
Abstract
Youth mental health is a global health priority due to its increasing prevalence and adverse outcomes. Although the relationship between metacognitions and anxiety is well-documented in adults, further research is needed for the younger populations. This research examines two questions: (a) What is the correlation between cognitive self-consciousness and anxiety in children and adolescents? (b) Is this correlation moderated by cultural and socioeconomic differences? Based on 22 effect sizes from 8,459 participants in 11 countries, a meta-analysis was performed to find the overall effect size, heterogeneity, publication bias, and the moderating effect of Hofstede’s four cultural dimensions and United Nation Development Programme’s (UNDP) Human Development Index (HDI). Using the random-effects model, the results revealed that cognitive self-consciousness (r = .312, p < .0001, 95% confidence interval: [.257, .365]) showing moderate effect size in association with anxiety in children and adolescents. Meta-regressions indicated that power distance, masculinity, and HDI were important moderators. The findings show a significant correlation between cognitive self-consciousness and mental wellness in youth. The results have important implications for understanding the influence of cultural beliefs and national-level context on the associations between cognition and psychopathology. This article provides consistent evidence that there is a lack of mental health research resources in the Global South.
Keywords
There has been a widespread public health concern about the emotional well-being of children and adolescents since the early 21st century (De Looze et al., 2020). A deterioration in adolescent life satisfaction and an increase in depressive disorders have been observed in many high-income countries (Cosma et al., 2020). One in five children and adolescents experience anxiety worldwide, a rate that has doubled since the start of the COVID-19 pandemic (Racine et al., 2021). Anxiety is associated with adverse long-term outcomes including substance use disorders and poor educational and employment outcomes (Morales-Muñoz et al., 2023).
Adolescence is a developmental period with heightened attention to self-scrutiny and peer influence (Rankin et al., 2004). This emerging self-consciousness is embedded in a relatively complex social context that includes a rapidly changing digital landscape for identity-building, self-expression, and relationship establishment (Eleuteri et al., 2017). As an important construct under the concept of metacognition (thinking about thinking), self-consciousness has been widely studied to understand motives and social interactions (Fenigstein et al., 1975). While the associations between self-consciousness and anxiety in adults are well-documented, there is a lack of research examining self-consciousness in children and adolescents (Takishima-Lacasa et al., 2014). In addition, despite the abundance of evidence showing different predictors and symptoms of anxiety across countries (Delvecchio et al., 2015), the role of country-specific characteristics in shaping the impact of self-consciousness on mental well-being has yet to be examined. Therefore, the focus of this research is to understand the relationship between cognitive self-consciousness (CSC) and anxiety in youth with consideration of the cultural and socioeconomic differences across countries.
Literature Review
Cognitive Self-Consciousness in the Metacognitive Model
Metacognition refers to the psychological structures and processes that are involved in the understanding and control of thinking (Wells & Cartwright-Hatton, 2004). The metacognitive model of emotional disorders asserts that problematic metacognition leads to excessive self-focused attention, and it serves as a main contributor to psychopathology (Wells, 2002). This model is also known through the Self-Regulatory Executive Function (S-REF) model (Wells & Matthews, 1996). Based on the S-REF model, scholars later developed Metacognitive Therapy (MCT) to focus on modifying metacognitive beliefs (Wells, 2009). MCT is regarded as a highly effective therapy for a range of psychological challenges, including clinically diagnosable mental health disorders and subclinical issues of mental distress.
Metacognitions Questionnaire (MCQ) was developed by Cartwright-Hatton and Wells (1995) with a 65-item measure assessing five subscales, including positive beliefs about worry, negative beliefs about worry, beliefs about the need for control of thoughts, beliefs about cognitive confidence, and CSC. The MCQ was later shortened to 30 items (MCQ-30) maintaining the same factor structure (Wells & Cartwright-Hatton, 2004). Nowadays, different versions of the MCQ have been increasingly used in studies of younger populations (Myers et al., 2019). They include the MCQ-C: Metacognitions Questionnaire for Children; MCQ-CR: Revised Metacognitions Questionnaire for Children; MCQ-C30: Metacognitions Questionnaire for Children-30 Item Version; the MCQ-A: Metacognitions Questionnaire for Adolescents; and the MCQ-30. The MCQ-30 has been localized into different languages, such as Chinese (Zhang et al., 2023) and Dutch (Wolters et al., 2012). Among the five subscales, CSC is operationalized through the self-assessment’s items that measure the “degree to which an individual focuses on their own thinking processes” (Cartwright-Hatton & Wells, 1997, p. 294). CSC may strengthen the impact that the other four metacognitive beliefs have on individual’s mental state (Palmier-Claus et al., 2013). This meta-analysis thus examines CSC as a subscale of MCQ and includes different versions targeting children and adolescents.
Self-Consciousness and Anxiety
Adolescence is a transitional period with significant development in physical growth, cognitive capacity, and psychosocial readiness (Peleg-Popko, 2004). In the process of gradually separating from their families of origin and integrating into the outside social world, adolescents start to develop a sense of self, attending to inner thoughts and seeing themselves as a social object (Fenigstein et al., 1975). Self-consciousness shapes students’ self-efficacy, which eventually forms an identity for them to carry over to adulthood (Aquino & Reed, 2002). Some students develop a sense of imaginary audience, which is the perception that other people pay as much attention to their behaviors as adolescents do themselves (Takishima-Lacasa et al., 2014). Evidence shows that this self-monitoring ability is significantly related to mental issues among adolescents (Mor & Winquist, 2002). An experimental study found that students with heightened awareness of the need to control their thoughts are more sensitive to artificial stressors (Palmier-Claus et al., 2013). Without effective coping mechanisms, younger populations experience greater emotional fluctuations and are more sensitive to external influence (Yeo et al., 2023).
Anxiety disorders are a broad concept covering generalized anxiety disorder (GAD) (Spitzer et al., 2006), panic disorder (Roy-Byrne et al., 2006), social anxiety disorder (Stein & Stein, 2008), separation anxiety disorder (Masi et al., 2001), and a variety of other phobia-related disorders. Anxiety among adolescents has been specifically associated with concerns over body image (Kowalski et al., 2006), stress in taking tests (Peleg-Popko, 2004), as well as struggles in developing peer relations (Tillfors et al., 2012). Scholars indicated a scarcity of information on how adolescents understand their psychological development and react to anxious and threatening situations (Rodriguez-Tomé & Bariaud, 1990). In addition, there has been a lack of knowledge on applying the metacognitive model on children under 12 years of age (Ellis & Hudson, 2011). A meta-analysis (Costello et al., 2005) shows that the percentage meeting the criteria for anxiety disorder is higher among children (12.3%) than adolescents (11.0%). Therefore, this study aims to provide insights for both children (6–10) and adolescent (11–18) populations. Overall, it is hypothesized that:
Hypothesis 1 (H1): CSC is positively associated with anxiety among children and adolescents.
Cultural Values and Mental Health
Cultural structures such as beliefs, values, norms, and institutions enable the formation of social relationships, as well as the different meanings that children and adolescents ascribe to their roles and experiences (Bronfenbrenner & Ceci, 1994). Research in the field of psychology and education has long advocated a cross-cultural approach to understanding individual development as “embedded” in their familial and cultural context (Szapocznik & Kurtines, 1993). Hofstede (1980) conceptualized culture as “the collective programming of the mind which distinguishes the members of one group from another” (p. 21). Hofstede’s (1980) study of cultural values among IBM global employees eventually led to a cross-national database with information on six dimensions of national culture—individualism versus collectivism, power distance, masculinity versus femininity, uncertainty avoidance, long-term orientation versus short-term orientation, and indulgence and restraint. Due to the lack of data on the fifth and sixth dimensions for most of the countries, this study only includes the first four key dimensions as the cultural variables.
Individualism and Collectivism
Hofstede (1984) defined individualism as a societal tendency to look after only oneself and one’s immediate family. He defined collectivism as a preference to be integrated into groups and let the group interests prevail. Overall, individuals from collectivist cultures score lower on hedonic well-being compared with people from individualist cultures (Chue & Yeo, 2023). Studies on test anxiety found that this problem is more prominent among Asian children and adolescents compared with their non-Asian counterparts mainly due to their achievement motivation that goes beyond individual achievement and includes a contribution to group harmony and collective success (Wang & Ollendick, 2001). Under the influence of group expectations and family involvement, it is more likely for children and adolescents from collectivist cultures to engage in self-monitoring (Gudykunst et al., 1987). Therefore, it is hypothesized that:
Hypothesis 2 (H2): For societies that emphasize collectivism, CSC has a stronger positive correlation with anxiety.
Power Distance
Power distance refers to the degree to which societies expect power to be unevenly distributed and accept inequalities (Hofstede, 2001). For countries with a greater power distance, their members tend to accept the differentiation of rights and group themselves into classes on various criteria (Gallego-Álvarez & Pucheta-Martínez, 2021). Prior studies revealed that power distance is negatively associated with well-being (Daniels & Greguras, 2014). The shared acceptance of inequality might lead to policies and behaviors that increase the lived experience of inequality (Hofstede, 1980). Indeed, members of high power distance cultures tend to experience higher status anxiety (Rösler, 2023) and more cyberbullying (Boronenko et al., 2013). The different perceptions of social inequality correspond with the key philosophical viewpoints of Eastern and Western school systems. Most pedagogical approaches in the West promote the significance of intrinsic motivation and critical thinking (Deci & Ryan, 1985). In contrast, many East Asian countries consider education as a path to elite academic placement and this pragmatic approach is a significant source of stress for children and adolescents (Cortina et al., 2017). Therefore, it is hypothesized that:
Hypothesis 3 (H3): For societies that emphasize power and authority, CSC has a stronger positive correlation with anxiety.
Masculinity and Femininity
The conception of masculinity and femininity is based on the assumptions that certain attributes are more salient in one gender over the other and individuals should think and behave appropriately to their gender group (Best & Williams, 1994). According to the masculinity-femininity index scores, the most feminine societies (e.g., Sweden) receive lower scores closer to zero and the most masculine societies (e.g., Japan) receive higher scores closer to 100 (Hofstede, 2010). In feminine countries, individuals are guided by the values of achieving solidarity, gender balance, and quality of life (Irfan, 2016). Masculine countries, on the contrary, are often characterized by clearly defined gender roles, dominance, and desire for material success (Hofstede, 2011). In the process of developing self-consciousness, children and adolescents are under the profound influence of the feminine and masculine psychology of the broader societies through, for example, gender portrayal on TV commercials (Moon & Chan, 2002). Since the association between masculinity and stress has been well-established among adults (Taylor, 2014), children and adolescents will likely display similar patterns. It is hypothesized that:
Hypothesis 4 (H4): For masculine societies, CSC has a stronger positive correlation with anxiety.
Uncertainty Avoidance
Uncertainty avoidance is “the extent to which the members of a culture feel threatened by uncertain situations” (Hofstede, 2001, p. 161). High uncertainty-avoidance cultures rely on structures in relationships, organizations, and societies to find stableness and their members place less value on emotional expression, diversity, and innovation (Hofstede, 2001). A cross-cultural study shows that a lack of tolerance for ambiguity results in higher levels of anxiety (Gudykunst et al., 1987). College students in Russia and Italy (high uncertainty avoidance) have lower stress levels compared with those in China and the United States (lower uncertainty avoidance; Delvecchio et al., 2023). The development of adolescents in high uncertainty-avoidance cultures is led more by social norms rather than their subjective sense of efficacy (Oettingen & Zosuls, 2006). The lack of cognitive flexibility in dealing with uncertainty results in potential challenges in adaptation and psychological independence (Zheng, 2024). Therefore, it is hypothesized that:
Hypothesis 5 (H5): For societies with high uncertainty avoidance, CSC has a stronger positive correlation with anxiety.
Socioeconomic Context and Mental Health
Anxiety prevalence is positively associated with a country’s developmental status, indicated by GDP per capita (Javaid et al., 2023). Academic pressure and emotional isolation are two salient mechanisms that couple societal wealth with adolescent mental distress (Luthar & Becker, 2002). Adolescents report higher depression rates in wealthy nations as they are situated in a more competitive growth environment with higher parental emphasis on extrinsic goals (e.g., wealth and reputation) as well as stronger personal strivings for perfection (Luthar & Becker, 2002). Affluent youth also develop intense emotional isolation from professional parents under their limited after-school supervision and eroded family time (Luthar & Becker, 2002). Meanwhile, self-consciousness accounts for a portion of the variance in youth anxiety disorders (Muris et al., 2018) and self-conscious emotion has been found to be the highest for Western countries such as the United States (Chung & Robins, 2015). It is likely that the advanced socioeconomic status partially shapes the psychological processing of thoughts in youth thus affects their perception of pressure.
At the country level, while studies have assessed different socioeconomic dimensions using different indicators separately, for example, GDP per capita for economic development (Maeda & Ziegfeld, 2015) and density of health workers and hospitals per population for accessibility of health services (Peters et al., 2008), current literature lacks an approach to quantify both economic and non-economic factors. The human development index (HDI) was created by the United Nations to measure human development and is a frequently cited alternative to GDP (Altman, 2012). It combines three elements of socioeconomic well-being: the ability to live a long and healthy life, knowledge access, and a sufficient standard of living (Altman, 2012). Given its broad range of socioeconomic components, HDI is used as a moderator of CSC and anxiety. It is hypothesized that:
Hypothesis 6 (H6): CSC has a stronger positive correlation with anxiety in societies with higher HDI.
Method
Inclusion Criteria
To be included in the meta-analysis, studies had to meet several criteria: (a) published as peer-reviewed journal articles, conference proceedings, or graduate theses; (b) published in English; (c) included samples with the age range of 6 to 18; (d) included non-clinical populations; (e) operationalized self-consciousness with the Metacognitions Questionnaires (CSC) and used one of MCQ derivates as a measurement tool; (f) reported the correlations between MCQ (specifically CSC) and anxiety instruments. Studies that identified college students as adolescents were excluded. Studies published before December 10, 2023, were included.
Search Strategy
First, Köcher et al.’s (2021) systematic review and meta-analysis on the assessment of metacognitions in children and adolescents was reviewed. It was utilized as the main source of reference for its usage of similar assessment tools and populations. The original meta-analysis included studies published before February 6, 2020, in the following databases: PsycINFO, PubMed, PSYNDEX, and ERIC (Köcher et al., 2021). In addition, the authors searched the reference lists of included studies and gray literature including doctoral dissertations (Köcher et al., 2021). The authors used the string “(children OR adolescents*) AND (meta cognition* OR metacognition* OR meta-cognitive belief* OR meta cognitive belief*) AND (anxiety OR worry OR phobia)” to identify studies that included participants age 18 or younger with or without anxiety disorders; assessed positive metacognitive beliefs about worry, negative metacognitive beliefs about worry, or meta-worry as an outcome variable; and were published in English or German (Köcher et al., 2021). The original study identified 24 qualified articles. From Köcher et al.’s (2021) study, only studies that reported correlations between CSC and anxiety (n = 11) were extracted. Two coders conducted the initial selection of studies based on the article references, and a third coder reviewed the completed list to ensure consistency.
Next, an additional literature search was performed to identify studies published between 2020 and 2023, in the databases of APA PsycNet, a comprehensive search platform for behavioral and social sciences. Keywords used were metacognitions questionnaire, anxiety, and children or adolescents. The search on APA PsycNet returned 23 results after removing duplicates and four of them were included in Köcher et al. (2021). The studies with only clinical samples (n = 5), different age groups (n = 1), scale development for different languages (n = 4), or without CSC and anxiety correlations in the reporting (n = 9) were eliminated. In addition, Google Scholar was used as a supplemental tool to identify studies published between the invention of the MCQ assessment tool in 1997 and 2023, as it offers higher precision, larger quantity of available studies, more gray literatures and greater access to free full-text publications than PubMed (Shariff et al., 2013). One coder screened the titles, abstracts, and methods to identify relevant studies from the first 50 pages of Google Scholar. Additional 26 full-text studies were identified in this process. The studies without reporting the correlations between CSC and anxiety (n = 10), with duplicates in Köcher et al., (2021) (n = 11), in non-English language (n = 2), or with samples of college students (n = 2) were removed. One doctoral dissertation from the United States was excluded as all the coders agreed that the study used significantly different version of the MCQ scale. In total, there were 13 qualified studies from this search. Three coders collaborated in the data coding processes to ensure accuracy and validity. One coder retrieved the studies from the databases and the other two coders verified the measurements, data collection, and reporting accuracy independently. For dissertations and master’s theses, the coders considered the credentials of the educational institutions as well as the quality of research. Three coders reached 92% agreement of the evaluations and consensus was achieved for the cases with discrepancies (n = 2). Finally, one coder further compared the research methods of the shortlisted 24 studies to identify sample overrepresentation issues and authorship bias. Two additional studies from Denmark with subsamples from the others were removed.
Data Extraction
A Google spreadsheet was created with the following columns: study author and year, sample size, age range, mean age, percentage female, country, Hofstede’s four dimensions, HDI, MCQ instrument, anxiety instrument, study type, post-Covid-19 influence, culture, and correlation between CSC and anxiety. If a study reported correlations separately for male and female samples, the coefficients were combined into a single correlation to better follow the heterogeneous assumptions of meta-analysis. When a study included both clinical sample and community sample, only the community sample data were used for coding. If two studies used identical subsample data or if the data were likely from the same project, only the study with a larger sample size was included. For each country, Hofstede et al.’s (2010) work was referenced to determine the scores for Hofstede’s dimensions and the United Nations Human Development Insights data center (UNDP, 2022) was used to retrieved HDI data. It worth noting that HDI metrics was initially developed in 1990, and it integrated several major updates in 2010, including changes to indicators, the aggregation method, and minimum and maximum values (UNDP, 2011). Acknowledging the changing metrics and national status, this study tailored the HDI data based on the publication year from 2004 to 2022 (two 2023 articles were based on the 2022 data).
Study Characteristics
The final analysis included 22 independent samples. The combined sample size was N = 8,459 with participants from 11 countries between 2004 and 2023. Three studies (n = 3) were gray literatures, with 2 master’s theses from the United States and 1 doctoral dissertation from Germany. Eight studies (n = 8) sampled both children and adolescents and 14 studies (n = 14) only included adolescents above 12 years old. Three studies (n = 3) included data collected after the outbreak of Covid-19. Two studies (n = 2) included community samples and clinical-based samples separately in their reporting and only community samples were selected. One study (n = 1) reported effect sizes for female and male subgroups separately and the combined score was used for analysis. Overall, one country from North America (n = 1), one from Oceania (n = 1), three from Asia (n = 3), and six from Europe (n = 6) were included in the data. Median sample size was n = 180 per study. Female percentage was in the range of 31% to 71%. Table 1 shows the characteristics of the included studies.
Cognitive Self-Consciousness and Anxiety Studies’ Participant Profile, Arranged by Year of Publication.
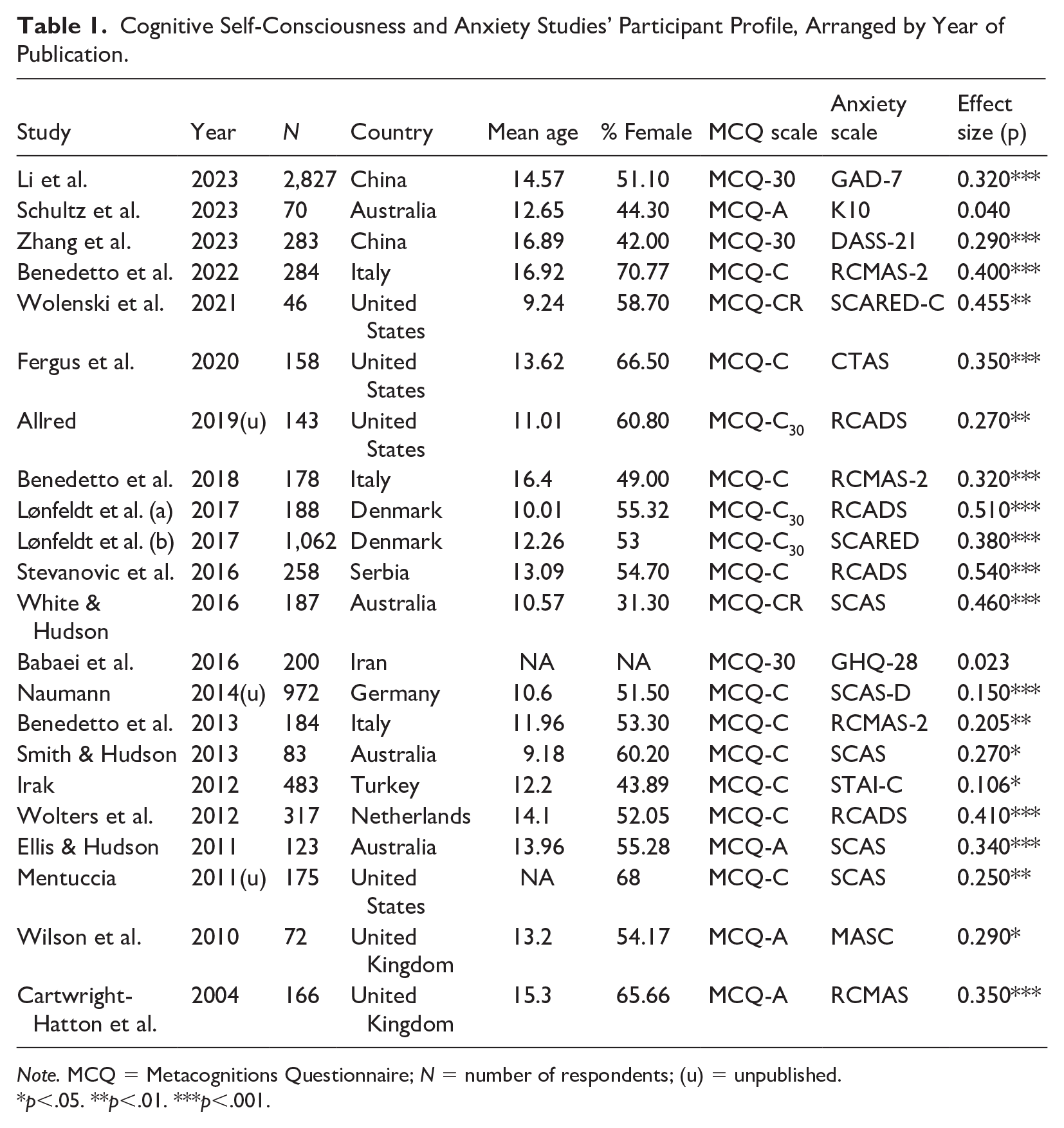
Note. MCQ = Metacognitions Questionnaire; N = number of respondents; (u) = unpublished.
p<.05. **p<.01. ***p<.001.
Meta-Analysis
Using Comprehensive Meta-Analysis Version 4.0 (CMA; Borenstein et al., 2022), the standard error and variance for each correlation coefficient was calculated. It used Fisher’s Zr-transformation to weigh the correlation coefficients based on the reciprocal error variance (Lipsey & Wilson, 2001). A random-effects meta-analysis model was used to compute a mean effect size and confidence interval, which were visually depicted with a forest plot. The random-effects meta-analysis model enables investigation of the heterogeneity of the effect sizes across studies, beyond the effect of sampling errors, one of the assumptions of the fixed-effects model (Borenstein et al., 2022; Lipsey & Wilson, 2001).
To test the heterogeneity of the effect sizes, Q and I2 were calculated (Higgins & Thompson, 2002). A Q statistic with a significant probability value (p < .05) and an I2 greater than 50% indicate a significant individual effect size variability. An exploratory subgroup analysis was conducted to examine if the impact varies from one context to another and sensitivity analysis was used to assess the robustness of results. Publication bias was assessed by using Duval and Tweedie’s Trim and Fill method, Egger’s Regression Intercept, and the classic fail-safe N. With Duval and Tweedie’s Trim and Fill method, if the effect sizes included in the meta-analysis fall symmetrically around the mean effect in the funnel plot, and if the trimmed and re-imputed studies do not significantly shift the main effect, then publication bias is low. Egger’s test creates a regression equation using the standardized effect sizes and precisions; if there is no publication bias, the regression intercept is zero (Lin & Chu, 2018). The classic fail-safe N test calculates the number of missing studies that should be added to make the combined effect size statistically nonsignificant (Orwin, 1983). Finally, a meta-regression analysis was conducted using the five moderator variables of individuality, power distance, masculinity, uncertainty and HDI. The overall model was evaluated first through R2 and Q, then considered the coefficient, standard error, confidence interval, Z-value, and 2-sided p-value for each moderator.
Results
Meta-Analysis
Using the random-effects model based on 22 effect sizes, the mean effect size (correlation) is 0.312 with a 95% confidence interval of [0.257, 0.365] (see Figure 1). This is classified as a medium effect size (Lipsey & Wilson, 2001). The Z-value is 10.478 with p < .001, meaning that the null hypothesis is rejected. Thus, it is suggested that in the universe of populations comparable to those in the analysis, the mean effect size is not zero.
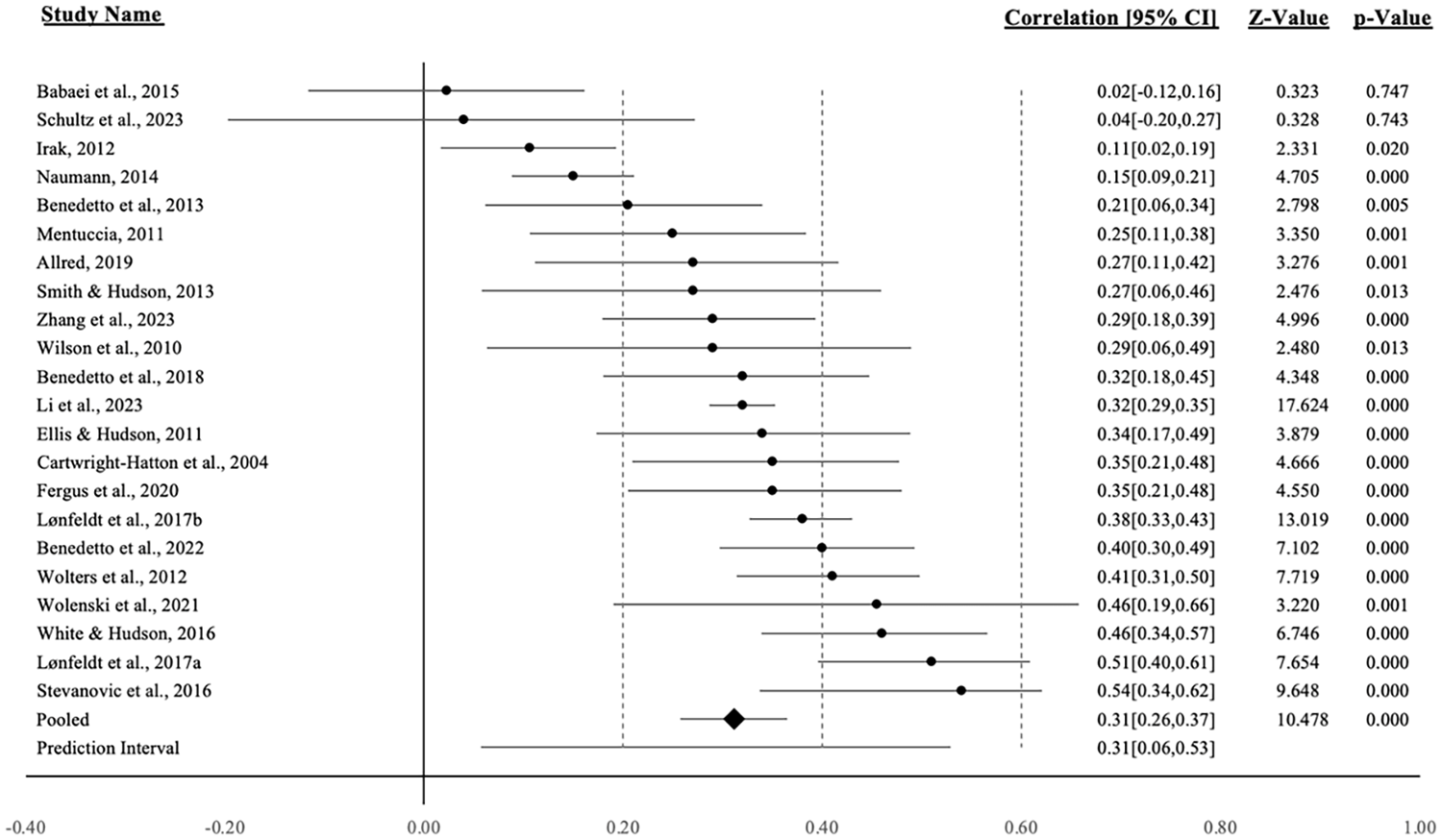
Forest Plot With Mean Effect Size
The Q-value is 129.340 with 21 degrees of freedom and p < .001. Therefore, the null hypothesis that the true effect size is the same in all these studies can be rejected. The I2 statistic is 83.76%, which tells us that about 84% of the variance in observed effects reflects variance in true effects rather than sampling error. The variance of true effect sizes (τ2) is 0.015 and the standard deviation of true effect sizes (τ) is 0.124 in Fisher’s Z units. The true effect size in 95% of all comparable populations falls within the prediction interval of 0.057 to 0.529, assuming that true effects are normally distributed in Fisher’s Z units. Therefore, hypothesis 1 on the positive correlation between CSC and anxiety in children and adolescents was supported. Table 2 displays the mean effect size and heterogeneity statistics under the random-effects model.
Mean Effect Size and Test for Heterogeneity Under the Random-Effects Model.
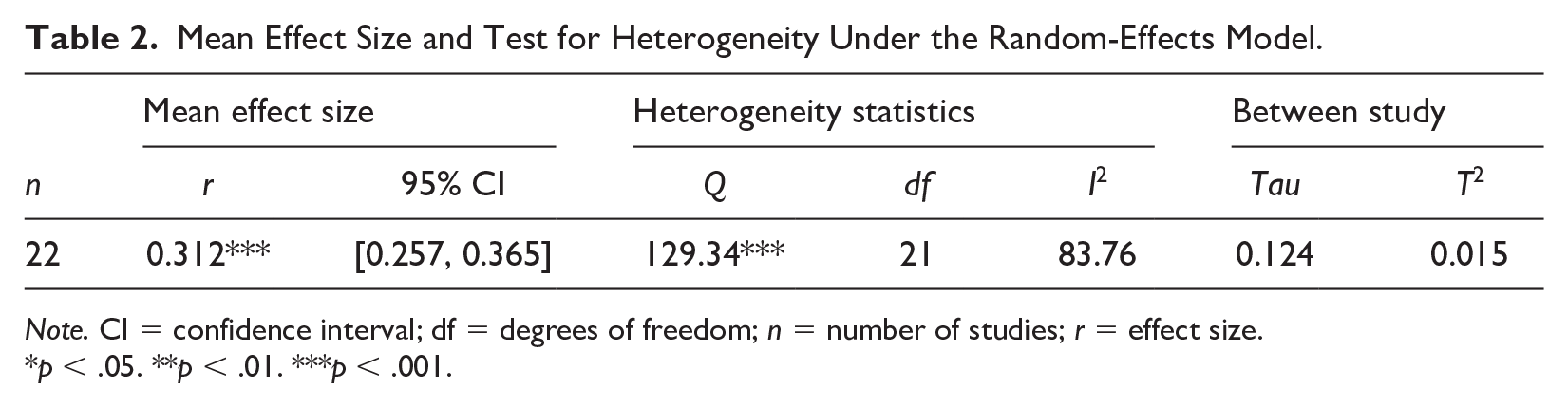
Note. CI = confidence interval; df = degrees of freedom; n = number of studies; r = effect size.
p < .05. **p < .01. ***p < .001.
Subgroup Analyses
Exploratory subgroup analyses by study type, culture, and Covid-19 influence were conducted to identify the potential contributing factors underlying variability. The subgroup analysis by study type indicated that the pooled effect sizes between published work (0.317) and unpublished work (0.259) differ from each other. Studies from Eastern countries (including West Asia, East Asia, and Central Asia) revealed a lower pooled effect size (0.194) compared with those from Western countries (0.342). Studies with data collected after Covid-19 reported a slightly lower pooled effect size (0.300) than studies with data collected before 2020 (0.316).
Sensitivity and Publication Bias
The sensitivity analyses were performed by removing one study at a time to assess the robustness of the results. The pooled estimates were not significantly shifted by excluding any single study, suggesting that the results were statistically robust. For publication bias, the point estimate and 95% confidence interval for the studies under a random-effects model was 0.306 (0.287, 0.325). Using Trim and Fill, the imputed point estimate was 0.293 (0.273, 0.312), meaning that the effect was slightly lower when adding the three trimmed studies. In general, the studies were symmetrically distributed around the mean (see Figure 2). Using Egger’s regression, the p-value for the intercept was not significant, suggesting low publication bias (β0 = 0.203, p =.847, t = 0.194, df = 20.000). The classic fail-safe N test revealed that 3,556 additional studies with nonsignificant results would be needed to make the p-value insignificant.
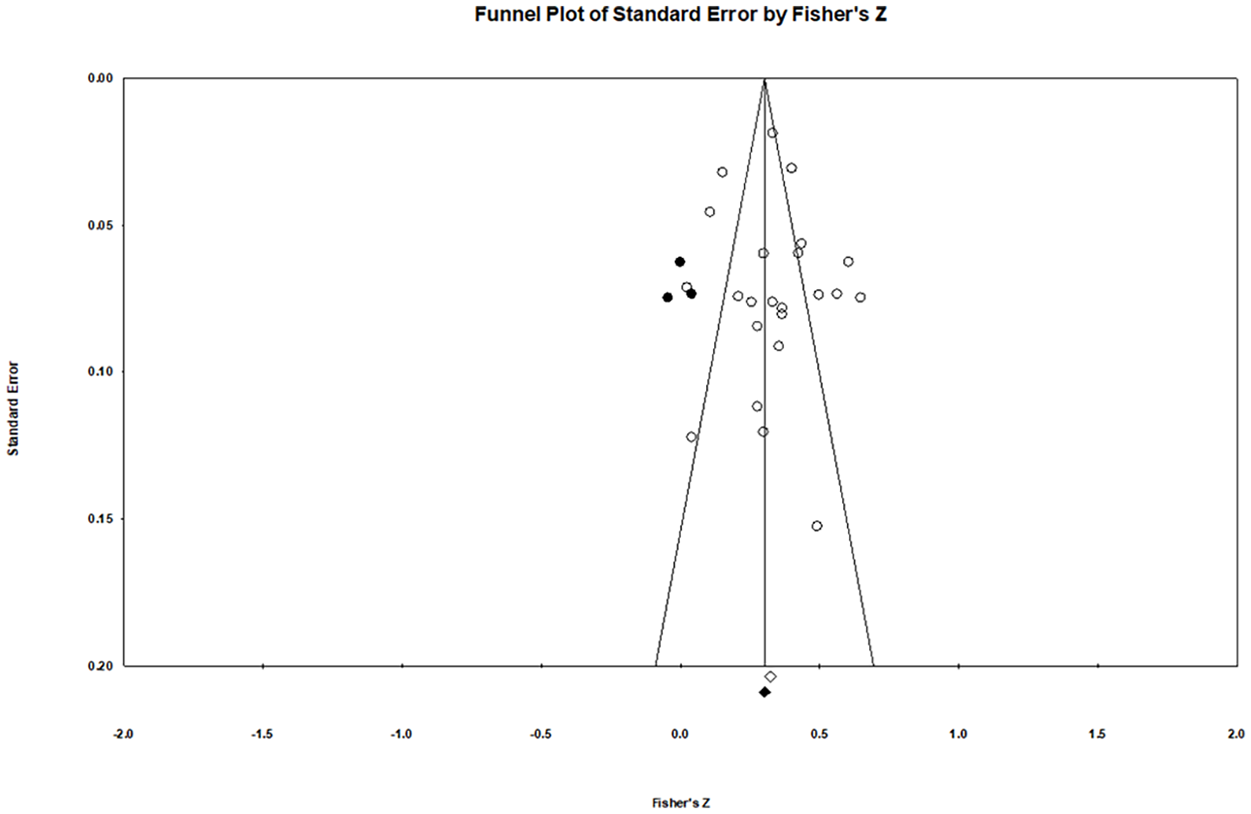
Funnel Plot for Publication Bias
Meta-Regression
The meta-regression model had an R2 of 0.33 and a Q-value of 14.19 with 5 degrees of freedom and p = .015, meaning that we can reject the null hypothesis and conclude that the mean effect size is related to one or more of the covariates. Table 3 displays the results of the meta-regression with five covariates, showing that CSC has a stronger correlation with anxiety for countries that emphasize the differences in power and authority more (coefficient = 0.014, p = .003), are less masculine (coefficient = −0.005, p = .007), and are more developed in national socioeconomic achievements (coefficient = 2.951, p = .010).
Meta-Regression Results.

Note. CI = confidence interval; HDI = Human Development Index; SE = standard error. For the test of the model, Q = 14.19, degrees of freedom = 5, and p < .05.
Therefore, Hypothesis 3 on the positively moderating effect of power distance, and Hypothesis 6 on the positive moderating effect of HDI were supported. Contrary to hypothesis 4, the data indicated a negative moderating effect of masculinity on the correlation between CSC and anxiety. The moderating effects of individuality and uncertainty avoidance were not significant. Figures 3 to 5 show the regression plots of Fisher’s Z on power distance, masculinity, and HDI, respectively.
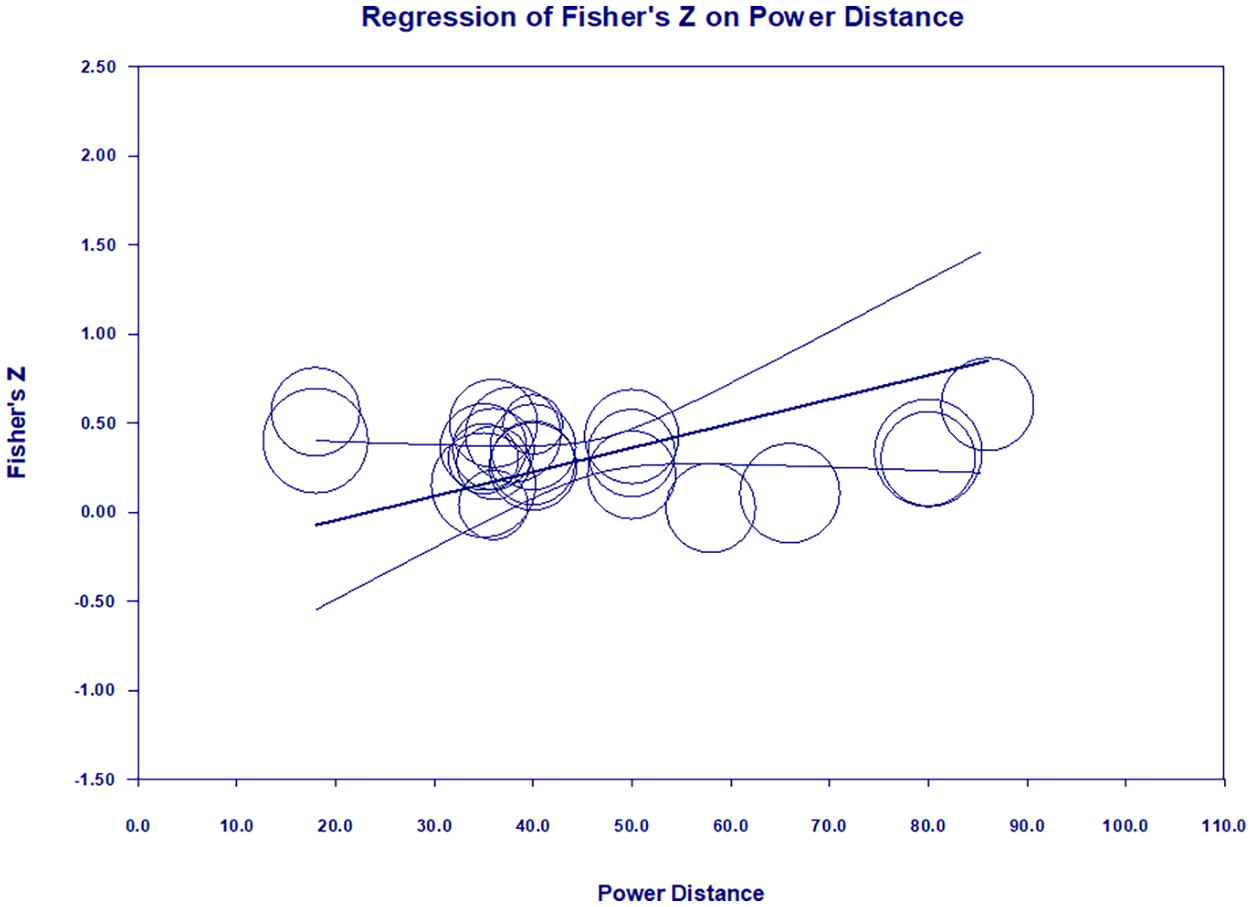
Regression Plot on Power Distance
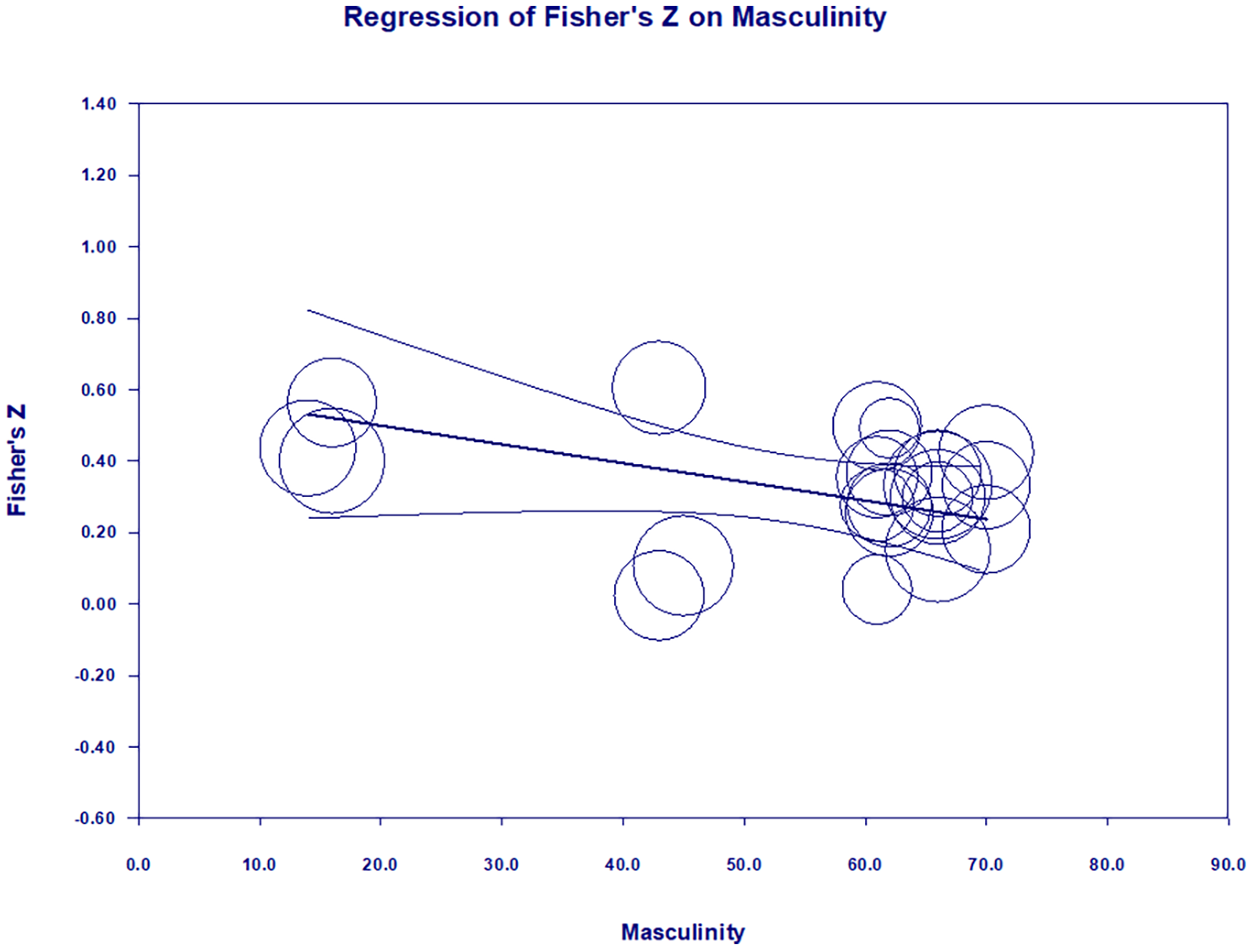
Regression Plot on Masculinity
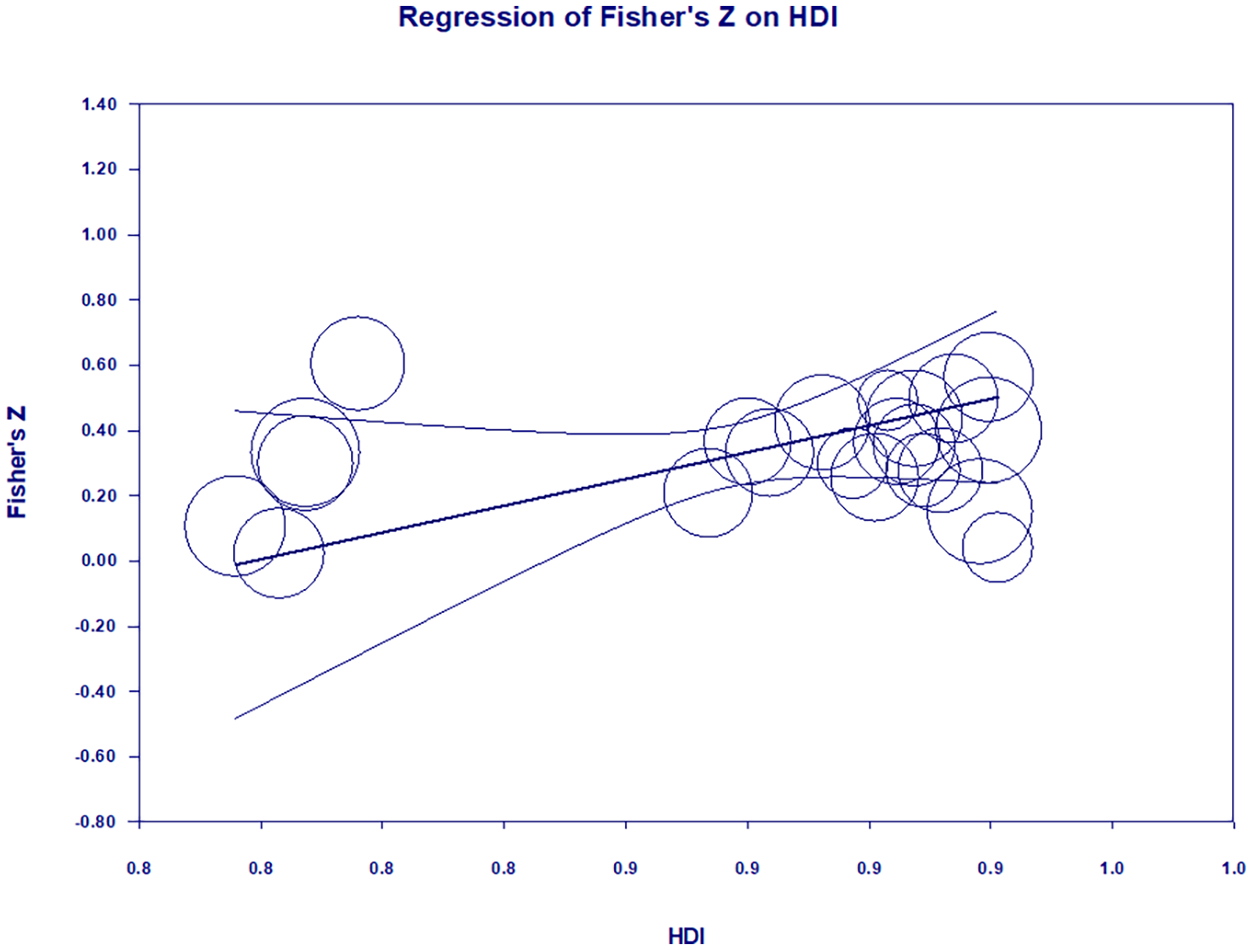
Regression Plot on Human Development Index (HDI)
Discussion
In response to the first research question, the correlation between CSC and anxiety in children and adolescents revealed a medium and significant effect size of 0.312 (Lipsey & Wilson, 2001). While previous studies argued that self-consciousness helps people understand their strengths (Yeo et al., 2023), this research provides evidence that self-focused attention may underscore one’s problems and undermine their mental health functioning. This positive relationship between CSC and anxiety builds upon existing studies that show a relationship between other metacognitions (positive and negative beliefs about worry) and anxiety in youth (Köcher et al., 2021). The results complement the research in the adult population which has found that metacognitions, including CSC, are associated positively, moderately, and significantly with anxiety (Capobianco et al., 2020).
In response to the second research question, the relationship between self-consciousness and anxiety was significantly moderated by two of Hofstede’s cultural dimensions: power distance and masculinity. The finding suggests that children and adolescents with a heightened focus on self-referential thoughts may have more intense feelings of tension in a social environment emphasizing acceptance of status inequalities and power difference. In the educational context, parental expectations, family relationships, socialization processes, and school systems in high power distance cultures might put excessive pressure on students for academic excellence and cause anxiety among school-age children and adolescents (Mertens & d’Haenens, 2014). It is speculated that the competitive learning environment and teacher-dominated classroom interactions may pose adverse impacts on students’ tendency to direct attention inward, resulting in low self-esteem and self-awareness.
The finding also indicates that younger populations might experience higher levels of anxiety when growing up in cultures stressing caring and nurturing behaviors. It means that a feminine and relationship-oriented society might provide a conducive environment for its members to engage in self-monitoring. Prior studies have found that adolescent females tend to report a stronger association between their self-monitoring ability and depression (Mor & Winquist, 2002). By differentiating the individual sense of culture on gender roles, this study shows that both adolescent girls and boys might develop higher levels of anxiety if they are in a context with less value judgment on gender. The result supports a prior finding among Turkish students that the idea of gender equality positively predicts the stress levels arising from gender roles (Kurtuluş & Bulut Ateş, 2021). It implies that a lack of societal appreciation on competitiveness may encourage self-scrutiny behaviors among teenagers. In educational context, the weakening effect of masculinity on the association between CSC and anxiety suggests that the recognition of gender differences in perceptual or cognitive abilities may help reduce students’ thought salience and the likelihood of negative thought appraisals (Marker et al., 2006).
The meta-regression results showed that increased human development, as indicated by life expectancy, education, and income, results in an increased effect size. In countries with higher socioeconomic achievements, children and adolescents’ thought-focused attention might evolve into stronger negative emotions. Although economic instability was argued to be associated with worse mental health in children and adolescents (Hudson, 2005), a larger scale survey of 150,000 adults in 26 countries revealed that anxiety is significantly more prevalent and problematic in high-income countries than in low- or middle-income countries (Ruscio et al., 2017). The most developed countries have the highest demands for investment in mental health care (Touburg & Veenhoven, 2015). Thus, self-referential thoughts about one’s cognitive processes may cause higher levels of anxiety in countries where the HDI is higher, there is more institutionalized education, and students have more access to mental health care.
Finally, this research sheds light on the treatment of anxiety in youth. Equipping children and adolescents with skills to prevent them from controlling their own thoughts may help to better adapt them to different situations and desensitize them to social stress (Palmier-Claus et al., 2013). MCT targets abnormal and psychologically distressing beliefs about thinking that can cause maladaptation and negative outcomes (Wells, 2002). It helps to reduce persistent negative self-referential processes such as worry and rumination, allowing patients to become more cognitively flexible in addressing underlying thoughts (Wells, 2002). In children, existing research shows the efficacy of MCT for GAD, even in those who have received previous types of therapy or counseling (Esbjørn et al., 2018). Awareness-based interventions such as dialectical behavior therapy, attention training, acceptance and commitment therapy, and integrative body-mind training (Dahl et al., 2020) could be utilized by education practitioners to improve children and adolescents’ psychological capacity surrounding the self. Parents are also advised to be aware of the parent-child dynamics that might shape children’s control of thoughts and understand the perspectives of their children to help them develop stress coping mechanisms.
Implications for Equity, Diversity, Justice, and Inclusion
Youth mental health is a global priority identified by The World Health Organization. Although it is a universal concern, its presentation and management vary based on cultural and socioeconomic factors. Some of the 8,459 participants in this analysis likely experienced potentially disadvantaged access to educational resources. Youth well-being is a possible source of inequality differences between Global South and Global North (Heshmati et al., 2008). This study points out a shortage of research of youth mental wellness in less developed countries. Research-generated knowledge is a critical resource in understanding the health needs in a region and forming effective intervention strategies (Thornicroft et al., 2012). A study in 2010 found that the number of publications was much lower in the continents of Africa and Asia in indexed-psychiatric journals (Razzouk et al., 2010). Among these less developed countries, there was also a problem of resource distribution inequity with Brazil, China, and India accounting for more than 40% of mental health publications (Razzouk et al., 2010). As shown in this study, the scarcity of available data in underdeveloped countries and the inadequacy of representation of diverse ethnical groups suggest the need for global inclusive research planning.
Limitations and Future Research
One limitation of this study is the use of different instruments for measuring CSC and anxiety. Different versions of MCQ were included in the meta-analysis with slightly different wording. However, each version operationalized CSC similarly, thus increasing confidence in effect size. The five derivates (MCQ-C, MCQ-A, MCQ-C30, MCQ-30, and MCQ-CR) included in this study align with the MCQ questionnaires used in another systematic review (Köcher et al., 2021). Likewise, the included studies utilized several different measurements of anxiety (e.g., SCAS, SCARED, and RCADS). To analyze anxiety from a broad perspective, the use of different scales allowed the inclusion of many studies from different countries. However, this exploration also points out a need for theoretical refinements and improvements to anxiety assessment. Future meta-analysis can explore the reliabilities of anxiety scales to facilitate research decision-making on selecting the appropriate scales for the target populations.
Another limitation on measurement is the use of HDI scores based on the publication year of the included studies. HDI measurement is frequently criticized due to measurement error within the three components, frequent computational changes in the index, implied trade-offs across the components, and correlation of the components (Ghislandi et al., 2019). The absence of a data collection timeframe in some of the studies limits the accuracy of the measurements. Despite these limitations, the HDI is cited profusely in policy and academics as well as popular media worldwide (Klugman et al., 2011).
Although the included 22 samples represent diverse geographical locations, nine out of the 11 countries included in the sample are developed countries, and only two are developing countries. More collaborative research on children and adolescents is needed in regions with less educational investment such as Latin America, Sub-Saharan Africa, and South Asia (Razzouk et al., 2010). Scholars could further explore the behavioral differences in anxiety reporting among high-, middle-, and low-income countries. It is likely that people in less developed countries tend to unconsciously underreport because of a lack of mental health knowledge or consciously understate their mental concerns due to societal stigma about mental disorders (Saxena et al., 2007). Longitudinal studies should investigate the stability of metacognitions over time as well as the longitudinal impact of metacognitions on adulthood mental health outcomes. Insights from a developmental perspective will help practitioners better determine how to adjust the adult metacognitive model of GAD for children, considering their cognitive capacity and experience (Köcher et al., 2021). The question of whether parental behaviors are mediating the impact of cultural values on children’s mental functioning is also ripe for future research.
Further research should explore the assumed intersection between youth culture and its associated national culture. This generation of youth, described as the “Net-generation” (Mesch, 2009), grew up in a media-rich environment with access to computers, social media, online games, virtual reality, and AI technologies from early childhood. The multiplicity of technology use among children and adolescents helps create different senses of self (Riley, 2008). With the globalization of culture and the increasing mobility between countries, the youth community worldwide is now more receptive to foreign cultural practices (e.g., language, lifestyle) and thus more likely to blur the boundaries of traditional national cultures in their thinking and behaviors (Heaven & Tubridy, 2003). A step forward in unpacking the nuance of cultural context is to analyze the convergence and divergence of youth subculture and national culture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.