
Abstract
This article looks at the influence strategies of actors involved in intersectoral collaborations set up during the COVID-19 pandemic to influence collective decisions. It is part of a participatory research project that sets out to analyze the emergence and implementation of intersectoral initiatives between the community and public services during COVID-19 to better meet the needs of refugees, asylum seekers and non-status migrants in Montreal and Sherbrooke. The data analyzed in this case study were collected from 28 front-line workers and managers in the health sector (8), the community (19) and another public sector (1). The results show that the actors involved in collaborations mobilized two types of strategies—intersectoral and intra-sectoral—to influence collective decisions. On the whole, the strategies developed in times of crisis are more or less the same as those used in non-crisis periods. The difference lies in the mechanisms (context, sources of power) on which they are based. Most of the influence strategies deployed during the pandemic were based on the context of urgency and turbulence in which collaboration took place. This study documents how intersectoral collaborations work in the context of crisis, making an important contribution to the theory and practice of intersectoral collaborations.
In a crisis context, intersectoral collaboration is strengthened by the pooling of resources and the management of organizational interests through compromise. Public managers must promote transparency, institutional openness and dialogue to reconcile collective and organizational interests. These practices foster partner engagement, prevent strategic withdrawals and maximize the impact of joint actions, while preparing actors to work together more effectively in future crises.
Keywords
General introduction
Intersectoral collaboration is widely recognized as a strategic lever for improving population health. The COVID-19 pandemic once again highlighted its importance in delivering health outcomes (Borvil and Gautier, 2022). The World Health Organization recommended a joint mobilization of the public, private and voluntary sectors to limit the spread of the virus and protect vulnerable groups, particularly migrants, as the group most at risk from the consequences of COVID-19. This recommendation led to the implementation of intersectoral initiatives at various levels of governance.
Intersectoral collaboration refers to interaction between actors from the “order-sectors” (state/public, private for-profit, private non-profit) and the “field-sectors” (health, community, school, etc.), with a view to achieving common goals. It is based on the synergy of resources, mutual adjustment and adapted coordination (Divay et al., 2013). Although its effectiveness has yet to be demonstrated (Potvin, 2012), many studies have identified context as one of its success factors (Calancie et al., 2021). Prior to the pandemic, intersectoral collaboration took place in relatively stable and predictable contexts. On the other hand, COVID-19 introduced a turbulent context, marked by unpredictability and uncertainty (Ansell et al., 2021); this significantly affected its operation in terms of speed, and the increased number and complexity of collective decisions (Biddell et al., 2022; Hamel et al., 2022; Richard et al., 2021). Considering that actor strategies shed light on collaborative dynamics in a crisis context (Foss, 2020), this study aims to analyze the strategies mobilized in the intersectoral initiatives implemented during the COVID-19 pandemic. This work stems from research into the responsiveness of intersectoral collaborations in times of pandemic (Gautier et al., 2023).
State of the art
As a multi-disciplinary concept, influence strategies draw on several disciplines. In management science and public administration, strategies are seen either as a process of planning and positioning on the market (Mainardes et al., 2014), or as a social practice (Jarzabkowski et al., 2007), where actors act in a given context, with limited resources and institutional constraints. In organizational sociology, they are conceived as a form of relational power in which actors use different types of resources to influence collective dynamics (Crozier & Friedberg, 1977). In public health, strategies are recognized as procedures for implementing public policies and actions (e.g. Health in All Policies) and for furthering health objectives in complex environments (Molnar et al., 2016; Ollila, 2011).
In this article, we adopt Jarzabkowski's (2007) definition, which presents them as an activity of actors involving interactions, negotiations and concrete actions in a given context. Strategies are thus understood as a dynamic practice, influenced by social relationships, institutional constraints and individual or collective objectives. With this in mind, by influence strategies we mean any intentional actions or decisions aimed at guiding collective decisions, taking into account organizational interests and the collaborative group (Borvil et al., 2022).
Empirical studies show that stakeholder strategies can facilitate or hinder the success of intersectoral collaborations (Nederhand et al., 2019; Sullivan et al., 2006). Nevertheless, this concept is under-explored in the literature on intersectoral collaboration (Molnar et al., 2016; Sullivan et al., 2006). A few empirical studies demonstrate how actor strategies shape the outcomes of intersectoral collaborations (Borvil et al., 2022; Ege et al., 2021; Molnar et al., 2016; Nederhand et al., 2019; Sullivan et al., 2006). Previous research suggests that the actors involved in these collaborations must reconcile the interests of their organization with collective interests (Benoît-Barné and Robichaud, 2021). Influencing strategies are an essential means of aligning these interests (Borvil et al., 2022) and minimizing the negative outcomes of collaborations (Panneer et al., 2021).
During the pandemic, research focused mainly on the responses provided by collaborations (Biddell et al., 2022; Kobashi et al., 2022; Latonen et al., 2023), the challenges encountered (Baril et al., 2022; Hamel et al., 2022; Richard et al., 2021), the roles and responsibilities of actors in managing the pandemic (Turner et al., 2022) and the lessons learned from collaborations (Direction régionale de santé publique de Montréal, 2021).
In the literature on crisis management, strategies have been analyzed mainly at the macro and meso levels, often from a governance or pandemic response management perspective (Anderson and MacKinnon, 2023; Diaz-Castro et al., 2023; Jing, 2021; Joyce, 2021; Kuhlmann, Hellström, et al., 2021; Pattyn et al., 2021; Van Hecke et al., 2021). Some politicians used the crisis to advance their agenda, influencing responses to the crisis to their advantage (Jing, 2021; Kuhlmann, Bouckaert, et al., 2021; Pattyn et al., 2021) and the perception of citizens (Pattyn et al., 2021). The study presented here adopts a different approach by focusing on the influence strategies developed at the micro level, as part of the intersectoral collaborations set up during the COVID-19 pandemic to respond to the needs of new arrivals to Montreal and Sherbrooke, two cities with a high concentration of migrants, particularly refugees and asylum seekers.
Theoretical framework
To identify the influence strategies mobilized by actors involved in intersectoral collaborations, we adopted the strategic analysis of Crozier and Friedberg (1977), based on the relationships between actors in a collective action. The authors postulate that, in collective action, actors mobilized for a common project make choices from among a set of possible actions to achieve their objectives. These choices are made according to the interests they represent. In other words, organizational or collective interests are what “incite” actors to develop strategies to influence collective decisions. In other words, actors can mobilize different strategies depending on the type of interests they are defending.
However, in collective action, actors are not totally free. They have to contend with certain “uncertainties” which give them a power that is not linked to the actors, but to the resources (authority, expertise, financial, material, etc.) at their disposal (Martin, 2012). According to Crozier and Friedberg (1977), these resources are sources of power that provide actors with opportunities for action, and on which strategies are based. These sources of power can be used by actors to maximize their personal interests (Crozier and Friedberg, 1977) or to further the collective interest (Purdy, 2012) depending on the circumstances. As a result, actors’ strategies evolve according to the constraints and resources they have acquired, and the other strategies at play. Finally, since collective action always takes place in a particular context, actors’ strategies always depend on the context in which they are deployed (Rouleau, 2011).
Methodology
This study is part of a participatory research project that was rolled out in four phases. The aim of this project—a multi-case study—was to analyze the emergence and implementation of intersectoral initiatives between the community and public services during COVID-19 in two Canadian provinces, Ontario (Toronto) and Quebec (Montreal and Sherbrooke), to better meet the needs of refugees, asylum seekers and non-status migrants. One of the specific aims of the project was to examine the challenges of implementing selected intersectoral initiatives in times of crisis, from the point of view of front-line actors and decision-makers. With this in mind, we analyze the strategies of the actors involved in intersectoral collaborations in Montreal and Sherbrooke. The project was approved by the Centre intégré universitaire de santé et de services sociaux (CIUSSS)—Centre-Sud-de-l’île-de-Montréal (CSMTL) Research Ethics Board (REB) and by the Comité d’éthique de la recherche en sciences et en santé (CERSES) for Montreal and Sherbrooke. The selected initiatives, which are considered as cases, were chosen through a deliberative process during the first phase of the project. The entire initiative selection process is described in Gautier et al. (2023). The selected initiatives are described here.
This exploratory study identifies the influence strategies of actors involved in intersectoral collaboration during COVID-19 in Montreal and Sherbrooke. Initially, we wanted to focus solely on the collaborative bodies of the initiatives selected in the first phase of the project, in order to identify the influence strategies of the actors involved. However, during data collection and processing, we realized that respondents had also participated in initiatives that had not been selected and/or identified by the research team, despite multiple calls for contributions. We also noted a certain bias in the responses. For example, several respondents could no longer remember exactly in which collaboration forum they had taken a particular action. In view of these limitations, we decided to extend our sample to all collaborative bodies set up during COVID-19 and in which the interviewees had been involved in both cities.
Our respondents (front-line community workers, professionals and managers) were interviewed in semi-structured individual interviews. The interview guide is available on request. Interviews lasting approximately 90 minutes were conducted between summer and fall 2022 by research assistants, including the first author of this paper. Respondents were asked to comment, among other things, on the actions they had taken and the decisions they had made during their involvement in collaborations to influence collective decisions. Respondents came from the community (19), healthcare (8) and other public sectors (1).
Twenty-eight players were interviewed (Table 1). Of these, 21 were involved in at least one collaborative body from start to finish. Seven actors were involved in at least one collaborative body during the pandemic.
Distribution of respondents.
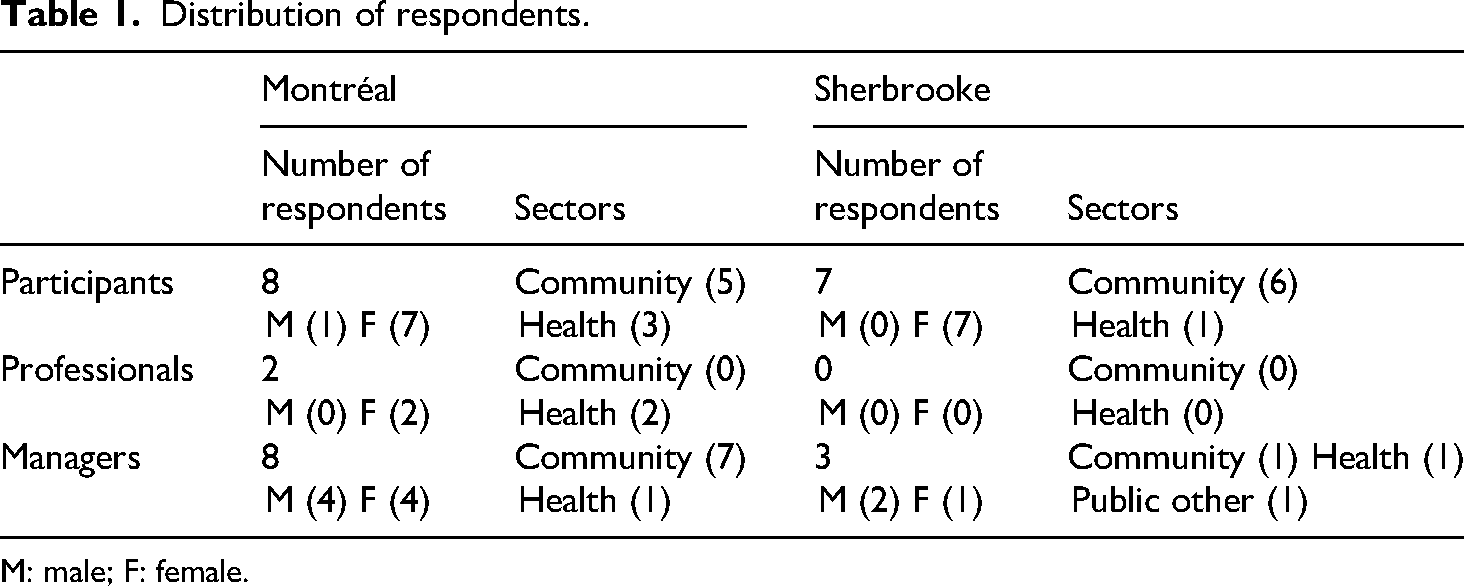
M: male; F: female.
Interviews were transcribed, anonymized and analyzed using QDA Miner software. We adopted conventional content analysis (Hsieh and Shannon, 2005) for an initial interpretation of the data (initial coding). We then carried out deductive coding based on the concepts of the theoretical framework (interests, strategies, sources of power, etc.). The list of codes has been grouped into sub-categories by axial coding, merging overlapping codes. Finally, we carried out a cross-sectional analysis to identify the main categories of strategies deployed.
Results
This section presents the interests, strategies and sources of power identified. Emerging terms are specified where necessary. The results are from an organizational perspective and do not reflect the individual characteristics of the respondents.
Interests reported
The actors reported three types of interest: collective, organizational and a combination of collective and organizational. Collective interests represent the objectives of the initiative around which the actors rally, whereas organizational interests refer to the objectives or priorities of the organization to which the actors involved in a collaboration belong.
Collective interests
Most respondents say they were involved in collaborations during COVID-19 to meet the needs of new arrivals in vulnerable situations (refugees, asylum seekers and non-status migrants). They felt that all the partners had a single objective and were working in the same direction to find solutions to the emerging problems in their community. Specifically, they say they wanted to help limit the spread of the SARS-CoV-2 virus, secure the well-being of their clients and ensure that they receive the information necessary to protect themselves, and take care of themselves and their families: It’s hard to answer because I think we had the same interests, which was to meet the needs of vulnerable populations, so we were all working in the same direction. [… I]t was more a question of seeing what we could do together to make things work for the communities. (P3_Intervenant.com.F_Verdun/Montréal)
Organizational interests
Depending on the results obtained, some players decided to sit on one or more collaborative bodies to better defend the interests of their parent organization. For them, the pandemic was an opportunity to promote their organization and increase its visibility in their neighborhoods, as shown in the quote below: In fact, as I said earlier, it’s part of our social role. In fact, as an organization, obviously, through [organization XXX], which promotes the program, it's clear that when we present our annual report, we refer to this collaboration, which gives [organization YYY] a certain visibility by saying [organization YYY] is a partner in the Sherbrooke community. (PGI.13_Gest.public.autre_H_Sherbrooke)
Collective and organizational interests
A significant number of the actors interviewed said they had taken part in collaborative bodies to defend both collective and organizational interests. Of these, some openly admitted that their organizational interests were perfectly consistent with those of the collective, and that it was easy for them to align the two: Yes, but the fact is that our organizational interest is really to make sure that we have, let's say our primary interest, our mandate, our mission is really to ensure that people from immigrant backgrounds, um, can access services. So that's what we want, and we’re doing everything we can to make it happen. (P07_Gest.Com.F_PEX/Montréal)
Influence strategies identified
Nine types of influence strategies are identified, grouped into two main categories: intersectoral strategies and intra-sectoral strategies. In this section, both categories are presented.
Intersectoral strategies
Intersectoral strategies include all decisions taken or actions implemented by consensus within collaborative bodies. Their aim is to ensure successful collaboration and the achievement of collective objectives, which are to meet the needs of people in vulnerable situations, in particular refugees, asylum seekers and non-status migrants. Intersectoral strategies include pooling, intersectoral compromises, negotiation, strategic alliances and mediation.
Pooling
Pooling mainly involved sharing human and material resources, information, and technical and logistical resources, as well as collective brainstorming to find solutions to problems specific to one or more members of the collaborative body. It was the most frequently used strategy. Indeed, all respondents, including those who openly stated that they had chosen to get involved to defend their organizational interests, mentioned that they had made use of pooling as part of their involvement in collaborative bodies. They explained that, in the context of a health emergency marked by the powerlessness of institutions and organizations, pooling had proved to be a necessity. Community actors reported that pooling even facilitated access to resources for their clients: Right from the start, it was done in a very collaborative way … we developed collaborative tools, we used Google Drive a lot […] But that was the goal, the whole point was for us all to be equals, then to do it all together. […] You know, we really put ourselves [at the service of others] because the goal is to support the members of the [working] committees. (P5_Gest.Com.F_NIM/Montréal)
Intersectoral compromises
Intersectoral compromises are those made between actors within collaborative bodies. They include all arrangements made by mutual agreement to achieve collective interests. The results revealed that in both cities (Montreal and Sherbrooke) community organizations (COs) were more inclined to compromise in order to meet certain CIUSSS demands. For example, health and social services organizations had asked community organizations to promote vaccination among their clients. Initially opposed to this approach, which they considered incompatible with their own, they finally agreed, after discussion, to go door-to-door to inform families of the existence of vaccines.
Negotiation
Respondents said they had used negotiation as a strategy to achieve common goals. Negotiation strategies consisted of attentive listening, openness and transparency. Listening and openness helped to reduce tensions resulting from diverse interests, and to better reconcile organizational and collective interests in some cases. Community players emphasized the openness of institutional players during the pandemic. This openness “opened doors that had been closed for too long”. For example, health and community organizations negotiated awareness-raising materials, including poster formats, developed by the health sector's communications department. Through exchanges, they expressed their respective needs and concerns. They agreed to adapt the media to clarify the messages and make them more accessible to vulnerable populations. Plus, there's this ability to be transparent and say why we can do things or why we can’t do them. It leads to better collaboration because people understand […] I think that openness and transparency are what made it possible to work better […] then the urgency of the situation, the desire to be on the same wavelength, for everything to go in the same direction. I’m talking about a common will. (P11_Intervenor.Pub_F_PEX/Montréal)
Strategic alliances
The majority of respondents felt that strategic alliances were not necessary during the pandemic, as “all players had the same interests”. However, public health actors claim to have forged alliances with community organizations. These involved supporting and accompanying them in the collaborative process, lobbying to ensure that the particular needs of migrants were taken into account, and raising awareness among other partners of the need to include them in the collaborative process so that they could participate in collective decisions.
Mediation
In Montreal, Montreal public health actors (e.g. public health professionals and community organizers from CIUSSS) acted as mediators to facilitate collaboration between institutional-level players and community organizations. The main aim of mediation was to advocate on behalf of low-resource community organizations, to ensure that their interests were not prejudiced, and to facilitate the implementation of “small initiatives” to reach their migrant clients. In Sherbrooke, mediation was used by community development officers to ensure the well-being of certain community workers and to facilitate communication between certain community organizations (high-resource versus low-resource COs) on the one hand, and between community organizations and public institutions (CIUSSS, school, city) on the other: I made a lot of calls after the informal discussion meetings, debriefings after these meetings to see what it generated, how we could work better together, how we could do better so that our efforts meet our own need, meet their need, so that we understand their reality, and, in turn, that they also understand our reality. I was very much involved in these spaces of mediation. (PGI17.Gest.com.F_Sherbrooke)
Intra-sectoral strategies
Intra-sectoral strategies include all actions or decisions taken by actors within their home organization with a view to collaborating constructively with the group while representing the interests of their organization. Intra-sectoral strategies include internal compromises, leadership, involvement in working committees and temporary withdrawal.
Internal compromises
In terms of internally developed compromises, the actors interviewed said they had temporarily modified their organization's mandate and the tasks of employees at all levels. These internal compromise strategies were reported mainly by actors from community organizations. As for the institutional actors, they claim that their superiors had temporarily modified certain internal rules that could have slowed down the collaboration process. They also showed flexibility with regard to their institutional boundaries. For example, the CIUSSS agreed to modify their internal communication rules so as not to slow down the collective process.
Some actors mentioned that they had been forced in some cases to prioritize COVID projects to the detriment of their usual projects. They explained that their involvement in consultative bodies was so demanding and time- and energy-consuming that they had no choice but to devote themselves to it full-time. Some also reported working overtime to coordinate field work and better support collaboration.
Leadership and involvement in working committees
Taking the lead in collaborative bodies and sitting on working committees are among the intra-sectoral strategies identified. A number of actors revealed that they had decided to take a leadership role in coordinating the implementation of COVID initiatives, in order to better influence collective decisions. Some said it was an effective way to ensure their organization's visibility, or to promote it. For others, it meant being better informed, getting an overall picture of what was being done in the field and better positioning their organization for the future. A minority of actors felt that getting involved in working committees increased their ability to better represent their organization.
Another strategy that emerged from the data is “temporary withdrawal”. It was mentioned by a community respondent who saw themselves as one of the key actors in a collaborative body. The respondent explained that, during the collaborative process, they had chosen not to take part in decisions that would commit their organization and with which they totally disagreed.
Sources of power and strategies of influence
Identified sources of power
Analysis of the data reveals that the actors involved in the collaborations studied had five sources of power (Table 2) which they could use to influence collective decisions. These include formal and informal authority, expertise, and human, financial and material resources. Formal authority is linked to the characteristics and organizational identity of the actors who hold it (health). Informal authority is indirect; that is, it is conferred by the other partners and is conditional on other sources of provision such as expertise (actors specialized in the reception and integration of migrants) or funding (philanthropy). As Table 2 shows, all the actors held some source of power in the collaborations. However, the intensity of power varied from one sector to another, and depended on the importance of the stakes involved in the resources held. Authority and expertise were mentioned most often by respondents. Actors in the healthcare sector and organizations with expertise in the reception and integration of migrants controlled the two most important sources of power, those inherent in authority and expertise.
Actors’ power sources.
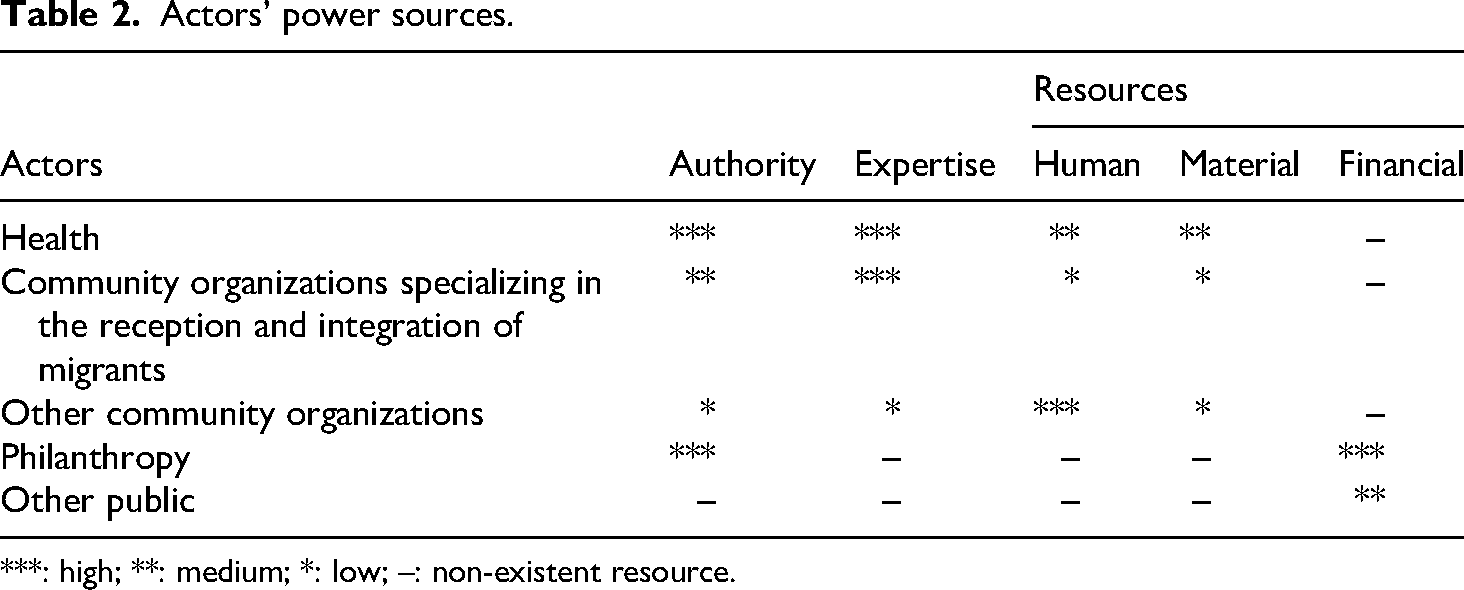
***: high; **: medium; *: low; –: non-existent resource.
Sources of power and strategies of influence
The vast majority of respondents said they had neither felt nor observed any use of a source of power by the best-positioned actors for the sole purpose of benefiting from decisions. The financial resources generally recognized as the most important source of power were not mobilized by the funding partners to influence collective decisions. According to the respondents, the context did not allow those with power to exercise it in the interests of their organization, because the collective stakes were too high: “I was just going to say that sometimes in collective approaches, there are little power struggles and … I didn’t feel that at all in this case” (P5_Intervenant.Pub_H_CDN/Montréal).
However, as can be seen from the quote below, the health sector had mobilized (formal) authority and legitimacy to take control of certain initiatives and impose their way of doing things. This observation was made, to varying degrees, in both cities: For example, we were working on creating communication tools. But at the same time, the healthcare network wanted to create its own network. What's more, the directive was such that it was as if, automatically, everywhere I talked about it, about leadership, at some point, the healthcare network came along and wanted to take back its leadership role. It's a public health issue, so it's the healthcare network that has to take initiatives, that has to be at the forefront, that has to be involved in every struggle, and that's reflected in the field. (PGI 2_Gest.com._H_Sherbrooke)
Discussion
Studies on the influence strategies of actors in intersectoral collaborations have highlighted their role in the functioning and success of collaborations. Different types of strategies have been identified from field studies. However, these studies were carried out in relatively stable socio-economic and political contexts. The aim of this article was to explore the influence strategies deployed by actors involved in intersectoral collaborations set up in unusual circumstances. The results show that two types of influencing strategies—intersectoral and intra-sectoral—had been mobilized by the actors to influence collective decisions. These two types of strategy differ in particular in terms of their objectives and the places where they are deployed. In fact, intersectoral strategies were deployed by consensus within the collaborative bodies to facilitate the success of the common goal. Intra-sectoral strategies, developed on a discretionary basis within the organizations to which they belonged, were aimed either at defending organizational interests or at reconciling organizational and collective interests. These results confirm assertions that during a process of intersectoral collaboration, actors deploy strategies both at the border of and within sectors to influence collective decisions to their advantage or otherwise (Borvil et al., 2022; Nederhand et al., 2019). Two facts in particular are worth mentioning. Firstly, all the actors emphasized the use of intersectoral strategies. Pooling remains the most frequently cited option for all categories of actors. The predominance of this strategy is linked to the fact that some collaborative bodies had set themselves the goal of supporting community organizations with few resources and which are close to the ground. Secondly, very few actors declared that they had mobilized intra-sectoral strategies solely to defend their organizational interests. This result could be explained by the fact that some respondents had not been directly involved in the collaborations, or were involved at different points in the collaborative process. However, the two categories of strategy are not totally independent of each other. In some cases, they were mobilized simultaneously to align organizational and collective interests.
The deployment of a strategy varies according to the type of interest defended by the actors. The data show that collective interests were prioritized by the actors during the collaboration process. Even those who confessed to having defended their own interests implied that they had been involved in the process to help achieve the common goal. In times of crisis, it was important for organizations to show selflessness, to relegate potentially contradictory objectives to the background and to converge their actions to meet collective expectations. This explains not only the overuse of intersectoral strategies such as pooling, but also the emergence of the third category of interest, which is a combination of collective and organizational interests. These results seem to confirm the popular belief that, in times of crisis, collective interests are prioritized to the detriment of organizational interests.
Moreover, as in all intersectoral collaborations, power relations were present in the collaborative bodies studied. However, it appears that the development of the vast majority of influence strategies was not dependent on the sources of power identified. Most respondents stated that the most powerful actors in terms of authority, expertise or financial resources had not used their power to influence collective decisions to their advantage due to the urgency of the crisis. In both cities, only the healthcare sector deployed power-based strategies. They felt they had the legitimacy to take the lead in public health initiatives, and this had an impact, among other things, on raising the profile of the community environment.
Conclusion
Our study presents important findings on the strategic behavior of actors involved in intersectoral collaborations during the pandemic. Overall, the data indicate that the cross- and intra-sectoral strategies developed in times of crisis, with the exception of pooling and temporary withdrawal, are virtually the same as those identified in a previous case study of an intersectoral initiative carried out in Montreal prior to the pandemic (Borvil et al., 2022). Pooling, which has always existed in embryonic form, was elevated to the status of an influence strategy during the pandemic, and was the one most used by actors to meet the new needs of vulnerable migrants brought about by the pandemic. As for the “temporary withdrawal” strategy, it illustrates the fact that, even in times of health crisis, actors are not prepared to sacrifice the interests of their organization for the collective good. The difference between intersectoral and intra-sectoral strategies before and during the pandemic lies in the role of the collaborative context and the way in which existing sources of power were used. Although most of the strategies deployed by actors during the pandemic were influenced by the emergency and turbulent context in which collaboration took place, those identified before the pandemic were linked primarily to the type of power available to the actors. As for the types of interests favored, both (organizational and collective) simultaneously governed the behavior of the actors during the collaboration. In theory, these results corroborate the role of context in the functioning and success of intersectoral collaborations.
This research has certain limitations. As in all retrospective studies, there is a possibility that the strategies identified may be limited due to certain cognitive biases. Indeed, during the interviews, respondents had some difficulty recalling all the actions they had taken one or even two years earlier. In addition, due to staff turnover, among other factors, we were unable to validate the strategies identified with respondents. We are aware that our analysis is based solely on what the respondents had to say; however, several studies carried out by our collaborators confirm some of the strategies we have identified, in particular “pooling” (Baril et al., 2022; Heck et al., 2022). Our findings on intra-organizational strategies corroborate other studies that have highlighted the importance of internal compromises (Béland et al., 2024) and leadership (Baril et al., 2022; Heck et al., 2022) in intersectoral collaboration processes at the local level during the pandemic. In conclusion, despite its limitations, this study, which is part of a larger research project, has the merit of documenting how intersectoral collaboration works in a crisis context. This represents an important contribution to the theory and practice of intersectoral collaboration. The results will be shared to inspire those working in the field. They will be invited to mobilize them to make informed choices and engage fully in intersectoral collaborations, in order to amplify their impact on communities.
The pandemic is not yet over, and further health crises are predicted by WHO (2023) for the coming years. What's more, in a context of budgetary restraint that will undoubtedly have repercussions on intersectoral collaborations (Mercier and Bernier, 2023), new knowledge about how actors interact in times of crisis would enable practitioners to be aware of their strategic behavior and better prepare to interact with their partners in order to maximize the results of collaborations in future crises.
Footnotes
Acknowledgments
We would like to thank Alfred Pierre for editing the latest version of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Canadian Institutes of Health Research (Research on Pandemic Preparedness and Health Emergencies priority announcement) (grant number PUU177961).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.