
Abstract
Background:
Although previous reviews have examined the relationship between heritage cultural maintenance and mental health outcomes among migrants, none have focussed specifically on migrant adolescents (i.e. those aged 10–24 years).
Aims:
To examine (1) the focus, scope and nature of quantitative empirical research investigating heritage cultural maintenance – including linguistic maintenance – and mental health outcomes among migrant adolescents globally and (2) the association between cultural and linguistic maintenance and migrant adolescents’ mental health outcomes.
Method:
Following the Arksey and O’Malley methodological framework for scoping reviews, we searched 11 electronic health, medical, social science and language databases from database inception until the search date (6 June 2023), using English search terms. We extracted data from included empirical studies using a template with pre-defined data items, which we present in comprehensive overviews and narrative summaries.
Results:
Thirty-four studies met our inclusion criteria. We identified considerable heterogeneity between studies regarding their research foci, methodologies, terminologies, outcomes and findings regarding the association between cultural maintenance and mental health outcomes. We specifically identified mixed findings regarding the latter, which cannot be transferred or generalised.
Conclusions:
The heterogenous nature of methodologies and outcome measures in the published literature, in addition to a scarcity of research from low- and middle-income countries, have hindered meaningful progress in this field. Efforts to address these issues, and to take adolescent context into consideration, will facilitate a more accurate understanding of how cultural maintenance relates to migrant adolescent mental health, and inform future interventions to improve mental health outcomes.
Introduction
In 2022, one in every 30 people worldwide was reported to be a migrant (also known as international migrant, or immigrant) (McAuliffe & Triandafyllidou, 2021), defined by the United Nations (2024) as people who live in a country different to the one in which they were born. This usually leads to differences between a person’s heritage (also known as native) and host (also known as dominant, or mainstream) cultures (Berry, 2005).
Studies investigating mental health outcomes in migrants have produced inconsistent findings. For example, while some studies have identified an ‘immigrant paradox’, in which migrant groups show similar or lower levels of adverse mental health outcomes than non-migrants (e.g. Vazsonyi et al., 2017), most other studies have identified increased levels of adverse mental health outcomes – including depression and suicidal ideation – among first- and second-generation migrants (e.g. Hovey & King, 1996). This highlights the need to better understand migrant vulnerabilities, to improve mental health support.
Research on acculturation (defined as ‘the dual process of cultural and psychological change that takes place as a result of contact between two or more cultural groups and their individual members’ [Berry, 2005, p. 698]) has investigated the impact on migrants of interacting with other cultures, with a focus on two key elements: (a) cultural maintenance – the subjective importance someone places on their heritage cultural identity and the continuation of related practices; and (b) contact and participation – the degree to which individuals choose to interact with the host culture or to remain within their heritage cultural groups (Berry & Sam, 1997). Based on these two aspects, Berry and Sam (1997) identified four acculturation strategies: (1) integration (heritage culture is maintained while seeking interactions with other groups); (2) assimilation (heritage culture is not maintained while seeking interactions with other groups); (3) separation (heritage culture is maintained while avoiding interactions with other groups); and (4) marginalisation (heritage culture appears difficult to maintain, and there seems to be little interest in interacting with other groups).
Numerous reviews have examined the relationship between acculturation strategies and mental health (i.e. Balidemaj & Small, 2019; A.-M. D. Nguyen & Benet-Martínez, 2013; Wyatt et al., 2015; Yoon et al., 2013). However, even though age has been identified as a key component of the relationship between acculturation and mental health (Yoon et al., 2013), no review of the literature has yet examined how heritage cultural maintenance is related to the mental health specifically of migrant adolescents (i.e. those aged 10–24 years [Sawyer et al., 2018]).
In this scoping review we aimed to answer the following two research questions:
(1) What is the focus, scope and nature of quantitative empirical research investigating heritage cultural maintenance and/or language maintenance and mental health outcomes in adolescents with an international migrant background worldwide?
(2) To what degree is cultural and linguistic maintenance associated with migrant adolescents’ mental health outcomes?
Methods
We followed the scoping review methodology outlined by the Joanna Briggs Institute (Peters et al., 2020), which is based on Levac et al.’s (2010) elaborations to the Arksey and O’Malley (2005) framework. Reporting adheres to relevant sections of the ‘Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews’ (PRISMA-ScR) (Tricco et al., 2018). The protocol outlining this scoping review’s methodology was published in 2023 (Hasnain et al., 2023).
Eligibility criteria
Our inclusion and exclusion criteria are listed below.
Inclusion criteria
Published, peer-reviewed empirical studies.
Any language (however, the search was only conducted in English, which indirectly excluded all studies without an English title, abstract or keywords).
Adolescent study participants between 10 and 24 years.
Studies focussed on mental health outcomes, symptom severity and diagnosis.
Studies measuring mental health outcomes, specifically depression, anxiety, self-harm, suicide, substance misuse and schizophrenia.
Studies measuring any nondominant heritage culture or language.
Exclusion criteria
Qualitative studies, literature reviews, book chapters, dissertations, conference papers, conference abstracts and editorials.
Participants younger than 10 years, or those who are 25 years or older.
Studies focussed on help-seeking, or interventions in mental health dimension.
Studies measuring trauma, self-esteem, life satisfaction or well-being.
Studies measuring the uptake of host language or culture without considering heritage language and cultural maintenance; studies measuring ethnic identity.
No restrictions were placed on publication date or study location. Despite including search terms relating to studies of Indigenous adolescents, the post-hoc decision was made to write a separate, stand-alone review focussing specifically on these studies. Literature reviews were also excluded. However, we screened relevant review reference lists to identify additional studies.
Information sources
We searched the following 11 electronic databases from database inception on 6 June 2023, with email alerts were set-up for each until 31 December 2023: APA PsycArticles Full Text (coverage from 1894); EMBASE Classic + Embase (from 1947); Ovid MEDLINE and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily (from 1946); Ovid MEDLINE all (from 1946); APA PsycInfo (from 1806); University of Melbourne full text journals; Science Citation Index Expanded (from 1900); Social Sciences Citation Index (from 1900); Arts & Humanities Citation Index (from 1975); Scopus (from 1970); and Linguistics and Language Behavior Abstracts (LLBA) (from 1973). Further, we screened relevant reference lists to locate studies that were not identified during the electronic search.
Search
The search strategy (see Appendix) was adapted to the specific requirements of each database (see an example in the Appendix [A1]).
Study selection and data charting
The first author (AH) conducted the search, and then exported, consolidated and screened study abstracts and titles, resulting from the searches, in a Microsoft Excel spreadsheet. The second author (JH) supported AH in applying the inclusion and exclusion criteria, as well as recording reasons for each outcome. AH then downloaded the full text of studies potentially meeting all inclusion criteria into the citation management software Zotero and read each study in full. JH and the third author (RB) reviewed at least 20% of excluded and included studies at each milestone – when two researchers did not agree, the third made the decision. AH extracted data from included studies using a predefined extraction template.
Results
Study selection
We identified 3,426 records, of which 34 met our inclusion criteria (see Figure 1).
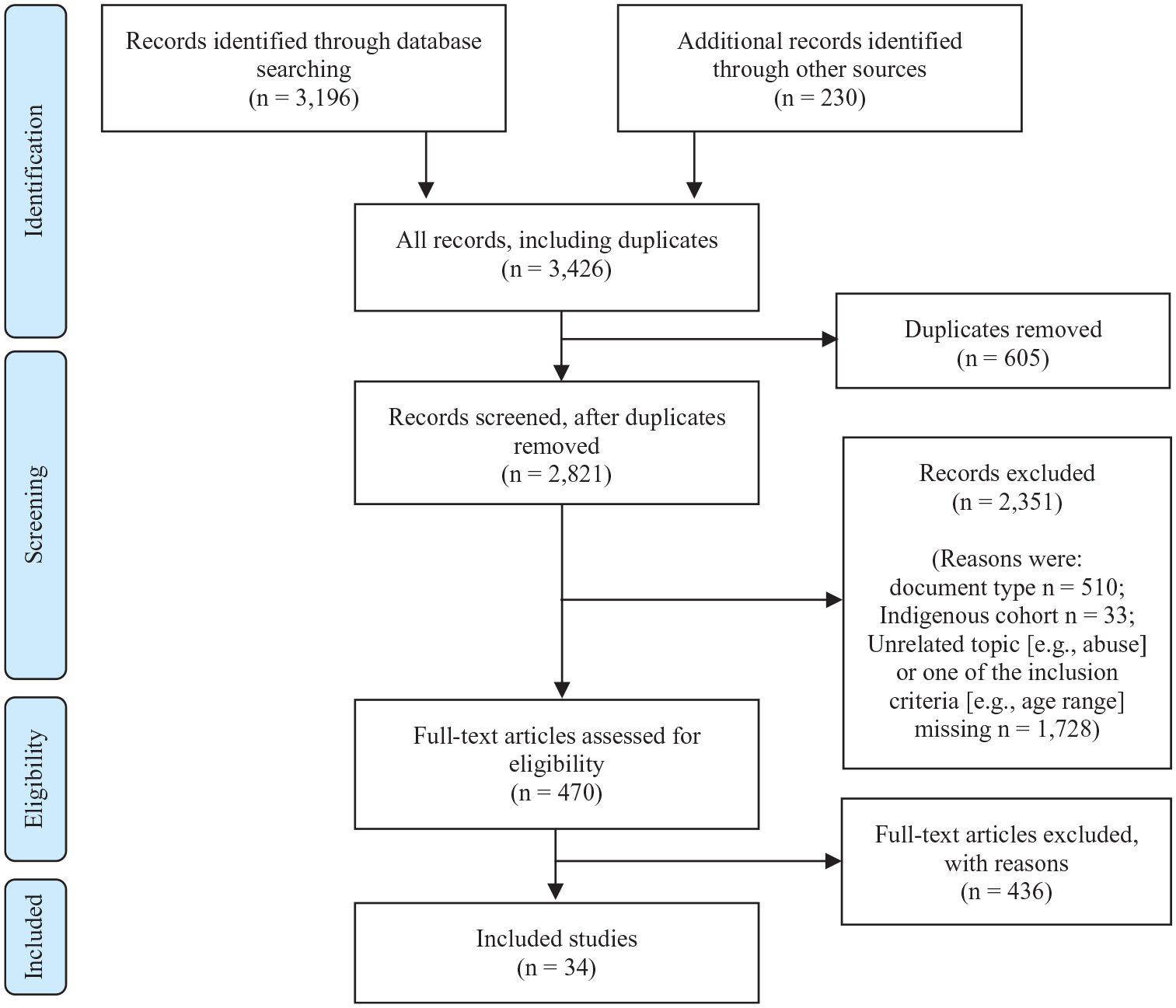
Study selection, following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) process (Moher et al., 2009).
Summary of results
The characteristics of included studies are listed in Table 1.
Characteristics of included studies.
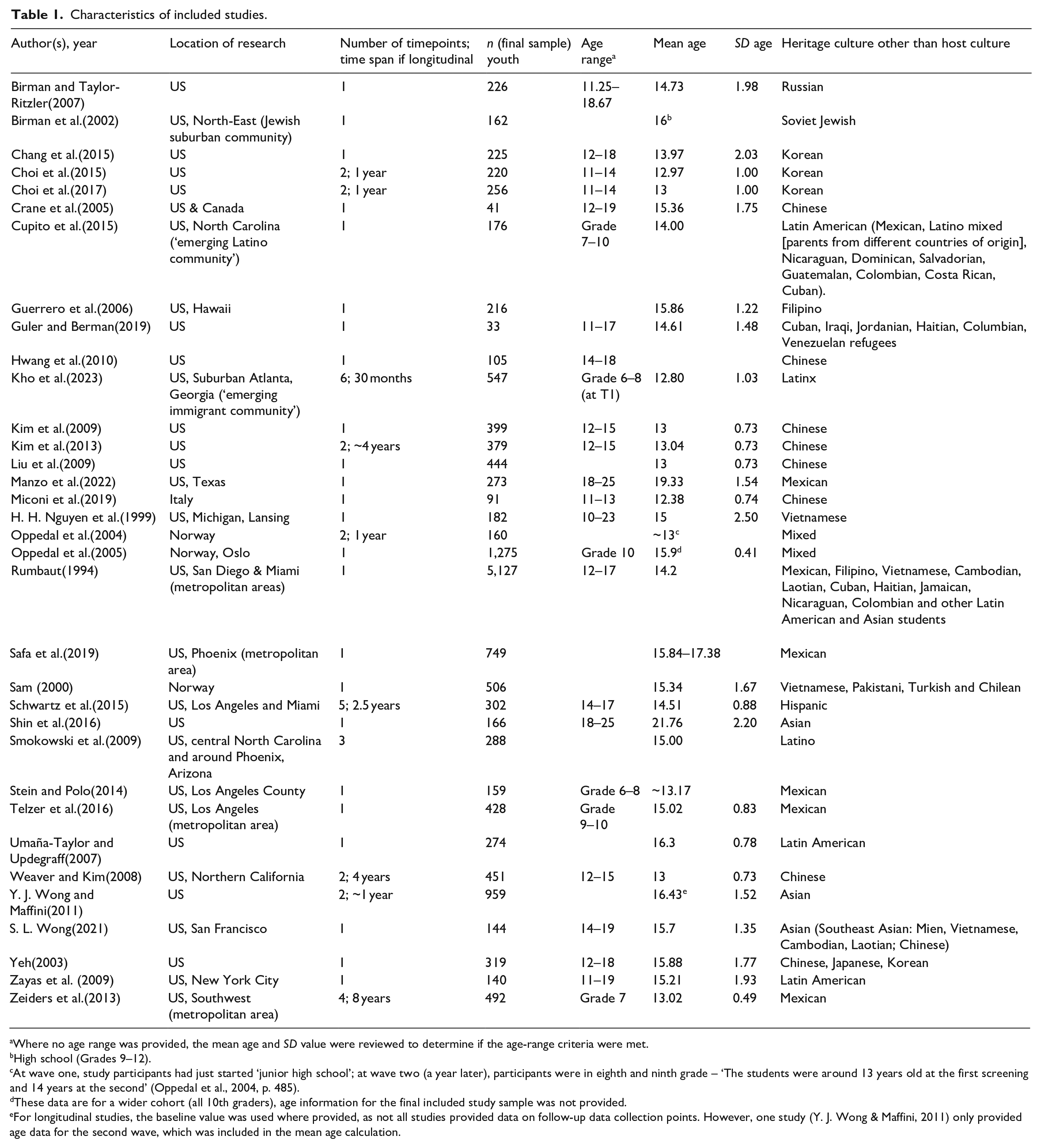
Where no age range was provided, the mean age and SD value were reviewed to determine if the age-range criteria were met.
High school (Grades 9–12).
At wave one, study participants had just started ‘junior high school’; at wave two (a year later), participants were in eighth and ninth grade – ‘The students were around 13 years old at the first screening and 14 years at the second’ (Oppedal et al., 2004, p. 485).
These data are for a wider cohort (all 10th graders), age information for the final included study sample was not provided.
For longitudinal studies, the baseline value was used where provided, as not all studies provided data on follow-up data collection points. However, one study (Y. J. Wong & Maffini, 2011) only provided age data for the second wave, which was included in the mean age calculation.
Scope, nature and focus
The 34 included studies had a combined total of 15,914 participants, with a mean sample size of 468 and a median sample size of 265. Across included studies which stated the samples’ mean age, the average mean age was 14.8 years. Thirty studies (88%) were conducted in the United States (US) (with one of these also including Canada), three studies (9%) were conducted in Norway, and one study (3%) was conducted in Italy. The 30 studies conducted in the US predominantly examined outcomes in adolescents with Asian (44.1%), and Latin American (32.4%) backgrounds.
Though all included studies measured cultural, or linguistic and mental health outcomes, they were heterogeneous in their research focus. Of those studies which included additional research foci, most (n = 20; 59%) looked at family functioning, specifically at how conflict or support relate to adolescent outcomes and how parent-adolescent relationships mediate the association between acculturation and adolescent mental health outcomes (e.g. Birman & Taylor-Ritzler, 2007; Choi et al., 2015, 2017; Crane et al., 2005; Guerrero et al., 2006; Kim et al., 2009, 2013; Miconi et al., 2019; Rumbaut, 1994; Schwartz et al., 2015; Shin et al., 2016; Weaver & Kim, 2008; Zeiders et al., 2013). Four studies (12%) focussed on mother-adolescent relationships (Liu et al., 2009; Manzo et al., 2022; Zayas et al., 2009), with one specifically focussing on acculturative family distancing (Hwang et al., 2010). Two studies investigated the ‘acculturation gap distress model’ with primary caregivers (Stein & Polo, 2014; Telzer et al., 2016), which suggests that children acculturate faster than caregivers, leading to the potential maladjustment of both. Beyond issues of family functioning, studies also tested theoretical concept validity (Sam, 2000), looked at social support (Oppedal et al., 2004), life domains (Birman et al., 2002) and interpersonal relationships in inner-city cohorts (S. L. Wong, 2021).
Mental health outcomes, scales and frameworks
The heterogeneity of included studies was also evident in the variety of mental health outcomes measured (see Table 2) and scales used to measure mental health outcomes. However, 14 studies (41%) assessed depressive symptoms employing the ‘Center for Epidemiologic Studies Depression Scale’ by Radloff (1977).
Mental health measures by study.
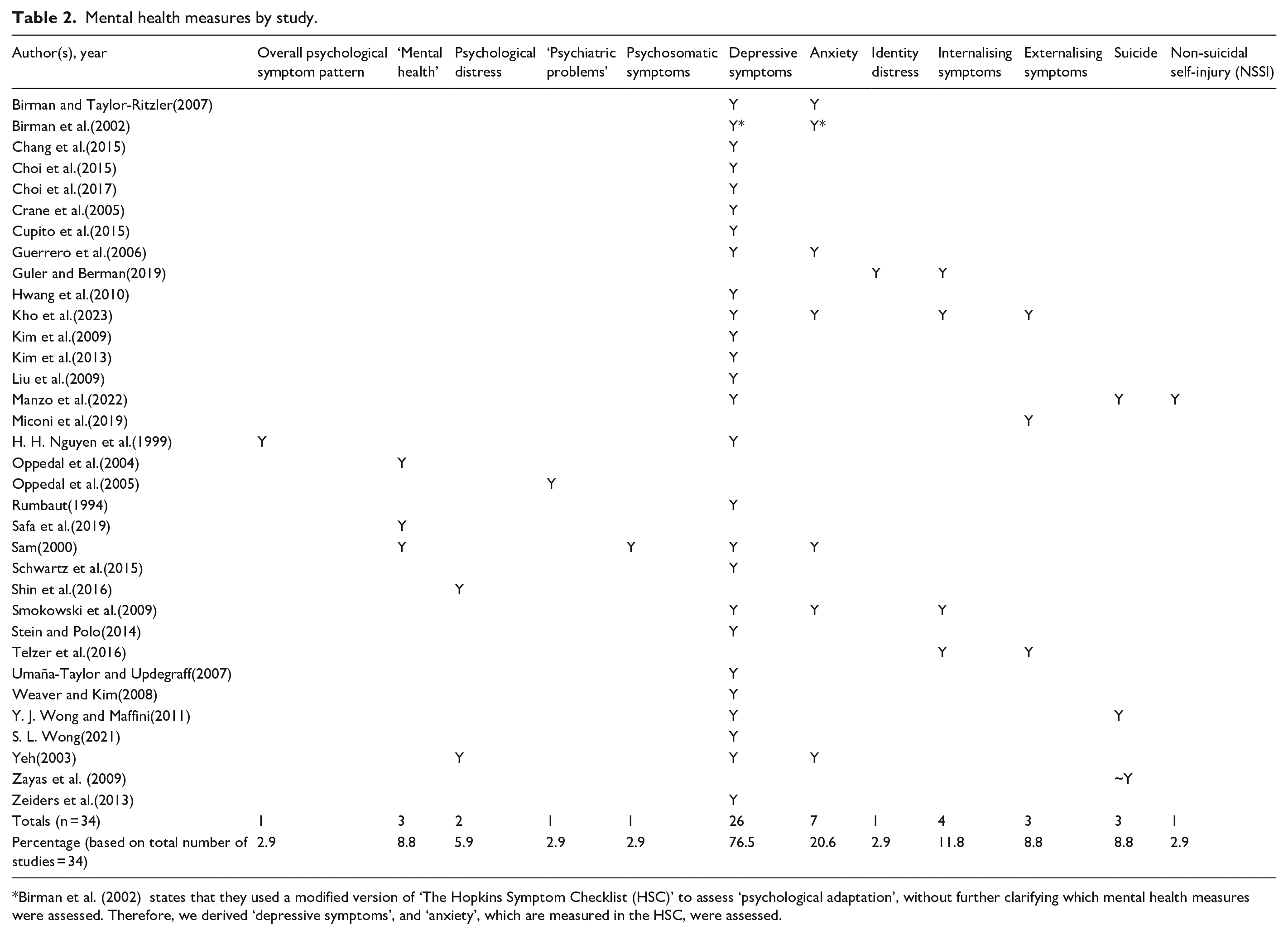
Birman et al. (2002) states that they used a modified version of ‘The Hopkins Symptom Checklist (HSC)’ to assess ‘psychological adaptation’, without further clarifying which mental health measures were assessed. Therefore, we derived ‘depressive symptoms’, and ‘anxiety’, which are measured in the HSC, were assessed.
Cultural and linguistic terminology, outcomes and scales
Terminology
Studies used different terms to describe the maintenance of heritage culture: 23.5% used enculturation (to the heritage culture) to distinguish it from acculturation (to the host culture) (Choi et al., 2017; Hwang et al., 2010; Kho et al., 2023; Manzo et al., 2022; Miconi et al., 2019; Shin et al., 2016; Telzer et al., 2016; Umaña-Taylor & Updegraff, 2007). However, some studies used acculturation to refer to the acquisition of heritage and host cultures (e.g. Birman et al., 2002; Birman & Taylor-Ritzler, 2007; Crane et al., 2005; Guler & Berman, 2019; Kim et al., 2009; Liu et al., 2009; Miconi et al., 2019). Furthermore, some studies used the term heritage culture (e.g. Kim et al., 2009; Miconi et al., 2019), while others used native culture (Birman et al., 2002; Birman & Taylor-Ritzler, 2007), or other terminology to refer to related concepts (e.g. Chang et al., 2015; H. H. Nguyen et al., 1999; Rumbaut, 1994; Safa et al., 2019; Smokowski et al., 2009), or a mixture of the above terms (e.g. Manzo et al., 2022; Schwartz et al., 2015; Telzer et al., 2016; Umaña-Taylor & Updegraff, 2007; S. L. Wong, 2021).
Scales
Studies used different, often modified scales to measure cultural orientations. Four studies (Birman et al., 2002; Birman & Taylor-Ritzler, 2007; Choi et al., 2015, 2017) used Birman and Trickett’s LIB scale (2001), measuring language, identity and behaviour; four (Hwang et al., 2010; Kim et al., 2009, 2013; Weaver & Kim, 2008) used the Vancouver Index of Acculturation (Ryder et al., 2000), measuring behaviour, participation, enjoyment and social affiliation; three (Kho et al., 2023; Manzo et al., 2022; Zeiders et al., 2013) used the Mexican American Values Scale (Knight et al., 2010).
Outcome measures
Studies derived adolescents’ cultural orientation from measures displayed in Table 3. Included studies predominantly appeared to assess host and heritage cultural orientation independently (bi-dimensional) on two separate scales, while relying on several cultural domains, with language, for example, just used as one indicator amongst others in assessing cultural orientation.
Heritage cultural and linguistic maintenance measures by study.
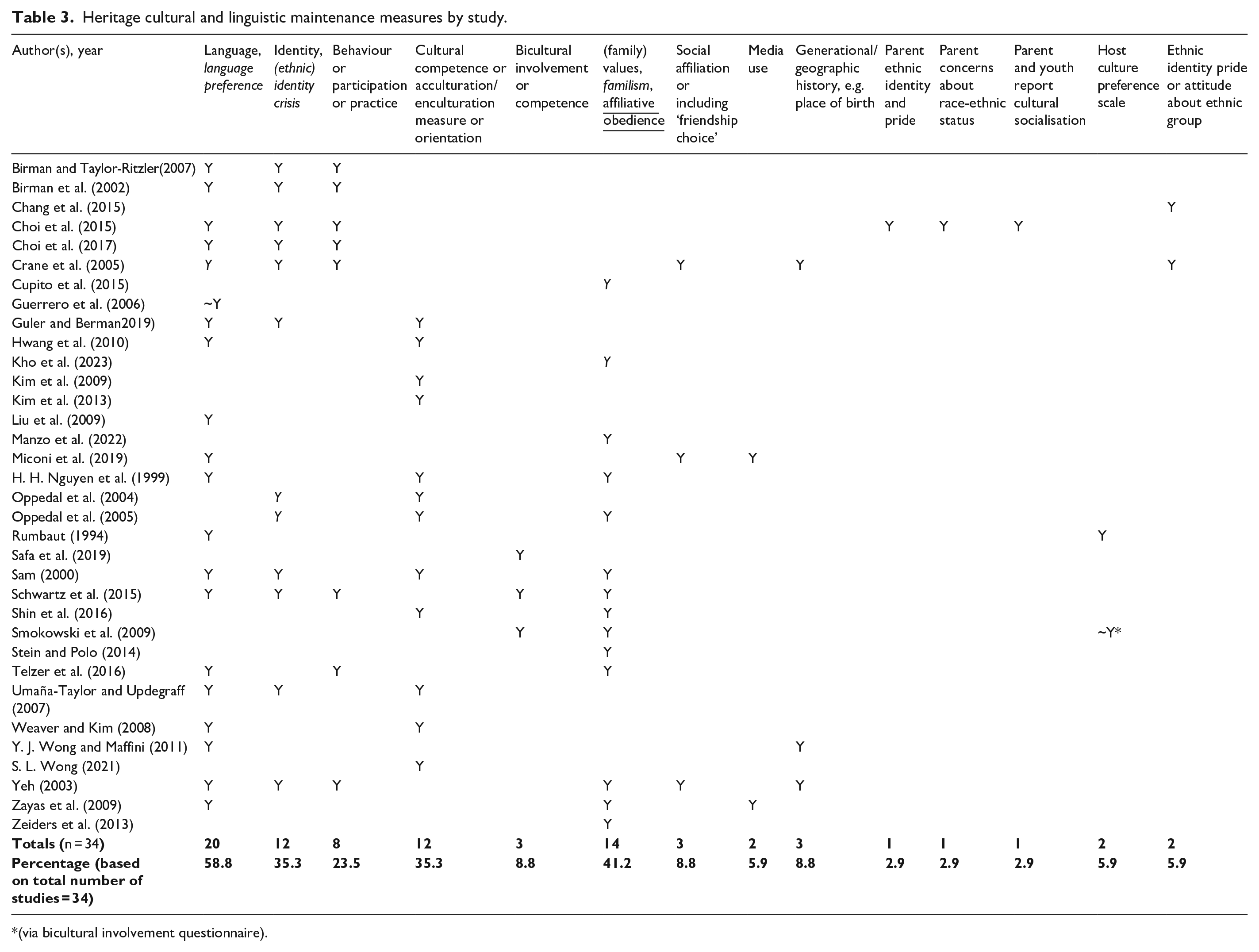
(via bicultural involvement questionnaire).
The association of cultural maintenance and mental health outcomes
Findings in response to our second question are collated in the Appendix (A2), as well as contextualised and discussed in the following section.
Discussion
This is the first scoping review to investigate the association between heritage cultural and linguistic maintenance and mental health outcomes among migrant adolescents.
Focus, scope and nature
Locations outside of North America were under-researched, with 88% of included studies conducted in the US. This finding is perhaps to be expected when it is considered that the US has – for more than 50 years – been the top destination globally for recorded migration, with more than 51 million documented international migrants residing in the US in 2022 (more than three times as many as Germany in second place, with 16 million international migrants) (McAuliffe & Triandafyllidou, 2021). However, despite the considerable imbalance in the number of international migrants in the US when compared to other countries, it was surprising not to identify more studies from outside the US. This may reflect the relative availability of resources between countries, as well as differing research priorities in different regions.
Almost all included studies (94%) have been published since 2000. This may reflect an increase in the prevalence of mental illness since this time (Bor et al., 2014), as well as the changing public perception of mental illness in recent decades, in response to large-scale mental health stigma reduction campaigns (Evans-Lacko et al., 2014; Henderson & Thornicroft, 2009). A systematic review of longitudinal cohort studies examining adolescent mental health trends before and after the year 2000 reported that, whilst the burden of externalising problems appeared to be stable over this period, most studies reported an increase in internalising problems in adolescent girls (but not boys) (Bor et al., 2014). The temporal spread of included studies also coincides with Berry and colleagues’ acculturation taxonomy, which was developed at the end of the 20th century. With an initial focus on adult migrants, this gave rise to studies looking at how cultural maintenance relates to adolescents’ mental health outcomes.
We identified considerable heterogeneity between study designs, sample sizes, age ranges, research foci, mental health and cultural maintenance outcome measures, which hinders the synthesis of findings. Our findings confirm the inconsistent use of terminology when referring to ‘cultural maintenance’, which has been previously identified (Kirshner & Meng, 2012, p. 1149). Some studies also failed to provide sufficient detail on the age range investigated (e.g. Birman et al., 2002; Y. J. Wong & Maffini, 2011).
With regards to cultural scales, the few studies which assessed host and heritage cultural orientation as part of the same scale, or assigned cultural orientation to adolescents using one domain (see Table 3), appeared less robust than other included studies, which independently assessed host and heritage orientation on separate scales, and used multiple domains to assign cultural orientation, respectively.
Framework
A number of included studies (e.g. Weaver & Kim, 2008; Yeh, 2003) found no evidence of Berry and Sam’s (1997) four acculturation strategies, and overall study findings did not support the claim that ‘integration usually leads to better outcomes’ (Berry, 1997, p. 24; cf. Rudmin, 2003). Instead, the heterogeneity of findings regarding the relationship of cultural maintenance and mental health outcomes supports the applicability of a developmental, ecological framework in which context is a primary consideration of analysis.
Despite issues of validity and practicability requiring further review, Pérez et al.’s (2021) ecological framework may provide a useful starting point to interpret findings [with some additions]:
(1) Global context (acknowledging ‘push-and-pull conditions’ affecting migration; ‘resettlement stress’; the effect of the climate crisis; post-traumatic stress disorder; ‘cultural stress’ which is comprised of discrimination, the context of reception and bicultural stress; cultural globalisation and remote acculturation (e.g. via mobile phones); ‘transnational ideologies’.
(2) Macrosystem context (acknowledges national and immigration policies; resettlement programmes; attitudes towards migrants [e.g. mass media, social services]).
(3) Microsystem context (acknowledges the neighbourhood, schools, families [peers, religious communities and health services]).
(4) Community cultural wealth (acknowledges ‘migration capital’, aspirational, linguistic, social, resistant, familial and navigational dimensions).
(5) Cultural adaptation (acknowledges cultural preservation and cultural restoration).
(6) Individual context (acknowledges foreign status, migrant farmworker status, undocumented status – (which may be Mexican-adolescent focussed in Pérez’ framework; but also sex, age, health, as well as existing protective factors and practices such as spirituality and religion [as identified by Wyatt et al., 2015]).
Heritage linguistic maintenance
Findings in relation to our second question about the association between cultural maintenance and mental health outcomes were highly heterogeneous and, at times, contradictory. A small number of studies report a direct association between heritage language maintenance and mental health outcomes (Guerrero et al., 2006; Liu et al., 2009). Other studies report an indirect relationship, specifically regarding heritage language proficiency being positively related to improved perceptions of the father (as part of the microsystem context), which in turn was associated with positive mental health outcomes amongst Asian-heritage cohorts in the US (Choi et al., 2017; Weaver & Kim, 2008). While some studies found bilingualism (i.e. proficiency in both heritage and host language) to be positively related to positive mental health outcomes (Choi et al., 2015, 2017; Liu et al., 2009), others only found this relationship for host – but not heritage – language proficiency (Rumbaut, 1994). In contrast, a number of studies, which all looked at cohorts with mixed heritage cultures, found no association between host or heritage language maintenance and mental health outcomes (Birman et al., 2002; i.e. Guler & Berman, 2019; Hwang et al., 2010).
Heritage cultural maintenance
Heritage cultural maintenance more broadly, was found to be protective for some adolescents (Smokowski et al., 2009; Telzer et al., 2016), especially refugees (Birman et al., 2002; Guler & Berman, 2019). Amongst Latin American cohorts, heritage cultural value maintenance, specifically, was found to be protective (Cupito et al., 2015; Kho et al., 2023; Zeiders et al., 2013). Amongst Asian cohorts, some studies found the association between heritage cultural maintenance and mental health to be mediated by improved adolescent-parent relationships (Chang et al., 2015; Shin et al., 2016), while others report it to be mediated through the association between discrimination and mental health outcomes (Umaña-Taylor & Updegraff, 2007). In contrast, other studies found host acculturation, but not heritage cultural maintenance, to be associated with reduced distress (e.g. Birman & Taylor-Ritzler, 2007; Oppedal et al., 2005; Sam, 2000; Yeh, 2003).
Biculturalism was associated with positive mental health outcomes in some studies. However, other studies did not find such a relationship, refuting the notion of there being an ‘ideal acculturation strategy’ for migrant adolescents, as these adolescents in the researched contexts were, for example, found to be pressured into exclusively orientating towards one culture in specific settings. Some studies report that when niches, such as school and community, do not appreciate an adolescent’s heritage culture, bicultural or heritage encultured, adolescents can suffer from poor mental health outcomes (Sam, 2000; S. L. Wong, 2021). Other studies which similarly found adolescents experiencing acculturative stress noted more depressive symptoms and suicidal ideation, possibly as they were ‘caught between cultures’ (Hovey & King, 1996).
Contextualising our findings
The findings of this review diverge from those of reviews investigating the association between cultural maintenance and mental health outcomes conducted amongst adult migrant cohorts, which found biculturalism to be generally associated with better psychological outcomes (e.g. Balidemaj & Small, 2019; A.-M. D. Nguyen & Benet-Martínez, 2013). Our findings promote a more nuanced understanding of this association, which mirrors Titzmann and Lee’s (2018) dynamic, development-focussed suggestions for acculturation research. It appears that adolescent’s cultural orientation must be understood as a dynamic, context-dependent, two-way process, which some included studies have attempted to capture (Birman et al., 2002; Chang et al., 2015; Guler & Berman, 2019; Kho et al., 2023; Miconi et al., 2019; Oppedal et al., 2004, 2005; Safa et al., 2019; Smokowski et al., 2009; Umaña-Taylor & Updegraff, 2007; Yeh, 2003). This is also in accordance with Delaruelle et al.’s (2021) findings, which also highlight the need of interventions to be ‘ecologically based’.
The central role family (microsystem) plays in adolescents’ acculturation and mental health was considered and investigated by 59% of included studies, with some exploring the ‘acculturation gap’ between parents and adolescents. Most of these studies report a host acculturation gap with parents to be associated with depressive symptoms (Crane et al., 2005; Hwang et al., 2010; Shin et al., 2016; Weaver & Kim, 2008). Other studies found heritage enculturation only to be related to less distress if positive family relationships are in place (Birman & Taylor-Ritzler, 2007; Choi et al., 2017; Oppedal et al., 2004). Previously mentioned studies also identified heritage language proficiency to be indirectly related to improved mental health outcomes, through improved parental (especially paternal) relationships (Choi et al., 2017; Rumbaut, 1994; Weaver & Kim, 2008). To an extent, these studies confirm a qualitative review’s finding that heritage cultural disruption and family conflict were linked to migrant adolescent depression (Rodriguez et al., 2024). A small number of included studies refuted the notion of a relationship between family and adolescent mental health outcomes (e.g. H. H. Nguyen et al., 1999, p. 25). Despite some contradictions, these findings highlight the important role family support as part of the microsystem appears to have on adolescent mental health (see also Berry, 2022; e.g. Chang et al., 2015; Guerrero et al., 2006; Rumbaut, 1994).
At the macrosystem level, the findings of the only study looking at Chinese-heritage adolescents outside of North America – in Italy (i.e. Miconi et al., 2019) – do not seem to align with those of a number of Chinese-heritage US studies. Miconi et al. (2019) found that adolescents who are more host acculturated than their parents are least likely to externalise problems, while US studies all found acculturation gaps with parents to be negatively related to adolescent mental health (Crane et al., 2005; Hwang et al., 2010; Kim et al., 2009, 2013; Weaver & Kim, 2008). This may exemplify how adolescents’ macrosystem, and different patterns of heritage culture perception in the US and in Italy, may affect the usefulness of different cultural orientations. However, this hypothesis requires further investigation.
Implications and future directions
This review provides several important implications for future research.
Firstly, we identified a dearth of research conducted in locations outside of North America, in particular low- and middle-income countries. Further, there is a need to standardise terminology (e.g. to distinguish enculturation from acculturation), the definition of adolescence (Sawyer et al., 2018), as well as cultural scales and mental health measures used.
There appears to be value in assessing adolescents’ cultural orientation and mental health outcomes dynamically, using, for example, longitudinal study designs and considering developmental aspects (i.e. puberty) of adolescence (e.g. age of migration, outlined by Titzmann & Lee, 2018). To appropriately measure cultural orientation, heritage language should be measured in conjunction with other (multiple) cultural maintenance domains using two independent dimensions (Rudmin, 2003).
Furthermore, family, and other ecological factors, appear to play an important role, possibly providing an explanation for between-location, group and gender differences identified between study findings. For an improved interpretation of what may be related to adolescent mental health outcomes, we highlighted the value of utilising an ecological framework which takes the contexts adolescents navigate into consideration. This scoping review has shown that there could be value in approaching the association between cultural maintenance and mental health outcomes by first gaining a better understanding of the cultural expectations, attitudes and demands adolescent cohorts should adhere to, to succeed in specific ecological contexts. Accordingly, what may be a protective factor for one cohort may present as a risk factor for another, depending on their ecological environment and the specific demands adolescents believe these have.
Considering an adolescent’s dynamic and context-dependent orientations and outcomes, culture should not be assumed to be homogeneous, but instead it could be idiosyncratic and could itself be affected by complex ecological processes, especially within multicultural societies (e.g. Usborne & de la Sablonnière, 2014). Further, none of the identified studies investigated how cultural values and beliefs relate to mental health outcomes (e.g. stigma) – a research gap also identified by others (Colucci et al., 2017). Accordingly, even though we only included quantitative studies, we suggest that future research takes an emic perspective, co-designing and testing its cultural measures’ appropriateness with study participants prior to conducting new empirical studies to avoid simplifying cultural bias (cf. Rudmin, 2003). The existing ecological frameworks should also be further examined and evaluated to ensure they are practical and provide a comprehensive account of an adolescent’s context.
None of the included studies examined ‘remote enculturation’, such as the role smartphones play in heritage cultural maintenance and mental health outcomes, which has for some time now been an important medium for adolescents’ cultural exchange (Anderson et al., 2023). This gap illustrates how much remains unknown about adolescents’ cultural maintenance and mental health outcomes.
Strengths and limitations
One limitation of our search was that we only used English search terms. However, relevant studies in other languages were reviewed by the second author who was proficient in them (French and Spanish), and none met our inclusion criteria. Another potential limitation was that we included broader search terms (e.g. ‘resilience’) than our inclusion criteria, to capture all eligible studies. This approach – going from broader to more specific – did not compromise the integrity of our approach. However, the identified heterogeneity of terminology this scoping review identified shows that there is value in adding terms (e.g. enculturation, native acculturation) in future systematic reviews.
Due to the highly varied nature of research results, which did not allow for a meta-analysis, we did not synthesise findings, and we cannot therefore generally summarise included studies. Our findings do, however, highlight the value of conducting scoping reviews to consolidate existing multidisciplinary research, gain clarity about approaches and future research needs, to enhance the understanding of migrant adolescent cohorts and develop more impactful intervention strategies in the future.
Conclusion
The evidence relating to the association between linguistic and cultural maintenance and adolescent mental health outcomes appears to be mixed in nature: some studies found a positive relationship, while others identified an indirect relationship, no relationship at all (highlighting the importance of host acculturation instead) or found adolescents to be ‘caught between cultures’. Importantly, research would benefit from a more standardised approach, while taking an emic perspective on culture and considering an adolescent’s complex and interrelated ecological and developmental factors. We encourage future research to be specific rather than generic, developing scales measuring levels of cultural maintenance that consider potentially global, as well as idiosyncratic concepts of culture, to better understand how cultural maintenance relates to migrant adolescent mental health outcomes.
Footnotes
Appendix
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Melbourne’s ‘Arts-MDHS Collaborative Research Initiative Seed Funding’, which provided funding in part. Rohan Borschmann receives salary and research support from a National Health and Medical Research Council (NHMRC, Australia) Emerging Leadership Investigator Grant (EL2; GNT2008073).