
Abstract
Background:
Effective mental health systems depend on the functioning of a variety of factors that can be systematically monitored across countries. Macro-level assessments are needed to identify potential areas for improvement in the health sector, particularly in countries that face significant access barriers such as Greece.
Aim:
To analyze Greece’s mental health-related indicators in comparison to countries with similar socioeconomic contexts and geography and identify priority areas for the national mental health system.
Methods:
Data was sourced from the Global Mental Health Countdown 2030, an initiative gathering 48 indicators from 193 countries, classifying metrics into four domains: mental health system performance, determinants of mental health, factors influencing the demand for care, and wellbeing. We analyzed 39 indicators available for Greece to perform a comparative analysis with three groups of countries (27 European Union, 55 high-income, and 52 upper-middle income nations). We employed content analysis to organize mental health system indicators into a framework to inform policy and practice.
Results:
Greece exhibited low performance in several indicators related to mental health provision, with four metrics falling below the 12.5th centile for all comparative groups (‘interventions in primary care’, ‘policy implementation’, ‘promotion and prevention’, and ‘frequency of collection of data’). A content-analysis framework grouped indicators into categories related to the mental health system, with low-scoring metrics clustering around ‘policy and planning’, ‘affordability of care’, ‘coordination of services’, and ‘data collection and quality assessment’.
Conclusion:
This analysis provides a contextualized overview of Greece’s mental health system, identifying areas for improvement based on a panel of evidence-based indicators. Priority policy actions should focus on enhancing mental health insurance coverage and freely-available mental health services, organizing provision into a stepped-care and coordinated service network, and establishing systematic data monitoring mechanisms with unified electronic registers.
Introduction
There is a compelling need to integrate evidence into action within mental health policymaking (Patel et al., 2023). Improving mental health for all is a central agenda of the UN Sustainable Development Goals (SDG), underscoring the need for high-quality scientific data for understanding needs and monitoring national mental health systems’ performance (World Health Organization, 2021a). This is particularly important for countries grappling with socio-economic challenges and fragile health systems, where such information can help drive policy and facilitate change (Erskine et al., 2017; Mental Health Atlas 2020, 2021; Patel et al., 2018).
Toward enhancing mental health data worldwide, the Global Mental Health Countdown 2030 was launched as a monitoring platform measuring indicators on the current state of mental health across countries (Saxena & Kline, 2021; United for Global Mental Health, 2023). This project is implemented by a consortium consisting of United for Global Mental Health, Global Mental Health at Harvard, Global Mental Health Peer Network, WHO, and UNICEF, drawing on sources for metrics such as the United Nations, the World Bank, and academic institutions for statistics. It compiles and presents national level data from 193 countries on a wide range of factors, including mental health system indicators, mental health impact, wellbeing, financing to services, and attitudes to mental healthcare. The database is made available to inform policymakers, scholars, and stakeholders (see https://data.unicef.org/resources/countdown-for-global-mental-health-2030-dashboard/).
Greece presents a compelling case for comprehensive macro-level assessment of the mental health landscape. Coming off a recent healthcare reform, the country still grapples with significant challenges in its healthcare system, as well as gaps in quality of care monitoring and epidemiological research (Economou et al., 2017; Koumoula et al., 2023; Myloneros & Sakellariou, 2021). Obstacles are particularly pronounced in the mental health care provision sector, characterized by an underdeveloped community-oriented system, a lack of services, and a shortage of specialists in many, especially rural regions (Kotsis et al., 2019; Marchionatti et al., 2024). Moreover, there are concerning figures in many social determinants that impact mental health, such as high unemployment and poverty rates following economic downturns, as well as the increased incidence of trauma following local natural disasters – wildfires in particular – during the summer months (Melidis & Tzagkarakis, 2022; To et al., 2021; UNICEF, 2021; UNICEF & The Hellenic Republic, 2020). The mental health impacts are considerably higher for socioeconomically vulnerable children and adolescents, and there are extensive reports of precarious living conditions for refugees and migrants (Basta et al., 2021; Ben Farhat et al., 2018; Paleologou et al., 2018; Triantafyllou et al., 2018; UNICEF, 2021). Social services face resource constraints in addressing these demands, and a cross-country comparison suggested that Greece’s public expenditure on the social sector is among the lowest in the EU, particularly in areas related to family and children’s welfare and educational infrastructure (UNICEF & The Hellenic Republic, 2020).
This study aims to assess macro-level indicators in Greece that reflect or influence mental health outcomes. In this endeavor, we consulted the Global Mental Health Countdown 2030 dataset to conduct a comparative analysis of Greece’s indicators against those of three country groups: European Union, high-income, and upper-middle income nations. We constructed a framework to synthesize indicators related to the mental health system, identifying priority areas and opportunities for action in Greece’s mental health care.
Methods
Database description
The Global Mental Health Countdown 2030 is a dataset freely accessible at https://data.unicef.org/resources/countdown-for-global-mental-health-2030-dashboard/ and classified into four domains of indicators: A – determinants of mental health; B – factors influencing the demand and need for mental health care; C – factors shaping the strength of the mental health system; and D – wellbeing (Saxena & Kline, 2021; United for Global Mental Health, 2023). There are 48 indicators classified into 17 categories under these domains, encompassing information on a broad spectrum of factors such as service accessibility, financing, societal stigma and discrimination, mental health burden, and mental health challenges faced by individuals in conflict zones or other humanitarian crises.
The selection of indicators was conducted by a Technical Working Group. As an initial reference, the team inspected indicators from the WHO’s Mental Health Action Plan 2013 to 2030, the Lancet Commission review of SDGs pertinent to mental health, as well as a diverse array of indicators from additional sources (Lund et al., 2018; Patel et al., 2018; World Health Organization, 2021a). Next, 140 potential candidates were assessed on the basis of their relevance, feasibility, and sensitivity to change, drawing these metrics from 15 credible sources such as UN, WHO, UNICEF, UNESCO, the UNHCR, the World Bank, academic reports (e.g. University of Oxford, UC Berkeley, Institute for Health Metrics and Evaluation at the University of Washington), international NGOs (e.g. Internal Displacement Monitoring Centre), and a renowned global polling organization (Data Gallup). In all, a core ensemble of 48 indicators was included in the study.
Data collection and statistical analysis
We collected all indicators that were available for Greece in the Global Mental Health Countdown 2030 dataset (see Supplemental Table 1 for details on the methods behind each indicator score). To provide contextualized comparisons, we categorized nations into three groups: European Union countries, high income countries, and upper-middle income (the platform classifies the latter in accordance with the World Bank classification; see Supplemental Table 2 for countries in each group). The same set of indicators was accessed for each country of these groups to compose our dataframes. During data processing, categorical indicators were converted into numerical values on a scale from 0 to 4. To ensure standardized basis for interpretation, we applied reverse scores to indicators in which higher values implied poorer performance.
In each group dataframe, we calculated centiles of Greece’s indicator’s score using the percent-rank function from the R package dplyr; a plot visually indicating the country’s position was developed with the ggplot package (Wickham et al., 2019). Tables informing Greece’s score value for each indicator, median score of high-income countries and Greece’s centile in this comparative were constructed using the gtExtra package (Mock, 2023).
All analyses were performed in the software R version 4.4.1 (R Core Team, 2024). The code is freely accessible at our Open Science Framework repository (https://osf.io/crz6h/; Schäfer et al., 2023).
Content analysis of indicators related to mental health system
We conducted a streamlined content analysis to organize indicators related to the provision of mental health care within a framework designed to inform policy and practice. Content analysis is a flexible method to systematically identify patterns and interrelations across data, eliciting meaning and constructing theoretical models to enhance interpretation and facilitate insight (Kleinheksel et al., 2020; Lindgren et al., 2020). Indicators from subdomain B2.1 (financial accessibility of care) and all indicators from domain C (factors shaping the strength of the mental health system) were included, even those with missing data. Using a data-driven approach, we labeled the manifest content of each indicator based on its name, description, and methodology, identified patterns across these labels, refined them into codes, and organized these codes into a multi-level hierarchical model of categories to derive analytical insights (Kleinheksel et al., 2020; Vears & Gillam, 2022). A conceptual map was created to visually represent this framework with interrelated categories, presenting the scores of each indicator in centiles as compared to high-income countries. The coding was initially led by one author (LEM) and then collaboratively discussed with two team members (JLS and KK) until consensus was reached. Analysis was managed using NVIVO software version 14 (QSR International Pty Ltd, 2023).
Results
Indicators comparison
Figure 1 summarizes a comparative analysis of Greece’s indicators in relation to 27 European Union, 55 high-income, and 52 upper-middle income countries. Table 1 displays the raw scores of Greece’s indicators alongside their corresponding centiles relative to high-income countries. Indicators were informed by 14 datasources, primarily by the WHO Mental Health Atlas 2020 (16 indicators), Institute for Health Metrics and Evaluation (IHME; four indicators), and the World Bank (three indicators). Nine indicators were missing for Greece (see Table 2), mainly related to determinants of mental health and factors shaping the strength of the mental health system (including the two indicators within the subdomain ‘sustainable financing’; Figure 2).
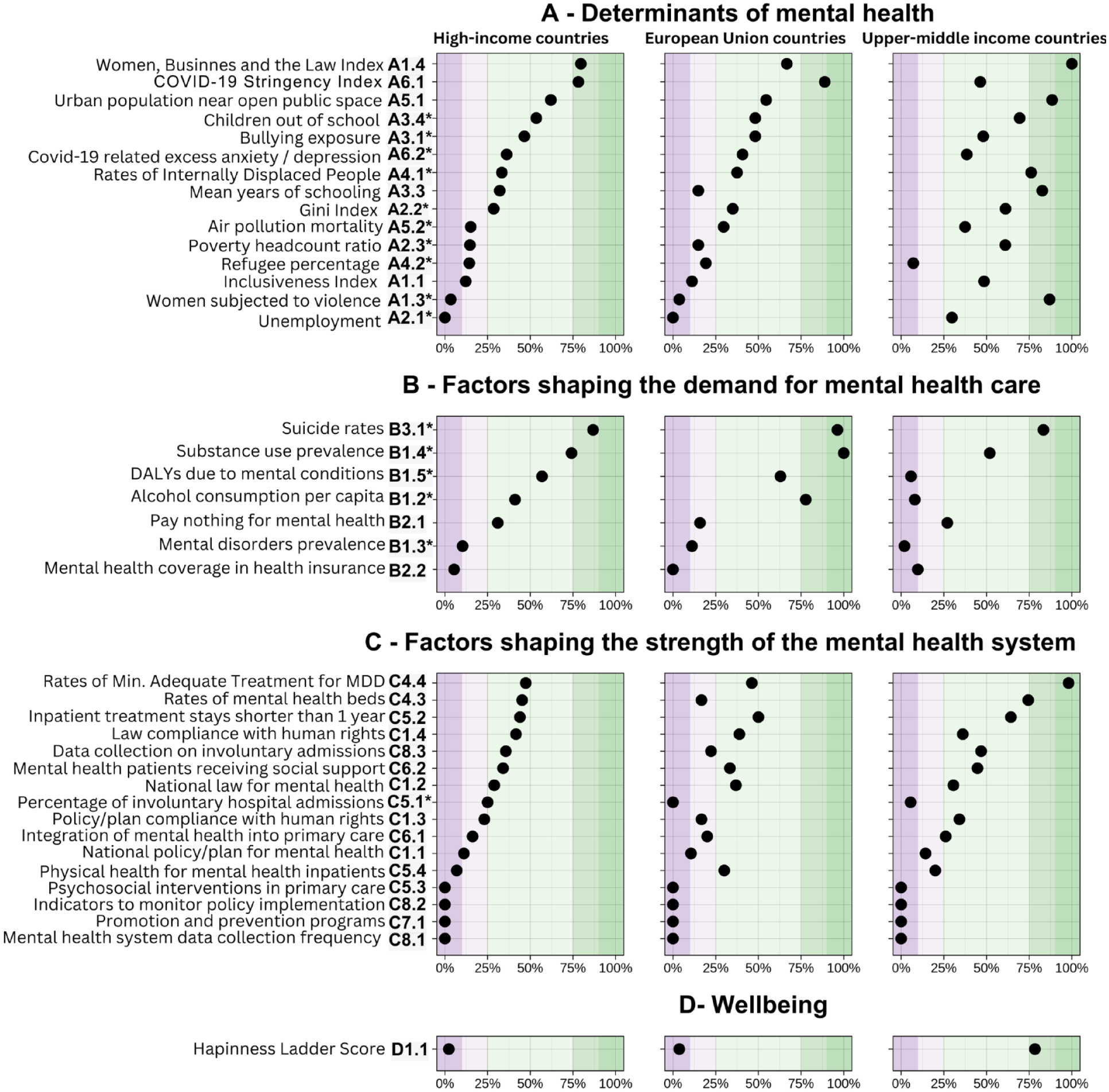
Comparative plot of Greek performance on mental health indicators as compared to other countries.
Greece’s and high-income countries’ indicators from the Global Mental Health Countdown 2030.
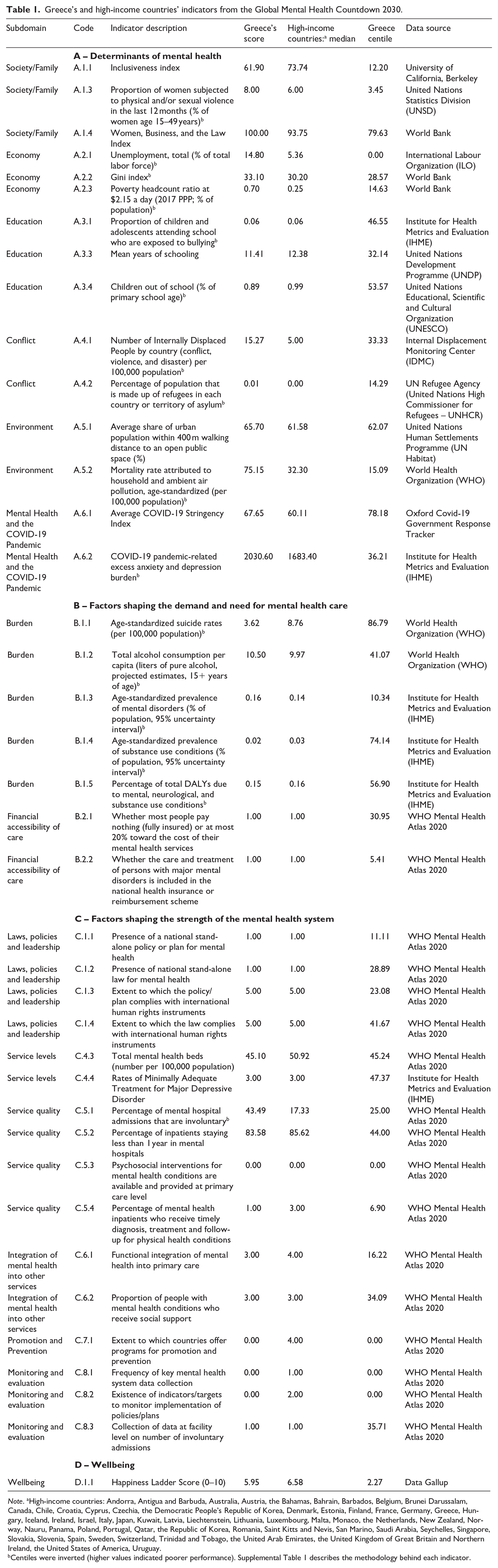
Note. aHigh-income countries: Andorra, Antigua and Barbuda, Australia, Austria, the Bahamas, Bahrain, Barbados, Belgium, Brunei Darussalam, Canada, Chile, Croatia, Cyprus, Czechia, the Democratic People’s Republic of Korea, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Israel, Italy, Japan, Kuwait, Latvia, Liechtenstein, Lithuania, Luxembourg, Malta, Monaco, the Netherlands, New Zealand, Norway, Nauru, Panama, Poland, Portugal, Qatar, the Republic of Korea, Romania, Saint Kitts and Nevis, San Marino, Saudi Arabia, Seychelles, Singapore, Slovakia, Slovenia, Spain, Sweden, Switzerland, Trinidad and Tobago, the United Arab Emirates, the United Kingdom of Great Britain and Northern Ireland, the United States of America, Uruguay.
Centiles were inverted (higher values indicated poorer performance). Supplemental Table 1 describes the methodology behind each indicator.
Missing indicators.

Note. IHME = Institute for Health Metrics and Evaluation; UNICEF = United Nations Children’s Fund; UNODC = United Nations Office on Drugs and Crime; WHO = World Health Organization.
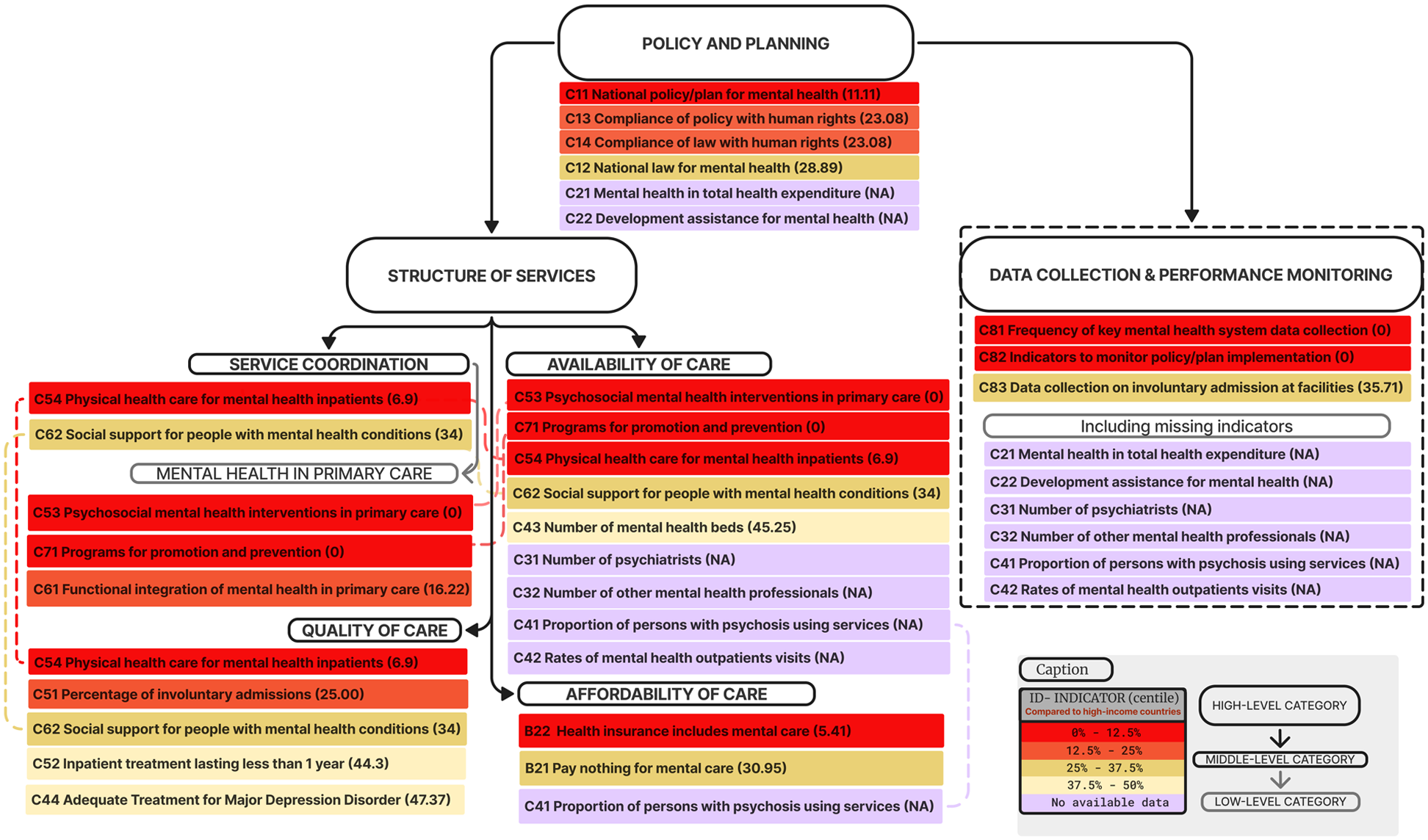
Framework for mental health system indicators.
In the domain ‘determinants of mental health’, Greece demonstrated above-median performance in indicators pertaining to ‘covid-19 pandemic’ and ‘environment’, and all indicators in ‘education’ were ranked within middle quartiles across all comparative groups. However, the subdomains of ‘economy’ and ‘conflict’ showed low performance when compared to high-income and European Union countries, with rates of ‘A2.1 – Unemployment’ falling below the 12.5th percentiles. The subdomain ‘society/family’ contained ‘A.1.1 – inclusiveness index’ and ‘A1.3 – violence against women’ ranking below the 15th percentile in comparison to high-income and European Union nations, although the indicator ‘A1.4 – women, business, and the law’ presented above-average scores across all comparative groups.
While the domain ‘factors shaping the demand for mental health care’ revealed mixed estimations on the ‘burden of mental health conditions’, all indicators related to the ‘financial accessibility of care’ fell below the 25th mark across all group comparatives. The domain ‘factors shaping the strength of the mental health system’ clustered low scores, with indicators such as ‘C5.3 – Psychosocial interventions in primary care’ significantly below median values across the three comparatives.
Mental health system: Conceptual framework of indicators
Figure 1 presents a framework of eight multi-level categories classifying 24 indicators related to mental health system provision (Supplemental Figures 1 and 2 for steps of the coding process). All 18 scored indicators fell below the 50th percentile when compared to high-income countries, with seven indicators in the bottom octile (0th–12.5th) and only three indicators approaching the median centile (37.5th–50th). Data was unavailable for six indicators.
‘Policy and planning’ is the first all-encompassing category, with its specific indicators highlighting the need for improved central-level planning for mental health (‘C1.1 – National policy/plan for mental health’ only reaches the 11.1th centile in relation to high-income countries). In the next tier, ‘data collection and performance monitoring’ exposes weaknesses in establishing systematic data collection mechanisms. This category includes six indicators with missing data, and two of its three specific measures scored zero in the group comparison (‘C8.1 – Frequency of mental health system data collection’ and ‘C8.2 – Availability of indicators to monitor policies/plans’).
At the same level, ‘structure of services’ encompasses closely related categories addressing the availability, quality, affordability, and organization of care. ‘Service coordination’ focuses on the integration across different levels of care and providers, clustering red-marked indicators. This is particularly evident in its subcategory ‘mental health in primary care’, showing marked fragilities in this level of provision (‘C5.3 – Psychosocial interventions in primary care’ and ‘C6.1 – Integration of mental health into primary care’). Several indicators under ‘service coordination’ are also assigned to other categories, which partially accounts for their poor performance metrics.
In the category ‘availability of services’, red-marked indicators highlight significant gaps, in particular the absence of mental health care in primary care settings as well as the lack of promotion and prevention programs. However, specialist-level services appear to be available, as indicated by ‘C4.3 – Number of mental health beds’ nearing medians of high-income countries. This category is also characterized by several missing indicators, resulting in gaps for assessing human resources and number of outpatient visits. In contrast, ‘quality of care’ shows points of strength, with high scores for ‘C52 – Inpatient treatment lasting less than 1 year’ and ‘C4.4 Adequate treatment for major depression disorder’; yet, concerns arise regarding the number of involuntary admissions.
‘Affordability of care’ emerges as an area of alarm. Not only is a crucial metric missing for the accessibility of care for individuals with severe disorders (‘C4.1 – Proportion of persons with psychosis using services’), but the available indicators suggests that health insurance does not adequately cover mental health care and that access to free mental health services needs expansion (‘B2.2 – Health insurance includes mental care’ and ‘B2.1 – Pay nothing for mental care’). Notably, this category is somewhat associated with the organization of services, as the unavailability of care in primary health settings limits free access to mental health assistance.
Discussion
Our analysis of 39 indicators provides a comprehensive overview of the mental health landscape in Greece contextualized through comparisons with countries in similar socioeconomic groups, including those in the European Union, high-income, and upper-middle income countries. Greece’s mental health care system metrics fall significantly behind those of other nations and were further examined through content analysis. This framework identified priority areas for policy making, including improving the affordability of care through health insurance coverage and freely accessible services (B21 and B22), better integration of primary care and prevention/promotion into mental health services (C53 and C71), addressing the high rates of involuntary admissions (C51), and strengthening mechanisms for data collection (C81–C83). Building upon this framework and supporting literature, Table 3 presents recommendations for policy with target indicators for monitoring progress.
Recommendations for improving mental health system with target indicators.

Centile in the comparison with high-income countries.
This comparative assessment quantifies a range of previously debated shortcomings in Greece’s mental health system. Low-scoring metrics related to service coordination reflect that the national mental health provision is not organized into a stepped-care model, lacking established patient pathways and presenting fragile integration across services and providers that often operate in isolation (Marchionatti et al., 2024). Despite recent forms, the consolidation of a primary care system in the country remains in progress, with insufficient services and professionals in place to achieve adequate populational coverage (Kousoulis et al., 2013; Myloneros & Sakellariou, 2021). In the absence of gatekeeping mechanisms, patients tend to access specialists directly, while primary care providers lack both the training and cultural orientation to address mental health needs (Economou et al., 2017; Emmanouilidou, 2021; Souliotis et al., 2017; Marchionatti et al., 2024).
Moreover, the development of a community-based mental health system has been hindered by underfunding of the public sector, leading to ‘passive privatization’ in the field (Marchionatti et al., 2024; Giannakopoulos & Anagnostopoulos, 2016). A shortage of public-sector professionals and long waitlists push individuals toward private care, resulting in services that are misaligned with population needs, concentrated in metropolitan areas, and centered around specialist care. The underprovision of services and lack of coordinated community care networks leave many mental health patients unassisted, allowing conditions to worsen until acute care is needed (Petrea et al., 2020). This has been cited as a contributing factor to the high rates of involuntary admissions consistently reported across Greece, a key issue in patient rights advocacy (Drakonakis et al., 2022; Petrea et al., 2020; Stylianidis et al., 2023). The lack of coordination across services is also attributed to the absence of a unified electronic health register operating in the national health system, which arguably contributes to issues on data collection and performance monitoring (Economou et al., 2017; Giannakopoulos & Anagnostopoulos, 2016; Kotsis et al., 2019; Marchionatti et al., 2024; Stylianidis et al., 2023).
While the availability of specialist-level services shows favorable scores in indicators such as the rate of mental health beds, research also indicates that facilities and human resources are unevenly distributed and results in coverage gaps in Greece (Marchionatti et al., 2024). In particular, a scarcity of specialized services in the public system has led to an increased reliance on out-of-pocket payments, a phenomenon described as passive privatization in the healthcare sector that represents a long-standing issue in Greece beyond mental health care (Emmanouilidou, 2021; Grigorakis et al., 2016; Kalavrezou & Jin, 2021; Myloneros & Sakellariou, 2021). Indeed, our framework displays concerning metrics on affordability of care, which is supported by a recent national survey indicating that approximately 75% of caregivers were discouraged from seeking professional assistance for children and adolescents due to cost concerns (Koumoula et al., 2024).
While recommendations for policy are provided, it is worth noting that Greece has been advancing an agenda to strengthen the community-based mental health system, appointing a dedicated deputy minister for mental health and launching new national plans (Marchionatti et al., 2024). Additionally, local UNICEF and WHO offices have been established to adopt international standards, with the latter focusing on care quality and patient safety (World Health Organization, 2021b). The country has also co-led the EU-funded JA ImpleMENTAL programme, which emphasizes the implementation of best practices in mental health (Konte et al., 2021).
Providing relevant insights into the specific context of Greece, this study addresses the call to integrate evidence-based data into mental healthcare system assessments (Patel et al., 2018, 2023). Drawing upon a high-quality repository, our analysis is presented in an intelligible manner, facilitating outreach to the diverse stakeholders involved in decision making. We adhere to principles of transparency and open science, sharing statistical codes for verification and reproduction (Vicente-Saez & Martinez-Fuentes, 2018).
This approach using macro-level indicators presents limitations. Such a global comparison is susceptible to anticipated discrepancies in data collection methodologies across countries, as well as variations in data quality and accuracy. The present analysis was further restricted by nine indicators with missing scores for Greece, such as the availability of mental health professionals, the expenditure on mental health, and children exposed to violence. While some of this information is available from other data sources (see Marchionatti et al., 2024, for an analysis of distribution of psychiatrists across the country), they are not standardized according to GMHC-2030’s collection methods. Greece also ranked in the lowest percentile for the frequency of collecting mental health measures, reflecting claims on insufficient data monitoring and research in the mental health system (Economou et al., 2017; Koumoula et al., 2023, 2024; Marchionatti et al., 2024). These factors could further introduce inaccuracies, biases, and outdated measures into the scores underpinning our analysis.
This study leverages the Global Mental Health Countdown 2030 platform to assess the mental health landscape in Greece, identifying key areas where the country lags behind other high-income nations. Public policy priorities include the affordability of mental health care, service coordination, integration of mental health into primary care, and the availability of promotion and prevention programs. These findings underscore the need to strengthen national mental health laws and policies to reinforce the public system’s role in coordinating public and private providers within a community-oriented, stepped care mental health framework that aligns with population needs and ensures equitable access to care.
Supplemental Material
sj-docx-1-isp-10.1177_00207640241303029 – Supplemental material for The state of mental health in Greece: An international comparative analysis using data from the Global Mental Health Countdown 2030
Supplemental material, sj-docx-1-isp-10.1177_00207640241303029 for The state of mental health in Greece: An international comparative analysis using data from the Global Mental Health Countdown 2030 by Konstantinos Kotsis, Lauro Estivalete Marchionatti, André Simioni, Julia Luiza Schafer, Sara Evans-Lacko, Shekhar Saxena, Sarah Kline, Antonis Kousoulis, Anastasia Koumoula and Giovanni Abrahão Salum in International Journal of Social Psychiatry
Footnotes
Acknowledgements
This work is part of The Child and Adolescent Mental Health Initiative (CAMHI) aimed to enhance mental health care capacity in Greece. The CAMHI is funded by the Stavros-Niarchos Foundation (SNF) and led by the Child Mind Institute (CMI) in partnership with multiple institutions and actors in Greece. The authors would like to thank SNF’s Co-President Andreas C. Dracopoulos for his leadership in creating, launching, and supporting the project. We would also like to thank Ms. Elianna Konialis, Ms. Dimitra Moustaka, and Mr. Panos Papoulias for their critical role in multiple steps of the conceptualization and implementation of the CAMHI objectives.
Author contributions
KK: conceptualization, methodology, validation, formal analysis, investigation, and writing – review & editing. LEM: conceptualization, methodology, software, validation, formal analysis, investigation, data curation, writing – original draft, writing – review & editing, and visualization. AS: software, validation, formal analysis, investigation, data curation, and visualization. JLS: conceptualization, methodology, validation, project administration, supervision, writing – original draft, writing – review & editing, visualization, and supervision. SEL, SS, SK, and AK: conceptualization, validation, writing – review & editing, and supervision. AK and GS: conceptualization, methodology, validation, writing – review & editing, supervision, project administration, and funding acquisition.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Stavros Niarchos Foundation (SNF) through The Child and Adolescent Mental Health Initiative (CAMHI).
Ethical approval
This study does not require ethics approval as it does not involve human or animal participants.
Data availability statement
This work utilizes openly available data from UNICEF’s Global Mental Health Countdown (![]() ). The statistical codes used in this study are available in a public repository at the Open Science Framework (http://doi.org/10.17605/OSF.IO/CRZ6H). A detailed description of the dataset methodology and the underlying codification process for the content analysis is provided in the Supplementary Material.
). The statistical codes used in this study are available in a public repository at the Open Science Framework (http://doi.org/10.17605/OSF.IO/CRZ6H). A detailed description of the dataset methodology and the underlying codification process for the content analysis is provided in the Supplementary Material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.