
Abstract
This study examined deinstitutionalisation in Thailand. Qualitative interviews were conducted with a total of 27 child welfare practitioners and policy actors to explore their perceptions of Thai alternative care provision. Findings show that participants perceive deinstitutionalisation as a complex policy challenge. Some felt that the institutions were necessary in order to meet demand, while others felt that cultural barriers prevent a shift to family-based approaches, such as foster care. However, data suggest that it would be difficult to characterise deinstitutionalisation as a ‘wicked policy problem’ as participants were hopeful for change, citing increased family- strengthening policies alongside efforts to implement foster care.
Introduction
The reasons for children entering alternative care differ across international contexts. For example, in high-income countries, the majority of children in public care are placed because of state interventions, often due to child protection concerns about abuse and neglect (Rogers, 2018). However, in low- to middle-income countries, the drivers resulting in entry to care can be more diverse. For example, in Thailand, among the estimated 55,000 children living in alternative care only 4.9 percent are placed because of child protection concerns, while the majority are relinquished into care by their parents, due to social factors such as poverty, parental migration for work, the death of a parent, disability and HIV (Kamolsirisakul, 2012; Saini and Vichit-Vadakan, 2015). For many children who enter alternative care, the situation is that they are often placed in institutional care settings. Globally, there are estimates upwards of 2.7 million children growing up within institutions (Petrowski et al., 2017). This predominant use of institutions runs contrary to a body of research evidence that shows the negative impact institutional care can have on a child’s emotional, social, behavioural and educational development (Petrowski et al., 2017). Institutional forms of care have at different points in time been the predominant forms of provision in many countries across the globe. It is important to acknowledge that in relatively recent history even high-income countries, such as the United Kingdom, have relied on institutions to care for children and other vulnerable groups. The process of deinstitutionalisation in the United Kingdom has been a long journey, and indeed for some groups of children, for example those involved in the criminal justice system, institutional care provision remains. The social work profession plays a key role in child welfare systems around the world and has been at the centre of enacting deinstitutionalisation, for example, with practitioners involved in family strengthening, case management and the placement of children in alternative care. Social work academics have also been involved in researching alternative care across differing cultures and contexts aiming to influence policy and practice.
The existing research evidence that examines the outcomes of children growing up within institutions shows the negative impact this form of care can have, particularly on the developmental needs of infants (Carr et al., 2020; Dumais et al., 2014). We know from Bowlby’s (1951) and Ainsworth’s (1964) seminal work on attachment in the United Kingdom about the benefits of consistent care, and the importance of developing nurturing bonds between an infant and a caregiver. Rutter (1998) highlighted how institutional forms of care in the Romanian context, with low staff to child ratios, have a detrimental effect on attachment and subsequently on a child’s development. In recent years, research reviews into alternative care have reinforced these seminal findings from the works of Bowlby, Ainsworth and Rutter. For example, Garcia Quiroga and Hamilton-Giachritsis (2016) undertook a systematic review of the literature on attachment and found that attachment security for children across alternative care was negatively affected but that the impact was greater for children in institutions.
Furthermore, Van IJzendoorn et al. (2008) undertook a review of the evidence, across 19 different countries, on institutionalised children’s IQ measures and found they had significantly lower results than their peers did in foster care, on average 20 points lower. Children’s physical growth, in terms of height, weight and head circumference, have also been found to be impaired (Van IJzendoorn et al., 2007). Moreover, Juffer and Van IJzendoorn (2005) reviewed the evidence on the mental health of adult adoptees in the United States and found those who had spent time in institutional forms of alternative care had the highest rates of mental health difficulties. Van IJzendoorn et al. (2011: 30) also reviewed the international literature that focuses on the effects of institutional care on developmental delay and resilience; they reached the conclusion that ‘the institutional setting itself is in most cases pathogenic and should be classified as a type of child maltreatment, particularly in the form of structural neglect’.
While the research evidence suggests that institutional care is detrimental to child development, it is important to recognise the limitations of applying evidence and universal concepts of child development and need, across different cultures and political economies (Williams and Rogers, 2016). Furthermore, recent studies provide a more nuanced account of children’s experiences of institutional care. For example, in some socio-political contexts, where families are experiencing challenges, such as forced displacement and/or extreme poverty, institutions provide families with an opportunity for their child’s basic needs to be met and can ensure children have access to health provision and education (Morantz and Heymann, 2010). Despite these institutions ensuring that children’s basic needs are met, they often achieve this by separating children from their families and communities. This results in the phenomenon of ‘paper orphans’ (Van Doore, 2016), whereby children are placed into an institution despite having parents and family nearby. This process may ensure that needs are met during childhood, but this is often at the expense of severing connections with their family and disrupting social networks, which could have served as vital support across the life cycle.
Deinstitutionalisation as a wicked problem
In 2009, the United Nations (UN) published guidelines for the provision of alternative care (United Nations General Assembly [UNGA], 2009). The guidelines cite the extant research evidence that focuses on developmental outcomes and call on member states to avoid the use of institutional care, particularly for children under the age of 3. The UN guidelines promote family-strengthening approaches that aim to reduce the ‘necessity’ of alternative care. Furthermore, they highlight where alternative care is needed: it should be in a suitable form of provision, for example in family- and community-based care settings. These guidelines have led to an increased number of countries developing policies to implement deinstitutionalisation, which has often been supported by international non-governmental organisations (NGOs), such as Lumos, Hope and Homes for Children and The Martin James Foundation. However, responses across UN member states have differed widely. For some countries, deinstitutionalisation is occurring at a rapid rate and on a large scale, and many children have been moved from institutions back to their own families or to substitute families. For example, in Rwanda, a sustained process of deinstitutionalisation since 2012 has resulted in a 75 percent reduction of children in institutional care (Milligan et al., 2017) However, for many other countries, nearly 10 years after the publication of the UN guidelines, processes of deinstitutionalisation have been slower, and in fact in some places, for example Uganda, the use of institutions has grown (Riley, 2012). Accordingly, in some countries it seems that the deinstitutionalisation of alternative care is a challenging and complex policy problem.
Policy problems such as this have previously been conceptualised as ‘wicked problems’ (Australian Public Service Commission [APSC], 2007). Head (2008) explains that the use of the word wicked in a policy context is not to suggest the problem is in some way evil, but to highlight that it is wicked in its complexity and thus challenging to find a resolution. Wicked problems have been characterised as malign, vicious, tricky and aggressive, with no single solution. The concept originated in the field of design, as a way to highlight where complex problems arise in the design of a product, which prove challenging to overcome (Rittel and Webber, 1973). This concept has subsequently been applied to the analysis of social policies to describe complexity. In this article, we apply the ‘wicked problem’ concept as an analytical tool to explore the complexity that states may face in implementing the UN guidelines on alternative care and achieving deinstitutionalisation. The concept has been criticised for conceptual stretch and because it is difficult to delineate and define a wicked problem. However, Danken et al. (2016: 18) reviewed 106 articles that used the concept, and despite it being used across a range of disciplines there were three core properties that emerged: (1) wicked problems resist a clear solution, and they tend to become chronic; (2) the management of wicked problems involves a multitude of stakeholders with typically diverging values and interests; and finally, (3) wicked problems defy full understanding and definition of their nature and implications.
Case study: Thailand
The study draws on qualitative data from 27 interviews with practitioners and policy actors who are involved in alternative care provision in Thailand. Thailand is a particularly important case study as it is a middle-income country that has been described as ‘one of the great development success stories’ (World Bank, 2018). In recent years, the government has also developed policies that have prioritised child welfare and child rights. Thailand was the first country in South East Asia to sign the UN Convention on the Rights of the Child and they have made significant progress regarding the Millennium Development Goals (MDGs; Vapattanawong et al., 2007). For example, Thai children are generally experiencing better outcomes, across health and education, than their regional neighbours Vietnam, Cambodia and Myanmar (Save the Children, 2017). In the past 30 years, literacy rates have risen from 60 to 98 percent (United Nations Educational, Scientific and Cultural Organisation [UNESCO], 2017) and infant mortality rates have also improved significantly (World Bank, 2017). However, significant challenges remain, and children are still vulnerable to trafficking and exploitation, particularly the many children who have migrated and who are undocumented (Tang et al., 2017). Thailand’s alternative care provision for children is predominantly institutional, with orphanages and boarding schools accounting for nearly 95 percent of placements (Saini and Vichit-Vadakan, 2015). Administrative data on the breakdown of these facilities are limited, particularly as many providers are not licensed and operate outside of the regulations; however, care is provided by a mixed economy of care, including state-run orphanages and NGO-run orphanages/residential schools. Thai governments have made attempts over the past 25 years to shift to family-based care (Kamolsirisakul, 2012; Saini and Vichit-Vadakan, 2015). However, despite these attempts, there are only an estimated 300 children in state-run foster family placements (Saini and Vichit-Vadakan, 2015). Accordingly, deinstitutionalisation in Thailand presents as a complex, potentially wicked, policy challenge. Although the Thai context of this project will mean the lessons learned for policy and practice are of most use in Thailand, these may also be applicable in other countries, particularly in South East Asia. However, one of the key lessons from this Thailand-specific study is that deinstitutionalisation strategies need to be tailored to the individual contexts and cultures of countries.
Why focus on policy actors and practitioners?
According to Danken et al. (2016), one of the key aspects of a ‘wicked problem’ is that the key stakeholders, who have a role in solving the issue, often seem to play a role in sustaining it. Therefore, this study explores practitioner and policy actors’ perceptions as they are key stakeholders in the Thai alternative care system. Furthermore, the existing literature that explores alternative care includes limited accounts of these stakeholders, which is a significant omission as they are central to its provision and have the potential to influence policy.
The study aimed to explore alternative care in Thailand and consider deinstitutionalisation through the analytical lens of wicked problems. It is framed by the following research questions: (1) How do the participants perceive the alternative care system in Thailand? (2) What are the practitioners’ and policy actors’ understandings of the current challenges and opportunities in the provision of alternative care in Thailand? (3) Can the process of deinstitutionalisation in Thailand be considered a wicked problem?
Methods
The study adopted a qualitative methodology to gain in-depth understanding of the participants’ perceptions and views. Semi-structured interviews were used to collect data. The interviews were conducted by a sole researcher who is a social work academic from the United Kingdom. The analysis of the data and the writing of this article are the results of a collaboration that included academics based at a University in Thailand. This cross-cultural research team ensured that the study attended to cultural nuances, which minimised the risk of uncritically applying knowledge from one international context to another (Thoburn, 2007).
A purposive sampling approach was taken, whereby we included participants who were directly involved in alternative care provision. They reflected the diverse system of care which is both regulated and unregulated, formal and informal. For example, the practitioners were predominantly trained for social work and were working across NGO and state-run services; they were either alternative care providers or practitioners involved in placing/monitoring children in alternative care. The policy actors came from a range of government departments involved in child welfare, as well as actors who worked for inter-governmental organisations and colleagues working for international NGOs who campaign for policy change. The sample also included a participant from a foreign embassy who had knowledge of alternative care and had been working with colleagues in the Thai government on developing policy relating to international adoption from orphanages.
The approach to the recruitment of participants was initially through convenience sampling, from the networks of colleagues based at the university based in Bangkok. This then led to a snowballing approach, which recruited a total of 27 participants. Twelve practitioners worked for NGO providers and four worked for state-run child welfare services. The participants who worked for NGOs were all employed by services that were licensed by the state (Table 1).
Distribution of participants across the settings they work in.
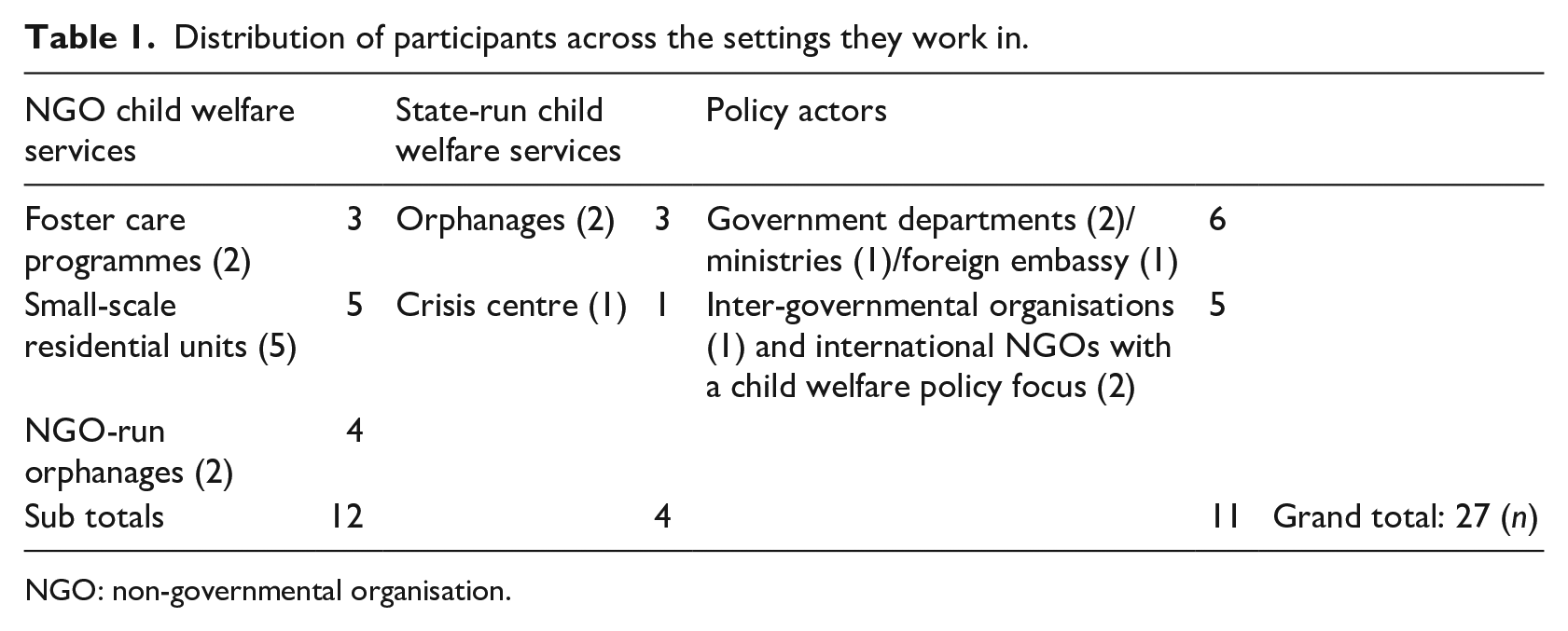
NGO: non-governmental organisation.
Ethical approval was provided by the University of Bath prior to the study commencing. All interviews were digitally recorded and then transcribed. The interviews were conducted in English; an interpreter was offered for people for whom English was their second language and three of the participants requested this. The interviews were transcribed in English. At the point of transcription, people’s names were replaced with pseudonyms and any other identifying information was fully anonymised. The transcripts are the source of data for this study and they were analysed using thematic analysis (Braun and Clarke, 2006). The transcripts were coded line by line and the codes were categorised under themes.
Findings
This section presents data relating to three key themes that emerged: (1) necessary institutions, a way to cope with demand; (2) NGOs, a magnet or a vital provision; and (3) disrupting family connections.
Institutions as a necessary way of responding with demand
Policy Actor P2: The demand is massive, that is the problem, if we didn’t have orphanages where are they going to go? We have to have these big institutions . . . I agree that smaller homes and foster families would be good, but the government only have limited resources. The economy is not that strong.
This quotation represents a view shared by all the participants who were employees of the government, both practitioners and policy actors. They felt the demand for alternative care was such that the use of institutions was necessary. This was in part informed by a belief that smaller group homes and foster care services are costly. Smaller scale provision and family-based care were seen as a luxury that the government could not afford. Institutions were also framed by these participants as providing a valuable service offering shelter and safety for children in a context where they may otherwise have been living on the street: Policy Actor P12: You have to remember, they are literally keeping children off of the streets. Ten, twenty years ago you would find many, many children living homeless on the street, this has stopped.
There were also views expressed by participants, across the sample, that any shift from institutional care to family-based care would come up against a challenge in recruiting enough carers, and some participants felt this was due to cultural beliefs: Policy Actor P12: Family is really important in Thai culture, people are very proud of their families, normally if there are any problems with children in a family the grandparents and aunties step in to help. There are lots of children raised by their grandparents and aunts, but we don’t get involved in other people’s family business . . . I think that is why foster care is not big here, it’s not in our culture.
This challenge was keenly felt by a practitioner from an NGO involved in the implementation of foster care. They stated: Practitioner P5: People in Thailand love children you see it everywhere, children are loved, and Thai people are generally just really kind people who follow their Buddhist traditions. You would think that would mean lots of people would foster but let’s face it, it is hard and there are easier ways to make merit than foster someone else’s child!
However, it is also important to highlight the experiences of another participant, who has been involved in a project with a state-run orphanage that has led to the recruitment of around 100 foster carers in a city in the North of Thailand. They explained, Practitioner P22: We often get people show an interest after they see other people in their community doing it (foster caring). I think it shows these cultural beliefs can shift, when people see what it is, and understand what it is, they become interested.
Alongside, these views that relate to demand and capacity, some participants held the view that the care within state-run institutions was of a good standard. A government social worker explained that state orphanages were preferable to NGOs and foster care programmes, as standards were in place and they were monitored: Practitioner P11: I would place a child in a state orphanage over an NGO or foster care . . . because I know they are of a good standard and unlike the NGO’s they are checked by the government.
This is in the context of extensive use of NGO alternative care provision, which remains largely unregulated (Saini and Vichit-Vadakan, 2015). However, despite the standards in place within state-run institutions, other participants highlight the challenges they face with low staff to children ratios: Practitioner P24: For the most part these institutions (state orphanages) have really caring staff and they are nice clean environments with lots of donated toys and food from local people. The kids’ basic needs are well met. But this is large scale childcare on an industrial scale . . . It’s the staffing numbers that are a challenge . . . One boarding school I visited had fifty-six kids in a dorm with two members of staff. With what we know about the importance of attachment, this has such a negative impact on their development.
One of the participants interviewed was a manager in a state-run orphanage and they explained the staff to child ratios in the baby unit, where the children were all under the age of 12 months:
What are the staff to child ratios in the baby unit?
We always have at least two members of staff during the day.
How many children are in there at the moment?
24 we never have more than 30 in there.
NGOs, a magnet or a vital provision?
The orphanages of both NGOs and state-run organisations are often supported by charitable donations, and it is common for Thai people to donate generously to the orphanages. This philanthropic motivation is often underpinned by religious beliefs and it is seen in Buddhist traditions as a way to ‘make merit’. For some, this philanthropy can go beyond donating to an orphanage and can involve setting up an NGO to directly provide care for children. Data from the transcripts suggest that there is a tension in how both practitioners and policy actors view alternative care provided by NGOs. These tensions were present in the accounts of participants regardless of whether they worked for a governmental agency or a non-governmental agency. The tensions centred on whether NGOs served as a vital provision for children in need or whether they acted as a magnet that promoted dependency and encouraged people to relinquish the care of their children: Practitioner P16: For poor people in the villages and the hill tribes, the NGOs here in Chiang Mai are seen as a place of opportunity, your kid gets educated, fed. When you are struggling, living in poverty, giving up your child and putting them in the orphanage, it’s a way to make sure they are looked after.
The unregulated nature of the NGO providers also concerned many of the participants. The absence of oversight of the sector raised concerns across the sample around ethical practice and the potential for exploitation: Practitioner P22: They are placed under private arrangements between the parents and the orphanage. This means the children without any legal guardian, and in some border provinces these can be the children of undocumented migrants, which means the children’s immigration status is uncertain too. It makes them very vulnerable especially if the NGO is unlicensed.
The participants also raised concerns about the competence and motivations of some foreigners in Thailand who set up foundations: Policy Actor P11: Some of these NGOs are well meaning, someone comes to Asia and falls in love with the place and they see that setting up a foundation is a way for them to stay here. Lots of them are religious too, so it fits with their beliefs. But often they don’t have any previous experience of working with kids . . . Another worry is the sustainability of some of their funding, I went to an NGO on my last field visit and a young German guy has set up an orphanage with his girlfriend, he is operating on a shoestring, basically on the good will of his church congregation back home. If it runs into difficulties what happens to the kids they have placed with them?
Despite these criticisms of NGO provision, data from the transcripts also show that a number are undertaking vital work supporting vulnerable children and families in crisis. The NGOs also operate in a policy and practice context, where there is limited regulation, and those involved in this study showed that they were aware of the tensions between support and dependence and demonstrated ways in which they were attempting to practice in an ethical way: Practitioner P16: We are really mindful of this, we don’t want people to be dependent on orphanages, especially when the kids are not really orphans and they have families . . . we have started respite services so one of our projects now focuses on caring for children whose parents have gone into prison.
The following participant from a licensed residential unit explained how some NGOs work outside of the state’s regulation and described the ways they were working in partnership with the state. They were also showing an awareness of the need to develop services that aimed to support families: Practitioner P5: Some NGOs take in the children directly from families, that is how the places without licenses operate. But we only get children placed with us from the state orphanage . . . we have a good relationship with the child welfare department. They come to us . . . We only have children with disabilities, they like to use us, its stops children going to Bangkok and keeps them close to family . . . The vision for our service in the future is to just offer a day service and respite care so the children can remain in their families.
Disrupting family connections
The use of informal kinship care (placements arrange by families) in Thailand is a widespread practice; however, formal kinship care (placements arranged and supported by the state) has a funding ceiling. The state provides funding for a maximum of 5000 kinship carers per year. Some participants, both policy actors and practitioners, felt this ceiling limited support to kinship carers: Policy Actor P26: Some grandparents go without any financial support, when they can really do with some help.
Another participant highlights how children living with grandparents can be vulnerable to entering alternative care if the grandparents are experiencing financial difficulties: Policy Actor P13: Migration is a big factor, so parents move to the city for work and leave the child with grandparents. For the parents work in the city is long hours and the minimum wage is low, so for some parents sending money back to care for the child often trumps going back to visit . . . Then as the grandparents get older they have no way of making money so they stop the child going to school because of the costs and send them to work and that is when children can get exploited or given up (to the orphanage).
Despite this funding limitation, data from the transcripts show that some practitioners on the ground were invoking their power to distribute what they receive from the government widely: Practitioner P2: We only get so much money for all the families (kinship carers), so we divide it up to make sure they all get something. It’s a smaller amount than they are supposed to get but we decided to try and give everyone something.
A practitioner from an NGO in the north of the country explained how the current alternative care system, which often moves children from region to region based on available places, can serve to disrupt family connections: Practitioner P16: With the state crisis shelters, they are nearly always full, a child from Isaan will probably end up in Bangkok, so even if the child isn’t initially abandoned permanently the chances of the family ever visiting the child again or making attempts to get them back is low . . . Poverty was the reason in the first place so having the money to go and visit in another part of the country, its not possible.
Another practitioner explained how families can then be forgotten and the possibility of reunification for children placed long term in alternative care is seldom explored: Practitioner P3: So when an institution loses touch with the families it means that they lose the possibility of ever reunifying the children with their families. No one goes back to see if things have changed and whether with support the child could go back. If they had better administrative systems they could follow these things up. At the moment everything is done on paper files . . . I am aware at our local state orphanage they had a go recently, each worker was given ten families to follow up, I think it was a hundred in total and after an assessment a good number of those children were actually able to go home.
The following excerpt from the transcript suggests that the children’s awareness of the reasons why they entered care is limited: Practitioner P8: I am not Thai but I have been living here for twenty five years and I have noticed in Thai culture people do not want to have difficult conversations with people, it comes from respect and I think it comes from really not wanting to hurt anybody’s feelings. So they avoid conversation that might cause any upset. I think that is part of the reason the children do not know why they are in the orphanage.
There is also little evidence of children having any contact with their family or any awareness of their family circumstances: Practitioner P10: A small number of the children here have contact with their parents, about ten of them (out of 135 children), but we limit it to once a year as it upsets them and upsets the other children who do not see their parents.
Discussion
The findings show the complex factors impacting on the alternative care provision in Thailand in this section, and each of the key themes is discussed in more detail with a focus on the challenges and opportunities.
Institutions as a necessary way of responding to demand
Most of the participants were aware of the UN Guidelines for the Alternative Care of Children and understood the global deinstitutionalisation agenda. Nevertheless, some justified the existence of institutions, and made the argument that there was a need for them, due to high demand and low resources. However, as Carter (2005) explains, resource arguments in favour of institutions are often based on assumptions and predicated on a false economy. Although, in the short term, there are increased costs when switching from institutional services to family and smaller scale provision, in the longer term once community-based alternatives are established they are more cost-effective (Carter, 2005). Carter calculated that institutional provision is on average twice as expensive as family-based care and eight times more expensive than preventive family support targeting vulnerable families. Therefore, aside from moral arguments that governments should value and invest in services for vulnerable children, there is a clear economic argument that is in favour of investing in the alternative care system. This investment could also negate future costs of supporting those leaving an alternative care system unprepared, which could leave them vulnerable to homelessness, involvement in criminal justice, and mental health services. Alongside the belief that institutions were necessary for economic reasons, several participants had faith in the state-run orphanages and believed that they were providing a good standard of care that provided safety, shelter and met basic needs. However, these beliefs about quality of care were contradicted in other participants’ accounts that highlighted low staffing ratios which they felt resulted in limited care and nurturing, which – as we know from the existing literature – can compromise the social, behavioural and developmental needs of children, particularly infants (Carr et al., 2020; Dumais et al., 2014). These two perceptions of institutional care that centre on its necessity and its perceived quality could serve as barriers to implementing deinstitutionalisation.
NGOs, a magnet or a vital provision?
Some participants were not entirely positive about the state-run orphanages and their perception of them could be understood as being the lesser of two evils. A number expressed greater concerns about care quality in the unregulated and unlicensed NGO providers. The participants were not only concerned about the suitability of the care provided, but also highlighted a need for standards of care and formal systems to inspect and monitor providers. This is important as the UN Guidelines for the Alternative Care of Children include a ‘suitability principle’ (Cantwell et al., 2012), which calls on states to ensure the care provided is suitable for meeting the children’s needs.
Some of the participants concerns around unlicensed NGOs not only centred on the perceived lack of monitoring and of oversight of care quality, but also on questions of ethical practice. For example, participants were concerned about the private arrangements made between the parent and the NGO at the point of placement, which in some cases had little to no oversight from the state. This is an important finding and highlights a need for social work and the development of case management where family assessments are undertaken at the point of entry. An assessment could have the potential to identify needs, and for a plan to be developed that provides support, which could enable a child to remain within their family and avoid being institutionalised. This approach would serve to strengthen families and ensure that NGOs were not ‘acting as magnets’, as some of the participants suggested. This magnet effect is important to consider in light of Van Doore’s assertion that the increase in ‘paper orphans’ can be considered in some cases as a form of child trafficking. The UN Guidelines for the Alternative Care of Children also introduced the ‘necessity principle’, and implementing this principle would offer a way to safeguard against exploitation, as this would ensure children only enter care when it is ‘genuinely needed’ (Cantwell et al., 2012: 22).
Disrupting family connections
The policy actors who were interviewed all highlighted the Thailand National Strategy 2017–2036 (National Economic and Social Development Board [NESDB], 2017) policy that aims to promote economic and social development, which includes plans for developing community childcare provision and early years support for families. This strategy does not mention alternative care, but it was framed by the policy actors as a way of strengthening families with the aim to stop entry to care. However, the participants with practice experience described several ways the current alternative care system served to do the opposite and disrupt family connections. The data in this study that highlighted the barriers to supporting kinship placements clearly illustrate this point. First, the number of kinship carers that receive financial support is capped, which serves as a potential limiting factor in the initial making of a kinship placement; second, in the longer term, a lack of finances was seen by some of the participants as a factor increasing the risk of grandparents relinquishing the children in the future.
Across the participants’ accounts, the importance of family strengthening was understood as a way to prevent entry to care and for family reunification. However, it was absent as a method to promote the wellbeing of the children and young people who remain in the alternative care system. Existing research shows that for children in care, an understanding of the reasons why they entered care and knowledge of their family and heritage could help as they develop their identity and sense of self (Watson et al., 2015). Rogers (2018) argues that in the absence of information, and connections to their past, children will develop their own understandings on an imagined level, whereas with practices such as supervised contact and life-story work (Watson et al., 2015) children can process their realities with the support of their carers and social workers. The promotion of contact could also enable children to maintain and build their social networks, which could lead to the possibility of reunification, or the option for young adults to connect with their kin when they transition out of the institution. There are potential lessons here for Thai social work practice around the need to consider developing contact and life-story work for children in alternative care. This would also be of importance to social work academics when training practitioners.
It is important to reinforce that the challenge of reforming alternative care in line with the UN guidelines is not unique to Thailand; it is a challenge for many other countries. Accordingly, there are lessons from these findings for social work as an international profession. This is particularly important if the profession’s commitment to social justice and human rights, at the core of the international definition (International Federation of Social Workers [IFSW], 2017), is to be upheld.
Conclusion
This aim of this article was to explore the following research questions: (1) How do the participants perceive the alternative care system in Thailand? (2) What are the practitioners’ and policy actors’ understandings of the current challenges and opportunities in the provision of alternative care in Thailand? (3) Can the process of deinstitutionalisation in Thailand be considered a ‘wicked problem’?
The participants perceived the alternative care system in Thailand as being able to meet the basic needs of children. They felt this was evidenced through a decrease in children living on the street and increased numbers of children being sheltered and safe. However, one of the current challenges is that the predominant placement option remains institutional, due to a lack of resources and large demand. Some participants felt the institutions run by the state were child-centred environments with caring staff; however, most acknowledged that the quality of care provided is impacted by low staffing ratios. Another challenge that emerged from the data in this study was the perception that some NGO orphanages acted as a magnet, bringing children into the alternative care system, which at times served to separate children from their parents and communities. There were, however, developments in alternative care provision that presented as opportunities and some participants were hopeful that the process of deinstitutionalisation would develop. For example, participants felt the implementation of foster care training in several state orphanages was positive, as well as the National Strategy policy that included family-strengthening measures. Both examples were perceived as a way to support children in families and reduce the need for institutions. However, the work to move children out of institutions into family-based care was focused on the government services, which fails to account for most of the children who are be being cared for by NGO providers. Therefore, it is important for future research to consider the extent to which alternative care is organised and delivered by the state and/or NGOs, as this will have implications for a deinstitutionalisation strategy.
In summary, findings highlight that the participants perceived significant challenges in the implementation of deinstitutionalisation. However, some also felt that progress has been made and that there was potential, hope and opportunity for change. Considering these findings, it is difficult to state whether the process of deinstitutionalisation in Thailand can be considered to be a definitively ‘wicked problem’ to solve. It is certainly a complex policy problem with multiple stakeholders, and areas of policy and practice that need development in order to make progress. If we refer to Rittel and Weber’s (1973) original definition of the concept where they state design problems can range from ‘tame to wicked’, the participants’ accounts would suggest an issue that was certainly further towards the wicked end of the spectrum than the tame one. However, regardless of how the issue is conceptualised when considering the numbers of children who are growing up without the care and support of a family, it is evident that in Thailand, and many other countries experiencing challenges in implementing the UN guidelines, there is a need for specific practice and policy responses that focus on deinstitutionalisation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by a Researcher Links grant, ID 2017-RLTG8-10500, under the Thailand Newton Fund partnership. The grant is funded by the UK Department for Business, Energy and Industrial Strategy and delivered by the British Council. For further information, please visit www.newtonfund.ac.uk. The researchers also received funding from the Martin James Foundation. For further information, please visit ![]() .
.