
Abstract
Propranolol is a nonselective β-adrenergic receptor antagonist that is efficacious in reducing facial pain. There is evidence that its analgesic efficacy might be modified by variants of the catechol-O-methyltransferase (COMT) gene. We tested the hypothesis in a subset of 143 non-Hispanic Whites from a randomized controlled trial of patients with painful temporomandibular disorder (TMD). Patients were genotyped for rs4680, a single nucleotide polymorphism of COMT, and randomly allocated to either propranolol 60 mg twice daily or placebo. During the 9-wk follow-up period, patients recorded daily ratings of facial pain intensity and duration; the product was computed as an index of facial pain. Postbaseline change in the index at week 9 (the primary endpoint) was analyzed as a continuous variable and dichotomized at thresholds of ≥30% and ≥50% reduction. Mixed models for repeated measures tested for the genotype × treatment group interaction and estimated means, odds ratios (ORs), and 95% confidence limits (95% CLs) of efficacy within COMT genotypes assuming an additive genetic model. In secondary analysis, the cumulative response curves were plotted for dichotomized reductions ranging from ≥20% to ≥70%, and genotype differences in area under the curve percentages (%AUC) were calculated to signify efficacy. Mean index reduction did not differ significantly (P = 0.277) according to genotype, whereas the dichotomized ≥30% reduction revealed greater efficacy among G:G homozygotes (OR = 10.9, 95%CL = 2.4, 50.7) than among A:A homozygotes (OR = 0.8, 95%CL = 0.2, 3.2) with statistically significant interaction (P = 0.035). Cumulative response curves confirmed greater (P = 0.003) efficacy for G:G homozygotes (%AUC difference = 43.7, 95%CL = 15.4, 72.1) than for A:A homozygotes (%AUC difference = 6.5, 95%CL = -30.2, 43.2). The observed antagonistic effect of the A allele on propranolol’s efficacy was opposite the synergistic effect hypothesized a priori. This unexpected result highlights the need for better knowledge of COMT’s role in pain pathogenesis if the gene is to be used for precision-medicine treatment of TMD (ClinicalTrials.gov NCT02437383).
Keywords
Introduction
Symptoms of painful temporomandibular disorder (TMD) are reported by 5% of U.S. adults, one-fifth of whom use prescription medication to manage the pain (Slade and Durham 2020). However, analgesics for TMD lack efficacy (Mujakperuo et al. 2010), and “action is urgently needed to improve care for individuals with a TMD” (National Academies of Sciences 2020). Yet, formidable barriers restrict the development of new analgesics, including the many years required to discover new analgesics and the high probability that they fail to show efficacy in phase III trials (Chaplan et al. 2010).
Effective analgesics might instead be identified using strategies from precision medicine (Niculescu et al. 2019). One strategy is to repurpose drugs developed for other conditions, using them to target biological pathways that modulate pain. Another strategy is to tailor drug therapy based on patients’ genotypes (Wilentz and Cowley 2017). Both strategies are applicable to propranolol, a nonselective β-adrenergic receptor antagonist, which was developed in the 1960s and is effective for migraine prevention (He et al. 2017). Recent findings from preclinical studies have shown that propranolol inhibits pain processes that amplify trigeminal nociception (Khasar et al. 1999; Shields and Goadsby 2005; Rodrigues et al. 2006; Ciszek et al. 2016; Boyer et al. 2017). Other studies suggest that propranolol’s analgesic efficacy is modified by genetic variation in the catechol-O-methyltransferase (COMT) gene. Specifically, the A allele of the rs4680 single nucleotide polymorphism codes for a valine-to-methionine substitution in the COMT enzyme, reducing enzymatic activity and slowing catabolism of catecholamines (Mannisto and Kaakkola 1999). One study found that people with the A:A genotype had heightened sensitivity to masseter muscle pain (Zubieta et al. 2003). Likewise, a COMT haplotype coding for reduced enzyme activity was associated with greater sensitivity to experimental pain and increased risk of developing TMD (Diatchenko et al. 2005).
These studies underpinned our premise that propranolol’s analgesic efficacy is enhanced in people whose COMT genotype is associated with reduced enzyme activity. Initial support for the premise came from a pilot, randomized crossover trial of 40 women with TMD who received propranolol and placebo (Tchivileva et al. 2010). Propranolol’s efficacy increased in a linear manner with each additional copy of the COMT haplotype coding for reduced enzyme activity, consistent with an additive genetic model (Clarke et al. 2011). Additivity was likewise found in an in vitro study in which COMT enzyme activity reduced with each additional copy of the A allele of the COMT gene (Smith et al. 2014).
This study aimed to determine if COMT genotype modifies analgesic efficacy of propranolol in a parallel-group randomized controlled trial (RCT). This represents the second aim of the Study of Orofacial Pain and Propranolol (SOPPRANO), in which propranolol was effective in achieving ≥30% and ≥50% reductions in TMD patients’ facial pain (Tchivileva et al. 2020). As specified a priori in the study protocol, we hypothesized that the A allele of rs4680 is associated with greater analgesic efficacy of propranolol.
Methods
The study was approved by Institutional Review Boards at the 3 enrollment sites: University of North Carolina at Chapel Hill, University of Florida, and University at Buffalo. All study participants provided signed informed consent. Full details of the study methods are reported elsewhere (Tchivileva et al. 2020) and summarized below using headings from the CONSORT statement (Moher et al. 2010).
The trial design was a double-blind, placebo-controlled, parallel-group, phase 2b RCT. Study participants were 200 adults aged 18 to 65 y with TMD myalgia (with or without arthralgia), as determined using the diagnostic criteria for TMD (Schiffman et al. 2014). There were 16 exclusion criteria based on propranolol’s contraindications and health conditions that could have affected pain ratings. Study participants were randomized using 1:1 allocation stratified by study site using fixed permutated blocks of 4. Randomization was initiated by study coordinators via an electronic web response system, thereby masking study personnel and all study participants. Study participants were allocated to one of the investigational products: capsules of 60-mg extended release propranolol or a matching placebo, both administered once daily for 1 wk and then twice daily for 8 wk.
As specified a priori in the study protocol, the primary outcome was a facial pain index, calculated as the product of daily facial pain intensity (reported on a 0 to 100 numeric rating scale) and pain duration (% of day with facial pain) divided by 100. Each was recorded in a daily pain diary, and their product (i.e., daily facial pain index) was averaged across the 7 d prior to study visits conducted 1, 5, and 9 wk after the randomization visit. The secondary outcome was the patient’s global impression of change (PGIC; Hurst and Bolton 2004) evaluated at weeks 5 and 9.
Genotyping
DNA was extracted from venous blood samples collected at the baseline visit. Genotyping was performed by LGC Genomics (Beverly, MA, US) using proprietary KASP™ assays based on competitive allele-specific polymerase chain reaction.
Statistical Methods
To reduce population stratification bias (Cardon and Palmer 2003), this analysis was restricted to non-Hispanic Whites. Regression models tested for an interaction of genotype and allocated treatment group to evaluate the hypothesis that the A allele of rs4680 is associated with greater analgesic efficacy of propranolol. For the primary endpoint of facial pain index, efficacy was quantified as change in the index, computed by subtracting the baseline value from the value at each follow-up visit (i.e., weeks 1, 5, and 9). The continuous measure of change was analyzed as the dependent variable using a linear mixed model for repeated measures (MMRM), while logistic MMRMs evaluated reductions of ≥30% and ≥50% relative to baseline, both of which are clinically meaningful thresholds of improvement in pain (Dworkin et al. 2009).
As specified a priori in the study protocol, the number of A alleles was modeled as a continuous fixed-effect variable (i.e., assuming an additive genetic model). Other fixed-effect variables were treatment group (2 groups), study visit (3 postbaseline categories), and all 2-way and 3-way interactions of genotype, treatment group, and visit. Fixed-effect covariates were baseline pain index (modeled as a continuous variable), study site (3 categories), and sex (2 categories). Study participants were included as a random effect. MMRMs used data from all available follow-up visits and programming statements (Davis 2014) tested for a 2-way interaction of treatment group with genotype at week 9. Other programming statements calculated odds ratios or mean differences between treatment groups at week 9 for each genotype. Model-adjusted mean values or proportions were calculated and plotted for descriptive purposes. A comparable logistic MMRM was used to analyze global impression of change, dichotomized from the 7-point response scale to classify patients who reported feeling “somewhat better” through “a great deal better” (Hurst and Bolton 2004).
To determine the efficacy across the full range of clinically meaningful reduction in pain, logistic MMRMs for reductions ranging from ≥20% to ≥70% were used to construct cumulative response curves (Farrar 2010). The percentage area under curve (%AUC) was calculated for each treatment group, with the %AUC difference representing the efficacy estimate. AUC values were calculated using the trapezoid rule, and bootstrap estimates of the standard error were obtained from 1,000 samples of the observed data. Genotype-group differences in %AUC were evaluated using Wald’s test.
The threshold for statistical significance of effect modification was P < 0.05 for the 2-tailed test of the null hypothesis of no interaction at week 9. To judge the overall credibility of the effect modification, we applied 11 qualitative criteria (Sun et al. 2010). Sensitivity analysis evaluated 1) our assumption of an additive genetic model, 2) components of the facial pain index (i.e., pain intensity and duration), and 3) the effect of restricting the sample to females, as occurred in the pilot study (Tchivileva et al. 2010).
Sample Size Justification
SOPPRANO was planned with a target sample of 200 randomized study participants, providing 90% statistical power for the primary aim of overall analgesic efficacy of propranolol. As initially envisaged, the sample was to be limited to non-Hispanic Whites, providing 61% power to detect an interaction between COMT genotype and treatment group using a threshold of P < 0.05 for type I error based on a 2-tailed test. However, at study initiation, enrollment was opened to all races, and hence this analysis was limited to the 143 non-Hispanic Whites, yielding power of 47% to test the same interaction. Other assumptions for the power calculation were based on findings from our pilot study, namely, a 1:2:1 ratio of study participants with 0, 1, and 2 copies of the A allele of rs4680 and percentage reductions in mean pain index of 9%, 27%, and 45% (respectively) for the propranolol group compared with 9% for each genotype in the placebo group.
Results
Baseline Characteristics of Study Groups
Between August 2015 and January 2018, 200 study participants were randomized to either propranolol (n = 100) or placebo (n = 100), and 199 study participants with follow-up data were analyzed to test SOPPRANO’s primary aim (see the study by Tchivileva et al. 2020, which includes the CONSORT flow diagram, details of treatment adherence, and overall results for efficacy and adverse events). This genetic analysis was limited to 143 non-Hispanic White study participants who had at least 1 follow-up visit (n = 78 propranolol, n = 65 placebo). The distribution of rs4680 genotypes did not depart significantly (P > 0.05) from Hardy–Weinberg equilibrium. At baseline, the mean age of the the participants was 33 y, three-quarters were women, and there were no meaningful differences between treatment groups in these or other baseline characteristics (Table 1). Likewise, there were only small differences in baseline characteristics according to COMT genotype (Table 2).
Baseline Characteristics of Participants in the 2 Treatment Groups.
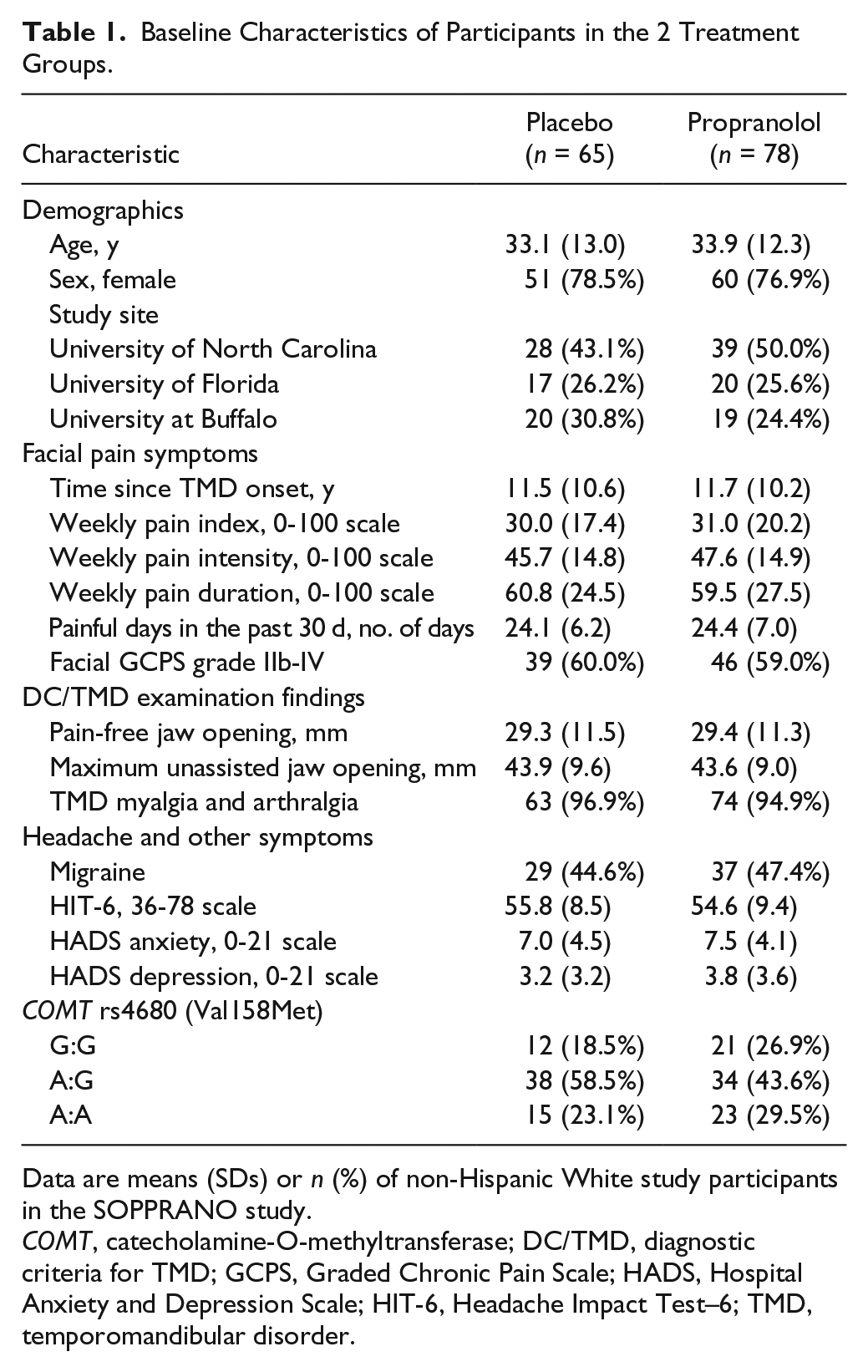
Data are means (SDs) or n (%) of non-Hispanic White study participants in the SOPPRANO study.
COMT, catecholamine-O-methyltransferase; DC/TMD, diagnostic criteria for TMD; GCPS, Graded Chronic Pain Scale; HADS, Hospital Anxiety and Depression Scale; HIT-6, Headache Impact Test–6; TMD, temporomandibular disorder.
Baseline Characteristics of Participants Classified by COMT rs4680 Genotype.

Data are means (SDs) or n (%) of non-Hispanic White study participants in the SOPPRANO study. P values are from 1-way analysis of variance F-tests (for continuous variables) and chi-square tests (for categorical variables) testing the null hypothesis that means or percentages (respectively) are equivalent among genotypes.
COMT, catecholamine-O-methyltransferase; DC/TMD, diagnostic criteria for TMD; GCPS, Graded Chronic Pain Scale; HADS, Hospital Anxiety and Depression Scale; HIT-6, Headache Impact Test–6; TMD, temporomandibular disorder.
Effect Modification of the Primary Endpoint by the COMT Genotype
Results for the linear MMRM analysis of the continuous measures of pain index revealed greater efficacy for G:G homozygotes than for A:A homozygotes, although the interaction was not statistically significant (Table 3; Suppl. Fig. S1). Among the n = 33 G:G homozygotes of rs4680, the adjusted percentage of study participants with ≥30% reduction in facial pain index at week 9 was 30.8% in the placebo group and 83.0% in the propranolol group (Fig. 1A), whereas among n = 38 A:A homozygotes, the corresponding percentages were 56.1% and 51.7% (Fig. 1C). The adjusted odds ratios of propranolol’s efficacy were 10.9 for G:G, 3.0 for A:G, and 0.8 for A:A, and the test for gene × treatment group interaction was statistically significant (P = 0.035; Table 3). A similar pattern was seen using the threshold of ≥50% reduction in facial pain index to define responders: odds ratios varied from 5.1 for G:G to 0.9 for A:A, although the test for interaction was not significant (P = 0.354; Table 3).
Summary of Efficacy Estimates and Tests for Gene × Treatment Group Interactions.
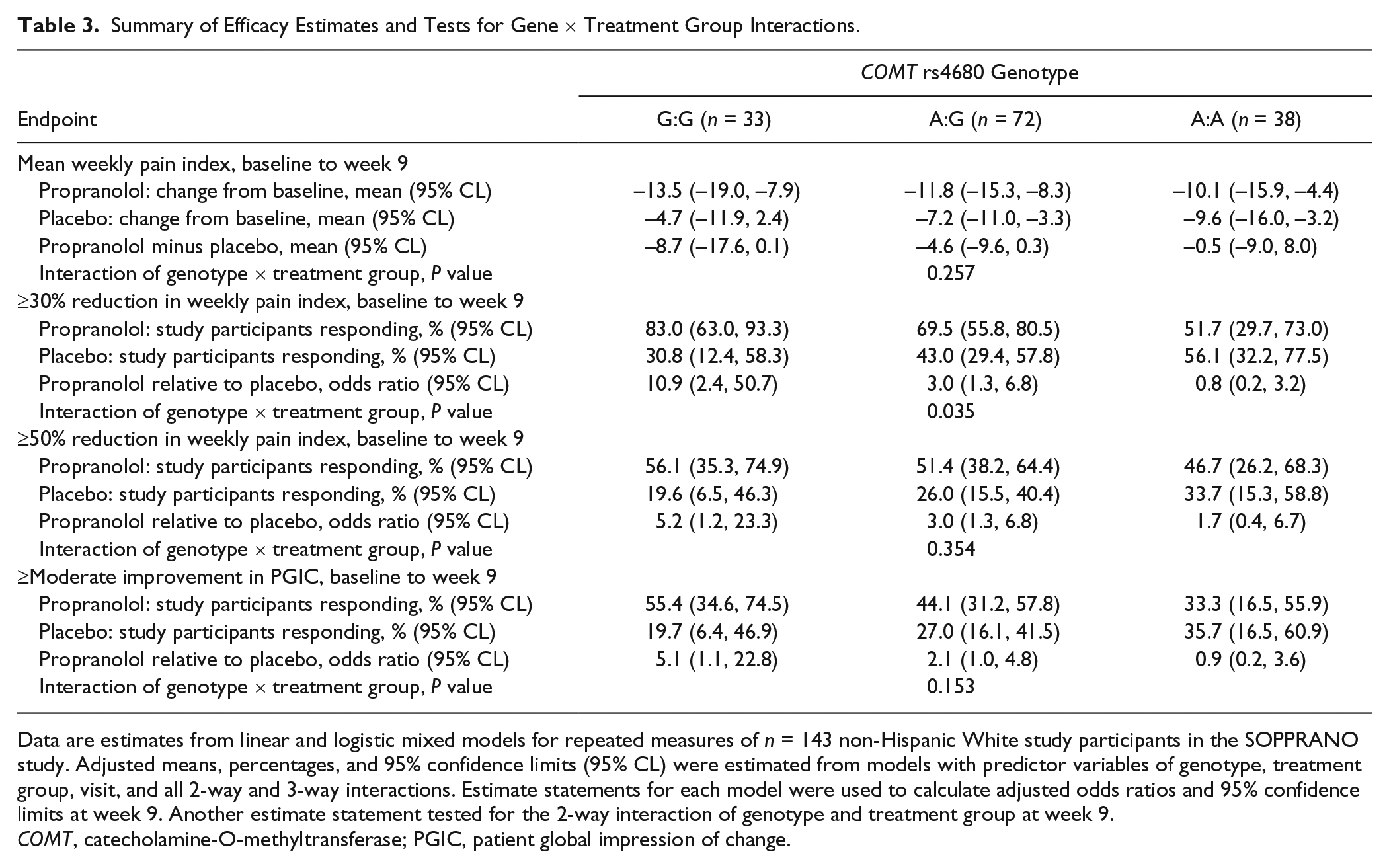
Data are estimates from linear and logistic mixed models for repeated measures of n = 143 non-Hispanic White study participants in the SOPPRANO study. Adjusted means, percentages, and 95% confidence limits (95% CL) were estimated from models with predictor variables of genotype, treatment group, visit, and all 2-way and 3-way interactions. Estimate statements for each model were used to calculate adjusted odds ratios and 95% confidence limits at week 9. Another estimate statement tested for the 2-way interaction of genotype and treatment group at week 9.
COMT, catecholamine-O-methyltransferase; PGIC, patient global impression of change.
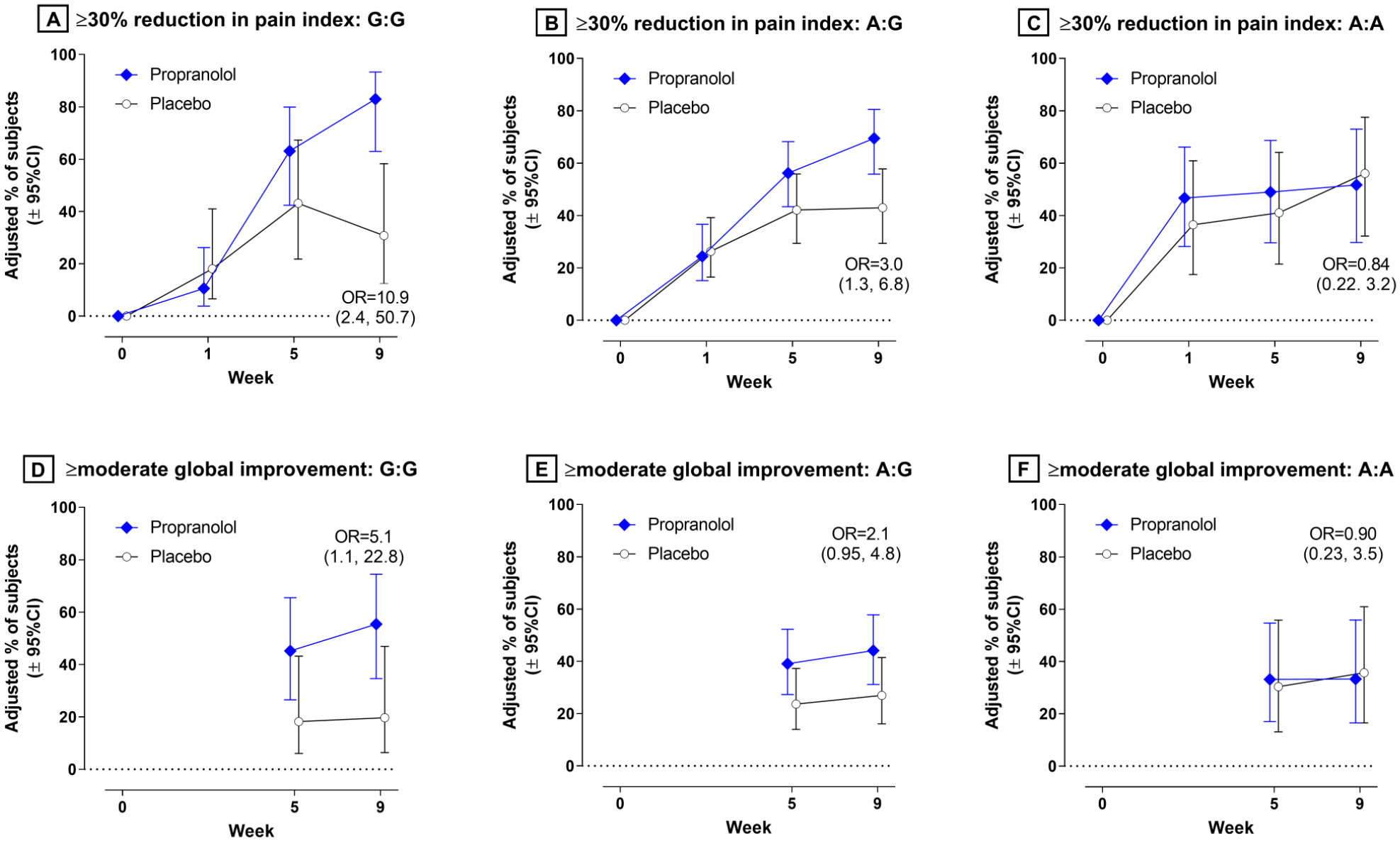
Change in 2 endpoints at 3 follow-up visits for study participants in 2 treatment groups stratified according to genotype of the rs4680 single nucleotide polymorphism of COMT. Endpoints were estimated for propranolol () and placebo () groups in regression models from n = 143 non-Hispanic White study participants in the SOPPRANO study. Endpoints were percentage of participants with at least 30% reduction in pain index plotted for (
When results were integrated for thresholds of 20% to 70% reduction in pain index, the propranolol-versus-placebo difference in cumulative response curves was greater for G:G homozygotes (43.7 percentage point difference in AUC, 95% CL = 15.4, 72.1) than for A:A homozygotes (6.5 percentage point difference in AUC, 95% CL = −30.2, 43.2). This genotype difference in treatment effect estimates was statistically significant (P = 0.003; Fig. 2). As shown in Figure 2, the attenuated efficacy in A:A homozygotes compared with G:G homozygotes was due to 2 factors: a lower probability of analgesic efficacy of propranolol and a higher probability of placebo analgesia.
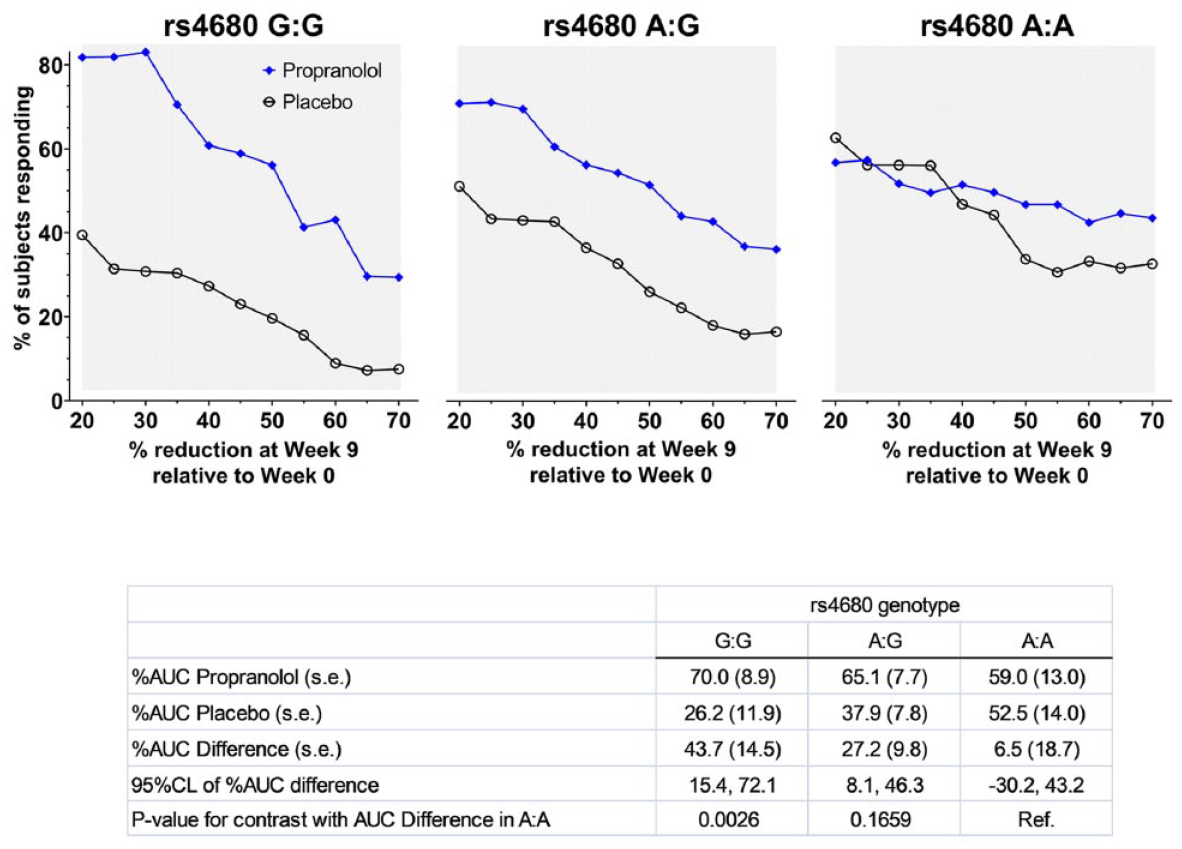
Cumulative response curves for facial pain index among study participants in 2 treatment groups stratified according to genotype of the rs4680 single nucleotide polymorphism of COMT: (
Effect Modification Analysis Using the PGIC Secondary Endpoint
Model-adjusted percentages of study participants reporting at least moderate improvement in their overall condition ranged from 19.7% (placebo) to 55.4% (propranolol) in G:G homozygotes (Fig. 1D), with a corresponding odds ratio of 5.1 (95% CL = 1.1, 22.8; Table 3). Odds ratios were 2.1 (95% CL = 1.0, 4.8) for A:G heterozygotes (Fig 1E:) and 0.9 (95% CL = 0.2, 3.6) for A:A homozygotes (Fig. 1F), although the interaction of genotype and treatment group at week 9 was not statistically significant (P = 0.153, Table 3).
Qualitative Evaluation of Credibility of the Overall Findings
The analysis fulfilled all 5 study design criteria used to evaluate the credibility of effect modification in RCTs (Sun et al. 2010), namely, 1) COMT genotype, the effect modifier, was measured at baseline; 2) efficacy was compared among subgroups within this study; 3) the hypothesis and 4) direction of the effect modification were specified a priori; and 5) the COMT genotype was the single effect modifier tested. There was mixed support for 2 analytic criteria (Sun et al. 2010), namely, 6) P values were significant at the P < 0.05 threshold for only 2 of the 5 analyses; 7) however, because those 2 analyses used the facial pain index, results were strongly correlated. There was also support for the contextual criteria (Sun et al. 2010), namely, 8) subgroup differences in effect estimates were large (e.g., odds ratios differed at least 5-fold across genotypes), 9) the interaction was consistent for the analysis of the secondary endpoint, and 10) there was a biological rationale for the hypothesized interaction. Overall, there is only moderate credibility of the effect modification because it was opposite to the hypothesized direction.
Sensitivity Analysis
When the COMT genotype was modeled as 3 categories, hence making no assumptions about the genetic model, estimates were very similar to the additive model (Suppl. Table. S1). Specifically, efficacy at week 9 was greatest for the G:G genotype, intermediate for the A:G genotype, and least for the A:A genotype. Results for the components of the facial pain index were similar to the index itself (Suppl. Table S2), and findings did not change appreciably when data were restricted to females (Suppl. Table S3).
Discussion
This RCT of study participants with painful TMD found some evidence that propranolol’s analgesic efficacy was modified by COMT genotype. Specifically, the A allele of rs4680 was associated with reduced efficacy, with the consequence that propranolol was superior to placebo in reducing the facial pain index among G:G homozygotes but not among A:A homozygotes. Although this constituted clinically meaningful differences in the magnitude of propranolol’s efficacy, the observed antagonistic effect of the A allele is counter to the hypothesized direction of effect modification.
Before considering the implications of this unexpected finding, the study’s limitations warrant consideration. For this secondary genetic objective, the statistical analysis plan specified that the primary endpoint be analyzed both as a continuous measure and after dichotomizing it at thresholds of ≥30% and ≥50% pain reduction. The 3 endpoints were consistent in showing antagonistic directions of effect for the A allele, although the gene × treatment group interaction was statistically significant only for the ≥30% threshold and in secondary analysis of cumulative response curves. This is counter to the conventional expectation that continuous variables yield greater statistical power (Snapinn and Jiang 2007). However, as noted for the primary paper from this study (Tchivileva et al. 2020), many study participants in the placebo group experienced reductions of <30% in the facial pain index, thereby reducing the efficacy signal from the continuous endpoint. Instead, there was greater power to detect a ≥30% reduction in pain, a measure that is favored as clinically meaningful for patients (Dworkin et al. 2009). In addition, calculated statistical power for effect modification was only 47% using the continuous endpoint. Nonetheless, the binary endpoint revealed statistically significant gene × treatment group interactions that were consistent with clinically meaningful differences in efficacy, although 95% confidence intervals were wide, making the estimates imprecise. However, we caution against overinterpreting the interaction P values that are less than 0.05 Instead, when all relevant criteria were considered (Sun et al. 2010), we found only moderately credible evidence for effect modification.
The current study has several strengths, including its randomized, placebo-controlled design with allocation concealment and masking. Consistent with the best practices for clinical trials of pain (Edwards et al. 2016), the primary endpoint was measured using daily pain diaries. The 9-wk follow-up period exceeded the minimum of 4 wk recommended for phase 2b trials (Gewandter et al. 2014). Pain-related characteristics measured at baseline did not differ appreciably between the treatment groups or COMT genotypes, making it unlikely that the gene × treatment group interaction was confounded by those characteristics. The sensitivity analysis revealed very similar results for different genetic models, and we therefore favor the additive model because it parsimoniously depicts the biological gradient.
The opposing directions of effect modification in the current and pilot study require scrutiny. Although both studies used the same endpoint, there were notable differences: the pilot study used a crossover design, enrollment was restricted to 40 women, the dose of propranolol was lower, and efficacy was analyzed after 1 wk. In general, parallel-group designs are favored for clinical trials because they require fewer assumptions when testing efficacy (Dubey 1986). The pilot study (Tchivileva et al. 2010) used a haplotype of COMT as the genetic marker, although the result for rs4680 was similar and hence does not account for the discrepancy with this study. In the current study, neither sex nor efficacy signals after 1 wk could account for the discrepancy.
A more salient difference between studies was the placebo group’s response: in the pilot study, there was effectively no reduction in facial pain in the placebo phase, whereas in the current study, there were substantial reductions in facial pain in the placebo group. In this study, the absence of efficacy for the A:A homozygotes was due as much to a heightened response (relative to G:G homozygotes) in the placebo group as it was to a diminished response in the propranolol group. Sizable responses in placebo groups are the norm in clinical trials of pain, suggesting that the antagonistic effect of the A allele seen here is more credible than the amplifying effect suggested by the pilot study. This effect of COMT on treatment response in the placebo group has parallels with a clinical trial of acupuncture for treatment of irritable bowel syndrome (Hall et al. 2012) and a study of experimentally induced placebo hypoalgesia in healthy human volunteers (Colloca et al. 2019).
Seemingly inconsistent effects of COMT have been reported in other clinical settings. One review concluded that the A allele of rs4680 is associated with a lower requirement for opioids in patients with a range of acute and chronic pain conditions (Vieira et al. 2019), whereas a subsequent study reported an opposing effect of the allele in postsurgical pain management (Matic et al. 2020). Likewise, systematic reviews of treatment for chronic postsurgical pain (Chidambaran et al. 2019) and neuropathic pain (Veluchamy et al. 2018) have reported opposing directions of association with the rs4680 genotype. Authors have speculated that the differences might be due to insufficient power (Landau et al. 2013), heterogeneity of patient populations (Chidambaran et al. 2019), or interactions with other pain regulatory systems (Matic et al. 2020).
Compared with the pilot study, these results provide stronger evidence that COMT modifies the analgesic efficacy of propranolol. It might therefore seem logical to recommend propranolol to TMD patients with A:G or G:G genotypes of rs4680. However, we caution that any such interpretation is premature. Instead, the contradictory directions of COMT’s effects seen here and in other pain studies demonstrate the need for biological and clinical research to reconcile the differences. This conclusion echoes a more general caution that “any plan to incorporate genotyping information into clinical pain practice is premature” (Mogil 2009). Indeed, this study adds to the enigma of COMT by revealing an antagonistic effect of the A allele of rs4680 on propranolol’s efficacy. The finding highlights the need for better knowledge of COMT’s role in pain pathogenesis if the gene is to be used for a precision medicine approach to TMD.
Author Contributions
G.D. Slade, contributed to conception, design, data analysis, and interpretation, drafted and critically revised the manuscript; R.B. Fillingim, R. Ohrbach, contributed to conception, design, data acquisition, and interpretation, critically revised the manuscript; H. Hadgraft, contributed to data acquisition, critically revised the manuscript; J. Willis, contributed to data analysis, critically revised the manuscript; S.J. Arbes Jr., contributed to conception, design, and data interpretation, critically revised the manuscript; I.E. Tchivileva, contributed to conception, design, data acquisition, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
DS_10.1177_0022034520962733 – Supplemental material for COMT Genotype and Efficacy of Propranolol for TMD Pain: A Randomized Trial
Supplemental material, DS_10.1177_0022034520962733 for COMT Genotype and Efficacy of Propranolol for TMD Pain: A Randomized Trial by G.D. Slade, R.B. Fillingim, R. Ohrbach, H. Hadgraft, J. Willis, S.J. Arbes and I.E. Tchivileva in Journal of Dental Research
Footnotes
Acknowledgements
The authors thank the SOPPRANO research staff and patients who participated in the trial. The authors also thank cardiologists Drs. Alan Hinderliter (UNC at Chapel Hill), David Sheps (University of Florida), and Thomas Cimato (University at Buffalo) for monitoring participants’ safety.
A supplemental appendix to this article is available online.
The trial is registered at ![]() , NCT02437383. Full details of the trial protocol are available at ClinicalTrials.gov.
, NCT02437383. Full details of the trial protocol are available at ClinicalTrials.gov.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the National Institutes of Health (NIH)/National Institute of Dental and Craniofacial Research (NIDCR) R34-DE022088 and U01-DE 024169 grants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.