
Abstract
Indigenous Sámi and Kven minority children in Norway were during the 20th century placed at boarding schools to hasten their adoption of the Norwegian majority language and culture. This is the first population-based study examining health, well-being and disability pension rates among these children. Data stem from two epidemiological studies conducted in 2003/04 (SAMINOR 1) and 2012 (SAMINOR 2) by the Centre for Sami Health Research. The SAMINOR 1 study included N = 13,974 residents (50.1% women, Mage = 52.9 years) and n = 2,125 boarding participants (49.6% women, Mage = 56.2 years). The SAMINOR 2 part included N = 10,512 residents (55.5% women, Mage = 47.6 years) and n = 1246 boarding participants (48.7% women, Mage = 54.1 years). Main outcome measures are mental and general health, well-being and disability pension linearly regressed upon the predictors. We observed minor differences between boarding and non-boarding participants that generally disfavored the former, of which many disappeared after covariate adjustment. Boarding school participants reported more discrimination, violence, unhealthier lifestyle behavior (smoking), less education and household income compared to non-boarding participants. The exceptionally long timeframe between boarding school and the current outcome measures (40–50 years) is a likely reason for the weak associations. The study supports the international literature on health inequalities and highlights the risk of ill health following boarding school placement of indigenous or minority children. On a positive note, participants reporting stronger ethnic belonging (strong Sámi identity) were well protected, and even functioned better in terms of lower disability rates than majority Norwegians.
Keywords
Introduction
There are numerous accounts in papers and book volumes of how the Sámi and Kven children in Norway experienced the enforced placement in boarding schools during the 20th century (Jensen, 1991; Lund, 2005–2013; Meløy, 1980; Minde, 2005). This school policy, which was put into meticulous action from 1905, required an agonizing geographical relocation of a large number of Sámi children obliged to be taught the majority Norwegian language and culture. While some children as adults have voiced stories emphasizing positive aspects of being offered systematic schooling, most stories concern painful separations from their parents and home environments that alienated them both linguistically and culturally. Many stories include accounts of discrimination, as well as emotional, physical or sexual harassment at the boarding schools (Tjelle, 2000). At home, the parents felt deep guilt toward their children, whereas the children felt abandoned by their parents, which shaped an experience of boarding schools as internment camps (Nergård, 2006; Tjelle, 2000). As studies have documented that adverse childhood experiences increase the risk of poorer mental health as adults (Merrick et al., 2017), one may expect that these Sámi children did not go through these experiences mentally unscathed.
A limitation of the existing studies is the exclusive qualitative methodological approach. During the last two decades, the Centre for Sami Health Research in Norway has conducted two epidemiologically designed studies on the health and living conditions of the Sámi people (SAMINOR 1 in 2003/04 and SAMINOR 2 in 2012). These studies included questions about boarding school attendance during the primary and secondary school periods, which provide an interesting retrospective opportunity to connect this information with the registered information about their mental health, well-being, and working capacity in terms of disability pension as adults.
Boarding School and Health, and Potential Mechanisms
Racism and discrimination are risk factors for ill health (Paradies, 2006). Contemporary studies on the Sámi indigenous people converge with such conclusions. Sámi adolescents (Bals et al., 2010) report more discrimination than majority adolescents, and Sámi adults being discriminated report more health problems than majority Norwegians, including cardiovascular diseases, obesity, metabolic syndrome or chronic pain issues (Hansen, 2015; Hansen et al., 2010; Hansen & Sørlie, 2012). Moreover, the Sámi were bullied substantially more often as children than majority Norwegians, which might have taken place at, for example, boarding schools (Hansen et al., 2008, 2016). Studies also report more frequent episodes of interpersonal violence during childhood, with women being particularly exposed (Eriksen et al., 2015). Those exposed, reported more mental distress and posttraumatic symptoms as adults (Eriksen et al., 2018), and more chronic pain (Eriksen et al., 2016). As such incidents may have occurred in school settings, as well as in homes, those with a boarding school history may have been at particular risk given the accumulation of ethnic- and school-related strains in these environments.
International studies examining the health implications of boarding schools portray a rather negative relationship between boarding school and various health conditions (Running Bear et al., 2019). For example, an Australian panel study observed a pronounced increase in anxiety and perceived stress during the schooling period, as compared to non-boarding students (Mander & Lester, 2017). Comparably, a Chinese study observed a higher tendency for depressive self-blaming and psychosomatic symptoms (Ma et al., 2013), a German study recorded an earlier debut and more frequent use of alcohol (Pfeiffer & Pinquart, 2017), and a Turkish study showed poorer self-rated health despite the fact that boarding students dined more regularly and were more normal-weighted as compared to non-boarding students (Kucuk & Gunay, 2016). In a review including 61 studies on the health and well-being of indigenous peoples having a residential school history in Canada, most of them being First Nations, confirmed the negative health effects of residential schooling, mainly through poorer self-rated health, more chronic diseases, less mental and emotional well-being, as well as addiction and substance abuse and suicidality (Wilk et al., 2017). A later study of American Indians by Running Bear et al. (2018), showed that punishment for speaking their native language and prohibition of practicing their culture were independently associated with poorer physical health in adulthood (Running Bear et al., 2018). A Norwegian study including 200 children of Norwegian missionaries who attended boarding schools in foreign countries during the latter half of the 20th century, reported limited emotional support, encouragement, and physical contact at the boarding schools (Bergås, 2008). In addition, about one-fourth reported neglect of care or abusive experiences. These findings mimic the boarding school experiences as told by the Sámi people in the qualitative studies (Jensen, 1991; Lund, 2005–2013; Meløy, 1980; Minde, 2005).
Some boarding school studies do report small or non-existent differences with regard to health habits, well-being, motivation and engagement (e.g., Agmon et al., 2015; Martin et al., 2014), but such studies are fewer. These between-study differences may relate to distinct contextual factors coming into play due to dissimilar objectives of the boarding school policy. As the Norwegian national ambition was to suppress Sámi and Kven languages and cultures, the policy was clearly negative and suppressive of cultural pride, whereas the policy in some other nations, as the English boarding school system aiming at gentrification of the privileged Victorian middle class (Duffel, 2000), had a quite opposite objective. Given the extant literature portraying a rather negative relationship between boarding school and health in countries with a somewhat comparable ethnic historical background as in Norway (e.g., First Nation people in Canada and American Indian), we expected similar negative health outcomes in the present study.
Prolonged separation from the family due to placement at boarding schools has been noted as a risk factor for permanently disrupting the bond between the child and the parent (Torres De Leon, 2020). The attachment and separation-individuation theories by Bowlby (1969, 1980) and Mahler (1974) may provide a framework for understanding the developmental challenges of children attending boarding schools. According to Bowlby, a secure attachment to an adult figure is a premise for children to confidently explore the environment, playing with others, and developing social competence. Inconsistent parenting may, on the other hand, form an insecure or anxious attachment to the caregiver. The attachment formation is a gradual process in which the early or preschool years dominates in importance (Bowlby, 1969; Fraley & Heffernan, 2013), yet highly stressful or traumatic events during school age may shift the attachment process into a more negative direction (Fraley & Heffernan, 2013). As the forced separation of Sámi children from their parents and local communities has indeed been described as highly stressful and traumatic for some children, securely attached children may have been prone to shift into more inhibited or insecure directions. Attachment problems may also have been cumulative as the separation from and reunion with their parents implied a continuous recycling between disconnection, mourning and reattachment. Moreover, the secondary attachment figures at the boarding schools could be unstable, neglectful and in some instances even abusive.
The separation-individuation theory Mahler (1974) proposes some requirements for children to develop an independent and stable self. A healthy separation and individuation process fosters emotional independence (the child manages well without an exaggerated degree of parental approval, agreement, closeness or emotional support) and conflictual independence (manages well without exaggerated feelings of guilt, anxiety, lack of trust, resentment or anger toward the parents). A more secure parental attachment is associated with more conflictual independence (i.e., fewer conflicting and ambivalent feelings toward the parent), which seems to reinforce educational perseverance in children (Wilchek-Aviad, 2005). Because placement at boarding schools also implies a physical separation from the parents, the emotional individuation process may be hastened at too young an age (Wilchek-Aviad, 2005) and form a pseudo emotional independence. Disruptions of normal attachment processes, which placement at boarding schools may cause, may for that reason negatively influence identity formation and consolidation, that ultimately spells out as problems in later life in terms of poorer health, well-being, work engagement and performance.
Historical Background for the Establishment and Practice of Boarding Schools in Northern Norway
The Sámi people have a long and continuous history as inhabitants of the Arctic areas that include parts of contemporary Norway, Sweden, Finland and the Kola Peninsula of Russia. As circumpolar people, the Sámi have evolved their own language (belonging to the Finno-Ugric branch of the Uralic language family), which represents a strong identity marker of their cultural inheritance (Pedersen, 2016). By law of 1739, school became compulsory (Jensen, 2005). It was organized as ambulatory schools (“omgangsskole”) where teachers traveled between communities and provided about twelve weeks of schooling a year. Teaching was held in the Danish language, which is very similar to the Norwegian language. In the beginning, the use of mother tongue teaching and adaptation of some learning material into Sámi language was accepted by the school ministry (Jensen, 2015). As time passed, the official policy of using Sámi and Kven language to support teaching became gradually less accepted (Jensen, 2015) until it was banned late in the 19th century when the policy of assimilation of the Sámi and the Kven minority (immigrants from northern Finland and Sweden) became official. In 1905, Norway became an independent nation after more than 500 years of union, first with Denmark (1380–1814) followed by Sweden (1814–1905). In the coming 50 years, more than 50 boarding schools for Sámi and Kven children were established in the northernmost county (Finnmark) in order to speed up their cultural transformation, but also for securing national educational policy ambitions as well as contemporary nation-building concerns related to border-security in the high north. This official policy, known as Norwegianization, represented the harshest assimilation period, which, eventually, permeated most aspects of social life (Zachariassen, 2011). Following World War II, Finnmark’s 50 boarding schools were reduced to 12 (Törngren, 2020) and in 1963 the policy was abolished by law. Two of the densest Sámi areas (Kárášjohka and Guovdageaidnu) still had boarding schools until 1999; hence, the repercussions of the boarding school practice are noticeable to this day. The situation at the boarding schools with regard to psychosocial and physical care, degree of knowledge of Sámi culture and Sámi language among the teachers, allowance of Sámi language among the pupils, as well as the general quality of teaching and teachers’ human character varied widely. Any systematic account is not feasible to provide, but is to some extent available for the interested reader in the six book volume of the Sámi school history by Lund (2005–2013) and Tjelle (2000). However, most accounts of the daily life at the boarding schools include banning of Sámi language and exclusive use of majority Norwegian language (also outside school hours by service staff), considerable amounts of physical labor work related to cleaning, heating, food gathering and preparations at the school, frequent bullying between the pupils that were poorly regulated by the service staff and a general feeling of apprehension.
A qualitative change in the national sentiment towards the Sámi people and their culture sparked off in connection with the planning of the Alta river hydro power plant in 1982, which aroused an effective Sámi cultural and political countermovement, widespread civil disobedience, environmentalist awakening, national political upheaval as well as international critique (Minde, 2001). The Alta controversy triggered the establishment of the Sámi act (‘Sameloven’) in 1987, soon followed by the establishment of the Sámi Parliament in 1989 (Minde, 2005). The national school curriculum of 1987 marked the beginning of a total renewal of the Norwegian Sámi school policy by recognizing the rights of Sámi pupils and ensuring, for the first time, that knowledge of Sámi culture applied to all pupils in Norway. This initiative was further strengthened in later revisions culminating with the first “Sámi national curricula for the 10-year primary school” (NOU, 2000). Today, the Sámi community has modern educational institutions offering bachelor and master level university courses (www.samas.no) that integrate Sámi culture, language and knowledge traditions in their pedagogical approach.
Based on these historical accounts, it is reasonable to assume that the Norwegianization policy inflicting loss of language and culture, in particular for the children at the boarding schools, have had negative repercussions for health, well-being, educational prospects and work engagement.
Outcome Measures: Mental Health, General Health, Well-Being, and Disability Pension
The present SAMINOR analysis included three dependent variables as indicative of negative health and functioning (depression, general health and disability pension) and well-being as indication of a positive condition. Depression was measured with the Hopkin’s symptom check-list, which is a well validated mental distress measure primarily related to depressive symptoms, but also to anxiety (Bjelland et al., 2002). The current study focused on the better defined depression measurement part of the HSCL (Sørlie et al., 2018), but also because it ranks substantially higher with regard to symptom burden and disability adjusted life years as compared to anxiety (Wittchen et al., 2011). Previous studies have shown non-existent (Bals et al., 2010), negligible (Heyerdahl et al., 2004) or weak relationships between ethnicity (indigenous Sámi vs. majority Norwegians) and behavioral/affective health, particularly after adjustment for background factors as discrimination (Friborg et al., 2017; Hansen & Sørlie, 2012; Sørlie et al., 2018). However, given the presumed burden of boarding school in connection with a minority status, makes it likely to expect a negative relationship between a history of boarding school and health, particularly among the Sámi and minority groups. The prediction for the measures of general health and well-being measures is the same. The single-item general health variable is valuable as it provides an indication of self-perceived health that includes somatic health symptoms. As reviewed above, the relationship between Sámi ethnic status and somatic health is more often negative than non-existent or positive, which also has been reported in SAMINOR (Hansen et al., 2010). The World Health Organization’s well-being index (WHO-5) has been used extensively world-wide, and complements the health symptom measures by assessing more positive and general aspects of health and good functioning. It has good “clinimetric” validity (Topp et al., 2015) implying that the WHO-5 index also is a good indicator of health related problems of a clinical character.
Finally, the disability pension variable represents a more functional indication underpinning any disease burden, and thus extends the above health measures by indicating whether subjects continue to work and by that function relatively well despite physical ailments or chronic illnesses. As of February 2020, 10.1% of the adult population in Norway (18–67 years) received DP from the Norwegian Labor and Welfare administration (NAV). The largest groups being granted DP are individuals with musculoskeletal (26%) and psychiatric diagnoses (36%), which amounts to almost two-thirds of the entire DP population (NAV, 2020). Risk factors for DP in the Nordic countries are related to gender (women most likely), age (elderly most likely), socio-demography (less educated most likely), occupation (health and care sector most likely), unhealthy lifestyle (smoking, alcohol and physical inactivity), obesity, and ill somatic or mental health (Bjørngaard et al., 2009). As indigenous people in general score higher on these risk factors, it is reasonable to expect a higher risk of DP in these subgroups. A single North-Norwegian analysis of DP comparing rates of DP between those living within and outside municipalities who had received financial support from the Sámi parliament for establishing or maintaining small business enterprises has been conducted (Brustad, 2010). It showed a somewhat higher prevalence of DP in the inside areas, especially in areas with a lower educational level. The study was however naïve to the participants’ ethnicity, which the present study overcomes.
Aims and Hypotheses
The study describes the participants in the first and the second SAMINOR population study with regard to boarding school experiences, and connects it with background characteristics such as demographic and socio-metric variables, ethnicity, exposure to discrimination and violence.
Moreover, we examined whether participants with and without a boarding school history differed with respect to depression, general health status, well-being and granting of a disability pension. Based on the reviewed international literature, we expected negative relationships between a boarding school experience and the health outcome indicators.
Finally, we examined whether the associations between childhood boarding school and health outcomes were modified by factors related to ethnicity, discrimination and violence by conducting interaction analyses, as well as empirical search strategies (e.g., mixture regressions and random coefficient models) to identify subgroups showing more negative or positive health outcomes associated with boarding school experiences.
Methods
Samples
The SAMINOR 1 and SAMINOR 2 are cross-sectional epidemiological population-based studies on the health and living conditions among inhabitants settled in areas with both Sámi and Norwegian populations. The SAMINOR 1 sample was collected during 2003/2004 and the SAMINOR 2 sample during 2012. Both studies included a health survey questionnaire, which is thoroughly described with regard to the target population, study variables and data collection procedures: SAMINOR 1 by Lund et al. (2007) and SAMINOR 2 by Brustad et al. (2014).
The SAMINOR 1 Sample
All residents aged 36 to 79 years were invited (N = 27,987) and 16,865 responded (60.6% participation rate). Number of participants reporting boarding school attendance was 2,613 (15.4%). The oldest participants went to a boarding school in 1932. Some residents were excluded due to completely missing outcome data (depression/general health: 2,408/1,003 cases), covariate information about ethnicity (219 cases) or demographic/socio-economic status information (1,669 cases), leaving 12,569 and 13,974 cases available for analysis of depression and general health, respectively.
The SAMINOR 2 Sample
All residents aged 18 to 69 years living in the same areas were invited by mail (N = 44,669). Given 1,424 invitations were returned unopened, 43,245 persons were eligible for the study. Among these, 11,600 persons consented by returning the questionnaire (27% participation rate). The number of participants reporting boarding school attendance was 1,442 (12.2%). The oldest participants attended boarding school in the 1950’s. Participants with completely missing outcome information were excluded (depression/well-being: 617/418 cases), covariate information about ethnicity (23 cases), violence (72 cases), resilience (152 cases), or background covariate information (423 cases), leaving 10,313 and 10,512 cases available for analysis of depression and well-being, respectively. A minor subsample (n = 3,798) participated in both SAMINOR data collection waves of which 569 had attended boarding school.
Boarding School Variables
The boarding school item in the SAMINOR 1 had the following wording: (a) “Did you stay at a boarding school when you attended primary or secondary school (0-secondary, 1-primary, 2-both and 3-no)?”, (b) “If yes, how many grades?”, and (c) “How long on average did you stay at a boarding school in each grade?”. The comparable item in the SAMINOR 2 was: Did you stay at a boarding school when you attended school (yes/no)?”.
Outcome Variables in the SAMINOR 1
The Hopkins Symptom CheckList (HSCL)
The HSCL is a 10-item short version of the 90-item Symptom Check List (SCL-90) that rates symptoms of mental distress (Derogatis et al., 1974), that is, depression (six items) and anxiety (four items). It uses a four-point scale with higher mean scores (1-not at all, to 4-very much) indicating more distress. The cross-cultural validity of the HSCL-10 is good for the ethnic sub-groups that were included in the SAMINOR 2 sample, as demonstrated by a factorial invariance study which confirmed that the items were interpreted similarly across all ethnic sub-groups for the majority of the items (Sørlie et al., 2018). As the six depression items fit best in a previous SAMINOR 2 analysis (Sørlie et al., 2018) and target depression symptomatology more directly, the present study used these items exclusively. Moreover, the existing cut-off criteria of 1.85, as indicative of psychological distress based on Norwegian data (Strand et al., 2003), may be safely used in all the ethnic Sámi sub-groups that the study defines (Sørlie et al., 2018). The internal consistency of the mean SAMINOR 1 depression score (Cronbach’s alpha) was .85.
General health
A single question was used to assess the general state of health, by the question: “What is your current state of health?”. Responses were recorded on a four-point scale with the following category labels: 0-poor, 1-not so good, 2-good and 3-very good.
Outcome Variables in the SAMINOR 2
The depression (HSCL) and the general health measures were repeated in the SAMINOR 2 study. The Cronbach’s alpha for the mean depression score was .87 in the SAMINOR 2 study.
Well-being
The Well-being index (WHO-5) of the World Health Organization is used across the world (translated into more than 30 languages) to assess psychological well-being. A systematic review (Topp et al., 2015) of 213 papers utilizing the WHO-5 indicated high psychometric validity and usability as a clinical outcome measure. Participants rate their well-being across five items with scores ranging from 1-all of the time to 6-not at all. Reversing the index score indicates higher well-being. The Cronbach’s alpha was .92 in the present study.
Disability pension
In SAMINOR 2, participants self-reported whether they received a disability pension (yes/no).
Predictor Variables
Ethnicity
Three classes of questions were used to decide the ethnicity: (1) language spoken at home (Norwegian, Sámi, Kven or other languages), either by the person, the parents or the grandparents), (2) ethnic self-identification, either as Norwegian, Sámi, Kven or Other, and (3) ethnic background, either as Norwegian, Sámi, Kven or Other. Based on these questions, the following five ethnic subgroups were created: (1) “Norwegian” if only Norwegian markers were endorsed, (2) “Norwegian KO” if a Kven or an Other ethnicity marker were additionally endorsed, hence representing a mixed ethnic category, (3) “Sámi background” if identifying oneself as Norwegian but additionally reports a Sámi ancestry (parents/grandparents speaking Sámi, or having parents with a Sámi background), (4) “Sámi affiliation” if reporting one or two Sámi markers (the person speaks Sámi, self-identify as a Sámi, or reports a Sámi ethnic background), and (5) “Core Sámi” if a participant endorsed all three Sámi markers.
Discrimination in SAMINOR 2
Exposure to any kind of discrimination was coded as 1 (yes) if participants responded positively to the question ‘Have you ever been discriminated against?’ either by ticking ‘Yes, during the last two years’ or ‘Yes, previously’. Those scoring ‘No’ or ‘I don’t know’ were coded 0. Participants responding positively received additional questions about: (i) frequency of discrimination (0-not at all, 1-seldom, 2-sometimes and 3-very often), (ii) number of assumed reasons (range: 0–11) for being discriminated (i.e., ethnicity, physical disabilities, sexual orientation, learning difficulties, gender, religion, nationality, geographical affiliation, age, illness or other factors), (iii) number of places (range: 0–13) where discrimination took place (i.e., internet, at school, at work, applying for a job, at voluntary work/in organizations, in contact with government agencies, within family/relatives, when renting/buying apartment/house, applying for bank loan, accessing medical treatment, in shops/restaurants, in the local community, or other places), and (iv) number of perpetrators (range 0–8) inflicting the discrimination (i.e., public employees, strangers, work colleagues, members of the same ethnic group, members of other ethnic group, fellow students, teachers/employees, or other people). The score distribution of the three last count variables was highly negatively skewed with a long tail flattening out at scores above 4, which were truncated to 4 (new range: 0–4). All scores were normalized and summed in an overall Dcrim score with a range from 0-complete absence to 100-maximum discrimination.
Discrimination/Bullying in SAMINOR 1
Exposure to any kind of discrimination (bullying) had a similar ingress question as in the SAMINOR 2. Those responding “yes” were prompted to describe types of bullying (gossiping, discriminating remarks, being ignored, or other types) and location of bullying (at school, at boarding school, at work, in the local community, or in other places). A normalized Dcrim score similarly as in SAMINOR 2 was computed.
Interpersonal violence
A recording of IV was included in the SAMINOR 2. The IV items were extracted from a validated questionnaire (the Norvold Abuse questionnaire, NorAQ) previously used in a Nordic study on abuse and violence (Wijma, Schei, Swahnberg, Hilden, et al., 2003), which had adequate reliability and validity (Wijma, Schei, & Swahnberg, 2003). The SAMINOR 2 covered three types of IV, that is, physical, sexual and emotional violence. Participants additionally reported when the IV occurred (before or after 18 years of age, or during the last year). These questions had also been used in another study to estimate the prevalence of IV among Sámi and non-Sámi populations (Eriksen et al., 2015), showing that the IV was higher for the Sámi than for the majority Norwegians.
Impact of Event Scale
Traumatic events may overwhelm an individual and disrupt normal functioning. The IES as developed by Horowitz (Sundin & Horowitz, 2002) represents a proxy measure indicating presence of intrusive memories, avoidance behavior and emotional numbness, which are prominent symptoms of a post-traumatic stress disorder. An abbreviated three-item version covering these domains were included in SAMINOR 2 (rated as 1-yes, but rarely, 2-sometimes and 3-often). This version has previously been used in the Nordic Study (Wijma, Schei, Swahnberg, Hilden, et al., 2003), in an European study on pregnant women (Schei et al., 2014), as well as in a previous sub-study of the SAMINOR 2 showing that childhood violence was strongly associated with posttraumatic stress in adulthood in both Sámi and non-Sámi populations (Eriksen et al., 2018). A principal component analysis of the three IES items yielded a single component with an eigenvalue 1 (R-sq = 66.6%), thus supporting the creation of a single sum score. The IES score (Cronbach’s alpha = .75) was used as a covariate and a moderator (interaction) as it may modify the relationship between IV and the measured health outcomes.
Short form of the Resilience Scale for Adults
The RSA measures protective factors associated with resilience (Friborg et al., 2003, 2005). The original RSA consists of 33 items assessing three overarching protective domains: (a) intrapersonal traits and characteristics (measured by four factors: personal strength, social competence, positive future and personal structure), (b) family cohesion and (c) social resources. A range of studies confirm the validity of these six RSA factors (Hjemdal, 2007; Windle et al., 2011), as well as cross-cultural validity (Hjemdal et al., 2011, 2015; Jowkar et al., 2010). A short version (12 items) was prepared for the SAMINOR 2 study by selecting four of the highest loading items from each of the three factors personal strength, social competence and family cohesion. The Cronbach’s alphas in the present study were .81, .77 and .86 for the three respective RSA factors.
Covariates
The following socioeconomic variables were included for the purpose of adjustment of the regression analyses: gender (0-female, 1-male), age (centered continuous score), education (total number of years of schooling), full-time work (0-no, 1-yes), and household annual income (0 < 150,000 NOK, 1 < 300,000 NOK, 2 < 450,000 NOK, 3 < 600,000 NOK, 4 < 750,000, 5 < 900,000 NOK and 6 > 900,000 NOK).
In addition, variables associated with the outcome variables used in the present study (i.e., mental and general health, and well-being) were adjusted for previous and current smoking, use of alcohol, physical activity, and geography as an indication of Sámi community denseness (i.e., no Sámi, minor Sámi <20%, medium Sámi 20% to 50% and major Sámi 50%). Sámi denseness has, in previous studies, shown associations with well-being, health and various living conditions, and that Sámi living in less dense areas (<50% Sámi) are more prone to marginalization, discrimination and social exclusion as compared to more dense Sámi area (Hansen, 2011, 2016; Hansen et al., 2008, 2016). Communities having more Sámi denseness also have more institutions that are better educated and accustomed to address requests or inquiries from the Sámi inhabitants.
Statistical Analyses
All descriptive and regression analyses were conducted in SPSS version 26. The regression models were fitted using a normal linear distribution model unless distributional assumptions were not met. The depression (HSCL) outcome data were severely skewed (Z-score 93) and kurtotic (Z-score 104); hence, these data were fitted using an inverse gamma distribution along with an additional sandwich estimator to correct the standard error bands for heteroscedastic residuals. The regression model for binary data (i.e., disability pension) were fitted using a binomial logit function (logistic model) but with the same sandwich estimator.
The covariates were examined in steps: As boarding school experience was of prime interest, it was entered in the first step, followed by ethnicity (step 2), exposure to discrimination (step 3), adjustment for geography/residency (step 4), and demographic and socio-metric variables (step 5). This model thus represented a fully adjusted model. The SAMINOR 2 study included a rating of the impact of events (IES) and resilience factors, which we assumed modified the potential impact of violence. We therefore added IES and resilience as moderators, that is, violence*IES and violence*RSA, between step 4 and 5. In the final step, we examined if ethnicity and discrimination modified the boarding school—outcome association. Type III Wald or F-tests were used. The alpha level was set to .05; however, given the multiple number of tests, p-values should drop down to around .01 in order to increase the confidence in correctly dismissing the null-hypothesis. The magnitude of mean score differences were interpreted using standardized Cohen’s d estimates with values of 0.2 and 0.5 representing weak to moderate effect sizes.
Results
Description of the SAMINOR 1 and the SAMINOR 2 Samples
Descriptive data for participants that attended boarding school are given in Table 1 for the SAMINOR 1 study in 2003 to 2004, and in Table 2 for the SAMINOR 2 study (2012) accompanied with comparable data for the remaining sample. Zero-order correlation tables for the nominal/continuous variables are available online (see Supplemental Table S1 and S2 for the SAMINOR 1 and SAMINOR 2 samples, respectively).
Descriptive Data for Those Attending Boarding School in the SAMINOR 1 (2003/04) Sample (N = 15,064).
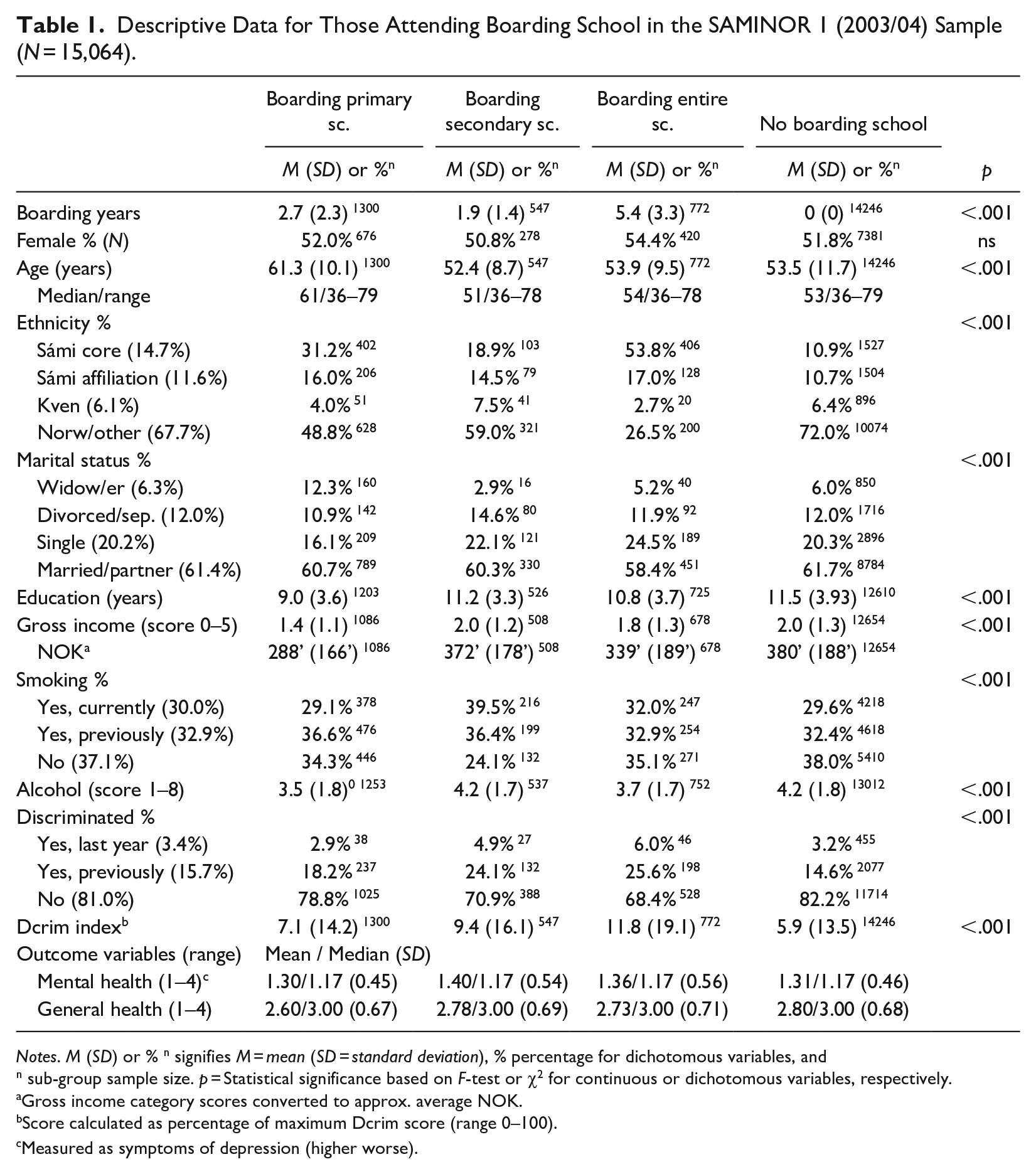
Notes. M (SD) or % n signifies M = mean (SD = standard deviation), % percentage for dichotomous variables, andn sub-group sample size. p = Statistical significance based on F-test or χ2 for continuous or dichotomous variables, respectively.
Gross income category scores converted to approx. average NOK.
Score calculated as percentage of maximum Dcrim score (range 0–100).
Measured as symptoms of depression (higher worse).
Descriptive Data for Those Attending Boarding School in the SAMINOR 2 (2012) Sample (N = 11,600).
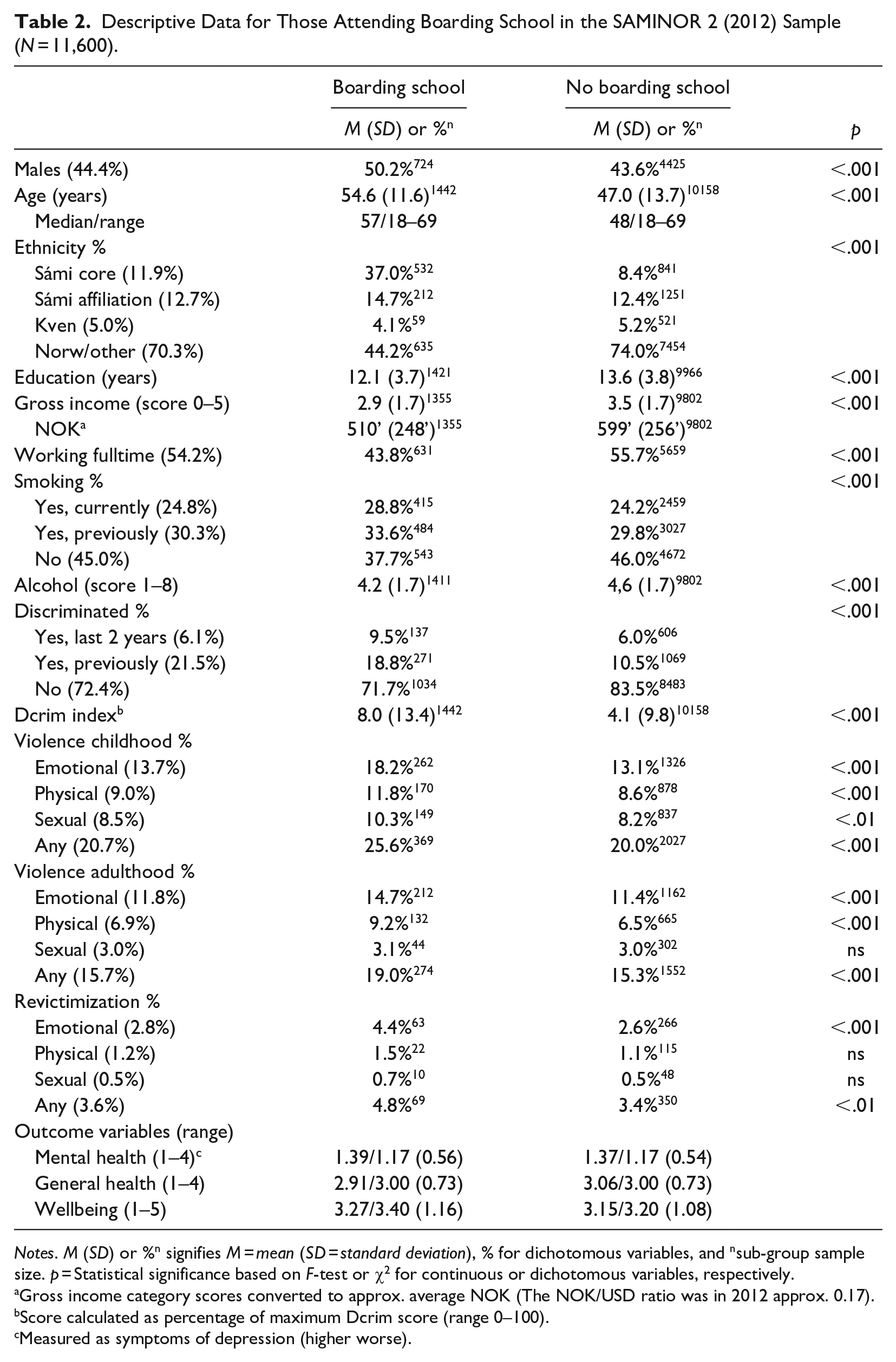
Notes. M (SD) or %n signifies M = mean (SD = standard deviation), % for dichotomous variables, and nsub-group sample size. p = Statistical significance based on F-test or χ2 for continuous or dichotomous variables, respectively.
Gross income category scores converted to approx. average NOK (The NOK/USD ratio was in 2012 approx. 0.17).
Score calculated as percentage of maximum Dcrim score (range 0–100).
Measured as symptoms of depression (higher worse).
Regression Analyses of Boarding school effects in SAMINOR 1
Two prediction models with depression and general health status as self-reported dependent variables were regressed on the predictors in steps (Table 3). Having a boarding experience was associated with more depression, especially among those attending boarding school during the secondary years as compared to the majority ‘no boarding’ group (p < .001, Cohen’s d = 0.21). However, this association disappeared after adding more covariates. Variables related to a history of smoking, but most notably current or previous experiences with discrimination, were the prime reasons for nullifying the boarding-depression association. As Table 1 shows, participants with a boarding school experience had a higher frequency of previous and current smoking, as well as recent-year and lifetime exposure to discrimination compared to the majority group. As these covariates connected with deterioration in depression, they overtook the role of boarding school as a predictor. Of note, participants with a Sámi core ethnicity had the best mental health status.
Regression Models for Depression and General Health in SAMINOR 1 (N = 15,064).
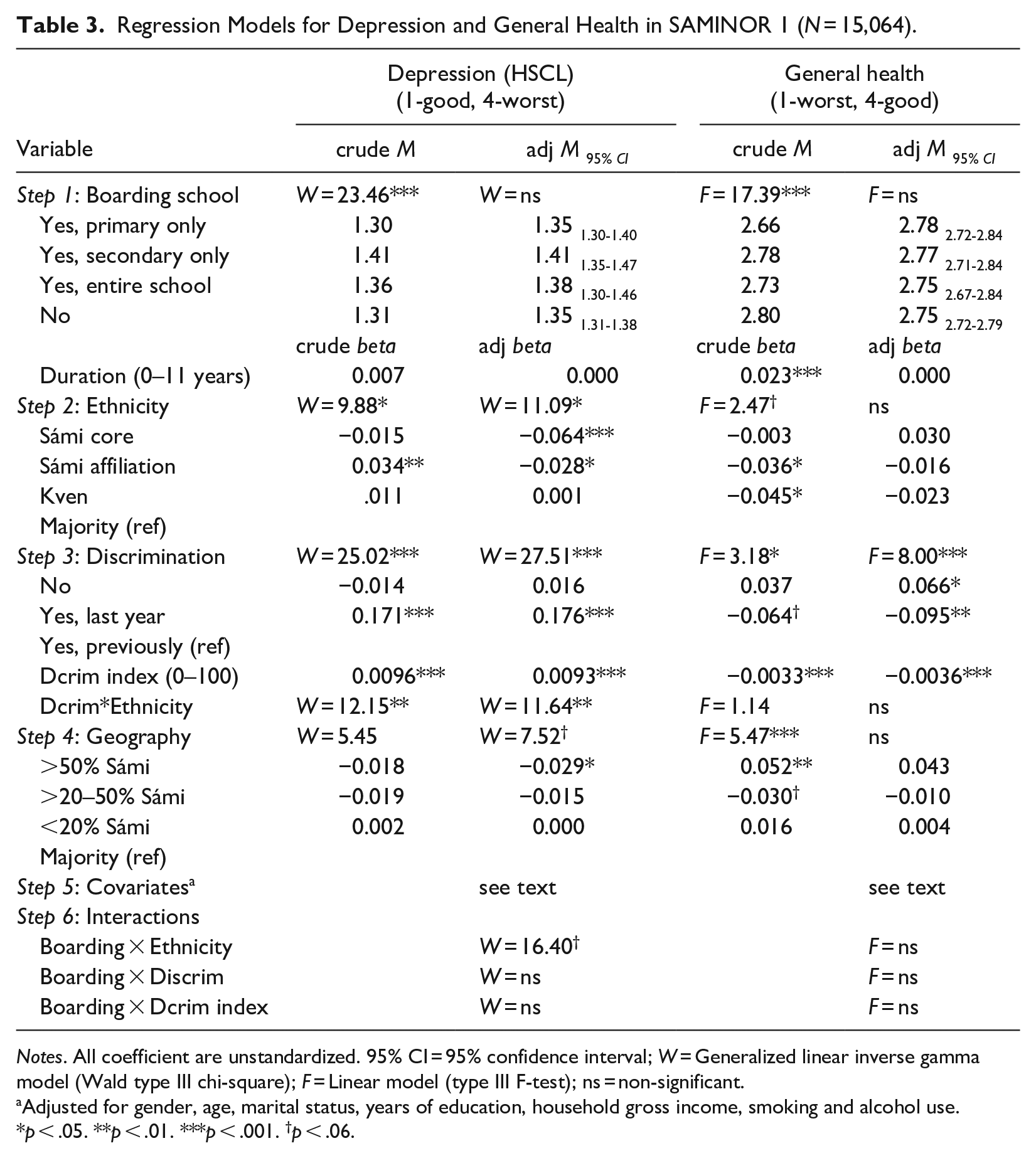
Notes. All coefficient are unstandardized. 95% CI = 95% confidence interval; W = Generalized linear inverse gamma model (Wald type III chi-square); F = Linear model (type III F-test); ns = non-significant.
Adjusted for gender, age, marital status, years of education, household gross income, smoking and alcohol use.
p < .05. **p < .01. ***p < .001. †p < .06.
The main covariate that nullified the initial significant relationship between boarding and general health status (showing a worse general health status among primary boarding vs. majority ‘no boarding’ participants, p < .001 and d = .20), was age. As participants with a boarding history was older and higher age connected negatively with general health status, age overtook this association.
Moderator analyses
With the fully adjusted model specified, we examined if the boarding-health relationships were moderated by ethnicity and discrimination. A tentative interaction emerged with regard to boarding×ethnicity (p = .059), which in a follow-up analysis revealed that minority participants attending boarding school during secondary school years, reported significantly more depression than the majority ‘no boarding’ participants. This association was only present within the Sámi affiliation group (M = 1.53 vs. 1.35, Mdiff = 0.184, p = .015, d = 0.40), and not in the other ethnic subgroups. The two moderators related to exposure and dosage of discrimination did not contribute as moderators, and neither did gender.
Summary of additional covariate effects: The covariates were of less importance, but showed the following significant relationships: higher age (less depression, b = –.0019***; worse general health, b = –.010***), women versus men (more depression, b = .089***; worse general health b = –.029*), divorced versus married (more depression, b = .064***), widow(er) versus married (better general health, b = .127***), longer education (better general health, b = .018***), higher household income (less depression, b = –.036***; better general health, b = .069***), current smoker versus non-smoker (more depression, b = .086***; worse general health, b = –.160***), previous smoker versus non-smoker (more depression, b = .042***; worse general health, b = –.092***), and higher alcohol consumption (more depression, b = .0064**, better general health, b = .022***).
Regression Analyses of Boarding School Effects in SAMINOR 2
Three prediction models with mental (HSCL depression) and general health, and well-being as dependent variables were regressed on the predictors (Table 4). Having a history of boarding school was not associated with depression, weakly negatively with general health (p < .001, d = 0.21) and weakly positively associated with higher well-being (p < .001, d = 0.11). The general health association was nullified after adding the covariates, primarily age and household gross income, in falling order. The well-being association was also reduced after adding the covariates, primarily related to age. As Table 2 shows, participants with boarding school had less household income and were older than the majority ‘no boarding’ participants, which was related to better general health and a higher well-being. With regard to well-being, the difference remained significant (p = 0.016) after full adjustment, but the magnitude was very low (d = .06). Of note, and comparably to the findings reported in Table 3 (SAMINOR 1), participants with a Sámi core ethnicity reported best general health and highest well-being.
Regression Models for Depression, General Health and Well-being in SAMINOR 2 (N = 11,600).
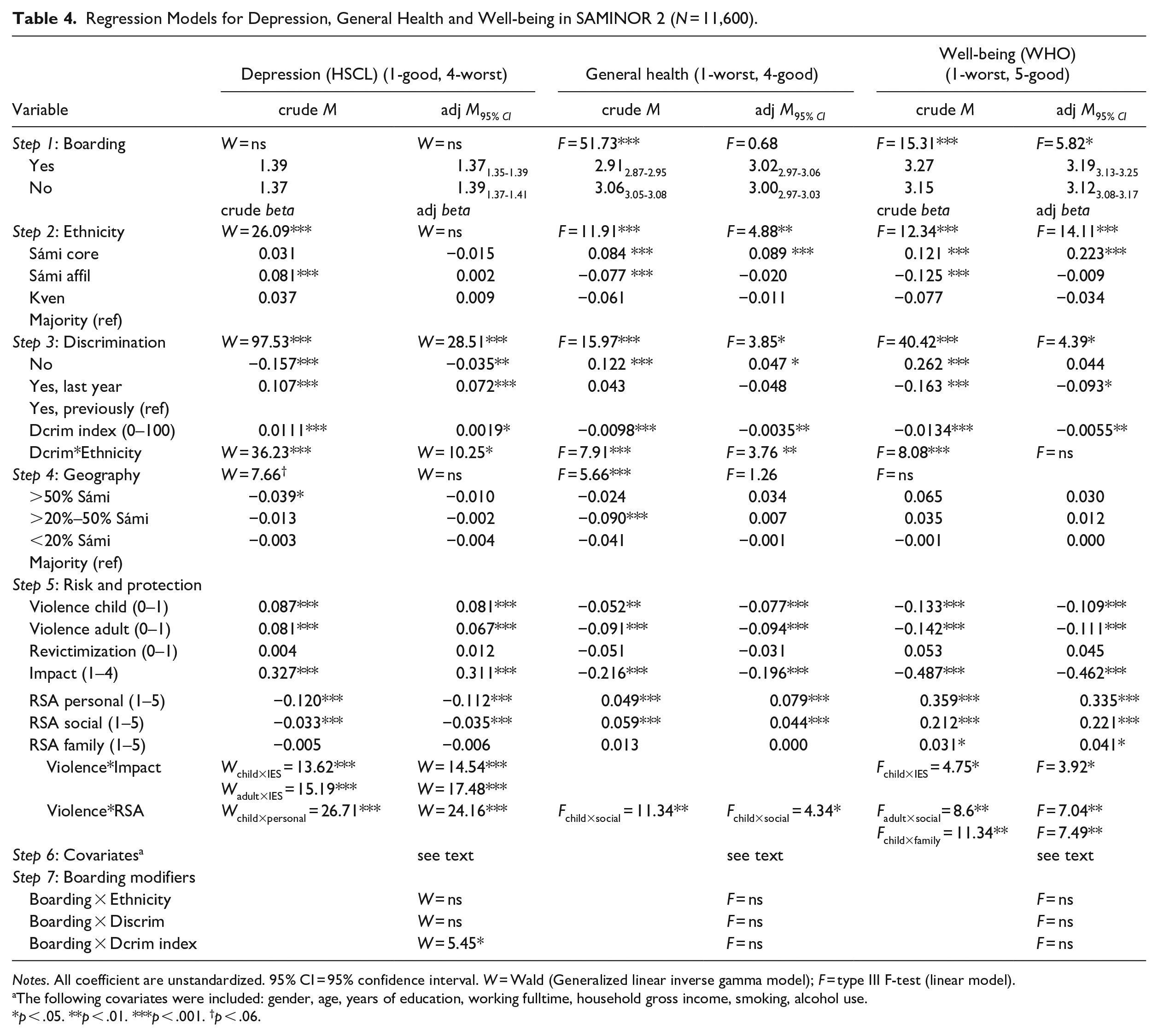
Notes. All coefficient are unstandardized. 95% CI = 95% confidence interval. W = Wald (Generalized linear inverse gamma model); F = type III F-test (linear model).
The following covariates were included: gender, age, years of education, working fulltime, household gross income, smoking, alcohol use.
p < .05. **p < .01. ***p < .001. †p < .06.
Moderator analyses
With the fully adjusted model specified, ethnicity and exposure and dosage of discrimination were additionally modeled as moderators. Among these, the Dcrim index (dosage) significantly moderated the boarding-depression correlation. Given no exposure to discrimination, which represented the 79.6 percentile of the sample, the boarding group had slightly better mental health than the no-boarding group (Dcrim = 0, HSCL = 1.365 vs. 1.387, p = .02, d = .04), comparable mental health at the 84.3 percentile (Dcrim = 14.6, HSCL = 1.404 vs. 1.393), and worse mental health at high discrimination levels (95 percentile, Dcrim = 29.4, HSCL = 1.445 vs. 1.402, d = .08, p = .10). No further interaction effects (exposure to discrimination, ethnicity and gender) were significant.
Covariate Findings Related to the Risk and Protection Variables
Among the three violence indicators, experience of childhood and adult violence were higher among the boarding group as compared to the non-boarding group (Table 2). In addition, the regression analyses (Table 4) showed that violent events occurring in adult- and childhood were negatively associated with all outcome measures, whereas revictimization did not reach significance. A higher negative impact of these events contributed strongly to further deterioration of mental health and well-being. As to the protection variables, the most important resilience factors were personal competence, social competence, and family cohesion, in falling order.
Given that the impact and resilience factors represent risk modifier variables, they were added as moderators of the violence-health correlation. With regard to depression, a high impact strengthened the negative effect of childhood violence (b = .077, p < .001) and adult violence (b = .074, p < .001), whereas personal resilience dampened the negative effect of child violence (b = –.075, p < .001), as expected. Comparable analyses with general health as outcome, observed a protective effect of social competence against exposure to childhood violence (b = .038, p = .037). Similar interaction analyses for well-being showed two unexpected results: a higher impact (b = .061, p = .048) and less social competence dampened the negative effect of childhood violence (b = –.069, p = .008), whereas, and as expected, more family cohesion offered an increased protection (b = .071, p = .006). These interaction terms were mainly included for adjustment purposes but were in addition informative on their own.
Summary of additional covariate effects on mental and general health, and well-being
The following covariates were significant: higher age (mental health and well-being better, bdepr = -.0008*** and bwell-being = .0064***; general health worse, b = -.0117***), women versus men (mental health and well-being worse, bdepr = .045*** and bwell-being = -.096***; general health better, b = .054***), longer education (less depression and better general health, bdepr = -.002** and bhealth = .0010**), higher household income (less depression and better general health, bdepr = -.004* and bhealth = .0279***), current smoker versus non-smoker (all worse, bdepr = .046***, bhealth = -.155*** and bwell-being = -.192***), previous smoker versus non-smoker (all worse, bdepr = .028***, bhealth = -.097*** and bwell-being = -.135***), and working full-time versus non-full time (all better, bdepr = -.050***, bhealth = .176 and bwell-being = .079***).
Extra Subgroup Analyses to Detect Boarding School Effects
In order to examine if the boarding variable effect might be masked by other variables or subgrouping factors in the SAMINOR 1 or SAMINOR 2 samples, we conducted three extra empirical searches to detect this possibility.
First, we explored if participants born in a particular year reported a different outcome as compared to all other participants by constructing an age variable coded as 1 (born in a particular year) or 0 (all else). Two adjacent years were combined in order to increase the subgroup sample size (e.g., born 1950-51), which produced 22 age group categorizations (1928-1968) in SAMINOR 1 and 26 age groups (1944-1995) in SAMINOR 2. We added this age_subset variable as a main effect along with the more interesting interaction effect (age_subset × boarding) to the fully adjusted model. Almost all confidence intervals were overlapping, thus showing no better (or worse) outcome statutes related to specific time periods when the participants attended boarding school.
Second, we added two random coefficients to the fully adjusted analyses: a random intercept coefficient representing the outcome baseline values, and a random slope coefficient representing the boarding school effects across all 24 municipalities where the participants grew up. None of the random coefficients were significant. The most important factor, the random boarding coefficient, showed almost no variance. Hence, any boarding effect was not masked by these reasons.
Third, we examined if the boarding variable might show a different relationship with the outcome variable depending on the level of the outcome score. This analysis corresponds to a mixture regression analysis, except we defined the intercept level of the subgroups manually. A three-group solution was preferred as it generally fit better than a two-group solution (lower BIC deviance), whereas further groups became impractical with regard to interpretation and small subgroup sample sizes. The fully adjusted regression analyses were rerun with this new cluster variable and its interaction term (cluster*boarding) added. The depression cut-values that produced the lowest BIC deviance were HSCL < 1.17, 1.18–2.0 and 2.0. None of these interaction tests were significant, thus indicating a similar boarding effect irrespective of depression levels. The well-being values that produced the lowest BIC deviance scores were <2.3, 2.31 −3.6, 3.61 (range 1–5). This interaction term was significant (Fdf = 2,10 467 = 13.50, p < 001). A follow-up analysis showed a more negative effect of boarding school in the lowest well-being group (M = 1.66boarding vs. 1.77no boarding, p < .001), but a positive boarding effect in the highest well-being group (M = 4.28boarding vs. 4.22no boarding, p = .002). These differences corresponded to small effect sizes, d = 0.11 and 0.06, respectively.
Regression Analyses of Disability Pension Effects in SAMINOR 2
In the second SAMINOR wave, participants self-reported whether they received a disability pension. The proportion of participants receiving a disability pension grows cautiously during early adulthood years and starts accelerating during middle age followed by abrupt downward shift before reaching normal retirement age. The age effect was therefore modeled non-linearly by adding an increasing number of squared centered age terms (e.g., cAge*cAge, cAge*cAge*cAge etc.) until the deviation statistics stopped improving as according to the Bayesian information criteria (BIC). This happened after adding the fifth degree polynomial age term (see Supplemental Table S3 available online). The boarding variable was added to this age-adjusted model, which was significant (OR = 1.28, Table 5) and disfavored participants with a boarding history as compared to the no-boarding group (see Supplemental Figure S1 available online).
Regression Models Predicting Disability Pension in SAMINOR 2 (N = 11,600).
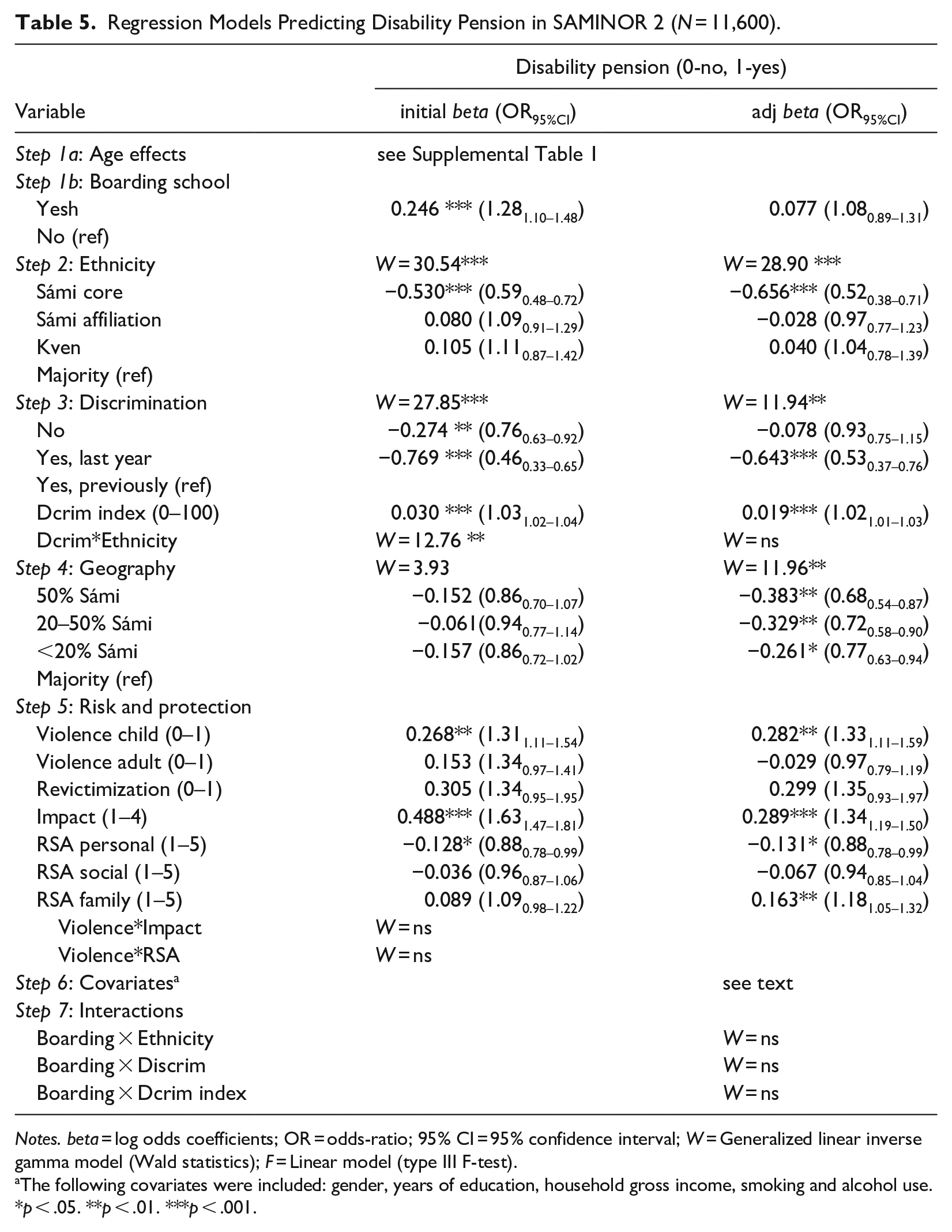
Notes. beta = log odds coefficients; OR = odds-ratio; 95% CI = 95% confidence interval; W = Generalized linear inverse gamma model (Wald statistics); F = Linear model (type III F-test).
The following covariates were included: gender, years of education, household gross income, smoking and alcohol use.
p < .05. **p < .01. ***p < .001.
The boarding effect vanished after adding further covariates to the model. The main covariates that nullified the relationship were household gross income and years of education, in declining order. Hence, the lower income and educational level of participants with a boarding history (as Table 2 also shows) were the underpinning reasons of the initially observed differences.
Moderator analyses
None of the moderators (ethnicity, the two discrimination variables and gender) contributed significantly.
Covariates Findings
Ethnicity
A notable covariate effect emerged for the ethnicity variable, which indicated a significantly reduced rate of disability pension in the Sámi core group compared to all other ethnic groups (see Supplemental Figure S2 available online). Moreover, the ethnicity effect was rather strengthened than weakened after adding the covariates adjustment. In the fully adjusted regression model, the proportion of participants with a Sámi core ethnicity that received a disability pension was significantly lower than that of the majority group, across a wide age span (most p’s < .001) which peaked between 62 and 64 years of age, with a proportion difference of approximately 0.12.
Violence and resilience
Childhood violence and the impact variable significantly increased the odds of DP, whereas violence in adulthood or revictimization were unimportant. Among the resilience variables, high personal competence lowered the odds of DP, whereas high family cohesion heightened the odds. An unexpected finding was that a recent-life exposure to discrimination lowered the odds of DP, possibly due to the higher occurrence of discrimination among high SES participants.
Summary of other covariates
The following covariates were significantly associated with the proportion of disability pension: women versus men (OR = 1.44***), longer education (OR per year = 0.92***), higher household income (OR = 0.64***), current smoker versus non-smoker (OR = 1.44***), previous smoker versus non-smoker (OR = 1.43***), higher alcohol consumption (OR = 0.96*).
The Role of Boarding School Experiences for Change in Health Status
The subsample that participated twice in the two SAMINOR studies (n = 3,798, of which n = 569 reported boarding school) was analyzed with regard to change in depression and general health status. We fitted a linear mixed regression model with robust estimation of error scores. A time variable represented the change in health status from study 1 to 2. The same covariates as in the SAMINOR 1 analysis were added. Moreover, we adjusted for the dependency (correlation) in the repeated data by estimating a random intercept coefficient, and for regression-to-the-mean effects by adding the interaction term time×baseline score (allowing for a larger change estimate for those with extreme baseline scores). The analysis revealed a non-significant change in depression from 2003/04 to 2012 (btime = –.01, p = .89), which was not modified by boarding school (btime×primary sc = –.02, p = .65; btime×secondary sc = .05, p = .33; btime×entire sc = .02, p = .71). Adding further covariates from the SAMINOR 2 study, that is, violence, IES and RSA, did not change this null finding. The same analysis with general health as outcome showed a significant improvement in health (btime = .22, p = .004) but the time×boarding interaction effect was not significant. These results thus converged with the findings from the cross-sectional analyses.
Discussion
The boarding school system in Norway was aimed at eradicating the language, cultural traditions, and spiritual beliefs of the indigenous Sámi and the Kven minority children by assimilating them into the Norwegian majority society (Hansen, 2018). The present study examined if participants who participated in two epidemiological studies (SAMINOR 1 and SAMINOR 2) about health and living conditions in Sámi areas, conducted in 2003/04 and 2012 by the Centre for Sami Health Research in Norway, observed any negative effects with regard to mental and general health, well-being and disability pension (DP), on average, 40 years after their boarding school experience.
Overall, we observed small differences in the health outcome variables in both SAMINOR studies. In the SAMINOR 1 study, participants attending boarding school reported slightly poorer mental and somatic health, but this difference disappeared after adding covariates to the model. In the SAMINOR 2 study, the mental health scores were comparable between the boarding and no-boarding participants, both in the crude and the adjusted models. The general health scores initially favored the non-boarding participants but became harmonized with the boarding participants after covariate adjustment. The crude well-being scores were even slightly better among the boarding compared to the no-boarding participants. This difference weakened after adding the covariates but without losing statistical significance. Basically, these findings reveal negligible differences between the participants with and without a history of boarding school. The covariates that nullified the initial minor differences were primarily related to discrimination, and additionally, to a history of smoking (SAMINOR 1), age and gross household income (SAMINOR 1 and SAMINOR 2).
The proportion of participants receiving a disability pension (in SAMINOR 2) was higher among the boarding compared to the no-boarding group. However, the difference disappeared after adding the covariates, of which gross household income and years of education were the main contributors to nullifying the relationship.
We conducted several additional empirical searches aimed at unmasking any potential missed boarding school effects in subgroups. One approach was the addition of moderator analyses to pull out subgroup differences related to ethnicity, and exposure and level of discrimination. In this respect, a tentative negative boarding effect emerged in the SAMINOR 1 study exclusively among participants that reported a weaker Sámi identity (Sámi affiliation), whereas higher levels of discrimination in the SAMINOR 2 study seemed to make the boarding-health outcome relationship more negative. However, the magnitude of these differences was minor.
In addition, we conducted a series of three other empirical searches with a similar purpose. First, we defined a range of age subgroups specifying the time-period the participants attended boarding school. As the Norwegianizing policy was lifted around 1960, this age recoding allowed an examination of whether participants attending boarding school before, during and after this time period (~1960) might have a different health status than non-boarding participants. Second, we conducted random coefficient analyses examining if the boarding school variable systematically varied between the 24 municipalities, of which 16 had been running a boarding school. Neither of these two approaches contributed new information. Third, we conducted a mixture regression analysis examining if the boarding effect might differ depending on the level of the health outcome status. We observed no differences with regard to mental health status, but observed a small negative boarding effect among participants with lower well-being, and a small positive effect among participants with higher well-being.
In sum, our findings show substantial individual differences in health statuses. However, having experience with boarding school showed no or negligible relationships with long-term health outcomes, as measured in this study. This finding contrasts previous studies as reviewed in the introduction, and in particular the studies examining Native North Americans, First Nations, Métis and Inuit in Canada, which indicate a rather consistent negative impact of placement at boarding school on health and well-being (Evans-Campbell et al., 2012; Wilk et al., 2017). We acknowledge that our findings may be at odds with prior assumptions about negative health consequences of boarding school. The retrospective design may be the main explanation of the attenuated observed effects as the boarding schools for Norwegianization purposes were abolished in the 1960’s. Hence, the retrospective analysis has an exceptional long timeframe with the data collection occurring on average 44 years after boarding school, and stretching up to 72 years for some individuals. The participants have thus lived a long and diverse life, experienced other and most likely more life-changing events, as well as passed through normal psychobiological aging processes that in sum may have substantially faded the significance of the boarding school years.
Another conceivable possibility is the more egalitarian aspects of the Norwegian society as compared to countries outside Norway and Scandinavia. Despite a harsh history of Norwegianization, some substantial changes have taken place during the last three decades in Norway, most notably the establishment of the Sámi parliament that has improved the official status of the Sámi people, as well as provided monetary reinforcements aimed at strengthening Sámi culture, language and commerce. The Norwegian health care and educational policies also assure free access to high quality specialist health services as well as higher education irrespective of socioeconomic class or ethnicity, whereas these services are not, to the same extent, free of charge outside Scandinavia. One may also mention that the Government has passed legislation along with strong guidelines aimed at sustaining Sámi language and culture in primary and secondary schools, and in kindergartens (The Norwegian Directorate for Education and Training, 2013). The Government has passed a revision to the Act relating to Primary and Secondary Education and Training (chapter 6 Sámi education) that ensures Sámi children’s right to receive teaching in Sámi language independent of residence (Lovdata, 1998). The change that have taken place in the Norwegian school system during the last decades is also illustrated by the existence of three boarding schools for Sámi children, which, in contrast to the original ones, aim to strengthen the Sámi language and culture. These schools also use digital distance learning methods extensively.
Finally, we also note that the non-existing or small boarding school differences at the group level do not contradict the fact that some have suffered a high level of mental distress related to their boarding school experiences. On the other hand, some Sámi children may have benefited from relocating to a boarding school where the majority of the children had a similar background as themselves, as opposed to Sámi children attending ordinary Norwegian schools dominated by Norwegian majority children, thus lacking the protection that in-group support and identification may provide.
A Negative Effect of Boarding School After All?
Despite the observation of few or no negative effects of boarding school on mental health and well-being in the adjusted statistical models, the present study showed that boarding school was associated with other negative characteristics: an unhealthier life style (e.g., previous and current use of tobacco), a more unfavorable socio-demographic situation in terms of lower education and less household income, as well as an increased exposure to discrimination and violence. Hence, it seems that boarding school attendance is associated with risk factors that connect with both health and well-being, and in this way, boarding school becomes indirectly negatively associated with health. The study by Running Bear et al. (2019) showed that the American Indian boarding school attendants not only had more chronic health conditions, but also a higher levels of unemployment, lower income levels, and were more frequently unmarried compared to the non-boarding Indians (Running Bear et al., 2018). As the boarding school context of the Sámi to some extent mimics the American Indian situation, we consider our findings as partially converging with that of Running Bear et al. (2018). Our findings were however weaker, which we relate to the longer retrospective timeframe of our study in addition to national differences related to free access to health services and education, as mentioned above.
It should be noted that the objective of the customary covariate adjustments that we conducted was to equate any sampling-related unbalances present across all subgroups as implied by the included covariates. However, if unbalances represent the true state of affairs, that is, that people attending boarding schools truly acquire less education, get less skilled jobs and earn less income, and over time suffer worse health, conventional statistical equating becomes futile as such differences represent naturally occurring phenomena. Why equate something that is truly unequal in nature? Such covariates might also be part of putative causal chains, which, if true, would require strategies aimed at delineating mechanisms instead. Unfortunately, this issue is not possible to ascertain in the present study, and hence we cannot dismiss that boarding school does play a larger negative role than the current results suggest, at least indirectly. Unfortunately, this issue is not possible to address in any future- and potentially better designed study as most of these participants are no longer alive.
Ethnicity and Disability Pension
A noteworthy and novel finding of the present study was the strong association between ethnicity and disability pension (DP). We observed that fewer participants with a strong Sámi identity (Sámi core), in particular those between 62 and 64 years of age, received a DP that was about 12% less than the amount received by majority Norwegians. Subjects with a weaker Sámi identity (Sámi affiliation) and the Kven minority did on the other hand report the highest rates of DP. These two subgroups may thus have been more prone to the Norwegianization policy by affecting their working capability more negatively. The only available Norwegian study touching upon this topic, is a study by Brustad (2010) who reported a somewhat larger rate of DP in municipalities receiving financial support by the Sámi parliament of small business enterprises. We, however, consider our finding as more valid, as we used individual-based data, a more sensitive geography location variable, as well as a strong method for deciding the ethnicity of the participants. The study by Brustad (2010) lacked access to this information. Moreover, the geographical location variable that we used to characterize areas with different degrees of denseness of Sámi ethnicity, showed a similar but less pronounced trend. A limitation of our analysis was the use of self-reported DP, whereas registry data would be preferable if legally allowed. This concern is relevant if the self-reporting of DP was biased or underreported in certain ethnic groups, as for example in the Sámi core group. However, we have no information available to suspect that this group would consider receiving a DP as potentially more stigmatizing than the other groups, and we therefore consider our finding as quite robust.
Vulnerability and Protective Factors: Violence, Discrimination and Resilience
Our findings converge with studies showing a higher incidence of violence in indigenous than in non-indigenous populations (Brzozowski et al., 2006; Curtis et al., 2002; Eriksen et al., 2015; Sundaram et al., 2004), and extends these findings by showing that boarding school participants also have been more exposed to childhood and adult violence than non-boarding participants. Moreover, the negative effect of violence was markedly stronger in sub-groups experiencing a higher negative impact of events (the IES scale) than in those experiencing them as less intrusive, thus indicating a traumatizing aspect of the exposure. A limitation with the IES measure was however the lack of specification for which events that were most intrusive.
The boarding school participants reported more discrimination in general than the non-boarding participants. Previous studies have shown that Sámi and Kven participants report more exposure to ethnic discrimination than the majority population (Hansen et al., 2008, 2016), which also have taken place in boarding schools (Hansen et al., 2008); hence, discrimination is a risk factor for poorer somatic health (Hansen, 2015). As the discrimination to some extent accounted for health differences between the boarding and non-boarding participants in the present study, the boarding school experience in the present study may imply comparable ill health effects albeit being small in magnitude.
Among the protection variables, the most important resilience factors were personal competence, social competence and family cohesion, in falling order. Social competence and family cohesion were more important for well-being than mental health status, which indicates that the protective role of social/family life seems more important for their quality of life than absence of depressive symptoms. Further, the importance of high personal competence converges with multiple studies confirming its protective role (Friborg et al., 2005, 2009; Hjemdal et al., 2012). The negative association between high family cohesion and DP was however unexpected, which may make more sense if looking into its measurement constituents as the scale includes items asking for family warmth, family support, cohesion and loyalty. With such connotations in mind, a high family cohesion may reinforce an earlier application for DP.
Strengths and Limitations
The strengths of the present study were its epidemiological design, the broad coverage of communities included, a rigorous measurement of ethnicity as well as large sample sizes ensuring strong statistical power.
Some limitations may be noted. The low response rate in the SAMINOR 2 study may clearly bias the results, which dropped from 60.6% in the SAMINOR 1 to 27% in the SAMINOR 2 study. This is a remarkable drop over time in the willingness to contribute to national health examinations and surveys. Such drops in response rates is a general trend that has become a considerable challenge for population-based health studies. In the present case, the SAMINOR 1 data collection lasted about two years and used more professionally trained research assistants than in the SAMINOR 2. The SAMINOR 2 data collection lasted just five months and was marketed via media, used advertisements and information campaigns. A clear response rate difference was noted for age, as the SAMINOR 2 study recruited fewer young participants than the SAMINOR 1. However, the age distribution between the two SAMINOR studies was comparable among older participants (43–69 years of age) (Brustad et al., 2014). These factors may in sum have contributed additionally to the general downturn in participation rates in population-based health studies. Nevertheless, the number of participants with Sámi ethnicity in the SAMINOR 1 and 2 studies were 26.3% and 24.6%, respectively, which indicate small differences in the ethnic distribution.
We note that the retrospective recording of adverse childhood experiences are prone to recall biases as negative mood, chronic stressors or depression seem to increase the likelihood of reporting adverse events that would otherwise not have been reported (Colman et al., 2016). As the Colman study indicated that more agonizing events (e.g., sent away, or physical abuse) are particularly prone to underreporting by un-depressed and healthy participants, the reporting of both violence and boarding school in the present study may be biased. But this variability in biased reporting should go in both directions, i.e., up and down for people developing or remitting from a depressive episode, respectively. Given that the general change in depression from 2003/04 to 2012 was minor, the group-level outcomes that we base our conclusions on should be less affected by this possibility.
The longitudinal analysis was limited in terms of sample size as the subsample participating twice was low compared to the entire sample. This is a design limitation of the SAMINOR population study as the second study wave introduced new health topics and recruited new participants for epidemiological reasons. We consider this as a minor threat as the longitudinal analysis did not represent a core analysis, nor did it contradict the main cross-sectional findings.
Conclusions
This study among indigenous Sámi, minority Kven and majority Norwegians observed minor differences in the health and functional status between participants with and without a history of boarding school. When differences emerged, they generally disfavored the boarding participants. Boarding participants also reported more frequent experiences with discrimination, violence and unhealthier lifestyle (smoking), less education and a lower income level than the non-boarding participants. Adjustment (or statistical equation) of these differences nullified in many instances boarding/non-boarding differences. However, as these differences more likely represent the true state of affair rather than being caused by sampling error, these findings indicate the ideal outcome given equality in these health and socioeconomic issues. The present study thus partly converges with the international literature on health inequalities and highlights the risk of poorer health and socioeconomic outcomes following boarding school placement of indigenous or minority children. The study also highlights the negative and positive roles of violence and resilience as opposing dimensions that point out general important sources to vulnerability and protection in indigenous societies. An unexpected positive difference was seen with regard to well-being favoring the boarding participants. Attendance at boarding school during childhood is therefore not all black-and-white, as some children may benefit from it given their contextual living situation. Other findings of note were the protective role of a strong Sami identity, which implied better general health and well-being. These participants also functioned substantially better in terms of marked lower disability pension rates than the majority Norwegians. Facilitating processes that invigorate ethnic status, belonging, identity and pride seem solely positive for the development of an autonomous, healthy and active participation in working life.
Supplemental Material
Supplemental_Material – Supplemental material for Do Childhood Boarding School Experiences Predict Health, Well-Being and Disability Pension in Adults? A SAMINOR Study
Supplemental material, Supplemental_Material for Do Childhood Boarding School Experiences Predict Health, Well-Being and Disability Pension in Adults? A SAMINOR Study by Oddgeir Friborg, Tore Sørlie, Berit Schei, Cecilie Javo, Øystein Sørbye and Ketil Lenert Hansen in Journal of Cross-Cultural Psychology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.