
Abstract
Mental health remains a critical concern within the Black communities in Canada, influenced by systemic racism, stigma, and cultural beliefs. Despite the importance and influence of intergenerational perspectives in seeking and use of care, research in this area is scarce. This study identifies mental health perceptions among Black youth and parents and examines how stigma, cultural beliefs, and experiences of racism influence these perceptions. We conducted semi-structured interviews with 32 Black youth aged 15 to 24, (mean age = 20.69 years, SD = 2.25) and 27 Black parents (mean age = 44.88, SD = 10.40) from May 2021 to April 2023. Interviews conducted via Zoom were transcribed and analyzed inductively and thematically using multiple rounds of coding, allowing themes to emerge organically without being guided by predetermined categories. Analysis identified three key themes showing important differences between Black youth and parents: (a) an acculturation gap characterized by older generations’ adherence to cultural norms and stigma surrounding mental health, (b) differing perceptions of stressors between youth and parents, with older generations prioritizing financial challenges and minimizing emotional struggles, and (c) youth-driven motivation for change, emphasizing greater mental health awareness and openness for future generations. Youth reported barriers to discussing mental health with older family members due to stigma, concerns about family reputation, and cultural expectations of resilience. This study highlights significant intergenerational differences in mental health perceptions within Black Canadians, shaped by acculturation, values, and social expectations. While older generations often prioritize cultural preservation, resilience, and privacy and minimize mental health struggles, youth are advocating for change.
Introduction
Despite efforts in recent years, such as the first publications on the prevalence and factors associated with common mental health problems, the creation of research centers on Black health, and the establishment of dedicated research funds by the federal government, mental health remains a critical public health concern within Black communities in Canada (Cenat et al., 2021; Cénat, Lashley, et al., 2024; Faber, Osman, et al., 2023; Public Health Agency of Canada [PHAC], 2018; Williams et al., 2022; Williams, Moshirian Farahi, et al., 2024). Stigma and silence continue to surround mental disorders in many families, often preventing open dialogue and access to care, especially among youth whose understanding of mental health frequently clashes with that of older generations (Fante-Coleman & Jackson-Best, 2020; Guruge et al., 2017; Kuo et al., 2015). Understanding and addressing mental health in Black communities also requires a critical examination of the broader social and structural determinants that place Black individuals at risk in Canadian society.
Mental Health Challenges in Canadian Black Communities
Studies conducted in recent years have shown that Black Canadians face a set of social factors that can be decisive for their mental health. Research conducted since the establishment of the Black Community Mental Health Fund by the Canadian federal government (Public Health Agency of Canada (PHAC), 2018) has identified individual, social, and cultural determinants of the mental health of Black people in Canada (Cénat, Darius, et al., 2023; Cénat, Dromer, Auguste, et al., 2023; Cénat, Dromer, Darius et al., 2023; Cenat et al., 2021; Cénat, Hajizadeh, et al., 2022; Cénat, Kouamou, et al., 2022; Cénat, Moshirian Farahi, Gakima, et al., 2025; Darius et al., 2024; Fante-Coleman, Jackson-Best, et al., 2023; Fante-Coleman & Jackson-Best, 2020). These determinants include socioeconomic status, educational disparities, unemployment, underemployment and job insecurity, poverty, income inequality, unfavorable environmental characteristics, poor quality and instability of housing, food insecurity, limited access to health care, challenging immigration experiences, and early adversities (Cénat, Dromer, Auguste, et al., 2023; Cénat, Kogan, et al., 2023; Cénat, Moshirian Farahi, Bakombo, et al., 2023; Cénat, Moshirian Farahi, et al., 2024; Chiu et al., 2015; Darius et al., 2024; Etowa et al., 2021; Fante-Coleman, Jackson-Best, et al., 2023; Kemei et al., 2023; Kogan et al., 2022; Konkor et al., 2021; Maynard, 2017; Nelson et al., 2019; Nguemo Djiometio et al., 2020; Patterson & Veenstra, 2016; Turcotte, 2020, 2015, 2016; Williams, Moshirian Farahi, et al., 2024). In addition, Black people also face various forms of social exclusion, daily experiences of discrimination and racism, racist microaggressions, as well as major experiences of discrimination and racism in different spheres of society, including education, housing, employment, health care, and racial profiling by the police (Cénat, 2024; Cénat, Hajizadeh, et al., 2022). Studies conducted at the Interdisciplinary Center for Black Health at the University of Ottawa have shown that racial discrimination is the most significant factor explaining psychosomatic symptoms, anxiety, depression, PTSD, as well as substance abuse, low self-esteem, and suicidal ideation among Black people in Canada (Cénat, Dalexis, Darius, et al., 2023; Cénat, Dromer, Auguste, et al., 2023; Cenat et al., 2021; Darius et al., 2024; Kogan et al., 2022).
Studies have also shown that Black Canadians encounter significant barriers to accessing mental health services. A scoping review revealed that Black youth face systemic barriers, including wait times, a lack of mental health professionals, and financial barriers, among others (Fante-Coleman & Jackson-Best, 2020). It also identified practitioner-related barriers, including racism and discrimination from providers and their inability to deliver culturally competent mental health care. This aligns with other research showing that clinicians lack the competence to provide culturally adapted and anti-racist care (Cénat, Broussard, et al., 2024). This review and other studies have also highlighted a critical shortage of mental health professionals from the community, as well as community-related barriers, including the persistent stigma associated with mental health in Black communities (Fante-Coleman & Jackson-Best, 2020; Sarr et al., 2022). In fact, even when services are accessible, there is often reluctance within Black communities to seek help due to distrust of a health care system that has historically marginalized and discriminated against racial minorities. Consequently, many Black Canadians turn to informal support networks or adopt coping strategies that do not always address their distress effectively (Jacob et al., 2023).
Beliefs and Stigma Surrounding Mental Health in Black Communities
Mental health remains a stigmatized issue within Canadian Black communities, thereby increasing challenges related to prevention and perpetuating stereotypes that hinder open discussions and discourage individuals from seeking help (Bodnar-Deren et al., 2017; Logie et al., 2016; Rose et al., 2011; Taylor & Richards, 2019). One of the most widespread stereotypes is the myth of weakness associated with mental health issues, often perceived as a personal failure rather than a legitimate response to psychological distress (Cénat, 2022; Fante-Coleman & Jackson-Best, 2020; Lindsey et al., 2010; Rose et al., 2011). This belief stems from cultural ideals that Black individuals must display “strength” in the face of adversity, leading many people to internalize “resilience” as a norm and to avoid revealing their personal struggles (Cénat, 2022). As a result, those who seek professional help may be perceived as lacking resilience, further reinforcing stigma and making access to care challenging without fearing social judgment (Fante-Coleman & Jackson-Best, 2020). This stigma linking mental health issues is still prevalent among Canadian Black men (Cénat, 2022). Often, there is a perception of weakness toward men who experience mental health problems or who have consulted a mental health professional. Since seeking help can be perceived as a sign of weakness, many individuals are reluctant to seek help to preserve their image and social respect.
Furthermore, for many Black Canadians, religious and spiritual communities play a central role in managing emotional and psychological stress (Alaazi et al., 2024; Bilkins et al., 2016; Fante-Coleman, Allen, et al., 2023). Some believe that prayer, faith, and resilience are the preferred solutions to mental health issues, which can lead to a reliance on spiritual support to the exclusion of professional care. Indeed, mental health issues are often perceived as a spiritual failure (Fante-Coleman, Allen, et al., 2023). In many Black families, when a mental health disorder or psychosis emerges in parents or youth, prayer is preferred over mental health care (Bilkins et al., 2016; Cénat, Dromer, Darius, et al., 2023; Cénat, Lashley, et al., 2024). This stigma is also fueled by the historical distrust that Black people in Canada have toward the health care system (Cénat, Moshirian Farahi, Bakombo, et al., 2023; Cénat, Moshirian Farahi, et al., 2024). This distrust is also associated with racism, discrimination, and mistreatment faced by Black individuals in the health care system (Cénat, 2024). This makes them hesitant to seek help for fear of misdiagnosis and because mental health professionals are not sufficiently trained to provide adequate care (Williams, 2020; Williams, Cénat, et al., 2024).
In response to mental health stigma, coping mechanisms in Black communities emphasize autonomy, spirituality, and community and religious support rather than professional intervention (Fante-Coleman, Allen, et al., 2023). While these strategies provide essential support, they are not sufficient for individuals with severe or chronic disorders. Their inability to cope on their own reinforces stigmatizing beliefs surrounding mental health care and the perceived weakness of those who seek it. Individuals are thus encouraged to manage their mental health issues privately, which can exacerbate their isolation and mental health difficulties.
Perceptions of mental health may differ based on the generation of Black people considered. However, no study in Canada, the United States, or Europe has addressed this issue with an intergenerational perspective, questioning both young people and parents. In Canada, very few studies explore mental health perceptions in Black communities. In addition, very few explore mental health perceptions separately among youth and the parents of adolescents and young adults.
The Present Study
Given the observed gap and the importance of exploring the perspectives of youth and parents of young people, this study explores intergenerational perspectives on mental health within Canadian Black communities. It focuses on how cultural beliefs, stigma, and experiences of systemic racism shape perceptions and attitudes related to mental health across generations. Since younger generations of Black Canadians are more influenced by Canadian norms and values, whereas older generations often retain cultural beliefs from their countries of origin, these intergenerational differences provide important insights into mental health perceptions within Black communities. This study aims to shed light on these complex experiences by identifying factors that promote or hinder openness to mental health care within families.
Understanding these intergenerational perspectives is essential for developing culturally sensitive and anti-racist mental health interventions that meet the specific needs of Black families. Without taking into account the cultural and racial influences that shape mental health beliefs, providers risk reinforcing stigmatization. By studying these generational attitudes, we hope to provide insights that will guide more inclusive mental health policies, reduce stigma, and improve mental health outcomes for Black Canadians.
The primary objective of this study is to examine perceptions and attitudes related to mental health across generations within Black Canadian families. Specifically, we seek to identify key themes in mental health perceptions among older and younger generations and to examine how stigma, cultural beliefs, and experiences of racism influence these attitudes. To achieve this, we address the following research questions:
Research Question 1: What are the predominant beliefs and attitudes regarding mental health among older and younger generations in Black Canadian communities?
Research Question 2: How do youth perceptions of mental health differ from those of the older generation?
Method
Procedure
This study utilized qualitative data from the Black communities’ mental health in Canada (BCoMHeal) project (Cénat, Manoni-Millar, David, Darius, et al., 2025; Cénat, Manoni-Millar, David, Moshirian Farahi, et al., 2025). Semi-structured interviews were conducted among two groups of Black youth and parents between May 2021 and April 2023. For Black youth, eligibility criteria for participants included: (a) self-identifying as Black, (b) being between 15 and 24 years old, (c) residing in Canada, and (d) fluency in either English or French (the two Canadian official languages). For Black parents, eligibility criteria for participants included: (a) self-identifying as Black, (b) being parents of Black youth aged 15 to 24 years old, (c) residing in Canada, and (d) fluency in either English or French. To address recruitment challenges commonly faced in health research involving Black communities in Canada, snowball sampling was used (Naderifar et al., 2017; Noy, 2008). Initial recruitment was facilitated by community organizations and religious institutions that serve Black communities in Canada, whereas digital recruitment materials were also shared on Instagram, Facebook, and Twitter, with paid advertisements expanding the reach. Ethical approval was obtained from the research ethics boards of the University of Ottawa and l’Université du Québec en Outaouais. Interviews were conducted on Zoom by research assistants fluent in French and English and lasted about 40 min in both groups. After research assistants explained the study’s objectives and informed participants about the recording, participants provided consent through an online form and completed a brief socio-demographic questionnaire, including gender, age, education level, and employment status. Following each interview, participants received a debriefing form to mitigate any emotional discomfort from discussing their experiences, along with a $30 electronic gift card as compensation. Interviews were transcribed verbatim by research assistants.
Participants
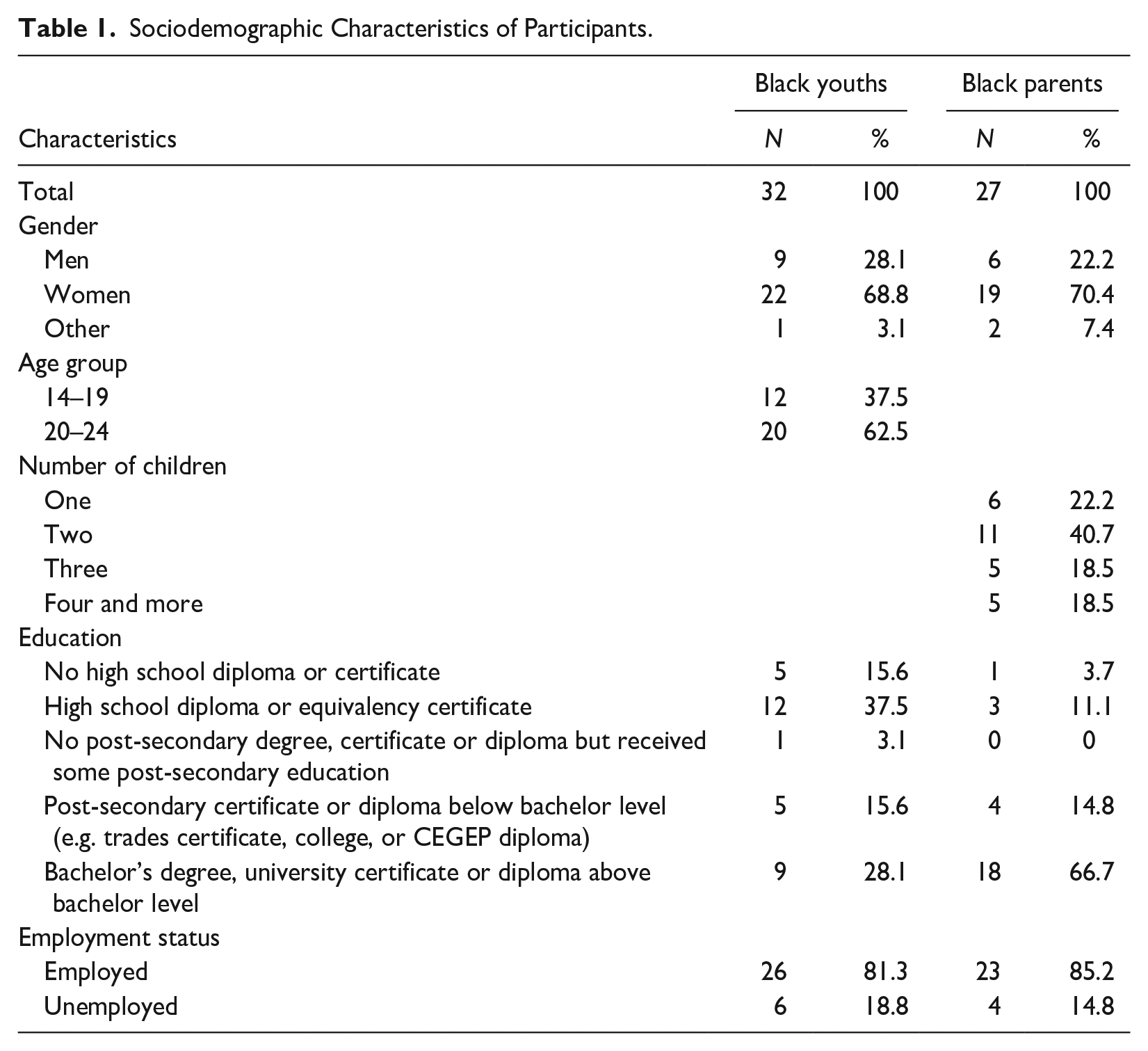
For the first group, a total of 32 Black youths, with an average age of 20.69 years (SD = 2.25) were recruited. Most participants (68.8%) identified as women. In addition, 81.3% of participants were employed and 37.5% held a high school diploma as their highest education level. Table 1 presents the sociodemographic characteristics of the sample. Data saturation determined the final sample size, achieved with 32 participants who met the study’s inclusion criteria. For the second group, a total of 27 Black parents (19 women) were recruited, with an average age 44.88 years old (SD = 10.40). Data saturation was reached after 13 interviews, indicating the end of recruitment. Table 1 presents the sociodemographic characteristics both samples.
Sociodemographic Characteristics of Participants.
Data Analysis
All interviews were transcribed verbatim and were analyzed in their entirety using NVivo 14. The data analysis used an inductive, data-driven exploration guided by Braun and Clarke (2006, 2024). The analyses were completed free of any pre-existing theories or framework and used Braun & Clarke’s six-step method for thematic analysis (Braun & Clarke, 2006, 2024)
To find the general themes, several iterations of coding took place. Interviews were first coded (Level 1) with descriptive codes by two researchers (SMM, AD) independently. The researchers then compared initial codes for similarities and discrepancies. When the descriptive codes were organized by similarity, we then developed thematic codes that aligned with the description. Next, the researchers collated the codes into potential themes gathering all initial codes relevant to each other. When themes were identified, SMM checked themes against each other in the original data set and recoded the data using the new themes and subcodes derived from the initial codes (Level 2). The new coded data set was then reviewed by AD. Ongoing discussion took place to refine the specific themes and generated clear definitions and names for each theme. The analysis achieved inter-rater reliability where the codes applied to the data remained consistent across Level 1 and Level 2 coding, thus ensuring the interpretation of the interview content was consistent between SMM and AD.
Throughout the methodology described above, we aimed to ensure rigor in part to acknowledge the researchers’ social placement and how our understandings may impact the research. Throughout the coding and analysis process, we used reflexive journaling and memo-ing to document and reduce researcher biases and stay true to participant narratives.
Researchers’ Positionality Statement
All the interviews were conducted by experienced and well-trained Black research assistants. As researchers, we acknowledge that our identities, backgrounds, and lived experiences influence our approach to this study. The first analyses were performed by SMM and AD. SMM is a White psychological researcher with a mental disability, whose training and expertise are rooted in community mental health. AD, a Person of Color, is both a registered counselor and a psychological researcher. Their diverse perspectives bring complementary strengths to the research process. However, throughout the analyses process, both were engaged in active reflexivity to minimize potential biases. In addition, given the cultural dimensions of this study, the analyses were informed by those with lived and professional expertise in Black communities. To this end, our coding and interpretations were reviewed in consultation with Black members of the research team (JMC, WPD, and AN). Furthermore, the principal investigator, JMC, a Black clinical psychologist and senior researcher, and the fifth author, a Black nurse and senior researcher, provided oversight to ensure that cultural and race-based nuances were accurately captured and appropriately contextualized. Finally, we used cultural humility in interpreting the results, recognizing the limitations of our perspectives while prioritizing the voices and experiences of the those interviewed.
Results
The analysis of the interview transcripts contained compelling narratives regarding mental health perceptions across generations. Three major themes were identified reflecting the values and beliefs of mental health over time. First, an acculturation gap and changing mental health beliefs, second a differing perception of present-day stressors, and third motivation for change in future generations. A breakdown of the themes and subthemes can be found in Figure 1. All names used are pseudonyms to protect participant identity.
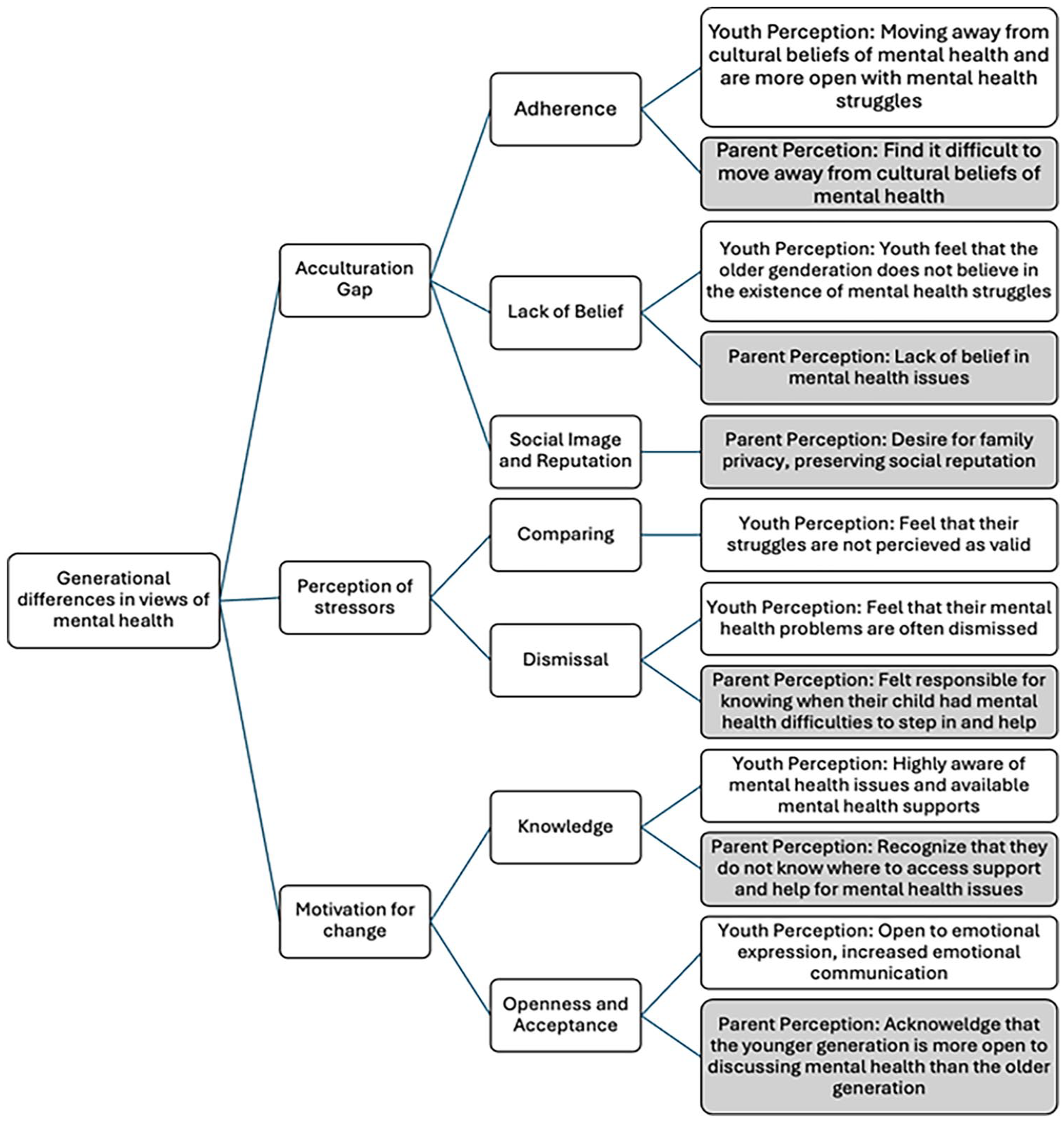
Thematic Analysis Codes and Themes.
Acculturation Gap and Changing Mental Health Beliefs
The acculturation gap is identified by the older generation’s adherence to culture, their lack of beliefs that mental health merits attention, and the emphasis on keeping up with a social image. When discussing adherence to cultures, despite being in a new environment youth felt that the older generations wanted to remain as close to the culture and values of the country and region of origin. Many youth indicate that they feel like strangers to their parents as they are immersed in a completely new culture and new values:
The perception of being a first-generation immigrant is, like literally the most insane and like, unique view and perception, because like, our parents lived in another country their whole lives and now they’ve come and now they have to raise kids in a new country that they know nothing about. And they are trying to keep the same values that they’ve learned- possessed- all they know, but like we are constantly being like exposed to a completely new different culture, values things like that so they are really, like, raising kids that are almost strangers to them. (Isabel, 22, Young Woman)
Because of this, youth do not feel like they are able to be open about their mental health because it is not in the culture of how they were raised.
When discussing mental health nearly all youth state that “often times parents don’t really, don’t really believe it or don’t really want to do something about it.” (Lillian, 18, Young Woman) Youth expressed that the older generation often characterizes the openness about stressors or struggles as simply overreacting. As parents, and members of an older generation, they do not believe that mental health exists or is something that merits attention, they have been taught not to sit with emotions and work hard. A parent shares:
[The cup is] not even half full! We are empty and we are pouring and are pouring and pouring. We burn out and we do not know how to process and take the time to say how am I feeling today? And sit there with it. Because it’s uncomfortable to sit there because we’ve been taught by our boomer parents: Grind, grind, grind. (Fatima, 44, Mother/Woman) . . .we were taught to work and put aside complaining, complaining, and complaining. It won’t solve anything. We were raised to keep moving forward and to arm ourselves with courage. (Widmark, 51, Father/Man)
Given this trend, youth tend to retreat and mask their mental health struggles, leaning into the assumptions that mental health is not something that is worth discussing: “because they don’t believe that like, like as long as you’re masking it well, then it doesn’t exist, right? So, like if you’re not really outwardly showing signs of mental unwellness then everything’s fine, everything’s smooth sailing.” (Delilah, 23, Young Woman)
Above all, the most discussed aspect of an acculturation gap was the emphasis on keeping up with social image and ensuring that the family name is not tarnished. One youth participant states: “They don’t want to bring like shame or dishonour to the family.” (Lillian, 18, Young Woman) Youth talked about how there was a greater importance for hiding their mental health struggles for fears of being labeled as “crazy.” One youth participant sought out therapy in secret to avoid the shame that it may bring on the family shares. They share:
I do remember when my dad passed away it was 2 years ago, um, I wasn’t allowed to see a therapist because my mom kind of saw that as me being crazy and I wasn’t really allowed to grieve either because as I said in my culture you can’t really like have feelings. (Tiana, 18, Young Woman)
In similar vein, a parent shares:
We also have the mentality even my parents or my aunts older than I am that would not seek counselling, do not tell others your business, keep it within the family but the family themselves do not have the resources and support for that. Especially for people from the Caribbean that come here and have the cultural differences then you don’t necessarily know how to deal with it. So we’re not equipped as parents either. (Yasim, 45, Mother/Woman) As Africans, we don’t like to talk much about our problems. In the past, the resources were within the family itself. Together, we found solutions to the difficulties we encountered. When someone had a problem, everyone was there. Even if we didn’t have the skills, together, it made a difference. (Donald, 47, Father/Man)
Moreover, within this acculturation gap there was an increased perceived desire for privacy among an older Black generation. This value of privacy was subsequently passed on to youth. Youth discussed that your problems do not need to be solved by letting strangers or professionals into your support network. One shares.
I think in the Black community or minority communities there’s a lot of-a lot of emphasis on privacy, right? On keeping everything inside the house inside the family [. . .] so a lot of Black people they have this certain image that they have and they [. . .] want to keep that image so even if they’re not well they’re not going to go look for professionals because they think-they think talking to friends, talking to your partner or talking to your family or going to church or praying to God or all that’s going to help. (Xavier, 22, Young Man)
Differing Perception of Present-Day Stressors
When youth shared their present-day stressors, they often shared that they found their parents and members of the older generation often responded by comparing them to stressors they had in their time. This was dismissive of the youths’ experiences. When youth express stressors, such as educational or relational, they are often faced with the response that those are not real issues. While parents did not discuss this comparison, it was evident that youth felt a distinction. They discussed that their parents saw financial struggles such as paying bills or maintain a house, as genuine challenges, whereas emotional struggles did not merit attention. As one youth participant shares:
Maybe sometimes parents have a tendency to minimize our problems without even realizing it, they’ll say ‘well I have to pay the bills anyway, electricity, water, rent, so I have more problems than you do,’ so they’ll minimize our problems and like they’ll just say, ‘just concentrate on your studies’ and that’s the end of it. (Brielle, 18, Young Woman. Translated from French)
Moreover, when youth would share mental health struggles, they shared that it would be followed up with a sense of perceived ungratefulness. This feeling stemmed from the perceived feeling that their parents and older generations emphasized the support and opportunities youth received. For example:
If you are crying like emotionally hurt as a kid your mom would tell you do you want me to give you something to cry more about? You know its just, growing up in that way you know like Black kids are supposed to be more resilient. (Elijah, 22, Young Man)
However, that parent participants discussed that they felt it was their responsibility to be aware of their child’s mental health and needs and seek out professional help. There was a significant disconnect in the youth and parent narratives on how parents approached these issues. However, despite the desire to help, they understood that there is an ingrained perception to be more resilient and that vulnerability is perceived as weak in their culture: “I think all communities, especially in the Black community where people are just like, the vulnerability is just not a safe space. Being vulnerable does not feel safe.” (Fiona, 44, Mother/Woman)
Motivation for Change in Future Generations
The youth in this study emphasize a desire for change in the community of younger Black individuals:
‘Cause there’s some kids who are going through, cause our parents thought we are born or we are made of wood, we don’t have any feelings, you can crush us we won’t you know? This is not gonna happen, we have feelings too and I think this is something that we should let parents, or not even parents but you know adults, African adults, Caribbean adults, Black adults in general knows that kids have problems. (Chantal, 21, Young Woman)
They held a positive vision for future generations and were motivated to change the view of mental health across their community. They talked about having more knowledge of what mental health is and displaying more acceptance and openness about experience and discussing mental health struggles.
Overall youth emphasized that they felt that their parents and members of the older generations, especially those who immigrated, were less aware of what experiencing mental issues meant. For example, one youth shares:
I don’t know if culturally that’s the case for everyone, but I know for me growing up, like my parents were not really aware of mental health. It wasn’t like a thing that was discussed about so it was more of so like “oh suck it up you’re just being a baby,” you know? (Destiny, 22, Young Woman)
Parents also shared that [T]hey don’t have the information and the knowledge as to where to seek help for their child? So they will not know who to call, who to advocate to or offer a kind of substantial information that can be beneficial to the-, to the individual. (Naomi, 46, Mother/Woman)
Similarly, a father highlights:
In general, Black parents don’t know where to seek help for their children. We fear that things will go wrong when requesting services. You don’t know if they will put this in your child’s file and if it will become a long-term disadvantage for them. (Ritho, 49, Father/Man)
Youth expressed that they lean on friends from the same generation for mental health support as there is a greater acceptance. In addition, they emphasize that while previous generations do not acknowledge mental health struggles, they hope that the knowledge about mental health and available resources is not neglected for future generations:
It’s like two different worlds (between youth and parents). Mental health really is important because it’s unfortunately our parents they don’t really understand to the point that how we understand. When because we grew up here so that’s really my only wish that we have a better umm until we work better on mental health, and that we neglect- That we stop neglecting the mental health of, of young black people, but I know we’re capable because we really have this potential in the future. (Simone, 19, Younger Woman)
As aforementioned, youth report that the older generation have the impression that if individuals display mental health struggles that people will view them as “crazy” or “weird” and that it may tarnish the reputation of the family. Highlighting this impression, a parent shares:
[W]hen people talk about mental health, sometimes the Black people the way they perceive it is like ok, umm, [. . .] mental health to them is like, oh, it’s crazy, it’s disorganized. Oh this is a lunatic person, that needs to be locked up. So they don’t like to use that language. If there’s another words that can represent mental, instead of using mental health, if they rephrase it to be, to be something else that is more, a little bit. . . uhh, easier. (Savannah, 52, Mother/Woman)
For this reason, youth are not open and do not trust the older generation when sharing their mental health struggles.
Youth report increased comfort disclosing their stressors to friends of similar age. They indicate that their generation are more likely to be open to listening to their experiences. To explain this, one youth shares:
I don’t think they would put their trust in older people just yet or else like maybe they’re afraid ‘cause there are a lot of different like um reasons I know that for some people they’re afraid that like um they’ll be seen as crazy or for other people they’ll be seen as like weird kind of um I do know that if I were ever upset I would tell my friends first I wouldn’t really tell my family or else they’ll like treat me differently. (Zendaya, 18, Young Woman)
Youth want to create a better future for the next generation by promoting greater acceptance and openness around mental health. They aim to improve mental health knowledge, support, and disclosure to better support youth in the future. One youth shares that with the lack of cultural barrier, future generations will be better equipped to cope with mental health, making it easier to have these conversations:
I think some parents think they know their kids, but they don’t. So that’s like, hard to talk about. But I think, like you know, the next generation will be we’ll probably, we’ll have these conversations a little bit better because we’ll understand, um, what they’re going through because we’ve lived in this country and understand what certain things are. (Isabel, 22, Young Woman)
Discussion
This study explored the mental health perceptions of younger and older generations of Black individuals in Canada. The findings revealed significant differences in mental health perceptions between youth and their older family members, largely influenced by acculturation, cultural beliefs, and social expectations.
Youth, often more immersed in Canadian society, were open to recognizing mental health as an important aspect of well-being. In contrast, parents or older generations adhered more strongly to cultural views that prioritize physical resilience and privacy, viewing mental health struggles as secondary to tangible challenges, such as financial stability or educational success. This difference left youth in the study feeling that their mental health experiences are dismissed or minimized, leading them to internalize struggles rather than seek informal support, or seek support without the knowledge of their families.
Cultural values of resilience, privacy, and maintaining a positive family image play a significant role in shaping parental attitudes toward mental health. Many youths expressed that their parents view mental health openness as a potential threat to family reputation or as a sign of weakness. This likely stems from cultural norms that discourage the outward expression of vulnerability. In addition, social stigmas around mental health within Black communities often links to the perception that seeking help implies weakness or instability. This discourages both youth and parents from engaging in open mental health discussions. These findings are echoed in a scoping review, supporting that Black youth in Canada may delay seeking mental health care due to cultural stigma and fear of judgment from family and community (Fante-Coleman & Jackson-Best, 2020). Many void acknowledging symptoms to prevent being labeled as “crazy.”
Moreover, our findings align with several Canadian studies that identify various stigmas perpetuating stereotypes related to mental health and prevent mental health seeking in the Black communities (Bodnar-Deren et al., 2017; Cénat, 2022; Cénat, Lashley, et al., 2024; Logie et al., 2016; Rose et al., 2011; Sarr et al., 2022; Taylor & Richards, 2019). Black Canadians face significant barriers to mental health access, including racial discrimination in health care, financial and socioeconomic challenges, over-pathologization and misdiagnosis (Cénat, 2024; Jarvis et al., 2023; Knight et al., 2021, 2023; Sarr et al., 2022). The shortage of culturally competent providers, and the lack of Black mental health providers further exacerbates the challenges for Black Canadians’ mental health access (Cénat, 2024; Jarvis et al., 2023; Knight et al., 2021, 2023; Sarr et al., 2022). Researchers highlight how racial discrimination in health care fosters mistrust, which increased stigma and reduces service use among Black communities (Cénat, 2024; Fante-Coleman & Jackson-Best, 2020). This issue, exacerbated during COVID-19, underscores the urgent need for equitable, culturally responsive mental health interventions.
Although the intergenerational differences highlighted in this study are particularly pronounced within Black families in Canada, they are not exclusive to them (Feng et al., 2023; Livingston et al., 2018; Philippe, 2022; Valenzuela, 2023). Indeed, studies conducted in Canada and elsewhere have shown similar stigmas among various cultural and racial groups, including Arab, Asian, Black, and Latinx individuals (Chang et al., 2013; Do et al., 2020; Feng et al., 2023; Guruge et al., 2017; Kuo et al., 2015; Youssef & Deane, 2006). These intergenerational differences are even more pronounced among immigrant families in Western countries, due to the acculturation gap and differing perceptions of mental health and the ability to deal with adversities (Chang et al., 2013; Do et al., 2020; Feng et al., 2023; Kuo et al., 2015; Rodriguez, 2024). The clash between cultural values from the country of origin and those of the host country, as well as the silence surrounding mental health issues and the associated stigma, are echoed in the narratives of both youth and parents from various ethnocultural groups (Chang et al., 2013; Philippe, 2022; Youssef & Deane, 2006). This suggests that while the expressions and contexts may differ, intergenerational dynamics related to mental health within racialized communities are, to some extent, shared across ethnocultural boundaries.
However, youth in the study sample exhibited a stronger motivation to shift these attitudes in future generations, aspiring to promote a more supportive and accepting environment. This motivation supports findings from a study conducted on the perception of mental illness and stigma among African Americans (Ward et al., 2013) that found increased psychological openness and help seeking tendencies in the younger African American population. The authors also found that the younger group preferred the use of professional help, informal support, and religious coping. Youth can experience the “best of both worlds,” adapting flexibly to new cultural contexts while forming a more open perspective on developing bicultural or multicultural competence and an integrated self-identity, youth are better equipped to navigate and reconcile diverse cultural expectations in their new environment (Phinney et al., 2001). Indeed, bicultural identity theory provides a valuable lens for understanding how Black individuals in Canada reconcile their cultural heritage with mainstream societal expectations, or navigate dual cultural expectations while fostering resilience (Meca et al., 2019; Medina et al., 2019). Unlike in the United States, where racial identity politics often shape experiences of belonging, Canada’s multicultural framework promotes integration while sometimes downplaying the systemic barriers that racialized communities face (Cénat, Hajizadeh, et al., 2022; Medina et al., 2019). This dynamic influences how different generations navigate their cultural identities and mental health perceptions (Fante-Coleman, Allen, et al., 2023).
The positive trend observed in Black youth is reinforced by a report from Harvard’s Graduate School of Education (Making Caring Common, 2023), which found that Generation Z young adults appear more emotionally aware and open about mental health challenges than any previous generation. As Black Canadians’ willingness to seek mental health services is often influenced by feelings of shame associated with needing help (Taylor & Kuo, 2020), there is valuable insight to be gained from the openness demonstrated by younger generations. Capitalizing on their increased comfort with mental health could help bridge the generational gap, fostering more acceptance within older generations and reducing stigma across the community.
Moreover, Canada’s publicly funded health care system, while offering universal coverage, does not always equitably serve Black communities (Cénat, Dromer, Darius, et al., 2023; Cénat, Lashley, et al., 2024; Faber, Khanna Roy, et al., 2023). Structural barriers, including a lack of culturally competent care, historical mistrust in medical institutions, psychiatric coercive care, and limited representation of Black mental health professionals, contribute to skepticism among older generations (Cénat, Lashley, et al., 2024; Faber, Khanna Roy, et al., 2023; Knight et al., 2023). These factors often discourage help-seeking behaviors, reinforcing stigma around mental health. By critically examining the socio-political and health care structures, we can gain deeper insight into how generational differences in mental health attitudes emerge. This underscores the necessity of culturally responsive interventions that not only acknowledge acculturation and resilience but also actively engage Black communities in addressing systemic inequities and fostering trust in mental health care.
Implications for Practice and Research
The insights gained from this study highlight specific implications for mental health practice and research. Developing culturally sensitive mental health education programs that address the unique stressors faced by Black youth is imperative, especially to first- and second-generation immigrant families (Cénat, 2020). These programs (implemented where we can find Black parents such as churches and mosques) could engage parents and older generation family members, bridging the gap between generational perceptions and enhancing understanding. A systematic review highlights that culturally sensitive training can play a significant role in lowering stigma related to mental health within Black communities (Codjoe et al., 2021). The review suggests that when mental health interventions are tailored to align with the cultural values and beliefs of Black individuals, particularly within faith-based settings, they become more effective in addressing mental health concerns and reducing stigma. A randomized study found similar results (Alvidrez et al., 2009).
Mental health professionals working with Black communities should be trained in culturally responsive care. By acknowledging and addressing the cultural nuances in how mental health is perceived, service providers can foster trust and more effectively address the mental health needs of Black youth (Cénat, Moshirian Farahi, Dalexis, et al., 2025). In addition, facilitating intergenerational dialogues within families can empower youth and parents to share perspectives and better understand each other’s experiences. Community and mental health organizations can host support groups or cultural events where families can discuss mental health openly to help reduce stigma and foster collective resilience. Religious and community organizations can play a vital role in engaging Black parents by providing mental health literacy programs, fostering open discussions, and mobilizing them toward care (Allen et al., 2010; McKenzie et al., 2015). Faith leaders, community and mental health advocates, with whom they already have a good rapport, can help destigmatize mental health, bridging generational gaps and fostering trust in culturally responsive mental health interventions (Allen et al., 2010; Bilkins et al., 2016; Fante-Coleman, Allen, et al., 2023).
Finally, further research exploring specific stressors experienced by Black youth and their mental health impact can deepen understanding. Longitudinal studies could examine how these perceptions evolve over time, especially in multicultural and newcomer environments where acculturation continues to shape identity as youth develop. In conclusion, this study underscores the need for mental health frameworks that respect and address cultural and generational contexts. Through increased awareness and culturally informed practices, mental health support for Black communities in Canada can become more inclusive and supportive for younger generations.
Limitations
Although its importance to understand intergenerational mental health perceptions in the Black communities in Canada, this study has several limitations. First, although the snowball sampling effectively facilitated participant recruitment, it may have introduced selection bias, limiting the diversity of perspectives within the sample. Second, while interviews were conducted online to increase accessibility, this approach may have excluded individuals without reliable internet access. Third, as a qualitative study, the findings provide in-depth insights but cannot establish causality or quantify the prevalence of the identified themes. Future research should address these limitations by employing mixed methods, expanding participant demographics, and exploring longitudinal changes in mental health perceptions across generations. Fourth, including perspectives from older generations, such as grandparents, could provide a more comprehensive understanding of intergenerational mental health dynamics within Black communities. Their unique experiences, shaped by different cultural and historical contexts, may offer deeper insights into the roots of stigma and evolving perceptions of mental health over time. Expanding the study to encompass these voices would likely strengthen the findings and provide a richer foundation for culturally sensitive and antiracist mental health interventions (Cénat, Haeny, et al., 2024). Finally, one limitation of this study is the lack of available literature on intergenerational differences in perceptions of mental health among other ethnocultural groups in Canada, including Arab, Asian, Black, Indigenous, and White communities. This gap restricted our ability to compare and discuss our findings more broadly and limited the depth of our discussion.
Conclusion
This study provides valuable insights into the generational dynamics influencing mental health perceptions within Black communities in Canada. Youth exhibited a greater willingness to acknowledge and discuss mental health struggles compared with older generations, who often prioritized resilience, privacy, and family reputation over emotional well-being. These differences are rooted in acculturation processes, cultural norms, and societal expectations, creating a disconnect that leaves many young people feeling unsupported and misunderstood. Despite these challenges, youth in this study expressed a strong motivation to challenge existing stigmas and foster a more open and accepting approach to mental health in future generations.
The findings emphasize the need for culturally sensitive and antiracist mental health frameworks that address these generational and cultural disparities. Programs aimed at fostering intergenerational dialogue could help families bridge understanding and reduce stigma, whereas mental health services must integrate culturally responsive and antiracist practices to build trust and provide effective support. Community-based initiatives, such as culturally tailored workshops or support groups, could further empower families to address mental health collaboratively. Findings underscore the need for culturally informed and antiracist interventions to bridge generational gaps and support mental health dialogue.
As Black youth increasingly adapt to Canadian cultural contexts while retaining aspects of their heritage, their openness to mental health presents an opportunity to transform perceptions within their communities. However, systemic barriers to equitable mental health care persist and must be addressed through concrete policy changes. Strengthening Black-led mental health initiatives and implementing culturally informed, antiracist interventions can help reduce disparities and improve mental health outcomes across generations.
Footnotes
Author Contributions
Availability of Data
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the grants #1920-HQ-000053 from the Public Health Agency of Canada (PHAC).