
Abstract
In recent years, India has established itself as the world’s ‘pharmacy hub’, and this claim was proven once again when it delivered COVID-19 vaccines to its citizens, neighbouring nations and across the globe. Following the philosophy of humanitarianism through the principle of ‘Vasudhaiva Kutumbakam’, India has decided to provide the COVID-19 health assistance to its immediate neighbouring countries. India’s immediate neighbourhood refers to the countries that are geographically adjacent to it. In addition, India’s vaccine diplomacy has exposed geopolitical fault lines in South Asia as China’s vaccine diplomacy aims to outpace India in the region. Against this background, the main objective of this paper is to explain and examine India’s vaccine diplomacy as an instrument of its ‘Neighbourhood First’ policy during the COVID-19 pandemic. It argues that India’s health-focused approach has proved effective and aligned with its national interests. This review demonstrates that India’s health diplomacy has had an impact on medical and humanitarian assistance reciprocation at the regional and international levels. As a result of this strategy, during the second wave of the pandemic, India received medical devices and vaccines from other countries in dealing with COVID-19.
Keywords
Introduction
The COVID-19 pandemic had drastic impacts on the regional and global geopolitical architectures, bilateral and international relations and so on. In some cases, it had become one of the rationales for worsening India’s bilateral and multilateral relations. Many countries have been pursuing global health diplomacy to fight the pandemic (Lisk and Šehović, 2020: 46). India, one of them, has become a pioneer in developing the COVID-19 vaccine. India has decided not only to vaccinate its people but also to assist neighbouring countries (Pattanaik, 2021: 97). Although in the recent past it has been observed that India’s relations with the neighbouring countries have been enervated given the internal and external dynamics and milieus, it has remained one of the peace-loving countries. The ‘Vasudhaiva Kutumbakam’ has held a pivotal place in Indian foreign policy (Mahapatra, 2016: 3). India always has prepared to help out the countries in emergencies such as tsunamis, floods, earthquakes, even pandemics/endemics and so on(Pattanaik, 2021: 96). When neighbouring countries faced the daunting task of providing timely treatment, medicines and vaccines, India took a humanitarian view of the global health crisis; and decided to provide vaccines to the neighbouring countries (Pasrich, 2021). Providing vaccines is considered an essential element of India’s Neighbourhood First Policy (Trofimov and Bellman, 2021). India’s Covishield vaccine, manufactured by ‘Serum Institute of India’ (SII), was delivered to all the South Asian Association for Regional Cooperation (SAARC) countries under the ‘Vaccine Maitri’ initiative except Pakistan. In this study, India’s immediate neighbourhood refers to the countries that are geographically adjacent to it. This initiative seems to have taken Beijing by surprise, emphasizing the geopolitical nature of India’s Neighbourhood First vaccine diplomacy. With Chinese Media’s smear campaign vis-à-vis India’s vaccine diplomacy, humanitarian perspective attained the region’s tone and tenor of geopolitical character. This review is aimed to examine India’s vaccine diplomacy (Vaccine Maitri programme) and in doing so, it answers two main issues – (1) How the vaccine diplomacy would affect its enervated relations with the neighbouring countries? and (2) to delve into the geopolitical and humanitarian perspectives of the vaccine supply, in which China has been attempting to outpace India in the region through vaccine diplomacy. It argues that, so far, India’s humanitarian approach has proved effective and aligned with its national interests. The results demonstrate that India’s health diplomacy has impacted medical and humanitarian assistance reciprocation at the regional and international levels. As a result of this approach, India received medical devices and vaccines from other countries dealing with COVID-19 during the second wave.
Method
We have conducted an extensive literature search for this narrative review which looked at the historical perspectives of India’s policies in the current pandemic since the first case of COVID-19 was detected in the country. The articles of potential interest were identified by searching the popular databases such as Scopus, Web of Sciences, PubMed and Google search engine using the following search strategy (‘Vaccine Diplomacy’ OR ‘Neighborhood First Policy’ OR ‘Humanitarian’ OR ‘Geopolitical’ AND ‘India’). The search was then refined by identifying articles discussing Indian policies, various practices, diplomatic relations with neighbouring countries, humanitarian assistance and geopolitical aspects that arose during the COVID-19 crisis. Only articles written in English were considered, and there was no restriction on the year of publication. Emphasis was given to published journal articles although some authentic ministry websites and annual reports were also included. It is also critical to understand India’s vaccine diplomacy from a civilizational standpoint. India’s narrative, particularly since the Bharatiya Janata Party came to power, frequently employs age-old civilizational ideas such as Vasudhaiva Kutumbakam. As part of COVID-19 humanitarian aid, it is fundamental to examine these ideas thoroughly.
Results
The major findings from the review of the included articles are divided into three main subthemes, as discussed subsequently.
India’s Neighbourhood First policy
The political, socio-economic and strategic landscape in India’s neighbourhood has been experiencing a tectonic change considerably in the 21st century. Although India has been trying to create a new international identity per se through its engagements with all the major powers/countries, it could not overcome the harsh realities of its difficult continental geography. India’s diplomacy primarily centred on managing its relations with its South Asian neighbours. This approach can be traced back to Nehru’s Panchsheel doctrine, which gave further impetus to the Gujral Doctrine based on the principle of non-reciprocity (Muni, 2017: 118). However, in the intervening years, a paradigmatic shift was experienced by India’s foreign policy taking volte-face from idealism to realism, particularly during 1962–1971, portrayed as the decade of realism and recovery (Das, 2016: 21). India’s role in Bangladesh and its peacekeeping operation in Sri Lanka had inflicted apprehensions among the neighbouring countries (Dahiya and Behuria, 2012). These countries have developed feelings about India’s use of bilateralism as an instrument of its coercive diplomacy. Consequently, the same has become instrumental in failing and strengthening the South Asian regional cooperation.
The 1990s decade was a watershed moment in South Asian regional cooperation due to the implementation of economic reforms. India had sought to promote regional cooperation through trade and business relations in the changing geopolitical and geo-economic interests and environment (Behuria et al., 2012: 240). On the contrary, the Gujral Doctrine played a key role in India’s ‘neighbourhood policy’, enabling other countries to rise above a complex regional security conundrum. It had provided the neighbouring countries with unilateral concessions without seeking reciprocity. Sikri (2009) argued that the Gujral Doctrine had served as a guideline for subsequent governments such as the National Democratic Alliance (1998–2004) and United Progressive Alliance (2004–2014). Consequently, the economic and security relations with the SAARC countries have seen a dramatic shift.
Even the current government (from 2014 to date) has consistently made efforts to strengthen regional cooperation, as evidenced by invitations to the heads of the SAARC and the Bay of Bengal Initiative for Multi-Sectoral Technical and Economic Cooperation (BIMSTEC) member countries. The incumbent Prime Minister Narendra Modi had expedited the diplomatic manoeuvres to strengthen the ‘Neighbourhood First’ policy further. In his address during the 69th session of the United Nations General Assembly (UNGA), he argued that ‘A nation’s destiny is linked to its neighbourhood. That is why my government has placed the highest priority on advancing friendship and cooperation with her neighbours’. Under the ‘Modi doctrine’, India’s Neighbourhood First policy seeks to strengthen its relations with its neighbours, which serves its socio-economic development and strategic interests in the region to indicate India’s commitment to regional connectivity (Singh, 2016). Some commentators like Mohan (2015) have remarked that the Modi government’s foreign policy was the beginning of an Indian ‘Third Republic’ with a non-ideological worldview, first being the social democracy in the Nehruvian era and second era of ‘economic reforms’ in the 1990s. Kaura and Rani (2020: 11) had pointed out that Modi often projects himself as an innovative and decisive leader who appeared to have been realized during his first regime when he invited South Asian leaders to attend his oath ceremony in 2014. On the contrary, Ganguly (2018) has observed that despite fundamental progress on several fronts, Modi’s diplomatic activism could not have yielded very positive results due to its policy gridlock and China’s outreach in the South Asia region. However, in the post-pandemic era, India has geared its pharmaceutical industry to prepare the vaccine for COVID-19, which has further proved instrumental in resurrecting its relations with neighbouring countries.
COVID-19-outbreak and India’s rise as a global health leader
The COVID-19 pandemic posed a global health crisis with subsequent massive losses in terms of manpower and material (2.42 million deaths; and about 110 million infected people worldwide, respectively) since it was declared a pandemic by the World Health Organization (WHO) on 11 March 2020. Almost every country had implemented various social distancing measures, focusing inward and closing their land borders until the vaccine was developed. Consequently, the concept of Global Health (Vaccine) Diplomacy has emerged as a cornerstone for foreign policies of major countries. The United Nations (UN) had recognized the COVID-19 pandemic as a security threat. The UN Secretary-General Antonio Guterres has warned that it could ‘potentially lead to an increase in social unrest and violence that would greatly undermine our ability to fight the disease’ (ANI, 2020a).
The pandemic has devastated even the richest nations causing huge economic losses and entering a recession. The G7 nations were quick to respond to such global health crises. This group could not do much as anticipated due to the rising burden of cases daily, increased number of deaths and lack of availability of effective vaccines (Nakatani et al., 2020). Until recently, only effective public health regulations such as social distancing, quarantine and isolation have been helping to cope with the pandemic. Such a pandemic scenario needs multi-pronged, multilevel and multilateral interventions and partnerships with a clear focus on keeping aside the political differences among the countries to ensure the basic human rights of health and security.
Foreign policy negotiations between countries with stakes in global health issues benefit greatly from the discipline of ‘Global Health Diplomacy’ (GHD), which aims to better understand the global health crisis (Kickbuscha et al., 2007). Many countries, including Cuba, China, the United States and India, now have a greater opportunity to play a role in global health leadership. Although health diplomacy remained an important part of the major powers or countries’ foreign policies, it has become an important element in a global health crisis. With India as a pharmaceutical hub and ambitions for regional and global leadership, the GHD has emerged as an integral part of Indian foreign policy in general and in the form of the ‘Neighborhood First’ policy in particular. The GHD, as an interdisciplinary concept, links the domains of health and international relations and addresses the needs of global health security through its binding or nonbinding instruments enforced by global governance institutions (Chattu, 2017).
According to WHO, the main goals of health diplomacy are (1) to ensure better health security and population health; (2) to improve relations between states; (3) to commit to improving health through the involvement of a wide range of actors; and (4) to achieve outcomes that support the goals of reducing poverty and increasing equity (WHO, n.d.). Chattu et al. emphasized that GHD holds some promise of enabling ‘policy coherence’ through the determinants of health and human security to ensure that health is seen as a global public good (Chattu et al., 2019). In this context, Tagizhade and colleagues have highlighted that GHD’s crucial role in addressing many of the global challenges (Taghizade et al., 2021), as many scholars have witnessed GHD’s role in the formulation of International Health Regulations (IHRs), 2005, Framework Convention of Tobacco Control, Universal Health Coverage (Sustainable Developmental Goals, UN Climate Change Conference 2019; UN, 2019 and most recently the COVAX Facility in 2020 (Kickbuscha et al., 2007)). Researchers have emphasized the critical role of GHD in promoting peace (Chattu and Knight, 2019), improving health and well-being (Chattu and Chami, 2020), strengthening global leadership and international cooperation (Javed and Chattu, 2020), global coordination (Fazal, 2020), negotiating for TRIPS waiver for COVID-19 vaccines (Chattu et al., 2021), promoting vaccine equity (Singh and Chattu, 2021) and strengthening the bonds between nations (Mol et al., 2021). A recent review by Gupta et al. emphasized the importance of foresight in reviving multilateralism for a more sustainable world through GHD (Gupta et al., 2021).
During the COVID-19 pandemic, India’s appropriate responses and responsible approach had come into more visibility when India had shown its willingness and capacity to deliver global health interventions. It has provided telemedicine services, vaccines, testing kits, personal protection equipment, respirators, extended credit lines, shared pandemic experiences and other services to address the health concerns of not only its neighbouring countries, but also the world at large, through its contributions to development, healthcare and peacebuilding (Sharun and Dhama, 2021: 1). The major development and significant contribution made on the part of India to promote global health security and healthcare in the past few months can be summarized in four broad areas that have gained global attention and appreciation by the world leaders irrespective of their political views.
First, by maintaining its potential as a ‘Pharmacy of the World’ with its proven history of manufacturing and supplying, India has activated its supply lines of generic drugs at very affordable. It is home to half a dozen major vaccine makers for polio, meningitis, pneumonia, rotavirus, BCG, measles, mumps and rubella, among other diseases (Chakraborty and Agoramoorthy, 2020). It has seen a dramatic increase in the production and exports of its pharmaceutical products, as shown in Figure 1. If we discern India’s present value of exports in pharmaceutical products in different regions compared to a decade ago, it concludes that India has witnessed a massive hike. The major four regions, Americas, Asia, Africa and Europe, have been figured significantly in India’s health and medical diplomacy. In the American region, India’s export value has increased from US$2.2 Billion in 2010–2011 to US$7.6 Billion in the financial year of 2019–2020, whereas, in Asia, Europe and Africa region, it witnessed more than 100% rise in India’s export value in pharmaceutical products. It shows India’s potential as the pharmacy of the world.
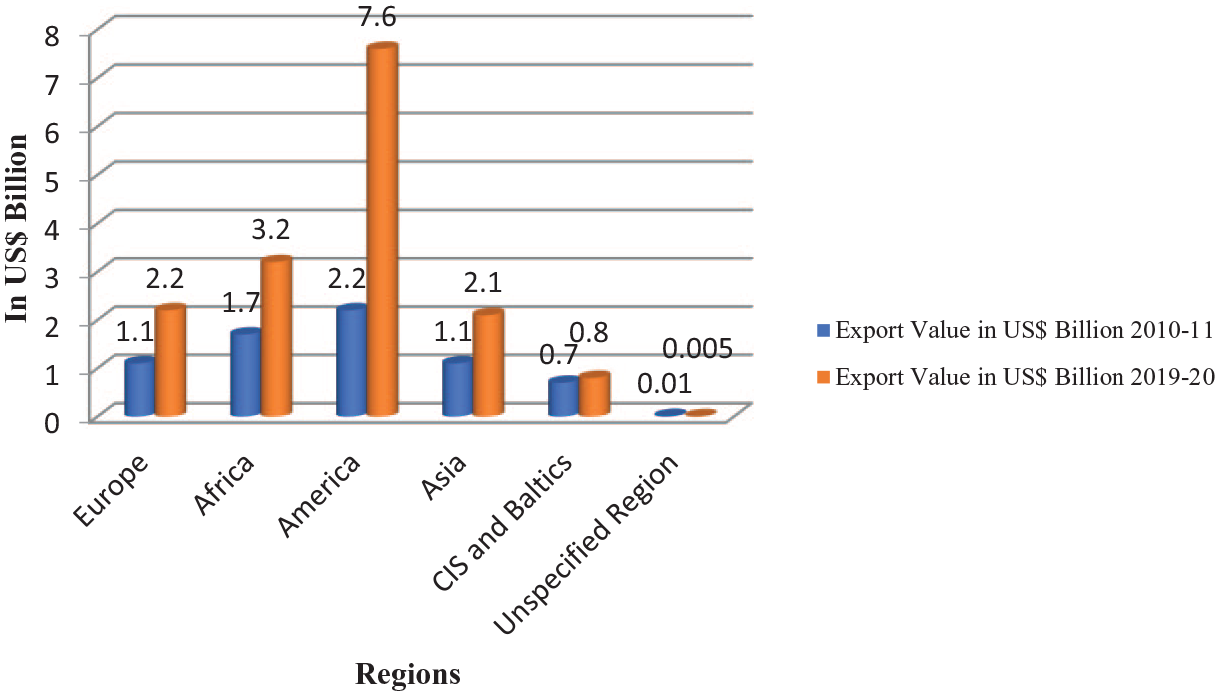
Region-wise distribution of India’s pharmaceutical product exports.
During the COVID-19 pandemic, around half a dozen Indian firms have collaborated with the United States, the United Kingdom and Russian pharmaceutical companies. India has been developing vaccines against the COVID-19, producing 1.5 billion doses per year and supplying around 20 vaccines to 165 countries. It has developed a ‘live-attenuated’ vaccine in collaboration with an American biotech (Raghavan, 2021). India has exported massive consignments of HydroChloroquine (HCQ) and paracetamol tablets to at least 100 countries during this pandemic. India has also delivered HCQ and paracetamol tablets to the Gulf Cooperation Council (GCC) countries (PTI, 2020a).
Second, health and vaccine diplomacy has remained one of the important elements through the multilateral platform engagements such as SAARC and G-20 countries; Quad virtual meeting; contribution in WHO healthcare programmes; the Global Alliance for Vaccines and Immunizations (GAVI); and Pan Africa E-Network. Through the various public awareness campaigns, India has convinced the heads of SAARC and G20 members to share reliable information, best healthcare practices and support each other in combating the ongoing pandemic (Pandey, 2021). At the insistence of India, these diplomatic activities have made spectacular progress. India has taken the leading role through various engagements to support several countries and address the health concerns of its stranded citizens in host countries.
Third, as a reliable global stakeholder, India has shown its outward focus and joined hands for global engagement since the beginning of the COVID-19 pandemic (Madkaikar et al., 2021). Although there were blame games among the major countries regarding the origin, expansion and transmission of the virus (Flinders, 2021), India had remained focused on its healthcare concerns and took appropriate steps in controlling and combatting the pandemic by initiating the lockdown in four phases. This extensive global outreach had departed from the past when India tended to look at itself as a nation with limited ability to shape global outcomes (Singh, 2017: 44). Chaudhury (2020) has argued that this new outward orientation is in tune with India’s larger foreign policy approach to project herself as the ‘Rising Elephant’ as a responsible global partner.
Finally, applying its humanitarian approach and implementing the vaccine diplomacy vis-à-vis COVID-19 pandemic, India had sent the teams of Indian military doctors to the countries like Nepal, the Maldives and Kuwait to help the local administrations draw up plans to combat the spread of the COVID-19 pandemic (ANI, 2020b). Indian medical staff has also been conducting online training for their counterparts from other SAARC countries, thereby helping them build their essential capacity buildings (Babu et al., 2020: 170). The Indian response has been much appreciated globally as is evident from various global leaders’ tweets and messages from the WHO. India’s proactive approach during this crisis, whether in terms of setting the global agenda or engaging in multilateral diplomacy, has highlighted India’s global health diplomacy (by supplying drugs and essential medicines, sending teams of doctors, evacuating people in distress from most infected areas and partnering with countries for vaccine development) for global good. Therefore, these actions will have a long-term impact on how the world views India. Although the Indian response to the pandemic may not have been effective to a certain extent, it demonstrated that India could rise to the challenge of managing global health crises with sincerity and integrity when called upon. Today, the world has been looking towards Indian leadership, particularly in health/vaccine diplomatic engagements. It has been substantiated by India’s outward-looking policy, which has included engagement with the SAARC, GCC, BRICS and G20 countries, among others. It is a crystal-clear indication that India has been emerging as soft power, particularly in health and vaccine diplomatic engagements.
India’s Maitri initiative and vaccine diplomacy: ‘Neighbourhood First’
The COVID-19 pandemic emerged as a global health crisis. As a result, there was an urgent need for the solution to be implemented through the collaborative efforts of regional organizations such as the South Asian Association for Regional Cooperation (SAARC). The first step in this direction was the imposition of lockdown in South Asian countries. India, Pakistan and Bangladesh were those South Asian countries that crossed over China in terms of the reported COVID-19 cases. In the wake of the global health crisis and transcending all differences, Indian Prime Minister Narendra Modi proposed a joint emergency fund based on international and regional health cooperation. India announced an initial contribution of $10 million, and with the pool of contributions made by all seven grief-stricken countries, the same had reached $21 million (Jha and Jha, 2020: 344). Except for Pakistan, all countries pledged to contribute directly to the SAARC COVID-19 Emergency Fund. Pakistan pledged $3 million and said that the fund would be deposited with the SAARC Secretariat to fight COVID-19. This action demonstrated India and Pakistan’s differences of opinion on how the fund should be administered and how regional vaccine diplomacy was shaped by the tenor of bilateral relations (Pattanaik, 2021: 103). Being one of the largest pharmacies in the world, the Indian leadership had realized the need to play a significant role in health cooperation and vaccination.
India is one of the largest manufacturers of pharmaceutical drugs and a home to half a dozen vaccine makers for various diseases like polio, rotavirus, meningitis, measles, pneumonia, tuberculosis, mumps, rubella and so on. These vaccine makers include Serum Institute of India (AstraZeneca), Bharat Biotech (Covaxin), Biological E. Ltd, Cadila Healthcare Ltd (ZyCoV-D), Hetero Biopharma and so on. Several other Indian vaccine manufacturing companies, including Dr Reddy’s Laboratories (Sputnik V), Biological E Limited (Janssen Ad26.COV2.S and Bio E COVID-19), Aurobindo Pharma (UB-612) and Indian Immunologicals (Live attenuated SARS-CoV-2 vaccine developed by Griffith University), have also obtained licences to manufacture vaccine candidates developed in other countries (Sharun and Dhama, 2021). Amid the novel COVID-19 pandemic, the Indian firms, for example, SII, has started developing anti-viral vaccines collaborating with the United Kingdom and the United States. Thus, India has been supplying around 60% of the total global requirement of BCG, DPT and measles vaccines (Priyankaraj, 2020). India’s Vaccine Maitri diplomacy has enhanced its credibility as a leading and reliable vaccine producer in the new world order, where equitable access to vaccines had become a challenge.
In the January 2021 session, the WHO Director-General, Dr Tedros Adhanom, expressed concern over unequal access to COVID-19 vaccines where humankind has been facing ‘catastrophic moral failures’. He added, ‘the developed countries monopolized the Pfizer and Moderna vaccines for their populations’ and failed to ensure access to vaccines in the developing countries (BBC News, 2021). In stark contrast to this statement, India has taken a humanitarian view through its ‘Vaccine Maitri’ initiative. Days after vaccinating some of its population, New Delhi had started delivering millions of doses of its COVID-19 vaccines to the SAARC countries including Myanmar and other parts of the world. As per the ‘Neighbourhood First’ policy, India had tried to translate the same into vaccine first and delivered the first consignment of the Covishield vaccine and Covaxin to its immediate neighbourhood – Afghanistan, Bhutan, Bangladesh, Nepal, Maldives, Sri Lanka and Myanmar (Sibal, 2021). It is worth mentioning that the SII manufactures the Covishield vaccine with the help of AstraZeneca and Oxford University. And Covaxin has also been locally developed and manufactured by Bharat Biotech. Besides this, the SII has also signed a US$150 million contract with Bill and Melinda Gates Foundation (Bery, 2021). As a part of this agreement, India has demonstrated its humanitarian approach by agreeing to provide GAVI and its COVAX facility with 100 million vaccine jabs. Also, India had shown its commitment to helping 95 underdeveloped countries worldwide, focusing on those in its immediate neighbourhood.
On 20 January 2021, Bhutan and the Maldives became the first two countries to receive 150,000 and 100,000 vaccination doses, respectively. The next day, Bangladesh and Nepal were two other SAARC countries that received 2 million and 1 million doses, respectively. In late January, India donated 500,000 doses of the COVID-19 vaccine to Sri Lanka, thereby kicking off the country’s vaccine rollout. In South Asia, China won over Pakistan and Nepal but had to contend with India’s vaccine diplomacy when Sri Lanka and Bangladesh chose Indian vaccines over Chinese vaccines. On 22 January, Myanmar (1.5 million doses) had become the next recipient of the COVID-19 vaccine (Table 1; Lee, 2021). Given their geopolitical importance, as part of India’s vaccine diplomacy, approximately one-fourth of the country’s total COVID-19 vaccine supply has been distributed to countries in South Asian countries. Table 1 demonstrates that India’s geographical neighbours remain the country’s top priority for vaccine supply, accounting for 29.44% of its total COVID-19 vaccine supply throughout the world. On 8 February 2021, India gifted more than half a million COVID-19 vaccine doses to Afghanistan, the war-torn nation. Afghanistan’s government has described India’s vaccine drive as a ‘strong sign of generosity and sincere cooperation’ (Al Jazeera, 2021).
India’s COVID-19 vaccine supplies so far to its geographical neighbours as of May 2021.
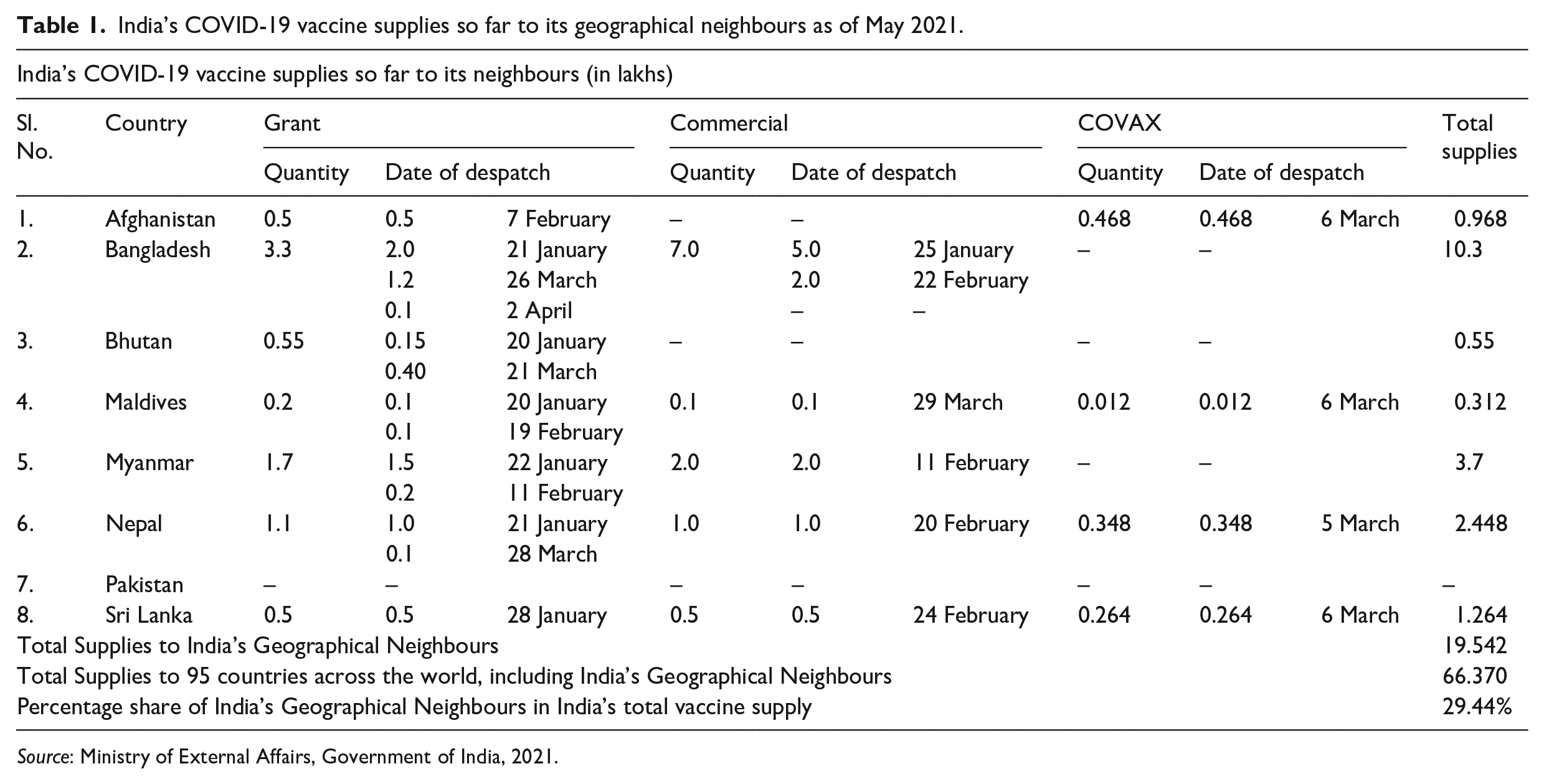
Source: Ministry of External Affairs, Government of India, 2021.
The impacts of India’s Maitri initiative can be observed as Bangladesh Health Minister said that India had played a strategic role during the Bangladesh Liberation War of 1971 and stood by Dhaka even during the current pandemic. Before this, Bangladesh had denied China for sharing vaccine trial costs (Awasthi, 2021). On the Nepal government’s request, India responded positively by delivering vaccines. For India, it is seen as an opportunity to recalibrate its relations with Nepal and other neighbouring countries when China has been expanding its geopolitical and economic influences in the region, and their territorial disputes strained their relations with China. While China was still considering providing the vaccine to Nepal, Sri Lanka, Bangladesh, Myanmar and the Maldives, India had already injected positive momentum into its vaccine diplomacy, which many experts regard as a reflection of some geopolitical elements seeking to outshine China’s power (Giri, 2021). With vaccine diplomacy, India appears to have lessened Chinese clout in the region. As a result, India’s vaccine diplomacy is driven by humanitarian interests and geopolitical considerations, becoming more evident and joining the fray.
Discussion
Contrary to this humanitarian perspective, the supply process for COVID-19 vaccines has been complicated by conspiracy theories, mistrust, vaccination campaigns and geopolitical pressures, all of which have linked this humanitarian perspective with new geopolitical imaginations. The preceding discussion on India’s vaccine diplomacy has reflected its humanitarian view towards the world in general and neighbourhood in particular. At the same time, another aspect of this diplomacy appears to be translated into foreign policy, which tangibly serves its geopolitical interests in the world in general and in its neighbourhood countries in particular. Both India and China have been locked in year-long military standoffs in the Himalayan region, Docklam Standoff, Galwan clash, military intrusion in Arunachal Pradesh and so on. Based on her essential concept of brotherhood, India was committed to pursuing vaccine/health diplomacy during the health crisis by issuing speedy clearances to export the anti-malarial drug HCQ to 55 countries, including her neighbours (Sahay, 2020). India’s decision to allow selective hydroxychloroquine export to coronavirus-affected countries and her geographical neighbours was a positive and humanitarian step (Purushothaman and Moolakkattu, 2021). However, this brotherhood and humanitarian perspective took on a regional and geopolitical tone when China’s disinformation campaign targeted India’s vaccine diplomacy. Thus, in Geopolitical terms, India had a difficult year because of China’s aggressive actions along the Line of Actual Control and the COVID-19 pandemic. They have also been using vaccine diplomacy to raise their profile across South Asia. Chinese’s vaccine diplomacy is more competitive with India than with the West. To be sure, China wants to win over India’s neighbours – Bangladesh, Pakistan, Myanmar, Nepal, Bhutan, Maldives, Sri Lanka and Afghanistan.
In this background, it is essential to understand India’s changing geopolitical perspectives taking China into account in connection with its Neighbourhood First policy. However, India’s policy towards the South Asia region was to keep itself and its neighbours isolated from the outside influence during much of the Cold War period. The last decade has prioritized regional connectivity and Neighbourhood First policy in both the global and the regional contexts. On the occasion of completion of the Modi government’s 100 days, the External Affairs Minister (MEA) S. Jaishankar applauded India’s neighbourhood policy as ‘the first circle of priority’ based on two-pronged schemes – high-level political exchanges and non-reciprocal policy (Yhome, 2019). However, the continuity of these dynamics could not escape the influence of Prime Minister Narendra Modi’s pragmatist approach towards the Indian foreign policy, given his style of rearrangements of India’s neighbourhood geopolitics.
In changing geopolitical matrices, China’s increasing role in the South Asian region has profoundly impacted India’s relations with its neighbours such as Pakistan, Afghanistan, Bangladesh, Sri Lanka, Maldives, Nepal and Myanmar. Using its economic strengths and Belt-Road-Initiative (BRI) projects assistance, China has been significantly successful in achieving its objectives of the Maritime Silk Route. With Pakistan, the China-Pakistan-Economic Corridor connecting Gwadar Port (Balochistan) to China has been considered a significant geopolitical move in the Arabian Sea. Pakistan, backed by China, may push India further out of Afghanistan. As vaccine diplomacy determines the fate of strategic equations in India’s Western neighbourhood, the halting of India’s vaccine outreach and the resulting opportunity for other regional and global powers to intervene could have serious implications for the region.
In Sri Lanka, China’s rapid pace in acquiring strategically located Hambantota port and its geo-economic and cultural diplomacy in Nepal can be seen as Beijing’s geopolitical manoeuvrings to control India’s rise in the region. In recent years, both India and China have been locked in year-long military standoffs in the Himalayan region, be it a Docklam Standoff, Galwan clash or military intrusion in Arunachal Pradesh. (Paul, 2019). In this context, one might argue that India and China have been building military infrastructures in the disputed areas (Gilgit Baltistan, Nimmu-Padam-Darcha highway in Ladakh, Kalapani, etc.) to exert their influence and dominance, which finally ended up annoying each other. This is where their geopolitical tussle enters the pandemic era. China has started adapting BRI to the ‘Health Silk Road’ India has also taken this as a geopolitical opportunity to strengthen its relations with the region. Since India has been striving to counter China’s new Silk Road, this would come as no surprise that New Delhi will make any different view for China’s Health Silk Road.
Mashal and Yee (2021) have argued that India is trying to counter China by using its vaccine diplomacy to expand foreign relations amid the territorial conflict. Despite Nepal’s geostrategic and geopolitical proximity to China, India took advantage of the opportunity to send vaccines to the country. Along with exerting influence over China and the Indian Ocean, India also provides doses of help to Sri Lanka in its diplomatic tug-of-war with Beijing. Kalyanaraman (2021) has also confirmed Chinese penetration in the Himalayan security perimeter by cultivating relations with Nepal and Sri Lanka. These developments have alarmed India about such geopolitical manoeuvrings in its immediate vicinity. Mashal and Yee (2021) suggested that India’s vaccine drive has given a retort to China’s years-long political gains in the neighbourhood countries.
Nepal holds a landlocked and buffered space in the geopolitical landscape of the Himalayan region between India and China. Nepal’s geopolitical and strategic significance has been highlighted by recent attempts by both India and China to use vaccine diplomacy to gain influence in the Himalayan region (Tan, 2021). With three high-level visits to Nepal in 3 months, India’s increased efforts to normalize relations between the two countries were on display. In November 2020, Indian Chief of Army Staff M.M. Naravane visited Nepal with medical equipment for the COVID-19 pandemic as a gift, following a visit by Chief of India’s Research and Analysis Wing (RAW) Samant Goel, who had visited Nepal in October 2020 to discuss the map and the Kalapani-Limpiyadhura-Lipulekh dispute with the Nepali government. In return, the Nepalese Army conferred the ‘Maharathi’ title on him (Nayak, 2020). A few weeks later, Indian Foreign Secretary Harshvardhan Shringla travelled to Nepal with 2000 vials of Remdesivir injections after Chinese Defence Minister Wei Fenghe paid a visit to the country in November. (PTI, 2020b). Thus, the vaccine ‘Covishield’ developed by India was hailed as the ‘Sanjivini Buti’ – the life-saving intervention for Nepal during this difficult time, according to Jha (2021). With its dwindling influence in the region, India’s media reported that China had begun pressuring Nepal to accept China’s vaccine without verifying its efficacy and efficiency. Thus, both nations place a high value on bilateral channels for advancing their vaccine diplomacy.
India’s maritime neighbours Bangladesh, Sri Lanka, Myanmar and the Maldives have held a significant place in India’s geostrategic calculus. During and post-COVID-19 pandemic, India had triggered its Security and Growth for All in the Region (SAGAR) mission under the vaccine maître initiative. India has extended all kinds of help to its maritime neighbours and supported the efforts of the governments of Bangladesh, Sri Lanka, Maldives and Myanmar by providing them with health-related consignments in the COVID-19 period (Sharma, 2020). Out of all the geographical neighbours, these four maritime countries have received approximately 80% (15.6 million doses of vaccines) of the total COVID-19 vaccine supply. In support of this mission, India had sent 7 million doses of COVID-19 to Bangladesh. Minister Zahid Maleque of Bangladesh’s health department has stated that his country can expect to receive up to 50 lakh vaccines per month from India. By April 2021, it had received 10.3 million doses of vaccines. These developments enraged China, especially when Bangladesh refused to use Chinese vaccines produced by Beijing’s Sinovac for clinical trials (Sharma, 2021).
On the contrary, Sri Lanka owed China $4.8 billion in loans under former President Mahinda Rajapaksa and increased its debt by $1 billion during the pandemic under his newly elected younger brother Gotabaya Rajapaksa (Mushtaq, 2020). Since India stopped exporting vaccines after the second COVID-19 wave, countries like Bangladesh and Sri Lanka have become more reliant on China for COVID-19 vaccines. China reportedly gave Sri Lanka 1.1 million doses of the COVID-19 vaccine. Bangladesh received 500,000 vaccines from China in May 2021, and Nepal has been promised another million. According to analysts, China is using vaccine diplomacy to regain influence in the strategic Indian Ocean (Bimal, 2021). With the COVID-19 crisis providing a much-needed platform for regional cooperation, India had serious political and strategic implications. To protect its own citizens, India should increase its vaccine production capacity and potentially resume vaccine deliveries to nearby countries.
China’s presence in the Bay of Bengal can be justified by its presence in Myanmar. It is vital to the Chinese Indian Ocean Strategy to cultivate Myanmar as a strategic partner (Awasthi, 2021). For India, it has become a source of great concern that China is being so aggressive in implementing its flagship ‘BRI’, including India’s maritime neighbours. Many experts believe that China is carrying out its encirclement strategy by using the ‘debt-trap’ diplomacy. As a regional leader, China’s growing influence has prompted India to seek closer ties with Myanmar. Chinese involvement in naval and intelligence facilities and industries and developing ports has increased concerns and tensions in India (Brewster, 2010). As a result, increasing Indian involvement in the Burmese military junta has assisted Myanmar in reducing the regime’s international isolation and decreasing its reliance on China. A refurbished and modernized kilo class (INS Sindhuvir) attack submarine was donated to the Myanmar navy by India during the COVID-19 pandemic in 2020 (Bhattacherjee, 2020). Hindustan Shipyard Limited did the refurbishing and modernization. Also, 3.7 million vaccine doses had been sent to Myanmar by India in the form of a grant and a commercial basis as a part of its vaccine diplomacy (Worldometers, 2021). However, Myanmar’s military coup had gone unnoticed by both China and India, which was very strange. To keep their geopolitical tussle over the Indian Ocean alive, both countries have continued to assist Myanmar through their vaccine diplomacy.
India is still dealing with the effects of a devastating second wave surge in May–June 2021, which saw complications related to treatment and limited health services, as well as an increase in infections and deaths (Asrani et al., 2021a, 2021b). As of 2 January 2022, India had 34,889,132 coronavirus cases, with 481,770 deaths (Worldometers, 2021). A shortage of vaccines and other medical equipment for domestic use also hampered its supply. For a long time, India, as the region’s ‘net security provider’, sought to maintain regional stability by providing humanitarian aid and disaster relief. After the first pandemic wave in early 2021, India provided substantial assistance to the affected region. After 17 years, the country received immediate assistance from its neighbours, enabling it to meet the rising demand for supplies such as cryogenic oxygen tankers and critical drugs (Ministry of External Affairs, 2021). As can be seen, only two countries (Bangladesh and Bhutan) in India’s immediate neighbourhood have responded with aid; neither the SAARC nor the BIMSTEC has responded (Ranjana, 2021). The pandemic has prompted Prime Minister Imran Khan to express Pakistan’s solidarity with India. However, he has also called on India to free imprisoned Kashmiri leaders. It was not surprising that Pakistan would take advantage; India is unlikely to accept Pakistan’s offer (PTI, 2021).
Bangladesh stands out as one of India’s most important allies. Bangladesh expressed its solidarity with India in May. On special instructions from Prime Minister Sheik Hasina, Bangladesh delivered over 10,000 Remdesivir vials and 30,000 personal protective equipment kits and tens of thousands of zinc, calcium, vitamin C and other supplements to the Indian border port of Petrapole. Bangladesh was among the first countries to receive vaccines from India’s Vaccine Maitri mission (Strategic Investment Research Unit, 2021). Bhutan has committed to supplying Assam with 40 metric tonnes of liquid oxygen per day from a new plant in Samdrup Jongkhar district (Scroll Staff, 2021). Bhutan was one of the first countries to receive medical supplies from India in 2020 as part of the COVID-19 Emergency Fund. When confronted with mounting domestic criticism over the early export of COVID-19 vaccines, which resulted in shortages, the government resorted to a narrative of goodwill, claiming that the foreign aid received is not the result of an international appeal but rather a form of humanitarian approach and a reciprocal response to India’s altruism (Bhattacharjee and Peri, 2021).
Beijing and New Delhi collaborate globally to fight the outbreak but compete regionally. As India’s capacity dwindled, China quickly stepped in to fill the void, offering vaccines to Nepal, Sri Lanka and Bangladesh. According to many experts, Beijing’s humanitarian response to the COVID-19 pandemic has given it a geopolitical advantage, allowing it to assert its leadership role and expand its geopolitical influence (Ziaul and Shuwei, 2021). China and India’s ambition, strategy and approaches to vaccine diplomacy differ significantly, and analysis shows that neither is engaged in pure altruism given their geopolitical interests. However, from the perspective of global health diplomacy, it is unrealistic to criticize India for taking advantage of its resources and expanding its geopolitical diplomacy, even at a time when the world is experiencing a global health crisis. No one can deny that India’s vaccine gifts will help to improve the country’s global image and increase public trust in the country, particularly in South Asia, where the country is frequently criticized for acting as a ‘big brother’. While the pandemic continues, vaccine diplomacy has become a new tool for international outreach and growing influence.
Conclusion
From the above arguments, it can be claimed that India’s vaccine/health diplomacy in giving humanitarian and economic aid has drawn the world’s attention and neighbouring countries close to New Delhi. It has given a new impetus to its geopolitical position in the region. Through ‘Vande Bharat’ mission, India has endeavoured to develop a model of regional partnerships and proved itself as the first responder to the natural calamities and current health crisis in its neighbourhood during the first wave of COVID-19. Although many immediate neighbourhood countries have become the COVID-19 vaccine recipients, it is difficult to conclude whether India’s health-related initiative in its neighbourhood would have a lasting impact on its regional connectivity pursuits under the Vaccine Maitri programme? However, it has been observed that India’s extension of cooperation in its neighbourhood in the health sector, particularly during the COVID-19 pandemic, has become an important landmark in its geopolitical manoeuvrings in the region.
The regional geopolitical order has been reshaped suddenly in the geopolitical, economic domains. India has always faced geopolitical challenges from China in its Neighbourhood First policy. It was also seen in their vaccine diplomacy when they entered into a competition to provide vaccines for geopolitical reasons. China’s trends in overtaking India in the South Asia region may see some slowdown in the near future, as neighbouring countries are likely to change their priorities in terms of health as a new challenge. The initiatives under India’s vaccine diplomacy have shown to offer value to the country’s health diplomacy and created a space in people’s hearts in the South Asian region. India’s ‘Vasudhaiva Kutumbakam’ and its humanitarian approach towards its immediate neighbourhood can inspire to reinvigorate vaccine diplomacy, which should go beyond geopolitics to serve humanity, considering the production capacity and health infrastructure.
Footnotes
Author Contributions
Conceptualization, Bawa S., and V.K.C.; methodology, Bawa S., and V.K.C.; investigation, S.S. and Balinder S.; resources, Bawa S.; data curation, Bawa S., S.S. and Balinder S.; writing – original draft preparation, Bawa S., S.S., Balinder S. and V.K.C.; writing – review and editing, V.K.C.; supervision, Bawa S. and V.K.C.; project administration, Bawa S. and V.K.C. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.