
Abstract
This article examines how the Post-New Public Management administrative model adopted by a teaching hospital in Portugal shapes innovation processes. We find that innovation is a multi-level organizational phenomenon that relies substantially on the interplay of three factors: (1) trust-based professional autonomy at the individual level; (2) an intra-organizational collaborative approach in innovation (re)design at the team level; and (3) staff involvement/commitment towards the hospital’s strategy in the implementation of innovations at the organizational level. Additionally, innovation is facilitated by interconnected formal and informal processes that mutually reinforce each other. The study contributes to the literature on innovation and administrative models by providing a nuanced understanding of how intra-organizational innovation processes take place within a Post-New Public Management model. As such, it is one of the first attempts to empirically analyse and link the administrative model of Post-New Public Management with innovation.
Points for practitioners
This research provides an account of how a Post-New Public Management administrative model can foster intra-organizational innovation through collaboration across different hierarchies and professions. The article also helps to better understand the role of organizational dynamics at individual, team and organizational levels on innovation, as well as how these can shape and be shaped by formal and informal processes.
Keywords
Introduction
Public sector reforms have been guided by administrative models, that is, ‘visions of what the substance of public management reform has been (or, in some cases, should be)’ (Pollitt and Bouckaert, 2011: viii). These models provide core ideas and guidance for management in the public sector. This also includes the scope and channelling of innovation processes (Hartley et al., 2013).
There is currently renewed scholarly interest in innovation in the public sector (De Vries et al., 2018). However, echoing Rashman et al. (2009) and Torfing and Triantafillou (2016), it remains so far largely unclear how innovation specifically unfolds in different administrative models. The recent innovation literature often looks at hybrid organizations, inter-organizational settings and the integration of stakeholders (Bekkers and Tummers, 2018; Osborne et al., 2016; Torfing, 2019; Van Eijk et al., 2019). Here, corresponding issues such as the role of innovation drivers, networking and leadership (Lewis et al., 2018), technology (Lember et al., 2018), or inter-organizational learning (Hartley and Rashman, 2018) are discussed. With this, however, current research has somewhat lost sight of the traditional processual perspective on innovation (Garud et al., 2013; Moore and Hartley, 2008), often targeting service-quality improvements (Damanpour, 2017).
Since the 1980s, reforms have mainly been underpinned by the models referred to as New Public Management (NPM) and Post-NPM 1 (Hood, 1991; Reiter and Klenk, 2019). While NPM envisioned increasing economic efficiency and results through innovation fostered by competition, Post-NPM focuses on advancing public value (such as social cohesion and enabling transparency) through innovation encouraged by the strengthening of collaborative governance (Bryson et al., 2014). In addition, as the main focus of these models is argued to be different, the relevance of performance dimensions is contingent on the adopted model (Bryson et al., 2014; Kuhlmann and Jäkel, 2013). For instance, key performance dimensions emphasized by NPM include efficiency and market competition (Diefenbach, 2009; Fattore et al., 2012). However, NPM reforms have been criticized for paying less attention to other performance dimensions, such as collaborative innovation and environmental performance, which are an integral part of Post-NPM reforms (Hartley et al., 2013). In this context, Bovaird (2008) states that Post-NPM performance dimensions should add value not only for the users of public services, but also for wider groups, including society, the environment and political stakeholders, with ramifications on how innovation unfolds.
Whereas the impact of NPM on performance has been substantially researched (Diefenbach, 2009; Smith, 1995), studies of these effects within a Post-NPM model, though growing (Reiter and Klenk, 2019), remain largely absent besides some rare attempts (see, for instance, Fattore et al., 2012). In particular, it remains unclear how innovation processes unfold within public organizations that rely on Post-NPM reforms (Torfing and Triantafillou, 2016). Drawing on a case study of a falls prevention group (FPG) at a public teaching hospital located in Portugal, the aim of the article is to theorize how Post-NPM shapes innovation processes.
Key findings highlight that innovation processes within a Post-NPM model rely substantially on the interplay of three factors: (1) staff involvement/commitment towards the hospital’s strategy in the implementation of innovations; (2) trust-based professional autonomy; and (3) an intra-organizational collaborative approach in innovation design. The remainder of this article is structured as follows. First, the next section reviews the literature on Post-NPM and how innovation is shaped according to the different administrative models. Second, the empirical design and methodology will be outlined, followed by the presentation of the findings from the case study. Finally, findings are discussed and conclusions are drawn.
Conceptual orientation
In order to understand how Post-NPM shapes innovation, this section reviews the literature on Post-NPM, its relationship to innovation and its contrasts with NPM given their linkages and the fact that the two are the most contemporary administrative models.
Post-NPM
Post-NPM can be identified as an attempt to challenge and modify the earlier NPM administrative model, which is argued to have resulted in partly undesirable consequences, such as an excessive emphasis on efficiency and overuse of the market for contracting public services (Christensen and Lægreid, 2007; Hartley et al., 2013). In addition, Torfing (2019) argues that the privileged role of public managers in NPM tends to neglect the importance of public employees. Notwithstanding a lack of general consensus among scholars of what Post-NPM entails (Reiter and Klenk, 2019), cross-sector collaboration, recentralization initiatives and a specific focus on outcomes (instead of outputs) are usually considered to be its characteristics (De Waele et al., 2015). Furthermore, Stoker (2006: 41) holds that in Post-NPM, the ‘state should steer society in new ways through the development of complex networks and to the rise of more bottom-up approaches to decision making’.
Within Post-NPM-steered organizations, public servants value collaboration through purposeful relational communication and an open-ended climate to reinforce the legitimacy of previously devolved institutions (Simmons and Birchall, 2005). Furthermore, public–private partnerships and cross-sectoral networks are incentivized to ensure participation, which blurs the organization’s boundaries (Hood, 1991). Post-NPM therefore refers to the trend of including a wider range of participants in decision-making processes for the reason that they are seen as legitimate members of these processes within contexts of considerable uncertainty and complexity (Hood, 1991). Finally, the organization’s objectives focus on outcomes by forming public values such as social cohesion and empowering transparency (Stoker, 2006). Outcomes in this respect refer to the accomplishments that have value for the organization and that are typically less quantifiable (Brown and Svenson, 1988).
Innovation and administrative models
Innovation can take various forms, ranging from continuous improvement (Bessant and Caffyn, 1997) to step-change transformations (Hartley et al., 2013). Following Torfing and Triantafillou (2016: 7, emphasis in original), our understanding of innovation is as ‘an intentional, yet inherently contingent, process that involves the development and realization of new and creative ideas that challenge conventional wisdoms and break with established practices in a particular context’ (see also Garud et al., 2013). Torfing and Triantafillou (2016) further identify how public sector administrative models can act as both drivers and barriers. Table 1 contrasts innovation in the NPM and Post-NPM administrative models, synthesizing aspects of the extant literature on the two topics.
Innovation in the NPM and Post-NPM administrative models.
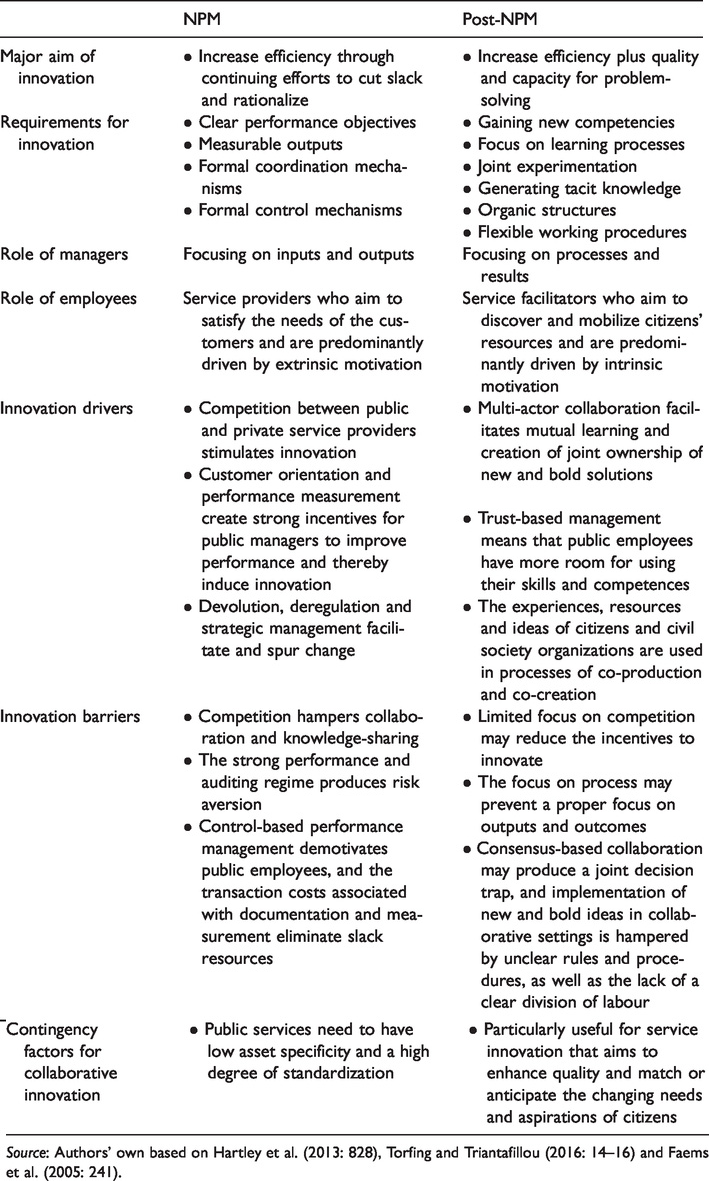
Source: Authors’ own based on Hartley et al. (2013: 828), Torfing and Triantafillou (2016: 14–16) and Faems et al. (2005: 241).
It can be argued that innovation is enabled by both NPM and Post-NPM, though with different foci. In his path-breaking work, Duncan (1976) identified exploitation and exploration as two strategies in innovation. While the former refers to ‘the refinement and extension of existing competencies, technologies, and paradigms’, the latter concept is defined as ‘experimentation with new alternatives’ (March, 1991: 71). In line with this, it can be argued that due to the key performance dimensions emphasized by NPM, this model has a propensity to mainly foster exploitation-type innovation as such innovation activities ‘benefit from clear performance objectives that are translated into measurable output controls’ (Faems et al., 2005: 241). On the other hand, post-NPM is more conducive to exploration-type innovation (i.e. ‘innovation embodying knowledge that is novel relative to the firm’s extant knowledge’ (Phelps, 2010: 980)) as this type of innovation emphasizes tacit and intangible knowledge exchange, requiring informal and personal modes of coordination and control in order to achieve ‘innovation projects that focus on novelty rather than efficiency’ (Faems et al., 2005: 241).
These arguments strongly resonate with prior findings from extant public administration literature. According to Hartley et al. (2013), innovation in NPM centres primarily on issues such as efficiency and using markets for innovation through competition. Examples of this are presented in the studies of Parker et al. (2000) on governmental agencies in Australia and Lubienski (2009) on education. Unlike NPM, Post-NPM emphasizes quality improvements and the capacity for public problem-solving through collaboration (De Waele et al., 2015; Torfing and Triantafillou, 2016).
The literature on innovation and administrative models identifies two main gaps. First, given the focus of contemporary research on the enabling conditions of innovation (e.g. Lewis et al., 2018), there is a lack of empirical studies regarding the underlying processes of innovation, as identified by Choi and Chandler (2015), Moore and Hartley (2008) and Torfing and Triantafillou (2016). Second, Bekkers and Tummers (2018) identify an important shift in public innovation literature from innovation being traditionally described as a matter of finding the necessary resources, to being considered today as the result of open processes of collaboration between stakeholders across various organizations. More precisely, Bekkers and Tummers (2018) refer to the relevance of how to activate stakeholders to join innovation processes, an idea that resonates well with Post-NPM (Bryson et al., 2014). Yet, it is contended that taking such an expanded concept of collaboration that emphasizes the role of public and private stakeholders (Barrutia and Echebarria, 2018), often in network-based collaborations (Torfing, 2019), and including users and citizens (Osborne et al., 2016), has downplayed the attention given to intra-organizational collaboration across different hierarchies and professions that continues to be relevant in Post-NPM. This article aims to address these two gaps.
Methodology
Research design
The findings of this study are based on an exploratory single case study for three reasons. First, this type of research is useful in providing a rich description of the complexities of a specific situation (Rossman and Rallis, 2003). Second, this research design is particularly suitable to answer research questions that focus on exploring the underlying processes of a given event (Baxter and Jack, 2008). Third, we aim to answer a research question that seeks to explain phenomena that are too complex for survey or experimental strategies (Yin, 2018).
Research setting
The study was conducted at an acute teaching hospital fully owned by the Portuguese National Health Service, purposively selected as it is known as one of the principal innovators regarding the quality of care provided. Ethics approval was obtained before the case study was carried out.
In the hospital, the quality of care provided has always been important. However, in 2000, following a change of board members, the focus on quality improvement became more formalized, leading to a series of initiatives, including the restructuring of the patient safety incidents reporting system around the year 2004/2005. A considerable number of reported falls spurred the formation of an FPG in 2006, a bottom-up initiative consisting of three members of the quality management department (QMD) and three nurses from the three clinical departments where most of the falls were occurring.
Data collection
In total, 46 in-depth face-to-face semi-structured interviews were conducted with 49 interviewees – 25 nurses, eight doctors, four nurse aides, three engineers, two administrative staff, two health and safety technicians, two managers, two social workers, and a laboratory technician – working in several clinical and non-clinical departments across the hospital. This would allow the obtaining of a more comprehensive picture of staff’s views on the hospital’s quality of care activities. Data were collected from August 2008 to February 2010. Data collection aimed at exploring the factors that led the hospital to establish the improvement of the quality of care as a strategic priority and the new projects it embarked on. A particular focus of the interview questions was the organizational dynamics associated with the FPG’s search, experimentation and/or invention of new alternative practices, as well as improvement of existing ones, including: who was involved and their roles; how the projects evolved; and the barriers to and facilitators of the process. Interviews were conducted in Portuguese and lasted 43 minutes on average. Interviewees were purposively identified using a snowball approach (Patton, 2002). The first author, who had previous work experience in another public hospital in Portugal, conducted the interviews until theoretical saturation was reached (Eisenhardt, 1989). In order to minimize social desirability bias, a series of strategies were adopted, including only providing interviewees with an overview of the study before the interview, rather than the interview guide, and telling interviewees that there were no right or wrong answers. Data obtained from interviews were supplemented by data from informal conversations, hospital documents, information about the hospital published in magazines and documents from the Portuguese Ministry of Health.
Data analysis
All interviews but two were audio-recorded and fully transcribed verbatim by the interviewer to ensure the quality of the transcripts. In the two cases where interviewees preferred not to be audio-recorded, extensive interview notes were taken. The original interview transcripts were inductively analysed following the method proposed by Braun and Clarke (2006). In a first step, the first author generated initial codes at the semantic level (using the wording of the interviewees). In a second step, the team of authors examined these initial codes from a more conceptual viewpoint and reduced them into themes. After reviewing these themes in a third step, the team defined and named three final themes (‘staff involvement/commitment towards the hospital’s strategy in the implementation of falls prevention innovations’, ‘trust-based professional autonomy’ and ‘intra-organizational collaboration as a source of innovation (re)design’). Although identified inductively, these themes are in line with the literature on innovation in the Post-NPM model, as summarized in Table 1, as well as with the wider management literature on innovation (e.g. Crossan and Apaydin, 2010; Damanpour, 2017, 2020), as later presented in the discussion and conclusion section. Quotes from the interviews were translated from Portuguese to English. In the following section, the findings are presented alongside these three themes, after an initial introduction of the FPG as an initiative underpinned by the Post-NPM model.
Findings
Innovation in the FPG underpinned by the Post-NPM model
Interview data evidence that since its creation, the FPG put in place a series of falls prevention innovations, involving significant improvements in existing practices or the exploration, experimentation and/or design of new alternative ones. Examples included: (1) conducting refurbishment works (e.g. the replacement of floor coverings and placing handrails in bathrooms); (2) the design of a novel incident reporting form exclusively for falls and the sensitization of staff regarding the importance of reporting falls and other incidents; (3) the creation and implementation of procedures to manage the physical environment surrounding the patient (e.g. substituting textile towels with paper towels in bathrooms to avoid patient falls); and (4) pioneering the implementation of the Morse Fall Scale (Morse et al., 1989), which allows the quantification of a patient’s risk of falling, in Portugal. The latter included its translation from English into Portuguese and the development and application of procedures to mitigate the patient’s risk, some of which were invented inside the case-study hospital (e.g. equipping high risk of fall patients with a pink wristband). As mentioned by a nurse: ‘falls have always been a matter of great concern to us because they could often cause serious injuries to patients, even death’. However, the falls prevention measures led to significant positive outcomes: ‘[with the falls prevention measures] while notifications continued increasing, the severity substantially decreased, with no deaths from falls in the past three years’ (FPG member).
The interviews also showed that Post-NPM is the administrative model underlying the hospital’s management, for example, as when interviewees highlighted key performance dimensions prevalent in Post-NPM (e.g. Reiter and Klenk, 2019). From the start, as pointed out by one of the group’s members, the objective of creating the FPG was not to reduce falls (in the sense of reducing the statistically known falls within the scope of a ‘tick-box exercise’ (Lapsley, 2009) – an output-centred measure, as emphasized by NPM), but rather to reduce the severity of falls (i.e. the impact of falls on patients) and to reduce second falls as falling patients often had a propensity to fall again (an outcome-based performance perspective, as suggested by Post-NPM). An interviewee explained this as follows: No, the objective was not to reduce falls because falls will always exist. The objective was to reduce the severity of falls. As a matter of fact, [since] we implemented falls reporting, the number of falls has always been increasing and that is important because people feel safe in reporting and are not afraid of reporting. So, it starts to be real. When few falls were reported, that meant that people were not reporting. (FPG member) For example, if I, in quotation marks, ‘invented’, if I create a certain procedure that doesn’t exist anywhere else … and if other hospitals know that the procedure that is being applied in this service, is being applied correctly and has a great impact for both professionals and users, and if they ask me [to share it with them], I will not say ‘No, this is mine, it was I who created it; it is for my service.’ (QMD member)
Staff involvement/commitment towards the hospital’s strategy in the implementation of falls prevention innovations
The implementation of the FPG’s projects (such as falls reporting, managing the physical environment surrounding the patient and the application of the Morse Fall Scale and related procedures) required action from other clinicians. Although their participation could have been elicited in several ways, such as through top-down-steered performance management systems, an essential characteristic of NPM (Torfing and Triantafillou, 2016), data from the interviews indicate that the FPG deliberately followed an informal and collaborative implementation approach, instead of a top-down, formal and structured method. The FPG adopted this approach as it considered that clinicians are intrinsically motivated to help the hospital improve the quality of services provided: Professionals are very involved in reporting and improving the quality of their services, i.e. if I’m working on my service and I see something with less [quality], I will say ‘This is less good’ and I will make a suggestion for improvement … . People are aware that they can play an active role and that we can all contribute. (FPG member) What happens here in the institution?! As the group of nurses is very big, the approach that they are adopting is [to communicate] to the chief nurse. Then [he/she] communicates this information in a session in a room. … Ah, then I can also manage in my way. (Chief nurse) The [QMD] provided clinical risk training in the hospital and this [training] was then conducted inside [clinical] services, cascading therefore through all services … . Falls were integrated into this. That is, when they provided clinical risk training, they also provided falls [prevention-related] training. Further specific training about falls prevention was provided by the group in clinical risk meetings with local clinical risk managers. (FPG member)
Trust-based professional autonomy
The implementation strategy of the FPG entailed both standardized and decentralized/tailored aspects. On the one hand, the FPG put in place projects and designed procedures to be adopted by virtually all medical and surgical departments inside the hospital. On the other hand, rooted in the trust the FPG had in clinicians – that, driven by their professional ethos, they are intrinsically motivated to do what is best for patients and are thus committed to the hospital’s aim of providing high-quality care and to the FPG’s initiatives – the group gave autonomy to local clinical risk managers, chief nurses and nurses belonging to the FPG to choose how to communicate the group’s projects to their peers. This resulted in the adoption of quite different approaches across the hospital units. The following examples of two clinical units illustrate the variety of communication methods (e.g. verbal communication, posters, written documents in a specific folder, communication at the time of shift handover, etc.) used by these intermediaries: I communicated to colleagues what was happening [update of the Morse Fall Scale], how to do it, and I put posters up and people went and read. We also have a folder. I told colleagues about the update and then [the information] was kept [in the specific folder] for them to read. (Local clinical risk manager nurse) The problem is to gather everyone … . So, the best possible way [is to deliver the information during] the shift handover. I used a sheet where everyone who was informed signs. Sometimes, I have to train a single person but everyone has to have the training. (Local clinical risk manager nurse) When we were first trained about the Morse Scale, we were full of doubts, calling this and that person … . I remember once calling Z [name of a FPG member], saying that I needed help, that I needed Z to come here to clarify. (Local clinical risk manager nurse)
Intra-organizational collaboration as a source of innovation (re)design
The fact that the FPG sought local clinical risk managers’ collaboration to not only disseminate information about the FPG’s projects, but also inform the group about what was happening in their clinical units, encouraged bilateral communication between the FPG and the clinical services. During an interview, a local clinical risk manager nurse described how this was fostered in the clinical unit where the nurse works: For example, in an early stage of implementation [of the Morse Fall Scale and related procedures], we provided on our noticeboard a sheet on which each nurse jotted down things whenever a difficulty emerged. We, intermediaries, then took this to the meeting with the members of the falls group. (Local clinical risk manager nurse) [W]e decided … to analyse what was happening here in the hospital. We went to evaluate some clinical services, we took some [falls] reports and we were able to specifically correct what was happening in some services. Some services had slippery floor in bathrooms and we changed it … we reduced the number of falls and the severity. (FPG member) [W]e reformulated everything, the interventions, etc. [because of received feedback on the adoption of the Morse Fall Scale and related falls prevention procedures]. People complained because … all shifts had to record what the patient did and people were not happy with the volume [of work]. (FPG member) So, the patient would come in, he/she would be evaluated [using the Morse Fall Scale] and, among us, we decided it was necessary to identify patients who had a high risk of falling in some way; and by our initiative, we didn’t use any outside model, we decided to institute a [pink] wristband. (FPG member)
Discussion and conclusion
This article focused on how Post-NPM might shape and affect innovation processes. The case showed that innovation is a multi-level organizational phenomenon, being facilitated through interweaved formal and informal processes that mutually reinforce each other. Innovation was fostered by the intra-organizational collaborative approach the FPG adopted, which, in turn, was enabled by both staff’s involvement/commitment towards helping the hospital in the provision of high-quality care to patients, and the existing climate of trust among staff, without which professional autonomy and hence true collaboration would not have been possible. In other words, innovation was driven by: (1) involvement/commitment at the organizational level (i.e. towards the organization’s strategy of providing the highest quality of care to patients); (2) trust-based professional autonomy at the individual level (i.e. between clinicians); and (3) intra-organizational collaboration at the team level (e.g. between the FPG and the clinical risk managers and chief nurses of the different clinical units) – all of which are in line with the Post-NPM model. The following list comments on each of these aspects:
From the start, and consistent with the Post-NPM model, the FPG and its success in designing and implementing falls prevention projects were influenced by clinicians’ intrinsic motivation and commitment to cooperate with the hospital’s strategy to provide the best care for its patients, that is, they were committed to providing public service value. Indeed, this patient-centred focus was the basis for the creation of the FPG as a bottom-up initiative that aimed at reducing the severity of falls and second falls. As discussed, although the awareness of the number of falls that triggered the creation of the FPG was only possible through the patient safety incidents reporting system, the objective of creating the FPG was not to reduce the number of falls (in the sense of a ‘tick-box exercise’ (Lapsley, 2009)), but rather to reduce their severity. As a result, in the case study, influenced by the Post-NPM model, the performance measurement system typically used in NPM as a control mechanism was instead used as a catalyst for collaboration. At the level of the interactions between individual clinicians, the existence of trust among individuals led the FPG to give autonomy to local clinical risk managers and chief nurses to choose the most appropriate methods to train and communicate the falls prevention projects to their colleagues. This trust-based management thus enabled the implementation of standardized processes through a tailored approach and therefore more in line with the contextual specificities of each clinical unit. This is in line with literature (e.g. Meyers et al., 2012) which advocates that engaging key staff in the implementation process is one of the effective strategies to secure their buy-in and decrease potential sources of resistance to change. From the interviews, it emerged that professionals created the necessary internal space for interacting ‘by (re)creating the organizational arrangements for collaboration’ (Schot et al., 2020: 336). This was visible, for instance, during the implementation process by not prescribing overly detailed processes for the ‘roll-out’ of innovations. Finally, the trust-based professional autonomy among staff facilitated the intra-organizational collaboration at the team level between the FPG and the key staff of the different clinical units. These clinicians and their colleagues felt at ease to raise their doubts with the FPG and to propose suggestions for quality improvement, some of which involved novel initiatives not available elsewhere. Our findings are in line with Trinchero et al. (2020: 125), who found by looking at public hospitals that ‘promoting inter-professional teamwork between, for instance, doctors and nurses is a step towards enhancing patient safety within healthcare organizations’. They also resonate with the wider literature on innovation in management (e.g. Crossan and Apaydin, 2010; Damanpour, 2017, 2020; Garud et al., 2013).
Furthermore, in the hospital, the spontaneous initiative of the falls prevention project and the main underlying processes that assisted its success were supported by both formal and informal structures. The FPG used formal structures of communication in informal ways, which helped the group to stay connected with ward clinicians. In turn, the feedback about clinicians’ experience with the FPG’s projects, as well as information on the impact and outcomes of their implementation, contributed to the redesign and improvement of the group’s projects.
In conclusion, in the hospital, the dynamics and mechanisms that had a key role in the innovation processes are integral features of the Post-NPM administrative model, therefore supporting the potential of Post-NPM in facilitating intra-organizational innovation. Findings also evidence the suitability of the Post-NPM model for ‘innovation projects that focus on novelty rather than efficiency’ given that explorative-type innovation relies more on ‘personal and informal modes of coordination and control’ (Faems et al., 2005: 241).
Our findings echo the literature which argues that a Post-NPM administrative model fosters innovation aimed at enhancing quality through organizational learning and multi-actor collaboration within a trust-based management where employees are given room to use their skills and competences to innovate (De Vries et al., 2018; Schot et al., 2020; Torfing and Triantafillou, 2016). Our results are also consistent with factors typically identified as determinants of organizational innovation, such as a clearly stated vision/strategy, the promotion of autonomy, low formalization, decentralization, the favourable attitude of managers towards change and strong internal communication systems (Crossan and Apaydin, 2010; Damanpour, 2020).
This study adds to the extant literature by providing a better understanding of how innovation processes take place within a Post-NPM model. In doing so, it addresses recent calls for further research on governance models and service innovation in the public sector (e.g. Rashman et al., 2009; Torfing and Triantafillou, 2016). It also adds to the literature in that it presents a case study from Portugal, a country that has been less the focus of the attested innovation studies, often based on the US/UK contexts (De Vries et al., 2018).
As all studies, the present one also has limitations, foremost due to the adopted methodology. Data were collected in a single case study hospital, hence limiting the generalizability of the findings to other contexts (Yin, 2018). Notwithstanding the limitations of the study, its findings provide insights into the role of organizational dynamics at the individual, team and organizational levels on innovation within a Post-NPM model that can be transferable to other contexts. Research on how innovation takes place within a Post-NPM administrative model would benefit from further studies to better understand its associated organizational dynamics. In particular, it seems promising to investigate the role of the individual, team and organizational levels deeper. Are all three levels equally important? For example, it would be useful to conduct studies in settings where staff are not as intrinsically motivated and committed to the organization’s strategy in providing the best value for their users. Looking at cases where innovation has failed (Garud et al., 2013) seems particularly important to avoid a bias ‘towards innovation “success”’ (Hartley and Rashman, 2018: 236).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research grant from Fundação para a Ciência e a Tecnologia (Foundation for Science and Technology, Portugal) (SFRH/BD/31350/2006).