
Abstract
Background:
Women are disproportionately impacted by depression and anxiety disorders and in particular, women from minoritised ethnic communities experience inequalities in access to outcomes of psychological treatment for these disorders. Better understanding from the views of service users about the factors that impact their access to, and experiences of care could help to optimise treatment for these groups.
Method:
This study explored experiences of treatment and gathered suggestions about treatment improvement, from the perspectives of women currently using psychological therapy services. Semi-structured interviews were conducted with 12 female NHS Talking Therapies for anxiety and depression (NHSTTad) service users from minoritised ethnic communities. Data were analysed using thematic analysis.
Results:
Four high-order themes were identified: (1) cultural identity and experiences of mental health and treatment, (2) challenges associated with treatment, (3) facilitators of good treatment experiences and outcomes and (4) improvements for women from minoritised ethnic communities.
Conclusions:
Findings showed that cultural sensitivity and awareness are important to minoritised ethnic women receiving therapy. Challenges included access difficulties and limitations of treatment options offered, alongside personal challenges of engaging in therapy. Facilitators of good treatment experiences and outcomes included flexibility on the part of the service, as well as therapist-related factors such as identity characteristics (age, gender and culture of therapist), a good therapeutic relationship and the therapist’s ability to deliver person-centred care. Improvements included ensuring care is culturally sensitive, reducing waiting times or providing better support for people on waiting lists, providing a flexible service that takes individual needs into account, increasing workforce diversity and reaching out to underserved communities. Many of the suggested improvements are generalisable to underserved minoritised ethnic groups, regardless of gender and could be applied to other psychological therapies services other than NHSTTad.
Keywords
Introduction
The prevalence of common mental disorders (CMDs, such as anxiety disorders and depression) is higher in women than in men (Jenkins et al., 2021; Riecher-Rössler, 2017) and women are more likely to access treatment for these conditions (Office for National Statistics, 2022). However, access and treatment rates can also vary by ethnicity, with certain minoritised communities less likely to be assessed or treated for their mental health in some services (Harwood et al., 2023). Women from minoritised ethnic groups can experience challenges with mental health treatment due to a range of factors including cultural insensitivity on the part of health services, lack of access to appropriate mental health information or cultural expectations and stigma (Spaducci et al., 2024; Watson et al., 2019). Data from the UK has shown that women from South Asian, Black African and African-Caribbean communities have the highest incidence of CMDs but are less likely to receive care for them relative to White-British women (NHS Digital, 2022). Although access to mental health support is one area in which ethnic and gender discrepancies are evident, there are also differences in experiences (Bansal et al., 2022) and outcomes (Arundell et al., 2024) of treatment when it is received.
There are several proposed ways in which experiences of services may impact outcomes for service users from minoritised ethnic communities, for example, experiences of services can impact the way treatment is received, it’s efficacy and this can impact engagement and outcomes (Bansal et al., 2022). In particular, negative experiences and opinions about service failings may lead to lack of faith in services (Hamed et al., 2022), hindering compliance with treatment and therefore, symptom improvement (Bansal et al., 2022). Additionally, services may not be deemed culturally appropriate to meet the needs of specific individuals with shared characteristics (e.g. ‘non-White-British’ females) rendering them less effective for these groups (Kirmayer & Jarvis, 2019).
Work to tackle ethnic inequalities has included a focus on cultural adaptations to treatment which have been shown to benefit some minoritised ethnic groups (Arundell et al., 2021). Suggestions to improve treatment for minoritised communities have included cultural competence training for practitioners (Kirmayer, 2012; Kirmayer & Jarvis, 2019), improved mental health awareness (Bhui et al., 2015) and better service integration (Silverwood et al., 2019).
Qualitative methods allow researchers to obtain a deeper insight into the experiences of the population of interest (Chafe, 2017; Pope & Mays, 1995). Research exploring service users’ experiences of mental health care has helped towards understanding the experiences and challenges faced by minoritised ethnic communities (Memon et al., 2015; Van Bortel et al., 2022). However, few studies have focussed on the unique experiences and needs of women and recent studies about women from minoritised ethnic groups have tended to focus on perinatal mental health care specifically (Millett et al., 2018; Pilav et al., 2022). This paper aims to discuss improvements that could be made to psychological therapy services for anxiety and depression to optimise outcomes for women from minoritised ethnic communities, from the perspectives of service users.
Methods
Study design and theoretical framework
A qualitative study using semi-structured interviews was conducted with female service users belonging to minoritised ethnic communities. A contextualist approach (Braun & Clarke, 2006) was used to address questions about the experiences of NHS Talking Therapies for anxiety and depression (NHSTTad) treatment from the service user perspective. Interpretations should be considered within the perspective of the corresponding author, a female PhD candidate of mixed ethnicity with knowledge of ethnic discrepancies in mental health care. Reporting was in line with COREQ (Tong et al., 2007; see Supplemental File 2). The study adhered to the protocol (Arundell, 2021).
Setting
The study was conducted across two north London NHSTTad services provided by the Camden and Islington NHS Foundation Trust. The ethnic diversity of the boroughs served by the Trust (Office for National Statistics, 2023a, 2023b) made it an ideal choice within which to explore ethnic and cultural differences in experiences of mental health care.
Participants
Participants were recruited through the NHSTTad services using purpose sampling. To participate, service users had to meet the following criteria:
Belongs to a minoritised ethnic group (including Black, Asian, Chinese or any other minoritised ethnic group; i.e. ‘non-White-British’), including mixed ethnicity, White-other and White-non-British
Aged 18 to 65 years
Identifies as female or as a woman - Service users who self-ascribed their gender as ‘female’ or ‘woman’ were eligible to take part in the study. It is acknowledged that ‘female’ more accurately refers to biological sex (or the sex a person is ascribed at birth), while ‘gender’ tends to refer to socially constructed roles, behaviours and identities (Heidari et al., 2016). Both terms ‘woman/women’ and ‘female’ are used in this study to refer to people who identify with either or both terms.
Currently using NHSTTad services in Camden or Islington, having attended at least two therapist-led treatment sessions
English-speaking
Development of interview questions
Draft questions informed by contemporary literature were brought to the Black, Asian and Minority Ethnic (BAME) Staff Working Group at the Camden and Islington NHS Foundation Trust for discussion. A further draft was developed to incorporate the outcomes of this discussion, and this was then updated to draw on developments in cultural adaptations research (Arundell et al., 2021). The Trust’s Service User Advisory Group was invited to comment on language, flow of the questions and missing topics. A final set of interview questions (Supplemental File 1) was agreed between study authors.
Procedure
Identification of potential participants was performed via a search of the services’ databases of service users who had consented to be contacted about research opportunities. Before contacting them, each person’s named clinician was contacted to check if they had any concerns about inviting the service user. Potential participants were contacted by email or telephone by one researcher (L-LA) and were given a summary of the study. Those who agreed to receive further information were provided with the Participant Information Sheet. Consent was taken via an electronic form. Participants also provided their ethnic group, age bracket and how many sessions of treatment they’d received via form (study materials are provided in Supplemental File 1). Semi-structured interviews were conducted by one researcher (L-LA) between February and April 2022. Interviews lasted 40 min to 1 hr and were held, recorded and transcribed remotely using Microsoft Teams (Microsoft Corporation, 2022). Field notes were taken by the interviewer to support with prompts and to track the discussion. Anonymised transcripts were transferred to NVivo 14 software (Lumivero, 2023) for analysis. Details of the data management processes undertaken to ensure safe handling and storage of qualitative data to maintain confidentiality and integrity (including data anonymisation, storage and access) are provided in Supplemental File 1. Participants were compensated £15 for their time.
Data analysis
Analysis followed the stages of Reflexive Thematic Analysis (Braun & Clarke, 2006): (1) familiarisation with the data, (2) coding of the data, (3) developing meaningful patterns of data or ‘themes’, (4) refining themes, (5) defining themes and (6) writing up. A contextualist approach was used as this sits between the essentialist and constructionist approaches to thematic analysis, allowing for the acknowledgement of the ways in which individuals derive meaning and make sense of their experiences (Braun & Clarke, 2006). Therefore, this approach was appropriate to address questions about the experiences of psychological treatment from the perspectives of females belonging to minoritised ethnic communities. First, important segments within the text were identified and highlighted during data familiarisation (before interpretation). A codebook (Crabtree & Miller, 1992) defined from existing work on cultural adaptations (Arundell et al., 2021) was applied as a means of organising the text data for interpretation. Analysis took a hybrid approach of both inductive and deductive coding (Fereday & Muir-Cochrane, 2006) to embed interpretation of themes into existing knowledge whilst allowing for the establishment of new codes.
Stages of data coding
Stage 1: Developing the codebook
Six broad categories formed the codebook (Table 1).
High-level deductive codes developed for text analysis of service user interview data.
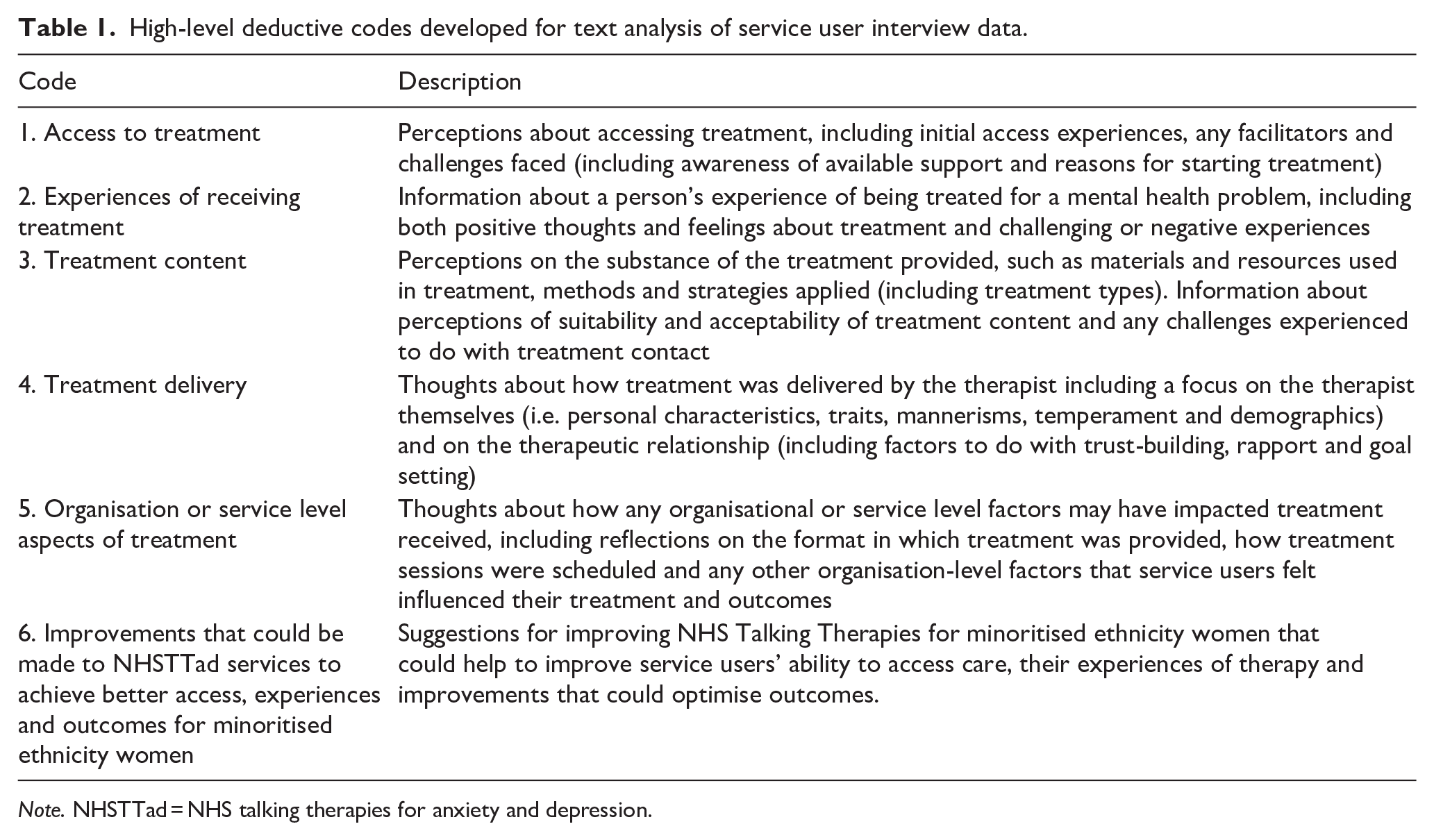
Note. NHSTTad = NHS talking therapies for anxiety and depression.
Stage 2: Testing the codebook
Two researchers (L-L, PB) independently applied the codebook (Table 1) to two randomly selected interview transcripts, to test use. Differences in conceptualisation of the data were identified and discussed. This led to the development of sub-codes to better organise the data within high-level codes.
Stage 3: Identifying and encoding important information
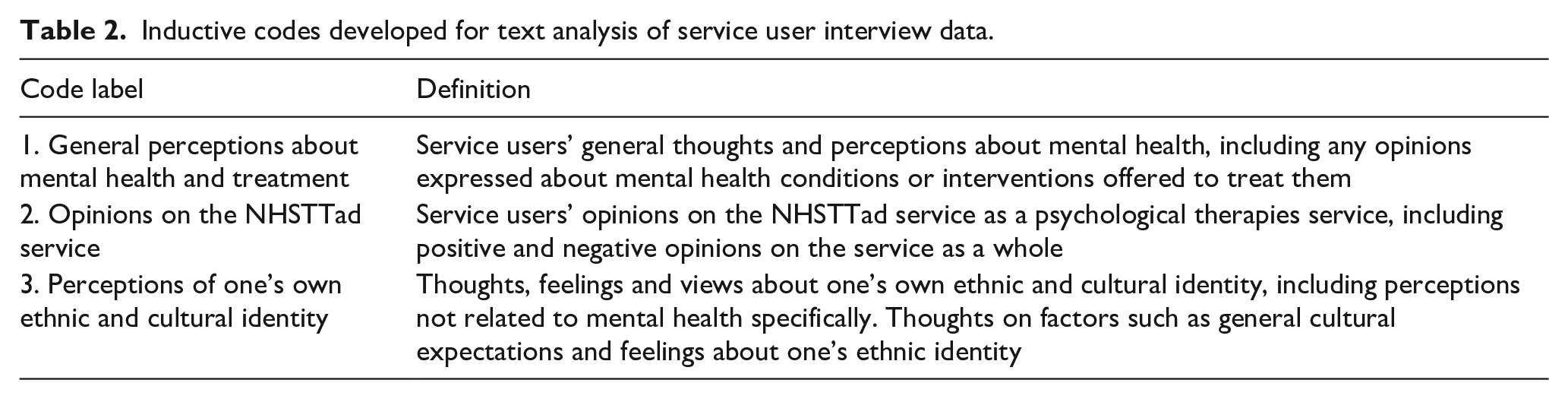
Codes were applied to the data using the six deductive high-level codes (Table 1). In addition, three high-level inductive codes arose from the data (Table 2).
Inductive codes developed for text analysis of service user interview data.
Stage 4: Applying the codebook and additional coding
Meaningful units of text were identified by applying both deductive and inductive codes to segments of text that represented the codes. Any additional relevant information or interpretation was highlighted using annotations.
Stage 5: Connecting codes and identifying themes
Codes were pulled together and used to derive themes – constructed patterns derived from the data to help meet the research objectives. Study authors discussed the themes and validated them using a portion of the data.
Ethics
This study received ethical approval via the Health Research Authority (HRA): Project EDGE ID: 138495XX; IRAS ID: 288406; Research Ethics Committee Reference: 21/SW/0094. The study protocol (Arundell, 2021) details the ethical and regulatory considerations undertaken, including assessment and management of risk to participants. The study was sponsored by the UCL/UCLH Joint Research Office (sponsor reference number: 138495). The Camden and Islington NHS Foundation Trust acted as a key collaborator for service user access, recruitment and management of the study but did not provide financial support.
Consent statement
All study participants provided written informed consent electronically. Participants consented to the inclusion of anonymised information (demographic information: ethnicity and age bracket).
Results
Twelve female service users took part. Six participants were aged 25 to 34 years (50%), four were aged between 18 and 24 years (33%) and two were aged between 35 to 44 years (8%) and 55 to 64 years (8%), respectively. Further characteristics are provided in Table 3.
Service user participant characteristics (n = 12).
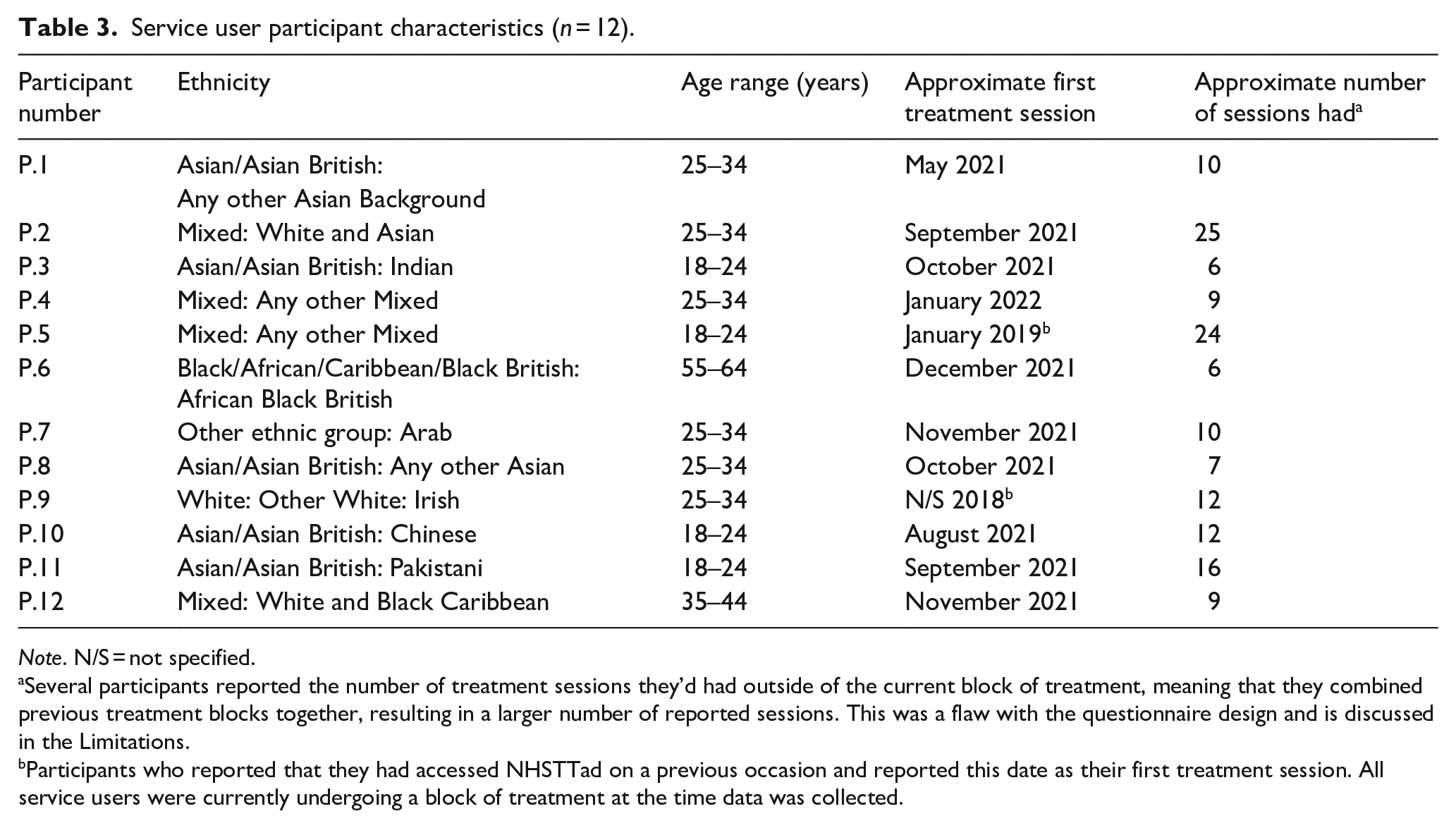
Note. N/S = not specified.
Several participants reported the number of treatment sessions they’d had outside of the current block of treatment, meaning that they combined previous treatment blocks together, resulting in a larger number of reported sessions. This was a flaw with the questionnaire design and is discussed in the Limitations.
Participants who reported that they had accessed NHSTTad on a previous occasion and reported this date as their first treatment session. All service users were currently undergoing a block of treatment at the time data was collected.
Themes
Theme 1: Cultural identity and experiences of mental health and treatment
Service users made reference to differences in how mental health is viewed across cultures:
People just saw it as. . .like you know, it’s almost crying. They’re being very dramatical and making things up. Yeah, I think mental health is not like, especially in a lot of cultures, is not seen as a real thing. [P.5]
Stigma was something service users often attributed to culture, expressing that in some cultures, including their own, mental health was not taken seriously or that problems were not understood:
I think, you know, even admitting that you. . .have mental health issue. It’s just such a stigma. You are seen as weak and it took me a long time accept. . . to accept my mental health status and, and then you know and even till today like you know my extended family didn’t accept it. . .Why is this such a scary thing for people in my culture? [P.1]
Service users highlighted the importance of therapists showing cultural sensitivity and awareness of cultural differences when treating women from minoritised ethnic groups:
I see the fact that he’s been really. . .open minded and understanding because I’m South Asian. So sometimes I find family dynamics and problems as such, like, do not resonate with lot of people who are not South Asian. . . [P.8]
Interestingly, although service users often spoke about cultural sensitivity and awareness on the therapist’s part, many did not report that cultural adaptations were made for them. This was not conveyed as something that people considered their treatment to be lacking, but that they did not feel that explicit cultural adaptations were necessary for them (Figure 1):
I didn’t [require cultural adaptations] and I guess that kind of shows how I feel like the system’s probably set up for people like me as in English speaking. . .There wasn’t anything that she needed to do. . . [P.2]
‘Cultural identity and experiences of mental health and treatment’ and second-order themes.
Theme 2: Challenges associated with treatment
A long wait was often the first thing participants reported when asked about challenges with accessing NHSTTad treatment:
. . .there was a huge delay from the time the referral was done back in May till I got my first session in November. . .So the GP referred, and I didn’t hear back until November. [P.12]
However, it should be noted that not all service users’ experiences of waiting times were the same. Some reported waiting a long time for assessment, followed closely by a treatment session after not much time, while others reported having an assessment very quickly, but having to wait a long time to be seen for treatment. Experiences varied considerably but wherever there was a short wait, this was viewed positively (Figure 2).
‘Challenges associated with treatment’ and second-order themes.
Another challenge was the limited support offered whilst waiting to begin therapy. While people did reference offers of self-help information or group sessions, this was either seen as insufficient:
. . .if you’re struggling, there’s like these videos online. . . on their website or something, they were useless. . . it was too general. . . so the information I can find from anywhere. . .. [P.5]
The amount of time given per session was often seen as insufficient and as such, this posed a challenge for service users:
. . .only having like half an hour session. . .I think with the treatment that I had because it was half an hour, she had to follow a very rigid structure. . .And that just felt like it took up a lot of time [P.3]
It was often the case that service users felt they needed more sessions or that they had not managed to work through everything they had wanted to:
. . .I guess it’s not, you know, a longer process. . .it’s not a program that’s meant to continue along with you. So, I guess there’s very much like goals that you intend to complete throughout the- the end of the program, but you know, obviously mental health issues like, continue. [P.10]
Some of the most common challenges expressed by service users related to their own personal challenges of therapy, such as the fact that talking about their mental health problems was difficult in itself:
In terms of the help for me it’s been OK, the only thing I would say that could be negative is just that the actual program itself like there are some parts that become difficult because of the nature of what is being spoken about. . . I think it’s more like revisiting memories I didn’t really want to revisit. That was the hardest part of it. [P.4]
Theme 3: Facilitators of good treatment experiences and outcomes
Developing a good therapeutic relationship between the service user and the therapist was thought to rely on several factors, including the therapist’s ability to establish a sense of trust with the service user:
. . .I think she was very. . . open and honest. . .and that obviously then made me trust her. Like obviously I was holding back a little bit because it was just a difficult subject. But actually, her explaining that ‘yes, it will be difficult’. . .preparing me for what each session was gonna hold, I suppose did help with trust. [P.9]
The temperament and manner of the therapist was also seen as a facilitator to trust-building and therapeutic rapport:
She was just very warm and empathetic. Curious. . . It felt very. . .really just like very patient centred like about me. . .I feel like she cared. . . [P.2]
Being non-judgemental and open-minded were therapist traits that service users reported helped them to feel comfortable during treatment:
Having some help from her was really good and then she was just like completely judgment free. It was amazing. . . [P.3]
Open-mindedness of the therapist was especially valued when there were clear cultural differences between the therapist and the service user:
You know, there was a point where I was confused about having a boyfriend or just going for arranged marriage, and I was really glad that she looked at arranged marriage with an open mind because she didn’t view it as a bad thing. . .it’s something people mix up with forced marriage. . .she made me feel really good. [P.11]
Perceived relatability of the therapist was another factor considered by service users to impact the therapeutic relationship. Interestingly, this was closely tied to the therapist’s personal identity characteristics:
You know, maybe the fact that she was younger. . . and you know, more relatable did kinda reassure me. . . it did feel a bit more relatable. . . [P.10]
Gender was considered one of the most important factors for service users:
. . .definitely the fact that she’s a female. . .. just feel like [therapist’s name] being female definitely was helpful. . .I think if it was like a White male [it] would have been very different. [P.1]
Having a female therapist was considered particularly important for service users who expressed negative or traumatic past experiences with males:
. . .’cause mostly the topics that I tackle are things that are related to like, maybe sexual trauma, let’s say or like anxiety that are triggered-triggered mostly by like events that happened with the male. . . and I feel like it’s very much easier for me to speak about that with the female. [P.7]
In some cases, the therapist having a similar cultural or ethnic background to the service user’s was considered a facilitator:
I think I trusted her because she was like a young woman of colour. . .She reminded me of, like, a family friend that I have to be honest. . . And then being. . .South Asian as well also helped. . . [P.3]
Flexibility in scheduling sessions was considered particularly important to service users:
She was very flexible with me. And, you know, when I had to cancel a session, like the session was gonna be Tuesdays to begin with, she was able to meet with me later on in the week. . . [P.12]
Flexibility in treatment format (remote or face-to-face) was also considered a facilitator to engagement:
I was open to remote appointments. Initially I didn’t realise how different and more effective it would be to do face to face and I guess she did for me. Yeah, but she basically she accommodated my, obviously, my preference to do face to face and I do face to face sessions now as opposed to remote sessions. . . [P.4]
Service users appreciated when they were given the option of longer or additional sessions (Figure 3):
We were supposed to stop at six [sessions], but I wasn’t feeling very mentally well, so we extended to seven. . . [P.8]
‘Facilitators of good treatment experiences and outcomes’ and second-order themes.
Theme 4: Improvements for women from minoritised ethnic groups
This theme was broken down into second- and third-order themes for deeper exploration and to extract and focus on actions that service users suggested could improve treatment for women from minoritised ethnic groups (Table 4; Figure 4).
‘Improvements for women from minoritised ethnic groups’ – second and third-order themes.
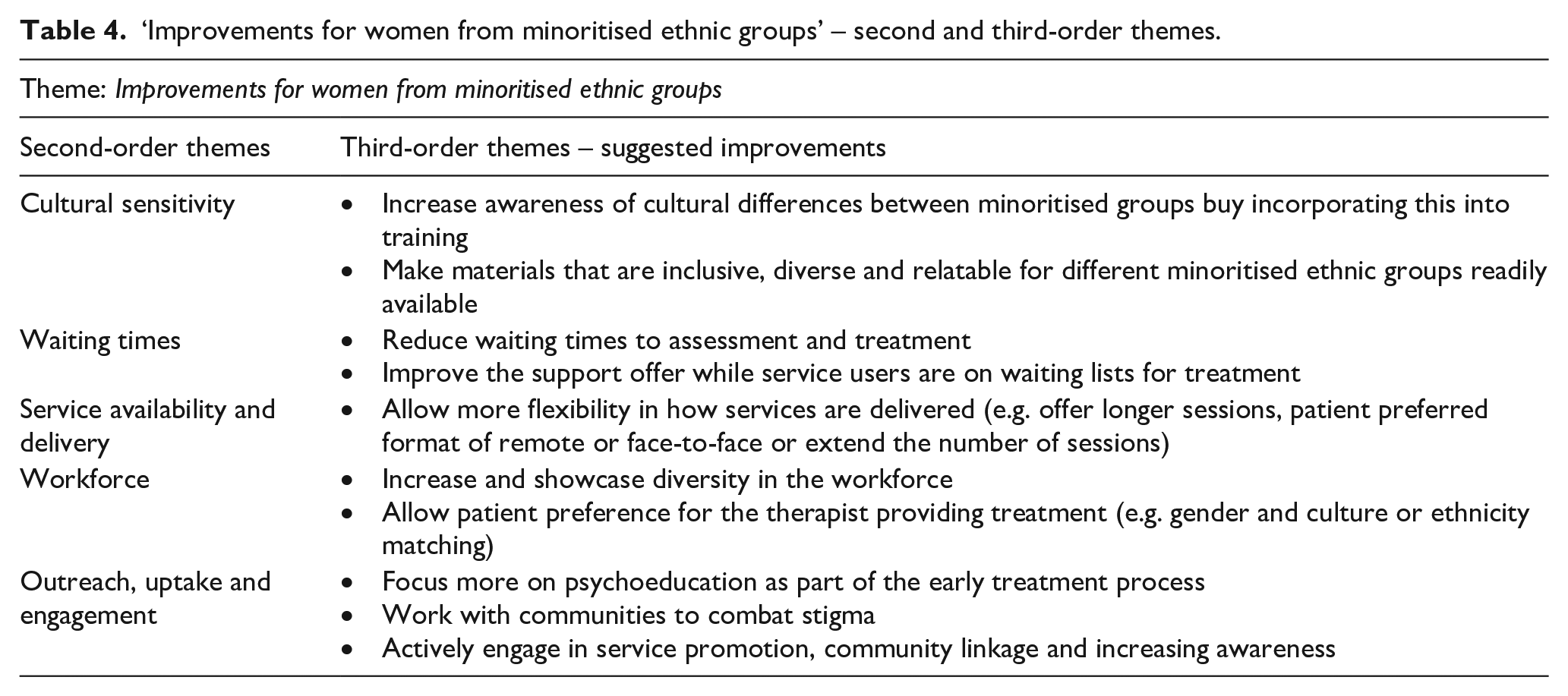

‘Improvements for women from minoritised ethnic groups’ and second-order themes.
Cultural sensitivity
Awareness of cultural differences between minoritised ethnic groups was something that service users felt could be improved:
I think that they need to get [an] understanding of our culture and one big misconception about us being Black is that because we’re Black, we’re all the same. . . you have to understand that a woman from Nigeria has different culture than a woman from Kenya, or a woman from South Africa, or a woman from America, or. . .a Black woman from the Caribbean. . .Yes, we may all have Black skin, but we all different, as our shades are different, so is our culture. [P.12]
Making sure materials and resources used in treatment are culturally appropriate and relatable to service users from diverse backgrounds was suggested:
. . . even examples that are used, you know when you’re reading about like what may be a worry would be or what like a low thought like having maybe more culturally related- it’s hard to like also not do a stereotype. . .you have to do it in a way that it’s not stereotypical. . . that feels relatable. [P.2]
Waiting times
Reducing waiting times was a commonly suggested improvement:
Honestly, I think just having. . .having less wait time. . .would make it. . .easier for people to join and more accessible and just kind of-of knowing that you could get an appointment within maybe a month or two. . . would be such a big, big difference [P.10]
Improving the offer of support whilst people are waiting for treatment was also suggested:
I think even if there is a long waiting list, there should be sort of maybe once every two months, have a call with a therapist or something like that. Just so. . .they can sort of give you other resources to use and like help you make a plan. . .just like once every two months seems reasonable for the people who are waiting. [P.5]
Service availability and delivery
A constant recommendation was around offering more sessions where service users felt this was needed:
I think I maybe would have preferred to have like. . .a couple of additional sessions. . .even just to have like a follow up call booked ‘cause I just kind of felt like it was really, really intense and we worked on so much stuff and then all of a sudden it was just over. . .’ [P.9]
Being able to request either remote or face-to-face treatment based on their preferences was suggested. While some service users reported receiving the offer of either treatment format, this was not consistent. Service users who were given this choice and flexibility expressed how much this was appreciated, while service users who were not expressed that they would have liked to have a choice:
. . .it was all done over the phone. We did have one or two sessions towards the end that were video call just It was. . . just a bit more of like a chat, then-maybe if it was on video, it would have felt a bit more structured or that would have added to it. [P. A9]
Workforce
Service users expressed that a more ethnically diverse workforce was key to improving experiences of care for women from minoritised ethnic communities:
I guess the simplest answer is having therapists whose [sic] from very different backgrounds. I think. . . Oh, if they had more, you know therapists of a diverse ethnic minorities. [P.1]
Service users suggested that therapists from minoritised communities themselves might be better placed to understand the struggles of minoritised ethnic service users, than White therapists:
I’m saying I think if I had, for example. . . a therapist who is from my same. . . who comes from the same place that I do, maybe it would have been very much easier to speak to now think about it. [P.7]
While several service users did appreciate seeing a therapist with whom culture was shared, this was not always what people wanted, recognising how culture matching may not be suitable for some people:
Maybe someone wouldn’t be comfortable in speaking with the other person like. . .their therapist coming from the same background that they are because it’s very personal. . .Because maybe someone would say ‘I don’t want them to be from my cultural background.’ [P.7]
As such, service users expressed mixed views as to whether ethnic or culture matching should be used as a strategy to improve experiences for women from minoritised ethnic communities:
But obviously if they’re paired up with-I can’t. . .it then goes into a tricky area of like, do you pair them up based on their ethnicity and religion? [P.1]
. . .if. . .they had more. . . therapists of a diverse ethnic minorities who. . .depending on whether it was relevant, could uh be assigned the patients, so, of that ethnic minority. . . that would be really helpful. [P.10]
Several service users suggested that services ask about preferences of the therapist’s gender:
. . .I don’t think I was asked for this, but I think they should, specifically at the bare minimum, ask about if they have a preference for gender. [P.11]
Outreach, uptake and engagement
Several suggestions focussed on outreach and promoting the service to increase awareness of its existence in communities of women who are underserved:
I mean, yeah, like going into those spaces, I suppose. So, kind of reaching out. . .. but making those links with communities. [P.2]
Psychoeducation was another suggestion linked to outreach, as service users felt that combined with a lack of awareness of treatment available, sufficient information about mental health or treatment options was lacking:
I think educational need, 100%, raising awareness for therapy is very much [sic] important. . . [P.7]
The need for services to contribute to combatting stigma was raised:
Why is this such a scary thing for people in my culture? And I think how to kind of get rid of. . .you need to remove the barrier. Well, people from my culture- you need to kind of get rid of that stigma first. . . [P.1]
More detail of themes, sub-themes and supporting quotes is presented in Supplemental File 1, including a Supplemental fifth theme ‘Reasons for seeking mental health treatment’.
Discussion
This study presents a qualitative exploration of the experiences of women belonging to minoritised ethnic communities who have received psychological treatment. The findings resonate with existing cultural sensitivity and mental health service improvement literature and add valuable contributions about actions mental health services could take to improve care.
Service users recognised the influence of culture on perceptions of mental health, help-seeking and treatment (Altweck et al., 2015; Bernal et al., 2009; Byrow et al., 2020) and made suggestions about improving cultural sensitivity on the part of clinicians. Culturally sensitive treatment and specifically, the importance of having a culturally competent therapist (Kirmayer, 2012; Kirmayer & Jarvis, 2019) was emphasised. Consistent and regular training for therapists was suggested as a way to improve cultural competence. Service users also suggested improvements such as ensuring materials and resources used in therapy are culturally appropriate (Beck et al., 2019). Interestingly, there was very little discussion about explicit cultural adaptations to treatment content. This is likely due to the fact that none of the service users interviewed reported that explicit cultural adaptations had been made because it was not necessary for them. For example, service users did not focus on language translation, and this is probably because none of them needed it, being fluent English speakers. It was apparent that participants understood the potential influence of culture on the therapeutic process given that they emphasised the importance of cultural competence on the part of therapists and services, as well as the use of culturally inclusive therapeutic resources. Exploration of how specific cultural elements influence the therapeutic process, building on the findings from the current study, could be helpful for future research, to examine more deeply how practices recommended in cultural competence frameworks align with service users’ experiences.
Service users placed much emphasis on service delivery and wider organisational factors linked to their experiences. The potential negative impact of a long wait to access mental health services on wellbeing and outcomes is well-documented (Clark et al., 2018; Reichert & Jacobs, 2018) and service users’ responses corroborated this, with several reporting that waiting to access assessment or treatment was challenging. While official reporting shows the percentage of people accessing services within 6 weeks of referral ranged between 90% and 92% between 2020 and 2023 (NHS Digital, 2020, 2022, 2023), service users in the current study often reported waiting longer than this. Even in cases where treatment was received within six weeks, service users in distress may still have still felt that this was too long. Limited support for people whilst on the waiting list led to suggestions about informal support from services whilst waiting.
Improvements arose regarding service availability and delivery. Many service users felt that 30-min per session was too short. Therapists are permitted to modify session lengths in cases where pacing or language interpretation might be required (National Collaborating Centre for Mental Health, 2024) but many service users felt this would also have benefited them even though they did not have these specific needs. Service users also reported feeling that the number of sessions offered was too few. On average, a person will receive eight sessions of treatment through NHSTTad (NHS Digital, 2023), yet service users felt that services should provide more where requested, and one specific improvement suggestion was that services could offer follow-up ‘check-in’ sessions on top of the treatment block. Studies have shown that increasing the frequency of treatment sessions (i.e. having twice-weekly compared to once-weekly sessions) can lead to significant decreases in depression symptoms (Bruijniks et al., 2020).
Preference for treatment format (i.e. online, telephone or face-to-face) varied and there was no clear consensus on the ‘better’ option. This finding emphasises the value in seeking service user preferences (Liberati et al., 2021; National Collaborating Centre for Mental Health, 2024) given that preference for format may depend on the individual and their circumstances. This finding should also be considered with regard to the timing in which the study was conducted; the COVID-19 pandemic altered how treatment was provided and may have impacted service users’ thoughts on remote vs. face-to-face care.
Workforce improvements included increasing the workforce diversity, linked to service users’ views on the value of diversity of experiences and knowledge on the part of therapists, and the perceived relatability of therapists from minoritised ethnic communities. Service users reported that facilitators of a good experience included a good therapeutic relationship (Benish et al., 2011) and the establishment of trust (Wampold, 2015; Wampold & Budge, 2012). Perceived relatability of the therapist (based on characteristics such as age, ethnicity and gender) was reported to impact the development of the therapeutic relationship. Although research exploring the benefits of gender matching in psychotherapy is inconclusive (Bhati, 2014; Schmalbach et al., 2022), the gender of the therapist was considered particularly important to, with several service users reporting that having a female therapist was essential, particularly when they had experienced past traumatic experiences with men. Views on the ethnicity and culture of therapists were more varied in that some service users reported that having a shared or similar ethnic or cultural background would be considered a facilitator, whilst others reported the opposite. In cases where this was considered a facilitator, this was often linked to perceptions about shared experiences and subsequent feelings of trust. However, research shows the effects of ethnic matching to be highly variable (Cabral & Smith, 2011). While some service users felt that people seeking mental health treatment should be able to express preferences about the therapist, there was no consensus on whether ethnicity- or culture-matching would be beneficial.
Improvements to support uptake and engagement for underserved groups of minoritised ethnic women included dedicated community outreach and service-led efforts to increase awareness, promote the service and to reduce barriers to treatment (Alegría et al., 2016). Psychoeducation both on the part of services and also on wider education systems (Lee-Tauler et al., 2018) was considered important to encourage help-seeking in communities where mental health might be stigmatised.
Although the current study focussed on women, many of the challenges of help-seeking and engagement mirrored those reported in studies of men from minoritised ethnic communities (Alam, 2023). As such, many of the suggestions made for improving treatment for women are likely to be generalisable across genders and as such, the findings have the potential for clinical application and utility beyond the demographics of the study’s sample. A series of recommendations for practitioners and services arising from the study findings, is provided below.
Limitations
The sample was limited to 12 participants of which the majority (83%) were aged 18 to 34 years. This young sample risks the generalisability of experiences across the lifespan as the study was not able to adequately capture the experiences of older adults. Although the recurrent emergence of themes suggested data saturation was reached, inclusion of older participants may have presented additional views, especially regarding generational differences in perceptions of mental health. The limitations of the generalisability of findings to services with starkly different population demographics should be noted; service user experiences and mental health outcomes may vary in regions where minoritised ethnic populations are proportionally smaller (Bécares et al., 2018; Das-Munshi et al., 2019). Participants were also required to speak English, limiting the exploration of language interpretation issues. None of the participants interviewed required any explicit cultural adaptations, despite reporting occasions where it was clear the therapist was practicing culturally sensitive care, limiting exploration of the impact of explicit cultural adaptations on experiences.
Using the questionnaire, several participants reported the number of sessions they’d had outside of the current block of treatment, meaning that they combined previous treatment blocks together, resulting in a larger number of reported sessions. This flaw with the questionnaire design skewed the reported number of sessions for each participant. Participants were invited to input on early interpretation of findings and identified themes but none responded to this request. As such, themes were not verified with participants, limiting validation of interpretation of findings. Interviews were conducted remotely due to COVID-19 restrictions when the study was designed. While remote interviews provide several benefits such as accessibility and efficiency, they may yield different findings than face-to-face interviews (Lobe et al., 2022). While thematic analysis was appropriate for this work, the use of methods such as framework analysis, might be considered for similar studies in future to structure themes systematically. Finally, additional methods, such as observational studies or focus groups to capture a broader range of experiences and further validate findings were not possible for this study but would have been useful to complement interviews, provide a richer dataset and triangulate findings. Future research using these methods is recommended.
Conclusions
This study contributes to existing evidence about improvements to psychological therapy services to provide better treatment for women belonging to minoritised ethnic communities by providing examples of practical actions services could take to improve care and optimise outcomes, from the perspectives of service users. The study emphasises the importance of culturally sensitive care and identifies some of the challenges and facilitators associated with delivery of treatment to minoritised communities. Most importantly, the study outlines improvements that services could make at the treatment delivery, treatment content and wider organisation levels to optimise experiences and outcomes. There was consensus that taking service user preferences into account, in terms of therapist gender, as well as treatment format, is key. This necessitates a stronger focus on workforce diversity and flexibility of service delivery. Outreach and increasing awareness in underserved ethnic communities of women was also considered vital to tackle access and engagement disparities. Many of the suggested improvements are generalisable to underserved minoritised ethnic groups, regardless of gender and could be applied to other psychological therapies services other than NHSTTad.
Recommendations for practitioners and services arising from the study findings
Psychological therapy services could improve the provision of culturally sensitive care by ensuring that culturally appropriate materials and resources used in therapy are easily available and accessible. Services could also seek to improve therapists’ awareness of cultural difference through more consistent, regular and updated cultural sensitivity and competence training.
Services should introduce or re-introduce strategies for community outreach to engage with communities, increase awareness of psychological treatments available and to combat stigma.
Services could set out to improve workforce diversity in areas where this might be lacking and explore avenues for diversifying the ethnicity of the workforce by looking at barriers to a career in psychological therapy that might be preventing people from minoritised ethnic groups choosing this as a career option.
Given the well-recognised challenges associated with reducing waiting times (high demand and resource constraints), services could explore other options to provide additional support for people on waiting lists. This could include a focus on increasing the workforce or supporting services to set up and trial short ‘check in’ appointments or notifications to provide reassurance and support to service users who are struggling with their mental health and awaiting formal support.
Services should ensure that provisions are in place to allow for flexibility in care delivery. Services should be equipped to support a range of different formats of therapy and service users should be provided with choice about whether they would prefer to receive treatment in-person, via video call or by telephone. Additionally, services should empower and enable therapists to extend or change the number of sessions provided if this is deemed necessary and appropriate for the individual service user. Service users should be made to feel comfortable and confident in requesting additional support where they feel it is needed so that this can be considered as part of their treatment package. With regard to preference of the therapist, as above, services might look to explore how gender matching female service users with female therapists might influence experiences and outcomes.
Supplemental Material
sj-docx-1-isp-10.1177_00207640241270800 – Supplemental material for Exploring perspectives on how to improve psychological treatment for women from minoritised ethnic communities: A qualitative study with service users
Supplemental material, sj-docx-1-isp-10.1177_00207640241270800 for Exploring perspectives on how to improve psychological treatment for women from minoritised ethnic communities: A qualitative study with service users by Laura-Louise Arundell, Rob Saunders, Phoebe Barnett, Judy Leibowitz, Joshua EJ Buckman and Stephen Pilling in International Journal of Social Psychiatry
Supplemental Material
sj-docx-2-isp-10.1177_00207640241270800 – Supplemental material for Exploring perspectives on how to improve psychological treatment for women from minoritised ethnic communities: A qualitative study with service users
Supplemental material, sj-docx-2-isp-10.1177_00207640241270800 for Exploring perspectives on how to improve psychological treatment for women from minoritised ethnic communities: A qualitative study with service users by Laura-Louise Arundell, Rob Saunders, Phoebe Barnett, Judy Leibowitz, Joshua EJ Buckman and Stephen Pilling in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The study authors would like to thank the participants who took part in the study. We also thank the members of the BAME Staff Working Group and the Service User Advisory Group at the Camden and Islington NHS Foundation Trust for their support in developing the interview questions.
Author contributions
Laura-Louise C. Arundell: Conceptualisation, Methodology, Validation, Formal analysis, Investigation, Data curation, Resources, Writing – original draft, Visualisation, Project administration. Rob Saunders: Conceptualisation, Methodology, Writing – review and editing, Supervision. Phoebe Barnett: Validation, Formal analysis, Writing – review and editing. Judy Leibowitz: Conceptualisation, Methodology, Resources, Writing – review and editing. Joshua Buckman: Conceptualisation, Methodology, Writing – review and editing. Stephen Pilling: Conceptualisation, Methodology, Validation, Resources, Writing – review and editing, Supervision.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors and was developed as part of the corresponding author’s doctoral thesis. SP is supported by the National Institute for Health Research (NIHR) University College London Hospitals Biomedical Research Centre. SP and RS are recipients of a grant from the Royal College of Psychiatrists: Psychological Processes and Clinical Effectiveness (2017–2025). None of these funders had a part in the study or the decision to submit the paper for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.