
Abstract
COVID-19 stretched health systems, exacerbated by concerns about those that are corrupt and lack equity. Twelve (12) health workers and 12 hospital social workers across Nigeria were purposively sampled and virtually interviewed to explore unaccountability and corruption effects on COVID-19 responses. Findings show that corruption and unaccountability negatively affected responses of frontline health workers to the pandemic. Lack of social care and justice services for patients and health workers across health facilities in Nigeria worsened the negative effects. Effectively mainstreaming social care and justice services into Nigeria’s healthcare led by well-trained social workers will improve the health sector via anticorruption.
Keywords
Introduction
A just healthcare system is that which is free from corruption and unaccountability (Dadwal, 2020). It offers a fair share of health resources across health service providers and users and places their welfare at the heart of the health system (Azevedo, 2017). Corruption and unaccountability are major obstacles constraining the achievement of a just healthcare system. These issues have been rife in Nigeria’s health sector, with effects on frontline efforts in containing COVID-19 (Onwujekwe et al., 2019, 2020a).
Existing health sector anticorruption efforts in Nigeria have reportedly appeared weak, selective and unjust (Ezeibe et al., 2020; Onwujekwe and Agwu, 2020). However, social workers who are trained to be the face of social justice and challenge activities that go against human rights and freedom are faced with an identity crisis in Nigeria’s health sector (Amadasun, 2020b). Identity crisis in this context means that the profession within Nigeria’s healthcare is considered nebulous by a vast majority, and not backed by an act of law as a profession (Okoye, 2019; Okoye and Agwu, 2019).
During pandemics, the fragility of most health systems is exposed, which is often severe for health systems that are notorious for corruption and unaccountability (Rhodes, 2020). This scenario was manifest in the outbreak of COVID-19 which devastating emergence could be traced to Wuhan, China, in December 2019, and February 2020 in Lagos, Nigeria (Ebenso and Otu, 2020; Steingruber et al., 2020). Since then, cases and fatalities have continued to rise and were at a time overwhelming for health systems across the globe, including that of Nigeria (Human Rights Watch, 2020; Worldometer, 2020).
At the onset of the fast-spreading virus, some important questions begging for answers were on the state of the structural and organizational preparedness of Nigeria’s health system (Ebenso and Otu, 2020; Odubanjo, 2020). A major possible constraint for answers to these questions is the effect of corruption and unaccountability for which Nigeria is notable, ranking 149th of 179 across the globe (Transparency International, 2021). Notably, there is a consensus among Nigerian health workers that health sector corruption mars their efforts, which is discouraging, and has forced many health practitioners out of Nigeria’s health system (Eze et al., 2021; Onwujekwe et al., 2020b). This implies that achieving a just and corruption-free healthcare system is a priority, and vital to pandemic preparedness and responses.
Corruption is endemic in Nigeria and most of Africa, and it is described as the use of publicly entrusted powers for private gains (Onwujekwe et al., 2018; Transparency International, 2020). It is similar to unaccountability, which in this context entails the inability to show stewardship or irresponsibility towards the utilization of public resources. Different types and drivers of corruption existing in the health sector of Nigeria have been identified to include absenteeism, informal payments, procurement-related corruption, employment-related corruption, health financing corruption and so on (Onwujekwe et al., 2020b). These types of corruption are driven by factors that are embedded in the governance structure of the country and its health system, as well as in the behaviours of health workers and managers (Balabanova et al., 2020; Onwujekwe et al., 2020b).
To contain COVID-19, strategies adopted by Nigeria were focused on lockdowns, contact-tracing, testing, treatment, social distancing and the use of face coverings and hand sanitizers. There was a Presidential Taskforce (PTF), currently identified as the Presidential Steering Committee (PSC), at the centre of driving these strategies, which comprised, among others, the Minister of Health, Minister of Social Development/Humanitarian Affairs and the Director General of the Nigeria Centre for Disease Control (Ezeibe et al., 2020). Resources were donated to the national and sub-national governments, and an about 13% increase was made to the health budget. As tracked and documented in Onwujekwe and Agwu (2020), about 150b naira (£275m) were raised in monetary and non-monetary terms to combat COVID-19 in Nigeria. While this should be appreciated as relatively adequate, there is popular opinion that the pandemic enriched a few Nigerians, as mobilized resources barely translated into improved conditions of health workers and their facilities, nor the provision of sufficient and reasonable palliatives to cushion lockdown effects (Eze et al., 2021; Ezeibe et al., 2020; Onwujekwe and Agwu, 2020). In a more recent event, the PTF was unable to provide a detailed breakdown of expenditures on COVID-19 (Ojekunle, 2021), and its resource-tracking website (http://ngcovid19resourcetracker.info/) only functioned for a little while. These are suggestive of a lack of transparency, which implies corruption and unaccountability.
Across literature, there are accounts of corruption and unaccountability during the peak periods of COVID-19 in Nigeria. Some of which include funding irregularities (Onwujekwe et al., 2020b), which affected the procurement of medical equipment and the remuneration/incentivization of health workers (Adebowale, 2020; allAfrica, 2020; Ewubare, 2020); massive price increases (arbitrary inflation) of personal protective equipment (PPE) and theft of PPE from facilities to be sold on the private market for higher prices (Balabanova et al., 2020; Rhodes, 2020); hoarding of palliatives and embezzlement of donated resources (Agwu et al., 2020a; Eze et al., 2021), among others. There are suggestions that these discouraging events have affected the overall management of COVID-19 in Nigeria and inspired a loss of confidence in the country’s health system. Consequently, citizens told lies about their health status even with obvious symptoms of the virus, hid their travel histories and disregarded safety protocols that were rolled out by the government (Agwu et al., 2020a; Ogunsemore, 2020; Onyishi et al., 2020).
Although social workers are important stakeholders in anticorruption, their presence in Nigeria’s health system is yet to be optimal, as they are sparingly employed, usually at the tertiary healthcare level. The recognition of the social justice and advocacy training of social workers indicates that they have a history of challenging corruption at different levels of governance (Moyo, 2018; Wamara, 2017).
While there is the dearth of clear-cut social work-anticorruption literature in the health sector, some Nigerian studies have shown the performance of social workers in ensuring that public health systems are improved by advocating for, as well as upholding right conduct (Agwu and Okoye, 2021; Onalu et al., 2020, 2021). They achieve some of these feats through education on rights, speaking on behalf of patients, helping the indigent to sort their bills, dialoguing with authorities, red-flagging inimical behaviours, to mention but a few. Unfortunately, the intensity and effects of such efforts have not been far-reaching owing to their professionalization status which is yet to be backed by an act of law in Nigeria. Therefore, with the social justice focus of the profession of social work, we are of the view that they will be key to anticorruption, and can hold health institutions accountable (Lewis, 2015; Teater, 2010). Their contributions would go a long way to strengthen health systems and galvanize effective responses during public health emergencies.
This article contributes new knowledge by first revealing several issues of corruption and unaccountability that affected the efforts of frontline health workers in containing COVID-19, and the challenges they faced while confronting such issues. The study also determines the relevance of social work in the context of health sector anticorruption and highlights the challenges and prospects of the profession within pandemic responses in Nigeria.
Methods
Study site and sampling procedure
Non-probability sampling techniques (purposive and snowballing) were used in the study to target 24 respondents comprising 12 frontline health workers and 12 social workers. They were purposively sampled from our networks on the ground in that they were considered well-experienced to provide the information we sought. Some hospital social workers that were not necessarily at the frontline but had good information to share were also interviewed. There were a few cases of referrals of respondents (snowballing), especially when a potential respondent was not available or felt that there was the need to engage a more knowledgeable person. The 12 health workers were all at the frontline (tertiary and secondary health facilities), drawn from Lagos, Abuja, Abia and Enugu. The 12 social workers also worked in tertiary and secondary health facilities, and were drawn from the Federal Capital Territory (Abuja), Ebonyi state, Edo state and Enugu state. The respondents were willing to share information over the phone.
Data collection
For 1 month, telephone interviews were conducted with the respondents. This strategy of virtual communication was necessary, owing to physical distancing protocols and lockdown. Verbal consent was sought as approved by the Research Ethics Committee. The reason for verbal consent is that we adopted telephone interviews. However, participants only consented on the premise that they were promised anonymity, which we accepted.
The interviews usually took more than an hour, and in some cases, could happen over 2 days and more, depending on the availability of the respondent, and if he or she had new information for us. Our interviews focused on issues of corruption and accountability in their facilities and across national and sub-national healthcare management. We also considered how such issues affected service delivery, and the roles of social workers as social justice professionals. We recorded the interviews using the call-recording feature available on android phones, and extensive notes were taken. All interview notes were saved in a diary over the study period. The conversations were in the English language, and timing depended on the availability and convenience of the respondents. We ensured that we had earlier communicated with the respondents for consent approval and choice of time so that our research activity does not interfere with their primary responsibilities.
Data analysis
After transcription of the recorded conversations, alongside making comparisons with the notes, themes were manually generated by carefully studying the transcripts for the generation of codes and sub-codes, in line with inductive deducting. Also, following a deductive approach and to achieve coherence, the codes and sub-codes were compared against the research questions and objectives of this particular study. A Microsoft Excel spreadsheet was designed, with codes (themes) and sub-codes (subthemes) aligned to columns, and details of each respondent in the top rows. Quotes were then placed appropriately in boxes that represent each theme or subtheme. Afterwards, the researchers and some peers took time to read through the analysis spreadsheet in line with observer triangulation and peer debriefing (Padgett, 2008). Suggestions were made for re-ordering of the quotes or deletion where applicable and merging of themes and subthemes as well. Overall, thematic analysis helps to achieve a proper organization of respondents’ insights into categories that will address the objectives of the study (Babbie, 2010). Our final themes as presented here included (a) specific instances of health sector corruption and unaccountability and influence on frontline operations, (b) challenges of health workers in confronting corruption and unaccountability, (c) relevance of social workers to anticorruption within healthcare settings.
Results
Demographic description of respondents
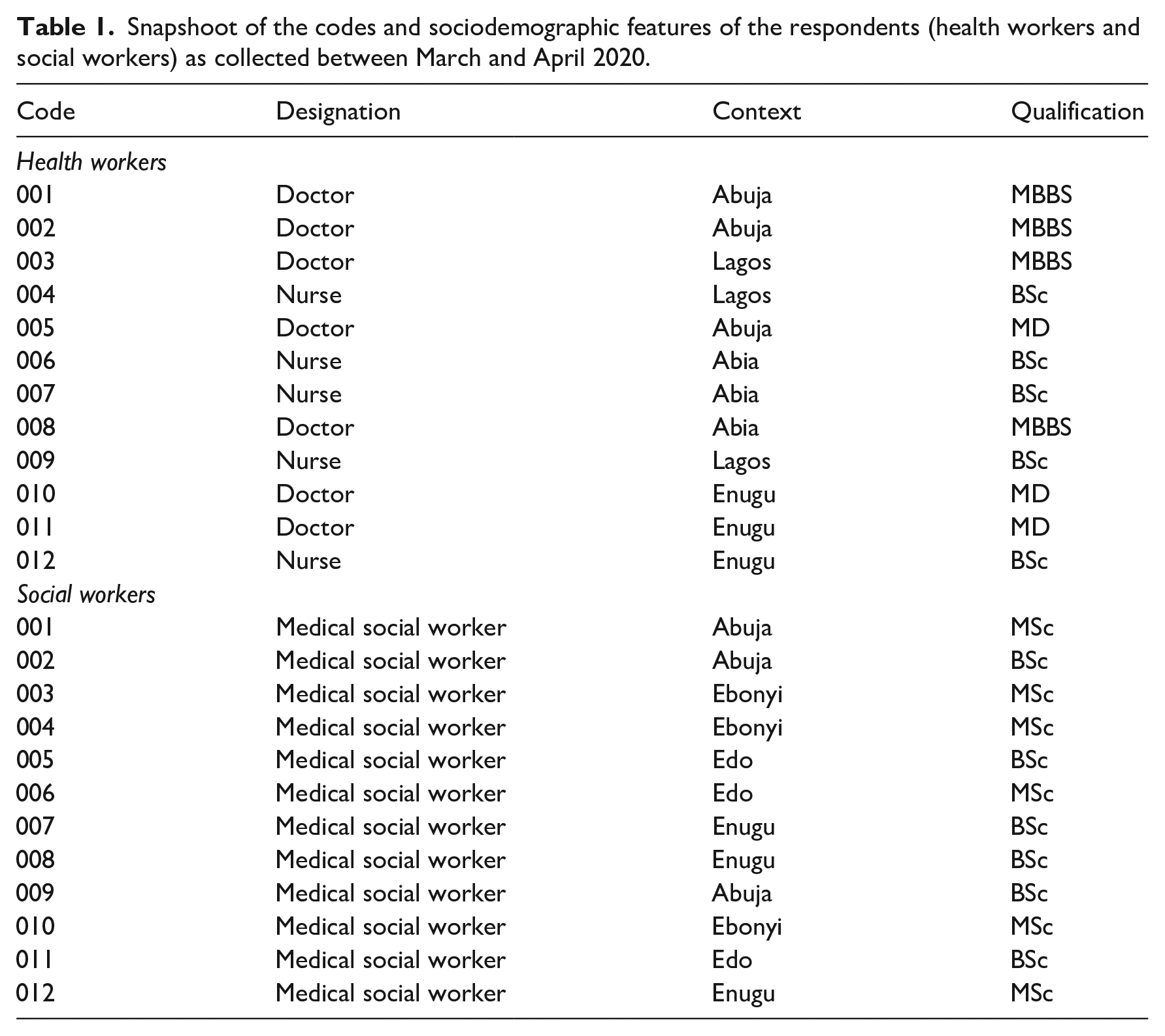
To keep a track of our respondents we allotted codes to each respondent we interviewed. The codes also serve as a means to anonymise the respondents. Table 1 shows the codes, as well as relevant descriptions of the respondents.
Snapshoot of the codes and sociodemographic features of the respondents (health workers and social workers) as collected between March and April 2020.
Influence of corruption and unaccountability on frontline health operations
Respondents were specific about instances of corruption and unaccountability that affected their efforts to contain COVID-19 during its peak periods. They reported that these concerns pertain to two levels – the structure (away from the facility and involving top healthcare management), and within their facilities. With regard to the structure, the respondents mentioned that allocated resources usually announced on the mainstream media never translated into improved conditions or protection for them. The resultant effect was that they had to protect themselves by deliberately avoiding suspected COVID-19 cases and discharging a lot of patients including those not due for discharge. A medical doctor said, Coronavirus started spreading in December. The government first allocated about 600m naira or so to the health sector to help contain the virus. In the whole of Abia State, we had no testing kit as of March. When health workers see a suspicious case, we run for our lives. Yet millions have been allocated to combat the virus and billions were given to the health sector in the 2020 budget. Who are we doing? If you come to our hospital now, we have discharged all elective cases, we only attend to emergency cases which we do with fear. (Doctor, Abia, 008)
The respondents blamed incessant strikes among health workers on poor incentives and welfare for health workers. They referred to their poor hazard allowances, which is nothing compared with what the politicians earn. To them, the politicians corruptly enrich themselves and give a pittance to health workers. Thus, some interviewed health workers reported nonchalance and apathy. See the quote below: When doctors are on strike, you should ask why? I get a hazard allowance of 5000naira ($12) and one politician goes home with millions and you expect me to put my life on the line. This is so unfair. Let the politicians go to hospitals and face coronavirus. I cannot risk my life for 5000naira. (Doctor, Lagos, 003)
Buttressing the lack of provisions for safety against hazards, which reflects a lack of accountability in the use of appropriations to the health sector to provide basic items like PPE, the same doctor as above recounted an experience during the Lassa fever outbreak. He mentioned that a colleague almost died because of the lack of PPE. And despite the risk the colleague took to save a life, she was abandoned by the government, and had to depend on contributions from colleagues to be treated. He mentioned that health workers who could recall that experience understood that the government cares less about their safety, which further contributed to the expressed poor commitment to their work.
During the Lassa fever outbreak, one of my colleagues in the process of treating a patient contracted the disease. PPE was not available to her but to save the life of the patient she risked her own life. The government did nothing to save her life. Colleagues had to contribute money to save her. I am happy she did not die but that has sent a strong signal that the government cares less about us. (Doctor, Lagos, 003)
Furthermore, some of the respondents talked about the unnecessary hike in the price of PPE and the hoarding of PPE even within their facilities.
We cannot deny the fact that some of the PPE are hoarded because of the skyrocketing demand currently . . . it should not be so. You can imagine that a carton of face masks I bought for 93,000naira [$186] last week, is now sold for about 400,000naira [$800]. A piece was sold for about 50 or 100naira [$0.2] before this time, now you buy it for like 500–700naira [$1]. Even the price of thermometer is so unimaginable now. This is too wicked of the companies, even while in the heat of a pandemic! (Nurse, Enugu, 012) Government might have provided PPE but they are hoarded in some of the facilities. They could be sold at the open market. (Social worker, Edo, 011)
Challenges affecting the fight against corruption and unaccountability by health workers
The health workers expressed interest in confronting the corruption situation; however, they listed some challenges they currently encounter. First was that they are preoccupied with clinical responsibilities and barely disposed to play the role of watchdog, as well as sustain intense advocacy. One of them said, We recently protested against not having PPE. Soon after the protest, they brought the PPE out. We lost time to our clinical functions, and patients were seriously affected. (Nurse, Abia, 007)
Second, the younger health workers especially talked about the need to respect senior health workers. On that ground, they were reluctant to confront issues involving the senior staff. Thus, they often find themselves tolerating certain excesses of their seniors, so that they do not get accused of insubordination.
There are times when our seniors will say to us that there are no PPE yet you still find them using PPE. Sometimes, they remind you that when they were younger they had no voice to make the demands we make now. At times too, they could reserve sterile gloves for themselves, and give you the younger one, latex glove. (Nurse, Abia, 006)
Third, they were of the view that some of their colleagues got employed on unmeritorious grounds. Thus, one does not expect such people to challenge the system because they could be embarrassed. This appeared to be a case of corruption fighting back.
Some health workers got the job through the backdoor. You do not expect them to speak up because they could be exposed or sacked. (Nurse, Lagos, 004)
Finally, the health workers said most of the corruption issues are inherent in the structure, and if they are to change things, they would have to begin by challenging the structure which comprises top government authorities and healthcare managers. For instance, they talked about unaccountability shrouding mobilized resources and believed that lack of transparency at the top translates to lack of transparency at the grassroots. A doctor is quoted as saying, We see donations flying here and there and no stewardship on how they are spent. It will shock you to know that even in this period, some of us are owed salaries. If [there is] no sincerity at the top, what do you expect at the bottom? (Doctor, Abia, 008)
Relevance of social work to health sector anticorruption in the COVID-19 context
Given the listed challenges faced by the health workers in confronting corruption and unaccountability that affected containment of COVID-19 at the frontline, we sought to know if social workers could help. A first things to note, most of the health workers had insufficient knowledge about social work roles, which affected how the profession was described. One of the doctors said, We have social workers around, but I cannot see how they can help us during this period of COVID-19. They often help us raise funds for poor patients, and assist those with psychological problems. They can aid those in antenatal care, do some public health education. (Doctor, Abuja, 005)
It was common to find ‘reductionary’ descriptions of the social work profession. One mentioned that social workers were disengaged in some facilities. At this point, we further asked what they think social workers could do differently in the health sector, with particular reference to addressing corruption concerns. So, they gave their views.
I suggest that they start with dialoguing with not just the hospital management, but the ministry of health so that their known scope of operations can be in the public domain. We need them to fish out those that are corrupt, especially in the procurement department because this hoarding we talked about often starts from there. (Doctor, Abia, 008)
A social worker added, If things work in Nigeria, we are expected to advocate for the welfare of the frontline health workers so that they do not use the time that should be given to their clinical responsibilities to do advocacy. We will also help to avert social actions like strikes that are not needed during this critical period and interface with authorities to at least do the minimum of the right things. (Social worker, Abuja, 009)
The health workers agreed that there is a need for watchdogs in health facilities and given the training of social workers, they can fill that gap.
So, I now see that the social workers even while employed with us can ensure that they speak truth to our faces, and that is what we need. Someone needs to bridge the gaps between patients and us; between juniors and seniors. It is important social workers are allowed to practice to their fullest mandate. (Nurse, Abia, 006)
Finally, we found that employment corruption also affects the recruitment of qualified social workers, which can be a constraint to how social workers can engage and improve anticorruption. One of the interviewed social workers said, My HOD did not study social work. She knows little about our expected job descriptions. I do not expect her to speak for us before the hospital management. (Social worker, Ebonyi, 004)
Discussion
The article provides more evidence on health sector corruption and how it affects the performance of the health workforce. In recent literature, health sector corruption is proven to be cancerous, especially for health systems in low resource regions, and it is beginning to gain more academic attention (Agwu et al., 2020a; Onwujekwe et al., 2018, 2019). Frontline health workers are key to containing public health emergencies, and COVID-19 was no exception. But to effectively face the challenges and threats that came with COVID-19, frontline health workers needed to be protected, incentivized and catered to. In contrast, our study found that in Nigeria this was not the case because of corruption and unaccountability. We discovered the need for a just health system as a vital component of addressing public health emergencies. Given the social justice and human rights training of social workers, we underscored their importance in contributing to a just healthcare system, and even more, health sector anticorruption.
Our study provides evidence on corruption within facilities and their governance structures. This had a negative influence on the efforts of frontline health workers in containing COVID-19. Incidentally, Nigeria’s health sector is listed among the top 5 corrupt institutions in the country (Sahara Reporters, 2019), and the emergence of COVID-19 seems to have made no difference. Respondents lamented poor welfare conditions of frontline health workers, citing meagre hazard allowances, absence of life insurance, poor and inconsistent salaries and human-induced scarcity of PPE. They recounted the several releases of funds as announced by the Federal Government through mainstream media outlets and many donations to the health sector to incentivize health workers, yet they were not optimally deployed. The indifference of the government even as prices of PPE skyrocketed by over 300% was to them a show of unaccountability. It was implied that such inflation was being exploited by those in the procurement department of the facilities as well as the senior health workers, as they were allegedly diverting hospital supplies to the private market for rent-seeking (manipulating or misusing public resources for private benefits) – a reason some respondents felt contributed to the dearth of PPE in the facilities. There were also alleged injustices happening within facilities that exposed the junior health workers to the risk of contracting the virus.
The experiences as summed up above suggest that the health workers were dissatisfied, affecting their attitudes to work. Job satisfaction comes from providing enabling working conditions, which our study has found were missing owing to corruption and unaccountability. The impacts of corruption at top healthcare management level could be seen. For instance, rationing and hoarding of PPE at the facilities might be connected with poor provisions of PPE by the government, despite the relatively huge allocated resources. We do not imply to make excuses for corrupt healthcare managers and procurement officials that might have deliberately hoarded PPE, as our findings reveal. However, we seek to further reinforce the importance of not allowing loopholes for corruption and unaccountability to thrive. To ensure this, the government should be honest about what resources are spent on, and effectively and transparently communicate such with health workers. This is one reason social workers are needed, to hold government accountable by advocating for clear communication on the receipt and spending of public resources.
The case of power relations in the health sector as a facilitator of health sector corruption is available in the literature (Agwu et al., 2020a, 2020b; Onwujekwe et al., 2019). This exists within and outside health facilities and could silence people’s voices. One aspect of power relations is the regard and respect junior health workers are expected to give their senior colleagues. Such acts go beyond the health setting, as respect is deeply rooted in the cultural values of Nigerians. However, our findings have shown that in the course of paying respect, juniors tend to lose their voices, even in the face of an obvious act of corruption or unaccountability perpetuated by a senior. It is for this reason that we found the need to bridge the divide between seniors and juniors through social workers. Social workers are trained to speak on behalf of the less powerful, as captured among their mandates (International Federation of Social Workers, 2014). Thus, in instances where juniors find it difficult to challenge the seniors, social workers can do so, as such role falls within their professional purview. Similar efforts are mentioned in literature (Lewis, 2015; Moyo, 2018; Wamara, 2017).
It was interesting to see how corruption could fight back. Persons who were employed on unmeritorious grounds were reportedly reluctant to challenge the system because they could be exposed. Employment corruption in Nigeria’s health system is high according to Onwujekwe et al. (2020b). This is a vital reason for scaling up conversations on health sector corruption, bringing it to the front burner of public domains. When competent persons are employed legitimately it goes a long way to build a strong and resilient health system that is needed to contain public health emergencies like COVID-19. Professional boundaries are spelt out, and dissatisfactions are expressed without fear.
With an understanding of social workers’ efforts in advancing and preserving social justice and human rights, even in the health sector (Moyo, 2018), our findings show that social workers in Nigeria still suffer an identity crisis and were relegated in the efforts aimed at addressing COVID-19. Similar findings exist in recent studies (Agwu and Okoye, 2021; Amadasun, 2020a; Nnama-Okechukwu et al., 2020; Onalu et al., 2020). We understand that social work in Nigeria is yet to be recognized as a profession by an act of law; however, we found social workers employed in hospitals. We got to know that some of the employed social workers had never studied social work. Therefore, while there is a need to ensure that the recruitment process of social workers into healthcare is based on merit and competence, those who are already working in these facilities should step up to performing their social justice roles, paying attention to anticorruption and unaccountability. Amadasun (2020a) is of the view that employed social workers within Nigeria must learn to be assertive in communicating and acting out their strengths and uniqueness as social justice professionals. Interestingly, there is evidence of the increasing involvement of social workers in anticorruption and political movement (Lewis, 2015; Wamara, 2017), and taking this into the health sector is needful.
Our findings show that the health workers agree that social workers will be meaningful in strengthening health systems, galvanizing social justice, promoting the voices of the less powerful, preserving human rights within their facilities and also facilitating better pandemic responses. They were of the view that they get distracted from their clinical functions when they at the same time simultaneously have to advocate against corruption and unaccountability. Thus, with social workers who are trained to advocate, mediate, mobilize resources and pursue social actions, taking up the fight for social justice and improved working conditions for the health workers in the context of any pandemic will help the health workers to be better placed to function at the frontline. In corroboration, Moyo (2018) argued that social workers must pay attention to issues of anticorruption and accountability in institutions, in addition to the normative psychosocial interventions they do with their clients.
Consequently, key social work actors such as the Association of Medical Social Workers in Nigeria (AMSWoN) and the National Association of Social Work Educators (NASWE) must begin a conversation with state actors like the Ministry of Health to allow for the widening of the scope of employed social workers in the health setting, in line with their social justice mandate. Just as the respondents recommended, the institutionalization of social work within the health sector has to be firmed up, and health workers should be educated about the expected roles of the social workers. Mainstreaming social work services into anticorruption in public services, as well as aligning interests with non-state actors like civil society organizations (CSOs), will also be vital.
Nigeria has a weak health system with very poor health indices, and the absence of social care and justice suffice for an important reason (Garcia, 2019; Onwujekwe et al., 2020b). While there is evidence to show that indeed the country’s health system bleeds, in which corruption and unaccountability play prime roles, there is no evidence to show if the country’s governments at all levels (Federal, State and Local levels) are passionately interested in anticorruption in the health sector (Onwujekwe et al., 2020a). Given such a gap, our evidence shows that the potentials of social workers can be harnessed in this regard, since they are the readily available social justice professionals within Nigeria’s healthcare, especially at the tertiary level. Even though the profession is not yet backed by an act of law, it could be a good start to improve anticorruption in health, further calling for the need to professionalize social work in Nigeria.
In conclusion, it was expected that after the 2014 Ebola crisis, the health system in Nigeria will be exceptionally revamped. Unfortunately, the health sector either remained the same or went backwards (Dadwal, 2020). Transparency International highlighted how the Ebola outbreak exacerbated corruption and unaccountability in the health sector of most low- and middle-income countries (LMICs) and Nigeria in particular (Transparency International, 2020). The organization predicted that lessons seem not to have been learned from the Ebola experience, and just like Ebola, coronavirus could make regimes in LMICs and their health sectors more corrupt. The fact that health workers stay away from the frontline battle against COVID-19 owing to poor working conditions is not encouraging, even when resources are available to cater to their concerns (Ewubare, 2020; Onwujekwe and Agwu, 2020; Ripples Nigeria, 2020). Hence, the more reason to institute accountability and anticorruption, of which hospital social workers can take the charge (Kavanagh et al., 2020; Odubanjo, 2020).
Finally, the limitation of this study can be said to be that the researchers were not physically present at these locations to triangulate responses with physical observations, especially those that are facility-centred. However, in several instances, we got corroboration from other studies and the media, particularly with regard to how corruption and unaccountability tend to have marred efforts at the frontline against COVID-19 in Nigeria. Also, perspectives from top actors in social work organizations were not captured. However, our respondents who are medical social workers are all members of AMSWoN, and their views could be representative of concerns in the organization. All in all, we believe our study has provided some insights to strengthening the Nigerian health system using social justice professionals like social workers. We hope that by the evidence we have provided, we can add to the call for professionalizing social work in Nigeria and engaging them as providers of social justice and care within the health sector.
Footnotes
Acknowledgements
We are grateful to the respondents who took time out of their busy schedules to respond to us. We equally thank the peers who read through the analysis spreadsheet and gave incisive comments that improved the quality of our analysis. The authors are members of the Technical Working Group on Action on Accountability and Anti-Corruption for the SDGs under Health Systems Global (HSG).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethics approval and consent to participate
Ethical approval was granted by the Health Research Ethics Committee of the University of Nigeria Teaching Hospital, Ituku-Ozalla (approval no. NHREC/05/01/2008B-FWA00002458-IRB00002323). Verbal consent was sought as approved by the Research Ethics Committee. The reason for verbal consent is because we adopted telephone interviews. However, participants only consented on the premise that they are promised anonymity, which we accepted.