
Abstract
Aims:
When the etiology of major depression is examined, the existence of psychosocial factors is undeniably important. Inadequate social support and use of dysfunctional coping strategies are psychosocial factors that play a role in the etiology of depression. This study investigated the perceived social support and coping strategies in patients with depression and whether they change with remission.
Design:
Both cross-sectional and longitudinal surveys were conducted.
Methods:
This study included 50 patients in the active phase of a major depressive disorder, 30 patients in the remission of depression, and 50 healthy controls. The Hamilton Depression Rating Scale (HAM-D), Multidimensional Scale of Perceived Social Support (MSPSS), and Assessment Scale for Coping Attitudes (COPE) were applied to all subjects. The same scales were repeated in 20 patients, who were in the active phase of depression at the beginning of the study and were in remission after approximately 3 years of follow-up. Psychometric test scores of three groups were compared with one-way ANOVA test, Kruskal-Wallis test, and post hoc tests. In the longitudinal analysis, the paired t-test and Wilcoxon tests were used.
Results:
The patients’ perceived social support scores were lower than the remission and control groups (p < .001). The total scores of non-functional coping attitudes of both the patient and remission groups were higher than those of the control group (p < .001 and <.001). The problem-focused coping and emotion-focused coping total subscale scores of the patient group were found to be lower than both the remission group (p < .001 and <.001) and the control group (p = .001 and .001). When the follow-up patients were evaluated while in remission, perceived social support scores increased compared to those in the active phase (p = .008 for total social support score). Non-functional coping scores decreased (p = .023). Perceived social support level associated with problem-focused and emotion-focused coping attitudes.
Conclusion:
The prognosis of depression might be affected by the perception of social support and coping attitudes.
Introduction
Major depression is a public health problem that is common in all societies and has an increasing importance because it causes disability and loss of a significant portion of patients due to suicide (Mathers et al., 2008). The prevalence and burden of major depressive disorder increased further with the impact of the COVID-19 pandemic, and depression is the most common mental disorder worldwide (Santomauro et al., 2021). For these reasons, understanding the etiology of depression and the factors affecting its process has become even more important. Neurobiological and psychosocial factors play a role in the etiology of depression. Inadequate social support and coping strategies are psychosocial factors that play a role in the etiology of depression (Remes et al., 2021).
Social support is the financial, emotional, or cognitive support provided by the close environment, such as spouse, family, and friends, which reduce the negative consequences of stressful situations, help to share values, emotions, and support the ability to adapt to social roles and difficulties of life (Sarason et al., 1983). Social support, which is emphasized as closely related to the mental health of an individual, reduces the feeling of anxiety and helplessness (Ardahan, 2006; Eker & Arkar, 2001). Perceived social support level is a description of how much an individual perceives the social support he/she receives from his environment and has been found to be more effective on mental health outcomes, such as depression and anxiety, when compared to social support levels (Haber et al., 2007).
Social support is seen as an important factor that plays a role in the prevention of depression and suicidal behavior and facilitates the recovery process in depressed patients (Bell et al., 2018). In cases where an individual’s perception of social support is insufficient, the severity of depression may increase (Wang et al., 2018). It has been shown that all types of social support, especially family social support, are protective against depression and anxiety symptoms (Roohafza et al., 2014). It was determined that perceived friend and family support scores were lower in patient with depressions and the most effective source of support was nuclear family members and relatives (Eker & Arkar, 1995). Perceived social support was found associated with depression in different populations such as adolescents (Hickey et al., 2017), elderly patients with vision problems (Horowitz et al., 2003), mothers during pregnancy, childbirth, and postpartum period (Ardahan, 2006; Langford et al., 1997), and patients with physical disabilities (De La Vega et al., 2019). A meta-analysis reported that people with depression found their social support insufficient and low social support was associated with symptom severity, poor recovery, and worse functional outcomes in depression (Wang et al., 2018).
Coping can be defined as all of the cognitive and behavioral effort given to reduce the physical, emotional, and psychological stressors caused by stressful life events and daily difficulties (Folkman et al., 1986; Wang & Patten, 2002). In the literature, the concept of coping has been classified with many different perspectives and theoretical explanations. Lazarus (1993) discussed coping strategies in two groups as emotion-focused and problem-focused. Problem-focused coping includes active behavioral and cognitive effort, such as planning to solve the problem, using the necessary resources, and generating ideas, which will enable elimination or reduction of the effect of a stressful event. In emotion-focused coping, the person tries to feel better by changing the meaning of the stressful event or by trying to manage his emotions as a result of the problem (Özarslan et al., 2013). In recent years, a different coping method has been defined apart from problem-focused and emotion-focused coping. Non-functional or maladaptive coping includes non-functional behaviors, such as refusing to acknowledge the problem, refusing to think about it, disengaging, and pretending that the stressful event never happened (Carver et al., 1989). Meta-analyses reported that more use of problem-focused and emotion-focused coping behaviors was associated with less depressive symptomatology and use of non-functional coping attitudes was associated with more depressive symptomatology (Littleton et al., 2007; Moskowitz et al., 2009). Coping attitudes are otherwise defined as active and passive attitudes. Active coping attitudes include behavioral or psychological responses aimed at changing or eliminating a stressor, while passive coping attitudes include avoidant coping styles that distance the stressor from it (Folkman & Lazarus, 1980).
It has been reported that problem-focused and emotion-focused coping strategies are used less and non-functional coping strategies, such as substance use and behavioral disengagement, are used more in depressive disorders (Özarslan et al., 2013). It was shown that depressed people tend to think that they have limited control over their own lives and use problem-focused coping strategies less in elderly patient with depressions (Hanevold et al., 2016). It has been reported that emotion-focused and problem-focused coping strategies are associated with less depressive symptomatology in caregivers of dementia patients (Li et al., 2012) and in diseases that cause chronic disability, such as organ failure (Ibrahim et al., 2013; Wingate, 2009). More use of emotion-focused coping strategies was associated with more depressive symptomatology in amputee patients (Falgares et al., 2019). It was shown that wishful thinking and thought suppression coping behaviors were used more in both the remission group and the depression group compared to the control group, and these two behaviors were found to be significantly higher in the depression group than in the remission group (Thimm et al., 2018). It is an avoidant coping style, as both coping methods lead to avoidance of the problem.
Social support may be related to coping strategies. Family, friends, and other important or special person social support types were showed to be associated with positive reinterpretation and growth, problem solving, seeking social support, and acceptance coping strategies (Roohafza et al., 2014). It can be argued that people with high social support will develop more effective coping skills in stressful situations. Patients with rheumatoid arthritis, who have high social support, had more successful cognitive processing, problem solving, and easier coping with pain (Holtzman & Newth, 2004). It has been found that high social support in caregivers of dementia patients, is associated with more use of problem-focused coping strategies and less depressive symptoms (Haley et al., 1996; Tang et al., 2015). In a post-disaster study, it was reported that social support has a significant negative correlation with depression and that social support has an effect on an individual’s ability to cope with the event (Kaniasty & Norris, 1993).
In summary, social support seems to influence coping resources and help develop more effective-adaptive coping ways. Social support may reduce stress by changing the perception of stressors, ways of coping, or problem-solving behaviors. Thus, it can improve the ability to cope with depression. It has been reported that there are changes in the perception of social support (Coulter et al., 2017) and coping skills (Ho et al., 2022) during the depression process, but it is not yet clear whether these are cause or result, or are only situational changes specific to the depression process. Based on these hypotheses, in this study, it was aimed to investigate the level of perceived social support and coping strategies used in patients with major depressive disorder and to examine the relationship between them. In addition, in order to investigate whether there is a change in these psychosocial characteristics during the active period of the illness and in remission, the patients were evaluated after remission.
Methods
Participants and procedure
In this study, 50 (41 women and 9 men) patients, aged 18 to 65 years, who were evaluated by clinical interview, were in the active phase of the disorder, were diagnosed with major depressive disorder according to DSM-5 diagnostic criteria were included in the depression group. They were followed up in the outpatient and inpatient clinics of psychiatry in a university hospital in Turkey.
Those, who had additional psychiatric disorders other than major depressive disorder or had a previous psychiatric disorder, received electroconvulsive therapy in the last 6 months, were illiterate, had a physical disease that might affect their functionality, mental disorders or neurological diseases that might impair their cognitive functions, and those with substance or alcohol use disorders other than smoking, were not included in the study.
The remission group consisted of 30 (27 women and 3 men) volunteers with a previously diagnosed major depressive disorder and in remission (HAM-D score <7) (Karamustafalıoğlu, 2010) for at least 1 month.
Fifty (37 women and 13 men) healthy volunteers in the same age range and without any known psychiatric disease were included in the control group. The same exclusion criteria were applied for the patient groups in remission and control.
This research was approved by the Ethics Committee of the Erciyes University, Faculty of Medicine. Written informed consent was obtained from patients and controls, who met the requirements, by explaining the purpose of the planned study and the way it was conducted.
Data collection forms to evaluate sociodemographic and clinical information of patients and controls included the Hamilton Depression Rating Scale (HAM-D) to determine depressive symptom severity, Multidimensional Scale of Perceived Social Support (MSPSS) to evaluate perception of social support, and Assessment Scale for Coping Attitudes (COPE) to determine coping attitudes.
Patients who were in the active phase of the illness at the beginning of the study were contacted after approximately 3 years. Twenty-one patients could not be reached and it was understood that the depressive symptoms of nine patients continued. Twenty patients found to be in remission for at least 4 months. They were evaluated by clinical interview. The scales were re-administered to these 20 patients.
Measures
Hamilton Depression Rating Scale (HAM-D)
The scale was developed by Hamilton in 1960 and Turkish validity and reliability study of the 17 items scale was performed by Akdemir (1996). Items in the HAM-D scale are marked between 0 to 4 and 0 to 2 according to symptom severity. A score of 0 to 7 on the scale indicates no depression, 8 to 15 indicates mild depression, 16 to 28 indicates moderate depression, and 29 and above indicates severe depression.
Multidimensional Scale of Perceived Social Support (MSPSS)
Turkish validity and reliability studies of the scale, which was developed by Zimet et al. (1991), were carried out by Eker and Arkar (2001). A 7-point Likert type scale consists of 12 items. The scale has three subscales that reflect sources of support; family, friend, and another important or special person, and each group consists of four items. The minimum-maximum scores is 4 to 28 for the subscales and 12 to 84 for total scale. A high score from the scale indicates high-perceived social support.
Assessment Scale for Coping Attitudes (COPE)
The scale was developed by Carver et al. (1989) to determine coping strategies used in stressful situations and its Turkish validity and reliability study was performed by Ağargün (2005). The scale is a self-report scale consisting of 60 questions. The COPE consists of 15 subscales: 1. Active coping, 2. Restraint coping, 3. Planning, 4. Seeking of instrumental social support, 5. Suppression of competing activities, 6. Positive reinterpretation and growth, 7. Turning to religion, 8. Humor, 9. Seeking of emotional social support, 10. Acceptance, 11. Behavioral disengagement, 12. Substance use, 13. Denial, 14. Mental disengagement, and 15. Focusing on and venting emotions. A total of 4 to 16 points can be obtained from each sub-scale. The sum of the scores of these subscales gives the problem-focused coping score (1–5), emotion-focused coping score (6–10), and non-functional coping score (11–16).
Statistical analysis
Distribution of the data was evaluated with the Shapiro-Wilk test. In the comparison of sociodemographic data and psychometric test scores of the groups, one-way ANOVA test and post hoc Tukey and Dunnet test were used for data with normal distribution, Kruskal-Wallis test and post hoc Bonferroni correction were applied for data with abnormal distribution. In comparison of the before and after scale scores of the patients included in the longitudinal analysis, the paired t-test was used for data with normal distribution and the Wilcoxon test for data with abnormal data. Categorical data were compared with the chi-square test. The Spearman correlation test was used to investigate the relationship between sociodemographic, clinical, and psychometric data. In the tables, data are expressed as mean ± standard deviation for those with normal distribution, median (interquartile range) for those with abnormal distribution, and number (percent) for categorical data. Only parameters with statistically significant values were included in the correlation tables.
Results
Results of cross-sectional analysis
There was no difference between the patient, control, and remission groups in terms of age and female/male ratio. There was a difference in marital status between the three groups, and the rate of married people in the control group was found to be lower (χ2 = 6,441, p = .040). It was found that 56% of the patients in the remission group, 30% of the patients in the depressive episode, and 16% of the control group had physical disease. The rate of accompanying physical diseases in the remission group was found to be higher than that of the other groups (χ2 = 14,579, p = .001). The rate of presence of mental illness in the families of the patients (18% of the patients) was found to be higher than that of the controls (10% of the controls; χ2 = 9,911, p = .007). The duration of education of patients with depression (8.5 years; p < .001) and remission groups (8 years; p < .001) was found to be lower than that of the controls (16 years; Table 1).
Sociodemographic and clinical characteristics of patients and controls.
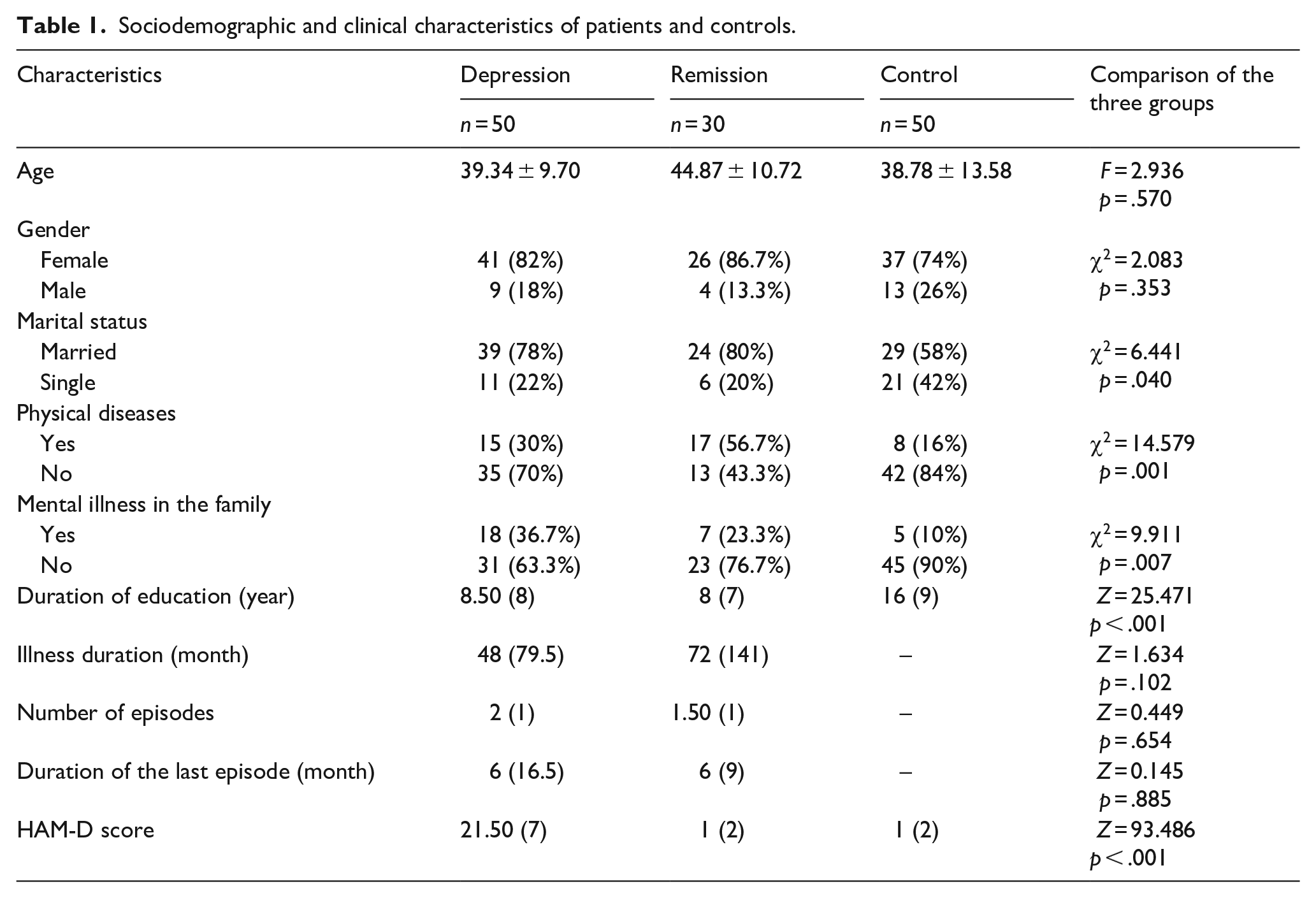
There was no difference between the patient and the remission groups in terms of illness duration, number of episodes, and duration of the last episode. The HAM-D score in the patient group was higher than those in remission (p < .001) and controls (p < .001; Table 1).
A significant difference was observed between the patient, remission, and control groups in all subscale scores of the MSPSS (p < .001). Other special or important person support, family support, friend support subscale scores, and total MSPSS scores of the patients were found to be lower than those of both the remission group (respectively; p = .003, <.001, .001, and <.001) and the controls (respectively; p = .001, <.001, .001, and <.001). There was no significant difference between the remission and control groups in terms of the MSPSS total and subscale scores (Table 2).
MSPSS scores of patients and controls.
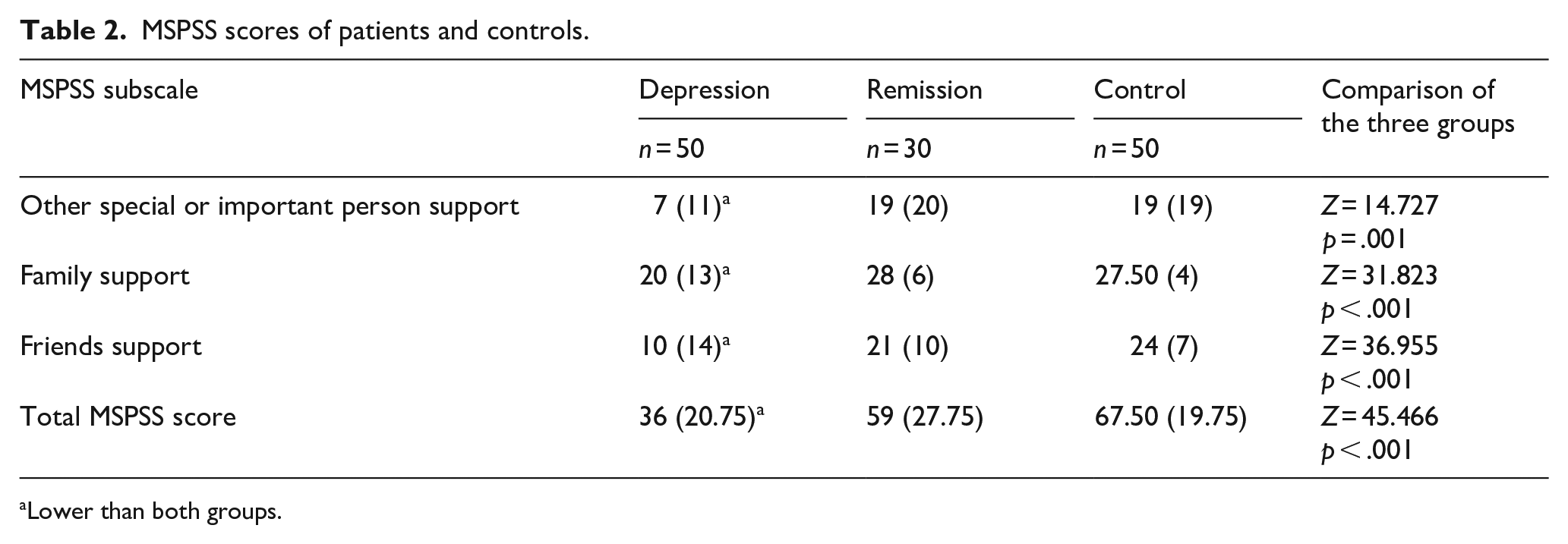
Lower than both groups.
Considering the total subscale scores of coping attitudes, the problem-focused coping and emotion-focused coping subscale scores of the patient group were found to be lower than both the remission group (p < .001 and <.001) and the control group (p = .001 and .001). While the total score of problem-focused coping attitudes was similar in the remission group and control group, the emotion-focused coping attitudes score was higher in the remission group than in the controls (p = .02). It was observed that the total scores of non-functional coping attitudes of both the patient and remission groups were higher than those of the control group (p < .001 and <.001; Table 3).
COPE total subscale scores of patients and controls.
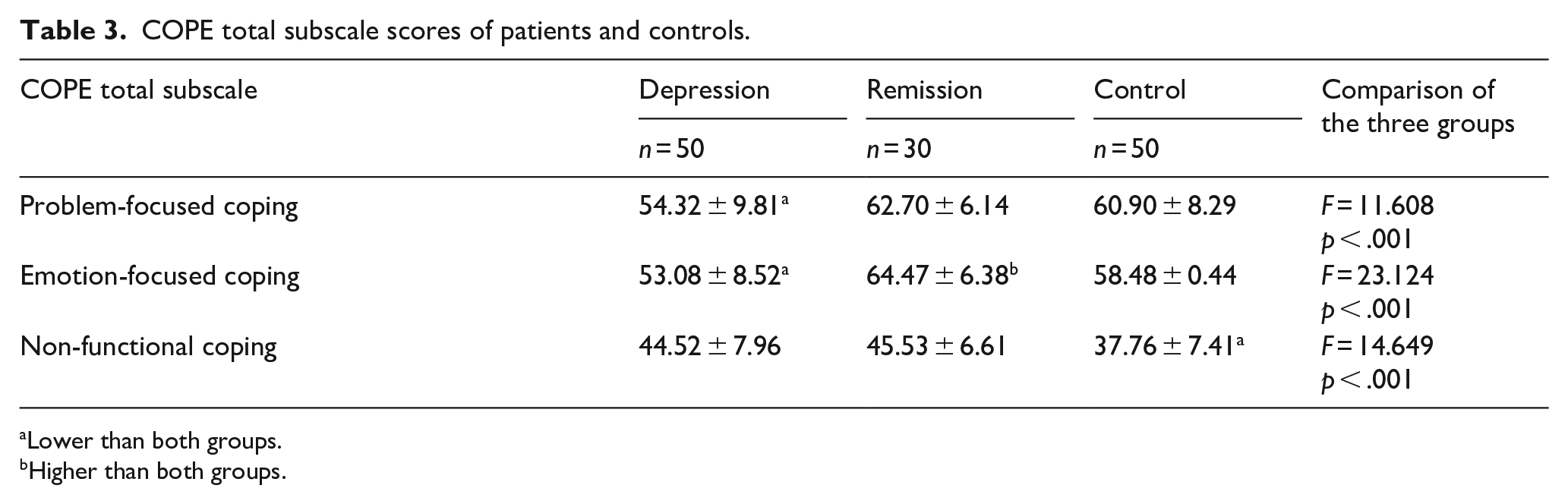
Lower than both groups.
Higher than both groups.
Correlation analyses in the patient group
A negative correlation was found between the severity of depression and the other special or important person support score of the MSPSS subscales (r = −.341, p = .015) and the total MSPSS score (r = −.293, p = .039). A positive correlation was found between the other special or important person support and emotion-focused coping scores (r = .363, p = .009).
Results of followed-up patients
Patients, who were in the active phase of depression at the beginning of the study were followed up for an average of 33.58 ± 1.82 (mean ± standard deviation; min = 31 and max = 37) months and the questionnaires were administered again at the end of the follow-up period. The mean HAM-D score of the patients whose depressive symptoms continued was 23.88 ± 4.85 (min = 17, max = 31). The mean remission duration of patients in remission was reported as 20.4 ± 10.58 (min = 4, max = 30) months.
When the MSPSS scores of the followed-up patients during the active depression and remission periods were compared, the perceived family (p = .003), friend (p = .046), and total social support (p = .008) scores were found to be higher in the remission period than in the active depression period. In other words, the level of perceived social support in other areas and in total, except for private person support, increased when patients went into the remission period (Table 4).
Comparison of MSPSS scores of follow up patients during active phase and remission periods.
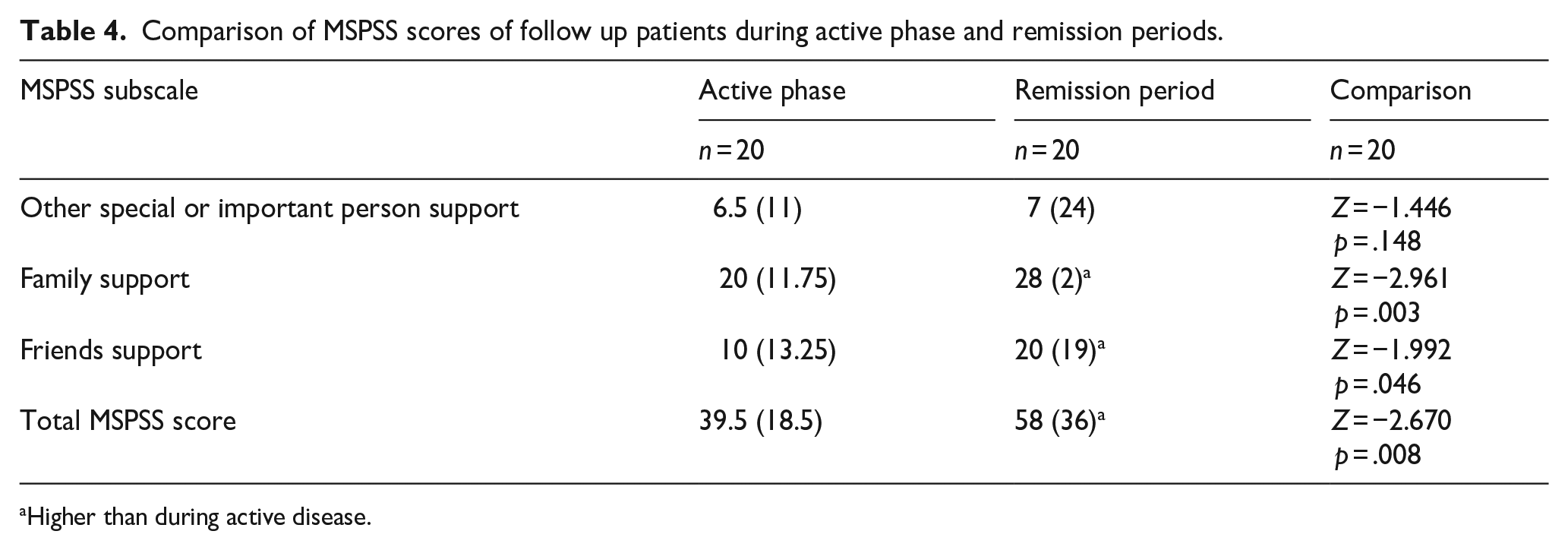
Higher than during active disease.
The subscale score of planning, one of the problem-focused coping methods, was found to be higher in the remission period than in the active period of the patients, who were followed up (p = .004). In patients in the remission period, positive reinterpretation and growth (p = .001), religiously coping (p = .005), and acceptance (p = .004) subscale scores, which are emotion-focused coping strategies, were higher than in the active phase; behavioral disengagement (p < .001) and substance use (p = .042) subscale scores, which are non-functional coping strategies, were found to be lower (Table 5).
Comparison of COPE subscale scores of followed-up patients during active disease and remission periods.
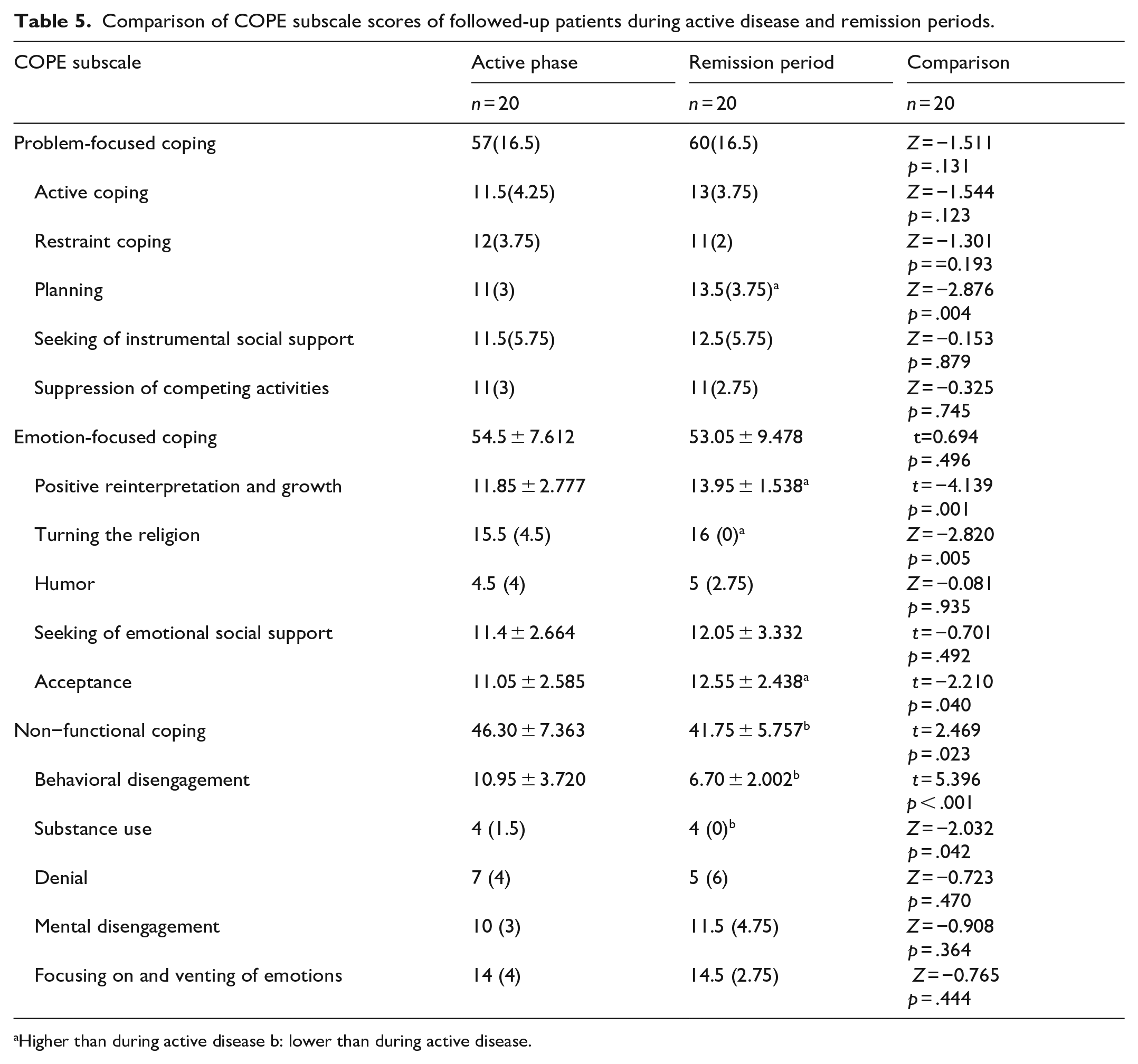
Higher than during active disease b: lower than during active disease.
In the followed-up patients, the non-functional coping subscale score was found to be lower in the remission period than in the active phase of depression (p = .023) and there was no difference in the problem-focused and emotion-focused coping subscale scores (Table 5).
Correlation analyses in the remission period in followed-up patients
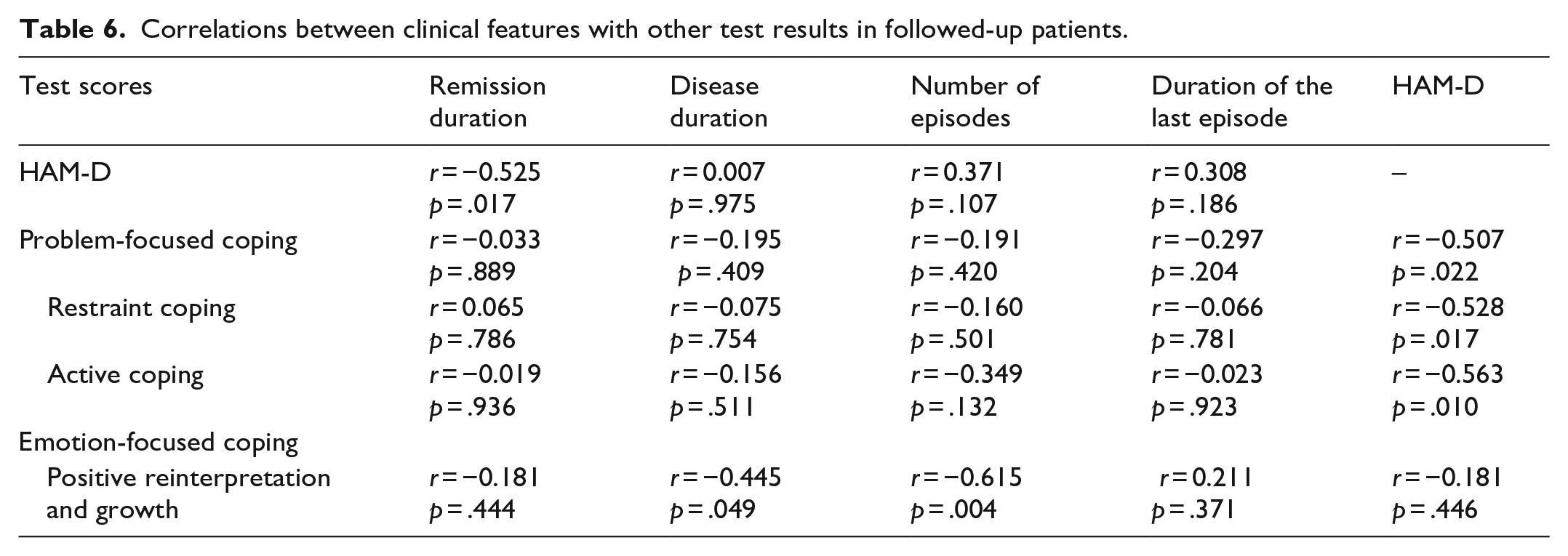
A negative correlation was found between the HAM-D score and the restraint coping, active coping subscales score and the total problem-focused coping subscale score. A negative correlation was found between positive reinterpretation and growth, one of the emotional-focused coping method, with illness duration and number of episodes (Table 6).
Correlations between clinical features with other test results in followed-up patients.
It was shown that while friends and total social support scale scores increased in patients, who were in remission, the HAM-D score decreased (Table 7).
Correlations between MSPSS scores and other test scores in followed-up patients.
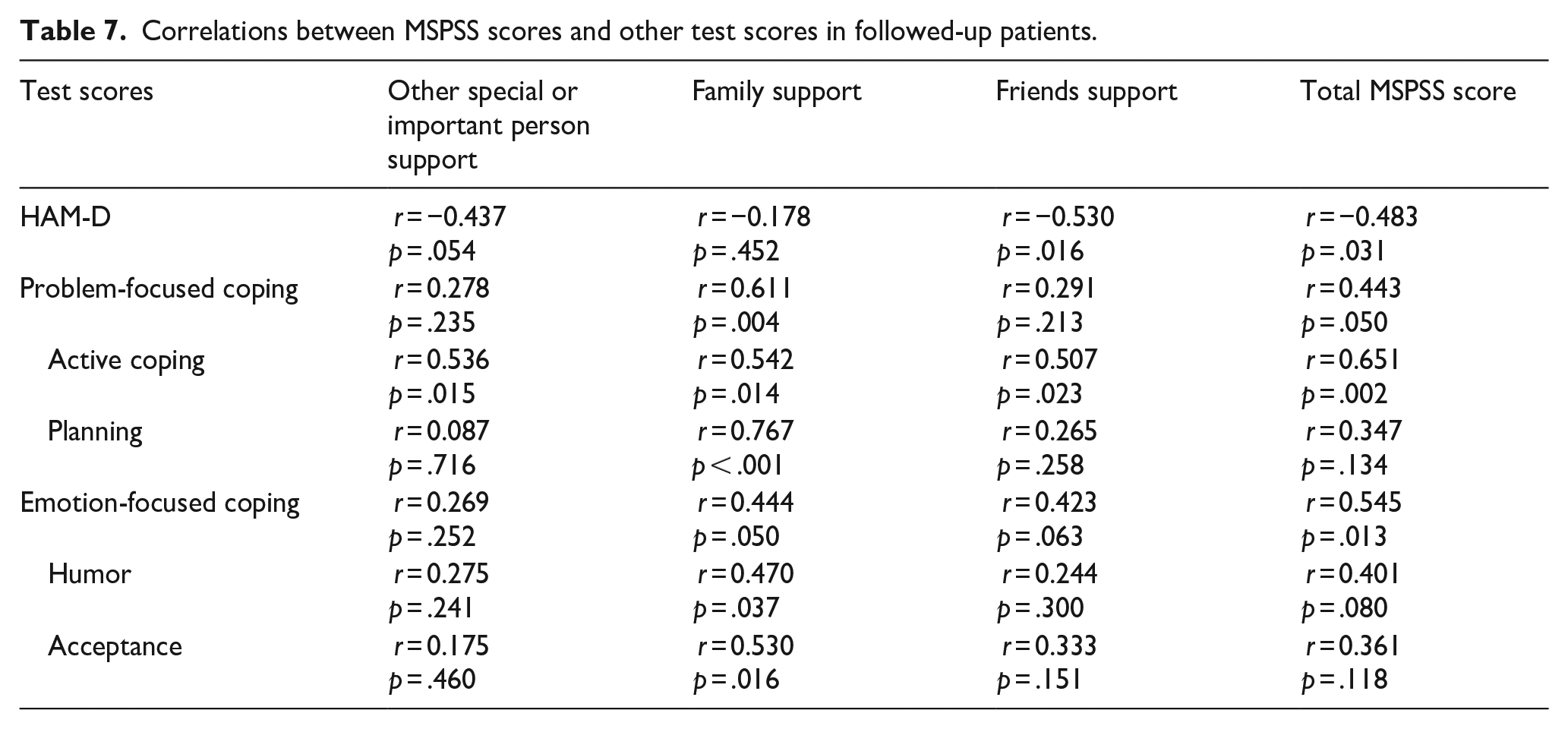
A positive correlation was found between active coping, one of the problem-focused coping methods, and all social support subscales and total social support scale. Planning was positively correlated with family social support. Humor and acceptance, which are emotion-focused coping methods, were also positively correlated with family social support. In terms of total coping subscale scores, a positive correlation was found between problem-focused and emotion-focused coping total subscale scores and family and total social support scale scores (Table 7).
Discussion
One of the major findings of this study is that the perceived social support is low in patients with depression. There was no difference in perceived social support levels between the remission group and the control group and the total social support and social support subscale scores of the patients in the active phase of depression were lower than those in both groups. It has been shown in previous studies that perceived social support decreases in depression and that high social support protects against depression (Gariépy et al., 2016). The contribution of our research to the literature is that we also followed-up the patients with depression and revealed the change in the perception of social support after the patients went into remission. It was shown that the perceived total social support levels, especially the perceived social support of family and friends, increased in the patients with depression, who were followed up when they were in the remission period, but the level of other important or special person support did not change during the illness and remission period. In other words, these findings obtained from both a cross-sectional and a longitudinal comparison showed that the low perception of social support is specific to the active phase of depression. Low perceived social support seems to be a state marker. One of the possible reasons for the low perception of social support during depression is that the social support of family and friends during the illness may be less perceived due to the negative automatic thoughts and cognitive distortions accompanying depression. Another reason is that depression may affect the social functionality of patients and cause a decrease in social support during the depression period. Since private person support may be a deeper support state in terms of quality, it may be less affected by cognitive distortions in depression, so there may be no difference in the illness and remission periods in the followed-up patients. On the other hand, the increase in family and friends support may contribute to the recovery from depression in these patients. In the literature, it was also shown that depressive symptoms decreased after interventions to increase social support in patients with physical limitations (De La Vega et al., 2019) and in patients followed up with cerebrovascular disease (Lin et al., 2019). These findings indicate that increasing social support or increasing the perception of already existing social support through interventions, such as cognitive-behavioral therapy, will contribute to the recovery process from depression. The relationship between social support and the severity of depressive symptoms also supports this.
In the study it was also seen that the severity of depression negatively correlated with the perceived social support level in patients with depression and when they reached remission. This finding is similar to previous studies. In studies conducted in different populations, a negative correlation was found between the level of perceived social support and the severity of depressive symptoms (Chan et al., 2022; Manne et al., 2018; Yoo et al., 2017). This finding of the study and previous studies revealed the association between scarce perceived social support and depressive symptoms. When the patients were evaluated in the remission period, the severity of depressive symptoms correlated with scarce perceived social support, which may be related to residual symptoms. However, it has not been possible to clarify whether longitudinal change is ‘cause or result’. It would have been possible to demonstrate this if we had been able to include patients who did not enter remission in the longitudinal part of the study and compare them. Nevertheless, the relationship between the perception of social support and depression seems clear. It can be said that the relationship between low level of social support and high depression symptoms is shaped as a result of reciprocal interaction. In other words, while low perception of social support increases the symptoms of depression, severe depression may also lead to a decrease in the perception of social support.
In the cross-sectional evaluation part of our research in terms of coping methods, it was determined that non-functional coping methods were used more in depressed patients, while problem-focused and emotion-focused coping methods were used less frequently.
Problem-focused coping and emotional-focused coping methods, which are important in coping with depression, are less used in the depressed patient group than in the remission and control groups. In a similar study in the literature, it was shown that patients with depression used less problem-focused coping attitudes and they used more non-functional coping attitudes (Özarslan et al., 2013). In the longitudinal evaluation part of our research, in the remission periods of the patients with depression, who were followed up, no significant change was observed in the total problem-focused and emotion-focused coping subscale scores compared to the active depression period. On the contrary, it was determined that they started to use less non-functional coping mechanisms, especially substance use and behavioral disengagement coping mechanisms. In the cross-sectional assessment, depressed patients used problem-focused and emotion-focused coping methods less when compared to a different remission group. That is, when the same individuals are followed, the use of problem-focused and emotion-focused coping methods is consistent, while the use of dysfunctional ones seems to change with the course of the disease. This may show that the use of non-functional coping attitudes can be considered as a state marker that increases in the depression period, but problem-focused and emotion-focused coping mechanisms can be considered as trait markers that indicate a person’s coping style. When the subscales of problem-focused and emotion-focused coping mechanisms were evaluated, we determined that when the patients were in the remission period, planning coping style, which is one of the problem focused coping methods, positive reinterpretation and growth, turning toward religion, and acceptance coping styles, which are emotion-focused coping styles, were used more. In other words, although the total emotional coping attitudes of the patients followed up did not change, the use of some emotional coping methods was observed to have increased. In support of this finding, we also found in the cross-sectional evaluation section that the emotionally focused coping total score of the patients in remission was even higher than that of the controls. That is, although the general coping styles showed trait characteristics, the use of some emotional methods to cope with disease states such as depression was observed to have increased. As a result, for example, the acceptance of unchangeable life stressors that may contribute to depression and the use of other emotion-focused coping mechanisms for adaptation may contribute to the remission of patients with depression.
In the patients we followed, we found that religious coping scores in addition to acceptance, planning, positive reinterpretation and growth scores, increased significantly during the remission period compared to the illness period. Religious coping method that is frequently used in our culture. In a study conducted in epilepsy patients in our region, religious coping was found to be the most used coping method (Unalan et al., 2015). In chronic disorders such as depression, which can reduce the quality of life, turning to religion, thinking that the disease comes from God, acceptance, and positive reinterpretation may be among the factors that facilitate the remission process. Additionally, religion is an important cultural factor in managing mental illness because it is an important part of daily life in many cultures and is important in coping with stress. Some authors reported that higher levels of religious involvement (attending religious services and participating in religious rituals), positive religious coping, and engagement along with intrinsic religiosity show lower rates of some psychiatric disorders such as depression, suicidal ideation, alcohol abuse, and have better quality of life (Bhugra & Ventriglio, 2024).
Positive reinterpretation and growth subscale scores were found to decrease while the illness duration and the number of episodes increased in the follow-up patients. It has been shown in the literature that positive reinterpretation and growth coping style protect against depression more than other coping styles (Roohafza et al., 2014). Recurrent episodes of depression lead to less use of adaptive attitudes, such as interpreting events from another perspective, gaining experience from the problems they have exposed, and on the other hand, the risk of relapse seems to increase while the positive reinterpretation coping attitude is less used. More use of active coping, restraint, and total problem-focused coping styles was associated with a lower HAM-D score in patients, who were in remission during follow-up. Psychosocial interventions that will enable patients to use problem-focused coping attitudes, especially active coping, can reduce the recurrence of depression.
The use of problem-focused and emotion-focused coping attitudes was corelated with the perceived family and total social support level when the follow-up patients were in remission. However, this correlation was not found in depressive group. Developing coping attitudes by social support in the remission period rather than in the depression period may contribute to the increase in the remission duration and the prevention of possible episodes. In a study conducted in elderly patients with hypertension showed that social support positively predicts adaptive coping strategies, such as seeking help and problem-solving, while negatively predicting maladaptive strategies, such as avoidance and self-blame (Li et al., 2025). Similarly, in a study in epilepsy patients found that positively significant correlation among the scores of perceived social support from a friend or someone special and positive reinterpretation and growth, focus on and venting of emotions, use of instrumental social support, active coping, restraint, use of emotional social support, acceptance, suppression of competing activities, and planning subscales (Unalan et al, 2015). It seems that increased social support provides more adaptive coping with stress.
Limitations of the study
One of the limitations of our study is the relatively small sample size of male participants. Additionally, the number of patients followed in the longitudinal analysis was considerably reduced. The small sample size may not allow generalization of the results. Another limitation of our study is that self-report scales may not have yielded objective results because they may have been affected by the negative perspective accompanying depression. There was a difference in sociodemographic characteristics, such as duration of education and marital status between the groups. These characteristics can affect the perception of social support and coping attitudes. However, statistical methods could not be used to control these confounding factors, as our data showed abnormal distribution. Another limitation of our study is that income status, which is a factor that may affect the level of social support and coping attitudes, was not asked.
Conclusions
In this study, it was shown that the level of perceived social support decreased, the use of adaptive coping methods decreased and the use of non-functional coping methods increased in depressed patients. When the patients with depression reached remission, perceived social support increased, the use of some adaptive coping methods increased and the use of non-functional coping methods decreased. In addition, it was shown that the level of perceived social support might be related to some coping methods in depressive and remission periods.
In line with the findings of the study, it can be said that increasing one’s perception of social support resources and social support will reduce the occurrence, persistence, and recurrence frequency of depression. Social support can affect the severity, chronicity, and coping skills of depression. Maladaptive coping attitudes are used more in people with insufficient social support. Increasing social support and acquiring adaptive coping skills can reduce the occurrence, recurrence, and chronicity of depression.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Scientific Research Project Unit of Erciyes University supported the study (grant number: TTU-2018-8245)
Ethical approval and informed consent statements
This research was approved by the Ethics Committee of the Erciyes University, Faculty of Medicine (decision number: 2018/227 and 2019/5247). Written informed consent was obtained from patients and controls.