
Abstract
Under the United Nations High Commissioner for Refugees’ (UNHCR) seven-decade mandate, Afghan refugees have faced some of the largest and most protracted experiences with forced displacement. This intergenerational exposure to forced migration has had innumerable consequences for the mental health of this population across different stages of their displacement. Afghan refugees who have resettled into Western nations face a unique set of challenges as they must navigate resettlement into societies that are linguistically, culturally, and spiritually distinct from their own backgrounds. This systematic review explores the (a) effectiveness and (b) cultural adaptation of interventions that have addressed the mental health of Afghan refugees resettled into Western countries since the year 2000. This systematic review will employ the Cultural Treatment Adaptation Framework (CTAF) to organize the extent of cultural adaptations. Through the systematic search of four databases, 1709 studies emerged from our search terms, seven of which met the criteria for this review, for example, study includes more than 2/3 Afghan participants; study includes outcome variables. Studies included programs in Germany, Serbia, Sweden, and Austria. The most common outcomes that interventions addressed included posttraumatic stress disorder (PTSD) (n = 5), depression (n = 3), and quality of life (n = 3). Program modalities ranged between Cognitive Behavioral Therapy (n = 4), emotion regulation (n = 1), family therapy (n = 1), and multimodal interventions (n = 2). Most studies only incorporated peripheral changes to interventions in the service of cultural adaptation, and only one intervention included core changes. This program reported the highest effect sizes in reducing PTSD and depressive symptoms when compared with the rest of the studies. These findings provide a direction for future studies as they consider whether the extent of cultural adaptations can influence the effectiveness of programs for Afghan refugee populations. We provide recommendations for mental health practice with this population, including a special attention to the role of daily stressors, the significance of faith and culture-based meaning making in the service of coping, and the salience of isolation.
Keywords
Following the U.S. military withdrawal from Afghanistan in August 2021, the U.S. Department of State (2023a) reported that about 90,000 Afghans were evacuated from the country and brought to the United States. Because there was very little time before knowing they had to leave, many people were unable to sell any property or access money from the bank. Additional predisplacement stressors included the chaos related to the speed at which the Taliban regained control and the resurgence of gender-based violence and discrimination (Covington, 2023). Most Afghans resettling in the United States currently fall under the humanitarian parole category. However, parolees do not qualify for lawful permanent residence unless they qualify for another resettlement designation, such as a Special Immigrant Visa (SIV) or refugee status (Greenberg et al., 2021). Many of the Afghans who fled worked with the American military, nongovernmental organizations, journalists, and their family members (Covington, 2023), but not all qualified for an SIV. Nearly 2 years later, thousands of more refugees are still waiting to be processed to enter the United States (Faiez & Santana, 2023), and some who were able to enter now worry about whether their visa will expire. Furthermore, humanitarian parolees are only made temporarily eligible for federal benefits and services following legislation passed in late September of 2021 (Butler & Sheriff, 2021).
Throughout the past four decades, key psychosocial challenges such as complex trauma, financial instability, and acculturative stress have persisted throughout generations of Afghan refugees in the Western countries. This has significantly impacted this population’s mental health. Scholarship on refugee well-being has consistently advocated for the use of psychosocial support (PSS) services that are attuned to the unique cultural and faith-related backgrounds of this population (Ocampo et al., 2021), specifically in the service of facilitating healing and growth (Fazel et al., 2012). Refugee communities find immense strength and wisdom embedded within their cultural and faith-based traditions to embody resilience (El-Khani et al., 2017; Magan & Elkhaoudi, 2023; Muruthi et al., 2020). However, the rampant fixation on the negative consequences of their forced displacement in academic circles can distract from the sophisticated processes through which they manage to cope with their unimaginable experiences. Resilience, capturing individuals’ dynamic capacities to avoid psychological harm or experience growth in the face of adversities (Luthar et al., 2000), can be strongly influenced by sociocultural worldviews (Ungar, 2012). Despite the salience of faith and cultural values for healing, however, past research has mostly only focused on exploring rates and trends of psychopathology among Afghans resettled in different Western countries. To our knowledge, research studies have yet to systematically explore whether and how evidence-based interventions (EBIs) have been adapted to benefit from cultural elements when working toward healing mental health challenges and promoting resilience. There are low numbers of Afghan refugees who seek mental health care due to limited self-recognition of mental health symptomatology and concerns about cultural mismatch with services (Slewa-Younan et al., 2017). As such, there is a timely need for practitioners to reconcile delivery of evidence-based practices with culturally relevant ideas and tools that are integral to the healing process. In this systematic review, we aim to (a) provide a brief sociohistorical background on the experiences of Afghan refugees in the United States, (b) delineate EBI that have targeted Afghan refugee mental health in Western countries with a specific focus on the types of outcomes they have addressed and their effectiveness, and (c) the extent of their cultural adaptations.
Sociohistorical Background
Throughout the past 40 years, Afghan refugees have been resettled into the United States across multiple waves. There are notable differences among individuals’ experiences and sociopolitical climates during each timepoint. The extent of sociohistorical data available for each wave of forced migration varied with the passage of time, with the first wave having the least and the current wave presenting the most detailed information. In the following section, we will briefly review past migration wave patterns before 2021. The first group of Afghan refugees was displaced during the invasion of the Soviet Union from 1979 to 1989. Between 1970 and 1989, the U.S. government admitted around 20,000 Afghan refugees for permanent resettlement. During this period most Afghans arrived in the United States on refugee status; others came as immediate family members under family reunification (Stempel & Alemi, 2020). Following the withdrawal of the Soviet Union, two civil wars from 1989 to 1992 and 1992 to 1996 led to the second wave of refugee resettlement. By 1993 the United States officially admitted 25,795 Afghan refugees for permanent resettlement (Lipson, 1993). Stempel and Alemi suggest that in the 1990s, Afghan refugees were much more likely to live at or below the poverty level and in larger families, with more family members of working age than the general American population. Only a small proportion of Afghan families gained financial security through adolescent and adult family members working in low-paying jobs. Many newly resettled people also faced employment challenges due to insufficient or accented English, most of whom were middle-aged or older.
In contrast, the U.S. military presence in Afghanistan from 2001 to 2020 led to a rapid increase in the number of refugees admitted to the United States. In 2008, the SIV program was established, through which a large number of Afghans gained long-term residency status. Refugees arriving during this period generally had a higher rate of high school degrees than the U.S. population (Stempel & Alemi, 2020). However, in constant dollars, the median family income of recent refugees was US$8,000 lower than the refugees who arrived in the 1990s (Stempel & Alemi, 2020). Across the protracted periods of displacement among Afghan refugees, this population has faced a series of consistent systemic challenges that can include economic instability, gender disparities, and language and cultural barriers to societal integration.
Sociopolitical Underpinning of Mental Health Challenges
Scholarship on the mental health of Afghan refugees in the United States has predominantly focused on the prevalence of psychopathology, including depression, anxiety, and PTSD (Turrini et al., 2017). Recent estimates suggest that approximately 30% of Afghans impacted by systemic violence and forced migration will need some level of immediate mental health intervention (Silove & Ventevogel, 2022). There are certain sociopolitical challenges that permeate the lives of many forcibly displaced populations across ethnic groups, which in turn can significantly hinder their mental health. For Afghans, these can include pre-migration stressors such as imprisonment, genocide, physical/sexual violence, traumatic bereavement, starvation, homelessness, and lack of health care (Cardozo et al., 2004; Scholte et al., 2004). Mental health challenges among refugees can also occur as a result of factors that happen after displacement. These can include discrimination, detention, denial of the right to work, denial of health care, and uncertainty on asylum application decisions (Bhugra & Jones, 2001).
In addition to the ubiquitous risks that many refugees face, forcibly displaced Afghans may be especially prone to certain challenges. For instance, given the religious background of most Afghan refugees as Muslims, an additional postmigration stressor leading to mental health challenges for those resettling in Western countries is Islamophobia (Ali & Awaad, 2019; Gokani et al., 2023). Similarly, Afghan refugees often refer to issues with cultural adjustment as some of the most potent sources of stress, including generational differences in values leading to parental-child conflicts, non-volitional changes in gender roles, and the lack of language fluency that causes unemployment and financial hardship. Furthermore, one of the most significant risk factors for the onset of mental health issues is diminishing social support and legal status (Alemi et al., 2014). While Afghan cultural values greatly emphasize social connectedness as a means to fostering well-being, language barriers can often limit the extent to which refugees can develop relationships with members of host nations. The lack of social support systems has especially impacted Afghan refugees from higher socioeconomic status (SES) backgrounds who have been more likely to find asylum in countries with lower rates of Afghan populations (Alemi et al.). While refugees to countries such as Iran and Pakistan have access to more robust Afghan communities, refugees to Western countries face an especially heightened risk for isolation, contributing to serious depressive symptoms.
Unlike the breadth of studies that have focused on the range of psychopathological sequelae and their underpinnings among Afghans resettled in Western countries, few studies have explored the repertoire of current interventions addressing the overall mental health needs of this population. To our knowledge, no scholarly work has systematically explored the extent to which these EBI have been culturally adapted to meaningfully address the mental health concerns of Afghan refugees in the United States or other Western countries. Mental health encompasses both the absence of psychopathology as well as the presence of psychological well-being (Galderisi et al., 2015). While the exact definition of psychological well-being is debated, scholars have consistently noted that in addition to ameliorating psychopathological symptoms, it is imperative to promote the presence of key psychosocial skills. These skills are integral for individuals to manage their daily stressors and live fulfilling lives in harmony with their environment (Manwell et al., 2015). As such, in this systematic review, we intentionally captured both EBI that reduce psychopathology as well as those that have addressed different components of psychological well-being. While we may have used the terms interchangeably, our goal was to capture overall mental health functioning.
Current Study
In this systematic review, our second aim was to delineate EBI that have targeted Afghan refugee mental health in Western countries. We specifically focused on the types of mental health outcomes that interventions have targeted, as well as their effectiveness rates. Our third aim was to categorize the extent to which EBI were culturally adapted for use with this population. Years of scholarship exploring the cultural adaptation of EBI has proposed frameworks guiding the various facets involved in the preparation of programs for delivery to diverse groups. Some programs focus on the nuances of adapting specific treatment components (Bernal et al., 1995; Chu & Leino, 2017) while others capture the logistical processes through which the adaptations must occur (Spanhel et al., 2021). Scholars have especially emphasized considering the extent to which treatment components can be attuned to the needs of target populations, and they often advocate for a distinction between changes to core versus peripheral elements (Lindegaard et al., 2022; Sangraula et al., 2021). The Cultural Treatment Adaptation Framework (CTAF) proposed by Chu and Leino provides practitioners with a systematic approach for exploring this dichotomy (e.g., core vs. peripheral). This framework enables researchers to determine the depth at which they wish to alter EBI treatment components. While other frameworks for categorizing cultural adaptations to treatment aspects exist, for example, The Ecological Validity Framework (Bernal et al., 1995), we find that the CTAF model provides a more concise and organized tool for the purposes of this study.
It is important to note that despite the potent role of faith beliefs for the treatment of mental health, specifically for refugee populations (Al-Nuaimi, & Qoronfleh, 2022), scholarship around cultural adaptations often neglects to recognize how EBI must be attuned to participants’ spiritual beliefs (Hodge, 2011). Given the particular relevance of faith and religious practice among certain groups of Afghan refugees (Gokani et al., 2023), we were intentional about defining cultural adaptations to also encompass how programs aim to meet participants’ spiritual beliefs.
Cultural Treatment Adaptation Framework
The CTAF provides a structure for organizing the degree to which treatment components in EBI can be impacted through cultural adaptations. Importantly, the goal of the CTAF model is to ascertain the degree or depth of adaptations as they occur (Chu & Leino, 2017). CTAF encourages categorizing the types of changes that can occur between Core and Peripheral components to organize the levels of EBI adaptations.
Core Components
Core treatment modifications consist of changes to the primary therapeutic elements—often backed by evidence— that are expected to affect symptoms of mental health disorders. This category is made up of four levels of change: Complete Treatment Change, Core Additions, Core Modification, and No Change. These four levels of change create a spectrum indicating the extent to which modification to the original treatment model is required. Complete Treatment Change indicates that “a traditional EBI is found to be a poor cultural fit and requires substantial changes to the extent of an entirely different treatment” (Chu & Leino, 2017; p. 50). The remaining three levels are less profound. Core Additions are appropriate when core components are relevant to the population and could be augmented by additional modules. Core Modifications occur when one or more core components need to be altered or removed due to cultural incongruence, while No Change indicates that the EBI is appropriate as it stands.
Peripheral Components
Peripheral components consist of intervention modifications that increase the responsiveness of a treatment for a specific population without adjusting any core elements. It entails two subcategories of Engagement and Treatment Delivery. Engagement is defined as the program’s success in reaching participants where they are at and connecting with them in a way that fosters a sense of involvement. Treatment Delivery consists of components such as Materials and Semantics, Cultural Examples and Themes, and Therapeutic Framework. Materials and Semantics modifications include changes to content such as language and graphics to make it more appropriate to the population. Cultural Examples and Themes encompass “incorporating cultural examples, identities, values, beliefs, and practices in treatment” (Chu & Leino, 2017, p. 50). Therapeutic Framework refers to the organizational structure that facilitates treatment delivery—such as the actual session structure. It can also encompass practitioner–client relationships—such as maintaining consistency with cultural values in interpersonal styles with the client. Finally, person/place concerns include inclusion of collaborators into the treatment and location of delivery.
Methods
Search Strategy
We searched PsycArticles, PubMed, and Google Scholar to identify studies of interest for this systematic review since the year 2000. To narrow down our search, we required the use of the term refugee in the title of the articles, with at least one of the following terms: effectiveness, evaluation, intervention, program, and trial. In addition, and when possible, we excluded words that did not pertain to our search from titles such as Syrian, Veteran, or Malaria. To augment this search, we explored previous studies synthesizing the state of mental health among Afghan refugees in the United States, including Lipson (1993) and Alemi et al. (2014). We conducted this systematic review in line with principles of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (Page et al., 2021).
Study Inclusion and Exclusion Criteria
Due to the limited number of empirical studies that have explored the effectiveness of EBI specifically for Afghan refugee populations in the United States and other Western countries, our search aimed to be as broad as possible in considering what constitutes as an evaluation study. We considered a study to meet inclusion criteria if it entailed any form of intervention that was quantitatively assessed and reported effectiveness of desired outcomes, even in the absence of baseline (pre) test measures. We therefore included a range between pilot assessments and rigorous experimental designs such as Randomized Controlled Trials (RCTs). We considered interventions that focused on any form of psychosocial outcomes, including systematically defined mental health disorders as well as general measures of well-being. We excluded any study that did not include a concrete outcome measure (e.g., Rosenberg et al., 2022). Importantly, we only included studies where Afghan participants composed the majority of the study ethnic composition—defined as over ⅔ or 67% Afghans. We excluded 16 studies because Afghans were less than ⅔ of the population. One study (Lindegaard et al., 2022) was excluded because while it included almost all Afghan participants, only two members completed the intervention.
No other demographic restrictions (e.g., gender, age, mental health diagnosis, or time of arrival) were included. EBI could have been implemented in both clinical and community settings, for example, community centers, and schools. We limited our search to programs that were implemented in non-Muslim majority countries in the Americas, Europe, and Australia.
Procedures
Upon selection of empirical studies falling within our inclusion criteria, one research assistant and the principal investigator agreed upon concrete definitions and examples of peripheral versus core adaptations as informed by the CTAF model. The research assistant then extracted any mention of cultural considerations and coded whether they could be categorized as a core versus peripheral change. After delineating the type of adaptations, the research assistant further distinguished between the subtypes of core and peripheral changes. The final list included type, subtype, and examples of each adaptation. In the last step, the principal investigator and research assistant discussed the results to reach agreement regarding the final CTAF categorization. To explore effect sizes of mental health outcomes in each study, we used two approaches. For studies that did not report effect sizes, our team calculated the effect sizes using the data reported in the body of the text or in supplementary materials. A second member of our team then reviewed the calculations a second time to ensure accuracy of the results. For studies that did include effect sizes in their results, we reviewed the analytical and statistical procedures to ensure rigor in their calculations.
Results
Of the total 1709 studies that emerged from our search, seven studies met our inclusion criteria for this systematic review. To organize this systematic review, for each study we will first report on the clinical intervention modality and outcomes, followed by a discussion of the extent to which cultural adaptations have occurred. Of the seven studies, three studies used cognitive behavioral therapy (CBT) or trauma-focused CBT (TF-CBT), one study provided a program focused on emotion regulation, one study specifically targeted families, and two studies used a variety of clinical treatments—hereon referred to as multimodal interventions. All programs included in this study entailed group activities, except a multimodal intervention evaluated by Knefel et al. (2022).
CBT or TF-CBT
1. In a pilot study of a culturally adapted CBT intervention, Kananian and colleagues (2017) evaluated the implementation of a 12-session program including psychoeducation and concrete strategies for the management of depressive, anxiety, and trauma symptoms. Results suggested that participants exhibited reductions in their severe depression, anxiety/insomnia, and social dysfunction rates, and improvements in general quality of life and affective coping skills. This program, as well as its reiteration in 2020, included the most extensive amounts of cultural adaptations when compared with all the other interventions. These adaptations are enumerated below.
Core Changes
Additions
The program facilitated exchange with peers and the Iranian/Afghan community since being with family and socialization were behaviors that improved resilience.
Modifications
The program implemented mindfulness through a spiritual and God-centric approach. This was because praying and accepting life’s situations as the will of God were common concepts to promote healthy behaviors but meditation as a Buddhist tradition was not well received.
Peripheral Changes—Treatment Delivery
Material and Semantics
The program incorporated idioms of distress in Farsi/Dari such as “asabi” (nervous agitation) and “gham” (sadness). Instruments that were not available and validated in Farsi were translated and back-translated.
Cultural Examples and Themes
The program changed metaphors. For example, those referring to an inner child were changed to an alarm system because refugees had previously indicated that they could not connect with the idea behind it. The program also used “bagh” (peaceful garden) for guided imagery in meditations as it was more culturally relevant. One of the main components of the intervention was a meditative exercise titled Loving Kindness Meditation, which asked participants to project loving kindness to all beings. This practice was adjusted to focus more on “benevolence and compassion for oneself, family members, and friends” rather than to all beings. This was because patients had experienced egregious adversities at the hands of members of their society (Kananian et al., 2017, p. 6).
Therapeutic Framework
In terms of person/place, the program included professionals who were well-versed in treating Afghan populations, and interviews were conducted by Farsi-speaking psychologists. Furthermore, a group setting was intentionally chosen as an intervention modality to destigmatize treatment through exchanges regarding symptoms with members of the same culture. This enhanced feelings of connectedness through group cohesion, especially when sharing experiences about asylum procedures. Given that in initial focus groups participants had reported a preference for participating in gender-homogeneous sessions, only male participants were included in this study.
2. Teaching Recovery Techniques (TRT) program is a TF-CBT-based intervention for children which includes practices such as psychoeducation, interpersonal skills, affective and cognitive regulation competencies, writing of trauma narratives, and exposure techniques (Sarkadi et al., 2018). Caregiver sessions include activities to prepare them for supporting their children as they cope with their trauma symptoms. Authors found that the program was able to reduce children’s short-term PTSD and depressive symptoms. The only adaptation involved in this program entailed a peripheral change. In the context of Treatment Delivery—Material and Semantics, the program included interpreters who were available during information sessions and translated Swedish materials into participants’ languages.
3. A more recent evaluation of the TRT program was completed by Solhaugh and colleagues (2023). The authors reported that the program was able to improve participants’ life satisfaction after the completion of the intervention, with sustained effects at 8-week follow-up. The authors only reported peripheral adaptations to the program, including in the context of Treatment Delivery—Material and Semantics where bilingual research staff ensured that participants understood measures adequately. Furthermore, measures were translated using professional translators and bilingual research staff, and refugee advisors ensured that the jargon was appropriate.
Emotion Regulation
4. A group of scholars (Koch et al., 2020) evaluated a program specifically focused on the management of difficult emotions. This intervention was titled Skills-Training of Affect Regulation—A Culture-sensitive Approach (STARC) and focused on emotion regulation as a transdiagnostic skill affecting multiple mental health challenges. Participating in the STARC program led to decreases in difficulties with emotion regulation and reductions in multiple indicators of psychopathology, for example, depression and anxiety/insomnia. This program only included peripheral changes by incorporating Cultural Examples and Themes. Clinicians used religious phrases narrated from key Islamic figures for sessions on management of anger and provocations.
Family Therapy
5. El-Khani and colleagues (2021) explored the feasibility of short family-based interventions titled Strong Families in Serbia with Afghan refugee families residing in Reception Centers across the country. Through this intervention, children and families participated in group-based child-only and caregiver-only sessions that were augmented by joint family meetings. The program focused on areas such as individual stress management, co-regulation, and positive discipline. Results indicated that the program was able to reduce children’s emotional, conduct, hyperactivity, peer, and total difficulties. In addition, parents reported improvements in their overall parenting.
The authors used a version of the Strong Families program which was previously culturally adapted, translated, and reviewed by the Afghan Ministry of Public Health and Education (Haar et al., 2020). The program was initially piloted with families in Afghanistan prior to El-Khani and colleagues implementing it in Serbia. However, the details of the adaptation are not made available, and we were unable to determine whether involvement of these Afghan stakeholders entailed core versus peripheral adaptations. The program did include a peripheral change in its Treatment Delivery—Material and Semantics because questionnaires were translated into Dari.
Multimodal Interventions
6. Kananian et al. (2020) implemented an augmented version of the pilot study in 2017 by incorporating problem-solving sessions to the original CBT approach. The authors reported improvements in general psychopathological distress as well as depressive symptoms, somatic complaints, quality of life, and emotion regulation. Participants also exhibited moderate reductions in PTSD symptoms. Most of the cultural adaptation considerations in this study were identical to those reported in the 2017 piece. However, this study entailed two unique changes.
Core Change—Additions
Informed by results of the 2017 study, the clinicians added a problem-solving training meant to “empower patients to take independent actions within their social contexts, to further their basic needs . . .” (Kananian et al., 2020, p. 6). Through this approach, the intervention aimed to focus on context-specific needs that Afghan participants had identified as relevant.
Peripheral Changes—Treatment Delivery
The authors used Cultural Examples and Themes as a form of peripheral change. Housing/accommodation-related difficulties, loss of culture and identity, “thinking too much,” and financial hardships were added as root causes when providing disorder-specific psychoeducation because Afghan refugees had previously mentioned them as explanations of depression (Kananian et al., 2020).
7. The only individual-based intervention was implemented by Knefel and team (2022). The authors evaluated the effectiveness of the Problem Management Plus (PM+) program. PM+ is an intervention that was previously designed by the World Health Organization as a transdiagnostic approach that addresses symptoms of common mental health challenges through “managing stress, managing problems, get going-keep doing, and strengthening social support (Dawson et al., 2015). The authors found that participation in the program improved general health, distress caused by postmigration living difficulties, PTSD symptoms, and quality of life. We were unable to determine if the program entailed core changes. The authors noted that the original PM+ program was culturally adapted for use with refugees, but they did not provide more information. They also noted that they added a fifth module on anger management and building self-efficacy as they were important for this population. However, it is unclear whether these additions were carried out based on sociocultural responsiveness or not. The program included peripheral change in its Treatment Delivery—Material and Semantics as questionnaires were translated into Dari by translators.
Discussion
The protracted nature of experiences with forced displacement among Afghan refugees has exposed this population to myriad risk factors across different time points that underpin challenges to their mental health. Forced migration to Western countries poses unique difficulties that are especially rooted in sociocultural incongruences between Afghan communities and host nations. This systematic review delineated EBI that have addressed the mental health of Afghan refugees resettled in Western countries. Specifically, we first reported on the mental health outcomes that these interventions have successfully improved. Second, we used the CTAF model to explore the extent to which these programs have been culturally adapted (Chu & Leino, 2017).
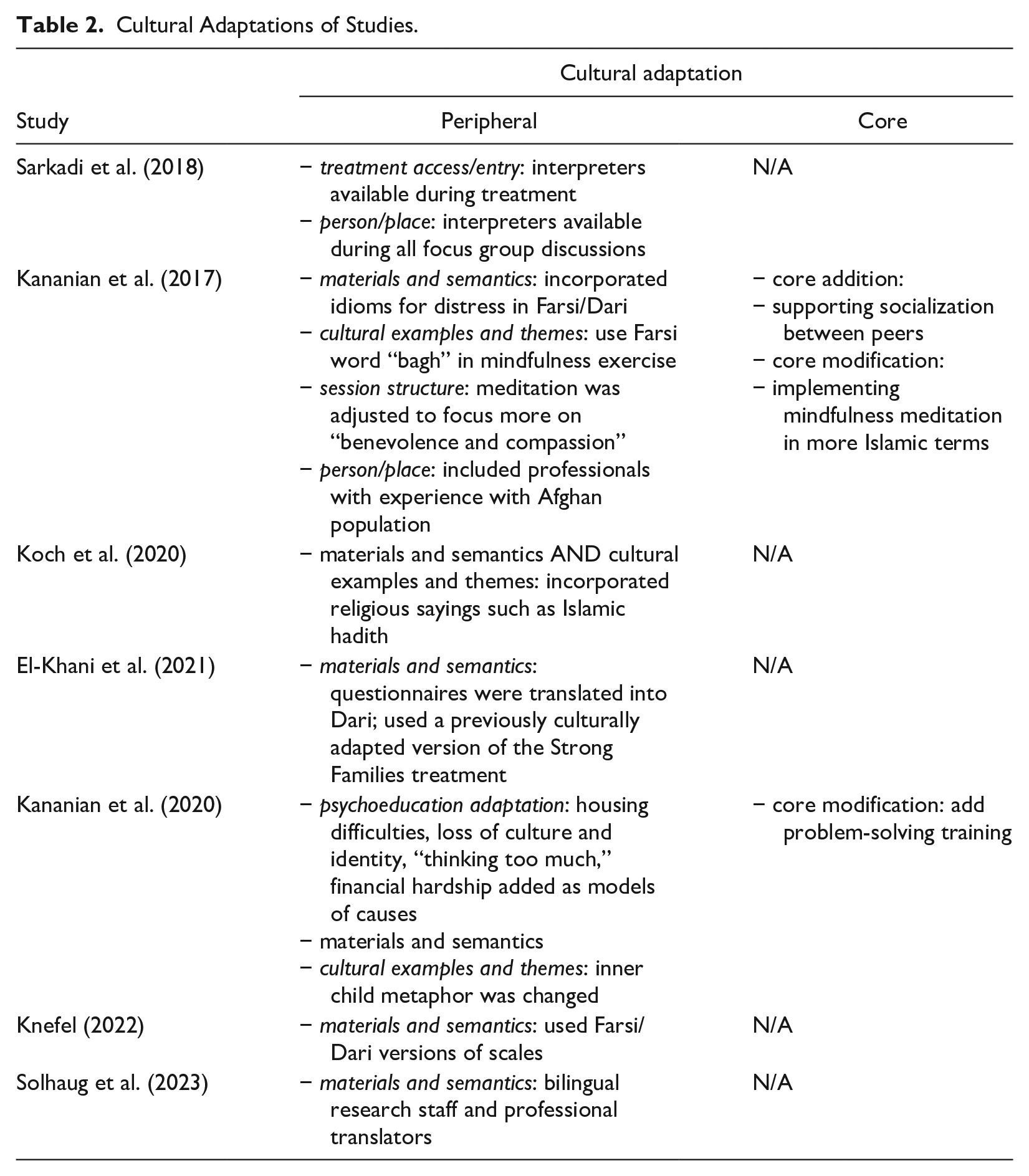
Among the seven studies that we included, interventions most frequently addressed and were successful at reducing PTSD symptoms (N = 5), followed by depressive symptoms (N = 3). Three studies also focused on improving overall quality of life (for a complete list of outcomes see Table 1). Furthermore, organized by the CTAF model, the most frequent type of cultural adaptation included peripheral changes through materials and semantics whereby all programs included trained translators to administer intervention content and measures (See Table 2). Four studies further included peripheral adaptations by employing cultural examples and themes that assisted participants in understanding and connecting with the content. Importantly, in the CTAF model this type of peripheral change is distinguished from core modifications. The use of cultural examples and themes assists with the comprehension and acceptance of core therapeutic ideas that are already a part of an EBI. For example, Koch et al. (2020) capitalized on teachings by historical Islamic figures to promote the idea of anger management, a core element that was already a part of the EBI prior to its adaptation. This approach is juxtaposed with core modifications in that a core modification alters what is assumed to be a therapeutic priority for intervention. For instance, Kananian et al. (2017) shifted from focusing on meditation as an essential therapeutic component to a mindful acceptance of adversities based on spiritual beliefs. Instead of finding a relatable way to teach meditation, as would a peripheral adaptation, this approach prioritized a different conduit for accomplishing inner peace through acceptance. Of note, only Kananian et al. (2017, 2020) included adaptations to core treatment components, including both core additions and modifications.
Characteristics of Studies Meeting Inclusion Criteria.
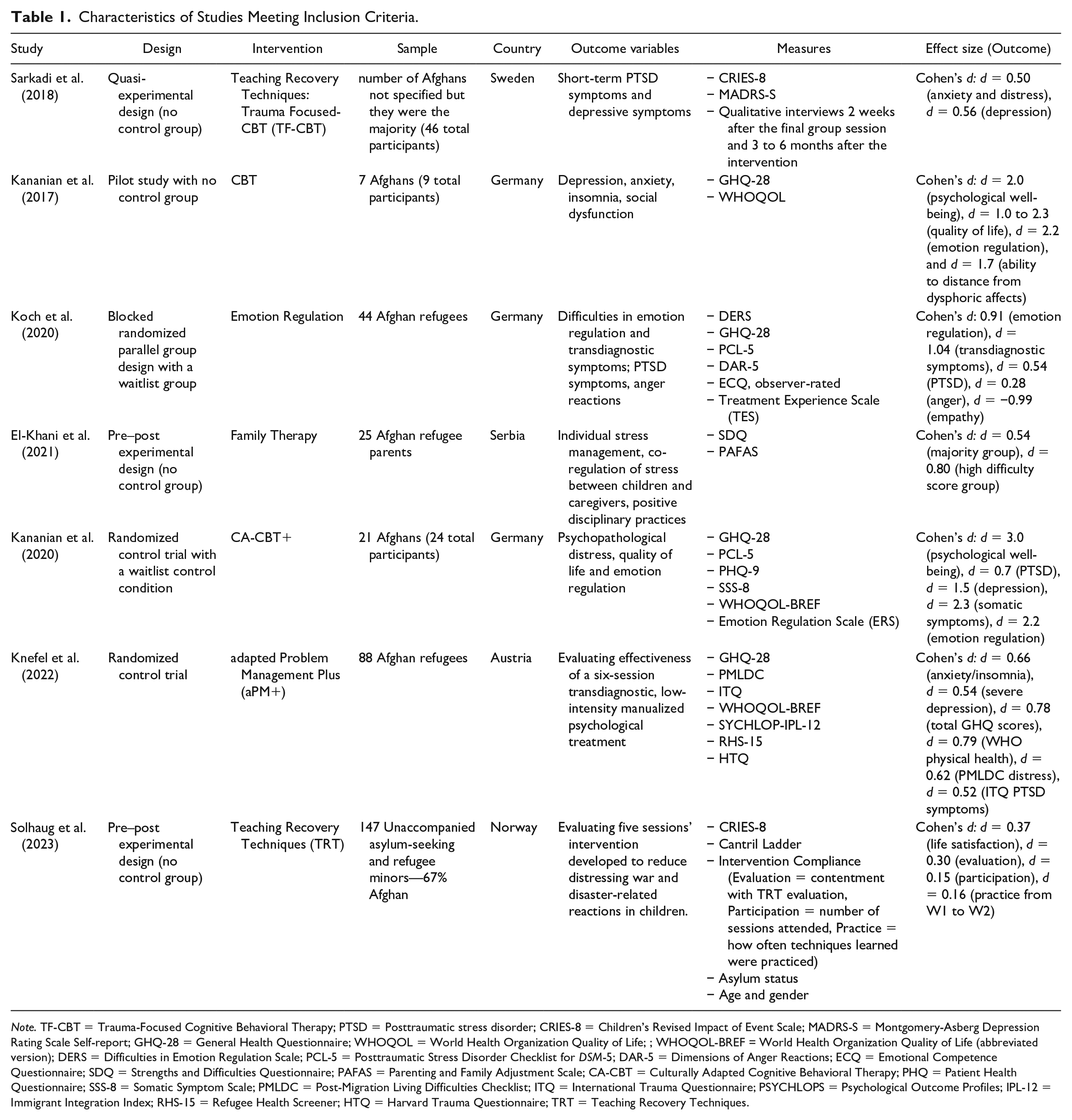
Note. TF-CBT = Trauma-Focused Cognitive Behavioral Therapy; PTSD = Posttraumatic stress disorder; CRIES-8 = Children’s Revised Impact of Event Scale; MADRS-S = Montgomery-Asberg Depression Rating Scale Self-report; GHQ-28 = General Health Questionnaire; WHOQOL = World Health Organization Quality of Life; ; WHOQOL-BREF = World Health Organization Quality of Life (abbreviated version); DERS = Difficulties in Emotion Regulation Scale; PCL-5 = Posttraumatic Stress Disorder Checklist for DSM-5; DAR-5 = Dimensions of Anger Reactions; ECQ = Emotional Competence Questionnaire; SDQ = Strengths and Difficulties Questionnaire; PAFAS = Parenting and Family Adjustment Scale; CA-CBT = Culturally Adapted Cognitive Behavioral Therapy; PHQ = Patient Health Questionnaire; SSS-8 = Somatic Symptom Scale; PMLDC = Post-Migration Living Difficulties Checklist; ITQ = International Trauma Questionnaire; PSYCHLOPS = Psychological Outcome Profiles; IPL-12 = Immigrant Integration Index; RHS-15 = Refugee Health Screener; HTQ = Harvard Trauma Questionnaire; TRT = Teaching Recovery Techniques.
Cultural Adaptations of Studies.
Effectiveness as a Function of Cultural Adaptation
A salient question among researchers and practitioners of cross-cultural psychology has consistently revolved around the most effective level of adaptation: How can providers balance fidelity to core psychological principles of interventions while ensuring cultural relevance? Scholarship in this area has emphasized the measurable benefits of cultural attunement for mental health outcomes (Hall et al., 2016; Hecht & Shin, 2015). However, the popular opinion is to prioritize keeping core psychological components intact and adapt interventions through changes to peripheral areas (Castro et al., 2004; Gonzales, 2017). In line with this paradigm, most EBI, including those included in this systematic review, only include peripheral adaptations (Chu & Leino, 2017). This practice is rooted in the idea that certain psychological processes are fundamental to human functioning regardless of environmental factors, substantiating avoiding changes to core components to facilitate what is assumed to be universal theories of change in human cognition and behavior. The main challenge with this idea, however, is that the same ostensibly universal cognitive processes can be contextually socialized to view the world through disparate lenses, leading to diverse definitions of desired psychological and health outcomes (Tsai, 2017). Importantly, these differences can impact refugees’ priorities and definitions of what healing and posttraumatic growth look like (Calhoun et al., 2010).
An evidence-based comparison of effectiveness rates between the seven studies in this systematic review is not feasible. Given the wide diversity in treatment modalities, local implementation factors, measurement tools, and participant demographics such as age, it is not possible to unequivocally determine the effectiveness of programs based on their approach to cultural adaptations. Recent systematic reviews exploring extant psychosocial support programs for refugees have reported similar challenges given the great heterogeneity between evaluation studies (Spanhel et al., 2021; Taylor et al., 2023). As such, we report observations regarding the performance of interventions in this systematic review depending on their level of cultural adaptations without making any directional claims.
While only one program (spanning two studies) incorporated changes to core elements, it reported higher effect sizes (Cohen’s d) in reducing PTSD and depressive symptoms. The study by Kananian et al. (2020; PTSD d = 0.7; Depression d = 1.5), which includes core adaptations, reports higher effect sizes than other studies such as Knefel et al. (2022; PTSD d = 0.52; Depression d = 0.81) and Koch et al. (2020; PTSD d = 0.54; Depression d = 1.04). This is an intriguing finding that merits further explorations. These differences may be due to a variety of factors such as treatment modality. For example, the intervention by Kananian et al. included multiple components such as CBT principles and problem-solving tools while Koch and colleagues only focused on emotion management. Alternatively, the observed differences may be informed by the use of different measurement tools. It may also be the case that programs incorporating core adaptations to EBI are better capable of addressing the mental health needs of populations whose experiences differ from those for whom the programs were initially developed. While these observations should be regarded with caution given the absence of statistical analyses, they support other scholarship that has encouraged the direct comparison of original and culturally adapted interventions in addressing the mental health of vulnerable groups (Spanhel et al., 2021). They further provide a direction for future meta-analyses. Future studies must consider the extent of cultural adaptations as a potential indicator of program success. Informed by the EBI surveyed in this systematic review, as well as our team’s clinical expertise with this population, the following section will provide recommendations for practitioners who implement mental health programs for Afghan refugees in Western countries.
Recommendations for Cultural Adaptations
Measurement
In the interest of construct validity, it is imperative that practitioners plan for capturing baseline and outcome indicators of mental health through reliable, interpretable, and properly translated measures. When available, it is preferred that practitioners use measurement tools that have been specifically designed for use with a particular linguistic and ethnic group, especially as they tend to incorporate cultural idioms of distress. Kananian et al. (2017, 2020) adapted their measurement tools to incorporate idioms of distress specific to the Afghan population, including Dari concepts such as “asabi” (roughly translated to nervous agitation) and “gham” (sadness). The use of culturally attuned idioms is particularly significant because they may reflect Afghan mental health more accurately than Western mental health diagnostic criteria (Wildt et al., 2017). In fact, Miller et al. (2006, 2009) found that using cultural idioms of distress for diagnosis may be more clinically beneficial than Western-based jargon.
Cultural Examples and Themes
When the incorporation of core adaptations to Western-based interventions is not feasible or recommended, it is imperative to consider the use of culturally attuned examples that can facilitate engagement with core therapeutic content. For example, Koch et al. (2020) incorporated Islamic sayings into the section of their intervention focused on anger management. This allowed the community to understand anger management through their own culture and religious doctrine. In turn, this approach facilitated a sense of acceptance and ownership over the complicated task of regulating strong emotions such as anger.
Daily Stressors and Problem-Solving
Daily, postresettlement challenges often place a great deal of burden on the stress physiological response system of refugees. This can sometimes exceed the effects of their past trauma exposure prior to and during their forced migration. Research has indicated that daily stressors can contribute to equal or even higher levels of depression, anxiety, and distress than the adversities that refugees experienced during their displacement (Behrendt et al., 2023; Hornfeck et al., 2023; Miller & Rasmussen, 2010). While the daily stressors that refugees face spans multiple domains, for example, acculturative stress, limited housing, threat of deportation, and restricted social capital, many interventions fail to adequately address them (Behrendt et al., 2023). Interventions that consider and account for a variety of daily stressors may improve mental health outcomes more than those solely focusing on pre-migration and displacement trauma. Kananian et al. (2017, 2020) and Knefel et al. (2022), for example, clearly focused on the importance of preparing refugees to know how to manage their postresettlement stressors. Those who partook in Kananian et al.’s intervention emphasized the importance of discussing their daily problems as a tool for concrete and collective problem-solving. An example of a daily stressor for recent Afghan refugees in the United States can include restricted mobility due to difficulties with navigating the transportation system and the process for attaining a driver’s license (Hosseini et al., n.d.). Practitioners who support Afghan refugee mental health must therefore plan for therapeutic models that incorporate capacity building opportunities, especially because struggling with challenges such as lack of access to basic needs, language barriers, and family separation can occupy most of the participants’ focus and energy at baseline. Ameliorating daily challenges can reduce the cognitive and emotional load that refugees must carry and enable them to focus on their healing and pursuit of dreams. Furthermore, interventions that solely focus on distal experiences with adversities may struggle with meaningfully engaging refugees as participants may not find the programs relevant to their daily demands.
Meaning-Making Around Adversities
Scholarship and practice addressing the mental health needs of Afghan refugees must critically explore how therapeutic models have defined core notions of overall adaptive psychological well-being and mental health. This can span what are considered normative cognitions, emotions, and behaviors. Importantly, clinicians must question whether Western worldviews that have informed the core cognitive principles of interventions are universal, and whether they can expect participants to adhere to those ideas (Ally & Laher, 2008). One critical manifestation of how diverse worldviews about ideal mental health functioning can impact therapeutic processes is meaning-making (Park, 2016). Cultural and spiritual backgrounds can significantly impact how individuals make sense of the adversities they have faced, which in turn can influence their mental health outcomes (Park, 2013). For instance, certain groups may situate their psychological well-being primarily within a social and collective context. When they experience personal adversities, they may locate the adverse experience in the broader context of what it means for their community (Raghavan & Sandanapitchai, 2020). Furthermore, their individual well-being may at least partially be intertwined with that of their community (Atkinson et al., 2019).
Afghan refugees in Western countries, for example, can face many difficulties that could be construed as severe risk factors for psychopathology. However, Afghans may be able to regulate the intensity of these challenges by ascribing a collectivist meaning to their experiences. They may contextualize their situation based on their ability and responsibility to strive toward better conditions for their family—especially those left in their country of origin. By focusing on their contribution to the well-being of those they care about, Afghan refugees may be able to reduce the visceral impact of adversities and use this meaning-making approach as a protective mechanism. Given this possibility, interventions that promote deep levels of self-awareness on psychosomatic reactions may do more harm than good. Practitioners must therefore be intentional about discussions of self-awareness relating to internal affective and cognitive functioning and pay special attention to the required balance between a focus on the well-being of the self versus the self as situated within a larger social context (Yeh et al., 2004).
Similarly, practitioners must also consider the role of faith in how Afghan refugees make sense of their negative experiences. Many of the adversities that refugees face are beyond their control. There is a plethora of research indicating that a lack of control, particularly over a long period of time or with no end in sight, can cause distress and negative psychological outcomes (Miller & Rasmussen, 2010). A deep understanding around how refugees make sense of lacking control can therefore be a critical first step before assisting them in reframing their perceived powerlessness. Hosseini et al. (n.d.) suggest that despite their challenges, Afghan refugees feel at ease when they put their trust in God’s plan, indicating a faith-based meaning-making approach. Similarly, Kananian et al. (2020) adapted their manual to incorporate the acceptance of their situation and finding meaning in their adversities through the will of God. Many Afghan refugees were able to make sense of their stressors, unpredictability, and trauma through a God-centric prism, in turn contributing to a sense of order when they perceived their life situation part of God’s plan. We therefore encourage practitioners to dedicate initial sessions with Afghan refugees to explore how they make sense of the adversities and lack of control they may face, as well how they find the strength to cope with these experiences. These initial sessions can support clinicians in offering therapeutic models that are in harmony with Afghan refugees’ core beliefs.
Cultural and Spiritual Heterogeneity
In addition to the variability between Afghan populations and other groups, it is imperative for EBI to consider the heterogeneity within Afghan populations who have diverse migration histories and cultural/spiritual backgrounds. As noted in this systematic review, Afghan refugee displacement is associated with long-standing histories of war and oppression from internal and external political forces, contributing to intergenerational trauma and mental health challenges. Mental health practitioners must critically examine how intersectional experiences with gender, ethnic and tribal affiliations, sectarian differences, education levels, and socioeconomic class may shape both premigration and postmigration experiences of Afghans. EBI must also explore the variability of faith and spiritual experiences of Afghan refugees and the extent to which they can be relevant for healing. Accordingly, we recommend that mental health providers seek training on the role of faith in the lives of Afghan refugees and seek to understand the diversity of narratives that exists within this population. For example, Afghan refugees who come from Shia backgrounds may have different experiences and histories of oppression due to their minority status in comparison with Sunni Muslim Afghans. Interventions incorporating elements of faith and spirituality must critically consider the unique experiences of diverse Muslim groups in the homeland, throughout various stages of migration, and as they seek to integrate into U.S. society.
Isolation as a Contextually Relevant Risk Factor
One of the most socioculturally salient risk factors that Afghan refugee populations resettled in Western nations face is social isolation. Given the strong interpersonal bonds and collectivist socialization processes embedded within this group, Afghan refugees encounter increased risks for the onset of mental health sequelae when faced with spiritual, linguistic, and cultural integration challenges. The success of EBI in promoting well-being is therefore intertwined with the extent to which they can address Afghan refugees’ needs to balance integration with ethnocultural and spiritual identity development. A rich body of literature has encouraged nuanced approaches to acculturation as a pathway for integration and well-being. A nuanced approach enables refugee individuals to freely explore their ethnocultural and spiritual identity development without perceiving threats to their involvement in host communities (Groen et al., 2018, 2019). While a connection with religious and cultural backgrounds of countries of origin has often been a protective factor for better mental health among refugees (Beiser & Hou, 2006; Ellis et al., 2010), individuals must also build clarity and confidence toward their optimal level of identification with their resettlement social contexts. This balancing act is person-specific and contingent on a host of sociocultural factors, including prior experiences in countries of origin, time since displacement, gender, SES, and religiosity.
In the context of recently arriving Afghan refugees in the United States, this is also impacted by the extent to which individuals were involved with American stakeholders (e.g., U.S. government and military) in Afghanistan prior to their displacement. As stated in the introduction, those involved with American stakeholders include Special Immigrant Visa Holders (SIVs) who are eligible to become U.S. lawful permanent residents if they worked as translators, and drivers for the U.S. government in Afghanistan (U.S. Department of State, 2023b). Given that they receive a permanent immigration status soon after their arrival in the United States, as well as their English proficiency, these individuals tend to face fewer challenges when integrating into the society (Gil et al., 2022). It is imperative to mention that there is limited research on the mental health outcomes of SIV holders and their non-SIV peers. Practitioners must provide enough flexibility in their structure so that their adaptations can facilitate participants’ explorations of their identities while promoting social cohesion. A key part of facilitating this balance is recognizing the role of family relations as a protective factor, whereby strong familial relationships may contribute to health equity outcomes of this population.
Transnational Families
Finally, mental health practitioners working with Afghan refugees should consider taking on a transnational approach in defining the family unit, as many Afghans have left family members either in Afghanistan, refugee camps, or other host societies. Adopting a transnational collectivist approach (Magan & El-Khaoudi, 2023) in service delivery allows us to consider the importance of the collectivist nature of Afghan culture as well as the role of family beyond nation-state boundaries. This approach also challenges Western mental health approaches that often center the individual without considering the role of the collective. It also positions us to critically examine how we define the collective as not only those who are in the immediate family unit and resettled in the United States but those who remain outside of the resettlement context. These family members still maintain strong ties via communication methods and even receive remittance support from their resettled family in the United States. These connections are critically important to consider as they impact the mental health of resettled refugees who cannot completely disconnect their experiences from their family members abroad.
Limitations
The strengths of this systematic review can be augmented by addressing a number of limitations in future studies. Perhaps the most pressing limitation was that we were unable to compare program effectiveness based on levels of cultural adaptations due to the wide heterogeneity in their dosage, treatment modality, measurement, and so on. Future research endeavors with Afghan populations—and refugee groups in general—must systematically ascertain whether there are differences in programs’ effectiveness based on the type of adaptation they use, that is, core versus peripheral. Moreover, while we only included studies whose participants were more than ⅔ Afghan, it is important to recognize that there may have been differences between studies that intentionally recruited this population versus those that were more open to other ethnic groups. This systematic review could also be more expansive by considering studies that were published prior to 2000 as we restricted our search to those that were completed afterwards. Previous scholarship that may have addressed trends among earlier waves of forced migration are not included in our results.
The small number of studies included in this review can also limit the amount of information we are able to glean about all EBI currently in practice with this population, although this limitation is a function of the overall lack of attention to this topic. Similarly, we conducted this search in English and did not include studies that may have been done in other languages. Among the studies that we did include, our ability to interpret effect sizes was further limited by the fact that some studies did not report their data analytical procedures. Furthermore, because some studies did not include control groups in the evaluation of their program effectiveness, we are unable to unequivocally determine the benefit of their program in its absence. We also found that many studies reported high rates of attrition. While this may be considered a limitation in our interpretive ability, we also find that this may be telling regarding the effectiveness of the programs in engaging refugee populations, perhaps informed by the prevalent tendency to only approach cultural adaptations peripherally.
Conclusion
This systematic review explored current EBI that address the mental health of Afghan refugees resettled in Western countries. EBI for this population have mostly been able to reduce PTSD and depressive symptoms, with only a few interventions attempting to elevate psychological well-being. Furthermore, most programs only incorporate peripheral adaptations to facilitate cultural attunement with the target populations. Only one group of authors used core adaptations to improve the effectiveness of their program, and they reported higher effect sizes in addressing PTSD and depressive symptoms when compared with other programs. In light of these findings, we have provided key considerations for researchers and practitioners addressing the mental health needs of this population. Importantly, we encourage practitioners to consider how sufficing to peripheral adaptations may be predicated on myopic and limited assumptions regarding the homogeneity of how different groups perceive ideal mental health functioning. Prior to determining the extent of adaptations to treatment components, those providing mental health care to Afghan refugees must critically reflect on whose assumptions are being prioritized in the implementation of programs. Afghan refugees often hold rich funds of knowledge regarding how to holistically navigate the challenges of post resettlement, much of which may be rooted in their unique culturally and spiritually informed notions of coping and healing. Peripheral adaptations can fall short in benefiting from these relevant and necessary sources of wisdom, potentially contributing to limitations in the extent to which EBI can be effective (Wessells, 2021). We join forces with other scholars who advocate for further rigorous explorations into how levels and types of cultural adaptations can impact program effectiveness and success (Taylor et al., 2023).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.