
Abstract
The aim of this study is to describe the context, resources and procedures for planning/implementing health promotion initiatives targeting the children and youth population in African Francophone countries. The method of work used multiple case studies with an online survey (n = 11) and individual interviews (n = 6) (2017–2018). Strategies to mobilize/use community’s available resources and assets were influenced by gender and professional status, as well as the stakeholder’s valorization and degree of community interest and engagement in the proposed health promotion initiatives. Major social impacts relate to the support provided by the community stakeholders with individual and collective assets. Evidence uncovered professional networking, collaboration and exchange that could help regional health promoters.
Keywords
Background
The World Health Organization (WHO) health promotion (HP) strategy for the African region outlines several objectives and priority interventions to develop and support HP in Africa (WHO, 2013). It also outlines a set of target actions to be met by 2018, one of which aims to establish a national network of HP practitioners in at least 15 additional African countries. In 2015, responding to this strategy, a consortium of eight international partners – Alliance des Ligues Francophones Africaines et Méditerranéennes contre le cancer (ALIAM), Ligue tunisienne de lutte contre le cancer (LTLC, Tunis), Ligue nationale contre le cancer (LNCC, France), Université Senghor (Egypt), Faculté de Médicine de Sousse (Tunis), Université Numérique Francophone Mondiale (UNFM; France), Université Saint Christopher (Liban) and Union International for Cancer Control (UICC) – launched an HP initiative in Africa with the financial support of the UICC. This HP initiative consisted of the creation of a training programme for social services and health professionals to educate them to be responsible for HP in school settings. The programme introduced the philosophy of HP and the concepts of social determinants of health (SDH), pedagogical methods and strategies within a participatory learning approach. The Ryerson University’s (RU) team joined the partners to perform a remote impact evaluation research with trainees in their home countries.
HP was targeted in this training programme because it has been recognized as a socially justifiable strategy to combat the increasing prevalence of non-communicable diseases (NCDs) in African countries, as well as in school settings (WHO and UNESCO, 2018). If implemented appropriately, these initiatives have the potential to produce effective results, allowing individuals to have more control over their health, and to improve it.
The ever-increasing burden of NCDs on low- to middle-income countries causes a disproportionate number of global NCD deaths (more than 75%), thus worsening poverty (Witter et al., 2020). This constant strain on governments and health care systems calls into question the effectiveness and appropriateness of the current HP strategies for the targeted populations. The state-of-the-art evidence on health system challenges for NCD prevention and control in low- to middle-income countries is limited, particularly in those of sub-Saharan Africa and post-conflict settings. Evidence is scarce and limited to the prevalence of NCDs (Witter et al., 2020).
For the purpose of this paper, one key target outlined by the WHO and UNESCO (2018) was considered: the development of HP education in academic systems. Schools are strategic platforms for delivering upstream primary health care (PHC) services, thus impacting a significant portion of the community. The WHO (2020) offers a warning about the overall relevance of youth health in low- and middle-income countries. They state that school health programmes have been shown to be a cost-effective approach to influencing healthy behaviours in youth of low- and middle-income countries. As it currently stands, 80% of youth lack adequate levels of physical activity, and obesity rates have increased 10-fold in the past four decades responding for high mortality for youth. The alarmingly high rates of poor youth health validate an urgent call to increase and improve HP through all school and community settings. Investments in youth health can have positive economic and social benefits, particularly in the aforementioned countries.
Research questions
RQ1. How did the process of identification, mobilization and use of the community forms of capital unfold in its interaction between the professionals and the health and education decision-makers, as well as other community stakeholders, to implement their new role and work for HP in the local schools?
RQ2. To what extent did professionals’ reflections on their skills, achievements and current practice uncover the effectiveness of their work with local decision-makers and stakeholders?
RQ3. What are the professionals’ views about their accomplishments and plans for HP having children/youth as social agents of change?
Research objective
The objective of this study is to describe the context, used resources and the procedures for planning and implementing HP initiatives targeting the children and youth population in schools located in African Francophone countries.
Conceptual framework
This study was framed by an original conceptual framework, comprising three major components: the context, the action and the features of community forms of capital used in the impact evaluation (see Figure 1). The inspirational contextual factors for the conception and deliverance of the HP training programme responded to the growing burden of NCDs and related HP needs (WHO, 2013). The training meant an action at the community level aiming to encourage further HP action at a governmental level. The evaluation considered trainees’ HP actions (planned, implemented and intended) in a collaborative participatory approach altogether to mobilize their community forms of capital.
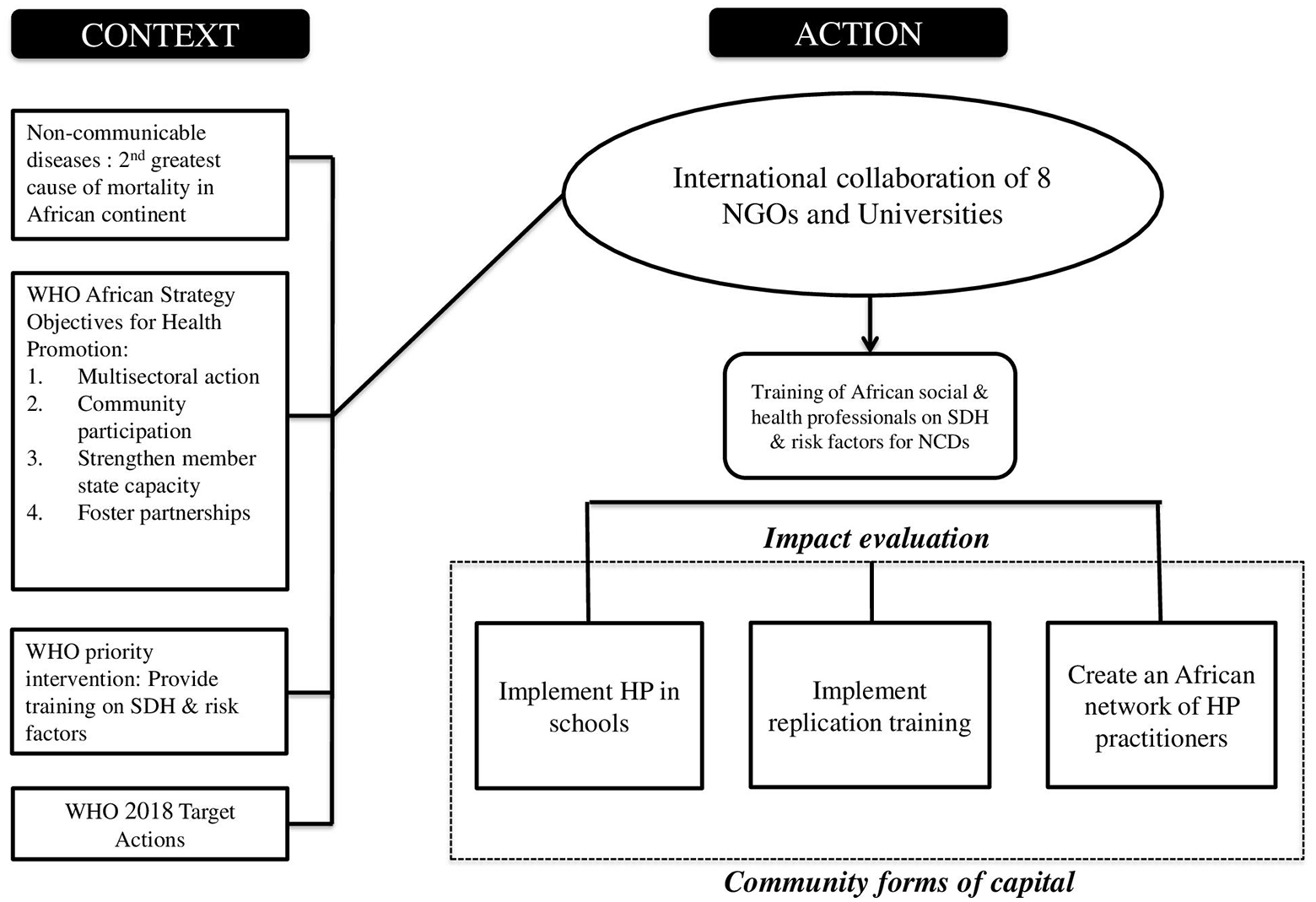
Conceptual framework.
Methods
This study used a multiple, temporal case study design (Yin, 2009), as it helps when researchers use a survey asking several questions simultaneously, such as who, what, where, how, how many and how much, and when researchers focus on contemporary social phenomena. The design was used to explore the scope of experiences, reflections and actions of the trainees in their attempts to implement the training programme in a variety of municipal schools in the region. Case study was the appropriate research design to study the aforementioned emerging new HP role in the region, because it contributes to the researchers’ understanding of individual, organizational, social and political phenomena. Having the features for planning and implementation as major variables, we used a simple time-series method, combining quantitative data and qualitative findings to get an insightful analytical perspective.
Population
The target population of 75 trainees originated from 14 out of 27 countries members of the ALIAM. A long (2 weeks) and a short (5 days) programme modalities had been implemented in Tunis (long: May 2015), Chad (short: October 2015) and Algeria (short: March 2016).
Sampling and recruitment
All trainees were informed that there would be a follow-up evaluation study by the RU researchers. Further contact would be made by email and postings in the alumnae community Facebook page. Trainees were informed that the Programme Coordination would support the research team in their attempts to reach prospective participants who may not have Internet access. In that case, participants knew that those trainees would be invited to go to the local health authority office to use their computer in order to participate in the evaluation study. Therefore, all trainees acknowledged their commitment to ensure the success of the study. Moreover, in order to avoid any direct influence of the social leadership and respect held by ALIAM and UNFM, the principal investigator used measures to prevent any issue of social desirability by being the only contact person. In order to ensure free participation, the recruitment used two strategies: (1) she sent out an invitation email and (2) she posted an invitation to the study on a Facebook page.
Criteria of inclusion
The inclusion criteria are as follows: (1) have attended professional training in becoming responsible for HP in a school setting; (2) have at least 2 months of field experience related to planning for the implementation of the programme in the municipalities’ schools, or have at least 2 months of field experience of an effective implementation of the programme in the municipalities’ schools; and (3) have voluntarily decided to participate in the study by responding to an online questionnaire.
Criteria of exclusion
The exclusion criteria are as follows: (1) had not attended the training, (2) did not have the minimum required 2 months of experience in planning of the school programme, (3) did not have the minimum required time of 3 months of experience in the implementation of the school programme and (4) intended to participate in this study in a non-voluntary manner.
Data collection
Data collection started in 2017 after the short- and long-programme delivery, which required 6 and 12 months of training completion, respectively. Each set of online questionnaires relating to a specific country constituted an individual case to be added to the sample of studied cases. Of interest was the emerging patterns of systemic barriers and limitations as related to the planning phase and the possible, major, underpinning political and financial issues (e.g. governance, social commitment, government priorities). The choice for the online survey responded to the particularities of Internet access across the African continent, which mainly consists of a cell phone, rather than a desktop or laptop computer. By doing so, all prospective participants were reached in their actual locations, including distant and rural areas. The online survey questionnaire operated through RU’s Opinio Survey was the main method of data collection. Online questionnaires have advantages when compared to postal questionnaires, and have been shown to have a lower participant non-response rate in comparison to postal questionnaires, reducing the non-response bias (Smith et al., 2013).
To expand data collection, an invitation for an individual interview was sent out. During the interviews, technical barriers to accessing social media platforms, and difficulties in typing long text using participants’ cell phones, since laptops and desktops were not available to them, were discovered, which could explain the lower rate of participation in the narrative responses.
Instrumentation
Data collection was done through an online survey comprising 30 questions, including 23 closed-ended questions and 7 open-ended questions, divided into four sections: sociodemographic identification, review of current practice, reflection of skills and practice, and prospective actions as well as testimonial. The questionnaire originally in English was translated and validated in its cultural perspective by three bilingual (French–English), Francophone African Master in International Health students at the University of Senghor. These students verified the words’ clarity and appropriateness to the prospective Francophone respondents. They then reviewed the French version and discussed the grammatical review of the survey. Questions in French language were pilot tested. The data collected from the online questionnaires were compiled as descriptive statistics (Grove et al., 2013). It is noteworthy to say that the questionnaire had five questions about testimonies and reflections about participants’ practice; none of them were answered. These questions were explored in individual interviews in French language by telephone.
Thematic analysis was used to analyse the open-ended question responses obtained from telephone individual interviews. Thematic analysis (Paillé and Mucchielli, 2016) guided the core idea explored in each of these questions. The analysis explored groups of descriptive ideas, classified them according to clusters of meaning aiming to create new conceptualizations and refined themes to respond to the research questions. Five predefined themes guided the analysis: (1) targeting HP actions with children and youth in schools as future health literate and health knowledge disseminating individuals; (2) learning due to unexpected results and achievements; (3) ideas for future evaluation of HP programmes; (4) bases for a regional, national and inter-African network for HP; and (5) 5 years’ career plan progression as a professional and advocate for social rights for HP in schools.
The results presented in the next section display the integration of evidence gathered from the responses to the online questionnaire and individual interviews.
Results
Out of 75 individuals who completed the training, we were able to contact 35. The survey was sent to all attendees, but only those who attended the 2015 training in Tunisia responded; 27 participants provided consent to complete the online survey, and only 11 participants actually provided responses to all the survey’s questions. In total, 26 out of the 36 questions were completed. All 26 questions were completed by 8 participants, while 17 of the 26 questions were answered by a mode of 11 participants, as it was not compulsory to answer all questions (see Table 1).
Sociodemographic profile of participants.
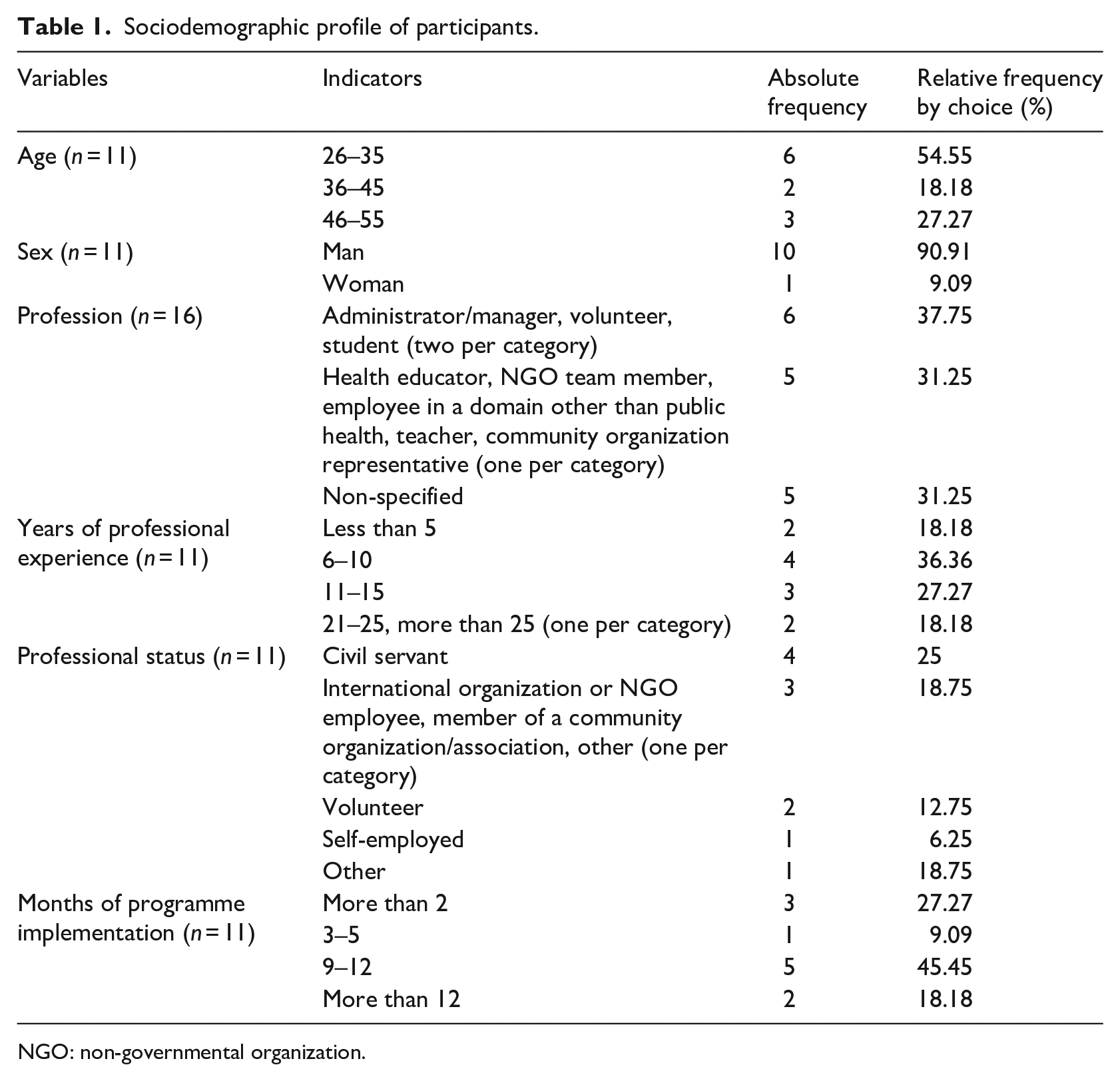
NGO: non-governmental organization.
For the online survey, the participation consisted of three participants working in the République Démocratique du Congo (RDC) and eight participants working in the following countries (one in each): Republic of the Congo, Bénin, Ivory Coast, Mali, Niger, Algeria, Mauritania and Morocco. All participants stated their thoughts about the influence of their masculine identity in their HP programme planning and implementation. It is noteworthy to say that 10 of them were men. Similar thoughts were shared about the influence of their professional title and status in such activities, with 81.8% affirming as much. For the participants, the access to stakeholders and the acceptance of their work by the community, decision-makers and the target population were at stake.
Interactions with community stakeholders and decision-makers during identification and implementation of forms of capital
All participants reported the following as major competencies for the work with stakeholders and decision-makers: (1) competencies to reinforce collaboration with health and education professionals (100%), (2) competencies for community education to enhance decision-makers’ knowledge about the HP pertinence (100%) and (3) competence to reinforce collaboration with parents and tutors (90%). The implementation of HP programmes required the mobilization and use of community forms of capital (see Table 2), as the types of interactions with stakeholders and decision-makers can allow an understanding of the effectiveness and efficiency of each form of community capital.
Mobilized community capital to develop HP projects.
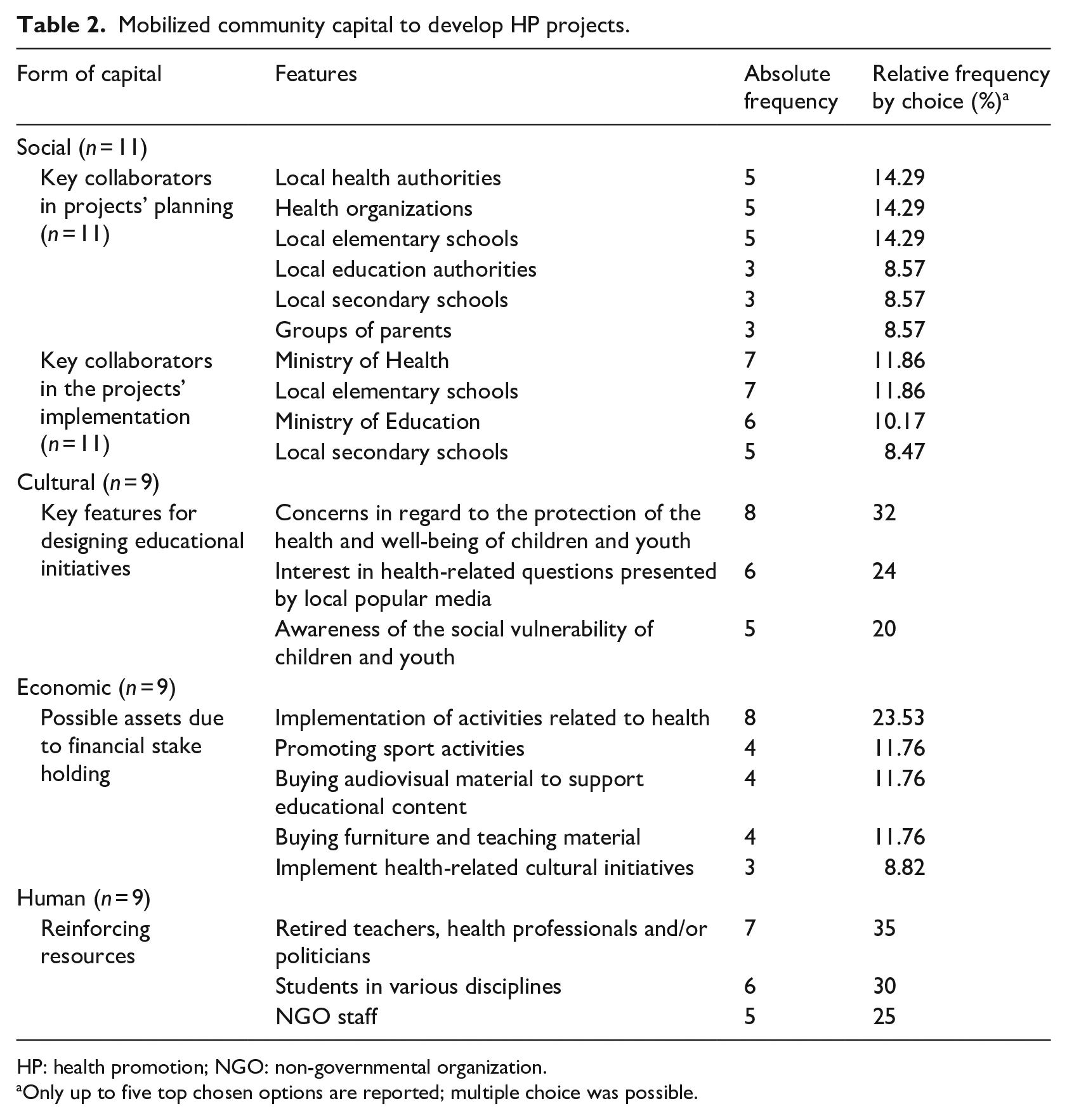
HP: health promotion; NGO: non-governmental organization.
Only up to five top chosen options are reported; multiple choice was possible.
The planning of HP projects involved actions with medical and health associations, local offices of non-governmental organizations (NGOs), volunteer groups and local media (5.7% each), and less collaboration with youth groups and universities (2.9% each). Two other clusters of collaborators for the implementation were medical and health associations (6.8%), as well as with less frequency (5.1%), the community associations, students’ associations, volunteer groups, parents’ groups and NGOs added to agencies of social development, local enterprises, local media, international organizations and advocacy groups (all 3.4% each). Interestingly, participants barely set up collaborations with youth groups, research groups, financial organizations, health organizations and universities (1.7% each).
To develop teaching strategies for children and youth, participants mobilized the communities’ cultural capital (see Table 3). Disclosures also included less interest in building local autonomy (12%), and strengthening personal capacity through political awareness to (8%) and initiating participatory learning about major health matters – tuberculosis, sexually transmitted diseases and so on (4%). Financial stakeholders also supported the acquisition of informatics supplies, development of new educational resources, maintenance and Internet fees, and actions against food insecurity (5.9% each). Religious groups had less participation in the aforementioned projects (10%).
Actual and potential communities’ social resources used for the development educational strategies.
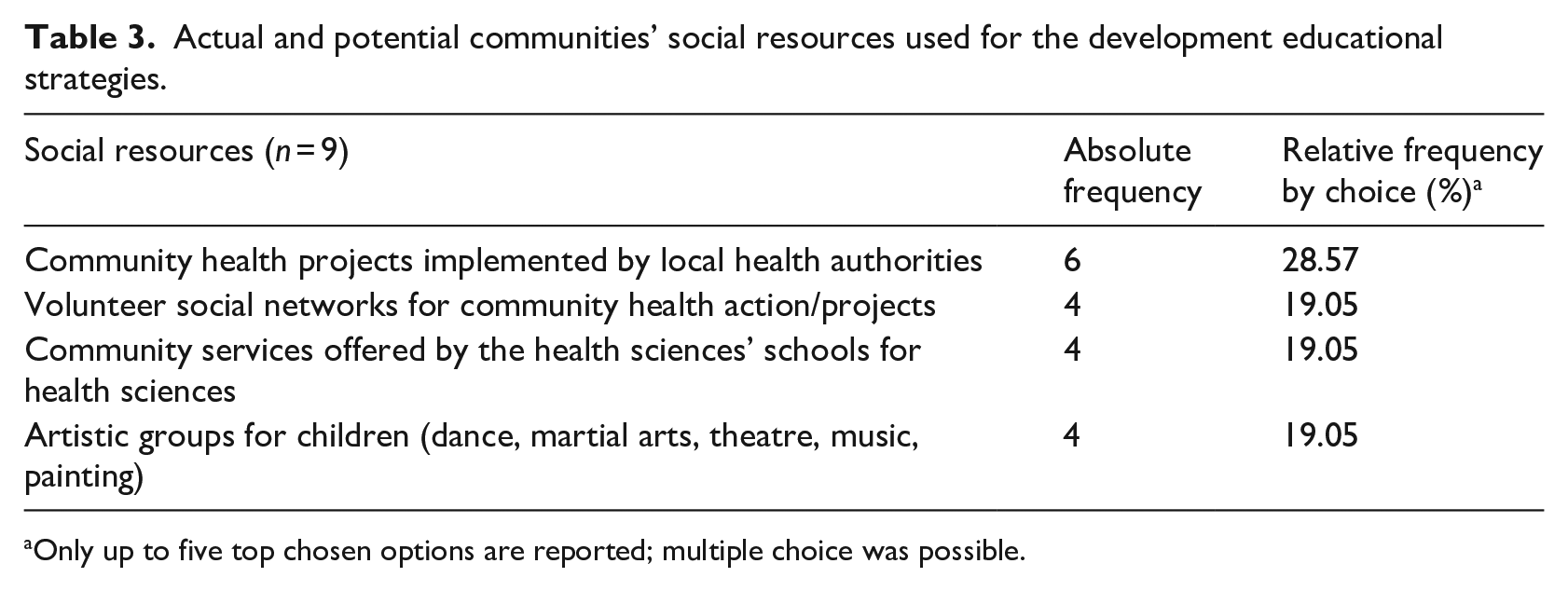
Only up to five top chosen options are reported; multiple choice was possible.
There was less use of arts youth groups, religious groups for children and youth, and social media influencers (4.8% each); however, among the non-durable actions, the NGOs’ work (77.78%) was listed at the top, followed by less consideration for the health and social development research projects implemented by foreign universities (11.11% each). Implementation actions unfolded in six major phases, addressing 31 multidimensional features (see Table 4) that characterized the complexity of HP work in African Francophone sociocultural settings.
The phases and features of the HP projects cited by participants.
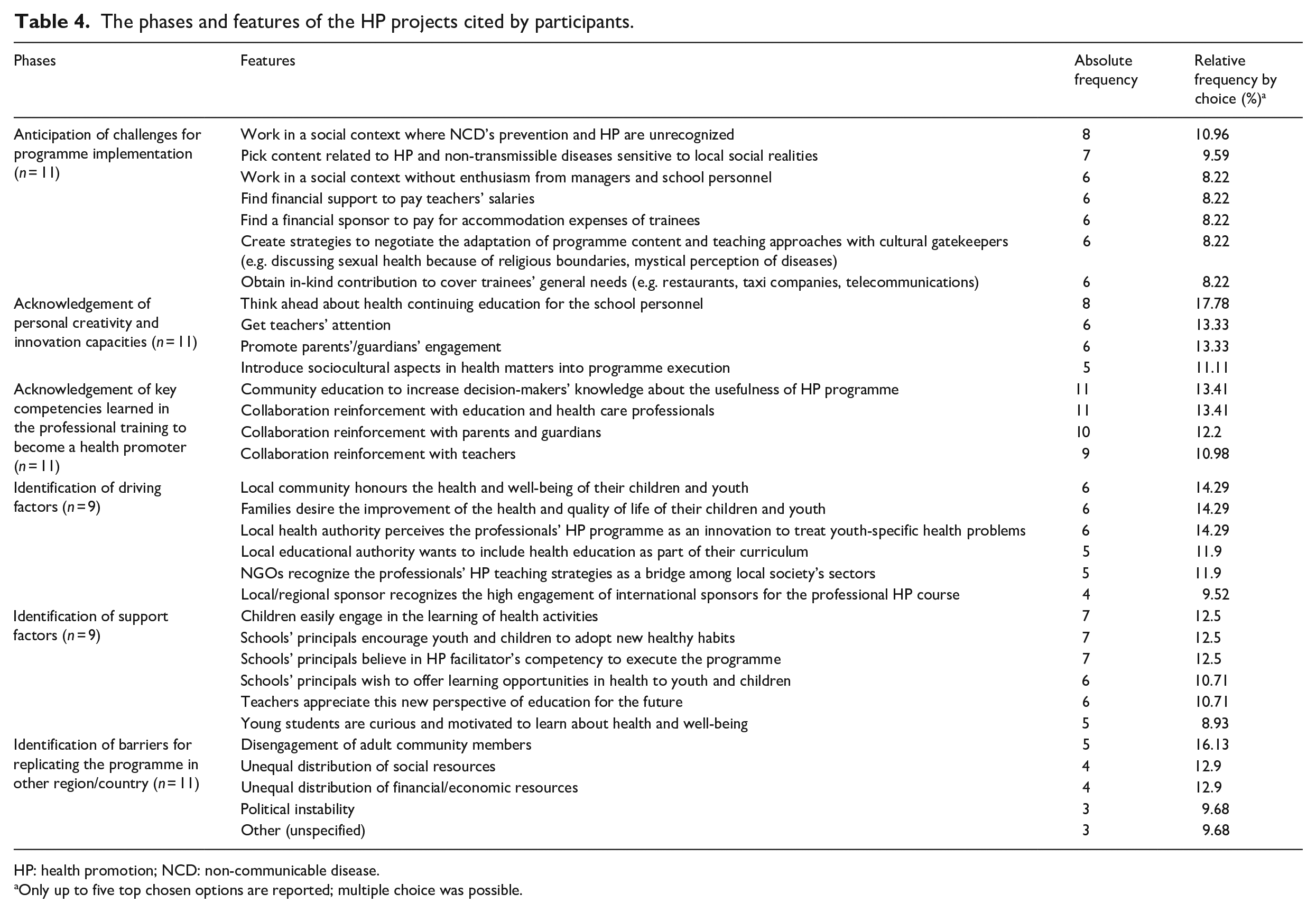
HP: health promotion; NCD: non-communicable disease.
Only up to five top chosen options are reported; multiple choice was possible.
Professionals’ satisfaction and self-reflection and how they are shaped by issues related to successful/unsuccessful approach in their work with decision-makers/stakeholders
Participants justified related satisfaction with facts regarding the school context, such as (1) be accepted by school personnel (12.28%), by youth (12.28%) and work with educational authorities (12.28%), and (2) have work accepted (10.53%) and (3) work with health authorities (10.53%), as well as with the community representatives (8.77%). Participants self-evaluated their work as health promoters (see Table 5), revealing that their knowledge was expanded and reinforced with easiness in concept application, increased critical thinking, as well as the mastering, applying and transferring of knowledge. See Table 5 for specific statements of self-evaluation.
Self-assessment as a health promoter.
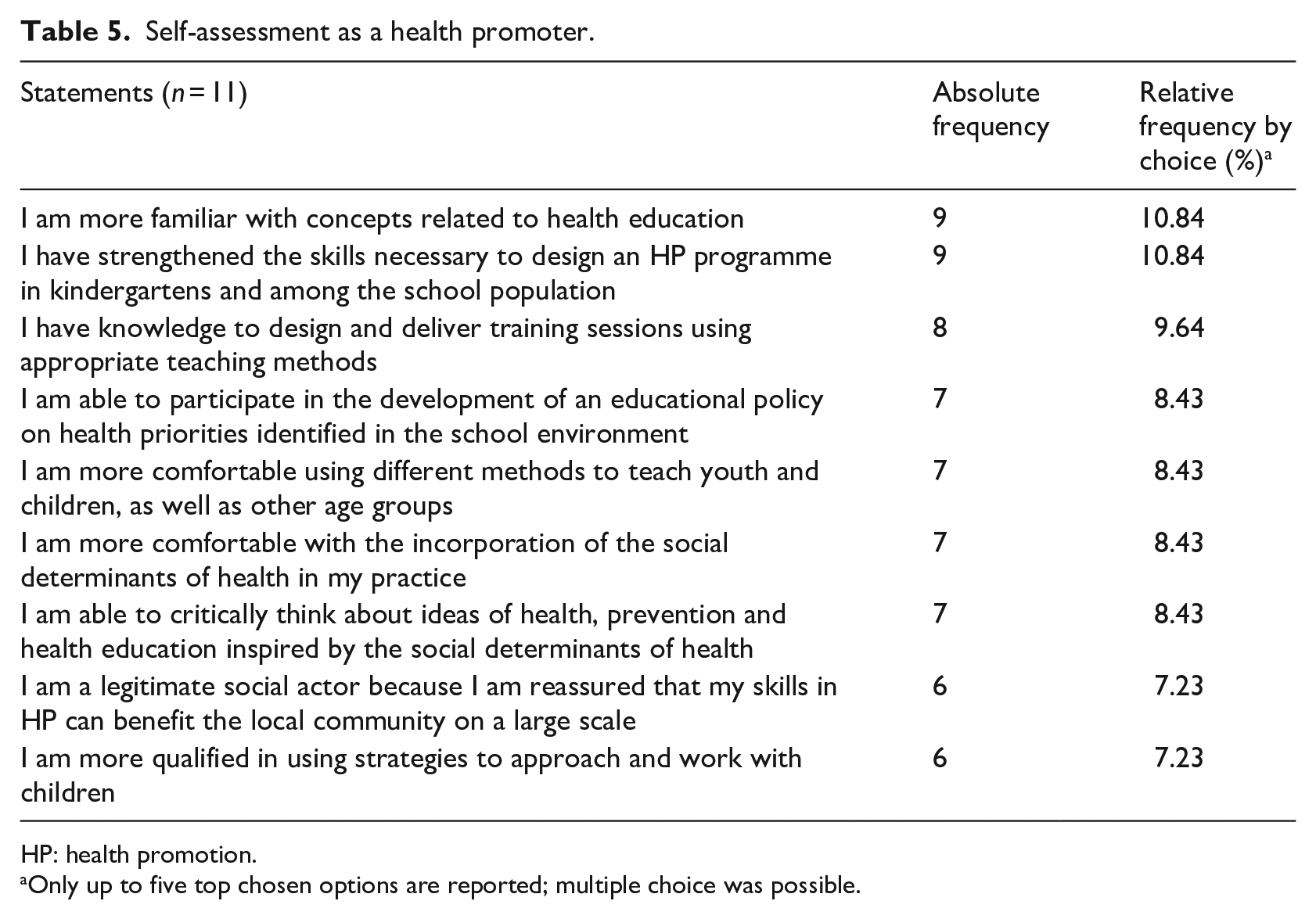
HP: health promotion.
Only up to five top chosen options are reported; multiple choice was possible.
Self-evaluations at several phases of the HP projects were helpful in determining the specific changes needed to ensure success in future endeavours. Using the professionals’ strengths and unique abilities, as well as addressing their weaknesses, helped improve their plans and lead to the creation of a successful inter-African HP network.
Professionals’ view about the future of the programme to tackle NCDs, using youth as the main social agent of change for HP
After the implementation of an HP programme, it was important to consider its sustainability. In doing so, its effects would be more prevalent within the given communities, encouraging further collective, social changes for the health of current and future generations. Table 6 details the different features of the HP programmes’ sustainability.
Future of the HP programme.

HP: health promotion; NGOs: non-governmental organizations.
Only up to five top chosen options are reported; multiple choice was possible.
Six male participants volunteered for the individual telephone interview (see Table 7 for participants’ identification). The interviews lasted an average of 50 minutes.
Interviewees’ sociodemographic characteristics.
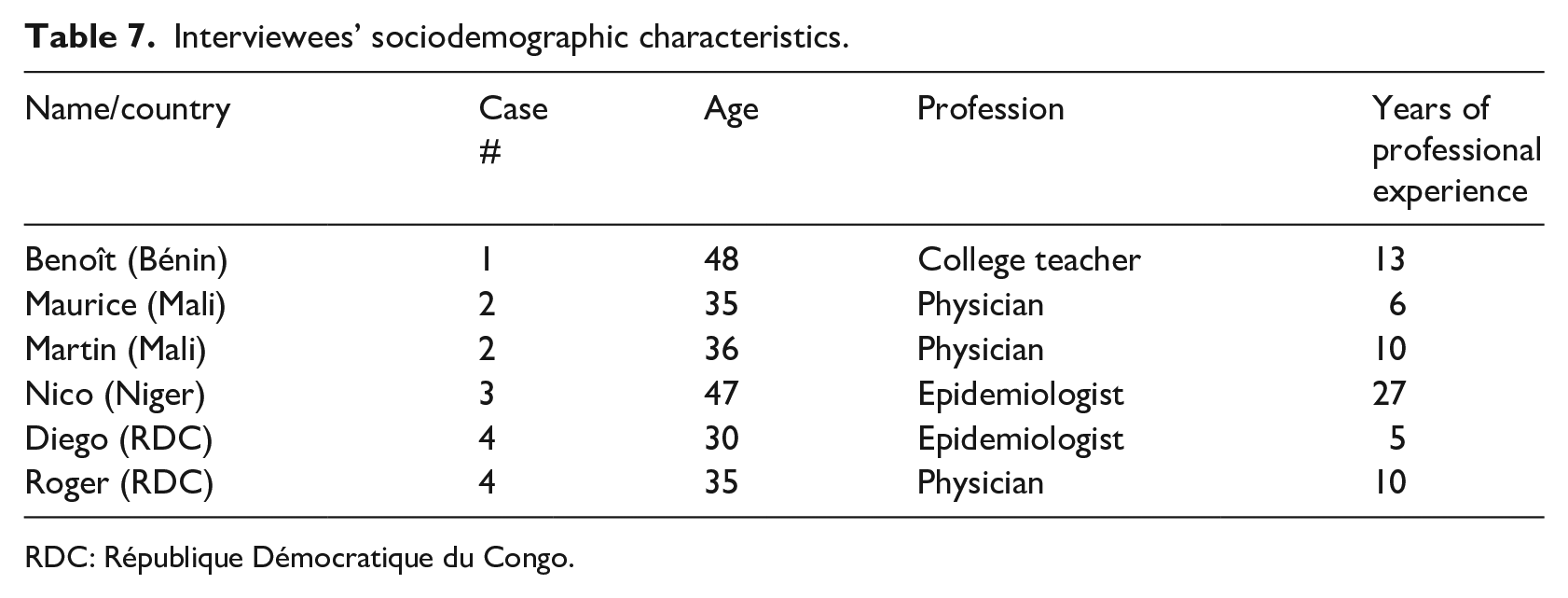
RDC: République Démocratique du Congo.
The upcoming paragraphs introduce participants’ accounts by the predefined analytical themes, as well as specific contents portraying multiple case studies. Their narratives cover features of the planning and implementation of the HP projects within the local context (where), profile of the promoter (who), situations (issues, problems), barriers/obstacles, decisions (what), actions (solutions), evaluation/appraisal, understanding/learning and unsolved issues.
Targeting HP actions with children and youth in schools as a future health literacy and health knowledge disseminator
Case #1: Bénin
Benoît developed and implemented HP programmes at 16 schools, each lasting for 2 months, with a total of 250 students. The Ministry of Health provided doctors and nutritionists. With a focus on NCDs, a consultation with the school administrations explored local health needs, and the chosen topic was the promotion of physical activity and high nutritional education. Afterwards, the students who engaged in the programme demonstrated changes in attitudes (free translation): . . . [they] take care of their health, they become actors of their own health instead of being observers.
Although the programme itself was conducted very extensively, time constraints were identified as the main rationale for a better evaluation. Evaluation reports were sent to the Ministry of Health and the Ministry of Education, but Benoît (free translation) ‘normally does not [expect to] receive any response’. This lack of responsiveness from the local political stakeholders can hinder the HP programme from being widespread and effective. The involvement of media and NGOs can enhance effectiveness, by prompting the allocation of required material to allow the Beninese HP professionals to access teaching material (overhead projector and computer), and the financial support to travel. Sine qua non conditions are teachers being trained on health matters to accurately transmit health information to the students, and students’ receptiveness to it.
Case #2: Mali
With financial support from the NGO, Maurice provided HP training to 24 health workers, as well as teachers’ and students’ representatives. Acknowledging the Malian culture, Maurice appealed to the individuals’ emotions by using family bonds as a justification to teach about smoking-related dangers threatening their family unit. Martin used a similar awareness-raising approach, which also involved putting children and the youth at the forefront of HP, both hoped to address their awareness issues related to HP in schools.
After correcting inappropriate health habits, both interviewees reported that parents began to cease to smoke in front of children, thus becoming parental role models (free translation): ‘And in front of [Maurice], people have broken cigarettes’.
Both interviewees aimed for a wider political awareness through youth training to become a trainer for others in their social environments. Due to the high number of illiterate youth not enrolled in schools, this social action might have a positive impact on health literacy and life expectancy, due to the increase of health knowledge about smoking-related dangers. Through effective dialogue and communication, the number of people who smoke can decrease, as Martin stated (free translation): . . . it depends on how you speak to them and . . . whether you are convinced of the message you want to get across.
Case #3: Niger
Through an epidemiological lens, Nico reiterated that sedentary lifestyles and low income, paired with poor diets, result in high rates of early-life diabetes or hypertension, and child obesity. The over-accessibility to students of unhealthy, low-price and unhygienic foods also presents a significant risk for NCDs to tackle these negative factors, suggesting that the school curriculum should have HP contents. In Niger, the Ministry of National Education implemented an HP programme, which was discontinued. Nico intended to relaunch that programme by relying on the national strategic plan and was considering the involvement of other global partners. While acknowledging the importance of curative care, Nico expressed his feelings regarding the importance of HP (free translation): We must first prevent [health issues] . . . Health should no longer be the sole concern of health workers. But it must be seen in a global framework.
Case #4: RDC
Similarly, in RDC, diabetes, hypertension and cardiovascular disease (CVD) plague the community. Actions for HP must be integrated and multisectoral (health and education), in order for there to be successful dissemination among students. To the Ministry of Health, Diego proposed launching a prevention-focused HP programme at a national university. With the approval and support of the Ministry, it would be piloted in four out of RDC’s 26 provinces. First, the programme would train certain university executives at the intermediate level, nursing staff at the provincial level and educational staff, allowing for the effective implementation of the project.
Two NGOs and parents’ associations were the financial stakeholders. Politicians were informed about the programme implementation but did not express a commitment to it. Roger outlined his attempt at nutritional awareness among kindergartners by establishing a small HP project. He focused on teaching children how to make informed choices regarding the kind of food and drinks they consume (free translation): ‘it was a small project that I wanted to put into action’.
In addition, other children were taught the importance of fighting the use of tobacco, so when they see their parents smoking, they have the ability to prohibit it. The lack of resources available to Roger made it difficult to expand the project and to involve those school staff in charge of HP.
Learning due to unexpected results and achievements
Case #1: Bénin
Benoît witnessed post-intervention behavioural changes in a number of students. Once children learned about hand washing, they asked their schoolteachers for hand washing stations to make it more accessible to all students. In addition, their teachers also better understood the necessary actions to implement health teachings.
Case #2: Mali
Despite the fact that the audience consisted of smokers, they understood the danger smoking presented to community health. After learning about smoking-related risks, the community suggested wide dissemination of this information to schools and health centres. Maurice was especially surprised when actions were taken by close relatives to stop smoking. Discussions had in an attempt to identify specific ways in which HP can be implemented among the youth population. Remarkably, Maurice received support from the community, which was very interested in setting up training activities for HP.
Case #4: RDC
Diego described how important it is to be persistent, and that even if there are not many resources, the HP project could start off small, using what was available. Diego also had an advantage in having connections with the school, and a site for the implementation of HP activities, allowing for the successful dissemination of health teachings.
Ideas for the future evaluation of HP programmes
It was reported that in Bénin, when the awareness training ended, the Ministry stopped offering human resources, but the HP project can continue by utilizing the knowledge previously shared by the physicians and nutritionists. In Mali, to evaluate the future HP projects, more robust data and observations will be made to document youth smoking reduction and cessation. For Niger, through the development of focus groups, participants can be invited to respond to surveys. New ideas for implementation in RDC include the professional media raising awareness to encourage the acceptance of the HP efforts that could affect future results. Nationally, radio broadcasts are easily accessible to everyone, but a lack of resources persists. Furthermore, evaluation could benefit from ALIAM’s sociopolitical leadership by becoming an intermediary political stakeholder between the Ministry and the professionals involved in the HP programmes. ALIAM would mobilize professionals in HP roles and present programme results to the government, furthering political support.
Bases for a regional, national and inter-African network for HP
Case #1: Bénin
ALIAM pursues their leadership actions by working with health promoters to organize other HP training courses. After training in Tunisia, all African trainees remained connected through a Facebook page to discuss further training opportunities and exchange information. Benoît created an NGO to legally congregate them in 23 countries, which makes them eligible for international funding and can assist in their future HP endeavours.
Case #2: Mali
Maurice ensured constant communication through emails to reach out to other trainees and the facilitators of the training programme. This networking allows for an inter-African collaboration. In fact, the implementation of the training programmes for HP initiatives enabled the creation of an inter-African HP network in the regional Francophone countries. Martin stated that participation at the International Junior Chamber (an NGO) allowed him and others to identify small community problems and design-specific interventions. Finding a viable partner for initiatives is always an issue.
Case #3: Niger
Nico stressed the importance of establishing global networks to support advocacy actions and the comparison of HP-related results by governments’ undertaken actions. Creating networks with other trainees enabled discussions of national health policy. He foresaw that the creation of future national HP directorates, in collaboration with the inter-African and global networks, would result in more robust advocacy for better health policies and an increased transparency in the governments’ actions.
Case #4: RDC
Diego and Roger received multiple support from a director of a health programme, United Nations Children’s Fund (UNICEF), private donors and the Ministry of Health for initiating their HP project. This favourable context allowed for a large-scale implementation with fewer obstacles. For that, they established a regional network, including about 20 professionals from certain African regions extensive to Central Africa ones. The work ensured a more sustainable and effective networking, because all participants were aware of the outlined goals in relation to HP, with a high understanding of plans of action. The aforementioned participants indicated that ALIAM could play a pivotal role in HP in the region, in strict collaboration with UICC. Figure 2 displays a representation of key ideas shared by them in such projected futures.
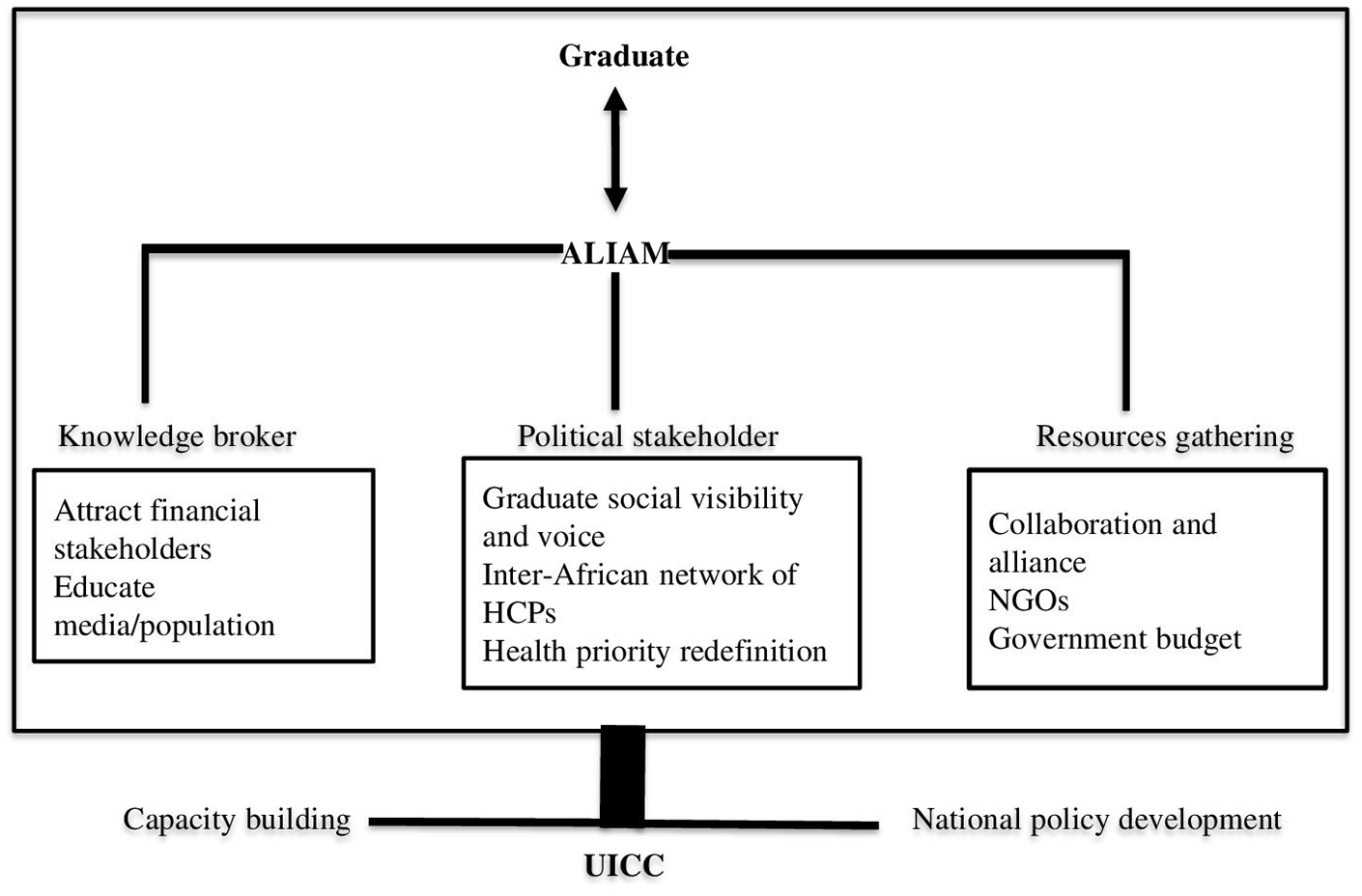
Future collaboration among graduates, ALIAM and UICC.
Five years’ career plan progression as a professional and advocate for social rights for HP in schools
Benoît expressed his interests in consolidating his professional future towards HP and prevention, since his successful creation of an HP NGO to educate other health promoters oriented towards school health. Due to his background as a sociologist–anthropologist, he expressed how being a representative of an NGO would allow him and others to tackle issues of social power in negotiation with governments. Nico intends to set up HP activities to bring the HP programme to the level of the Minister of Public Health. This implies a career redirection from maternity care to a return to an HP branch to work with the Ministry and other sectors. Diego’s main goal was the successful implementation of HP in schools across the country, in all 26 provinces. Roger expressed his interest in a master’s degree in social economy and solidarity to provide tools for the set-up of a social project, including a new role of an HP officer in a school environment.
Discussion
It is noticeable that the most support among all four forms of community capital was provided by professionals in the fields of health or education, and the least support was provided by parents. In comparing the support received by both stakeholders and decision-makers through social capital, it can be concluded that the decision-makers provided support to a greater extent, although by a slight margin. This is not to devalue the support provided by the stakeholders, but rather to better understand the sources of the contributions as they relate to each form of capital, in order to both evaluate the effectiveness of the support received by each party and how best to navigate future interactions.
The results illustrate how, as a continent, Africa is facing challenges in delivering timely and appropriate health care services to citizens but is also challenged by the inability to tailor health services to the specific communities’ greatest needs. Results also confirmed that types of HP strategies should be considered when engaging with community members, which can have a significant impact on minimizing the severity and spread of communicable diseases (Laverack and Manoncourt, 2016). Witter et al. (2020) found that, although community members had relatively high levels of knowledge of NCD risks, they lacked the time and knowledge required to improve these issues. A lack of evidence of efficacy regarding NCD HP interventions can lead to the misallocation and mismanagement of valuable resources delivered in low- to middle-income countries (Jeet et al., 2018). Poor health policy oversight makes it challenging for governments and health staff to capably monitor and manage policy processes and their performance (Lane et al., 2020).
Results confirmed that, in addition to providing opportunities for school communities, strong school health policies also serve as positive modelling behaviours for the larger scale community (WHO, 2020). To achieve stakeholder’s buy-in, students, teachers, parents and the community should be involved in the implementation and analysis of healthy school policies that stretch beyond the curriculum. An emphasis should be placed on life skills educators receiving extensive training in utilizing participatory approaches, as they can have an important impact in the development of healthy behaviours and the capacities needed for improved life skills teaching (WHO, 2020). HP has the potential to positively impact large populations, owing to the fact that the population of youth under 18 currently represents 50% of Africa’s population, a statistic that is expected to increase to 40% of the global youth population in 2050 (UNICEF, 2017).
Future initiatives may consider the development of HP programmes that rely on elements of popular culture that is appreciated by youth. It can be done by the mobilization of local artistic companies, martial arts, circus arts, production of music videos, creation of e-apps and so on. As examples, the readers are invited to watch: https://www.youtube.com/watch?v=4Qk22iVm1HI&t=1s, https://www.youtube.com/watch?v=BtulL3oArQw, https://www.youtube.com/watch?v=wGoodWEtV8c, https://hhph.org/repository/
Limitations
The unknown context of the new role being implemented and the lack of feasibility of being immersed in the African context of HP have been taken into consideration as limitations. We have made a conscious attempt to reach a theoretically significant interpretation of the results, identify rival explanations and minimize threats to the internal validity that was not reached due to the paucity of in-depth evidences. Limited (not a minimum of three participants per country) and superficial evidences per countries restricted an in-depth data analysis. It is noteworthy to say that the minimum number of three participants per country does not allow for the procedure of intragroup comparison as a qualitative analysis procedure. Therefore, this methodological limitation restrains the transferability of findings (Paillé and Mucchielli, 2016).
Contribution to the field
This study was necessary to evaluate the impact that health education and teachings directed at health professionals in the public school system could have on the implementation of HP in Francophone African countries. Its contribution to the field of HP relies on the identification of key community forms of capital to be mobilized and invested, mainly the community and professional stakeholders.
Conclusion
This evaluation disclosed that the major social impacts of HP projects relate to the support provided by the community stakeholders mobilizing their own individual and collective assets. The contextualized HP actions unfolded according to WHO objectives for youth health for the region, intertwining deeds in partnerships and new alliances to tackle compromised SDH for NCDs. Despite limited support from political stakeholders (justified by historical, philosophical, and political gaps and misdeeds) at the frontline level, the health promoters were somehow successful in awakening youth’s, children’s and parents’ awareness for the pressing need to adopt HP behaviours. Financial and political stakeholders should ensure the feasibility of HP projects in school settings. The evidence also uncovered professional networking, collaboration and exchange that could help regional health promoters to make their professional plans in the field of HP a reality. A larger number of cases would have made the reached conclusions more tenable. A future follow-up study with a larger sample should be conducted.
Footnotes
Acknowledgements
The authors acknowledged the contribution of Mr Clément Picot Ngo, PhD candidate, who reviewed the early draft of this manuscript. We also wish to thank the study participants for their cooperation and enthusiastic support that made this study possible despite all the operational and technical difficulties. Special thanks to Robyn Huizenga for her support in the preliminary literature review.
Author contributions
M.S.Z., C.M. and M.K. conceived the study. M.S.Z., C.M., C.H. and A.G.G. designed the questionnaire. M.S.Z. and C.M. piloted data collection methods. M.S.Z. and C.M. managed data collection. M.S.Z. and M.E.D. conducted interviews, M.E.D. transcribed and coded the interviews verbatim. M.S.Z., M.E.D., F.-M.A. and A.H. undertook data analysis. M.S.Z. led in preparing the manuscript with M.E.D., F.-M.A. and A.H. with inputs from D.Z., C.M., M.K., C.H. and A.G.G. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the 2016 Ryerson University Study-Work programme scholarship earned by M.E.D. Publication was supported by Ryerson University, Faculty of Community Services, Writing Week Initiative, Winter 2021.
Ethical approval and consent to participate
This study was reviewed and approved by the Ryerson Research Ethical Board (REB 2016-129). All participants provided an oral and/or an implicit online informed consent.