
Abstract
In this article, we apply theories of non-citizenship assemblage to conceptualise the dynamic relationship of social determinants of health for international students in Canada who face barriers to accessing COVID-19 vaccines and verifying their vaccination status. Social workers’ roles in responding to and reducing these inequities are also discussed with attention to micro practice, meso service integration, and macro public policy advocacy. Through theorising assembled inequities emerging from Canada’s COVID-19 vaccination policies, this article offers guidance for future social work research and practice towards promoting justice and equity for transnational populations who are often excluded from domestic social welfare programmes.
Introduction
The population of international students has been increasing worldwide in recent decades, rising from an estimated 2.1 million in 2001 to 5.3 million in 2019 (Project Atlas, 2019). Canada, a popular study destination, had also admitted an increasing number of international students, from 225,295 in 2010 to 642,480 in 2019 (El-Assal, 2020). Before the pandemic, this population had already been experiencing inequitable access to social and health services, financial precarity and uncertainty regarding maintaining their immigration status post-graduation (Firang, 2020; Goldring et al., 2009). For example, international students are ineligible for publicly funded fellowships (e.g. Tri-Council Canada Graduate Scholarships; Government of Canada, 2021a). They are also required to pay for private health insurance (CIC News, 2014), which provides less access to medical services, is expensive and sometimes confusing to health care providers who are unaccustomed to billing outside of the public system. These structural barriers that international students experienced before the pandemic can be seen as a larger trend in Canada and similar immigrant-receiving nations around the world that excludes temporary and precarious immigrants. As Goldring et al. (2009) discuss, the intertwined effects of the global inequalities, domestic immigration, social welfare policies and individual agency lead many international students in Canada to live within the shadows of Canadian society. Maleku et al. (2021) also call this group a ‘hidden minority’ whose concerns are either ignored or considered private concerns.
Disruptions in international travel and migration since the onset of the COVID-19 pandemic further negatively impacted international students’ well-being. For instance, due to the closed borders, students were unable to return home and, in some cases, sequestered as the only people on campuses that were closed to prevent the spread of COVID-19 (Firang, 2020). Among these dilemmas, the urgent one emerging from the pandemic is international students’ unequal access to COVID-19 vaccines and proof of vaccination amid the COVID-19 vaccination plan in Canada that started in late 2020 (e.g. Ontario, Government of Ontario, 2021b).
To better understand how precarious immigration contributes to inequities in COVID-19 vaccination faced by international students, we develop a dynamic analysis of social determinants of health (SDH) using non-citizen assemblage theories in this conceptual paper. The framework of SDH is well-established for public health policy and research in Canada, as it uncovers various intertwined factors from both society and vulnerable populations that profoundly shape their health outcomes (Hynie, 2018). However, it has been critiqued as producing static and ambiguous constructions of the ‘social’ without attention to dynamic power relations. Towards expanding the analysis of the SDH framework, we draw upon theories of non-citizenship assemblage to illustrate how multiple factors that stem from macro-social contexts, micro individual conditions and migrant agency jointly shape structural inequities (Goldring and Landolt, 2013) faced by international students in Canada’s COVID-19 vaccination policies.
We further consider these inequalities as embedded in the Canadian immigration system that shapes immigrants’ and migrants’ health and well-being, as well as social work practice with immigrants. Particularly, social work scholars have previously called attention to the limited information that social workers receive during their training (Yan and Chan, 2010), a situation that results in social workers feeling less prepared to work with immigrants who are not citizens or denying that immigrants face additional systemic barriers as compared to their citizen counterparts (Park et al., 2021). This article contributes to the currently limited but emerging research in social work on the health and well-being of international students, including the role their temporary immigration status plays in accessing health and social services.
In this conceptual paper, we first present an overview of the context of the COVID-19 pandemic and related public health requirements for international students in Canada. We then discuss how the process of vaccine distribution and requirements for documenting vaccination status have further marginalised international students living in Canada or arriving from abroad with vaccinations that are not officially recognised by the Canadian government. After providing an overview of existing knowledge of SDH with emerging theories of non-citizenship assemblage, we present an integrated framework to explore how social workers should consider the dynamic social systems associated with immigration status and adjust micro practice, meso service integration and macro policy to improve health and well-being of international students and the larger population of immigrants.
Policy context: International students’ access to COVID-19 vaccines in Ontario
Despite the Canadian government’s early investment in COVID-19 vaccines at the beginning of the pandemic (e.g. signing contracts with Western pharmaceutical companies), the public experienced difficulties accessing COVID-19 vaccines due to shipping issues and a lack of domestic manufacturing capability (MacCharles, 2021; Walsh and Gray, 2020). After a slow start, vaccines became more widely available, and the federal and provincial governments (e.g. Ontario) first prioritised the distribution to people working in health care and long-term care facilities, and vulnerable populations such as Indigenous populations (Government of Ontario, 2021b). By July 2021, all remaining people were eligible for at least one form of COVID-19 vaccine (Government of Ontario, 2021b), though access to the vaccine continued to be a challenge due to high demand.
Although the Ontario government authorised universal access to health care for anyone with COVID-19-related symptoms from the start of the pandemic, irrespective of immigration or insurance status (e.g. international students; Gagnon et al., 2021), access to the COVID-19 vaccines for people who did not have an Ontario Health Insurance Plan (OHIP; Ontario’s version of Medicare) was at first unclear, despite consistent advocacy among activists to remove this barrier (e.g. Jones, 2021). Even though the federal government ultimately issued statements that migrant workers and international students would be eligible for COVID-19 vaccines (Thevenot and Miekus, 2021), there was no specific information about when and how these populations were able to get vaccinated. While the provincial public health system allowed people who had an OHIP to book vaccine appointments online or by phone (Tunney and Kapelos, 2021), this system offered no options for people who were uninsured or who had private insurance, including international students attending a university in Ontario. Provinces across Canada (e.g. Ontario) later offered mobile clinics to deliver vaccines promptly and serve marginalised communities (i.e. communities with high concentrations of low-income workers who cannot take time away from work) (Newport, 2021), as well as enable people to access vaccines without a provincial health card and appointments (FCJ Refugee Centre, 2021). However, information regarding these mobile clinics remained largely unclear and hard to access, such as when and where these mobile clinics would be. It is noted that some social media (e.g. Vaccine Hunters on Twitter) have been playing an increasingly important role in disseminating messages regarding vaccines to the public (Treble, 2021), yet the large population of migrants with precarious status (e.g. international students, refugees) may not be able to receive these messages, due to various reasons such as their unfamiliarity with the local context, limited social connection, and language barriers (Edmonds and Flahault, 2021; Gagnon et al., 2021).
Even after the vaccine supply became abundant, relevant information regarding how international students can access the vaccines remained unclear or difficult to access. Educational institutions play a role in sharing relevant information and guiding students in this process; however, as the federal and provincial public health authorities are the ultimate policymakers, and relevant policies were not fundamentally clarified from their end, educational institutions, thus, cannot provide information that directly solves international students’ concerns, but instead promulgates existing policies that are inadequate in addressing inequities.
Exclusionary policies for verifying vaccination status
As the vaccination rate gradually increased and the economy rebounded in Canada (Olive, 2021), policies regarding proof of vaccination emerged as a strategy to enable economic activities to resume while maintaining public safety (e.g. Government of Ontario, 2021a). Particularly, when accessing non-essential businesses (e.g. restaurants), individuals were required to show proof of full vaccination (DeClerq, 2021). Similar to the online system set up for people to schedule a vaccination appointment in the provincial health care system, the online system created to verify proof of vaccination did not include options for people who do not have an OHIP, including international students (Government of Ontario, n.d.). Even though some temporary solutions had been put forward, for example, migrants without health cards can call the local public health agency to get the temporary code to log into the system (Government of Ontario, n.d.), these alternative measures required significant time and knowledge of how to navigate the complex public health care system amid the pandemic, especially when many workers continued to work remotely. In addition, these calls had led to long wait times and been transferred between different extensions with many staff who were unfamiliar with the procedures or who had no support when working with someone with limited English/French language.
Epistemic bias from the accreditation of non-Western COVID-19 vaccines
Another major challenge for international students in Canada is the accreditation of non-Western COVID-19 vaccines. Initially, Health Canada only accepted limited types of COVID-19 vaccines (e.g. Pfizer, Moderna) developed by Western countries (MacCharles, 2021), and travellers with one of the approved vaccines were exempted from quarantine measures upon arrival (Chase and Walsh, 2021), even though other COVID-19 vaccines (e.g. Sinopharm) produced by non-Western countries were also recommended by the World Health Organization (2021). Privileging vaccines produced in Western countries reinforced Canada’s epistemic bias towards Western knowledge production and economic interests, in ways that structurally disadvantaged the vast majority of international students who originate in the Global South (particularly China and India) (Büyüm et al., 2020). It also exacerbated the colonised links between systemic racism and cultural racism in the global economy and Canada’s domestic policies that perpetuate Western hegemonic power (Best, 2021).
When Canadian border restrictions were relaxed in late October 2020, international students were allowed to enter Canada again (Thevenot, 2020), yet they were still in limbo, even though some of them might be vaccinated with non-Western vaccines. As these vaccines are not recognised by the Canadian government, international students still needed to comply with quarantine measures, and further face difficulties in accessing recognised COVID-19 vaccines, being qualified as fully vaccinated as well as obtaining proof of full vaccination. Although Canada issued a guideline to further vaccinate individuals with unrecognised vaccines (e.g. Government of Canada, 2022), there was still limited information regarding how they can be reconsidered as being fully vaccinated in Canada, and whether and how they can get proof of full vaccination. This dilemma may further impose restrictions on their life in Canada (e.g. they cannot take public transport such as planes; Government of Canada, 2021c) and affect their settlement in this new country. Moreover, even though the Canadian government has announced that some vaccines (e.g. Sinopharm) produced by China and India will be accepted after 30 November 2021 (Government of Canada, 2021b), how those students who enter Canada with these newly accepted vaccines can obtain proof of vaccination is also not clear, and there are still vaccines produced by other countries that are not accepted.
These abovementioned situations illustrate how international students are marginalised by the Canadian healthcare system at this critical time, and further accentuate the urgent need to tackle these inequities and promote justice for international students.
Approaches to social determinants of immigrant health in Canada
These inequities regarding COVID-19 vaccination that international students in Canada are faced with can be analysed through the theoretical framework of SDH. This framework accentuates how health outcomes result from the macro-social context, which can thus connect with the current pandemic, and further help us understand unprecedented damage caused by COVID-19 to public health and vulnerable populations’ health equity (Turner-Musa et al., 2020). For instance, Burström and Tao (2020) used this framework to briefly analyse how social groups with low socioeconomic status are in an adverse situation due to various factors such as housing and pre-existing health issues. Singu et al. (2020) also analysed how vulnerable populations, particularly those with preexisting health issues, are profoundly affected by the pandemic through interrelated social determinants such as community contexts and education. The SDH framework has been mainstreamed in Canada and is used extensively to address issues related to structural racism. For example, Greenwood and de Leeuw (2012) analysed how Indigenous children’s health equity and well-being can be continuously improved by considering different determinants (e.g. loss of their culture due to colonisation). Abdillahi and Shaw (2020) analysed how structural racism that Black Canadians experience also leads to their unequal health outcomes, and some social determinants such as education (e.g. unable to complete high school) and housing (e.g. poor living conditions) profoundly impact this process. Even though SDH identify important social entities as impacting health disparities beyond biomedical factors, post-positivist ontological assumptions of social determinants related to social context and individual backgrounds are often presented as fixed entities, thereby overlooking the dynamic, changing and heterogeneous relationship between health equity, individual behaviours and social context (Golden and Wendel, 2020).
Introducing non-citizenship assemblage as an SDH
We draw upon the concept of non-citizenship assemblage to further our understanding of international students’ health disparities amid the pandemic using a dynamic lens. Migration scholars have turned to assemblage theory, as developed by Deleuze and Guattari (Buchanan, 2015), to explore how precarious immigration status contributes to prolonged periods of social and economic insecurity through interconnected structural factors, individual factors as well as migrant agency (Goldring and Landolt, 2013; Landolt and Goldring, 2015; Villegas, 2015). Particularly, structural factors are illustrations of the hegemonic power of the nation-state in regulating immigrants and migrants to align with its national demands and interests, and normally include immigration policies, public health policies and so forth (Landolt and Goldring, 2015; Wimmer and Schiller, 2003). Immigrants and migrants are monitored and can only navigate host countries within the scope specified by these policies. Individual factors refer to immigrants’ and migrants’ personal backgrounds including their language ability and social connections (Goldring and Landolt, 2022). These factors affect their perceptions of host countries and actions taken accordingly, and further determine the scope of their activities in host countries. Migrant agency shapes how immigrants and migrants dynamically navigate host countries through the influence of both institutional and individual factors (Landolt, 2022; Landolt and Goldring, 2015). For instance, as migrants navigate immigration requirements, their status shapes access to education, housing and so on; they form and rely upon different social networks to receive relevant information that they need, such that these social connections affect their ability to further act on such information. Migrant agency, however, operates in relation to the conditions placed on migrants’ eligibility for a range of social, economic and political rights (Goldring and Landolt, 2013). For instance, international students must maintain their status by remaining full-time students in good standing. Any lapse in their status as students (including poor marks) can jeopardise their right to remain in Canada. International students who wish to remain in Canada after graduation face an additional set of bureaucratic requirements that require them to demonstrate their worthiness through employment in a desirable occupation that would confer eligibility for permanent residence. The transition from a study permit to permanent residency thus depends on employment, health, the absence of a criminal record and financial assets. These situations show how individuals with precarious status are being monitored by the nation-state, as the nation-state makes it clear how immigrants and migrants can be recognised as being deserving to stay. Individuals may internalise this deservingness and either fight for their equal access to social and public services with the support from their social networks (e.g. migrant caregivers’ long-standing call for ‘status on arrival’; Bhuyan et al., 2018) or understand their exclusion as justified as a result of inadequate help or misinformation from their social connections (Landolt, 2019). Focusing on migrants’ unequal access to the public health system, Landolt (2019) elaborated on the above discussion through a framework that includes national law and policies, individuals’ membership under national sovereignty, various social network actors and migrants’ agency. Through this integrative framework, Landolt (2019) depicted the complex and dynamic effects of both contexts and individuals on jointly assembling migrants’ precarious non-citizenship status as well as reshaping the consequent barriers when accessing the Canadian healthcare system. Overall, Landolt (2019) illustrated the innovative role of non-citizenship assemblage in understanding precarious migrants’ lived experiences in the context of healthcare, which is an important discussion yet one which still has not obtained enough attention. This article adopts this framework to further understand international students’ barriers to COVID vaccination policies in Canada, a framework which reflects instant and influential changes in current public health policies related to COVID-19 and their consequences.
Applying a dynamic assemblage lens to understand SDH
Even though understanding social determinants that affect migrants’ vaccination at this challenging time is crucial, relevant studies are still extremely limited. One timely systematic review identified several determinants that affect migrants’ access to (e.g. literacy, legal barriers) and acceptance of (e.g. refugee status) vaccines such as the COVID-19 vaccines (Crawshaw et al., 2022). SDH primarily focuses on various determinants that shape migrants’ unequal health outcomes (Preda and Voigt, 2015). However, dynamic changes in these factors are not further considered and their dynamic interrelations and joint effects are also under-theorised. These issues are the major limitation of SDH that needs to be addressed particularly at this critical time, since there have been rapid changes in basically all levels of policies and relevant practice during the pandemic, such as border rules and vaccination documents. The public, including precarious migrants, need time to be aware and adjust to new policies, and those in supportive roles (e.g. social service providers) also need to quickly apprehend these dynamic changes and implement them accordingly. In response to these urgent situations, theories of non-citizenship assemblage can shed light on the dynamic landscape of Canada’s COVID-19 vaccination inequities, particularly within the population of international students.
Through the lens of non-citizenship assemblage, we consider how international students’ precarity with regard to COVID-19 vaccination is produced through the intertwined effects of the nation-state (e.g. the need to regulate immigration/migration in the nation-building process), sub-national institutional factors (e.g. document requirements of higher education and public health), and individual factors (e.g. migrants’ language ability and financial situation), as well as their complicated interrelationships. For instance, as the way of regulating temporary international students, Canadian policies and laws of international higher education and immigration reflect the dominant power of the nation-state in managing international students to align with the nation’s interests and demands (e.g. profitable knowledge economy; potential immigrant source), and thus distinguish this population from those with complete citizenship who are also entitled to social services and legal rights (Johnstone and Lee, 2014). This situation further indicates unequal access to the healthcare system between international students and others. However, the pandemic accentuated the urgent need to protect all individuals’ health. It disrupted the nation-state’s abovementioned strategies in managing immigrants and migrants, and exposed the limitations of regulating temporary residents based on the visa restrictions, especially when issues about access to vaccines and proof of vaccination abruptly emerged, and there were no existing strategies to promptly deal with this situation. Moreover, not recognising non-Western COVID-19 vaccines further showed the dominant power of the Canadian nation-state in monopolising the healthcare system, as these vaccines challenge the dominant role of Western nation-states in managing immigration and migration from other countries through healthcare services. Hence, not recognising non-Western vaccines can be a symbol to understand how Western nation-states have formed a hegemonic hierarchy in which immigrants and migrants from non-Western cultures are on the periphery (Landolt, 2019; Wimmer and Schiller, 2003).
Even though the Canada Health Act that previously excluded migrants from accessing the Canadian healthcare system was expanded to migrants during the pandemic (e.g. free healthcare related to critical conditions caused by COVID-19) (Gagnon et al., 2021) to respect the basic human right of physical health, how vaccination should be rolled out for them was not explained clearly in Canadian public health policies; this lack of clarity in public health policies (e.g. where and how to get the vaccines) at the beginning of vaccination in Canada could be a major institutional factor that barred international students from accessing COVID-19 vaccines and proof of vaccination. Factors on the individual level can further exacerbate the situation. For example, international students’ language barriers can prevent them from accurately accessing and understanding vaccination information, and lack of social support or connection (e.g. no one guides them to relevant resources) also imposes another barrier on them during this process. If international students further compromise and accept the inaccessibility of vaccines and proof of vaccination as the result of their temporary legal status, then this type of migrant agency in assemblage may further intertwine with the abovementioned institutional and individual factors, and eventually, marginalise them in terms of COVID-19 vaccination. Hence, their precarious status in COVID-19 vaccination can be viewed as a process of assemblage in which different factors exert intertwined influences. It is also a dynamic process such that any changes in these factors and their interrelations can result in different outcomes (Landolt and Goldring, 2015). SDH further show the health impact of COVID-19 in this assemblage. It illuminates how inequities in vaccination are not just behavioural and cultural, but rather a structural issue that reflects the dominant role of the nation-state in immigration and migration (Castañeda et al., 2015), as well as in healthcare policies (Landolt, 2019). Specifically, factors mentioned above such as restrictive immigration policies, unclear public health policies and insufficient social support for international students can be possible social determinants that deeply structure inequities in vaccination.
Discussion
The above discussion about SDH and non-citizenship assemblage can further inform positive changes in practice and provide new insights for social workers to better work with international students and combat these inequities in COVID-19 vaccination. We propose a conceptual model (Figure 1) that reflects this dynamic assemblage of understanding SDH that sets up barriers for international students in terms of COVID-19 vaccination and tackling these inequities through social workers’ integrated participation with international students. This framework includes micro, meso and macro practice levels, as previous literature has shown that integrated efforts on these levels can optimise the delivery of social work services and improve their quality (e.g. Zhao et al., 2022a, 2022b).
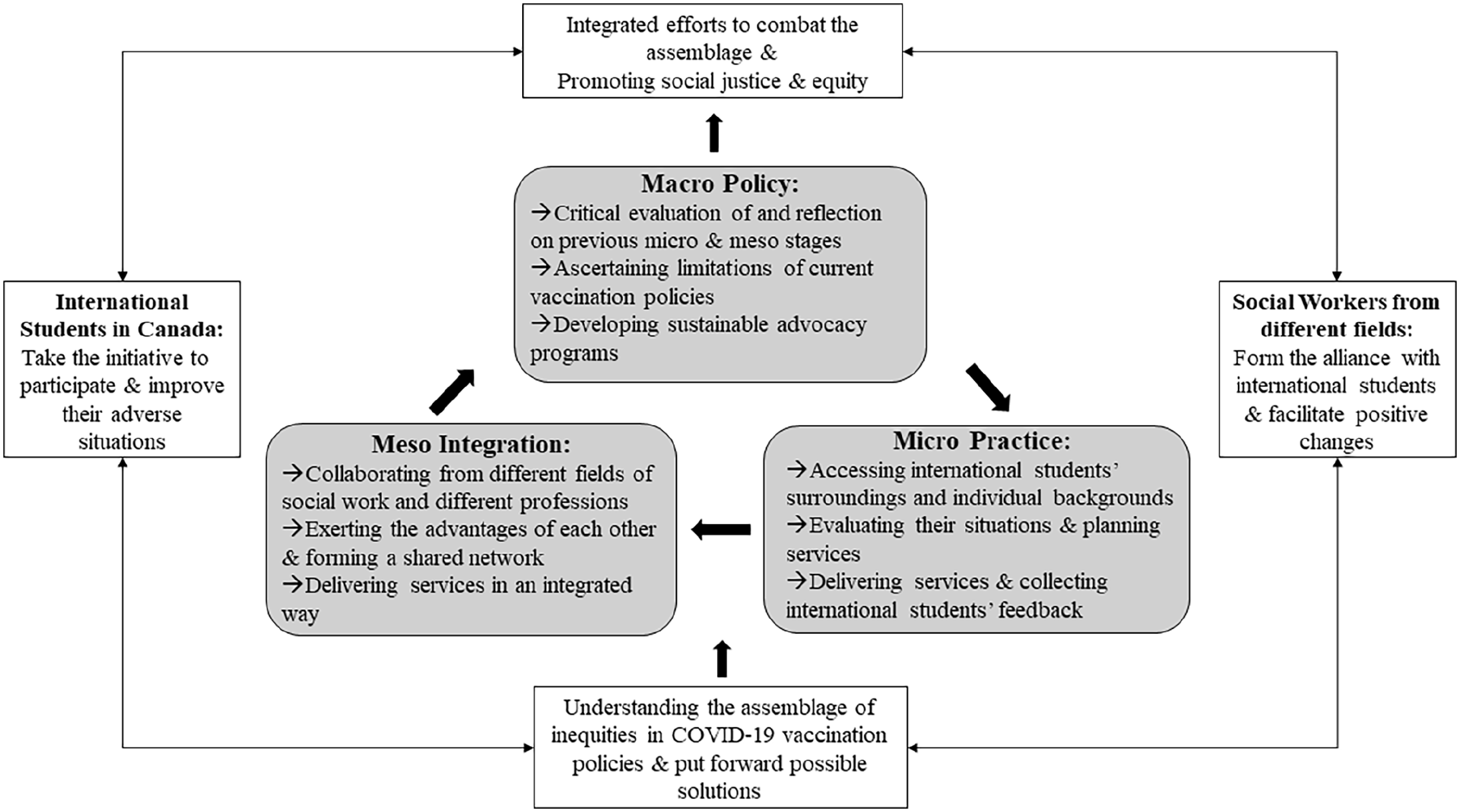
A conceptual model to tackle structural inequities in COVID-19 vaccination policies.
The micro-interactions between social workers and international students are the foundation, as this step aims to build a rapport and provide more outreach efforts towards international students. Particularly, this level can involve different sequential stages. The first stage is for social workers to familiarise themselves with international students. Specifically, social workers need to take international students’ various cultural and individual characteristics into consideration to better understand inequities that they face; social workers should also consider the effects of international students’ surroundings (e.g. communities that they are in) on further shaping these inequities. There should also be more outreach efforts in settings that are closely related to international students such as their communities, their educational institutions and social media through their native languages, so that international students can get better informed and further access these services. This stage shows the need to ally with this migrant group to understand their struggles caused by intertwined and complicated institutional and individual factors (Firang, 2020). The second stage is to evaluate international students’ circumstances, in which social workers review the assemblage of international students’ inequities in vaccination policies by considering social determinants that exert influence. During their interactions with international students, social workers need to carefully assess international students’ various situations in vaccination, so that proper resources and suggestions can be further directed to them. Social workers also need to contemplate how to adapt cultural sensitivity and diversity into their design and conduct of interventions on different levels (Fernández-Borrero et al., 2016), as unique epistemological stances from different cultures can significantly impact the implementation of social work services (Zhao et al., 2021). The third stage can be providing services and collecting feedback, as social workers can deliver information or services that international students need (e.g. where to get the vaccine), and obtain their feedback to further optimise services. Their feedback and suggestions as service participants can further inform the improvements of this micro-level service (Nápoles and Stewart, 2018). This level of practice should be client-centred and implemented with close participation of international students, as previous literature has shown that the engagement of clients can significantly improve implementation and outcomes of services (Tsang, 2013; Zhao et al., 2022b).
In terms of the meso service integration, it should be a dynamic process whereby social workers in different areas such as settlement services, healthcare services and community engagement can form shared networks to better assess and work to address the needs of international students. For example, frontline social workers specialising in settlement and immigration services can be expected to better understand migrant students’ situations, and further guide them to deal with challenges arising from the pandemic. In terms of vaccination, these social workers can further cooperate with their colleagues who have expertise in social and public health policy, as they can provide information on how extant public health policy regarding vaccination can help international students with their struggles. Social workers with clinical and health backgrounds can further participate in this cooperation and connect with medical doctors to give suggestions to migrant students regarding vaccines.
Building upon experiences and feedback from the previous two stages, macro policy advocacy and reform provide a larger platform for social workers to advocate for international students during the pandemic to the policymakers as well as the public, and further design potential advocacy programmes to improve international students’ situations. This level can also involve three different stages. First, social workers need to critically evaluate their interactions with international students and existing integrated resources to find whether there are limitations on these two levels that are inadequate in addressing international students’ issues regarding vaccines, proof of vaccination and accreditation of non-Western vaccines. This stage can be the foundation for further policy advocacy and reform, as it enables social workers to discover potential improvements in current public health policies (Cummins et al., 2011). Second, social workers from different specialisations can discuss these limitations by bringing in their expertise, so that what can inform positive changes in current policies can be better assessed in an integrative manner, and pave the way for the following policy reform. Third, international students’ engagement is also crucial in this process. Discovering how public health policies can reflect international students’ benefits and further protect them during this difficult time requires their involvement. Specifically, international students can participate throughout the process by giving their suggestions or feedback based on their experiences as well as their insights on how the policies should be better deployed and implemented.
Hence, these three levels are interconnected and require concrete efforts from the social work profession to tackle structural inequities assembled in society during the COVID-19 vaccination. This conceptual model can be a timely response to structural barriers emerging from the current healthcare system during the pandemic and can be a starting point to explore how social workers can reduce these structural inequities from different aspects. This model contributes to the current discussion on how the Canadian healthcare system can be more inclusive to marginalised groups such as international students during this difficult time. Approaching health inequities through dynamic theories of assemblage can also invite social workers to develop interventions at multiple scales, to better address and reduce structural inequities in the healthcare system, towards promoting social justice and equity. This comprehensive model can also guide social workers in other countries to work with migrant students who might also face similar situations in COVID-19 vaccination policies. Building upon this conceptual analysis, social workers worldwide can further examine their own contexts and come up with research and practice ideas to constantly test this model.
This model, however, has some limitations that require future investigation. First, there should be more theoretical and empirical elaboration on the potential for collaboration among social workers with different specialisations and migrant students from different backgrounds, to work together to enrich the content of this model. Social workers also need to consider ethical concerns when working with international students. For example, as international students may fear losing their precarious status through participating in policy advocacy (e.g. activism), confidentiality thus needs to be maintained with their consent. As social work researchers and practitioners need to critically evaluate the application of this model to complex real-life situations through their judgement and creativity (Bogo, 2018), the model can be further developed with new insights into the dynamic processes and components that shape non-citizenship assemblage in various contexts. Second, how experiences from this model can inform planning in anticipation of future similar public health and environmental crises, take care of marginalised groups in a sustainable manner and constantly promote social equity in the healthcare system needs more investigation from social work researchers and practitioners.
Overall, this conceptual model provides a good start for understanding how social workers, not just in Canada but also in other countries, can undertake different roles and form an integrated force on different levels to combat structural inequities assembled in vaccination policies. It helps us understand intertwined determinants that shape international students’ unequal health outcomes in vaccination. It also emphasises the client-centred perspective to understand how the assemblage of international students’ precarious non-citizenship exacerbates structural inequities in vaccination policies. Integrated efforts of social workers shown from the framework not only contribute to the extant literature on social equity and COVID-19, but also can be the solid foundation for future research and practice in promoting more inclusive healthcare services.
Conclusion
The COVID-19 pandemic exposed structural inequities in healthcare systems in Canada and worldwide, specifically for transnational populations who are often overlooked by domestic public health and social welfare programmes. Through developing a dynamic lens to consider assemblages of SDH, this article sheds light on structural inequities that unfolded through Canadian COVID-19 vaccination policies and how they marginalise international students. Considering the centrality of ecological models in social work which encompass many levels of practice, social workers can play a significant role in identifying inequities faced by international students in public health guidelines, access to health services and advocacy to promote social equity which are heightened in times of crisis (Cummins et al., 2011). While the conceptual model focuses on the context of Canada’s COVID-19 vaccination policies, this framework could inform response to subsequent public health emergencies and their ever-changing effects on vulnerable populations worldwide. With the ongoing rise of transnational migration, further research is needed to understand the pressing concerns and long-lasting effects of structural inequities that international students and other migrants with precarious legal statuses face in the countries where they reside, especially as the COVID-19 pandemic remains an evolving situation with emerging uncertainties that may require future vaccination and related public health measures.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.