreatment sample is relatively small and confidence intervals are wide, so caution must be used when interpreting the results, but it appears that that those who have not experienced treatment expect it to be worse than it turns out to be, whereas those with experience of treatment rate discomfort and problems as less important.
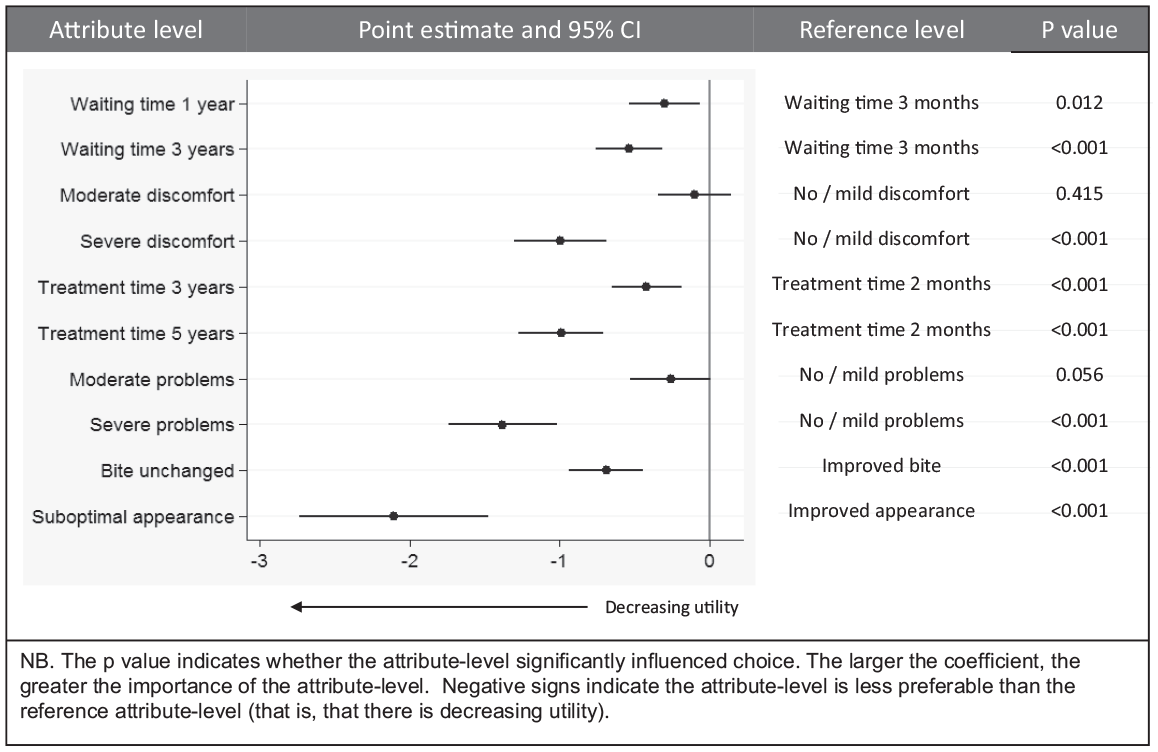
Preference weights estimates for attributes of hypodontia care relative to the reference level estimated using the mixed logit.
Calculation of distribution curves for each of the attribute levels (Revelt and Train 2000) identified significant heterogeneity in preferences (Appendix Fig. 6). For this reason, latent class analysis was performed. Four distinct groups of respondents with similar preferences were found (Fig. 3):
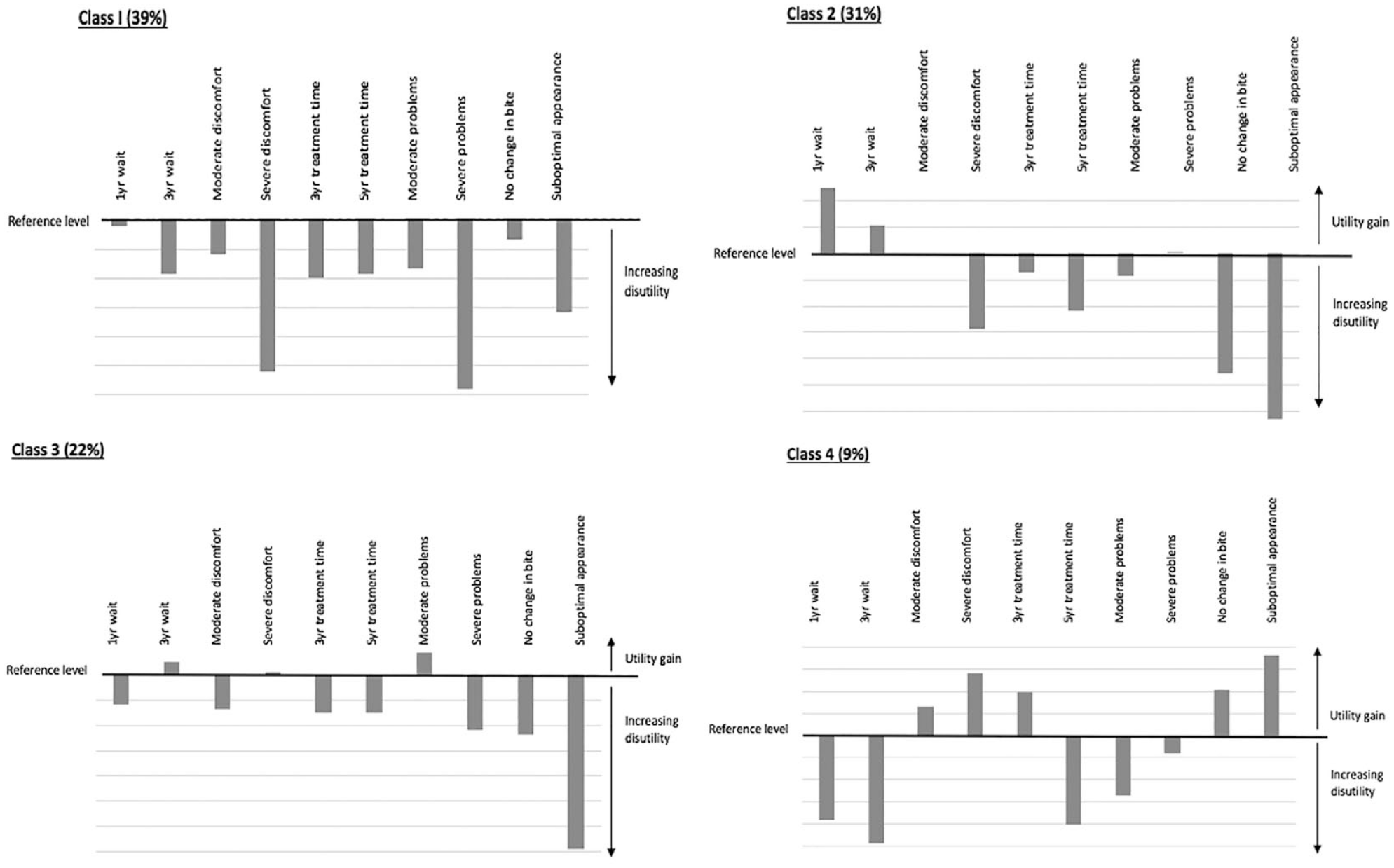
Summary of preferences of respondents in the 4 latent class groups. Preference weights derived from the latent class model cannot be compared across classes due to potential differences in scale parameter; hence, preference weights should only be used only to compare preferences within the class.
Examination of predicted membership did not identify any significant associations between respondent characteristics and likelihood of belonging to a certain group. This may be due to the small sample size of subgroups.
Examination of the selection of “no treatment” found the majority of respondents (58%) did not opt out of treatment in any tasks, while 12 respondents (5%) selected “no treatment” in all choice tasks. In total, “no treatment” was selected in 18% of all tasks. The odds of opting out were higher for those with mild hypodontia, dental anxiety, males, parents, online respondents, and, unexpectedly, those with a high quality-of-life impact from hypodontia (Appendix Table 3).
Decision-Making Process
Individual engagement with tasks appeared to be primarily related to how challenging respondents found the choice task, and some admitted trade-offs were challenging.
It’s like being asked would you rather be eaten by a lion or a tiger. (Father)
Parents were generally more analytic and deliberative in approach, while young people appeared more heuristic in their response, often making a quicker decision based on 1 attribute.
I don’t care as long as it looks OK. (15-y-old male with severe hypodontia, mid-treatment)
Parents would more often pick an optout, whereas young people often felt they “needed” treatment so were reluctant to opt out.
Anything is better than how they are. I’d never pick nothing ’cos then I’d be stuck with my teeth like this. (16-y-old female with mild hypodontia, pretreatment)
One parent discussed that because she does not understand how the bite feels, it was difficult to value it changing.
I guess because I can’t feel the bite and she eats everything, I don’t really see it as a problem. I can’t imagine how it would change or that it really matters. (Mother)
Observation of the dyadic interaction for negotiation of joint preferences identified 2 different approaches: “mutual negotiation,” where there was a collaborative approach to selecting a joint preference, and “dominant respondent,” where 1 participant selected their preferred choice (Fig. 4). There was no apparent association between the approach taken and individual respondent characteristics.
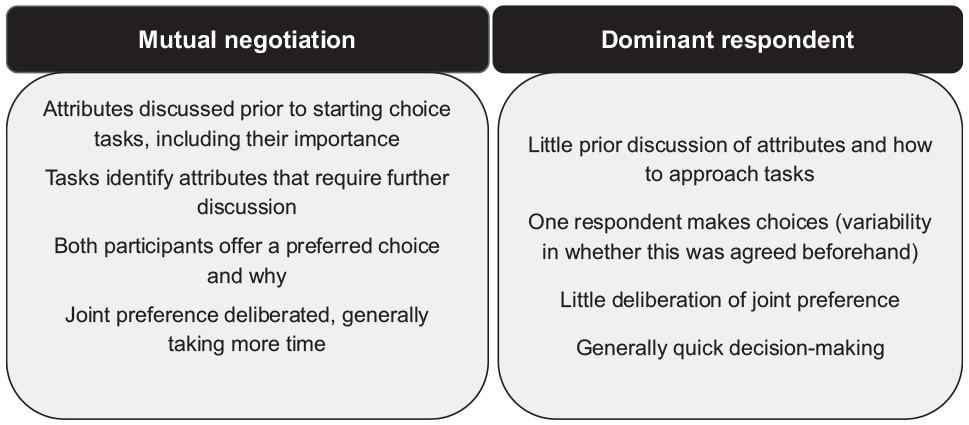
Characteristics of dyadic approaches to joint preference selection.
Choices in individual and joint DCE choice tasks for the 15 observed dyads were directly compared. Approximately half the dyads (52%) selected the same alternative when completing the choice tasks individually and together. Where individual choices differed, the joint choice matched the young person’s choice in 22 tasks (18%), parent’s choice in 28 tasks (23%), and was a new choice for both in 8 tasks (7%). Observation suggested young people and parents may select the same option for different reasons. An individual with a strong preference for a specific attribute was often keen to promote this attribute, but greater deliberation did not necessarily change preferences.
Observed and reported effect of completing trade-off tasks varied across the respondents. Some reported finding the choice tasks useful and described a change in their approach to thinking about options. This tended to be those who reported they were unsure which treatment to choose prior to completing the questionnaire and wanted to find out more about treatment and those who were interested in the research method.
Completing the choice tasks was reported to help facilitate an exchange of knowledge and understanding between the young person and parent. The conversation included discussion about what was important and coping with treatment: I didn’t realise she’s such a tough little thing. (Mother)
Talking through the task information helped respondents explore their understanding of the information and identify their limits: That’s not likely to happen . . . you only “might have” problems. (Mother) Severe discomfort for 5 years, that’s a no. (14-y-old female with moderate hypodontia, pretreatment)
Challenges in the task design were identified—namely, respondents did not believe the attribute level existed, or they felt the attributes were inherently related so some choice tasks were not realistic: . . . but it always hurts. (14-y-old female with severe hypodontia, mid-treatment) How could you have severe problems and minor discomfort? To me that doesn’t make sense. (Father)
Some young people reported uncertainty about the usefulness of the DCE as a decision support tool because they already had a strong preference for a single attribute and they were sure of their treatment decision. A small group of respondents reported to not find the tasks useful because they did not see the real-life treatment choice as a decision between options where trade-offs are needed. In some cases, there was evidence of vacillation without progress toward a decision. This may reflect the group whose preferences were allocated to group 4.
Discussion
This is the first published DCE study to elicit child–parent dyadic preferences, individually and together. Previous dyadic DCE studies are limited to adult couples (Beharry-Borg et al. 2009) and child–parent dyads where respondents answered separately (Bray et al. 2016) or parents answered on behalf of their child (Brown et al. 2010; Lloyd et al. 2011; Waschbusch et al. 2011). Our novel approach proved valuable in getting a better understanding of preferences and the value of trade-off tasks for helping people identify their own preferences. Understanding preferences of young people and their parents, and examining how dyads interact, is important for helping multiple stakeholders recognize each other’s perspective. Discordant or ambiguous preferences may contribute to decisional conflict (Légaré et al. 2012) and uninformed care choices, resulting in dissatisfaction with the treatment process or outcome (Mulley at al. 2012). Finding ways to systematically reason about different preferences within consultations may enable more shared decisions about treatment.
In this sample, appearance was the most important attribute in hypodontia treatment. The impact of compromised dental appearance on OHRQoL in people with hypodontia is widely reported (Laing et al. 2010; Meaney et al. 2012). Examination of preference heterogeneity, however, demonstrated that appearance is not the only important attribute. For a large group of people (group 1, 39%), appearance was less important than potential complications during treatment, while for others (group 2, 31%), improvement in function was equally important as dental appearance. In this sample, 70% of respondents reported some degree of functional concern related to their hypodontia, which aligns with functional limitations reported in previous studies (Wong et al. 2006; Locker et al. 2010).
Evidence of preference heterogeneity emphasizes the need to elicit what is important from every individual to support discussion of options, risks, and consequences in a meaningful way (NICE 2021). Risk discussion is complicated by variation in an individual’s perception and tolerance of risk, the nature and consequence of the risk, and how this risk is understood (Price 2017). Information used by health professionals to support their clinical reasoning may differ from the information required by patients to reach an informed choice (Breckenridge et al. 2015).
No accurate data could be found about real-life uptake of dental treatment by people with hypodontia and how treatment decisions, including the uptake of treatment, vary across different conditions, societies, and health care systems. In this sample, “no treatment” was selected in nearly a fifth of tasks and a minority opted out in all tasks, suggesting respondents felt the treatment options in the choice task were insufficiently beneficial. Most participants in this sample had, however, chosen to undergo dental treatment, which may indicate young people and parents are not fully aware of the attributes of own treatment or that they have not considered treatment with such an explicit risk-benefit approach.
A notable level of self-reported uncertainty arounddecision-making for hypodontia was found, particularly the risks and benefits of options and whether people felt they know what is important to them. There is little existing literature about decisional uncertainty in hypodontia or other craniofacial conditions. Making trade-offs appeared to help some individuals think about and discuss treatment in a different way, identify their own preferences, and understand their own willingness to accept a compromise between process and outcome. The usefulness of trade-off tasks in decision support tools is recognized (IPDAS, 2017), and some people reported trade-off tasks facilitated deliberation, leading to crystallization of preferences. Future research should examine how such methods can be used across dental treatments to improve understanding of treatment, increase satisfaction with choices, and increase adherence. For other respondents, however, the tasks appeared to cause vacillation, and preference analysis identified a distinct group of people for whom preference estimates were ambiguous. This may be people who were not interested in the research, but it might also represent those who lacked a clear preference, who experienced difficulties in assimilating the information, or who have low health literacy. This group of people may require additional decision support such as decision coaching or question prompt lists (Stacey et al. 2017).
A limitation of this study is that the sample is not representative, with a higher representation of severe hypodontia and predominantly White respondents (96% compared to 87% White UK population), which may limit generalizability, and there is also a risk of sampling bias arising from respondent self-selection. However, no individual characteristics were found to be significant predictors to class membership, making it difficult to predict how sampling bias would affect preference estimates.
The validity of using hypothetical choices as a proxy to real-life decision-making is a recognized area of methodological debate (Quaife et al. 2018). To optimize the validity of design choices, best practice was followed during development and testing of the DCE. External validity is most important where DCEs are being used to generate quantitative data to predict treatment uptake or determine the optimum configuration of services, rather than to understand general trends in preferences as in this study.
Conclusions
Appearance is highly important in decisions about hypodontia treatment, but for 39% of respondents, potential complications were more important than appearance, and for 22% of respondents, improved function was also very important.
A minority (9%) of respondents provided unclear preferences either due to a lack of engagement with choice tasks or a true lack of preference.
Joint decision-making varied, with some child–parent dyads discussing and negotiating their joint preference, while other dyads were dominated by 1 individual.
Trade-off type tasks helped some people to think about treatment and identify their preferences.
Author Contributions
S. Barber, contributed to conception and design, data acquisition, analysis, or interpretation, drafted and critically revised the manuscript; H. Bekker, contributed to design, data interpretation, critically revised the manuscript; J. Marti, contributed to conception and design, data analysis and interpretation, critically revised the manuscript; S. Pavitt, contributed to conception and design, data interpretation, critically revised the manuscript; B. Khambay; contributed to design, critically revised the manuscript; D. Meads, contributed to design, data analysis and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345221111386 – Supplemental material for Adolescent and Parent Preferences for Hypodontia: Discrete Choice Experiment
Supplemental material, sj-docx-1-jdr-10.1177_00220345221111386 for Adolescent and Parent Preferences for Hypodontia: Discrete Choice Experiment by S. Barber, H. Bekker, J. Marti, S. Pavitt, B. Khambay and D. Meads in Journal of Dental Research
Footnotes
Acknowledgements
Our gratitude to the dental teams at all recruitment sites, the study participants, and all our patient and parent contributors.
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute for Health Research (NIHR) Doctoral Research Fellowship (DRF-2015-08-052) held by S. Barber. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.