
Abstract
Sexual violence by armed groups is common in civil wars. Qualitative studies have shown that victims and their families experience social stigmatization. Stigmatization is viewed as a central mechanism to social exclusion and disintegration impeding post-conflict social, political, and economic recovery. We provide new theory on the social conditions under which rape-related stigma intensifies and decreases. Drawing on an original population-based survey in eastern Democratic Republic of Congo, we find that victims and their families experience higher levels of stigma compared to unaffected families and these effects are dependent on community attitudes and norms. Furthermore, we find that humanitarian support interventions designed to address the social nature of stigma can reduce stigma. Our article significantly expands prior knowledge on a central mechanism in post-conflict recovery by providing a refined theory on wartime rape-related stigma and the role of humanitarian aid in mitigating negative effects based on representative data.
Introduction
Sexual violence is a widespread form of violence in civil wars (Wood 2006; Cohen 2013). How does wartime sexual violence, in particular rape by armed groups, affect victims, their families and communities? 1 In addition to physical consequences for victims, stigmatization is commonly viewed as an immediate adverse effect. Stigmatization is understood as a central mechanism that leads to social exclusion and community disintegration which can adversely affect trust, social networks, and cooperation. These qualities are important for post-conflict social, political, and economic recovery and it is therefore critical to understand the determinants of micro-level variation in social stigmatization in the context and aftermath of armed conflicts.
In this article, we develop a theory that describes the conditions under which rape by armed groups leads to stigma and how humanitarian aid programs might help to mitigate these adverse effects. We assess the observable implications with original representative survey data from eastern Democratic Republic of Congo (DRC). While our evidence is specific to eastern DRC, our theoretical contribution about the conditioning effects of the social context provides new and refined arguments that go beyond DRC and provide valuable future research avenues to scholars in peace and conflict research, gender studies, and social psychology.
During the last 10 years, there has been a surge of research on the micro-level consequences of armed conflicts. Many studies show that people’s exposure to violence is associated with prosocial behavior including social trust, political, and social engagement and cooperation (for an overview, see Bauer et al. 2016). Other studies show that wartime trauma is highly gendered and can lead to detrimental maternal health outcomes and increased levels of intimate partner violence (Østby et al., 2019; Urdal and Che 2013).
However, two limitations should be noted. First, studies on consequences of armed conflict rely on composite measures of violence exposure that include displacement, property destruction, loss of family members, and sexual violence. Few studies disaggregate forms of exposure to consider specific effects on post-conflict outcomes. 2 This is unfortunate, given variation in forms of violence across conflicts (Gutiérrez-Sanín and Wood 2017) and the need to tailor post-conflict humanitarian support interventions (Autesserre 2012; Koos 2017, 2018; Lindsey 2021).
Second, the mechanisms of how exposure to violence affects post-conflict outcomes are not sufficiently understood. While prior studies have sought to explain the emergence of prosocial behavior using concepts such as posttraumatic growth, there is little theorization of other mechanisms or the conditions under which prosocial behavior may emerge.
This article makes three contributions. (1) We address the first limitation by disaggregating people’s exposure to violence into three key categories: rape by armed groups (our main interest), homicide, and displacement. (2) We address the second limitation by focusing on stigmatization, an important but under-researched mechanism in the literature on the legacy of violence. Furthermore, we develop and test a refined theory that explains under which social conditions we should expect rape to increase or decrease stigmatization. (3) We test the observable implications with original survey data from eastern DRC, a well-suited case because of relatively high levels of sexual violence and local variation in the social context. It is also a case where establishing the effects of rape by armed groups and the effectiveness of efforts to reduce it in a representative sample can be particularly useful to advocacy and practitioner efforts.
Our first finding reflects what has been meticulously described in qualitative studies; household exposure to rape is significantly related to self-reported experiences of stigma. Our main analyses then build on this research by providing evidence of the social nature of stigma. We show that experienced stigma is moderated both by (1) the prevalence of community norms of blaming victims and (2) the prevalence of rape by armed groups in a community. A vignette experiment then provides causal evidence that (3) one distinct mechanism connecting rape by armed groups and stigma operates through social norms rather than fear of HIV/AIDS. Finally, we provide suggestive evidence that (4) a combination of humanitarian support interventions designed to address survivors’ social reintegration can reduce stigma.
Existing Research on the Legacy of Sexual Violence in Conflict
Wartime sexual violence has been shown to negatively affect the lives of victimized individuals in terms of physical and mental health, social relationships, and economic outcomes (Amowitz et al. 2002; Johnson et al. 2010; Longombe et al., 2008; Dumke et al. 2021). A robust qualitative literature has traced how such negative effects manifest in the lives of countless victims and their families, with particular attention to stigma (Woldetsadik 2018; Josse 2010). The secondary trauma of family and community rejection has even been described equitably to the first trauma of rape (Kelly et al. 2012). The consequences of wartime rape can extend beyond immediate victims. In Northern Uganda, Woldetsadik (2018) documents not only how female victims perceive continued hardships related to community stigma but also how secondary trauma impacts their families. This framework begins to approach the claim that rape not only affects individuals but tears apart the social fabric of societies, impacting entire communities. It is important to keep in mind that social disintegration can adversely impact communities’ collective action capacity and hamper post-conflict development.
Other channels through which wartime rape is thought to impact societies include fostering children of war, increasing impunity for perpetrators of rape, interrupting the marriage market, and spreading HIV (Boesten 2007; Carpenter 2007; Østby et al., 2019; Josse 2010). 3 However, many of these theorized repercussions depend on an implicit association with stigma (Koos 2017). For example, women with children born of rape face stigma that leads to lost economic opportunities, lack of access to education, and impediments to owning property (Carpenter 2007).
Such damaging social effects associated with rape raises questions for quantitative scholarship establishing that armed conflict has prosocial effects (Bauer et al. 2016). Do prosocial outcomes emerge in contexts where there are high levels of rape by armed groups? Koos (2018) finds that families affected by sexual violence become more socially engaged and altruistic in Sierra Leone. He suggests that affected households anticipate social exclusion and respond with efforts to overcome it. In this theory, it is the victim’s altruistic response to potential stigma that fosters resilience to sexual violence in the long-term. However, stigma remains a theorized but unexamined mechanism. In their study of sexual violence in Sri Lanka, Traunmüller et al. (2019, p. 2016–2019) suggest, but do not explicitly examine the relevance of stigma for learning about armed group targeting of sexual violence in different populations.
Kuwert et al. (2014) study whether sexual violence has unique effects on stigma among female victims of WWII by using a matched pair design to compare effects of sexual and non-sexual trauma. The findings are mixed. Women exposed to sexual trauma during WWII report greater posttraumatic growth but less social acknowledgment of their trauma. 4 In Uganda, a statistical study finds that exposure to rape during rebel captivity has negative repercussions for perceived stigma and functioning (Amone-P’Olak et al. 2016). However, this survey sample is specific to former female LRA combatants and relatively small.
Overall, stigmatization is viewed as a central mechanism in the qualitative literature on wartime sexual violence, but quantitative research on stigmatization remains limited. The few quantitative studies that assess the relationship between wartime sexual violence and post-conflict outcomes acknowledge the importance of stigma, but often do not provide a theoretical contribution about its role or examine stigma empirically.
A Theory of Rape by Armed Groups and Social Stigma
Stigma is both an individual and community-level attribute; it is felt by individuals and implemented by members of the society. Accordingly, there are two features of the effects of rape by armed groups that we examine in this study: (1) the effect of rape by armed groups on an individual’s experience of stigma and (2) the effect of others and their treatment of survivors.
Erving Goffman (1963) defines stigma as “an attribute that is deeply discrediting” and results in the reduction of a person or group “from a whole and usual person to a tainted, discounted one.” Following Goffman (1963) and Jones (1984), we define stigma as the relationship between an “attribute and a stereotype” where, stigma is a “mark that links an individual to an undesirable characteristic” (Link and Phelan 2001 p. 365). Stigma experiences include perceived incidents when a respondent has been gossiped about or excluded from community life (Kelly et al. 2012; Kelly et al. 2011). The process of stigmatization can thereby lead to polarization and social fractionalization within communities which can negatively affect social trust, cooperation and networks—all of which are important determinants of collective action potential and thus matter for post-conflict development.
Stigma can stem from many sources such as former combatant status, forced displacement, employment, membership in ethnic minority groups, as well as sexual violence (Mcmullin 2013; Dumke et al. 2021). Stigma associated with sexual violence is experienced by both male and female victims (Sivakumaran 2007). Stigma can also extend beyond the victimized individual him or herself (Woldetsadik 2018; Jina and Thomas 2013). When sexual violence is perpetrated against a man’s wife or daughter, he may be stigmatized because of his failure to protect his family members, an expectation highly relevant for men in DRC (Lindsey 2021). Community members may also ostracize a rape victim’s husband (and family) for failing to reject his wife (Kelly et al. 2012). Through such dynamics, stigma extends beyond victimized individuals, creating conditions that can divide and weaken communities.
Therefore, our first proposition suggests that rape by armed groups has implications for those that have been directly victimized as well as other household members (that have not been directly victimized) in a representative sample of the population.
Since stigma is a social phenomenon, the likelihood that an individual experiences stigma as a result of rape in the household will also be dependent upon community-level factors.
Norms, defined as beliefs about how others in a community think one does or should behave, determine the extent to which a characteristic (such as exposure to rape) is “undesirable” and thus something that fellow community members will stigmatize. Behind the perception that victims hold an “undesirable” characteristic is the belief that victims are (at least in part) to blame for rape and are thus complicit in violating a social norm. Victim-blaming is not constrained to the DRC context and is acknowledged as one component of “rape culture” that decreases both rape reporting and its investigation (Baum et al., 2018).
Even when it is very difficult for society members to blame a woman’s dress or habits for her victimization, community members may still ostracize a woman that has been raped because of beliefs that the victim is to blame for violating community norms of sexual fidelity. Qualitative evidence from eastern DRC suggests that rape victims experience stigma similar to that associated with female adulterers (Kelly et al. 2011). Male victims, on the other hand, are often blamed for violating the norm of heteronormative sexual behavior due to being victimized by other men (Sivakumaran 2007). We argue that the perception that victims have violated community norms foments divisions between norm upholders and norm violators—between those that stigmatize and are stigmatized.
In order for individuals to be stigmatized, there must be a “mark,” meaning people must “see” or know about this undesirable attribute. 5 Because rape by armed groups tends to be brutal, public, and marked by multiple-perpetrator rape (Wood 2014), rape becomes more difficult to hide from the public view. Even when rape occurs in private, victims will often seek medical assistance due to its extreme brutality and will thus be unable to hide the event from neighbors, family, and friends.
If stigma occurs because of a perceived violation of community norms (e.g., of sexual fidelity and heterosexuality), people will stigmatize rape victims more in communities where there are high levels of victim-blaming. Thus, the effect of rape on experiences of stigma will be amplified in communities where a higher proportion of respondents (other than the victimized individual him or herself) believes that the woman is to blame for rape.
However, there are important limits to how much and how many victims a community can ostracize. To sustain itself, a community subjected to mass rape will need to adapt to the circumstance and accept and integrate victimized members as part of the community. By evolutionary logic of necessity, at any point in time, only a certain threshold of people can be ostracized through tactics such as gossip, social isolation, and expulsion for society to function; and communities will not continue to uphold norms when it impedes their collective integrity and cohesion.
Because armed conflict often features higher levels of sexual violence in a consolidated period of time (Wood 2014, 464), the social effects of wartime rape might differ from other contexts of sexual violence in structural ways. When a high percentage of individuals are raped and the community knows about it, there may be greater acceptance of survivors.
By this evolutionary logic of necessity, the relationship between rape by armed groups and stigma within any community will depend on the proportion of people in a community that have been exposed to rape. We suggest that the likelihood that any exposed individual (or their fellow household members) will experience stigma will decrease as more households within a community are exposed to rape. 6
What leads people to stigmatize those within their communities that have been exposed to rape? While we have proposed a social norms framework, other frameworks suggest that communities stigmatize victims because of fear of HIV/AIDS rather than norms. An investigation of how focus group participants explained their stigmatization of individuals with HIV/AIDS in South Africa provides evidence that fear can drive stigma (Campbell et al., 2007). In DRC, focus group respondents also describe HIV/AIDS as an important component of choosing to accept or reject victimized family members (Kelly et al. 2012).
Fear and norms can be mutually reinforcing, where norms are further bolstered by perceived health risks posed by AIDS infection to families and communities of survivors. Yet, the mechanism is important to tease out, because a norms mechanism suggests that interventions should seek to change norms; but a fear mechanism suggests that interventions should target the misinformation that bolsters fear.
The norms-based theory of stigma suggests that victimized individuals will be ostracized, even when there is no accompanying fear of a health risk. We use a vignette experiment to differentiate fear mechanisms from norms mechanisms in order to learn about people’s subconscious motivations for choosing to stigmatize victims of rape. If social norms are a central source of stigmatization and distinct from fear of HIV/AIDS, information about a victim’s HIV-negative status should not affect stigmatization compared to no information about a victim’s HIV status.
If rape increases a household’s experience of stigma, is there an effective way to mitigate stigma through humanitarian support? We examine several common designs of humanitarian interventions that seek to mitigate the harmful impacts of wartime rape.
Victim-centered interventions take the individual, his or her spouse, and family as the focal point for mitigating harmful effects of rape. For instance, individual counseling seeks to address the trauma experienced by rape victims by helping victims to overcome psychological effects such as PTSD, fear and depression. Victims of rape may also become directly involved in community sensibilization programs that work to mitigate harms of stigma that victims experience.
Rather than working with victims directly, some community-level programs and practices seek to reduce stigma by altering gender norms within the community and promoting norms of reconciliation and inclusion. These interventions target the behavior of norm implementers (people that stigmatize others) and, sometimes, the norms themselves rather than providing tools for victims to cope with ostracization.
Our understanding of the social nature of stigma leads us to believe that such community-level interventions will be most effective in reducing stigma experienced by victims, because they focus on potential stigmatizers and thus the source of stigma. Victim-centered interventions such as counseling will be less effective because they focus on stigmatizers less directly. Other common victim-centered interventions such as income-generation (e.g., skills training) may help rape victims to reintegrate in society and overcome joblessness associated with injury. However, this type of program does not address the social nature of stigma so will be unlikely to affect stigma.
Context
Before turning to our research design, we introduce the context and conditions in which we assess our theory of stigmatization. Our study focuses on eastern DRC where rape by armed groups has been widespread and perpetrated by all parties to the ongoing conflict. Rape by armed groups in this context also takes place alongside a range of other abuses against civilians, including displacement. It is thus informative to examine its effects on stigma, taking other abuses as potential sources of stigma under consideration. Finally, DRC is a context where numerous humanitarian actors seek to address harmful effects of sexual violence and where we can learn about the effectiveness of different forms of programming.
Armed Conflict and Rape in the DRC
The wars and the continuing armed conflict in its eastern regions have generated massive displacement and high levels of human suffering, including an estimated loss of over 2 million lives (Human Security Report Project 2011, 131).
The First Congo War erupted in 1994, following displacement of the Rwandese population as Hutu genocidaires and others fled across the border into Congolese territory. The Second Congo War followed closely thereafter, with numerous international and domestic actors taking up arms in the regions. While the second war officially ended with a peace agreement in 2002, local violence has continued in North and South Kivu.
As North and South Kivu have been militarized by ever changing networks of ethnic and political loyalties, violence against civilians has become an increasingly dominant tactic used by parties to the war (Autesserre 2009). Armed groups, militias and the military have all committed acts of mass rape, described as a vicious cycle of sexualized violence aiming to terrorize, humiliate and displace the civilian population (Bartels et al. 2010). Interviews with soldiers and militia members explain acts of rape in terms of biological urges such as “lust,” “needs” as well as domination and “othering” ethnic rivals (Ingelaere and Wilén 2017; Eriksson Baaz and Stern 2009).
Rape and Stigma in the DRC
In eastern DRC, as in many traditional societies, there is significant inequality between the sexes. Women are viewed as a form of property, where fidelity is linked to a woman’s value. Victims of rape describe the logic behind stigma that they experience in terms of marriageability, harm to husbands and losing value (Kelly et al. 2012). The brutality of rape (e.g., public rape, multiple-perpetrator rape, and object rape) directly attacked these norms and combined with fear of HIV/Aids to reinforce stigma and its consequences.
Rich qualitative evidence from eastern DRC shows that stigma has severely impacted the lives of victims and their families, particularly those admitted at medical facilities in South Kivu (Kelly et al. 2011; Kelly et al. 2012). The same literature has also revealed the importance of community norms in determining when someone is stigmatized by communities or rejected from their families. But questions remain about the generalizability of these accounts to the wider population. Victim-blaming is treated as homogenous in focus group settings, leaving variation across communities unexplored. We examine whether and why rape transmits these effects in some communities more than others, providing insights into uncharted variation in rape prevalence and victim-blaming attitudes.
Humanitarian Interventions against Rape and Stigma
Humanitarian agencies have launched programs to assist rape victims with medical and psychosocial support. A number of hospitals such as Panzi Hospital in Bukavu and Heal Africa in Goma have helped thousands of women to overcome physical damage to their bodies and supported them as best as possible to regain control over their lives (Albutt et al. 2017; Bartels et al. 2010). For example, in a randomized controlled trial implemented in a few villages in eastern DRC, Bass et al. (2013) find that a group psychotherapy intervention was effective in reducing PTSD and anxiety while increasing people’s perceived ability to accomplish tasks. In another evaluation, Amisi et al. (2018) find that support programs by the Panzi hospital in Bukavu increased economic and social well-being of sexual violence survivors.
Studies about experiences and effectiveness of care largely report about victims who have been admitted to NGO support facilities (see, e.g., Bartels et al. 2010; Albutt et al. 2017; Kelly et al. 2012; Kelly et al. 2011), which remain out of reach to much of the population. Our study, being independent and conducted with a representative population sample, removes immediate threats to inference presented by sample selection bias. Being conducted outside the environment of a specific program also helps to address issues of social desirability bias in many onsite program evaluations.
Research Design
Ethical Aspects
Research with vulnerable populations in conflict contexts and with victims of violence requires rigorous safeguards to ensure the interests, rights and well-being of respondents, enumerators and local research assistants. This research would not be possible without the invaluable contributions from many local research assistants of Research Initiatives for Social Development in Bukavu. Enumerators provided full disclosure to potential respondents that the survey would include sensitive questions about experiences of violence, including sexual violence, prior to obtaining respondent consent to take part in the survey. Then, the outset of each violence module included a pause in which respondents were asked if they were comfortable to continue, preferred to pause or quit. Due to the sensitive and emotional nature of the subjects being discussed, two local gender experts from an international NGO (a) contributed valuable feedback to contextualize and adapt the survey instrument and (b) conducted an enumerator training about how to listen, empathize, and support respondents throughout the survey and after. Attention was also paid to enumerators in light of trauma that may be incurred from engaging in discussions. A full discussion of ethical aspects of the design and implementation of the project is found in section A1 in the online appendix.
Survey
To gather data on the relationship between rape by armed groups and stigmatization as well as the moderating social effects, we administered a survey to a random sample of 1000 respondents (in 100 randomly sampled villages) in South Kivu, eastern DRC (see Figure 1).
7
This research took place between February and March 2017 and was not associated with an evaluation of existing programs. It thereby warrants a high degree of academic independence. We employed a multistage cluster sampling protocol which is explained in detail in section A2 in the appendix. Map of Survey Locations in South Kivu. Note: Borders identify the territoires in South Kivu (Territoire Shabunda is excluded). The little crosses indicate survey locations. Rough terrain indicates mountain ranges and dense jungle areas with low population density.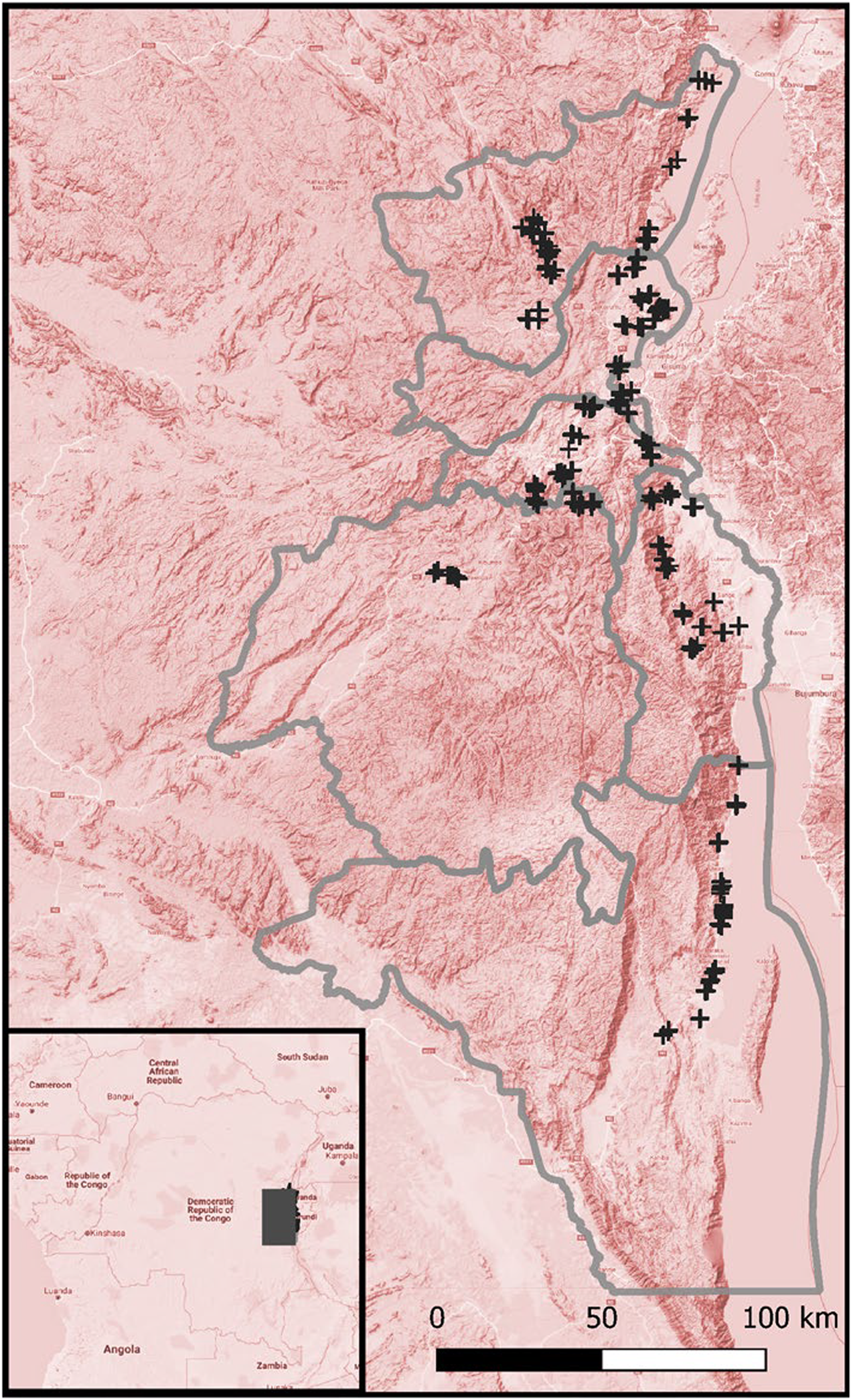
The sample was equally split between female and male respondents. About 10 percent of the sampled villages were replaced due to security reasons, mostly because of ongoing fighting and abandonment of villages. 8 Therefore, our sample leans more towards villages that, at the time of the survey, were sufficiently safe. This is common among surveys in conflict-affected contexts, but such selection effects could influence our results. We assess the potential of village selection to affect the survey’s representativeness and our study’s results when introducing our measurement of rape by armed groups in the following section.
Operationalization and Variables
To measure our dependent variable, stigma experience, we calculate the mean response of each respondent to two stigmatization questions. These questions are drawn from studies of HIV-related stigma (Stangl et al., 2012). 1. In the last 12 months, how often have you been aware of being gossiped about? 2. In the last 12 months, how often have you been excluded from social gatherings or activities?
We suggest that victim awareness of gossip and knowledge of exclusion (rather than actual levels) represent the felt components of stigma that we highlight in our theory. Responses are coded on a 4-point scale, including never (0), a few times a year (1), monthly (2), and weekly (3). Note that the questions do not ask whether the respondent experienced stigmatization due to rape; this allows us to include stigma from other sources such as displacement or poverty. Figure 2 shows that over half of the respondents reported stigma experience at least a few times in the last 12 months. The mean value of stigma experience is 0.776 (±0.91). Distribution of stigmatization variable.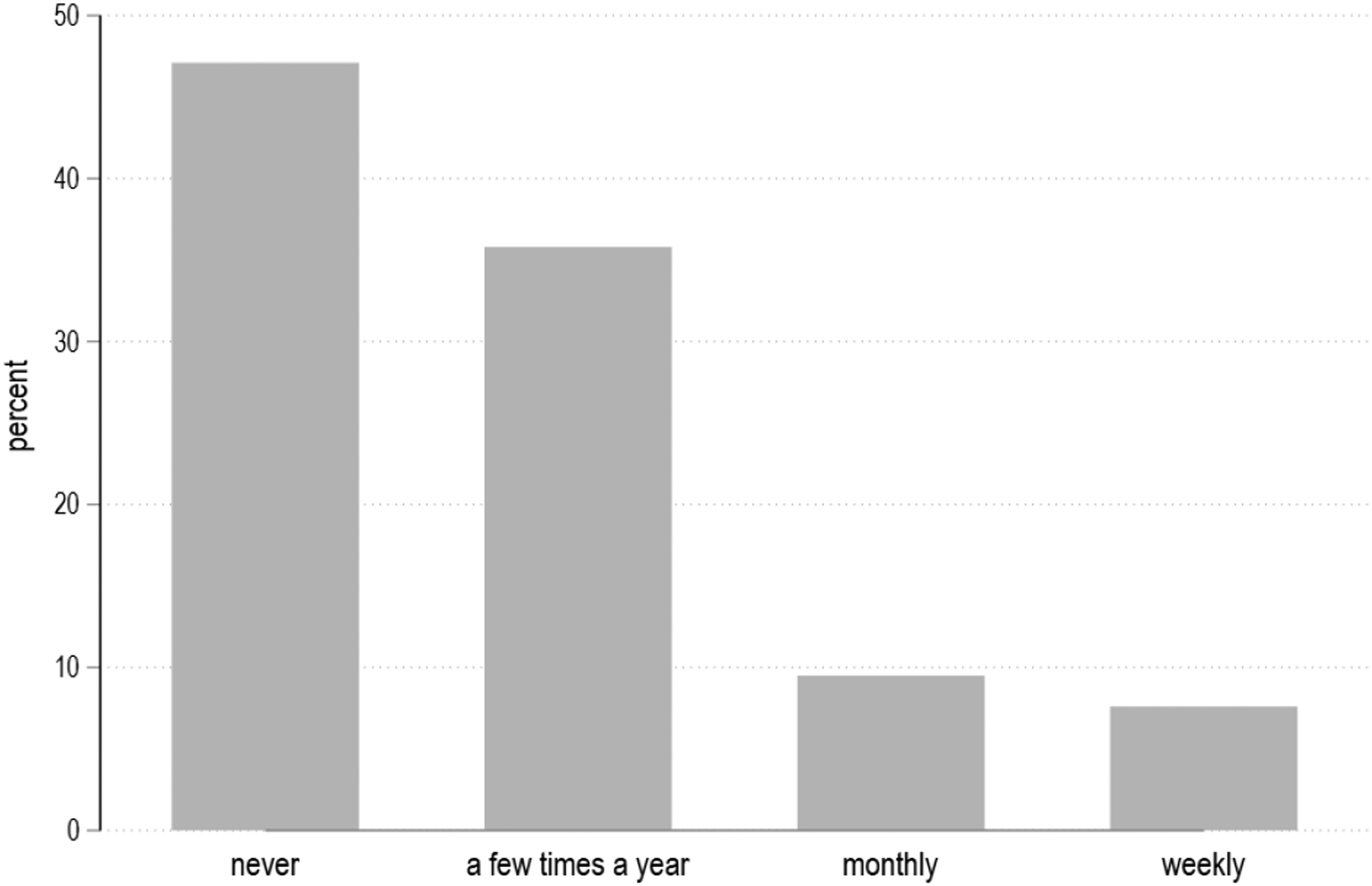
To operationalize our independent variable, exposure to rape by armed groups, respondents were asked whether they or anyone else in their household had been raped by armed groups since 2002. The survey instrument defined rape as being physically forced to have sexual intercourse. Out of 1000 respondents, 6.8 percent report that someone from their household has been raped by members of armed groups.
Because we had to replace 10 percent of sampled villages due to insecurity, our survey is likely to underestimate the prevalence of rape in the population of South Kivu. The estimated prevalence rate of rape by armed groups is 5.5 percent in villages that reported no violent events between 2015 and 2017 (based on our village survey), 7.89 percent in villages with one to ten violent events, and 13.3 percent in villages with more than 11 events.
However, we do not believe that this affects our estimation of the effect of rape on stigma. Our existing data suggest that replacing currently unsafe villages with currently safer ones would change both the incidence of rape by armed groups and the reported levels of stigma. Average levels of stigma are 0.71 in villages with no violent events, 0.79 in villages with one to ten violent events, and 1.22 in villages with 11 or more violent events. Our central analysis of H1 also employs village-level fixed effects, making sure that we only compare variation of rape and its effect on stigma within the same village.
Another concern is that social desirability bias could lead to underreporting of rape, meaning that true prevalence of rape by armed groups is higher than measured here. 9 The majority (78 percent) of respondents reporting household rape exposure noted that the incident had occurred publicly or that community members knew about it already. This suggests that the tendency to report rape exposure in the survey is linked to public knowledge of rape. A focus on public rape is appropriate for our study because the stigmatization by community members is only possible if community members know about it in the first place. We do not suggest that rape outside the public eye results in less suffering, but the social implications for victims and their families examined here are contingent on the fact that other community members know about it.
Moreover, under or over-reporting of rape by armed groups would likely understate our findings. If an individual chooses not to report rape exposure but does choose to report stigma, that will decrease the likelihood of finding a statistically significant correlation. If stigma is the reason that people do not report household exposure to rape by armed groups, then this would also bias against statistically significant findings.
We observe gendered reporting patterns in our measure of rape. Of households reporting exposure, 59 percent are female and 41 percent are male respondents. Section A3 of the online appendix provides further analysis of this gendered difference. We account for gendered reporting differences in our full models by including controls for respondent sex and by testing whether the effect of rape on stigmatization is moderated by gender. Through control variables and coarsened exact matching, we emphasize the comparison of female with female respondent households and male with male respondent households. If male respondents tend to underreport more than female respondents, as indicated in the data, we may be less likely to find a relationship between household rape among male respondents than female respondents. Differential findings between men and women require careful interpretation.
The estimated prevalence rates of rape also differ significantly by territoire (i.e., the first administrative level below the province). In Kabare, 1.7 percent report rape by armed groups, whereas in Kalehe the rate is at 11.9 percent. Other territories have values between 4 percent and 7 percent. These differences are accounted for through territoire or village fixed effects in our models.
Beyond considering our independent variable and its measurement, the models that we employ aim to estimate the effect of rape by armed groups on experienced stigmatization. Therefore, our conditioning strategy and the selection of control variables aim to block the backdoor paths—that is, non-causal associations—between our explanatory variable rape and stigmatization (Morgan and Winship 2014; Pearl 2009).
In armed conflict, many forms of violence and potentially stigma-inducing experiences occur simultaneously. To help isolate the effect of rape by armed groups from other conflict-related experiences, we include variables on whether a household member has been murdered (homicide) or whether the household has been displaced (displaced). 10
In DRC, rape victims are often sent away from their homes and subsequently accepted in other households. To account for this potential transfer of stigma across households, we include variables based on questions asking respondents whether a member of their household has been expelled (expulsion) or taken in recently (integration). 11
Finally, to begin accounting for variables that may determine both reporting of and exposure to rape by armed groups that may simultaneously be determinants of stigma, we include controls for age, sex (female), and education of the respondent, household size and economic status (assets) in our basic models. We also control for respondents’ prior survey participation experience since this has been shown to affect response patterns (De Juan and Koos 2021). 12 Summary statistics are available in Supplemental Table A1 and the survey questions are described in section A4 in the appendix.
Assumptions and Evidence on Causal Identification
Because our analysis aims to estimate the effect of rape by armed groups on stigmatization, its validity rests on the assumption that no omitted variables such as stigmatization or social exclusion prior to victimization make people and households more likely to be victims of rape in the first place. Because our data are observational and cross-sectional in nature, we cannot directly make this causal claim. 13
We account for this in three ways. First, we include the aforementioned control variables which may simultaneously predict both the likelihood of exposure to rape (e.g., targeting by armed groups) as well as experiences of stigma. Second, we provide evidence that speaks against selection effects of rape exposure and suggests a degree of randomness. We conduct a balance check to compare the mean values of demographic and socioeconomic variables between rape-affected and unaffected households. Supplemental Table A2 in the appendix shows that across a wide range of socioeconomic variables there are no statistically significant differences between rape-affected and unaffected households.
Other studies on sexual violence in eastern Congo lend further support to the near-random pattern of rape victimization. Bartels et al. (2010, 5) study 1021 records from Panzi Hospital in Bukavu, a major referral hospital in the area, and find no distinct patterns among rape victims. They observe that rape “affects young, old, single, married, divorced, and widowed women. It affects the educated and the uneducated, as well as women of different occupations and different ethnicities.” In another study, Peterman et al. (2011) analyze Demographic and Health Survey (DHS) data and find that reports of sexual violence were independent of individual-level characteristics.
As an additional source of information, our survey asked chiefs and administrators of the 100 sampled villages in South Kivu which households they believe are usually targeted in attacks involving rape by armed groups. 61 percent answered that it is “almost random,” 34 percent said “those along the road,” 18 percent agreed with “those near the center of the village,” whereas 21 percent “those far away from the center.” 44 percent said that “rich households” are targeted and 12 percent said “poor households” are targeted (multiple responses were allowed). While most chiefs agreed with the “random” victimization notion, the other responses do not indicate a distinct victimization pattern.
Third, we conduct a sensitivity analysis (Cinelli and Hazlett 2020) to quantify how large a confounder would need to be to overturn our finding that rape increases the experience of stigmatization. We provide this analysis in the online appendix in Supplemental Figure A5. Using the female variable as one of the most powerful predictors in our model as a benchmark, we find that even a confounder three times as large as the female variable only insignificantly changes the effect of rape on stigma. This further strengthens our confidence that the models estimate the effect of rape by armed groups rather than other (omitted) factors.
Analysis
Before analyzing the data, we employ the coarsened exact matching (CEM) algorithm to create more balanced data between rape-affected and unaffected households. CEM removes observations from the data for which there is no common empirical support on the covariates between rape-affected and unaffected households. Through this procedure the distribution of the covariates in both rape-affected and unaffected households is more alike, and thus reduces model dependence and statistical bias (Iacus et al., 2012; Blackwell et al. 2009).
We match our data on age categories (18–30, 31–45, 46–60, 60+ years), education levels (no education at all, primary school, above primary school), gender and pre-exposure social activity levels (low vs. high activity) as reported in the survey. We lose 175 (unaffected) observations due to a lack of common empirical support. Consequently, the L1 statistic as a measure of overall imbalance improves from 0.63 to 0.53. Due to the decrease of observations in the CEM sample, the prevalence of rape increases to 8.2 percent compared to 6.8 percent in the unbalanced data.
Since our dependent variable measures the frequency of experienced stigma and has a left-hand skewed overdispersion (see Figure 2), we employ negative binomial models with standard errors clustered at the village level.
We assess our hypotheses in turn. H1 suggests that exposure to rape by armed groups within the household increases experiences of stigma. Figure 3 shows a marginal effect plot where we present three specifications: (a) the bivariate relationship between rape and stigma, (b) a basic model with demographic controls including gender, age, education, household size and assets and (c) the full model including violence-related controls to isolate the effect of rape from other experiences of violence.
14
The plot shows that rape has a significant positive effect consistent across all models. Exposure to rape increases the frequency of experienced stigmatization by about 0.3 on the 4-point scale. The effect size is comparable to that of female, which means that female respondents in households that have not experienced rape by armed groups—experience stigmatization as widely as men in households that have been exposed to rape by armed groups. Women, in general, seem to experience more stigma. Again, however, differential findings between men and women should not be overstated since such differences may reflect differences in reporting of rape and/or stigma. Average marginal effects of rape on experienced stigmatization (H1). Note: The dependent variable measures experienced stigmatization on a 4-point scale. All panels (a) to (c) present average marginal effects with point estimates and 95 percent confidence intervals. All estimations rely on a negative binomial link function and standard errors clustered at the village level. For each panel (a) to (c), we estimate either territoire or village fixed effects (see legend).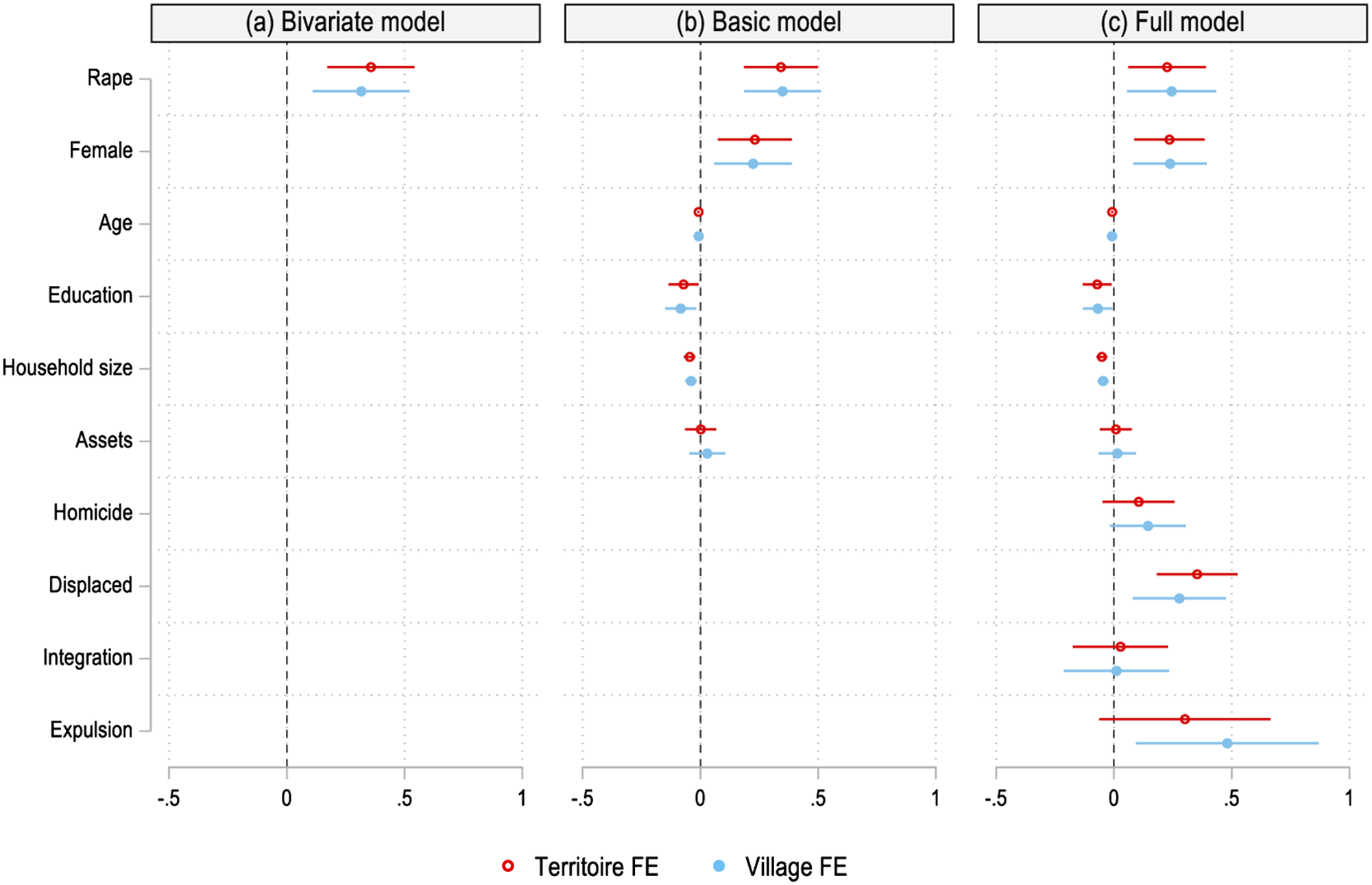
In model (c) we include other violence-related variables. As in previous models, a household member’s exposure to rape increases experiences of stigma. It is noteworthy that displacement has a similarly strong effect on stigmatization. This similarity may be due to local understandings that displaced populations are more likely to have been subjected to rape and infected with HIV/AIDS (Spiegel 2004). The statistical association could also reflect that displaced people have lived in the community only briefly so are more often discriminated against (Jacobs and Kyamusugulwa 2018).
The same analysis shows that respondents belonging to households which have expelled a household member recently (expulsion), report higher levels of stigmatization. On the other hand, taking in or accepting an outside person into the household (integration) does not affect stigmatization. These variables are included to assess spillovers of stigma as household members may have been sent away from former families and integrated in others. While we cannot confirm whether the expelled or integrated person was a victim of rape, the analysis suggests that expelling a victim might not end stigmatization for members of the remaining household. This finding counters previous accounts that suggest households rejecting rape victims can get rid of household-level stigmatization (see, e.g., Albutt et al. 2017).
Next, we turn to H2, which begins our examination of the social roots of stigma. H2 suggests that the prevalence of victim blaming in a community will amplify the harmful effect of rape by armed groups on stigma. To assess this proposition, we use an attitudinal question asked of all respondents (not only rape-affected households) about the degree to which they agree with the statement: When a woman was raped, she usually will have done something careless to put herself in that situation.
15
We then calculate an individually-varying village measure of victim-blaming, by taking the mean response value to this question within each of the 100 villages but exclude the respondent’s response.
16
The average level of victim blaming approximates a normal distribution with a mean value of 1.80 indicating disagreement with victim blaming (see underlying density plot in Figure 4). Effect of rape on stigma conditional on victim blaming norms (H2). Note: The line represents the predicted point estimates and the gray area 90 percent confidence intervals of the marginal effect of rape on experienced stigmatization (left y-axis) conditional on the average level of victim blaming norms in a village (x-axis). The underlying density plot shows the distribution of victim blaming norms (right y-axis).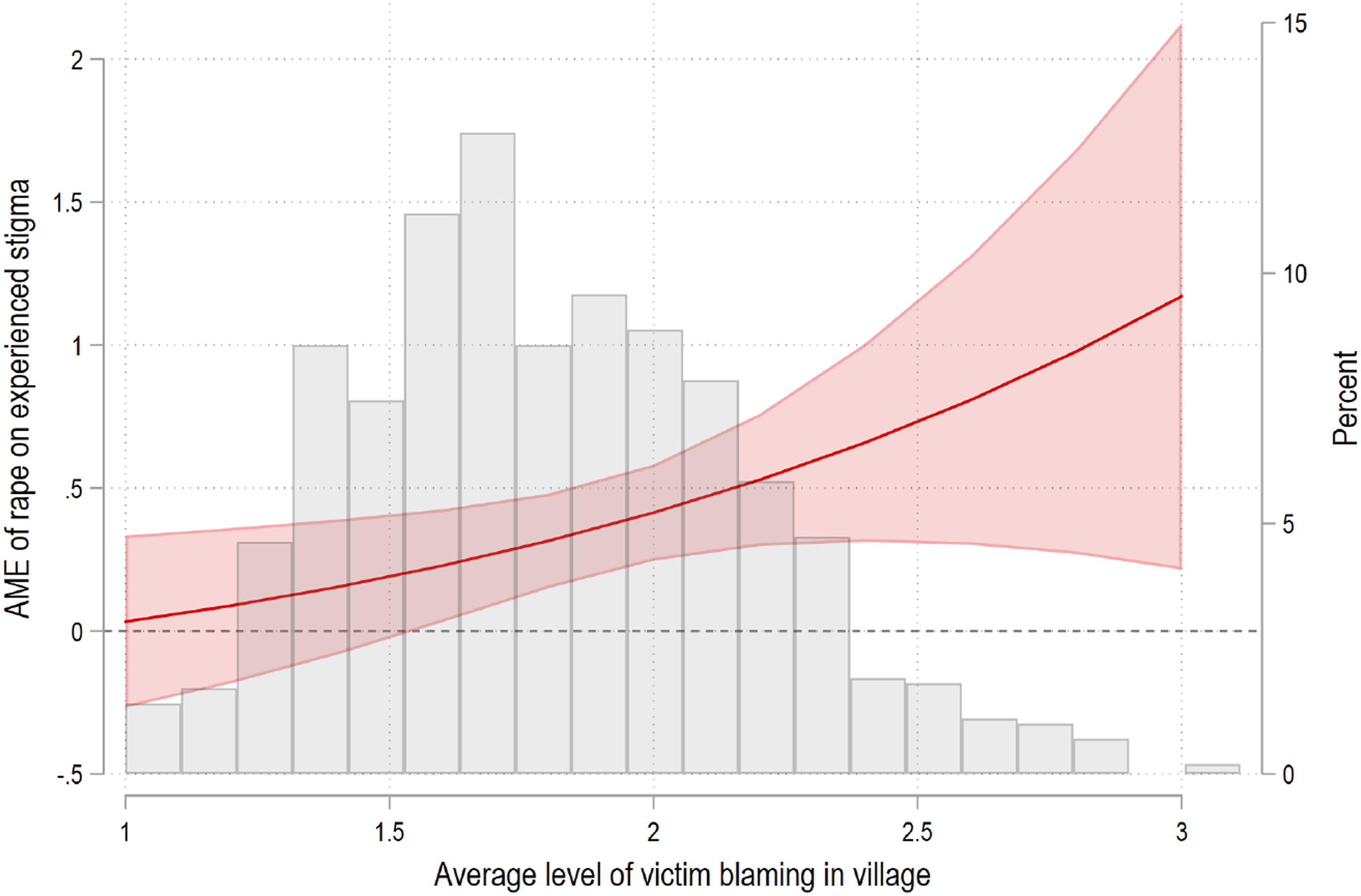
We then regress the dependent variable, experienced stigma, on the interaction of household rape and the village-level average of victim blaming as well as the control variables used in model (c) in Figure 3. Figure 4 below shows the marginal effect of household rape exposure on experienced stigmatization conditional on the village-level average of victim blaming. 17 The results indicate that the effect of household exposure to rape on individual experiences of stigma is indistinguishable from unaffected households in villages with low rates of victim blaming. However, once victim blaming increases beyond a threshold of 1.6, rape by armed groups has a substantive effect on stigmatization. At higher levels of victim blaming the confidence intervals get larger due to fewer observations (see underlying density plot), but the results still suggest the same upward trend.
To what extent is there attitudinal consensus about blaming victims in each village? We examine the extent to which village-level consensus on victim blaming, measured as the standard deviation within the sample of village respondents, moderates the effect of rape on stigma. Supplemental Figure A3 in the online appendix shows that as the standard deviation in victim blaming increases (i.e., less consensus), the effect of rape on stigma also increases. Note that there is a moderate positive correlation (r=0.42) between the village-level mean and the standard deviation in victim blaming. Supplemental Figure A4 shows that high-consensus villages have lower average levels of victim blaming norms than low-consensus villages. These results may indicate that a small share of victim blamers may suffice to intensify individuals’ experiences of stigma and that humanitarian support interventions might be most effective by strengthening collective reflection on gender attitudes and norms. We consider this more directly in our analyses of different forms humanitarian assistance (H5).
Linking these results back to our theory (H2), we find support for the argument that higher levels of victim blaming attitudes in a community amplify stigmatization of rape-affected households. 18
Continuing with the analysis of community dynamics and its effect on stigmatization, H3 suggests that increased presence of other rape victims within communities will change the relationship between rape by armed groups and stigmatization. The logic is that for societies and communities to function, only a certain share of members can be ostracized. To examine this hypothesis, we calculate the village-level prevalence based on reported exposure to rape by armed groups in the household-level survey (density plot shown in Figure 5).
19
According to this measure the village-level prevalence varies between 0 and 33 percent (mean: 6.8 percent). Effect of rape on stigma conditional on village-level rape prevalence (H3). Note: The black line represents the predicted point estimates and the gray area 90 percent confidence intervals of the marginal effect of rape on experienced stigmatization (left y-axis) conditional on the percentage of rape victims per village (x-axis). The underlying density plot shows the distribution of village-level prevalence of rape victims (right y-axis).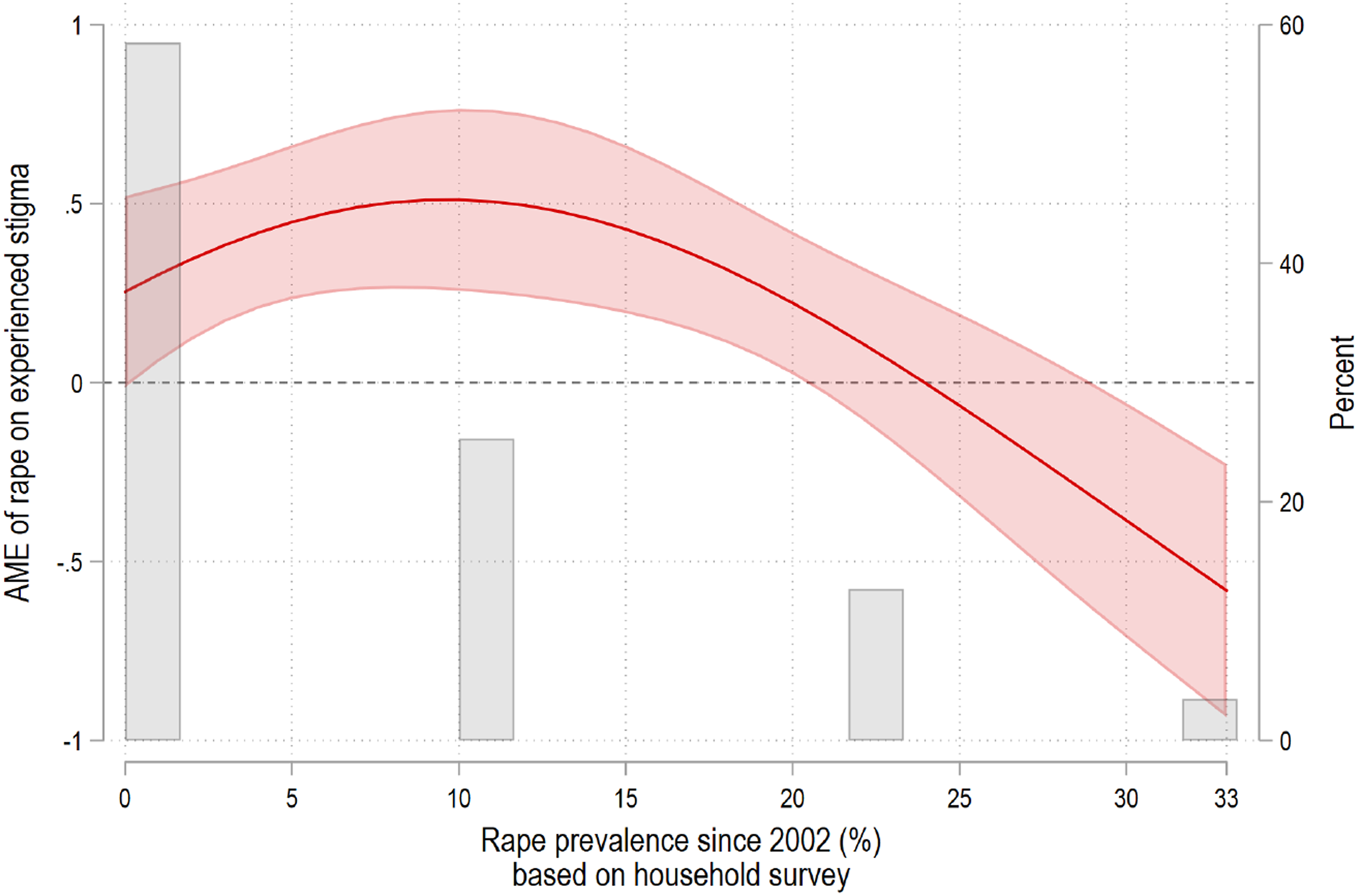
Figure 5 depicts the marginal effect of rape exposure on stigma conditional on the share of rape-affected households per village. The inverted U-shaped curve suggests that the marginal effect of household-level exposure is significantly associated with higher levels of stigma in villages with a rape prevalence of up to 20 percent. Above 20 percent of village-level prevalence, the effect of rape on stigmatization is either insignificant or even negative. 20 While this empirical pattern supports hypothesis 3, that is, that the effect of rape tapers off when more people in a community have become victims, we are cautious about the negative effect at prevalence rates of about 30 percent since this applies to few villages. 21
H4 explores the roots of stigma by examining the extent to which community norms drive stigma by isolating the norms mechanism from fear of HIV/AIDS. Because respondents themselves are often not cognizant of whether fear or norms drive behavior, we use a vignette experiment embedded in the household survey to probe whether information about the HIV status of a victim of rape changes people’s stigmatizing responses towards victimized individuals. The control condition provides no information on HIV/AIDS and closely approximates the people’s situation on the ground where normative pressures and health-related fear are not differentiable.
Our emphasis on the role of norms in driving stigma suggests that the control condition and HIV-negative information conditions will look similar—and demonstrate that rejection is driven substantively by norms, as distinct from fear of HIV/AIDS. The HIV-positive information condition presents a scenario in which health-related fear likely dominates the stigmatizing response. Each respondent was randomly assigned to the control or one of the two treatment conditions:
Control condition
The wife of a dear family friend of yours was raped publicly by several militia members. Many people in the community saw this horrific event. Her husband is torn between keeping her and rejecting her.
Treatment 1 (HIV-positive)
The wife of a dear family friend of yours was raped publicly by several militia members. Many people in the community saw this horrific event. Her husband is torn between keeping her and rejecting her. The raped wife has done an HIV/AIDS test. The test confirms that she is infected. She does have HIV/AIDS. 22
Treatment 2 (HIV-negative)
The wife of a dear family friend of yours was raped publicly by several militia members. Many people in the community saw this horrific event. Her husband is torn between keeping her and rejecting her. The raped wife has done an HIV/AIDS test. The test confirms that she is not infected. She does not have HIV/AIDS.
After receiving this information, respondents are asked which advice they would give their family friend: (1) to keep and support or (2) to separate from his wife. Figure 6 presents the share of respondents in each of the three conditions who advise their friend to separate from his wife.
23
In the control condition, 6 percent of respondents would advise their friend to separate from his wife. Under treatment 1 (HIV-pos) 29 percent of the respondents advise separation. Under treatment 2 (HIV-neg) 7 percent support separation. While knowledge of a victim’s HIV-positive status has a large effect on separation as compared to control, knowledge of a victim’s HIV-negative status has no effect on recommendations for separation as compared to control. The latter comparison provides suggestive support for H4: social norms are relevant for explaining stigma independently of HIV-related fear. Because the control condition reflects standard situations in DRC where the HIV status of a rape victim is largely unknown, the results also indirectly support the notion that social norms are primary determinants of stigma in this case. Vignette experiment on fear of HIV (H4). Note: Each bar indicates the treatment/control condition (x-axis) and the height represents the percentage of respondents in that condition who would advise their friend to separate from his wife (y-axis). Respondents have been randomly assigned to one of the three conditions.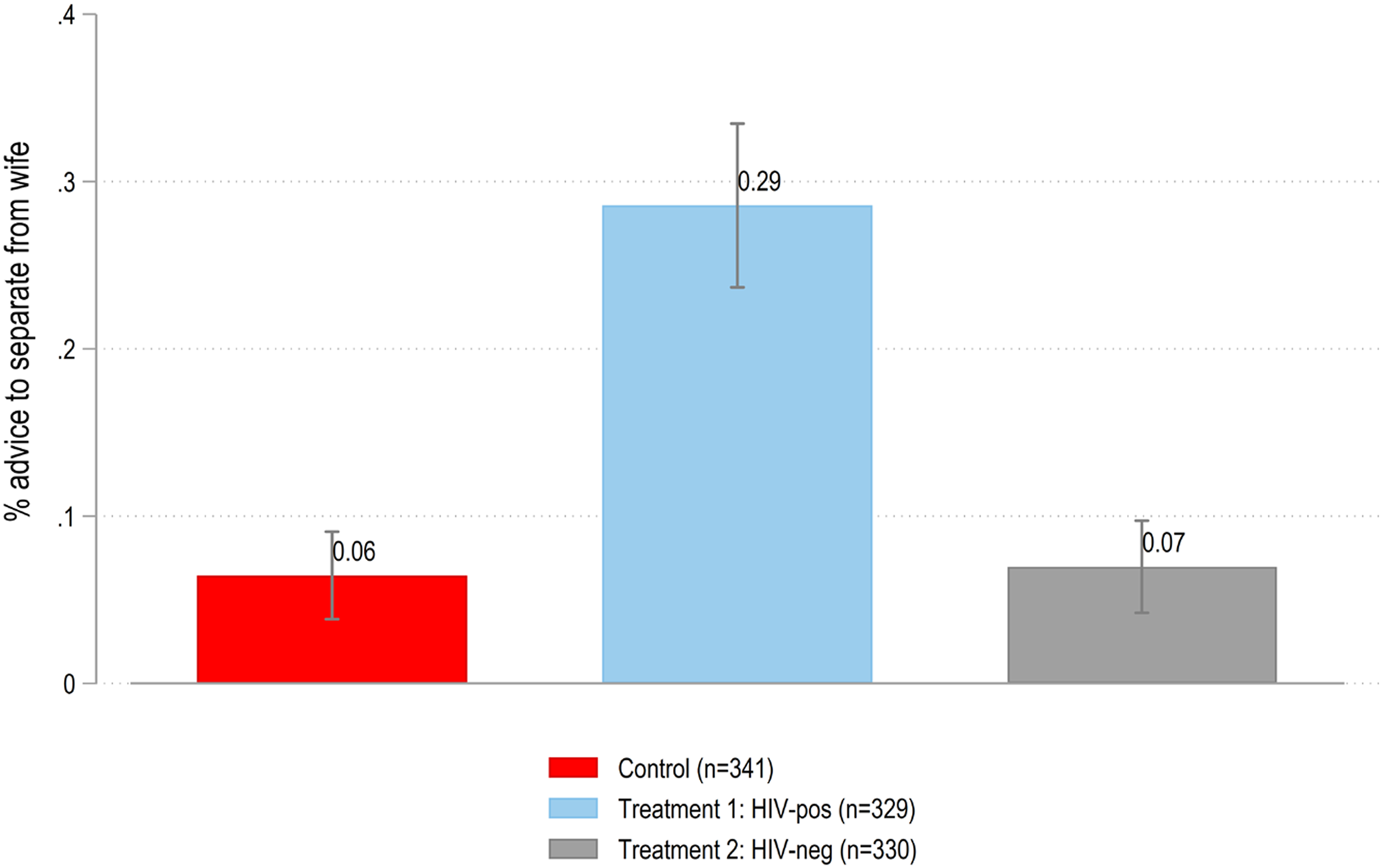
Finally, we turn to H5 which furthers our inquiry into the social nature of stigma by examining whether experienced stigma can be mitigated through different types of humanitarian support interventions. First, we consider whether household members have taken part in individual or family counseling (household interventions), which can be categorized as victim-centered interventions that are geared towards addressing the “felt” social aspect of stigma within a victim’s immediate social circle. 24 Second, we draw from a village-level indicator of whether gender norms campaigns have been implemented in the village more broadly (community interventions). 25 Community-level interventions intend to reduce stigmatizing behaviors by changing attitudes and norms among community members broadly. Third, for comparison, we also look at respondent participation in programs such as skills training that focus on income-generating activities (income interventions). Our depiction of stigma as the product of social factors suggests that community norms interventions will be most valuable in addressing stigma.
Figure 7 plots the marginal effect of rape exposure on stigma conditional on whether the respondent or a household member participated in specific support interventions.
26
The models include individual-level control variables as in previous models, groupement fixed effects and match on the same covariates as in the main analysis using CEM; however, differences in what drives individuals to select into different intervention types likely still exists.
27
We do not make causal claims about intervention effectiveness, but rather explore the consistency with our norms-based framework for understanding stigma. The effect of rape on stigma conditional on humanitarian interventions (H5). Note: Each panel shows the marginal effect of rape on stigma given that a respondent or family member (a) participated in a household intervention (individual and family counseling), (b) participated in a community-level gender norms campaign, (c) participated in an income generation intervention, or (d) has participated in both household and community interventions. The left bar represents the point estimate and 90 percent confidence intervals for rape-affected households which did not and the right bar those that did participate.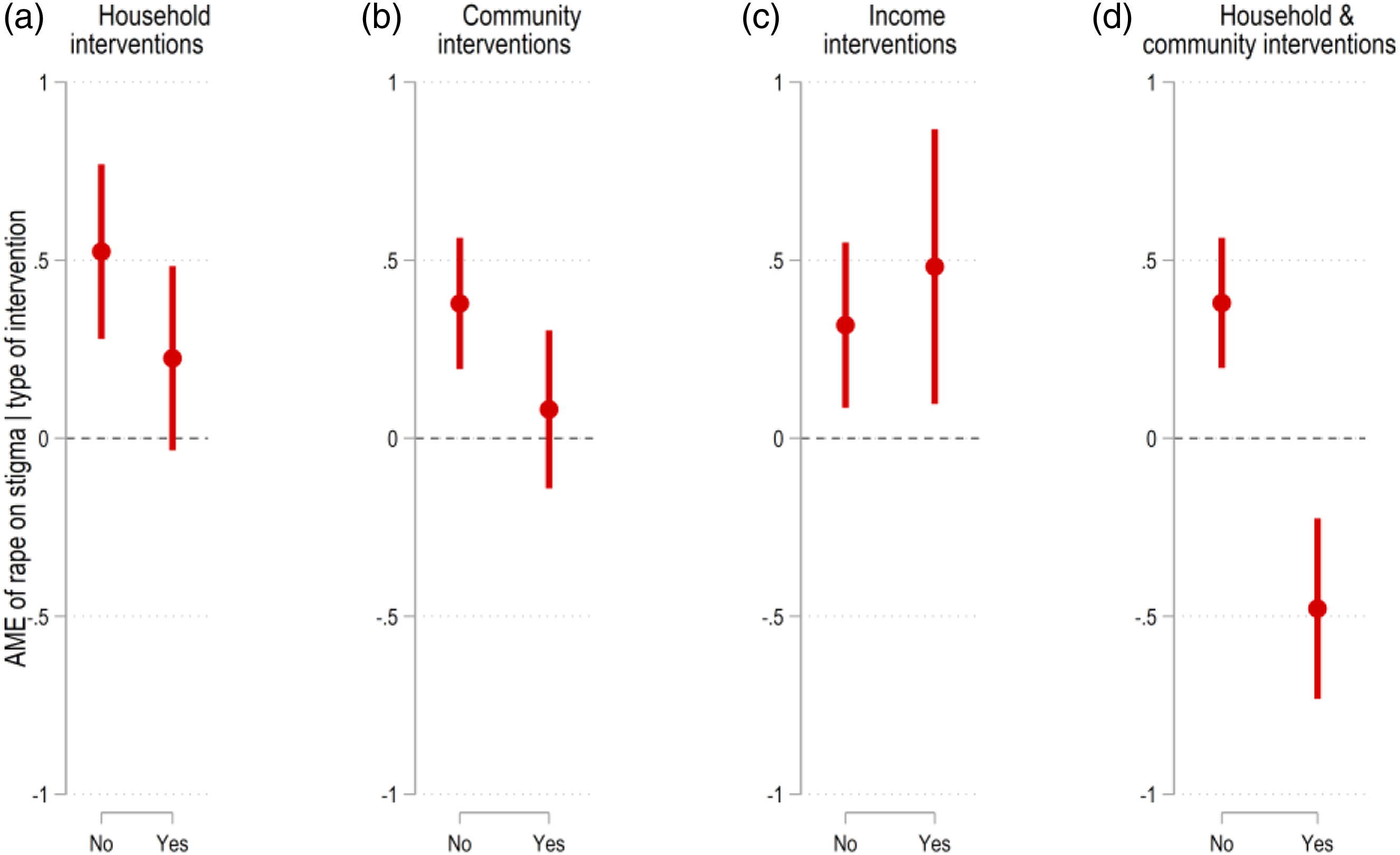
Figure 7 shows that household (panel a) and community-level interventions (panel b) reduce the levels of experienced stigmatization for rape-reporting households, but these differences are not statistically significant. Participating in income generating interventions (panel c) has no effect on reducing stigma. However, households that have participated both in victim-centered household interventions and community norms interventions (d) experience a substantively large and statistically significant decrease in stigma.
In line with H5, community-level interventions are conducive to reducing the adverse effect of rape on stigma, but only when combined with victim-centered household programming. We interpret this contingent effect as support for the social nature of stigma; interventions should aim to address both the behaviors of stigmatizers at the community-level as well as the individually “felt” aspects of stigma primarily addressed in victim-centered household programming.
While this quantitative contribution is unable to capture the nuances, difference of circumstances and meanings associated with rape by armed groups and stigma that has been so strongly emphasized in previous qualitative work—in combination with this literature—our findings significantly expand theory and evidence for wartime sexual violence, experiences of stigma, its social nature and the potential for interventions and community practices to address it.
Conclusion
This study has examined the effects of rape by armed groups on social stigma, a key mechanism by which wartime rape is thought to destroy the social fabric of communities and impede post-conflict development. Using data from an original representative survey and embedded experiment, this article has established the quantitative relationship between rape by armed groups and stigmatization, revealed community-level factors that drive experiences of stigmatization, and shows that interventions designed to support victims and alter social norms can ease at least some harmful effects.
In line with the qualitative literature studying the effects of wartime sexual violence in the eastern DRC (Albutt et al. 2017; Kelly et al. 2011), we find that household exposure to rape by armed groups increases experiences of social stigmatization, an important but understudied dimension in research on the legacy of civil wars. However, our article goes beyond existing research by assessing the social conditions under which stigmatization increases and decreases. We forward a novel argument about the social nature of stigma, describing how community dynamics moderate the effect of rape by armed groups on individual exposure to stigma. We find supportive evidence for the two theorized conditionalities. First, exposure to rape is more strongly associated with stigma when communities blame women for rape victimization. Second, the effect of rape on stigmatization is substantive in villages with low to medium prevalence rates of rape but disappears in high-prevalence villages. Often depicted as homogenous in nature, this finding also introduces previously unexplored variation in attitudes and stigma across villages in eastern DRC.
To further explore the norms mechanism, we use an embedded survey experiment to show that the mechanism linking rape victimization to stigma extends beyond fear of HIV/AIDS victims alone. Respondents choose to ostracize confirmed HIV-negative victims at similar rates to victims whose HIV status is unknown. While fear of HIV does, indeed, have a large effect on stigmatization, fear does not fully account for ostracization associated with rape in DRC. This base level of stigmatizing behavior is plausibly related to compliance with social norms.
Finally, we provide suggestive evidence for the effectiveness of a diverse range of humanitarian aid interventions that seek to improve the lives of rape victims in eastern DRC (Bartels et al. 2010; Albutt et al. 2017; Amisi et al. 2018; Dumke et al. 2021). By drawing on a population-based sample in a survey delinked from a program-specific evaluation, our examination of the effectiveness of humanitarian support interventions presents a difficult test. Yet, we still uncover that a combination of household interventions and community norms programming can significantly reduce stigma associated with rape. The finding further supports our depiction of stigma as a phenomenon that varies with social norms.
This article significantly contributes to the literature on the social effects of armed violence (Bauer et al. 2016; Gilligan et al., 2013; Blattman 2009; Avdeenko and Gilligan 2015; Voors et al. 2012) and underscores the need to disaggregate forms of violence that individuals and communities experience when considering social outcomes (Koos 2018; Gutiérrez-Sanín and Wood 2017).
Taken together, our theory, data and evidence suggest the importance of theorizing, measuring and targeting community-level variation in norms, attitudes and stigma. Yet, there is considerable room to further refine and develop the village-level measures we introduce here. With additional data sources, researchers might account for sampling error associated with estimating village means from a small sample of respondents using small area estimation methods (see, e.g., Jiang and Rao 2020). 28
Overall, our article demonstrates the value of micro-level quantitative approaches to address research questions informed by established qualitative work. To that end, our article joins and strengthens the novel field of research on gender and conflict that employs innovative micro-level data collection and quantitative analyses to investigate complexities within conflict-affected populations (e.g., Koos 2018; Traunmüller et al., 2019; Østby et al., 2019; Lindsey 2021; González and Traunmüller 2020).
Supplemental Material
sj-pdf-1-jcr-10.1177_00220027211064259 – Supplemental Material for Wartime Sexual Violence, Social Stigmatization and Humanitarian Aid: Survey Evidence from eastern Democratic Republic of Congo
Supplemental Material, sj-pdf-1-jcr-10.1177_00220027211064259 for by Carlo Koos and Summer Lindsey in Journal of Journal of Conflict Resolution
Footnotes
Acknowledgments
We are grateful to Research Initiatives for Social Development based in Bukavu, South Kivu, who implemented the survey. In particular, we are indebted to Emmanuel Kandate, Pépin Benedict Mugisho, the late Jean-Paul Zibika, and 20 engaged enumerators for their research contributions. We also thank reviewers and editors of the Journal of Conflict Resolution, Ismene Gizelis, and participants of the annual WomanStats symposium 2020 for generous feedback.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors kindly acknowledge funding by the German Research Foundation (Grant number: KO 5170/1-1).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.