
Abstract
The long-term effectiveness of powered toothbrushes (PTBs) and interdental cleaning aids (IDAs) on a population level is unproven. We evaluated to what extent changes in PTB and IDA use may explain changes in periodontitis, caries, and tooth loss over the course of 17 y using data for adults (35 to 44 y) and seniors (65 to 74 y) from 3 independent cross-sectional surveys of the German Oral Health Studies (DMS). Oaxaca decomposition analyses assessed to what extent changes in mean probing depth (PD), number of caries-free surfaces, and number of teeth between 1) DMS III and DMS V and 2) DMS IV and DMS V could be explained by changes in PTB and IDA use. Between DMS III and V, PTB (adults: 33.5%; seniors: 28.5%) and IDA use (adults: 32.5%; seniors: 41.4%) increased along with an increase in mean PD, number of caries-free surfaces, and number of teeth. Among adults, IDA use contributed toward increased number of teeth between DMS III and V as well as DMS IV and V. In general, the estimates for adults were of lower magnitude. Among seniors between DMS III and V, PTB and IDA use explained a significant amount of explained change in the number of caries-free surfaces (1.72 and 5.80 out of 8.44, respectively) and the number of teeth (0.49 and 1.25 out of 2.19, respectively). Between DMS IV and V, PTB and IDA use contributed most of the explained change in caries-free surfaces (0.85 and 1.61 out of 2.72, respectively) and the number of teeth (0.25 and 0.46 out of 0.94, respectively) among seniors. In contrast to reported results from short-term clinical studies, in the long run, both PTB and IDA use contributed to increased number of caries-free healthy surfaces and teeth in both adults and seniors.
Introduction
Periodontitis and caries account for about 60% of tooth loss in Germany (Glockmann et al. 2011). From a patient’s perspective, tooth loss is the most important outcome from dental diseases (Steele et al. 2004). Current data indicate that oral health has considerably improved over the past decades in Germany (Micheelis and Reich 1999; Micheelis and Schiffner 2006; Schützhold et al. 2013; Jordan and Micheelis 2016; Schwendicke et al. 2018; Jordan et al. 2019; Schwendicke et al. 2020).
Plaque is the main cause for periodontitis and caries (Löe et al. 1965; Marsh and Nyvad 2008). The mainstays of periodontitis and caries prevention are meticulous removal of supragingival plaque and use of fluoride toothpastes, respectively (Walsh et al. 2010; Tonetti et al. 2015). Although manual toothbrush is a quintessential tool, mastery over brushing skills is needed to remove plaque effectively. Powered toothbrushes (PTBs), on the other hand, are effective in plaque removal even with improper brushing skills. Despite being on the market for decades, only a few studies have documented their long-term effectiveness (Dörfer et al. 2016; Pitchika et al. 2019).
Toothbrushing is insufficient as a standalone oral hygiene regimen (Ciancio et al. 1992), because proximal surfaces are left untouched (Lindhe and Koch 1967). Hence, interdental cleaning aids (IDAs) such as dental floss, interdental brushes (IDBs), or toothpicks should be included in the oral hygiene routine to prevent periodontitis and caries. Dental floss, which is most widely used, has been proven to be effective through in vitro (Smith et al. 1986) and clinical studies (Mwatha et al. 2017; Graziani et al. 2018), whereas IDBs were found to be more effective compared to flossing in managing gingivitis (Sälzer et al. 2015; Kotsakis et al. 2018). Recent reviews concluded that the evidence suggesting the effectiveness of floss or IDB ranged from weak to moderate with clinically unimportant effect sizes. Furthermore, besides gingivitis and plaque, no further patient-relevant outcomes such as interproximal caries or periodontitis were reported (Amarasena et al. 2019; Worthington et al. 2019).
Concurring with past recommendations by dentists and industry, PTB (14.2% to 47.7%) and floss (20.9% to 35%) use has increased among German adults over the past 17 y (Jordan and Micheelis 2016). Thus, it needs to be clarified whether there are any additional oral health benefits from PTB and IDA use on a population level. Using data from repeated cross-sectional population-based German Oral Health Studies (Deutsche Mundgesundheitsstudien [DMS]), we estimated to what portion changes in 1) periodontal health in terms of mean probing depth (PD), 2) caries experience in terms of number of caries-free healthy surfaces, 3) number of teeth, and 4) having ≥20 teeth between DMS III and DMS V and DMS IV and V can be explained by changes in PTB and IDA use.
Materials and Methods
Study Population
The Institute of German Dentists (Institut der Deutschen Zahnärzte [IDZ]) has been conducting repeated cross-sectional studies representing the German population since 1989 to assess the oral health status of the German population. For this study, repeated cross-sectional data from 1997 (DMS III), 2005 (DMS IV), and 2014 (DMS V) were considered (Fig.). For all 3 studies, random cluster samples stratified by federal state and by community category with an oversampling for East Germans were drawn, comprising 90 municipalities each. Participants were excluded in later surveys if they were already a part of the previous DMS study. All study participants signed the informed consent.
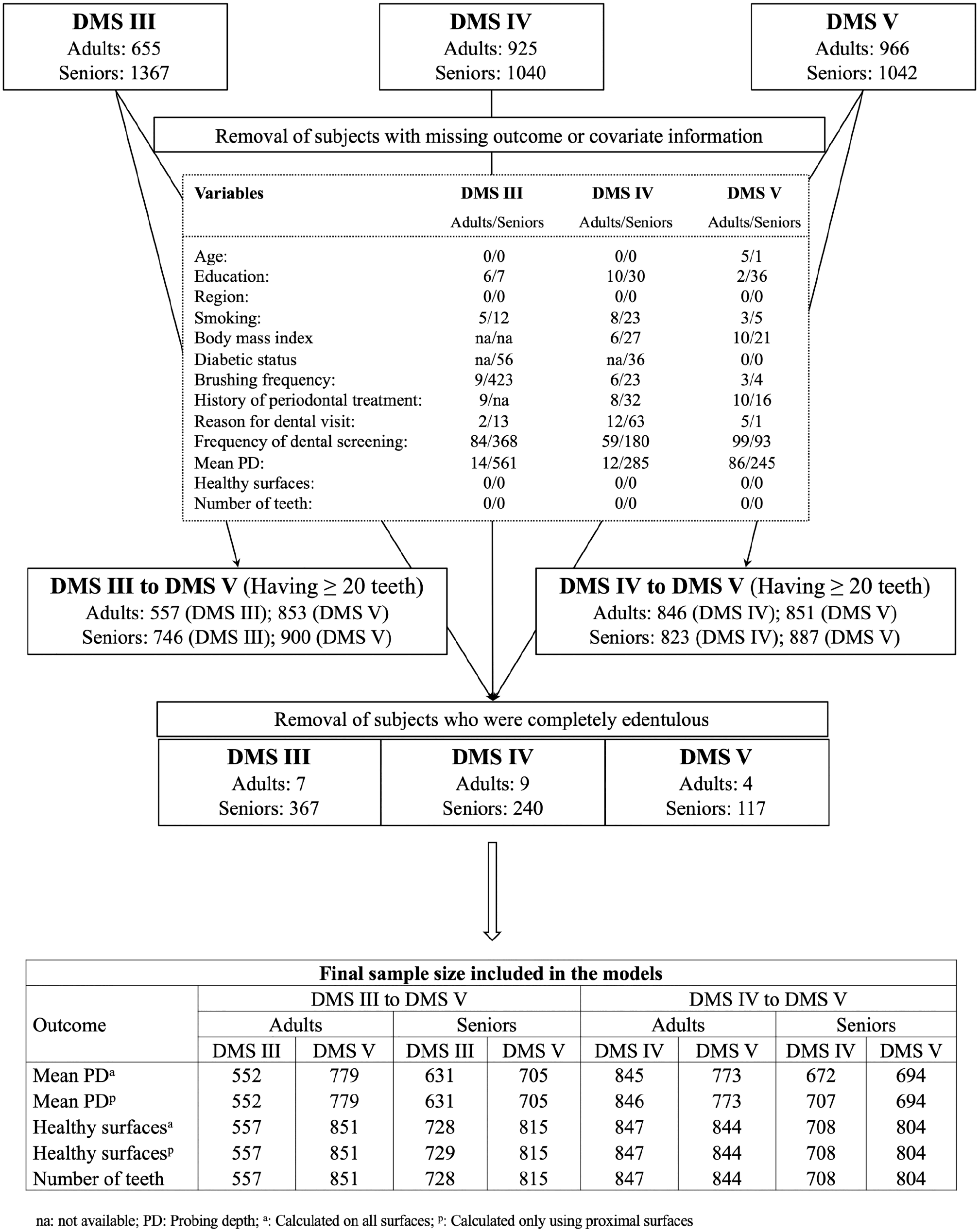
Overview of the flow of study participants leading to final sample size for the different models analyzed in the study.
Dental Examination
Detailed information on dental examination can be found in the Appendix.
Variables of Interest
Participants were asked about PTB or IDA use (Question: Which oral hygiene appliance/s do you use? [multiple answers were possible]: Manual toothbrush? Powered toothbrush? Dental floss? Toothpicks? Interdental brushes?). Participants answering for both PTB and manual toothbrush were assigned to the PTB group. Differentiation between the types of PTB (sonic/vibratory/oscillatory-rotatory) was not made. A binomial variable (no/yes) and a categorical IDA variable (non-IDA user/exclusively dental floss user/exclusively toothpicks user/exclusively IDB user/multiuser [participants using a combination of 2 or more IDAs, e.g., dental floss and IDB, toothpicks and IDB, etc.]) were generated.
Statistical Analyses
Descriptive statistics and analyses were stratified by age group (adults: 35 to 44 y, seniors: 65 to 74 y) and examination (Table 1). Mean PD (dentates only), number of healthy surfaces (dentates only), number of teeth (dentates only), and having ≥20 teeth (including completely edentulous subjects) (Fédération Dentaire Internationale 1982) were considered as outcome variables. Periodontitis and caries models were repeated, restricting to proximal sites/surfaces. Adjusted covariates were selected a priori based on clinical knowledge (Table 1 and Appendix).
Characteristics of the Entire Study Sample Cross-Sectionally at DMS III, DMS IV, and DMS V.
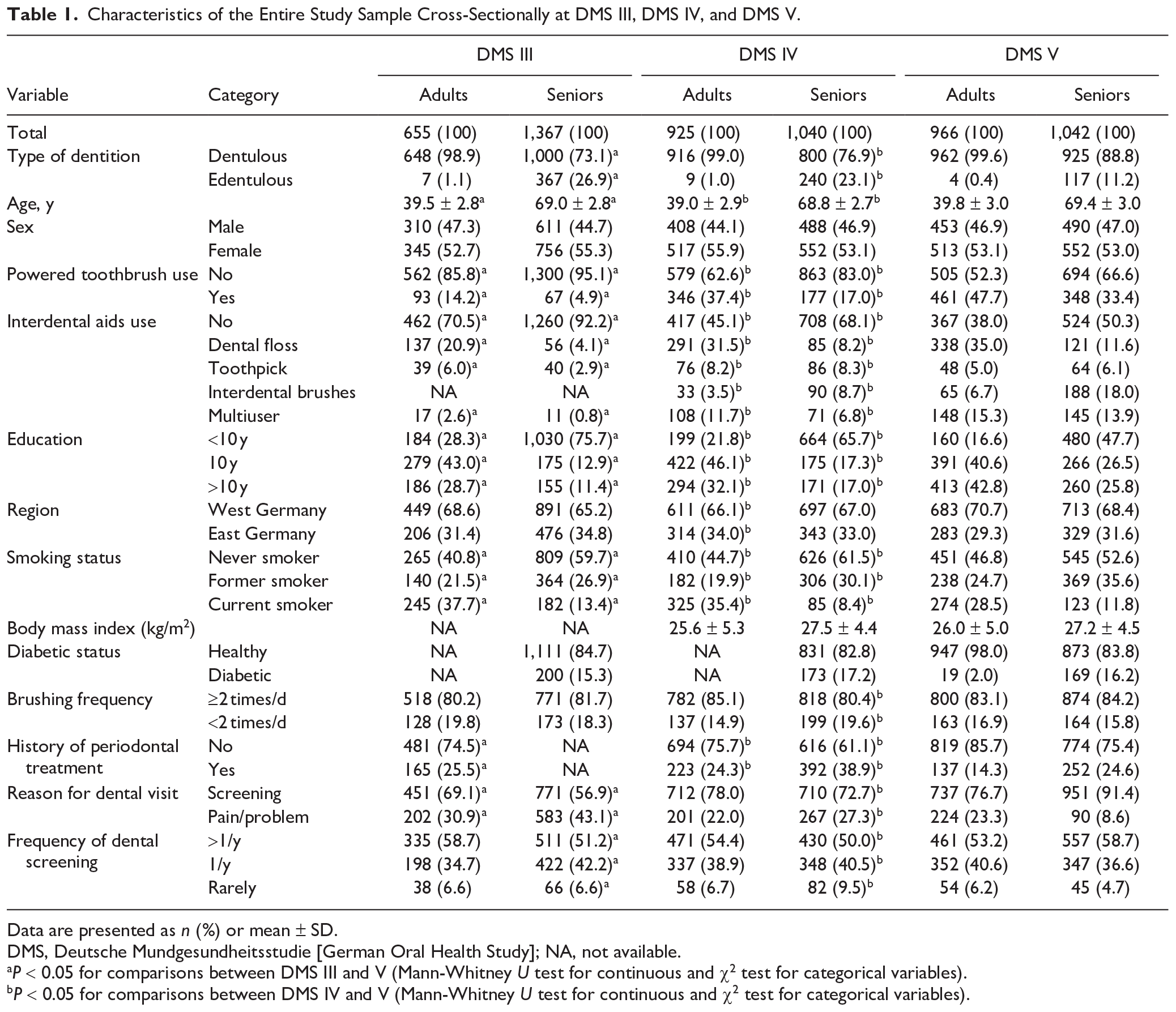
Data are presented as n (%) or mean ± SD.
DMS, Deutsche Mundgesundheitsstudie [German Oral Health Study]; NA, not available.
P < 0.05 for comparisons between DMS III and V (Mann-Whitney U test for continuous and χ2 test for categorical variables).
P < 0.05 for comparisons between DMS IV and V (Mann-Whitney U test for continuous and χ2 test for categorical variables).
Oaxaca decomposition analyses (O’Donnell et al. 2008) were performed to evaluate to which extent changes in oral health outcomes between 2 time points (DMS III to V; DMS IV to V) might be explained by changes in PTB and/or IDA use. Predicted means were estimated, and changes between 2 examinations were divided into explained and unexplained components by the Oaxaca decomposition. The amount of change attributed to PTB/IDA use within the explained component was tabulated.
We also assessed cross-sectional effects of PTB and IDA use (both included in the same model) on different outcomes constructing multiple linear regression models at each time point, adjusting for covariates. Adjusted effect estimates, 95% confidence intervals, and corresponding P values were calculated.
In sensitivity analyses, we repeated all Oaxaca decomposition models by replacing the binomial IDA variable with the categorical one to attribute the changes to different IDAs. Analyses were conducted using Stata/SE 14.2 (StataCorp).P values <0.05 were considered statistically relevant. The recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were applied for reporting (von Elm et al. 2014).
Results
Study Characteristics
The proportion of PTB (adults: 14.2% to 47.7%; seniors: 4.9% to 33.4%) and IDA (adults: 29.5% to 62.0%; seniors: 7.8% to 49.2%) users increased from DMS III to DMS V (Table 1). Meanwhile, the overall study population characteristics in terms of other covariates also improved (Table 1).
Periodontitis
Crude mean PD levels increased between DMS III and V (adults: 2.19 to 2.23 mm; seniors: 2.60 to 2.73 mm). Among adults, Oaxaca decomposition also predicted an increase in mean PD (all sites) of 0.08 mm (Table 3). While the model explained an overall reduction of 0.10 mm (of which IDA use explained a reduction of 0.04 mm), an increase of 0.18 mm was unexplained, which might be attributed to covariates not included in the model. In seniors, neither PTB nor IDA use significantly explained changes in mean PD between DMS III and V (Table 3). Restricting to proximal sites, a mean PD reduction of 0.12 mm in adults (seniors: 0.17 mm) was explained by the model, out of which a reduction of 0.05 mm (seniors: 0.09 mm) was attributed to IDA use. Sensitivity analyses revealed that floss and multiusers were most effective in reducing mean PD in both adults and seniors (Table 4).
Distributions (Unadjusted Values) of Dental Variables in Adults and Seniors in DMS III, DMS IV, and DMS V.
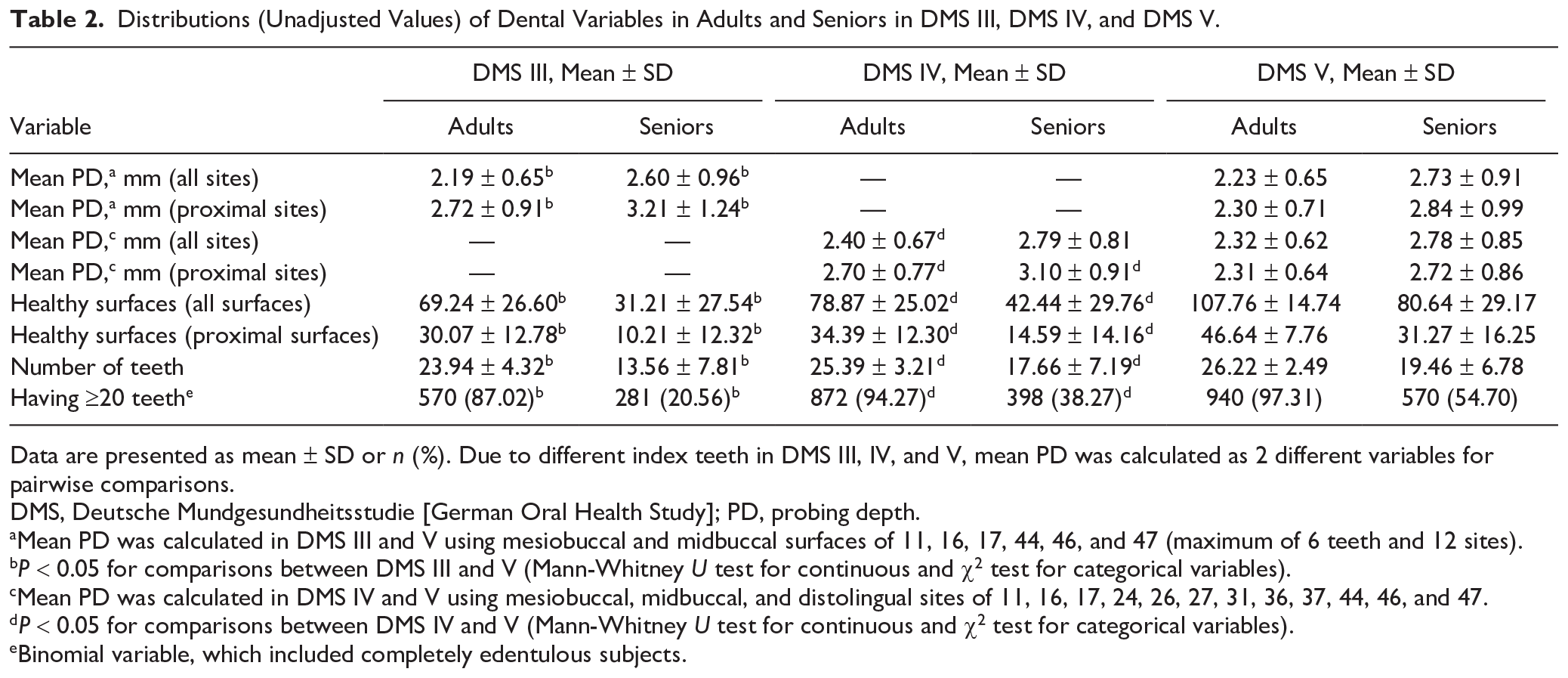
Data are presented as mean ± SD or n (%). Due to different index teeth in DMS III, IV, and V, mean PD was calculated as 2 different variables for pairwise comparisons.
DMS, Deutsche Mundgesundheitsstudie [German Oral Health Study]; PD, probing depth.
Mean PD was calculated in DMS III and V using mesiobuccal and midbuccal surfaces of 11, 16, 17, 44, 46, and 47 (maximum of 6 teeth and 12 sites).
P < 0.05 for comparisons between DMS III and V (Mann-Whitney U test for continuous and χ2 test for categorical variables).
Mean PD was calculated in DMS IV and V using mesiobuccal, midbuccal, and distolingual sites of 11, 16, 17, 24, 26, 27, 31, 36, 37, 44, 46, and 47.
P < 0.05 for comparisons between DMS IV and V (Mann-Whitney U test for continuous and χ2 test for categorical variables).
Binomial variable, which included completely edentulous subjects.
Contribution of Changes in Powered Toothbrush (PTB) and Interdental Aids (IDA) Usage to Changes in Dental Parameters Between DMS III and V and DMS IV and V Using Blinder-Oaxaca Decomposition.
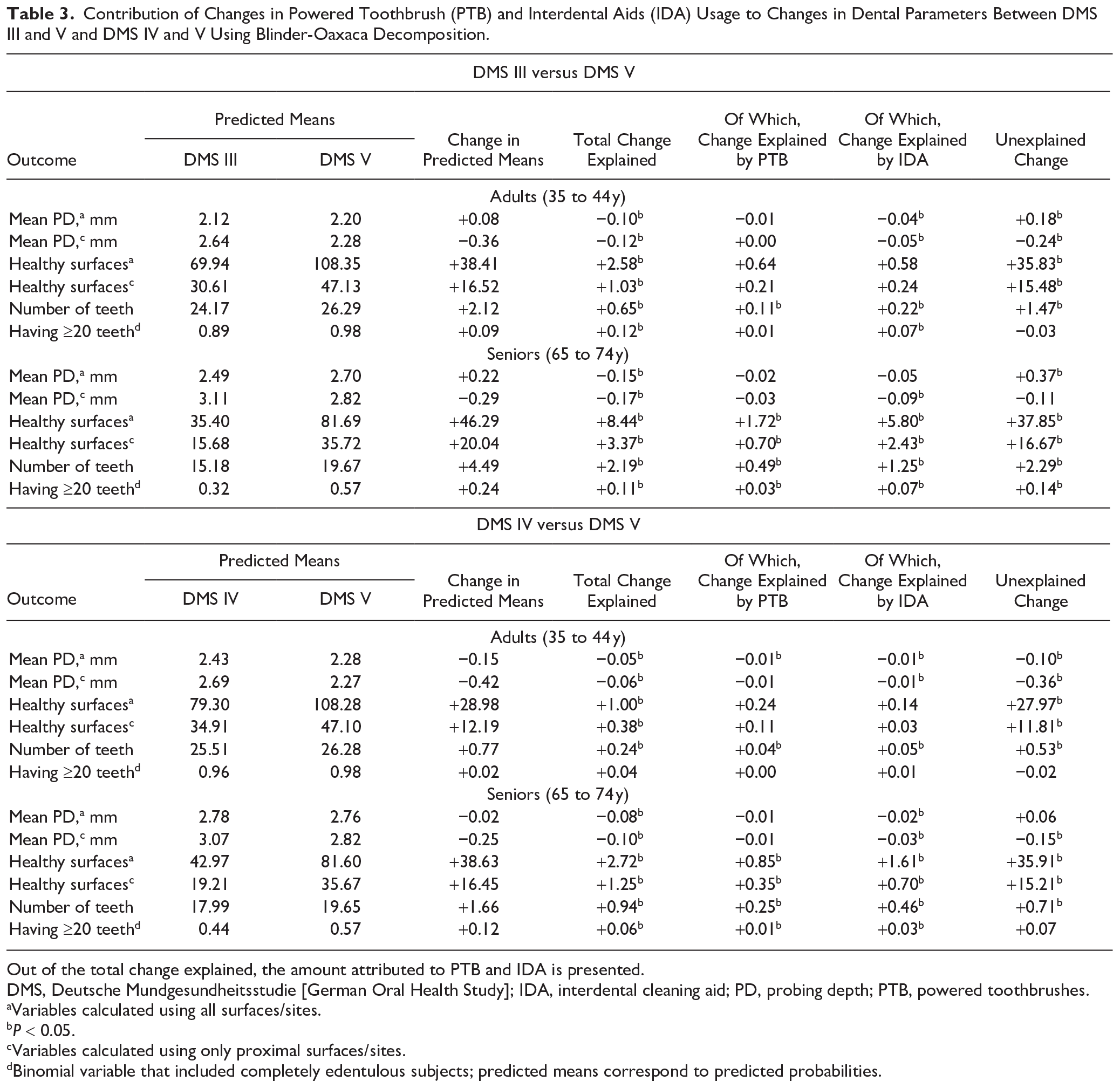
Out of the total change explained, the amount attributed to PTB and IDA is presented.
DMS, Deutsche Mundgesundheitsstudie [German Oral Health Study]; IDA, interdental cleaning aid; PD, probing depth; PTB, powered toothbrushes.
Variables calculated using all surfaces/sites.
P < 0.05.
Variables calculated using only proximal surfaces/sites.
Binomial variable that included completely edentulous subjects; predicted means correspond to predicted probabilities.
As Sensitivity Analyses, Contributions of Changes in Usage of PTB, and Different Types of Interdental Cleaning Aids to Changes in Dental Parameters between DMS III and V and DMS IV and V Using Blinder-Oaxaca Decomposition.
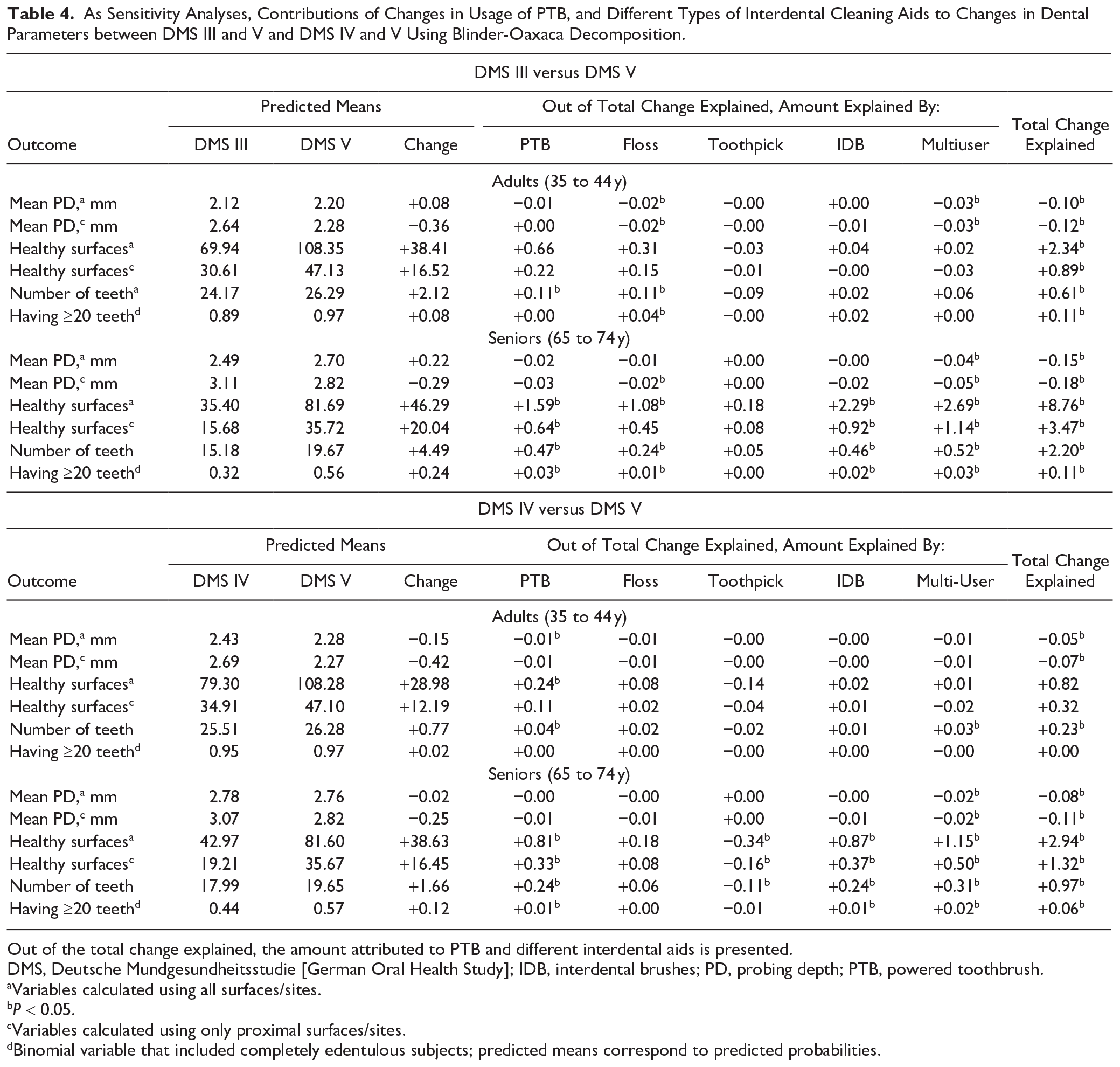
Out of the total change explained, the amount attributed to PTB and different interdental aids is presented.
DMS, Deutsche Mundgesundheitsstudie [German Oral Health Study]; IDB, interdental brushes; PD, probing depth; PTB, powered toothbrush.
Variables calculated using all surfaces/sites.
P < 0.05.
Variables calculated using only proximal surfaces/sites.
Binomial variable that included completely edentulous subjects; predicted means correspond to predicted probabilities.
Crude mean PD decreased between DMS IV and V (adults: 2.40 to 2.32 mm; seniors: 2.79 to 2.78 mm) (Table 2). Among adults, Oaxaca decomposition predicted a decrease of 0.15 mm, of which the model explained a decrease of 0.05 mm and, out of which, PTB and IDA use each contributed to a 0.01-mm reduction. In proximal sites, a reduction of 0.06 mm was explained by the model, of which 0.01 mm was attributed to IDA use. Apart from PTB, changes in frequencies of IDA subgroups did not explain changes in mean PD. In seniors, only IDA use significantly contributed to reductions in mean PD (all/proximal sites). However, only the multiuser group significantly contributed to reduced mean PD levels (Table 4).
Caries
The number of caries-free healthy surfaces increased considerably between DMS III, IV, and V (adults: 69.24, 78.87, and 107.76; seniors: 31.21, 42.44, and 80.64; Table 2).
Between DMS III and V, neither PTB nor IDA use significantly contributed to an increase in healthy (all/proximal) surfaces among adults. In seniors, they increased by 46.29 surfaces (Table 3), and the Oaxaca decomposition model explained an increase of 8.44 surfaces, out of which PTB and IDA use together explained 7.52 surfaces. Results were similar when the data were restricted only to proximal surfaces. Specifically, PTB, IDB, and multi-IDA use contributed to estimated increases (Table 4).
Among adults between DMS IV and V, the total change explained by the model was low (1.00 out of 28.98); neither PTB nor IDA use explained predicted changes. In seniors, the number of healthy surfaces increased by 38.63; PTB and IDA use together attributed to an increase of 2.46 out of 2.72 surfaces that were explained by the model. Restricting analyses to proximal surfaces, an increase of 1.25 out of 16.45 surfaces in total were explained by the model. PTB and IDA use collectively explained an increase of 1.05 surfaces (Table 3), and on stratifying the IDA variable, PTB, toothpick, IDB, and multiple IDA use significantly explained the change (Table 4).
Number of Teeth
Crude mean number of teeth increased between DMS III, IV, and V (adults: 23.9, 25.4, and 26.2; seniors: 13.6, 17.7, and 19.5; Table 2). Comparing DMS III and V, the Oaxaca decomposition predicted that the number of teeth increased by 2.12 teeth in adults (seniors: 4.49 teeth), of which a change of 0.65 teeth (seniors: 2.19) was explained by the model (Table 3). In adults, an increase of 0.11 and 0.22 teeth (seniors: 0.49 and 1.25) was attributed to PTB and IDA use, respectively. A similar trend was observed among adults and seniors when the binomial variable of having ≥20 teeth was analyzed. Furthermore, contributions of IDA in adults were mainly explained by use of floss, while in seniors, use of PTB, floss, IDB, and multiuser contributed significantly to an increase in number of teeth (Table 4).
Between DMS IV and V, the number of teeth in adults increased by 0.77 teeth (1.66 teeth in seniors), of which 0.24 teeth (0.94 in seniors) were explained by the Oaxaca decomposition model. An increase of 0.04 and 0.05 teeth (0.25 and 0.46 in seniors) was attributed to PTB and IDA use, respectively. Among seniors, use of PTB, toothpicks, IDB, and any IDA (multiuser) mainly contributed to the increased teeth numbers. The probability of having ≥20 teeth increased by 12% in seniors, half of which (6%) was explained by the model (PTB and IDA together account for 4% increase in the probability).
Discussion
This study assessed to what extent changes in frequencies of PTB and IDA use explain the changes in mean PD, number of caries-free healthy surfaces, number of teeth, and having ≥20 teeth between DMS III and V as well as DMS IV and V. Our main findings suggest that the PTB and IDA use increased over the DMS timeline, and they explained a significant portion of explainable changes in mean PD, number of caries-free healthy surfaces, number of teeth, and the probability of having ≥20 teeth between DMS III and V as well as between DMS IV and V. In general, the contributions were more pronounced for IDA use (vs. PTB use) and among seniors (vs. adults). For example, comparing attributions of PTB and IDA use to changes in the number of teeth among seniors between DMS III and V, PTB versus IDA use explained an increase of 0.49 versus 1.25, respectively, out of 4.49 increase (DMS IV to V: 0.25 vs. 0.48 out of 1.66 increase) in the number of teeth.
When trying to understand protective effects of personal mechanical plaque removal on periodontitis, caries, or tooth loss, we would like to concentrate on seniors between DMS III and V. Out of 4.49 additionally retained teeth, 0.49 were explained by PTB and 1.25 by IDA use (together 1.74 teeth or 38.8% of effect explained), whereas PTB and IDA use only explained 1.72 and 5.80 surfaces, respectively (together 7.52 surfaces or 16.2% of effect explained) out of 46.29 additional caries-free healthy surfaces. The number of totally explained healthy approximal surfaces was nearly half as many as all surfaces (3.37 vs. 8.44), because approximal caries are usually treated by drilling through the occlusal or smooth surfaces, and thus each treatment of a cavitated approximal surface might be accompanied by destruction of a sound surface. Hence, the benefit of retaining a healthy approximal surface is double. This explains why IDA was more effective than PTB on both the surface and the tooth level. Usually, the increase in caries-free surfaces is attributed to fluoridated toothpastes (Walsh et al. 2019), while the use of IDAs is regarded as a mainstay for preventing periodontitis. In line, a recent Cochrane review evaluated IDBs to be effective in reducing gingivitis and plaque; however, the evidence was rated as very low due to inclusion of less studies and high risk of bias (Worthington et al. 2019). In contrast, unsupervised flossing did not contribute to caries risk reduction in children and adolescents who were followed for 2 y (Hujoel et al. 2006). However, our study provides epidemiologic evidence that IDA use moderately contributes to caries prevention in addition to the use of fluoridated toothpastes (approximately 90% of all toothpastes in Germany are fluoridated; Schulte 2005), thereby retaining more teeth. Hence, personal interdental plaque removal should not be neglected in terms of caries prevention.
We could only presume the impact of PTB and IDA on periodontitis because, besides PDs, meaningful information on clinical attachment loss (CAL) throughout the DMS examinations is unavailable. Among seniors, predicted reduction in mean PD at approximal sites was 0.29 mm between DMS III and V, whereof IDA use explained a meager 0.09-mm reduction, which probably translates into a higher tooth retention rate. Although the estimates for mean PD were minimal (Appendix Tables 2 and 3), IDA could explain one-third of the explained change, which is remarkable for a population-based study. This conclusion contrasted with a study in which similarly aged dental professionals with better oral hygiene practices were not found to be associated with periodontitis (Merchant et al. 2002). Last decade, there was a fierce debate among public and consumer press about whether flossing has any benefit on oral health, because the US Department of Health and Human Services and US Department of Agriculture (2015) removed the recommendation of flossing from their Dietary Guidelines. Contrastingly, a recent study associating flossing with oral diseases among seniors (>65 y) also confirmed that the extent of periodontitis, caries, and tooth loss was less among flossers over a 5-y observation period (Marchesan et al. 2020). Our results pinpoint the difference between RCTs and observational epidemiological studies. Probably results from RCTs will never provide definitive conclusions with tooth loss as an end point because of ethical considerations and time restraints to observe any significant tooth loss. Based on observational evidence with all its pitfalls, dental professionals should recommend the appropriate IDA on an individualized basis depending on dexterity and embrasure size (Sälzer et al. 2015; Worthington et al. 2019).
PTB is an effective tool in maintaining oral hygiene. It has to be reiterated that a Cochrane review in the past rated the quality of evidence on this topic as low (Yaacob et al. 2014). To fill this void, we recently assessed effects of PTB on 11-y changes on oral health parameters using longitudinal data from the Study of Health in Pomerania (Pitchika et al. 2019). PTB users showed reduced progression of mean CAL and mean PD and improved tooth retention. As expected from our previous study, estimates of explained change for mean PD in this study were small but noticeable for number of teeth, which is of utmost importance from patients’ perspective. In a recent analysis we reported, CAL predicts tooth loss better than PD (Houshmand et al. 2012). This observation fits together with the present results that even if estimates on PD were negligible, tooth loss may be prevented by use of PTB and IDA because they have a more pronounced effect on CAL than on PD.
The main strength of our study is the availability of repeated cross-sectional data with similar sampling strategies providing dental data representative for Germany. Our study followed a repeated cross-sectional design, in which it is not possible to assess subjects longitudinally; however, this design is best suitable to analyze effects of higher prevalence of exposure use on outcomes (Blanchard et al. 1977). It is understood that a factor has to change over time to change the outcome prevalence (Table 1), and it must be a risk factor for the outcome (Appendix Table 1). As these 2 criteria were satisfied, it is plausible that PTB and IDA use might have contributed to changes in the prevalence and severity of oral diseases. Improvements in the German population’s oral health was also reflected by increased expenditures for oral health products from €1.35 to €1.50 billion between 2010 and 2016 (corresponding to increased use of floss [14% to 21%] and PTB [25.8% to 36.6%] according to marketing research; Olbrisch 2017).
Approximately 2 decades of time between DMS III and V resulted in different demographic characteristics. DMS III was sampled shortly after the German unification, with tremendous ramifications on the population at that time. Apart from increased use of PTB/IDA and improved education and smoking status, DMS V participants had regular dental screenings, which might indicate an improved dental awareness. Our results also support the notion that industry marketing and motivation by the dental fraternity affected oral health in Germany (Särner et al. 2010). In addition to cohort effects (Schützhold et al. 2013), remuneration rates for prosthodontic treatments were reduced over the years, which might explain the increased number of teeth in DMS V and also some PD increase in general.
Our study also had few limitations. All DMS studies applied partial periodontal recordings. To compare mean PD between DMS III and V, measurements of 2 sites on 6 index teeth on the right side (DMS IV and V: 3 sites on 12 index teeth) were considered, resulting in considerable bias with unclear direction in estimating mean PD (Beltrán-Aguilar et al. 2012) and a dilution of effect estimates toward the null (Akinkugbe et al. 2015). Although we collected toothbrushing frequency, we do not know the type of PTB used or whether interdental cleaning was done regularly or how effectively it was performed. Although CAL reflects long-term periodontal disease severity, the quality of CAL assessment in DMS examinations was questionable, leaving us with mean PD as the only periodontal outcome. Similarly, other caries variables (decayed surfaces/teeth [DS/T], decayed and filled surfaces/teeth [DFS/T], and decayed, missing and filled surfaces/teeth [DMFS/T]) were skewed in distribution, so we used only number of healthy surfaces as a caries-related outcome. Furthermore, residual confounding from variables not considered in decomposition models, such as socioeconomic status, income, diet, medications, physical activity, lifestyle, and stress, could modify the models. Therefore, care has to be taken to measure and include as many meaningful covariates to avoid overemphasizing the effects on limited variables.
In summary, changes in PTB/IDA use between DMS III and V significantly contributed to observed improvements in periodontitis, caries, and the number of teeth. Although estimated contributions to changes in mean PD and number of caries-free healthy surfaces were low in general, these changes seemed to translate into more teeth among seniors in the long run, which is clinically relevant. Since tooth conservation is of utmost importance from the patients’ point of view, recommending PTB and IDA might have a significant public health impact.
Conclusion
PTB and IDA use significantly contributed toward reduction of mean PD and an increase in the number of caries-free healthy surfaces and teeth over the course of 17 y. Compared to PTB use, increased frequencies of IDA use had more pronounced effects on the number of healthy surfaces and teeth, especially in seniors. In conclusion, this study provides further evidence in favor of recommending PTB and IDA use to the public.
Author Contributions
V. Pitchika, contributed to data analysis and interpretation, drafted and critically revised the manuscript; R. Jordan, W. Micheelis, contributed to conception, design, and data acquisition, critically revised the manuscript; A. Welk, contributed to conception and design, critically revised the manuscript; T. Kocher, contributed to conception, design, data acquisition, and interpretation, critically revised the manuscript; B. Holtfreter, contributed to conception, design, data acquisition, analysis, and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-pdf-1-jdr-10.1177_0022034520973952 – Supplemental material for Impact of Powered Toothbrush Use and Interdental Cleaning on Oral Health
Supplemental material, sj-pdf-1-jdr-10.1177_0022034520973952 for Impact of Powered Toothbrush Use and Interdental Cleaning on Oral Health by V. Pitchika, R. Jordan, W. Micheelis, A. Welk, T. Kocher and B. Holtfreter in Journal of Dental Research
Footnotes
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The German Oral Health Studies are proudly financed by the German dental professionals via the German Dental Association (Bundeszahnärztekammer—Arbeitsgemeinschaft der Deutschen Zahnärztekammern—[BZÄK] e. V.) and the National Association of Statutory Health Insurance Dentists (Kassenzahnärztliche Bundesvereinigung [KZBV] KdöR). V. Pitchika was funded by a grant from the IDZ.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.