
Abstract
This study examines the sex-specific impact of marital trajectories among older adults on successful aging to help social workers identify those most at risk for sub-optimal outcomes who may benefit from targeted interventions. Binary logistic regression analyses were used to investigate 7641 older Canadians who were classified as ‘aging successfully’ in the baseline wave of the Canadian Longitudinal Study on Aging. Men who were continuously married, continuously widowed, or became married between the waves were more likely to age successfully than their never-married counterparts. For women, marital trajectories played a modest role. Social work interventions are discussed.
Introduction
Canada’s population is rapidly aging, with more older adults than ever. The 2016 Census marked the first time that there were more older adults aged 65 and over (5.9 million) than there were children aged 14 and under (5.8 million) (Statistics Canada, 2016). The gap between the number of older adults and the number of children continues to widen. By 2021, the number of older adults aged 65 and over had risen to 7 million (18.3%), representing nearly 1 in 5 Canadians (Statistics Canada, 2022).
In addition to the burgeoning of the aging population, Canada’s family structure is also changing. Studies have shown that cohesive family structure and social support are important factors in successful aging (Howie and Troutman-Jordan, 2014; Rowe and Kahn, 2015). The average size of Canadian households has decreased from 5.0 persons in 1901 to 2.4 persons in 2016 (Tang et al., 2019). The number of one-person households has grown from 7% in 1951 to 28% in 2016.
This study investigates the prevalence of successful aging among older Canadians who were never married, divorced, separated, or widowed and the sex differences of trajectories of marital status on successful aging in the Canadian context. Using data from a national, population-based, longitudinal study on aging, the Canadian Longitudinal Study on Aging (CLSA), this study investigates the prevalence of successful aging among males and females based on marital status and the sex differences of trajectories of marital status on successful aging.
Review of the literature
Successful aging
As has been discussed elsewhere (Ho et al., 2022, 2023), the concept of ‘successful aging’ was chosen as the guiding notion of this study instead of other concepts of aging well (e.g. ‘active’, ‘effective’, ‘harmonious’, ‘healthy’, ‘optimal’, ‘positive’, ‘productive’, and ‘thriving’ aging) because of its relatively long history (Pruchno, 2015), popularity (Liang and Luo, 2012), and comprehensiveness (Fernández-Ballesteros, 2019). However, the concept of ‘successful aging’ is not without its critics (Rowe and Kahn, 2015).
There are also discrepancies between researcher-derived classifications of successful aging, in which only approximately one-third meet the stringent criteria, and the perspective of older adults, where the vast majority (92%–94%) perceive themselves as aging successfully (Bowling, 2006; Depp and Jeste, 2006). The reality is that most older adults do not live with near-perfect health but have various forms of chronic diseases and physical disabilities (Morris et al., 2018; Statistics Canada, 2021). Therefore, a more balanced definition of successful aging is needed that genuinely reflects the experiences and perceptions of older adults.
Among existing models of successful aging, Young et al.’s (2009) multidimensional model of successful aging attempts to explore the coexistence of successful aging and chronic illness. They suggest that successful aging may coexist with physiological limitations such as physical illnesses and disabilities if compensatory psychological and/or social resources are available to deal with the physical limitations. Their suggestion addresses the limitations of researcher-derived classifications of successful aging and reflects the reality of older adults living with various health conditions. Young et al.’s (2009) model offers a broader perspective on understanding successful aging (Swift and Tate, 2015).
Marital status
Earlier research studies on the health benefits of marriage went back to 1858 when British epidemiologist William Farr studied the mortality rates of the ‘unmarried’, ‘the married’, and the ‘widowed’ using birth, marriage, and death records (Parker-Pope, 2010). This pioneering study found that unmarried people were more likely to die from disease compared to their married counterparts, while widowed people fared even worse. Recent studies indicate that marriage usually has positive effects on health behaviors (e.g. alcohol consumption, drug use, smoking, body weight, and exercise), health care access, use and costs, mental health (e.g. depressive symptoms), physical health (e.g. chronic health conditions), and longevity (The Assistant Secretary for Planning and Evaluation, 2007; Vaillant, 2015). Researchers have also found that marriage protects people’s mental health during disruptive times, such as the COVID-19 pandemic (Jace and Makridis, 2021).
A 75-year longitudinal prospective study followed 268 Harvard-educated men since the 1940s. The research team later found that the men who reported the best outcomes (e.g. high income, low psychological distress, good physical and mental health, availability of social supports, closeness to children) were married earlier and stayed married longer compared to those who reported the worst outcomes (Vaillant, 2015). It was concluded that ‘loving people for a long time is good’ (Vaillant, 2015: 221) and being in a good marriage or a happy and long-term relationship is important to age well. This idea is consistent with other studies that showed successful agers were more likely to be married or live with someone than those who were not considered successful agers (81.2% vs 77.8%) (Sabia et al., 2012).
The profile of Canada’s population has changed substantially in the past few decades with respect to marital status. According to the 2016 Census data, about 26% of older adults aged 65 and over lived alone, while 74% lived with a spouse or common-law partner, a child, other relatives, or non-relatives (Statistics Canada, 2017a). As women had a higher life expectancy than men, and women also tended to marry men older than themselves, older women (33%) were more likely to live alone than older men (18%) (Statistics Canada, 2017b). Between 1981 and 2016, older adults who lived alone and were widowed decreased (from 33% to 22%), while those who lived alone and were separated or divorced were more than tripled (from 9% to 32%) (Tang et al., 2019), indicating changes in family composition over time. However, to the best of our knowledge, there is no study on the relationship between trajectories of marital status and successful aging in Canada or worldwide.
Studies have shown a strong association between social isolation and wellness in later life, especially during the COVID-19 pandemic (Clair et al., 2021), and research indicates those with children are less vulnerable to premature mortality (Barclay and Kolk, 2019), and older adults with adult children have higher levels of happiness than their childless peers (Guy, 2019). However, to the best of our knowledge, there has not yet been a study on the relationship examining the interaction between social isolation status and successful aging among those with and without adult children. Therefore, these variables are included in the study to see if they have an impact on older adults experiencing various trajectories of marital status. Social work implications for program, policy development and future research will be discussed.
Conceptual framework
The study of successful aging has been criticized for focusing primarily on individual success and neglecting various social and structural factors that influence aging (Martinson and Berridge, 2015). Furthermore, researcher-derived studies on successful aging have also been criticized for not reflecting the reality and experiences of older adults (Teater and Chonody, 2020). This study uses a synthesized conceptual framework composed of three theoretical perspectives: ecological systems theory (Bronfenbrenner, 1979; McLeroy et al., 1988), a multidimensional model of successful aging (Young et al., 2009), and the concept of complete mental health (Keyes, 2002). The ecological systems theory (Bronfenbrenner, 1979; McLeroy et al., 1988) emphasizes the importance of understanding the connections between people and their environments (Pardeck, 1988). It helps illuminate how structural factors (e.g. economic, organizational, political, and social environments) may influence the aging process. Young et al.’s (2009) multidimensional model of successful aging postulates that successful aging may coexist with chronic illnesses and functional limitations if psychological or sociological mechanisms compensate for physiological decline and promote successful aging. It proposes multiple pathways to successful aging despite one’s physiological limitations. Keyes’ (2002) concept of complete mental health covers the emotional, psychological and social aspects of mental health and argues that ‘mental health and mental illness are not opposite ends of a single continuum’ (p. 209). It provides operational definitions of emotional, psychological and social well-being. Combining the ecological systems theory (Bronfenbrenner, 1979; McLeroy et al., 1988), the multidimensional model of successful aging (Young et al., 2009), and the concept of complete mental health (Keyes, 2002), a comprehensive integrative conceptual framework for the study of successful aging has been developed and more fully described in our previous publications (Ho et al., 2022, 2023). This study defines successful aging as a combination of physical, psychological, mental, and social wellness wherein psychological, mental, and social reserves can compensate for physical limitations. In other words, an older adult can still experience successful aging if s/he is living with chronic diseases and/or disabilities.
The concept of successful aging used in this study is built on both objective and subjective measures of aging. In keeping with many researcher-derived definitions (e.g. the presence of physical, mental, and social functioning, psychological resources, and life satisfaction) (Swift and Tate, 2015), the new concept includes the absence of memory problems, serious mental illness, and chronic disabling pain, as well as the presence of adequate social support (Ho et al., 2022, 2023). With respect to physical health, we have modified the usual restriction that successful agers must be free of any chronic health conditions. Instead, our definition requires that individuals have no limitations in activities of daily living (ADLs) and instrumental activities of daily living (IADLs), regardless of the number of chronic illnesses they have. In addition, we have incorporated the older adults’ subjective perception of their aging process, physical health, mental health, and emotional well-being (e.g. happiness and life satisfaction) as good.
This study examines the association between marital status, including trajectories of marital status, on successful aging among older men and women by addressing the following research questions:
Research Question 1 (RQ1). Are trajectories of marital status associated with successful aging at time 2?
Research Question 2 (RQ2). Does adjusting for 21 baseline characteristics attenuate the association between trajectories of marital status and successful aging?
Research Question 3 (RQ3). Are there sex differences in the relationship between marital trajectories and successful aging at time 2?
Research Question 4 (RQ4). Which trajectories of marital status are associated with successful aging at time 2 for males and females?
Methods
Study population
As has been discussed elsewhere (Ho et al., 2022, 2023), among approximately 50,000 respondents between the ages of 45 and 85 years involved in the CLSA, 21,000+ respondents were interviewed through the telephone (Tracking Cohort), and 30,000+ respondents were interviewed at home and assessed at one of the data collection sites (Comprehensive Cohort) (Raina et al., 2009). All respondents will be followed every 3 years for at least 20 years or until death. Baseline data of the CLSA Comprehensive Cohort were collected between 2011 and 2015, while time 2 data were collected between 2015 and 2018. The CLSA has gone through 13 research ethics boards across Canada. Further information about the CLSA can be found at www.clsa-elcv.ca (accessed on 28 August 2022). Data used in this study were drawn from the baseline and follow-up 1 data (hereafter referred to as time 2 data) from the CLSA Comprehensive Cohort. Among the 30,097 respondents at baseline, 27,799 respondents participated in wave 2. Among them, 18,978 respondents were 60 years or older at time 2. Of these respondents, 10,375 were excluded because they were not aging successfully at baseline, and 962 had missing entries in any analyzed variables at time 2. The final sample size was 7641 respondents, of whom 3926 were male and 3715 were female. This study involving secondary data analysis of CLSA data was approved by the Health Sciences Research Ethics Board of the University of Toronto (protocol number: 38284).
Measures
Dependent variables assessed at both baseline and time 2
Successful aging
Respondents who met all four sets of criteria of (1) physical wellness (i.e. having no limitations in performing [ADLs] and [IADLs], and no chronic and disabling pain that limits activity); (2) psychological and emotional wellness (i.e. not having anxiety, depression; Hann et al., 1999; Radloff, 1977); memory problems and post-traumatic stress disorder [PTSD]; (Prins et al., 2016), feeling depressed rarely or never, or some of the time, feeling happy occasionally or all of the time, and feeling satisfied with life occasionally or all of the time (Diener et al., 1985); (3) social wellness (i.e. having someone to advise them about a crisis, having someone to show them love and affection, and having someone to confide in or talk to about themselves or their problems at least most of the time); and (4) self-rated wellness (i.e. having ‘good’ to ‘excellent’ self-rated aging process, physical health, and mental health) were classified as successful agers (Ho et al., 2022, 2023). Otherwise, they were considered typical agers. Successful aging status was identified at both baseline and time 2.
Independent variables assessed at the baseline wave of data collection
Trajectories of marital status between baseline and follow-up
The primary focus of this study is to examine the sex differences of trajectories of marital status on successful aging. Trajectories of marital status were categorized in the following: (1) never-married; (2) continuously married; (3) continuously widowed; (4) continuously divorced or separated; (5) from not married (i.e. single, widowed, divorced, or separated) to married; (6) from married to not married (i.e. widowed, divorced, or separated); and (7) other changes.
Social isolation status
The variable was derived from responses to questions on respondents’ last contact with their children, siblings, other relatives, close friends, and neighbors who did not live in the same household (Tong et al., 2021). It was coded as ‘not socially isolated’ if respondents had contacts with relatives, friends, and neighbors in the past week or two; ‘mildly socially isolated’ if respondents had contacts with relatives, friends, and neighbors in the past month but not in the past week or two; and ‘extremely socially isolated’ if respondents had no contact with relatives, friends, and neighbors in the past month. As the numbers of respondents who were ‘mildly socially isolated’ (n = 110) and ‘extremely socially isolated’ (n = 41) at baseline were small, it was coded as ‘not socially isolated’ (n = 7490) and ‘socially isolated’ (n = 151).
Have a child or not
This variable was dichotomized as ‘had no child’ and ‘had 1 child or more’ responses based on the question asking respondents how many living children they have. It included children whom respondents gave birth to, adopted, stepchildren, and their partner’s children.
Covariates
To understand what baseline factors were associated with successful aging at time 2, we included a wide range of demographic, socioeconomic, lifestyle and health-related variables in our analysis. The exact questions used for these measures are available elsewhere (please see https://www.mdpi.com/1660-4601/19/20/13199#; accessed on 13 October 2022).
Statistical analysis
SPSS Version 28 was used to conduct all analyses in this study. The sample sizes are presented in their unweighted form, but the percentages and odds ratios are weighted. The weights provided by the CLSA were normalized/standardized to produce population representative estimates while maintaining the original sample size. Bivariate analyses such as chi-square tests and t-tests were conducted to compare successful agers and typical agers. Three binary logistic regression analyses were conducted for all respondents, with the trajectories of marital status as the exposure of interest and with successful aging at time 2 as the outcome. In Model 1, only trajectories of marital status were included. In Model 2, age and sex were added to the analysis. In Model 3, all the other baseline covariates were added to the model. To determine if there were differences by sex in the relationship between marital trajectories and successful aging, an interaction effect was calculated. Once this interaction term was determined to be significant, analyses were conducted separately for male and female respondents. A significance level of .05 (p < .05) was considered statistically significant for all the tests, and 95% confidence intervals (95% CIs) were used in the logistic regression. Hosmer–Lemeshow test and variance inflation factor (VIF) were calculated to check for multicollinearity.
Results
Descriptive statistics
The characteristics of successful agers are provided for the full sample and for men and for women in Appendix 1, Table 1. In which, all variables were at baseline, except the trajectories of marital status variable which was created by comparing respondents’ marital status at baseline and at time 2. Descriptions of the sample size (unweighted counts) and chi-square statistics (based upon the normalized weighted percentages) of the final sample (n = 7641) are presented. Among all 7641 respondents, 97.5% rated their aging process as excellent, very good or good when asked, ‘In terms of your own healthy aging, would you say it is excellent, very good, good, fair, or poor?’ Description of sample characteristics by successful aging status is described in Appendix 1, Table 2, and trajectories of the marital status of respondents and sex are shown in Appendix 1, Table 3.
With the newly defined measure of successful aging proposed in this study, the prevalence of successful aging at time 2 was 70.5% (95% CI = 0.70, 0.72). More than 7 in 10 (72.3%) of those who rated their aging process as good to excellent were identified as successful agers using the expanded definition of successful aging described in this study:
Research Question 1 (RQ1). Are trajectories of marital status associated with successful aging at time 2?
The results of the binary logistic regression models (see Appendix 1, Figure 1) confirmed that the age-sex adjusted odds of achieving successful aging at time 2 were significantly higher among continuously married older adults (aOR = 2.01, 95% CI = 1.54, 2.62), continuously widowed older adults (aOR = 1.45, 95% CI = 1.04, 2.01), continuously divorced or separated older adults (aOR = 1.42, 95% CI = 1.03, 1.96), and older adults who became married between baseline and time 2 (aOR = 2.96, 95% CI = 1.69, 5.19) when compared to their never-married counterparts, while the adjusted odds ratio of older adults who became not married since baseline was not significantly different from their never-married peers:
Research Question 2 (RQ2). Does adjusting for 21 baseline characteristics attenuate the association between trajectories of marital status and successful aging?
In comparison to respondents who were never married (see Appendix 1, Figure 2), the unadjusted odds of achieving successful aging were almost double for respondents who were continuously married (unadjusted OR = 1.92, 95% CI = 1.47, 2.50) and almost triple for respondents who became married since baseline (unadjusted OR = 2.92, 95% CI = 1.67, 5.10), and 38.6% more for respondents who were continuously divorced or separated (unadjusted OR = 1.39, 95% CI = 1.01, 1.91) when only trajectories of marital status were considered.
In the Full Model, which adjusted for 21 factors, the adjusted odds of achieving successful aging for respondents who were continuously married (aOR = 1.60, 95% CI = 1.17, 2.18) and those who married between the waves (aOR = 2.51, 95% CI = 1.40, 4.48) remained significant, but were slightly attenuated. The continuously divorced or separated group’s odds of successful aging were also substantially attenuated after we adjusted for 21 factors so that it no longer reached statistical significance (aOR = 1.35, 95% CI = 0.95, 1.92). With respect to other variables in the analyses, social isolation status was significant, but having a child was not significant:
Research Question 3 (RQ3). Are there sex differences in the relationship between marital trajectories and successful aging at time 2?
The prevalence of successful aging at time 2 among males (70.5%, 95% CI = 0.69, 0.72) and females (70.4%, 95% CI = 0.69, 0.72) was similar. However, the adjusted odds of successful aging were significantly higher in females than in males once control variables (i.e., demographic, socioeconomic, lifestyle and health-related variables) were taken into account (aOR = 1.21, 95% CI = 1.08, 1.36). The prevalence of successful aging by marital trajectories varied for men in comparison to women (never married: male − 51.6%, 95% CI = 0.42, 0.62 vs female − 63.5%, 95% CI = 0.57, 0.72; continuously married: male − 72.6%, 95% CI = 0.71, 0.74 vs female − 75.3%, 95% CI = 0.73, 0.77; continuously widowed: male − 62.5%, 95% CI = 0.54, 0.71 vs female − 59.1%, 95% CI = 0.55, 0.63; continuously divorced or separated: male − 59.7%, 95% CI = 0.51, 0.68 vs female − 69.3%, 95% CI = 0.67, 0.71; became married since baseline: male − 74.6%, 95% CI = 0.64, 0.85 vs female − 83.0%, 95% CI = 0.72, 0.94; became not married since baseline: male − 48.2%, 95% CI = 0.37, 0.59 vs female − 49.6%, 95% CI = 0.41, 0.59) (analyses not shown in a table).
Interaction effect
To determine if the observed differences indicated sex differences, we investigated if the interaction between marital trajectories and sex was statistically significant, and we found that it was, χ2(6) = 14.3, p < .05. Thus, sex-specific analyses were warranted:
Research Question 4 (RQ4). Which trajectories of marital status are associated with successful aging at time 2 for males and females?
As shown in Appendix 1, Figure 3, for the 3926 male respondents, significant positive associations between marital status and successful aging were observed in respondents who were continuously married (aOR = 2.56, 95% CI = 1.53, 4.28), continuously widowed (aOR = 2.50, 95% CI = 1.22, 5.09), or became married since baseline (aOR = 3.83, 95% CI = 1.67, 8.77) when compared to their never-married peers.
In contrast, for the 3715 female respondents, there were no significant differences with respect to successful aging between never-married individuals and any of the other marital categories (i.e. continuously married, continuously widowed, continuously divorced or separated, became married since baseline, and other trajectories of marital status since baseline), with the one exception being that those females who transitioned from married to not married between the waves had significantly lower odds of successful aging (aOR = 0.48, 95% CI = 0.28, 0.81).
Assessment of model fit
The results of the Omnibus Tests of Model Coefficients were highly significant – all respondents’ model: χ2(37) = 441.9, p < .001; male respondents’ model: χ2(36) = 221.0, p < .001; female respondents’ model: χ2(36) = 251.0, p < .001 – indicating that the final models are significantly better than the baseline models. The Nagelkerke’s R2 values equal to 0.079 to 0.094 (all respondents’ model: Nagelkerke’s R2 = 0.081; male respondents’ model: Nagelkerke’s R2 = 0.079; female respondents’ model: Nagelkerke’s R2 = 0.094) implying that the final models explain 7.9% to 9.4% of the variation in successful aging status. All VIFs of the predictor variables in all three models (i.e. all respondents’ model, male respondents’ model, and female respondents’ model) ranged from 1.00 to 1.18 (VIF < 10), indicating that multicollinearity was not a concern.
Discussion
This study introduced an expanded measure of successful aging by combining modified researcher-derived classifications of successful aging and lay perspectives of successful aging. The concept of successful aging used in this study as having no limitations in performing ADLs and IADLs, no chronic and disabling pain that limits activity, the absence of mental illness and memory problems, having adequate social support, in addition to the older adults’ subjective perception of their aging process, physical health, mental health and emotional health (e.g. happiness and life satisfaction) as good (Ho et al., 2022, 2023). Using this new definition of successful aging, the prevalence of successful aging at time 2 was 70.5% (95% CI = 0.70, 0.72), and more than 7 in 10 (72.3%) of those who rated their aging process as good to excellent were identified as successful agers. The new measure of successful aging addressed the discrepancies between researcher-derived classifications of successful aging (i.e. approximately one-third of older adults met the stringent criteria of successful aging) and lay perspectives of older adults (i.e. 92%–94% perceived themselves as aging successfully) (Bowling, 2006; Depp and Jeste, 2006), and provided a more balanced definition of successful aging.
This study found that the prevalence of successful aging was significantly higher among respondents who were continuously married, widowed, divorced, or separated, or became married since baseline when compared to never-married respondents. Fewer respondents who became widowed, divorced, or separated since baseline achieved successful aging compared to their never-married counterparts. However, when all 21 variables were taken into account, only those who were continuously married or who became married after the baseline interview differed significantly with respect to successful aging in comparison to their never-married peers.
Our sex-specific analysis underlined the importance of considering sex differences in future research. In particular, trajectories of marital status were of only minimal importance for women (with only those transitioning from married to not married differing from the never-married group). In sharp contrast, among men, almost every marital trajectory was significantly more likely to achieve successful aging than men who were never-married, except for men who were continuously divorced or separated. The prevalence of successful aging at time 2 among males and females was similar.
Manfredini and colleagues (2017) synthesized the findings of 48 articles on the relationship between marital status, cardiovascular diseases, and cardiovascular risk factors. They found that marriage was associated with better physical health for both men and women, while single men generally had the poorest physical health outcomes. They further suggested that married people might have ‘healthier meals, better sleep, less stress, financial benefits, and better mood’ compared to single people (Manfredini et al., 2017: 630). Wang et al. (2020) found that single men had a higher risk of stroke and a higher risk of all-cause mortality compared to single women, while divorced or separated men experienced a higher risk of cancer mortality and a higher risk of cardiovascular disease mortality. Stimpson and Wilson (2009) also reported that both men and women who were single or widowed had lower odds of getting cholesterol screening in comparison to married individuals. Future research is required to understand the connections between marriage, health behaviors, and health outcomes and to inform social work practice in these areas.
Several factors associated with successful aging were similar for males and females: Being younger (i.e. for male respondents: 55–79 years old; for female respondents: 55–74 years old), not being socially isolated, engaging in strenuous sports, and not having sleeping problems were significant baseline factors observed in both male and female respondents. However, there were some differences with respect to particular baseline factors, which were significantly associated with successful aging for one sex but not the other. Unique significant baseline factors for male respondents included being continuously married, continuously widowed, becoming married since baseline, not being obese, not smoking, and living without heart disease or osteoporosis. For female respondents, having higher income (i.e. above poverty line income), engaging in moderate sports, and not having arthritis were significant factors. Contrary to what was observed in the male respondents, trajectories of marital status were not significant among female respondents, except transitioning from married to not married over the course of the study was associated with significantly lower odds of successful aging in comparison to the never-married respondents. When we compared the subsamples for each of the six marital trajectories (e.g. continuously married, never married), there was not even one baseline characteristic which was consistently associated with successful aging in all of the marital trajectories.
Consistent with the findings in this study, the existing literature also indicates married people have better health outcomes (Parker-Pope, 2010; Shmerling, 2016), and a higher rate of successful aging than those not married (Gopinath et al., 2018; Pruchno et al., 2010). A more nuanced comparison of the results of this study with the previous literature is hampered because there exist more than 100 different variations of the concept of ‘successful aging’ but no agreed-on standard for measuring it (Pruchno and Carr, 2017; Rowe and Kahn, 2015). Furthermore, little research on successful aging has been published in Canada (For notable exceptions please see Meng and D’Arcy, 2013; Tate et al., 2003). Research investigating the relationship between marital status and successful aging is rare. Future research is required to understand factors contributing to successful aging among older adults with various marital statuses and their implications on social policies and social work interventions.
Respondents who were married or became married between baseline and time 2 had higher age-sex adjusted odds of achieving successful aging, while respondents who became widowed, divorced or separated since baseline had lower age-sex adjusted odds of achieving successful aging. Those who were not socially isolated (i.e. those who got together with relatives, friends, or neighbors in the past month) had higher age-sex adjusted odds of achieving successful aging. Additional research is needed to help understand the reasons behind the observed associations and how social workers can support older adults who never married or who have experienced widowhood, separation, or divorce in later life.
Limitations
The findings of this study needed to be interpreted considering the following limitations: First, as has been discussed elsewhere (Ho et al., 2022, 2023), the construction of the successful aging status variable used in this secondary data analysis study relies on variables available in the CLSA data. Second, respondents are disproportionally very well-educated. Most of them have post-secondary education (79.5%), which may not reflect that 55% of Canadians aged 65 years and over have not received post-secondary education (Statistics Canada, 2017c). Third, we cannot determine if the changes of marital status occurred before or after a decline in successful aging, so findings must be interpreted with caution. Furthermore, the short span from baseline to time 2 (i.e. 3–4 years) may minimize changes in the trajectories of marital status used to explain successful aging. When more cohorts of data become available in the future, a longer span may reveal more about the association between the trajectories of marital status and successful aging for both men and women. Despite these limitations, the analyses of baseline and time 2 data of the CLSA capture valuable information on how people change over time and allow us to study what baseline factors may attenuate the relationship between marital status and successful aging, particularly trajectories of marital status from baseline to time 2.
Conclusion
Successful aging as a concept of aging well physically, psychologically, mentally, and socially is a ‘worldwide aim’ for older adults and social workers who have devoted their lives to the care of older adults (von Faber et al., 2001: 2694). This study found that the prevalence of successful aging was significantly higher among respondents who were continuously married, continuously widowed, continuously divorced or separated, or became married since baseline than in never-married respondents. Continuously married or newly married older adults had a higher rate of successful aging than their never-married, widowed, divorced, or separated counterparts. Older adults who experienced widowhood, divorce or separation in later life did not do as well as their counterparts. Social policies and social work interventions are needed to support older adults in connecting with others, and developing a social support network that may help them achieve successful aging in later life. Additional research is needed to illuminate the causal pathways between marital trajectories and successful aging, and to further clarify the implications of this research for gerontological social work practice. This study also found other significant baseline factors associated with successful aging and marital status. These included being younger, having a higher income, not being obese, engaging in moderate or strenuous sports, and not having sleeping problems, heart disease, or arthritis. These findings are crucial as many of these factors are modifiable lifestyle and health-related factors. For example, exercise programs and nutrition education can help people who are obese and encourage more people to exercise; sleep health education can support those who have sleeping problems; positive psychology education and cognitive behavioral therapy can help people to improve their outlook on life; heart health programs can help prevent and/or minimize the impact of cardiovascular disease, and exercise programs for arthritis can support people who have the condition. Social policies and social work interventions that are described above can be developed to support older adults, especially those who have experienced widowhood, divorce, or separation in later life. These programs can support older adults in connecting with others and developing a social support network that may help older adults achieve successful aging in later life.
Footnotes
Appendix 1
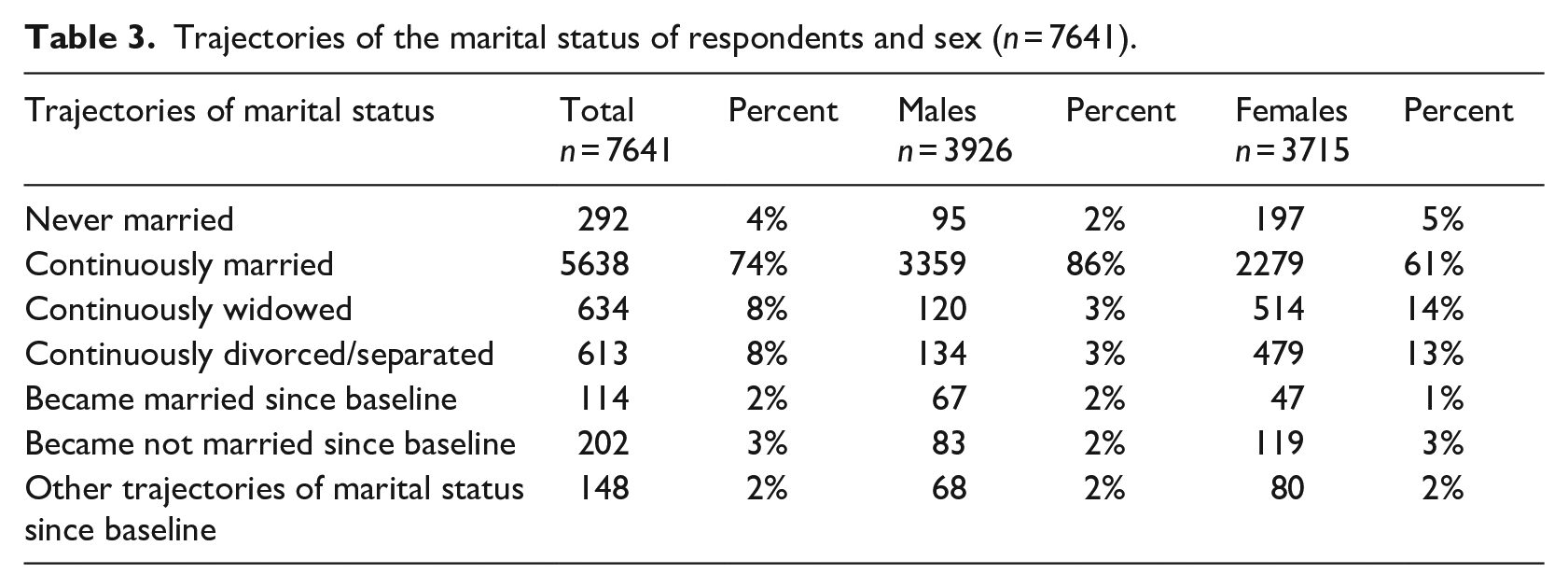
Trajectories of the marital status of respondents and sex (n = 7641).
| Trajectories of marital status | Total |
Percent | Males |
Percent | Females |
Percent |
|---|---|---|---|---|---|---|
| Never married | 292 | 4% | 95 | 2% | 197 | 5% |
| Continuously married | 5638 | 74% | 3359 | 86% | 2279 | 61% |
| Continuously widowed | 634 | 8% | 120 | 3% | 514 | 14% |
| Continuously divorced/separated | 613 | 8% | 134 | 3% | 479 | 13% |
| Became married since baseline | 114 | 2% | 67 | 2% | 47 | 1% |
| Became not married since baseline | 202 | 3% | 83 | 2% | 119 | 3% |
| Other trajectories of marital status since baseline | 148 | 2% | 68 | 2% | 80 | 2% |
Acknowledgements
This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding from the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. This research has been conducted using the CLSA Baseline Comprehensive Dataset version 4.1 and Follow up 1 Comprehensive Dataset version 3.0, under Application ID 1909014. The CLSA is led by Drs Parminder Raina, Christina Wolfson and Susan Kirkland. M.H., a doctoral student at the University of Toronto, was provided with the CLSA data for free through the CLSA trainee fee waiver. M.H. is deeply grateful to her thesis supervisor Dr E.F.-T. for her teaching, guidance, and support during the entire study, and is truly thankful to Dr D.B. and Dr E.P. for their help and support. M.H. would also like to thank Dr Karen Davidson and Dr Hongmei Tong for their guidance regarding the creation of the social support and social isolation variables. The opinions expressed in this manuscript are the authors’ own and do not reflect the views of the Canadian Longitudinal Study on Aging.
Author contributions
Conceptualization: M.H. and E.F.-T.; Data curation: M.H. and E.F.-T.; Formal analysis: M.H. and E.F.-T.; Investigation: M.H., E.P., D.B., and E.F.-T.; Methodology: M.H. and E.F.-T.; Project administration: M.H. and E.F.-T.; Resources: M.H., E.P., D.B., and E.F.-T.; Software: M.H. and E.F.-T.; Supervision: E.F.-T.; Validation: M.H., E.P., D.B., and E.F.-T.; Visualization: M.H. and E.F.-T.; Writing – original draft: M.H. and E.F.-T.; Writing – review & editing: M.H., E.P., D.B., and E.F.-T. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board statement
The study protocol of the CLSA has been approved by 13 research ethics boards across Canada. Details about the study are available at ![]() . The secondary analysis of CLSA data conducted in this paper was approved by the Health Sciences Research Ethics Board of the University of Toronto (protocol number: 38284 and date of approval: 12 October 2022).
. The secondary analysis of CLSA data conducted in this paper was approved by the Health Sciences Research Ethics Board of the University of Toronto (protocol number: 38284 and date of approval: 12 October 2022).
Informed consent statement
CLSA was responsible for obtaining consent from the respondents. Authors of this paper did not have access to identifiable information of the respondents.