
Abstract
The article describes a quantitative cross-sectional study of a sample of 674 university students enrolled in social work programmes in four countries: Belgium, Canada, Chile and Switzerland. The study aimed to assess HIV/AIDS knowledge and attitudes among participants. The median HIV-KQ-18 score for the sample was 14.0, which Carey and Schroder classify as indicating borderline low levels of knowledge. Based on the results, the authors argue that social work education and training programmes should more comprehensively address HIV/AIDS within their curricula to better equip future social workers to challenge stigmatising and exclusionary practices rooted in long-standing lack of knowledge and erroneous beliefs about the disease.
Introduction
Multiple studies have examined knowledge of and attitudes towards HIV/AIDS among students in higher education (Labra, 2015; Labra et al., 2017; Maimaiti et al., 2010; Tulloch et al., 2012; Tung et al., 2013). Numerous other studies, in addition, have examined the same themes in relation to populations such as caregivers (Labra and Dumont, 2012; Vandebroek et al., 2011), men involved in sexual relations with other men (Larmarange, 2020), drug users (Wagenaar et al., 2012; Wolfe et al., 2010) and native communities (Guthrie et al., 2000; Negin et al., 2015; Sumari-de Boer et al., 2012). These studies show that the range of factors influencing knowledge of and attitudes towards HIV/AIDS include education levels, religious identity, socio-economic status and personally knowing people living with HIV/AIDS (PLHIV/AIDS).
The literature shows also that certain practices on the part of health professionals perpetuate a stigmatisation of PLHIV/AIDS; these practices result from fear, lack of information and education, lack of contact with infected individuals and non-premeditated behaviours (Davtyan et al., 2017; Labra and Thomas, 2017). And while the emotional and psychological support of nurses and social workers has been shown to have a positive impact on infected individuals’ perceptions of their own condition (Stowers Johansen and Kohli, 2012), stigmatisation, in contrast, has been identified as a cause of physical and mental health problems, as well as the decreased use of health services (Belenko et al., 2016; Geter et al., 2018; Logie et al., 2018; Stringer et al., 2016).
Since the outbreak of the AIDS pandemic, social workers have played crucial roles in the delivery of services to people infected by HIV/AIDS, as well as in the dissemination of knowledge about the disease (Kaplan et al., 2004; Linsk, 2011). The social work discipline’s tenets and approaches have positioned it to play a highly useful role within efforts deployed to meet the complex challenges of managing the epidemic (Sacramento, 2015). Within the body of Canadian literature, only a very few studies have addressed HIV/AIDS knowledge and attitudes among populations of healthcare students (Hoffart et al., 2012; Jaworsky et al., 2017) and it is necessary to look further afield to identify research examining these themes in relation to populations of social work students (Handal, 2017; Koob and Harvan, 2003; Natale et al., 2010). Indeed, it seems that, over the last 20 years, few studies have aimed to examine HIV/AIDS knowledge and attitudes among higher education students in general (Cassidy et al., 2015; Labra et al., 2017).
This dearth of research on the subject is problematic because social workers have privileged access to not only the most affected but also the most marginalised populations of PLHIV/AIDS and must, therefore, be able to respond adequately to those populations’ prevention and intervention needs (Bowen, 2013). This is all the more so because the challenges which the pandemic presents continue to evolve, notably due to the ageing of infected populations (Beuthin et al., 2015; Hasse et al., 2011) and because social representations of the disease remain in flux (Goodwin et al., 2004; Labra, 2015). As Dubois-Arber et al. (2001) warned over 15 years ago, it is imperative to ensure that the normalisation of HIV/AIDS does not lead education programmes to forego integrating notions of prevention into their curricula, since this would lead to a regression of HIV/AIDS prevention knowledge and practices. Corroborating this forewarning, Wolf and Mitchell (2002) found that practitioners whose education had included components on HIV/AIDS were more likely to have conducted interventions than practitioners who had received no training related to the disease. Studies conducted outside Canada show that multiple social work training programmes fail to address HIV/AIDS themes, or do so summarily (Handal, 2017; Koob and Harvan, 2003; Natale et al., 2010; Rowan and Shears, 2011).
Since social representations of HIV/AIDS, as well as the life conditions of infected individuals, continue to evolve, this study aims to remedy the lacunae in the research literature, noted above, by examining levels of knowledge about and attitudes towards the disease and PLHIV/AIDS among social work students enrolled in university programmes across four countries: Belgium, Canada, Chile and Switzerland.
Methodology
A cross-sectional study was carried out on a convenience sample of students enrolled in social work programmes at institutions across three continents, specifically, Haute École de Namur-Liège-Luxembourg (Belgium), Université du Québec en Abitibi-Témiscamingue (Canada), Universidad de Concepción (Chile) and Haute école de travail social et de la santé Lausanne (Switzerland). The study involved students who were enrolled during the Fall 2018 and Winter 2019 semesters, both in full-time and part-time social work studies. In September 2018, participants were invited, by way of messages sent to their institutional email accounts, to fill out a questionnaire designed to assess their knowledge of and attitudes towards HIV/AIDS. Follow-up reminder messages were sent in February 2019. The study used SurveyMonkey® software for the online questionnaire platform, accessible to participants throughout two data collection periods, that is, 17–28 September 2018 and 11–22 February 2019.
The questionnaire opened with an introduction designed to ensure free and informed consent. The first question aimed to assess social work students’ HIV/AIDS knowledge levels using a 5-point Likert-type scale, ranging between ‘very low’ and ‘very high’. The participants’ knowledge levels were further measured using the Brief HIV Knowledge Questionnaire (HIV-KQ-18) (Carey and Schroder, 2002). This validated scale consists of 18 points to be answered in the ‘True / False / I don’t know’ format. Scores range from 0 to 18, with higher scores indicating higher levels of knowledge. A score of 13 of 18 (just above two thirds of correct answers) indicates a low level of HIV/AIDS knowledge (Wagenaar et al., 2012). The questionnaire also addressed participants’ attitudes towards HIV/AIDS, employing a series of elements: a 5-point Likert-type scale ranging from ‘very low’ to ‘very high’, having personally known someone with HIV/AIDS (Yes or No), as well as closed and semi-closed questions on attitudes towards HIV/AIDS, drawn from questionnaires designed to gauge attitudes among Canada’s francophone population, developed by the Public Health Agency of Canada (Agence de la santé publique du Canada, 2003, 2006). This study has been approved by the UQAT Human Research Ethics Committee (Certificate no. 2018-06).
Data analysis
Measures of central tendency and dispersion were calculated to describe the sample, in particular, in terms of the participants’ median level of knowledge and most frequently reported attitudes in relation to HIV/AIDS. The average HIV-KQ-18 score was tabulated and analysed as quartiles (very low, low, average and high levels of HIV/AIDS knowledge). An assessment of variable multicollinearity was followed by a contingency analysis (chi-square test) to ascertain the level of dependence between variables indicating HIV/AIDS-related beliefs, perceptions and knowledge (also analysed as quartiles of the average HIV-KQ-18 score).
In addition, a principal component analysis (PCA) was carried out to detect differential behaviours, that is, dominant factors, such as beliefs about and perceptions of HIV/AIDS, to categorise participants into sub-groups, defined by significant intergroup differences and less significant intragroup differences, in relation to social representations and knowledge of HIV/AIDS. Collected data were processed using IBM SPSS Statistics® software.
Results
The participant sample was composed of 674 participants studying at institutions based in Chile (CH: 30.7%), Belgium (BE: 28.6%), Switzerland (SU: 23.1%) and Canada (CA: 10.5%). The sample was overwhelmingly composed of women (84.6%), while men represented only 14.8 percent of respondents. A majority of participants were single (67.7%), while 30.8 percent reported being in a relationship and 1.5 percent had divorced or separated. In terms of age distribution, 25.7 percent of participants were aged 19 years or younger, 54.9 percent were between 20 and 24 years of age and 19.3 percent were aged 25 years or older. More than half of the participants were unemployed (61.6%), approximately a third held part-time employment (33.0%) and a small minority held full-time jobs (5.2%). In terms of place of residence, 48.7 percent of participants lived in urban areas, 36.9 percent resided in rural communities and 14.1 percent lived in mixed urban-rural areas.
The total HIV-KQ-18 score of participants was calculated to assess student knowledge of HIV/AIDS. As shown in Table 1, below, the median score of the sample was 14.0, which, according to Carey and Schroder (2002), represents borderline low levels of knowledge. It is important to note that 36.8 percent of participants considered their level of knowledge to be high or very high, while 48.7 percent described their knowledge as average and 14.2 percent indicated low or very low knowledge levels. The study also identified participants’ sources of information on HIV/AIDS. While most respondents reported drawing on multiple sources of information, those cited most frequently were school (80.5%), television (62.2%), family and social circle (54.9%), Internet (53.4%), community organisations (39.7%), public service messages (34.7%) and physicians (31%). Tellingly, only 28.3 percent reported social work studies as a source of information on HIV/AIDS. It is noteworthy that participants had obtained information from a wide variety of sources: only 1 in 10 reported gaining information on HIV/AIDS in up to two of these sources and close to half of the respondents had drawn on three to seven of the sources, while a third reported gaining information from eight or more of the sources cited above.
Students’ levels of HIV/AIDS knowledge in relation to age.
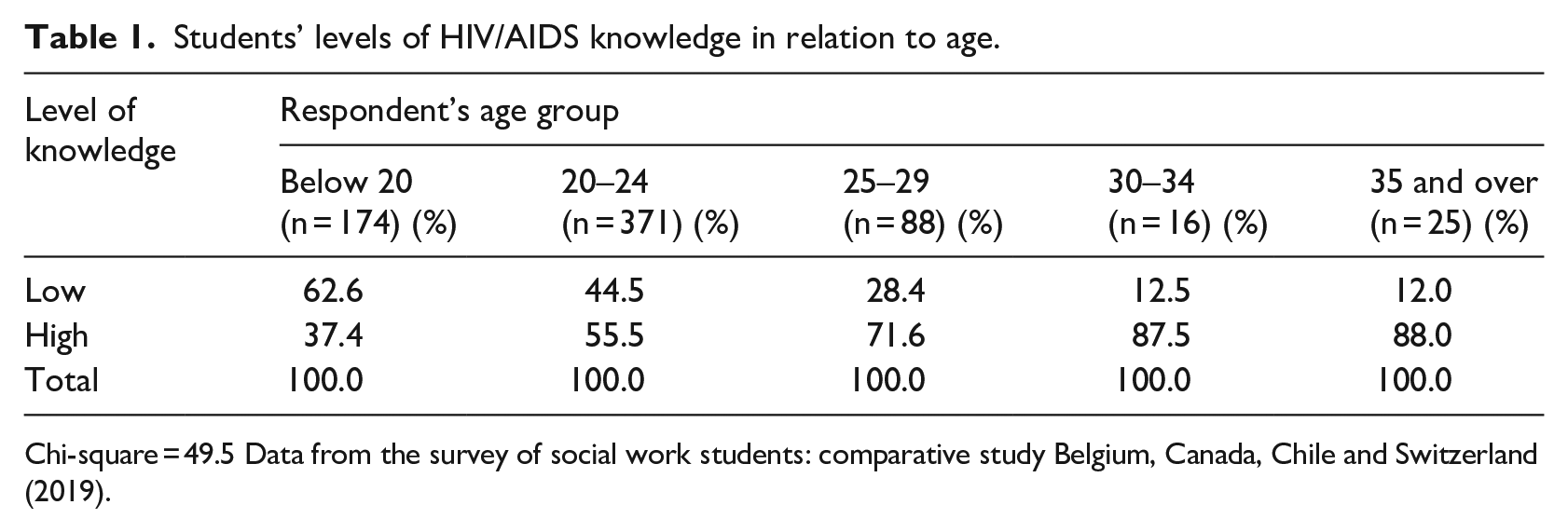
Chi-square = 49.5 Data from the survey of social work students: comparative study Belgium, Canada, Chile and Switzerland (2019).
Notwithstanding this informational breadth, 77.9 percent of participating students considered that the risk of contracting HIV/AIDS was low or very low. However, fully 88.3 percent of participants felt that HIV/AIDS represents a serious or relatively serious ongoing problem. It is important to mention, as well, that respondents scoring 14 or higher on the HIV-KQ-18 were proportionally more likely to know someone infected with HIV/AIDS (chi-square = 17.9). More precisely, 132 respondents (19.3%) knew someone living with HIV/AIDS; of this proportion, a majority stated that the disease had not changed (60.2%) or only slightly changed (26.7%) their behaviour towards the infected individual. The principal changes in behaviour towards PLHIV reported by participants were increased emotional support (37.3%) and empathy (24.0%).
Following the analysis of HIV-KQ-18 scores, participants were separated into two groups to ascertain whether respondents’ characteristics had an impact on levels of HIV/AIDS knowledge. The analysis showed that three characteristics had statistically significant links with knowledge levels: age, country of studies and socio-professional status.
When test scores are correlated with participants’ age, it becomes apparent that knowledge levels rise with age, thus the older the social work students, the higher their levels of knowledge on HIV/AIDS.
The second significant variable was the participants’ country of origin. The data show, for example, that Belgian students were more likely to have low levels of HIV/AIDS knowledge, while students in Switzerland generally possessed higher levels of knowledge (Table 2).
Students’ levels of HIV/AIDS knowledge in relation to country of origin.
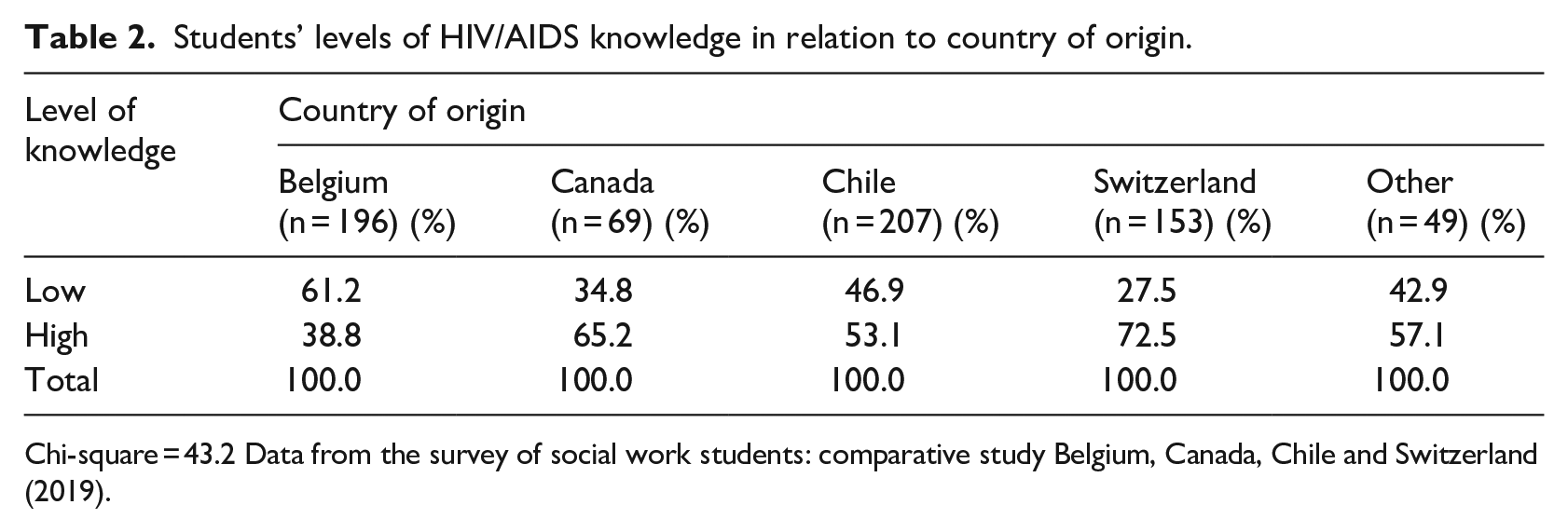
Chi-square = 43.2 Data from the survey of social work students: comparative study Belgium, Canada, Chile and Switzerland (2019).
Finally, the analysis noted a dependency relationship between students’ socio-professional status and levels of knowledge about the disease: participants engaged in full-time employment were proportionally more likely to possess higher levels of knowledge on HIV/AIDS.
In terms of students’ attitudes, the data collected for the purposes of this study show that social work students convey relatively positive attitudes towards PLHIV/AIDS (see Table 3). A comparative analysis did, however, identify several elements of note. For example, participants with an HIV-KQ-18 score of 14 or higher were proportionally more likely to answer that they fully agreed that PLHIV are able to exercise professions in direct contact with the public (chi-square = 21.0).
Students’ attitudes towards PLHIV/AIDS as percentage of agreement with statements, by country.
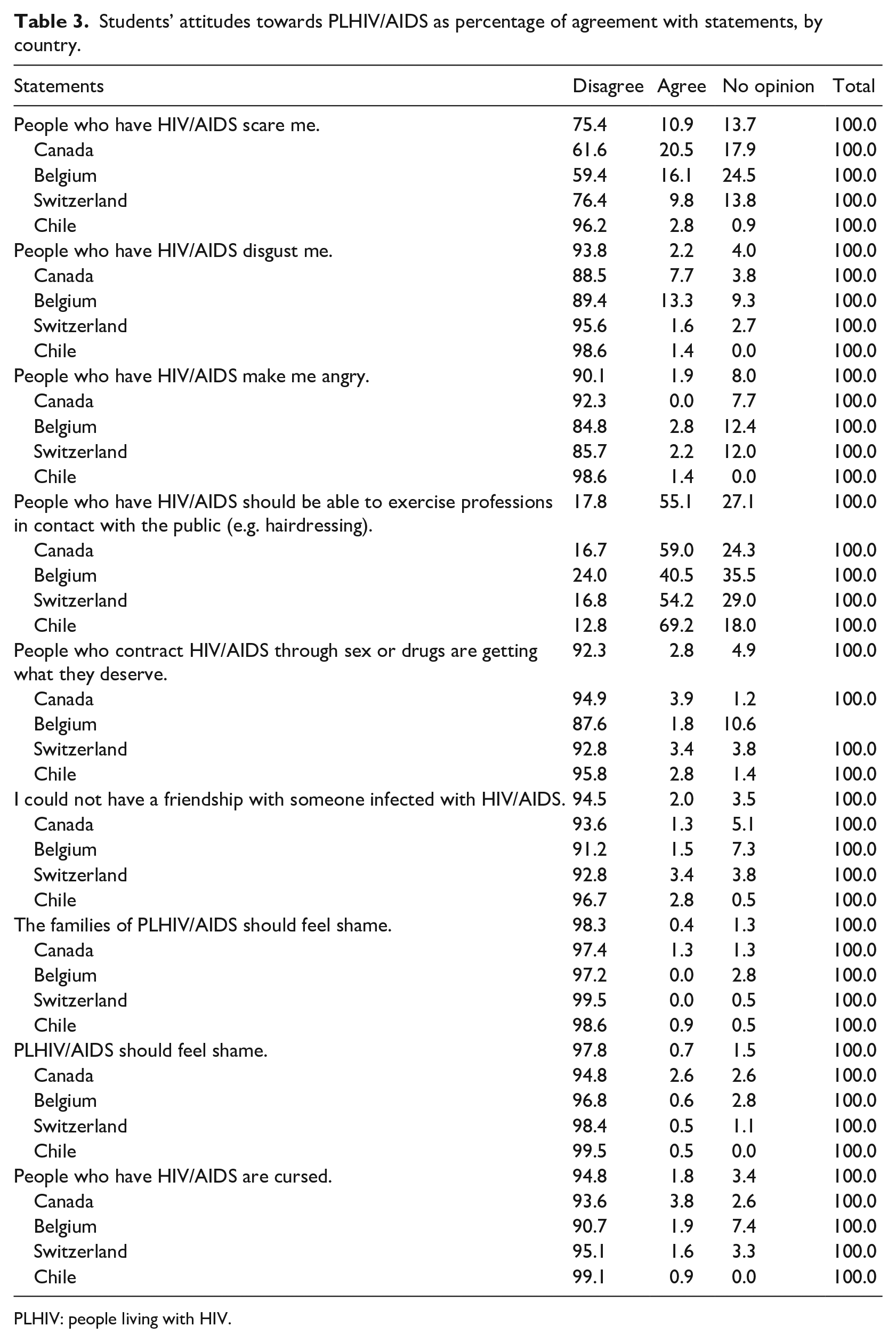
PLHIV: people living with HIV.
The study aimed also to assess participants’ opinions on social ostracisation of PLHIV/AIDS (see Table 4). The results show that high proportions of respondents indicated having no opinion on the statements presented in the questionnaire relative to ostracisation. Nevertheless, the answers of those who did report an opinion show that PLHIV/AIDS experience peer rejection and loss of respect in their communities. However, respondents also negated notions of other forms of ostracisation. It is imperative to note, in addition, that 52.6 percent of respondents studying in Chile disagreed with the notion that PLHIV/AIDS should be allowed to participate fully in socio-cultural activities. This is in stark contrast to answers provided by students from the other countries considered in the study. It is also noteworthy that participants’ HIV-KQ-18 scores, assessing their knowledge of the disease, seem to have no correlation with the attitudes expressed in this part of the study, except in relation to two statements, discussed below.
Students’ opinions on the ostracisation of PLHIV/AIDS in their communities as percentage of agreement with statements, by country.
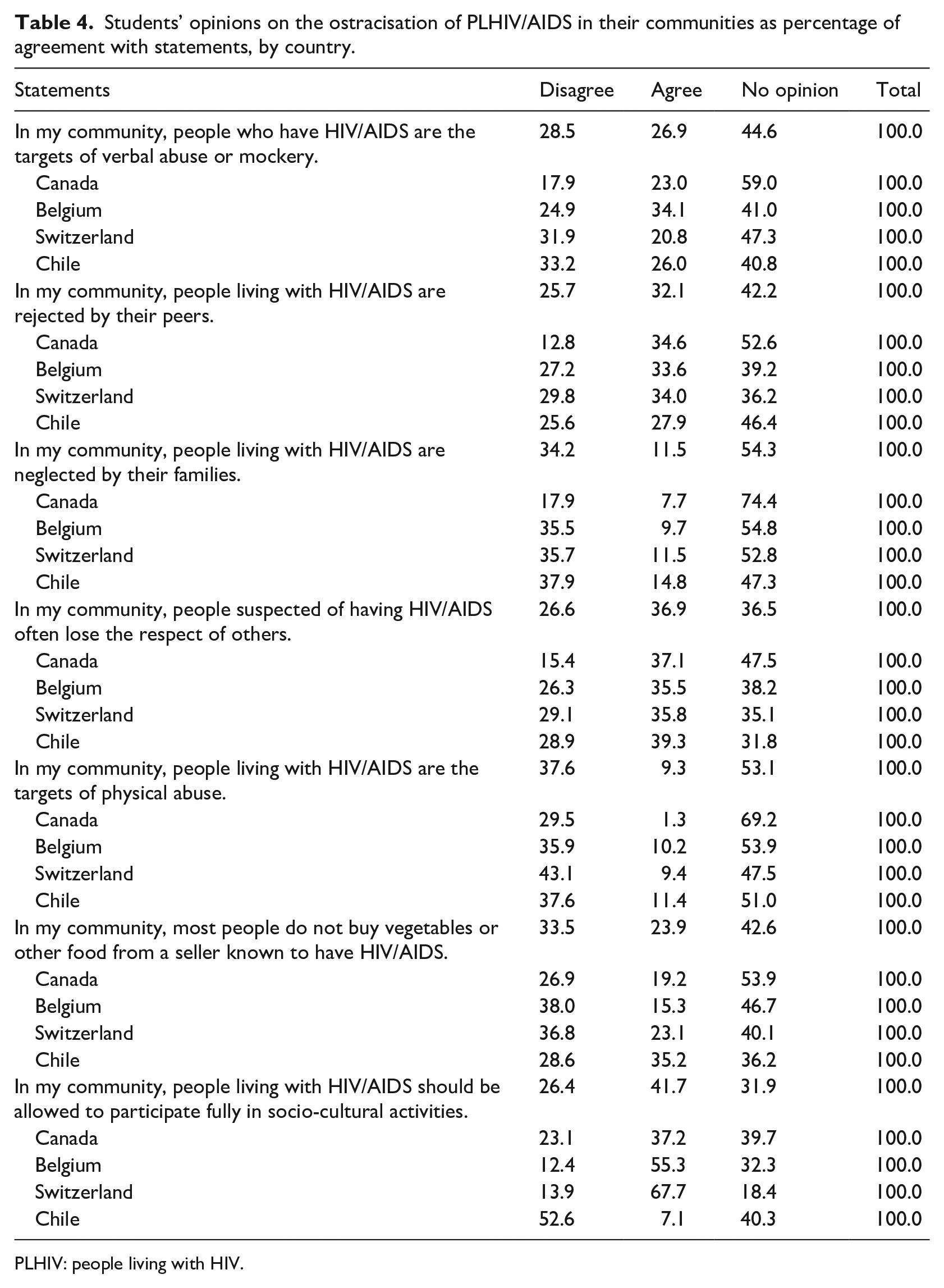
PLHIV: people living with HIV.
Furthermore, in terms of the levels of comfort expressed by students in relation to situations involving PLHIV/AIDS, two results stand out. First, it appears that respondents scoring 14 or higher on the HIV-KQ-18 questionnaire were proportionally more likely to be very comfortable with their child attending a school in which another student had been diagnosed with HIV/AIDS (chi-square = 33,366). Second, it appears also that respondents scoring 14 or higher on the HIV-KQ-18 scale were proportionally more likely to be very comfortable with a close friend or family member having close contact with someone diagnosed with HIV/AIDS (chi-square = 27,644). Overall, however, it must be noted that the majority of students across the four countries under study reported feeling comfortable in a variety of situations involving PLHIV/AIDS, as shown in Table 5.
Students’ comfort levels in situations involving contact with PLHIV/AIDS as percentage, by country.
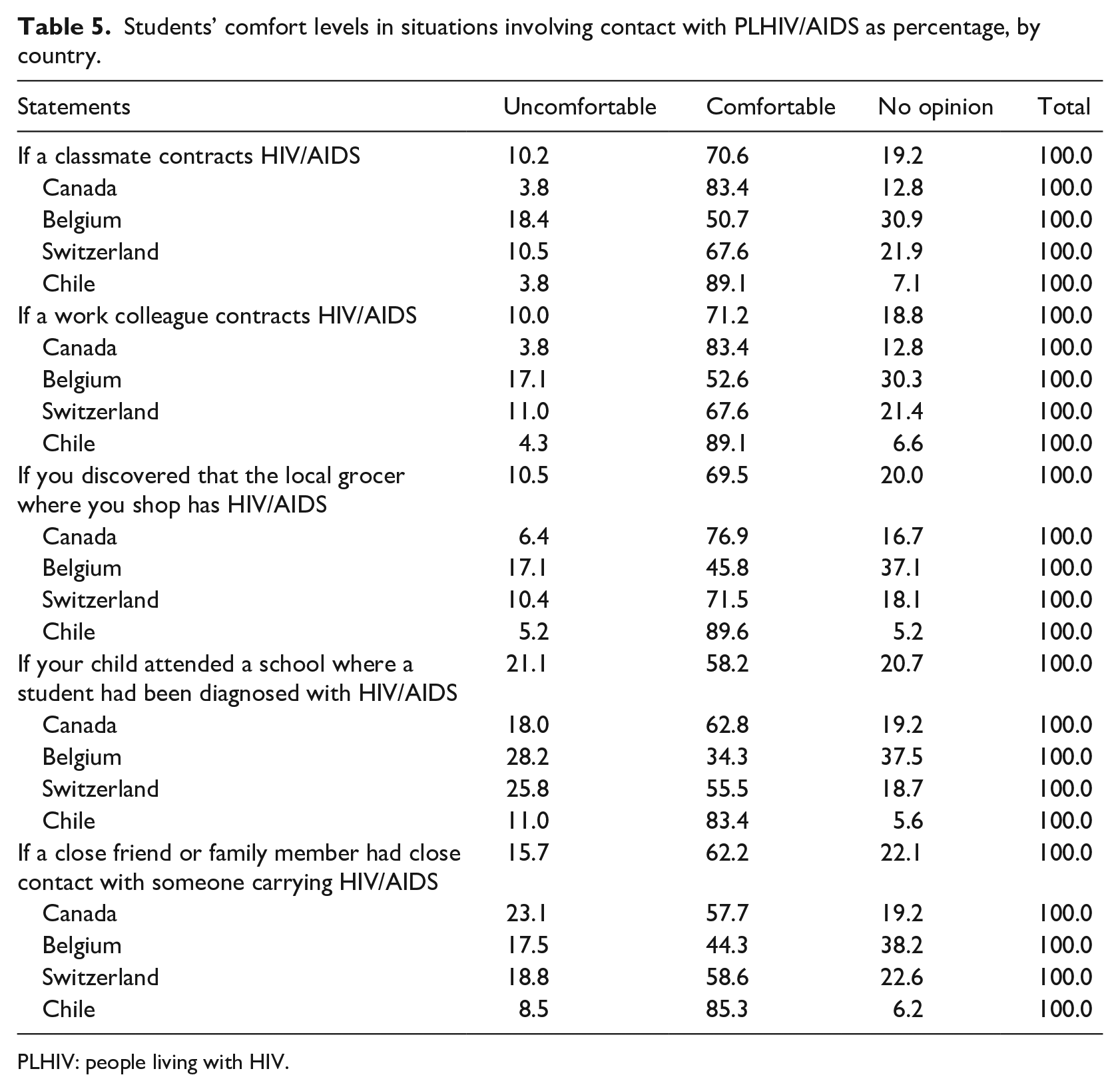
PLHIV: people living with HIV.
Discussion
The present discussion will focus on the two major themes addressed in the ‘Results’ section, above, that is, HIV/AIDS-related knowledge and attitudes among social work students enrolled at higher learning institutions across four countries. The discussion will aim to identify participants’ social representations of the disease.
To begin, we must acknowledge that social work students’ knowledge of and attitudes towards HIV/AIDS are largely informed by the collective imagination and social representations of the disease that have been evolving worldwide since cases were first identified in the United States in the early 1980s (Labra, 2015). In the intervening decades, it seems that the spread of general knowledge about HIV/AIDS has not kept pace with the spread of the disease, a reality that is reflected in the results of this study. The median HIV-KQ-18 score of 14.0 (Carey and Schroder, 2002) achieved by study participants leads us to conclude that, overall, undergraduate university students enrolled in social work programmes in Belgium, Canada, Chile and Switzerland possess relatively low levels of knowledge about HIV/AIDS. This result parallels that obtained by a previous study by Labra et al. (2017), in which 20.3 percent of student respondents achieved scores of ⩽13 on 18, also indicating low levels of knowledge. Similarly, a study of homosexual African-American men by Wagenaar et al. (2012) obtained comparable results.
The low levels of HIV/AIDS knowledge noted among students participating in the present study are accompanied by the finding that a majority (77.9%) considered themselves to be at low risk of infection by HIV/AIDS. How might we explain this perception of low risk, founded, as it is, in a lack of knowledge? A plausible hypothesis is that students do not assess the risk of infection realistically. Indeed, a glaring contradiction emerges from their testimonies: how can one feel protected without having the knowledge necessary to protect oneself? Do other variables lead students to perceive themselves as being at low risk of contagion? An abundant literature shows clearly that a dearth of information on HIV/AIDS correlates both with infection risks and with discriminatory practices (Labra and Dumont, 2012; Negin et al., 2015; Sumari-de Boer et al., 2012; Tulloch et al., 2012).
In terms of variables influencing low levels of knowledge on HIV/AIDS among students participating in the study, an analysis of the results shows that knowledge levels correlate with age, specifically that knowledge increases with increasing age and that, consequently, younger participants possess less knowledge. Adrien et al. (2013) had noted that knowledge about HIV/AIDS tends to be limited in younger populations. As mentioned above, levels of participants’ knowledge related to HIV/AIDS varied also by country. Across the four countries considered in the study, students in Switzerland were proportionally more likely to possess high levels of knowledge, while students in Belgium presented the lowest levels of HIV/AIDS knowledge among the participating groups. Given the links between knowledge and risk perception noted earlier, it appears that students in the Belgian sub-sample are more vulnerable to the risk of infection in comparison with Canadian, Chilean and Swiss social work students (see Table 2). In addition, the results point to a dependency relationship between the variable of socio-professional status and levels of HIV/AIDS knowledge. Specifically, among the study participants in the four countries under discussion, those who held full-time employment were more likely to possess good levels of knowledge about the disease than were those employed part-time or unemployed. The question that arises, therefore, is what is the link in the apparent correlation between full-time employment among students and their levels of HIV/AIDS knowledge, in comparison with those who work less or who do not work outside their studies? Possible answers will have to wait for further studies of variables impacting on the knowledge levels of students.
In terms of the attitudes of social work students towards the disease and towards PLHIV/AIDS, the results indicate that they are generally positive among participants scoring higher than 14 on the HIV-KQ-18 scale (Carey and Schroder, 2002). This finding suggests that social representations of HIV/AIDS have changed since the first critical years of the pandemic, specifically in that they have evolved positively, as reflected in the views of social work students. It is noteworthy, for example, that only 17.8 percent of participants across the four countries disagreed with the notion that PLHIV/AIDS should be able to work with the public in professions such as dentistry or hairdressing. This implies that the favourable attitudes of some participants are subject to the condition that PLHIV/AIDS are not perceived as exposing others to the risk of infection. This suggests, furthermore, that an essentially well-founded fear of infection nevertheless accentuates the ostracisation of PLHIV/AIDS, especially by limiting their access to various ‘hands-on’ professions in fields such as healthcare and the beauty industry, which previous research has identified as ‘socially forbidden’ for PLHIV/AIDS (Infante et al., 2006).
In addition, participants’ answers on the representations of PLHIV/AIDS in their communities suggest the continued existence of stigmatisation. In relation to the seven statements pertaining to PLHIV/AIDS in their communities on which participants were asked to give their opinion, the results show that social acceptance is not the norm. Thus, almost 40 years since cases of HIV infection were first identified (Markova and Wilkie, 1987; Schlebusch et al., 1991), negative representations of PLHIV/AIDS persist in the collective imagination, specifically those that portray infected individuals as socially marginal and deviant (Labra and Dumont, 2012). Research published in the last 20 years undoubtedly points to a positive evolution of HIV/AIDS social representations in comparison with the two preceding decades (Joffe and Bettega, 2003; Labra, 2015). Nevertheless, disdain, stigma and fear of the disease and its carriers persist within the social environments of students who participated in this study.
Persistently negative attitudes towards PLHIV/AIDS have been the subject of multiple studies (Al-Rabeei et al., 2012; Iwoi et al., 2017; Linguissi et al., 2018). It is important to underline that the results of this study show that social work students scoring higher than 14 on the HIV-KQ-18 scale (Carey and Schroder, 2002) responded favourably to the notion of sending their children to a school where another student was diagnosed with HIV/AIDS. The same sub-group communicated an openness towards PLHIV/AIDS within the social and family circle. Finally, the generally positive attitudes towards the disease and PLHIV/AIDS, as expressed by participating social work students in Belgium, Canada, Chile and Switzerland, corroborate a positive trend noted in other studies carried out over the past 5 years (Labra et al., 2017; Labra and Lacasse, 2015).
Social work and HIV/AIDS education
The results of this study raise two fundamental questions related to the education and training of social workers. First, given that social workers play a crucial role in delivering interventions to PLHIV/AIDS, how can we explain the low HIV-KQ-18 median scores, noted above, which indicate borderline low levels of knowledge about the disease (Kaplan et al., 2004; Linsk, 2011)? Part of the answer may lie in the normalisation of the disease: it is possible that an excessive confidence in HIV/AIDS prevention has led to a perceived lesser need to teach knowledge about the disease and the challenges faced by PLHIV/AIDS within existing curricula (Dubois-Arber et al., 2001). Such gaps in education and training may have highly deleterious effects on interventions delivered by future social workers, since the lack of knowledge and awareness of the realities of the disease frequently results in practices that stigmatise PLHIV/AIDS (Davtyan et al., 2017; Labra and Thomas, 2017). The research literature shows, indeed, that healthcare workers and institutions are not exempt from perpetuating various forms of stigmatisation and discrimination with regard to PLHIV/AIDS (Arrey et al., 2017; Pezeril, 2017; Wagner et al., 2016). This lack of knowledge, beyond the impact it may have on social work professionals’ capacity to empathise with PLHIV/AIDS, can also impact their know-how, notably in terms of recourse to inclusive practices. A study by Désilets (2019), for example, showed that practitioners who delivered services to women both living with HIV/AIDS and victims of domestic violence demonstrated sometimes low levels of knowledge of one or both of these issues, resulting in difficulties in delivering effective interventions.
The second question we must address in relation to low HIV-KQ-18 scores among social work students relates to the ethical dimensions of interventions, that is, how will future social workers be able successfully to face the ethical challenges of interventions for PLHIV/AIDS if they do not acquire adequate levels of knowledge about the disease and its realities within the course of their education (Gonin and Tellier, 2018)? This is a crucial issue. When faced with questions relating to the exclusion and stigmatisation of PLHIV/AIDS in their communities, the overwhelming majority chose not to answer, which suggests that social work students are largely unaware of the impact of discrimination on people living with the disease (Observatoire SIS Association, 2019; Pezeril, 2017; Public Health Agency of Canada, 2015). Yet interventions for PLHIV/AIDS are potentially fraught with ethical challenges, such as, for example, divulging a service recipient’s HIV positivity (Legault, 1999).
Solutions to redress these fundamental shortcomings in social work education and training must focus on three elements, namely, (1) raising awareness among both instructors and students of the realities of PLHIV/AIDS and the ongoing nature of the disease, to counteract a widespread banalisation of HIV/AIDS and the notion that it exists only elsewhere, far from one’s own community, (2) integrating HIV/AIDS into the core courses of social work curricula as an actual social problem, to provide students with ready access to knowledge on the realities of PLHIV/AIDS and (3) promoting the broadening of research into HIV/AIDS themes in social work schools, especially such dimensions as the lived realities of PLHIV/AIDS, community intervention models and ongoing student support, among others.
Conclusion
This study aimed to assess levels of knowledge and determine the attitudes of social work university students in four different countries in relation to HIV/AIDS and infected individuals. We can conclude that the variables of knowledge and attitudes examined in the present study, among 674 social work students, are improving slowly, especially in terms of the basic knowledge that can reasonably be expected of undergraduate students.
The HIV/AIDS pandemic, in particular because of its specific history, places unique responsibilities on social workers. Social representations of the disease have evolved from those of a lethal affliction towards those of a chronic condition (Labra and Lacasse, 2015). What remains to be raised is the need to include HIV/AIDS in the training of social work students. The development of biomedicine has enabled HIV/AIDS to progress from a fatal disease to a chronic disease. But the fight against the stigmatisation and exclusion occasioned by the pandemic makes social workers indispensable in their role as agents of social change and defenders of individual freedom, autonomy and self-determination for those living with the disease. Within this context, the support that social workers deliver to PLHIV/AIDS and their loved ones, especially for those in the terminal stages of the disease, plays a key role in the intervention domain. It is crucial, therefore, that social work education and training focus on systemic perspective analyses, which consider PLHIV/AIDS not in isolation, but as belonging to an environment that includes their families, social circles and communities. Social workers can thus fulfil a crucial need in PLHIV/AIDS intervention, in particular by drawing on pluridisciplinary approaches. Overall, social work education must more comprehensively incorporate HIV/AIDS themes into its curricula if we are to train professionals who are knowledgeable, committed and cognizant of the realities of PLHIV/AIDS.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.