
Abstract
This article presents a current knowledge synthesis of empirical studies on cross-cultural psychotherapy since 1980. Guided by a critical review framework, our search in seven relevant databases generated 80 studies published in English. Main themes are organized into (1) therapists’ cultural competence (n = 46); (2) therapy process in cross-cultural dyads (n = 22); and (3) cross-cultural differences in gender, sexual orientation, or social class (n = 12). Compared to previous reviews on cross-cultural psychotherapy, the findings of this review highlight a broad range of methodological rigor in both quantitative and qualitative studies. Most studies examined actual therapy participants rather than participants in analog studies, thus emulating more therapy-near experiences in cross-cultural psychotherapy research. Also, several studies explored cross-cultural compositions beyond racial and ethnic majority therapist-minority client dyads, and included therapists of color as the participants, exploring reverse power dynamics in therapy and giving voices to foreign-born therapists. The therapy process research provides rich and full descriptions around the dynamic and interactional therapy process in cross-cultural dyads, which can be used to foster cultural sensitivities among therapists in their practice and training. We discuss the limitations of the studies included in the review and its implications for psychotherapy practice, training, and future research.
Keywords
American demographers note that nearly half of people born after the mid-1990s identify as racial or ethnic minorities; as of 2017, 13.6% of the population are foreign-born in the United States, the highest since 1910; and this percentage is even higher for 25 nations, such as Australia (29%), New Zealand (23%), and Canada (21%) (Cilluffo & Cohn, 2019). Given this increasing global diversity, clinical practice invariably consists of both clients and therapists representing diverse racial/ethnic backgrounds as well as other cultural backgrounds including age, social class, dis/ability, nationality, religion, and sexual orientation, constructing various compositions of cross-cultural dyads. Central to cross-cultural psychotherapy is a therapist’s capacity to accurately understand a culturally different client’s stories, to negotiate with dis/similar values and views that may exist between the client and therapist, and to collaboratively and effectively work with the client.
To assist therapists in fulfilling these tasks, there has been a steady proliferation of studies synthesizing themes and factors that are associated with effective practice recommendations in cross-cultural psychotherapy (Arredondo et al., 2005; D’Andrea & Heckman, 2008; Pope-Davis et al., 2001). Among these earlier reviews, only one specific journal was used (e.g., Journal of Counseling Psychology) as the search source, and searches were within a limited time period (e.g., 5–15 years) in both empirical and non-empirical studies while exploring themes of race and ethnicity and/or people with racial and ethnic minorities (Arredondo et al., 2005; Leach et al., 1996; Perez et al., 2000; Ponterotto, 1988; Pope-Davis et al., 2001). Recent reviews expanded their search using multiple databases (e.g., EBSCOhost, PsycINFO, PubMed, etc.) and/or setting a wider time frame for study extraction (e.g., 20 years to open duration), focusing on empirical studies only (D’Andrea & Heckerman, 2008; Hall et al., 2016; Soteo et al., 2018; Tao et al., 2015; Worthington et al., 2007).
These reviews critically examined and synthesized the state of knowledge in cross-cultural psychotherapy research and have undoubtedly moved the field forward in building therapist awareness, knowledge, skills, and competencies when working with culturally diverse clients. However, the existing reviews have a few limitations. First, most of the reviews tended to draw an equivalence between culturally competent practice and practice with racial or ethnic minority clients. While there has been an increasing voice calling to de-center the focus on client’s culture (Park, 2005), most reviews explored studies on racial and ethnic minority clients, while other therapeutic processes occurring within the cross-cultural dyad were neglected. Instead of putting the client’s culture under a microscope to be essentialized, problematized, managed, and/or fixed, critical clinical researchers underscore the importance of re-focusing on cross-cultural similarities and differences that exist between the client and therapist (Lee, 2010).
Second, while focusing on racial and ethnic minority clients, most existing reviews assumed therapists are coming from dominant groups of power and privilege in terms of race, ethnicity, and other diversity factors. This assumption makes therapists of color or of other marginalized status in diversity factors invisible in practice and gives little attention to their experience in research. It is important to explore how therapy works in cross-racial or cross-ethnic dyads where both clients and therapists come from various compositions of racial and ethnic groups, and how these similarities and differences are negotiated and further interfere or facilitate therapeutic process and outcomes. In addition, other dimensions of diversity such as gender, sexual orientation, and class are rarely included in discussions of cross-cultural therapy. It remains unclear whether the inclusion of these factors in analysis yields similar findings as when focusing exclusively on racial and ethnic differences. Last, previous reviews highlight that culturally competent or responsive practice is beneficial to clients, yet yield little findings demonstrating “how” this benefit clinically manifests itself in the therapy process (Worthington et al., 2007).
Cross-Cultural Psychotherapy
Culture has been defined in multiple ways. Geertz (1973) defines culture as “an historically transmitted pattern of meanings embodied in symbols” (p. 89). Triandis (1972) proposed the term subjective culture to highlight that individuals are not representing meanings of a monolithic form of culture that exerts its inescapable effects upon us, but rather, we are subjectively interacting and making meanings in a plurality of culture, each exerting a multiplicity, and complexity of influences upon us. Similarly, Ho (1995) underscores the subjectivity of culture and proposed internalized culture as a more relevant one to psychotherapy, defined as “the cultural influences operating within the individual that shape personality formation and various aspects of psychological functioning” (p. 5). Draguns et al. (2004) elaborate that “cultures differ then not only in their artifacts, but in their languages, subsistence and production systems, and philosophies of life, both implicit and explicit” (p. 1). Scholars highlight how subjective cultures are embedded and represented in narratives and stories and suggest paying attention to language and its use in cross-cultural communications (Lee, Tsang, Bogo, Wilson, et al., 2018b; Lee et al., 2019). Therefore, culture is subjective, complex, dynamic, and representative of a multifaceted experience encompassing individuals, languages, and larger systems. The subjective account of culture suggests subjective and internalized meaning-making derived from “a broader and more inclusive understanding of culture, cultural variables, and cultural differences,” (La Roche, 2013, p. 67) including not only racial/ethnic differences but also many other socially constructed identities, such as gender, sexual orientation, class, religion, language, age, and dis/ability.
Psychotherapy has been a widely used modality of treating human distress. Draguns (1975) articulates that psychotherapy is “always a procedure that is sociocultural in its ends and interpersonal in its means: it occurs between two or more individuals, and is embedded in a broader, less visible, but no less real cultural context of shared social learning, store of meanings, symbols and implicit assumptions concerning the nature of social living” (p. 273). It is thus critical to consider a dynamic interaction of the context and the person in psychotherapy. All therapy relationships between clients and therapists can be viewed as “meetings between cultures” and involve “dimensions of cross-cultural communication” (McNiff & Barlow, 2009, p. 103). In this regard, Pedersen’s (1991) earlier claim is aptly accurate that all psychotherapy should be “culture-centered” and the cross-cultural perspective is generic to all psychotherapy. Toward these ends, we note a long history of studying the cultural context of accurate assessment and appropriate interventions in counseling and psychotherapy (see Pedersen et al., 2016). In this paper, we intentionally use cross-cultural psychotherapy to represent the broad construct of culture as aforementioned and to refer to therapy dyads in which cultural differences exist between two systems of culture—the client and the therapist (Maxie et al., 2006). Aims of cross-cultural psychotherapy are “both to heal individuals and to change inhumane systems” (LaRoche, 2013, p. 47) to ameliorate clients’ sufferings, prevent relapse, and empower clients.
To conduct a more up-to-date synthesis of empirically supported cross-cultural psychotherapy research, the present critical review aims to (1) identify salient themes in the empirical cross-cultural psychotherapy literature over the past four decades, (2) critically examine the strengths and limitations of the current state of literature, and (3) propose future directions for research and practice.
Methods
We followed a critical review method as this allows researchers to “take stock” (Grant & Booth, 2009, p. 93) of the state of literature and explore its contribution to the field. The goal of a critical review is not to demonstrate formal methods of search, synthesis, and quality appraisal required in other reviews, such as a systematic review (Grant & Booth, 2009). Instead, a critical review approach seeks to not only identify salient themes relevant to the researched concept but offers “a new interpretation of the existing data” (p. 93). A critical review has a series of steps to follow to systemically retrieve and categorize the existing research under examination (Grant & Booth, 2009). Figure 1 is a summary of the search process and outputs.
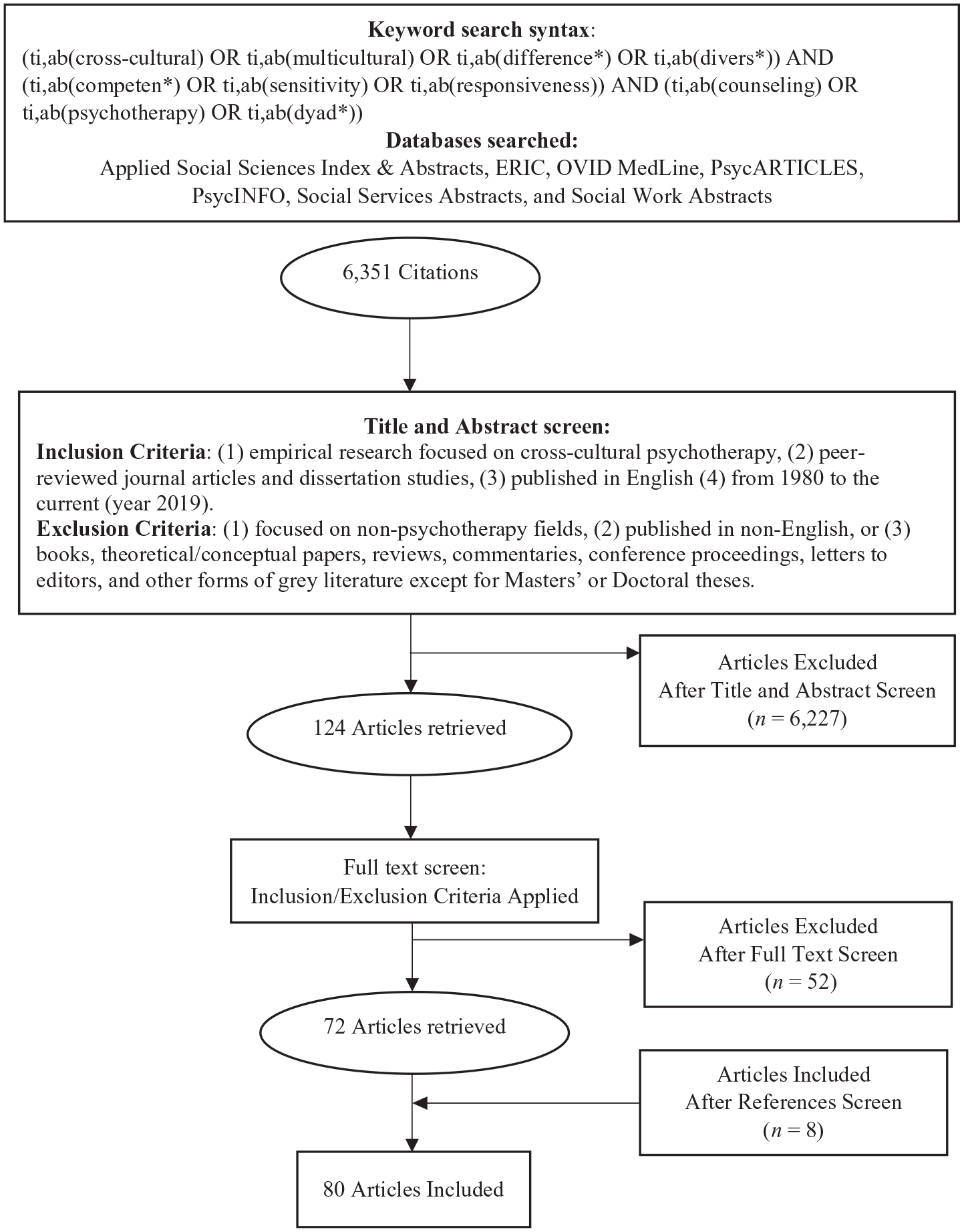
Flow diagram: a search and screen of cross-cultural psychotherapy research studies.
The initial search was conducted from September to December 2019, using the search syntax as follows: (ti,ab(cross-cultural) OR ti,ab(multicultural) OR ti,ab(difference*) OR ti,ab(divers*)) AND (ti,ab(competen*) OR (ti,ab(sensitivity) OR ti,ab(responsiveness)) AND (ti,ab(counseling) OR ti,ab(psychotherapy) OR ti,ab(dyad*)). 1 We used multiple databases—Applied Social Sciences Index & Abstracts, ERIC, OVID MedLine, PsycARTICLES, PsycINFO, Social Services Abstracts, and Social Work Abstracts. These key terms were searched in titles and abstracts. We also limited the inclusion criteria to (1) empirical research focused on cross-cultural psychotherapy, (2) peer-reviewed journal articles and dissertation/master’s thesis studies, (3) published in English (4) from 1980 to the current (year 2019). We chose this period since several monumental scholarly works on multicultural counseling and therapy emerged in the early 1980 (Sue, 1981; Sue et al., 1982). This was a significant turning point promoting a shift from the exclusive research focus on racial/ethnic minority clients to the research focus on cultural differences in therapy dyads. Studies were excluded if they were (1) focused on non-psychotherapy fields (e.g., physician-patient medical appointments), (2) published in non-English, or (3) books, theoretical/conceptual papers, reviews, commentaries, conference proceedings, letters to editors, and other forms of gray literature except for theses research.
The search retrieved 6,351 articles. The second and third authors conducted the title and abstract search using the in/exclusion criteria, resulting in 124 studies retrieved. The second author conducted the full-text review of these studies given the in/exclusion criteria. Throughout the screening process, the first author cross-checked to validate the accuracy. They came to consensus that 72 studies met our inclusion criteria. By checking the references of the 72 studies, we identified eight additional articles that met the inclusion criteria, resulting in a total of 80 empirical studies on cross-cultural psychotherapy published in the past four decades. Finally, a critical analysis involved identification of key information from each article according to research aims (i.e., main themes, strengths, and limitations). The code development was an iterative process through which the second and third authors reviewed and coded each article and consulted the first author on an ongoing basis. Once all articles were coded, the team met and categorized codes to find emerging themes and related subthemes, and then finalized the main themes to be reported. Key themes of each article were then extracted and critically analyzed and synthesized for their content, research focus, setting, participants, nature of therapy, main findings, and limitations for future research areas.
Results
Of the 80 studies included for this review, 68 are peer-reviewed journal articles, and 12 theses including three master’s theses (Cohen, 2016; Millard, 2017; Suderani, 2016) and nine doctoral dissertations (Asbrand, 2012; Foster, 2013; Goettsche, 2014; Goren, 1992; Kirkland, 2018; Naser, 2018; Okonowsky, 2019; Rasheed, 2011; Su, 2012). Except four studies that conducted a secondary data analysis (Flaskerud, 1986; Howard, 2003; Kozuki & Kennedy, 2004; Shiner et al., 2017), all collected original data. It is also noteworthy that all, except six, analyzed samples of actual therapy participants who were in therapy or recent clients at the time of data collection. The other six studies that did not sample actual therapy participants (Burkard et al., 1999, 2003; LeVine & Franco, 1983; Moleiro et al., 2018; Naser, 2019; Ridley, 1986) used analog methods recruiting volunteers (e.g., undergraduate or graduate students) who participated in a study to watch simulated case materials.
Study Participants: Sociocultural and Demographic Information
While most studies reported participants’ race and ethnicity, some did not note participants’ race and ethnicity but explored other aspects of diversity, such as gender, age, sexual orientation, and social class (Cohen, 2016; Goren, 1992; Millard, 2017; Shiner et al., 2017; Ziguras et al., 2003). Five studies provided rather broad (or very limited) information about participants’ socio-demographics (Kozuki & Kennedy, 2004; Miranda et al., 2003; Moleiro et al., 2018; Ortega & Rosenheck, 2002; Taylor et al., 2006).
Among the 80 studies, 11 studies (13.75%, noted with a superscript of “1” in the reference) included cross-cultural dyads of therapists from racial and ethnic majority groups (e.g., White therapists) and clients from minority groups (e.g., non-White clients). Thirty-one studies (38.75%) included both clients and therapists as research participants rather than including only clients or therapists (noted with a superscript of “2” in the reference). Among them, in only four studies (5%) the therapists recruited for the research were from racial/ethnic minority groups (Crisante & Ng, 2003; Naeem et al., 2010; Okun et al., 2017; Shafi, 1998). Fifteen studies (18.75%) recruited therapists only as participants (noted with a superscript of “3” in the reference), and 18 studies were conducted with clients only (22.5%, noted with a superscript of “4” in the reference). There is one additional study with directors/supervisors only (Howard, 2003). Of the 15 studies with therapists only, only a few included therapists from minority backgrounds: One included therapists of color (Bayne & Branco, 2018), one included foreign-born immigrant therapists (Nino et al., 2015), and one recruited therapists of working class (Millard, 2017). Overall, there were only five studies (6.25%, noted with a superscript of “5” in the reference) exploring therapists who came from racial and ethnic minority status.
Research Sites
Most studies were conducted in the United States (n = 63), eight in Canada (Lee & Bhuyan, 2013; Lee & Horvath, 2013, 2014; Lee, Tsang, Bogo, Johnstone, et al., 2018a; Lee, Tsang, Bogo, Wilson, 2018b; Lee et al., 2019; Suderani, 2016; Tsang et al., 2011), two in the United Kingdom (Farsimadan et al., 2007; Moran & Bunn, 2019), and one study each in Australia (Crisante & Ng, 2003), Austria (Ziguras et al., 2003), Greece (Kastrani et al., 2015), the Netherlands (Knipscheer & Kleber, 2004), Norway (Møllersen et al., 2005), Pakistan (Naeem et al., 2010), and Portugal (Moleiro et al., 2018). Most studies were conducted in outpatient mental health and social service settings, with close to one-third (n = 24, 30%, noted with a superscript of “6” in the reference) being conducted in a university setting.
Research Methods
Of the 80 studies, 45 were quantitative, 27 qualitative, and eight mixed methods (Constantine, 2007; Hsiao et al., 2004; Lee & Horvath, 2014; Moleiro et al., 2018; Naeem et al., 2010; Naser, 2018; Paris et al., 2005; Tsang et al., 2011). We found various rigorous research methods from randomized controlled trials (Dansereau et al., 1996; Kanter et al., 2010; Kaslow et al., 2010; Miranda et al., 2003; Ngo et al., 2009; Wintersteen et al., 2005), to experimental (Burkard et al., 2003; Kim et al., 2002, 2003; LeVine & Franco, 1983; Li & Kim, 2004; McCullough et al., 1997; Ridley, 1986; Wade & Bernstein, 1991; Wong et al., 2007), quasi-experimental (Chinman et al., 2000; Crisante & Ng, 2003; Dillon et al., 2016; Evans et al., 1984; Farsimadan et al., 2007; Kim et al., 2005, 2009; Møllersen et al., 2005; Okonowsky, 2019; Yamamto et al., 1984; Zane et al., 1994; Ziguras et al., 2003) and non-experimental studies (n = 18, noted with a superscript of “7” in the reference) in the quantitative studies.
Various qualitative studies include thematic analysis (Cohen, 2016; Millard, 2017; Moran & Bunn, 2019; Nino et al., 2015; Okun et al., 2017), Interpretive Phenomenological Approach (Foster, 2014; Goettsche, 2014; Kastrani et al., 2015), Consensual Qualitative Research (CQR, Burkard et al., 2006; Knox et al., 2003), Case Study (Kozuki & Kennedy, 2004; Lau et al., 2010; Shafi, 1998), Grounded Theory (Suderani, 2016; Thompson et al., 2012, 2015), Phenomenology (Asbrand, 2012; Bayne & Branco, 2018), Phenomenology and CQR (Chang & Berk, 2009), Hermeneutic Phenomenological Approach (Kirkland, 2018), Critical Discourse Analysis (CDA) in Case Study (Lee, Tsang, Bogo, Johnstone, et al., 2018a; Lee, Tsang, Bogo, Wilson, 2018b; Lee et al., 2019), Conversation Analysis (CA, Lee & Horvath, 2013), CDA and CA (Lee & Bhuyan, 2013), Critical Ethnography (Su, 2012), and Narrative Analysis (Taylor et al., 2006).
Our critical review yielded three primary themes for our study focus: (1) therapists’ cultural competencies (n = 46); (2) therapy process in cross-cultural dyads (n = 22); and (3) cross-cultural differences in gender, sexual orientation, or social class (n = 12). These themes and their related sub-themes are summarized in Figure 2.
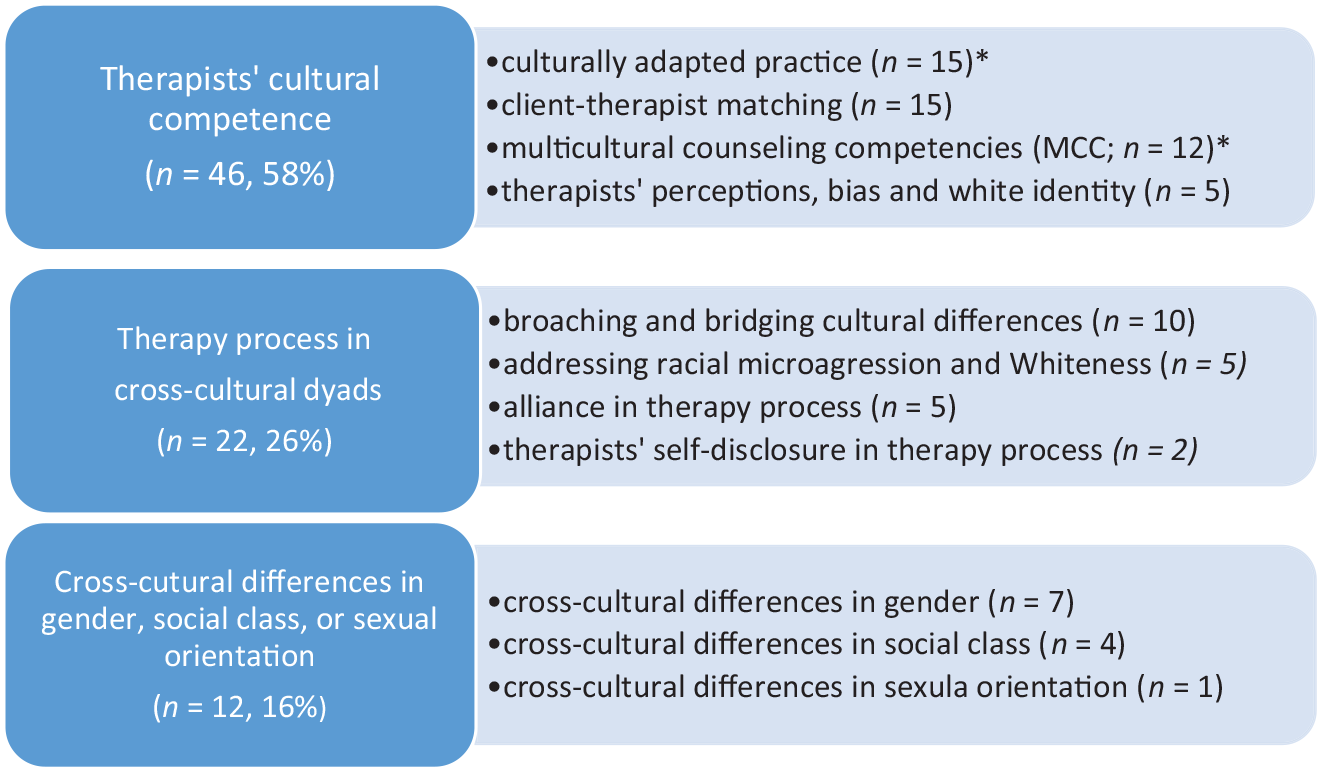
Main themes and sub-themes in cross-cultural psychotherapy research studies (N = 80).
Theme 1. Therapists’ Cultural Competence
A total of 46 studies focused on therapists’ cultural competence, including four subthemes: culturally adapted practice (n = 15), client-therapist matching (n = 15), multicultural counseling competencies (MCC) (n = 12), and therapists’ perceptions, bias, and White identity (n = 5). One study (Kim et al., 2002) addressed two subthemes of culturally adapted practice and MCC, thus counted once in the total.
Subtheme 1-1. Culturally adapted practice
Fifteen studies examined various ways to adapt general psychotherapy approaches to meet clients’ cultural needs. Two types of adaptation were reported: The first type centered on culturally adapting therapists’ communication style or therapy contents (Dansereau et al., 1996; Hsiao et al., 2004; Jackson-Gilfort et al., 2001; Kaslow et al., 2010; Kim et al., 2002, 2003; Li & Kim, 2004; Moran & Bunn, 2019; Ngo et al., 2009; Wong et al., 2007). For instance, Dansereau et al. (1996) used an assessment tool that visualizes client concerns (e.g., mapping out thoughts, actions, and feelings and showing their relationships) in an effort to promote a “common language” (p. 363). The study found that this approach reduced communication barriers between counselors and clients and increased positive outcomes in a substance use treatment program. Other studies found that therapists using directive (Li & Kim, 2004; Wong et al., 2007), immediate problem-solving (Kim et al., 2002), or structured (Hsiao et al., 2004) approaches were rated stronger in alliance and preferred by Asian American participants. Others also explored culturally related specific themes that enhance or interfere with therapy engagement with African American youth (Jackson-Gilfort et al., 2001) or in psychotherapeutic weight loss groups (Moran & Bunn, 2019). Compared to non-culturally adapted treatments, two studies found culturally adapted approaches with better outcomes in addressing depression with African American women (Kaslow et al., 2010) or ethnic minority youth (Ngo et al., 2009). Cultural adaptation included training staff on cultural sensitivity issues, tailoring examples used in programs to be culturally relevant, using clients’ language when possible, and providing cultural consultation to meet with cultural values of each client and family (Ngo et al., 2009). Kim et al. (2003) studied the effect of therapists’ self-disclosure on the therapy outcomes and found that using “different types” of European-American therapist disclosures impacted East Asian American clients’ satisfaction with the therapy: “disclosures of strategies” were beneficial to the clients closely adhering to Asian cultural values when compared with “disclosures of approval, facts or feeling” (p. 324).
The second type of culturally adapted practice aimed at adapting the intervention elements of conventional therapy models to be culturally attuned (Crisante & Ng, 2003; Kanter et al., 2010; Lau et al., 2010; Miranda et al., 2003; Naeem et al., 2010). For instance, two studies described culturally adapted Triple P (Positive Parenting Program) (Crisante & Ng, 2003) and Incredible Years (Lau et al., 2010) for Chinese parents. Kanter et al. (2010) examined the culturally and linguistically adapted Behavioral Activation therapy for Latino clients and found positive treatment outcomes and enhanced retention, compared to non-culturally adapted treatment. Integrating Urdu equivalents of CBT language and folk stories and examples of the life of the Prophet Muhammad and Quran, Naeem et al. (2010) examined a culturally sensitive CBT program for depression in Pakistan, and found improvements on measures of depression, anxiety, as well as somatic symptoms. Miranda et al. (2003) supplemented CBT therapy with case management (e.g., telephone outreach, addressing housing, employment) provided by bilingual and bicultural social workers for ethnically diverse and impoverished clients with depression and found a decrease in both mental health symptoms and program dropout rates for particularly Spanish-speaking patients.
Subtheme 1-2. Client-therapist matching
Fifteen empirical studies have focused on understanding the role of the client-therapist cultural matching in cross-cultural practice. Both benefits and challenges of matching clinical dyads were found. First, four studies found little support for client-therapist racial and ethnic matching (Chinman et al., 2000; Knipscheer & Kleber, 2004; Ortega & Rosenheck, 2002; Shafi, 1998). For instance, two studies on big data with African American and White (Chinman et al., 2000; N = 1,790) or Hispanic and White (Ortega & Rosenheck, 2002; N = 5,795) found no evidence to support racial or ethnic matching. The other two studies found that therapists’ competence, empathy, warmth, genuineness and/or compassion were much more valued than racial and ethnic matching among Turkish and Moroccan clients (Knipscheer & Kleber, 2004) and Muslim Asian female clients (Shafi, 1998).
On the contrary, five studies reported positive effects of racial and/or ethnic matching on therapy outcomes with Arab American college students (Naser, 2019) and Hispanic clients (Paris et al., 2005) in the U.S., as well as various racial/ethnic clients in Australia (Ziguras et al., 2003), the U.K (Farsimadan et al., 2007) and the U.S. (Flaskerud, 1986). Among them, two studies also included language matching (Flaskerud, 1986; Paris et al., 2005). Both Flaskerud (1986) and Farsimadan et al. (2007) noted that clients in matched dyads had initially expressed a preference for racial or language matching which facilitated stronger alliance building and better outcomes. These studies highlighted the effects of the clients’ self-determination around the matching preference on the resulting positive experience of these clients.
Six other studies examined other cultural factors used for client-therapist matching. Kim et al. (2002, 2005, 2009) found that Asian-American clients paired with European American therapists and matched specifically on worldview around the source of the client’s problem reported strong working alliance and successful therapeutic outcomes. Wintersteen et al. (2005) found that gender-matched client-therapist dyads (N = 600) in cannabis youth treatment sites in the U.S. reported higher alliance and retention rates, and found that racial mismatching negatively affected client retention rates particularly for White and person-of-color dyads. In Yeh et al.’s (1994) study with children and adolescents (N = 4,616), matching clients with culturally similar therapists led to better service outcomes in adolescent participants. While both ethnic and language matches were not found to predict outcome variables for children, ethnic matching was found to be a significant predictor of lower dropout rates in adolescents in outpatient mental health services. In addition, ethnic minority adolescents were more positively impacted by ethnic matching. Møllersen et al. (2005) explored therapy approaches between client-therapist dyads matched on Sami backgrounds and dyads not matched on Sami backgrounds (N = 359) and found the positive alliance rating in the matched pairs.
Subtheme 1-3. Multicultural counseling competencies
Multicultural counseling competencies (MCC; Sue et al., 1982) refer to a counselor’s: (1) attitude and beliefs—self-awareness of one’s own values, assumptions, biases, and privileges; (2) knowledge—understanding the worldview of culturally diverse clients; and (3) skills—developing appropriate intervention strategies and techniques in cross-cultural practice. Tao et al.’s (2015) recent meta-analysis identified a strong association between client perceptions of therapist MCC and therapy processes (i.e., working alliance, client satisfaction, general counseling competence and session impact) and outcomes (i.e., symptom reductions). However, our review revealed mixed findings regarding the relationship between MCC and therapeutic process and outcomes in the seven studies. Specifically, some studies found a positive relationship (Anderson, et al., 2019; Fuertes et al., 2006; Middleton et al., 2005; Owen, Tao, et al., 2011a; Rasheed, 2011), whereas others reported little association between MCC and therapy success (Dillon et al., 2016; Owen, Leach, et al., 2011b).
A closer look at these studies revealed more complexities in the effects of MCC on therapy outcomes and processes. For example, Anderson et al. (2019) noted that therapists’ lower MCC was associated with a higher risk of premature termination of therapy among women of color and sexual minorities. However, when all clients’ social identity-related diversity factors were adjusted, MCC was not significantly associated with premature termination. Similarly, Middleton et al. (2005) found that “developmentally mature” (p. 444) White racial identity among European-American mental health practitioners (N = 412) was positively correlated with their self-reports of MCC. Also, a strong association between client-rated MCC and alliance was found in a few studies (Fuertes et al., 2006; Owen, Tao, et al., 2011a; Rasheed, 2011). On the contrary, Owen, Leach, et al. (2011b) found that clients’ and therapists’ racial and ethnic identities were not significantly related to clients’ rating of their therapists’ MCC. Similarly, Dillon et al. (2016) found a lack of correlation between improved well-being in clients and clients’ rating of their therapists’ MCC.
Other factors related to MCC have been studied in an effort to foster cultural competence, by assessing the impact of a therapist cultural orientation or sensitivity training program (Evans et al., 1984; Wade & Bernstein, 1991; Yamamoto et al., 1984) or examining other conceptual (Taylor et al., 2006) or contextual (Howard, 2003) components of MCC. For example, studies on the therapist cultural trainings found their positive impacts on racialized clients’ view on therapy and therapist competence (Evans et al., 1984; Wade & Bernstein, 1991; Yamamoto et al., 1984). Taylor et al. (2006) conducted in-depth interviews with nine therapists working with Latino families to examine how therapists from various cultural and ethnic backgrounds working with Latino American families constructed the idea of cultural competence and found five themes: (1) the use of language in therapy, (2) the impact of social class, (3) gender and power on the therapeutic relationship, (4) immigration and culture clash, and (5) Latino construction of family boundary. Howard (2003) found that substance-abuse treatment centers located in African American communities have higher rates of MCC workers due to organizational, funding, staffing and client factors.
Subtheme 1-4. Therapists’ perceptions, bias, and White identity
Five studies explored if and how therapists’ perceptions and bias against clients of color compromise therapists’ capacity to provide culturally competent services. For example, Ridley (1986) explored Black and White American male therapists’ (N = 40) ratings of their clients based on status of race (Black or White) and degree of client self-disclosure (i.e., explicit statements of feelings). Ridley (1986) found that a higher-disclosing client was rated more favorably by therapists of both racial identities. Interestingly, therapists rated a low-disclosing Black client more favorably than a White low-disclosing client. In addition, Black therapists rated White clients higher on depression scales with the same finding for White therapists and Black clients. In delivering culturally sensitive mental health services to 85 clients, Zane et al. (1994) found significantly poorer treatment outcomes for Asian-American clients than for White clients. Asian-American clients self-reported lower satisfaction across all measures and reported higher rates of depression, hostility, and anxiety after treatment. One other important finding in this study is that therapists (N = 34) rated Asian-American clients as having lower psychosocial functioning than White clients at the end of treatment and rated these clients as less suitable for therapy after one session. This raises serious concerns around therapists’ predetermined attitudes that may exist within the cross-cultural dyad prior to beginning treatment as well as the need for culturally responsive processes within treatment. Also, Burkard et al. (1999, 2003) explored the impact of therapist’s White racial identity on the working alliance with same-race and/or cross-racial clients and found race to have a significant association with alliance in both dyads. They concluded that White racial identity of the therapist was associated with the working alliance regardless of the race of the client. Okonowsky (2019) also explored the relationship among White American counseling trainees’ (N = 226) perspectives of racism as a zero-sum game (i.e., one group’s gain is another group’s loss), political ideology affiliation (i.e., liberalism or conservatism), and completion of multicultural counseling course, and found that those having completed the course had the lowest zero-sum belief, whereas there was a significant correlation between conservative political ideology affiliation and a high degree of zero-sum belief.
Theme 2. Therapy Process in Cross-Cultural Dyads
Twenty-two studies in this review primarily focused on providing analytical attention to the therapeutic process of negotiating differences within cross-cultural dyads and less on the relationship between therapists’ cultural competence and client outcomes. These studies were focused on a range of issues within the therapy process, including broaching and bridging cultural differences (n = 10), addressing racial microaggression and Whiteness (n = 5), alliance in therapy process (n = 5), and impacts of therapists’ self-disclosure on therapy process (n = 2).
Subtheme 2-1. Broaching and bridging cultural differences
Ten studies examined how cultural differences were addressed in cross-cultural dyads (Asbrand, 2012; Bayne & Branco, 2017; Chang & Berk, 2009; Knox et al., 2003; Kozuki & Kennedy, 2004; Lee et al., 2019; Maxie et al., 2006; Moleiro et al., 2018; Okun et al., 2017; Su, 2012). Bayne and Branco (2017) explored the experiences of eight counselors of color broaching cultural dialog with clients. Broaching is defined as “the practice of directly addressing racial and cultural factors within the counseling relationship” (p. 75). Participants reported positive impacts of broaching, such as increasing the client’s level of comfort and allowing space for discussions around systemic issues that may impact the client. Knox et al. (2003) also found that African American therapists reported regularly addressing race with clients of color whereas European American therapists reported addressing race only when clients initiated this discussion. However, both groups of participants reported positive implications from broaching race in therapy discussions. In a survey with 689 American Psychological Association-licensed therapists, Maxie et al. (2006) found that although most participants (85%) reported having discussions with their clients about differences, less than half (43%) did so in cross-racial/ethnic clinical encounters. In Moleiro et al.’s (2018) study, 31 therapists watched video-taped cases with various marginalized groups of clients, diverse in race, migration history, sexual orientation, and religion. They were interviewed about their case conceptualization and how they would integrate diversity in therapy. A thematic content analysis of these interviews illustrates that 70.5% content units were either not mentioning diversity issues at all in case conceptualization or explicitly noting that “the perceived diversity would make no difference” (p. 196). Among diversities, issues of religion and migration background were identified by some participants. Other dimensions such as race, sexual orientation, and socio-economic status were invisible in case conceptualization, and dominant group clients (i.e., White, heterosexual, Christian) were rarely perceived as cultural.
Lee et al. (2019) focused on how therapy goals and tasks become a site to negotiate cultural differences in a therapy dyad. The authors demonstrated discursive patterns of incompatibility between therapy goals and tasks due to a White therapist enacting her own cultural values leading to essentializing the racially different client’s culture. Goals and tasks became compatible when the therapist closely follows the client’s talk and cultural values. Analyzing videotaped sessions in intra- or inter-racial dyads in a hospital clinic (N = 44), Okun et al. (2017) found that non-Latino White clients paired with therapists of color made efforts to bridge differences between them through strategies of joining against a third party (e.g., you/therapist understand me/client but not my families/third party) and describing their socioeconomic difficulties (e.g., I/client cannot afford things, thus being marginalized like you/therapist of color). They, however, were more likely to call into question their therapist’s qualifications (e.g., did you have a Ph.D.?), compared with clients matched with non-Latino White therapists. Therapists of color were found to make more self-disclosures and were found to present themselves more formally than their non-Latino White peers. This formality was interpreted as overcompensation to maintain professional stance being used in reaction to potential racism from White clients. Su (2012) analyzed transcripts of 12 sessions between a White therapist and a Korean international student in the U.S. and found that the seemingly smooth therapy process around different problem-solving approaches was shaped by the client’s desires to learn from the therapist’s American ways of coping with issues and the therapist’s tacit agreement on the client’s stance as a good foreigner. Su argued that, despite a good alliance, this dynamic compromised their discussion on cultural issues and diverted them from broaching and confronting differences in their perspectives.
Chang and Berk (2009) interviewed racial minority clients satisfied or dissatisfied with therapy and discussed both universal and culturally specific aspects of therapeutic relationship building. Efforts made by both the client and the therapist to bridge differences in the therapy process were considered as an important factor contributing to the building of therapeutic alliance. The study also revealed the importance of therapists’ competence in identifying and addressing clients’ core needs, as well as therapists’ attentive attitudes, responsiveness and ability to address ruptures, proper use of self-disclosure, taking a directive approach and providing guidance, and having culture-specific knowledge and attending to how race shapes the client’s experience. Kozuki and Kennedy (2004) examined the impact of White therapists applying Western interventions of psychodynamic therapy when working with Japanese clients in the U.S. Findings indicated that (1) therapists’ cultural stereotypes (i.e., associating clients’ western cultural assimilation with healthy adaptation) negatively impacted therapy; (2) therapists did not validate the cultural interpretations of clients (i.e., concepts of “death” and “dying”); and (3) western therapist pathologized clients’ characteristics that were unfamiliar to them and their culturally ignorant and often harmful practices were unrecognized.
Subtheme 2-2. Addressing racial microaggression and Whiteness in therapy
Four studies discussed client experiences of microaggressions perpetrated by therapists in the process of therapy (Constantine, 2007; Foster, 2014; Lee, Tsang, Bogo, Johnstone, et al., 2018a; Owen et al., 2014). Sue et al. (2007) defined racial microaggression as “brief and commonplace daily verbal, behavioral, or environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative racial slights and insults toward people of color” (p. 271). In Foster’s (2014) study with 13 clients of color in the U.S., all participants reported having experienced racial microaggressions in therapy and this experience negatively impacted their therapy experiences and often led to early therapy termination. In Owen et al.’s (2014) study with racial and ethnic minority clients (N = 120) from an American university counseling center, approximately 53% of the participants had experienced microaggression in therapy, and 76% of the participants reported that microaggressions were not discussed in therapy. In Constantine’s (2007) study with 24 African American clients, experiencing racial microaggression resulted in not only poor therapeutic alliance with White therapists (n = 19) but also low counseling satisfaction. Lee, Tsang, Bogo, Johnstone, et al. (2018a) analyzed audio- and/or video-taped therapy sessions conducted in community mental health clinics where race and culture issues were conversed in eight cross-racial dyads. Their findings demonstrated the pervasiveness of racial microaggression in therapy and illustrated six dominant themes related to racial microaggression: alienating in own land, color blindness, the myth of meritocracy, denial of individual racism, the ascription of intelligence and knowledge, and second class/less-worthy clients. Finally, Lee and Bhuyan (2013) analyzed therapeutic dyads and reported discursive strategies used by both White therapists and clients of color to negotiate Whiteness within the encounter. The study revealed how therapists normalized Whiteness when clients shared cultural practices.
Subtheme 2-3. Alliance in therapy process
To identify dialogical strategies of joining, engaging, and building alliance in cross-cultural dyads, Lee, Tsang, Bogo, Wilson, et al. (2018b) conducted a discourse analysis of family therapy with a Pakistani mother-daughter dyad with a White female therapist in Canada. They identified discursive interactions of both tracking and non-tracking of clients’ verbalization of cultural content in cross-cultural dialog and found that the therapist’s enactment of her own assumptions of the family culture resulted in missing opportunities to engage with the family. A lack of engagement around cultural content was also identified by Lee and Horvath (2014). Through audio and/or video-taped sessions, they identified abrupt changes in session focus by the White therapist when culturally relevant dialog occurred with racially different clients, although the same therapist was appropriately responded to them in non-cultural clinically important contents. Lee and Horvath (2013) also found a similar lack of engagement with clients of color when White therapists missed opportunities to integrate cultural content into clinical dialog, thus injuring the therapeutic alliance and making cross-cultural dialog into the client’s cultural monologue. Tsang et al. (2011) conducted a narrative analysis of clinical processes of first sessions in cross-racial/ethnical dyads (N = 18) and found that positive engagement occurred when therapists explicitly communicated cognitive understanding of the client’s needs, demonstrated emotional attunement to clients, and appropriately responded to clients’ culturally related experiences rather than dismissing them. Through interviews with 13 foreign-born therapists working in the U.S., Nino et al.’s (2016) highlighted the importance of both emotional attunement and human-to-human engagement are crucial in cross-cultural therapy.
Subtheme 2-4. Therapists’ self-disclosure in therapy process
Two studies focused on therapist self-disclosure and how it affects the cross-cultural therapy process. Suderani (2016) found that disclosure occurred sooner and with greater ease when therapists (N = 9) have a shared cultural background and/or common ethnic heritage with their clients. Burkard et al. (2006) also found that White European American therapists (N = 11) typically shared their reactions to clients’ experiences of racism/oppression, and these self-disclosures often improve the therapy relationship and had positive effects in therapy.
Theme 3. Cross-Cultural Differences in Gender, Sexual Orientation, or Social Class
Considering the lens of intersectionality through which multiple forms of social diversity co-exist in therapy relationship, 12 studies focused on differences in gender (n = 7), social class (n = 4), and sexual orientation (n = 1) within the therapy dyad.
Subtheme 3-1. Cross-cultural differences in gender
Two studies explored the relationship between the gender of clients or therapists and alliance. Goren (1992) specifically explored the relationship between client and/or therapist androgynous gender role and working alliance and found no significant difference was found between androgynous and non-androgynous status in terms of working alliance scores. Significant relationships were, however, found between client sex and working alliance; female clients working with female counselors rated the working alliance more positively in comparison to male clients (Goren, 1992). This “female effect” was also found in Bhati (2014, p. 565), wherein female clients matched with female therapists reported alliance ratings higher than dyads with a male therapist.
McCullough et al. (1997) explored the relationship between gender and religiosity in therapy. Participants (N = 239) who self-identified as Christian viewed videotapes of either male or female therapists interacting with male or female clients around religious issues. Findings also revealed that female therapists were viewed as more religious and effective than males, and that the level of perceived religiosity mediated the perceived association of therapists’ gender and treatment interventions (either supportive or challenging). In other words, a therapist’s gender is translated into perceptions of their competence and female therapists who were perceived as more religious were rated more competent even to challenge clients’ religious beliefs than less religious male therapists.
Shiner et al. (2017) explored gender matching for American Veterans with post-traumatic stress disorder (N = 506,471) and its association with therapy retention. They found that all clients seeing a female therapist had higher retention rates than the female client-female therapist matched dyads, whereas male-male dyads had the lowest rates. However, when other factors (i.e., age, disability, war-related data, and history of abuse) were included in the analysis, gender no longer presented as a significant predictor of retention. LeVine and Franco’s (1983) study with 811 simulated clients (all college sophomores) found that a therapist’s gender, ethnicity, and verbal style were associated with a client’s interest in seeking therapy. They found that Anglo-American males and females as well as Mexican American females were more likely to indicate interest in therapy when male therapists employed a directive verbal style, whereas Mexican American females showed interest regardless of Anglo-American female therapists’ directive or nondirective approach, as opposed to being neutral.
Kastrani et al. (2015) examined Greek female client experiences (N = 27) of gender within the therapeutic relationship and reported that some female clients indicated their therapist’s female gender as being among the most important factors of the relationship since similarities in thinking and experiences (i.e., child rearing) benefited the relationship particularly around developing trust and facilitating self-disclosure. However, preference for a male counselor was also identified as beneficial by some participants who sought a male perspective on their concerns or wanted to engage with their perspective of how a male operates. Kirkland (2018) explored the lived experience of seven therapists with gender diverse clients and found that therapists’ training on gender diversity issues may improve the lives of their gender diverse clients by reducing transprejudice, transphobia, and other forms of bias.
Subtheme 3-2. Cross-cultural differences in social class
Four studies have considered the role of social class in therapy, and all demonstrated that classism exists and can be identified within therapeutic processes. For example, Millard (2017) interviewed twelve self-identified working-class therapists and explored their experiences of how classism impacts therapeutic alliance. They found that all participants reported having experienced feeling of being alienated and silenced due to the lack of systemic attention to classism. Given this, finding the author urged class conscious practice to be attended to as a significant aspect of cross-cultural competence. Thompson et al. (2012) explored the therapeutic experiences of 16 clients identifying as low-income and found more or less positive experiences when therapists acknowledged or dismissed therapist-client differences in social class. Participants benefited when therapists initiated such social class related dialog as this demonstrated genuine interest and understanding of clients’ needs. Thompson et al. (2015) also found that therapists working with low-income clients faced difficulties discussing income-related topics in practice. They also noted countertransference with clients about their own economic status and acknowledged subsequent feelings of judgment and biases in their work with clients. In exploring the topic of broaching social class in therapy with 12 therapists, Cohen (2016) found that therapists tended to acknowledge issues of social class with clients more often when the client’s social class was perceived to be lower than the therapist and to discuss less about class issues when clients were perceived as being in a higher class. When social class was discussed within the dyad, Cohen found that it is often clients, rather than therapists, who initiated such discussion, and that clinicians typically focused only on the clients’ status.
Subtheme 3-3. Cross-cultural differences in sexual orientation
Goettsche (2015) described perspectives of seven clients, engaged in similarly matched dyads around sexual orientation and those in unmatched dyads, and noted the importance of therapist self-reflection, ability to discuss sexuality, and acknowledge clinical ruptures. They also found the significance of affirmative therapeutic work regardless of the therapist’s sexual orientation and the sexual minority clients’ perception of having benefited from the experience of acceptance from therapists in dominant sexual identity.
Discussion
A critical review does not demonstrate the systematicity of other literature reviews (e.g., a systematic review), thus does not require a formal quality assessment of included studies. Its findings are interpretive and open for “further evaluation, not an endpoint in itself” (Grant & Booth, 2009, p. 97). The current critical review thus provides a renewed understanding of cross-cultural psychotherapy, with the hope that this interpretation yields further inquiries. The current review has several notable contributions to cross-cultural psychotherapy: (1) highlighting the current state of empirical research on cross-cultural psychotherapy using a variety of methods and published in the past 40 years (1980-2019); (2) identifying various cultural compositions of client-therapist dyads that have been studied; (3) giving analytical attention to therapy process factors and micro-analysis of cross-cultural communications, which may sensitize therapists in their interactions with diverse clients in everyday practice; and (4) broadening the construct of culture by raising attention to additional dimensions of culture, such as gender, sexual orientation, or social class, in addition to race and ethnicity.
Overall, research on cultural competence was the most dominant theme identified within the included studies. All studies on cultural competence exclusively focused on racial and ethnic minority clients when examining the impact of therapy approaches. There has been a criticism about how culturally competent therapy (i.e., exclusively focuses on racial and ethnic minority clients and positions therapists in a blank screen) further otherizes racial and ethnic minority clients and reifies Euro-centric notions of psychotherapy (Lee, 2010). In our review, most of the studies attempted to clarify details of demographic information with some variations in its detail except five studies (Cohen, 2016; Goren, 1992; Millard, 2017; Shiner et al., 2017; Ziguras et al., 2003). Although the focus of these studies is on gender, sexual orientation, or class, it also raises some concerns around how culture is conceptualized: understanding gender role in therapy dyads should not be separated from each therapy participant’s cultural values and contexts. Some studies discussed racial and ethnic descriptions of their clients while exploring studies on gender and low income (Wintersteen et al., 2005; Evans et al., 1984; Okun et al., 2017). However, other than using diversity as descriptors of participants, there is little examination of how diversity factors interact with one another and their impact on cross-cultural encounters.
For therapists’ demographic information, some studies expanded on descriptors including the level of clinical training, years of practice experience, exposure to multicultural training, and experiences of working with culturally diverse clients. Paying attention to these therapist factors is promising given the psychotherapy research finding that the therapist factor explains variances in outcomes even in a manualized treatment (Beutler et al., 2016). Also, it highlights that therapist factors are more nuanced than their race, ethnicity, and gender in cross-cultural psychotherapy. Furthermore, all studies exploring therapist factors, such as therapist bias, perceptions, and White identity in cross-cultural or intra-cultural dyads, found that therapists’ responses to clients differ depending on the client’s ethnic identity (i.e., White versus people of color), highlighting the impacts of the therapists’ preconceived notions/biases/White identity on therapeutic relationship building and treatment outcomes (Burkard et al., 1999, 2003; Ridley, 1986; Zane et al., 1994). These studies certainly contribute to current psychotherapy research by de-centering focus solely on racial and ethnic minority clients and re-centering what therapists contribute to cross-cultural encounters in therapy.
Most studies in our review reported minimal information related to the actual implementation of clinical interventions. While 56 studies (70%) mentioned a particular therapy model, most did not provide information such as the total number of sessions, therapists’ therapeutic orientation, and therapy and contents. Only eight studies (Crisante & Ng, 2003; Dansereau et al., 1996; Li & Kim, 2004; Miranda et al., 2003; Moran & Bunn, 2019; Lee & Horvath, 2014; Lee, Tsang, Bogo, Wilson, et al., 2018b; Naeem et al., 2010) provided somewhat detailed therapy descriptions, mainly culturally adaptive or micro-therapy process studies. There are always content variations when applying any therapy model in any therapy dyad composition. If racially matched dyads have better or worse therapy outcomes compared to their counterparts, it would be critical to see under what therapeutic conditions this outcome is valid. Overall, we found a lack of information on the therapy itself, despite the main inquiry being on (cross-cultural) therapy. We wonder if empirical research in cross-cultural psychotherapy may assume the therapy intervention is static while exclusively focusing on demographic cultural differences that exist in therapy dyads. Cultural adaptation is not monolithic but highly multifaceted and contextual. To inform therapists in practice, it would be critical to explicitly document the nature of therapy in future studies.
Recent reviews highlighted the importance of exploring the therapy process in cross-cultural dyads (Worthington et al., 2007; Tao et al., 2018). In our review, we observed increased research on the theme of therapy process in cross-cultural dyads. Specifically, of the 22 studies focused on different therapy process factors in cross-cultural dyads, the majority (71.4%, n = 15) were published after 2010. Untangling complexities among various process factors in cross-cultural dyads, these studies focus on multiple cultural differences that exist between clients and therapists. Some studies focused on process dynamics of White therapists and racial and ethnic minority clients (Burkard et al., 2006; Change & Berk, 2009; Lee & Bhuyan, 2013; Lee & Horvath, 2013, 2014), whereas some explored dynamics of the reverse dyads between therapists of color and White clients (Bayne & Branco, 2018; Okun et al., 2017). Others consider both clients and therapists coming from various cultural diversities (Foster, 2014; Knox et al., 2003; Lee, Tsang, Bogo, Johnstone, et al., 2018a).
In terms of cultural differences residing within therapy dyads, 12.5% of the reviewed studies (n = 10) focused on exploring a process of broaching cultural differences, and others exploring a process of bridging cultural differences. Findings indicated that efforts to bridge, particularly on the part of the therapist, distinguished successful therapy dyads from unsuccessful therapy dyads (e.g., Bayne & Branco, 2017). This demonstrates the critical need to incorporate bridging behaviors into the therapy encounter. In terms of broaching, most studies indicated that not all therapists choose to discuss issues of culture and race with their clients, with several studies noting the negative impacts of racial microaggressions on therapy alliance and outcomes (Foster et al., 2014; Constantine, 2007) yet still little broaching of this experience in therapy (Owen et al., 2014). Further research is needed to examine barriers to broaching within the clinical dyad.
Paying attention to micro-details of cross-cultural encounters in therapy, eight studies of therapy process research utilized audio- and/or video-taped actual therapy sessions (Okun et al., 2017; Lee & Bhuyan, 2013; Lee, Tsang, Bogo, Johnstone, et al., 2018a; Lee, Tsang, Bogo, Wilson, 2018b; Lee et al., 2019; Lee & Horvath, 2013, 2014; Su, 2012). Their findings further demonstrated dynamic processes of cross-cultural interactions. Specifically, these subset studies used naturalistic methods to examine minute-by-minute negotiations within the dyads, allowing for a practical understanding of how culture is negotiated and discussed in cross-cultural clinical encounters that may not be apparent in other forms of research. Instead of focusing on nominal values of race and ethnicity as the parameters of studying cross-cultural competence, these studies pay attention to how differences and similarities are negotiated through a dance of therapy process, which is dynamic, interactive and context-dependent. Using discourse analysis and conversation analysis in process-oriented psychotherapy research may be both methodologically innovative and practically meaningful as these research approaches unveil the complex dynamics of cross-cultural processes.
Our critical review also showed that sexual orientation and class issues were under-conceptualized in studies examining cultural differences in therapy dyads. We found that clients of culturally dominant groups (e.g., heterosexual upper-middle-class men) were rarely perceived as cultural; culture in therapy is positioned as solely linked to the marginalized groups of clients (Moleiro et al., 2018). Despite the importance of clinicians’ self-reflection and capacity to discuss these differences and potential clinical ruptures (Goettsche, 2015), process-oriented psychotherapy research in cross-cultural encounters found that therapists do not often intentionally start conversations with clients about cultural issues (Lee & Horvath, 2013, 2014). For instance, Cohen (2016) found that it is not clinicians but largely clients who initiate conversations about social class and that clinicians typically discuss only the clients’ social class not their own.
Implications for Cross-Cultural Psychotherapy Practice, Training, and Future Research
This review has several implications for practice, training, and research. First, therapists’ self-awareness and critical reflection of their own biases and cultural positions have long been recognized as critical aspects in cross-cultural psychotherapy (Sue et al., 1992). This review revealed that these important tasks of critical reflection are challenging, especially when therapists’ Whiteness and biases are not addressed. Further, not addressing these issues may have detrimental effects on clients, the therapy process, and client outcomes. It is thus critical to continue studying how therapists may engage in critical reflection regularly and identifying approaches that help therapists to mitigate sociocultural biases in their cross-cultural practice.
Second, cultural presentations are subtle and implicitly conveyed, and so it is difficult to illustrate naturally occurring nuanced cultural dynamics and train therapists how to discuss them with clients toward alliance building and achieving therapy goals. Findings from therapy process research provide rich discussion around the complexities of clinical process in cross-cultural dyads. These research examples may work as practice materials to re-script cultural misunderstandings toward repairing alliances in cross-cultural practice and can be used for examples in training therapists, thus closely linking research into practice and education.
Lastly, given the complexities of multiple diversities, clinical dynamics and power are shifting constantly within cross-cultural therapy dyads. With further empirical research on various sources of similarities and differences perceived and experienced by both therapists and clients, we may have more confidence in psychotherapy research being truly cross-cultural.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Royal Bank Fellowship of Canada (PI: Eunjung Lee, Fellow: Andrea Greenblatt).