
Abstract
Background:
Mental health disparities persistently cause inequity and social exclusion. Extensive research underpins the need to embrace the social determinants of health and facilitate network learning at various ecosystem levels. Despite valuable quality frameworks and ratified conventions, local practices which counter health inequity are scarce.
Methods:
The Dutch HOP-TR study collected health and needs of Homeless Service Users (HSU) in a rights-based, transdiagnostic, recovery framework. We assessed the survival modes and conducted a socio-ecological analysis, exploring what happened in care pathways at three ecosystem levels: individual HSU, caregiver networks, society. While documenting vital conditions for growth and citizenship, we explore major opportunities to develop ‘fair space for life’.
Results:
Under low distress levels, prosocial behavior is prominent (32.9%). High distress levels are found with an avoidant (42.0%) or aggressive mode (24.9%). Rising distress levels give more frictions in relations, psychiatric admissions, and police-justice contacts. The distress-induced descent in the social hierarchy causes social withdrawal, alienation, and marginalization. At society level, fair conditions for growth and citizenship are challenged by the cumulative impact of distress over the HSU’ lives.
Discussion:
This care monitor uncovers the impact of distress on caregiver interactions. The care pathways reveal that the survival strategies reflect a systematic, pervasive neglect. Unfair representations hold HSU personally responsible of their situation, disregarding the cumulative impact of environmental conditions over their lives. The diverse sources of unfairness are intrinsic to the health care system and culture. Therefore, the survival modes ask for profound culture transformations in a whole-system-whole-society approach.
Conclusion:
Given the need for action on health equity and the social determinants of health, this paper provides an example of a dynamic care monitor. The actionable data elicit dialogs and stimulate to enrich opportunities for inclusion and growth in communities and societies.
Introduction
Naturally, human beings aspire freedom of choice and self-determination. Their interactions reflect social rules of dignity and growth. Ideally, intuitive processes guide individuals and communities to develop adequate responses to threats, preserving autonomy while supporting disadvantaged fellows. Yet, health inequity remains a pervasive problem, despite homeostatic processes, ratified human rights conventions, and extensive research evidence.
Health inequity particularly affects populations at the edge of societies (Marmot, 2007). Social norms induce bias and sustain social hierarchies. The Commission on the Social Determinants of Health (SDH) acknowledged that ‘health inequities result from unequal distribution of power, prestige, and resources among groups’. She addressed the unfairness of systematic, reasonably avoidable, health differences within and between countries. To reduce inequity, economic growth, and single-sector improvements do not suffice. Increasing empowerment is necessary to enable all citizens to lead flourishing lives. It requires material support for a decent life, self-determination and control, and political will. Therefore, the World Health Organization (WHO) launched an ecological SDH-centered framework, to foster fair space for life in a whole-system-whole-society approach (Marmot et al., 2008, 2012). Scholars in the public mental health field accentuated the significance of SDH for normal growth and mental health (Alegría et al., 2018; Kirkbride et al., 2024; Rosen et al., 2020; Stansfield & Bell, 2019).
In modern societies, mental health disparities persistently cause inequity and social exclusion (Benjaminsen, 2016; Bramley & Fitzpatrick, 2018; Santos et al., 2018). The dismantling of psychiatric hospitals in the end-twentieth century increased societal challenges on the neediest. Rooted in the consumer/survivor movement, the recovery movement continually addresses power imbalances in mental care (Voronka et al., 2014). By giving voice to psychiatrized people, it eases developing mutual relations and meaningful roles. Five decades of advocacy strengthened the significance of rights-based, integrating care strategies for shaping fundamental conditions for growth (Harding et al., 1987). Assertive Community Treatment (ACT) became the preferred model, aimed at care needs of people with Severe Mental Illness (SMI) in communities (Aubry et al., 2020; Mueser et al., 1998). Though ‘Housing First’ with case management proved effective for ending homelessness (Roy et al., 2024), its implementation rate remains low (Benjaminsen, 2018). Currently, resource groups are implemented to support symptomatic, social, and relational needs. Triadic care, provided by personal resource support, adds meaningful (in)formal caregiver relations (Malm et al., 2015). Mutual collaboration can safeguard fairness in interactions, naturally breaking the dominant cycle to medicalize social and existential needs.
Besides, research disclosed the extent and transgenerational effects of health inequity in socially deprived populations (Aldridge et al., 2018; Nilsson et al., 2017; Termorshuizen et al., 2014). Therefore, ‘inclusion health’ is proposed to better serve socially excluded populations with interdependent needs (Luchenski et al., 2017). ‘Commoning’ uncovers local attempts to overcome governance obstacles and minimize the social divide (Zielke et al., 2021). The US Institute for Healthcare Improvement has shown how organizations can make health equity a strategic priority and tailor resources and organizational processes to that aim (Wyatt et al., 2016). Still, practices motivated by equity, remain scarce. The impetus for care specialization increases the underservicedness of people with complex, intensive needs (Rosen et al., 2013). Kilbourne et al. (2018) demonstrated that improving mental health-care quality is a team sport, which requires a ‘learning health care system framework’. Conjoint learning in multi-stakeholder networks facilitates overcoming barriers and leverage opportunities at various ecosystem levels. Then learning collaboratives of service users, caregivers, services, and payers provide meaningful content to ‘value-based care financing models’.
In practice, mental health needs are everywhere. The COVID-19 pandemic increased awareness of the preexistent health inequity of socially excluded citizens. Patel et al. (2023) outlined how states can transform health-care systems to counter the emerging mental health crisis. Robust monitoring of population health needs ensures accountability and promotes acting on policy impacts. Rios et al. (2021) demonstrated the value of InterRAI questionnaires for assessing marginalization in populations. Building on SDH and socio-ecological recovery knowledge, scholars propose to replace categorical illness-oriented models with transdiagnostic, contextual strategies (Van Os et al., 2019, Van Os, Pries, et al., 2023; Shah et al., 2020). The WHO embraces this vision, ascertaining that people, irrespective of disabilities, have the right to participate as normal citizens in society (World Health Organization, 2023).
Situated in the Netherlands, this paper describes what happens to socially excluded populations deprived of a home. The extensive health care system consists of highly specialized services (Van Os, Scheepers, et al., 2023). The specialist mental health treatment, forensic, and long-term mental care are distinct, siloed service systems. Ambulant outreach provided by Flexible ACT teams constitutes the standard for SMI people in need of integrated care. Municipalities are responsible of work support, welfare benefits, and homeless services. Besides, they should organize connections between various health-care domains. From 2006 to 2014, a national homelessness strategy intended to end nuisance due to street homelessness. From 2015 on, the municipal responsibilities for disadvantaged and disabled citizens increased. Local authorities were considered better placed to coordinate local care. Austerity measures, aiming to safeguard the fiscal sustainability of the health care system, colluded with the decentralization. A narrative review questioned the universal health coverage on the right to health (Kuipers et al., 2022). Consequently, urgent information needs of local authorities resulted in the Homeless People Treatment and Recovery (HOP-TR) study (Van Everdingen et al., 2021a, 2021b, Van Everdingen, van der Velden, & Delespaul, 2023). The health patterns of Homeless Service Users (HSU) demonstrated that 3 out of 4 (72.5%) have dynamic, intensive care needs related to SMI. Vital care needs, integrating health and welfare domains, were hardly matched.
Serving socially excluded populations is no routine care. Worldwide, caregiver networks experience similar struggles (Kerman & Sylvestre, 2020). Ethnographic researchers in Alabama interviewed HSU about formal caregiver relations (Moore-Nadler et al., 2020). Compromised systems, professionalism, dehumanization, and (dis)engagement caused instability, funneling HSU into downward trajectories. Vignette studies show how health disparities arise from power imbalances and unmatched needs. In social hierarchies, curtailing freedom causes distress and harms people’s health and self-esteem. The urge to use power instead of engaging in collaborative relations demotivates and traumatizes professionals, as well (Sweeney et al., 2018).
Instead, promoting growth requires fair space in natural, safe environments. Belonging and social connectedness are crucial. The multi-motive model aims to better understand responses to discrimination, stigmatization, ostracism, and other forms of interpersonal rejections (Smart Richman & Leary, 2009). It distinguishes prosocial, avoidant, and aggressive modes, which match the fight-flight responses to threats. Facing threats, the desire for social acceptance can trigger prosocial behavior. Then optimism about opportunities promotes to engage in various relations or to create alternative sources of social support, using cognitive strategies. Conversely, the fear of future pain incites avoidant reactions when the relation’s value and repair chances are perceived as low. Finally, anger and indignation provoke aggressive behavior when the perceived unfairness is strong and the repair chances low. Under these circumstances radical survival strategies emerge. This often combines with lowered empathy and difficulties in self-regulation.
The Dutch HOP-TR study demonstrated that health inequity affects HSU (Van Everdingen, van der Velden, & Delespaul, 2023). The unavailability of paid work support and the failure to match integrating care needs over concurrent domains are potential causes of health inequity. Many HSU expressed disappointment or indignation about how care providers, municipalities, or society treated them (Van Everdingen et al., 2021a). Therefore, we reviewed essential conditions for growth and citizenship. Three questions explore opportunities to develop fair space for life: (1) How do HSU respond to daily hassles and other stressors? (2) What interaction patterns emerge between HSU and caregiver networks? (3) What can we learn from emerged interaction patterns to improve care of HSU in society?
Methods
Strategic information needs on HSU incited municipalities and care providers to conduct local reviews (Van Everdingen et al., 2021a). In need of strategies to improve care quality, each review was initiated and presented in a participatory approach. A dual snowball sampling conducted between 2015 and 2017, resulted in a representative sample of facilities (N = 16) and users (N = 436). Semi-structured interviews collected health status and needs using a rights-based, recovery framework. Part of the standardized instruments was the interRAI Community Mental Health questionnaire (Hirdes et al., 2020). Life histories were transcribed. Transdiagnostic Mental Health (MH) perceptions and behaviors were assessed over the past 3 months. The Mental Health-Related Care Needs (MHRCN) were assessed, discriminating between no needs, (temporary) conditional needs, and (long-term) intensive needs related to SMI. Also, concurrent physical monitoring needs and basic (administration and paid work) needs were computed. The quantitative and narrative data was structured in the dimensions of positive health and recovery (Figure 1). Reproducing HSU’ and professional perspectives, data allows to explore what happened over time between HSU and communities, care services, and society. We assessed the individual’s dominant survival mode and conducted a socio-ecological analysis of care pathways. Supplemental Appendix A contains the sources and operationalization of the variables.
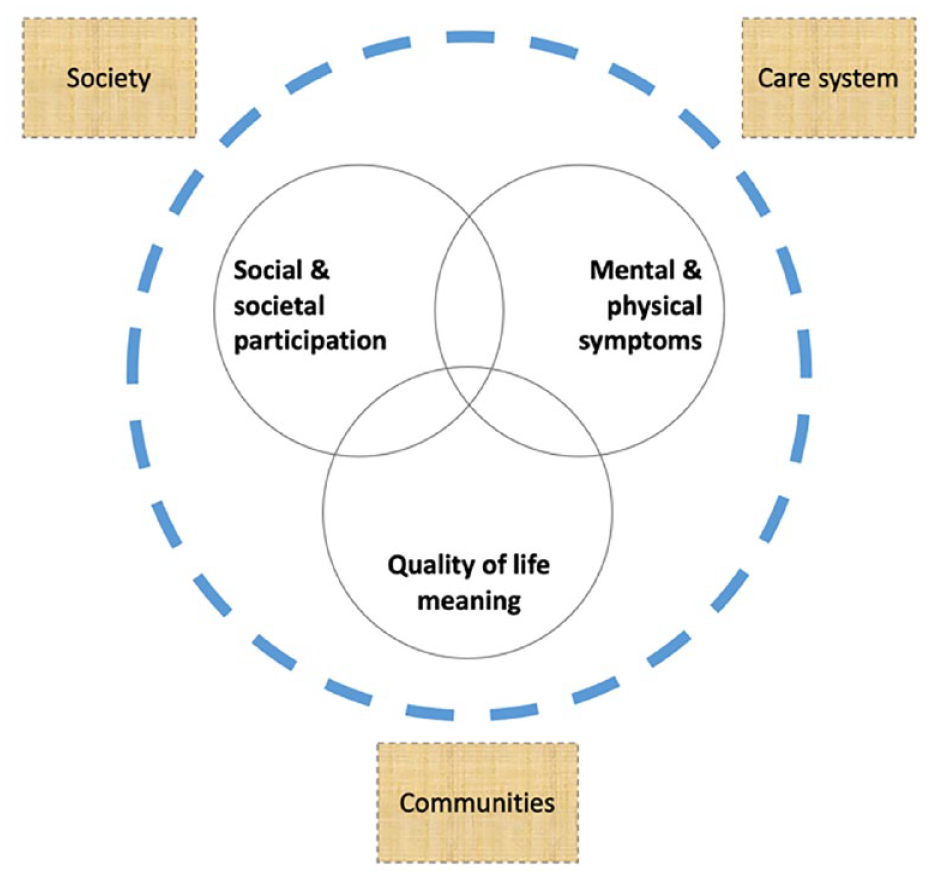
Social, personal, and symptomatic dimensions.
Survival mode assessments
We assessed the dominant responses to daily hassles and unusual stressors in the preceding months. From a socio-ecological viewpoint, marginalization and recovery are a continuum. Homelessness, SMI, and concurrent problems impact upon this continuum. This allows to explore pathways. By reviewing quantitative and narrative data, HSU were coded in three survival modes: prosocial (PRM), avoidant (AVM), and aggressive (AGM). Based on the life histories, background, and health patterns, we considered motives and actions in various roles. A decision tree (Figure 2) guided the coding of behavior and perception of context. We focused on acts of physical violence, motives to engage in relations, and attention to needs for growth. If violent acts were unreported, pervasive patterns with recurrent violence or intentional misuse of relations could also result in a classification as AGM. Conversely, HSU with incidental violence classified under PRM or AVM. In absence of violence and misuse of relations, remaining resilient while striving for growth led to PRM. The narrative data was leading. Assessments based on single incidents were avoided; the mode should be sustainably present. CvE made primary assessments; PBP executed the quality control of 10% of cases (4.8% no match). In less than 1% of the cases, data was missing.
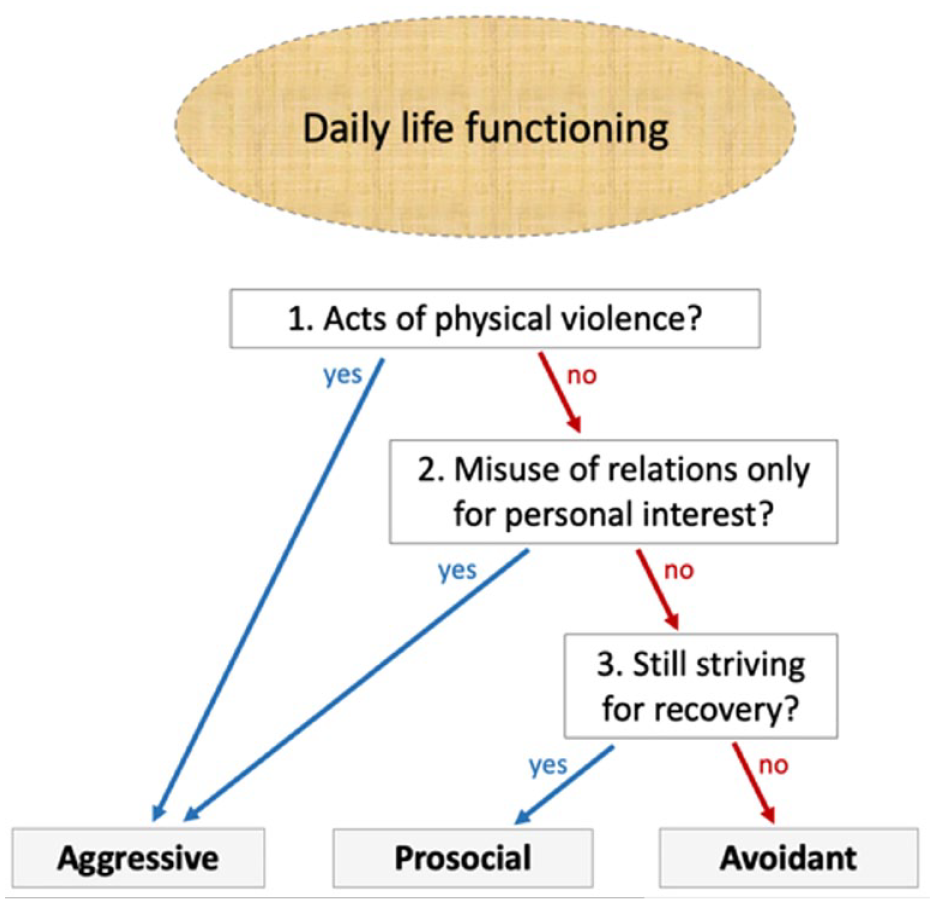
Guided survival mode assessments.
A socio-ecological analysis of pathways
We divided the sample by survival mode. In four steps, we explored what happened at three levels of the health-care ecosystem: individual HSU, caregiver networks, society. Step 1 compared the health and welfare needs, including a rights-based assessment of the ‘future living status’ after leaving the services. Step 2 explored the patterns of stress-related perceptions and behavior. We used the self-harm indicators for computing the lifetime prevalences of internalized distress. We computed the externalizing manifestations based on violence expressions in the last year. We analyzed the impact of increasing distress levels on (in)formal relations. Next, we computed a coping indicator, describing the distress expressions. Step 3 examined the distress effects upon various relations. Step 4 examined the conditions for growth and citizenship at society level. ‘Serviced needs’ relate the delivered services to present needs. Assessment norms were based on professional standards, such as the Consensus EPA/SMI (Van Everdingen et al., 2021a). We selected a vignette of each survival mode. Statistical analyses were done in Stata 16.1. Chi-square tests were run to compare the groups.
Results
Survival strategies
All HSU face interdependent problems. The most common survival mode is avoidant (AVM = 42.0%), followed by a prosocial (PRM = 32.8%), and aggressive mode (AGM = 24.8%). As shown, demographic backgrounds do not differ substantially (Table 1). The AVM-group is more often native.
Health and needs patterns (in %).
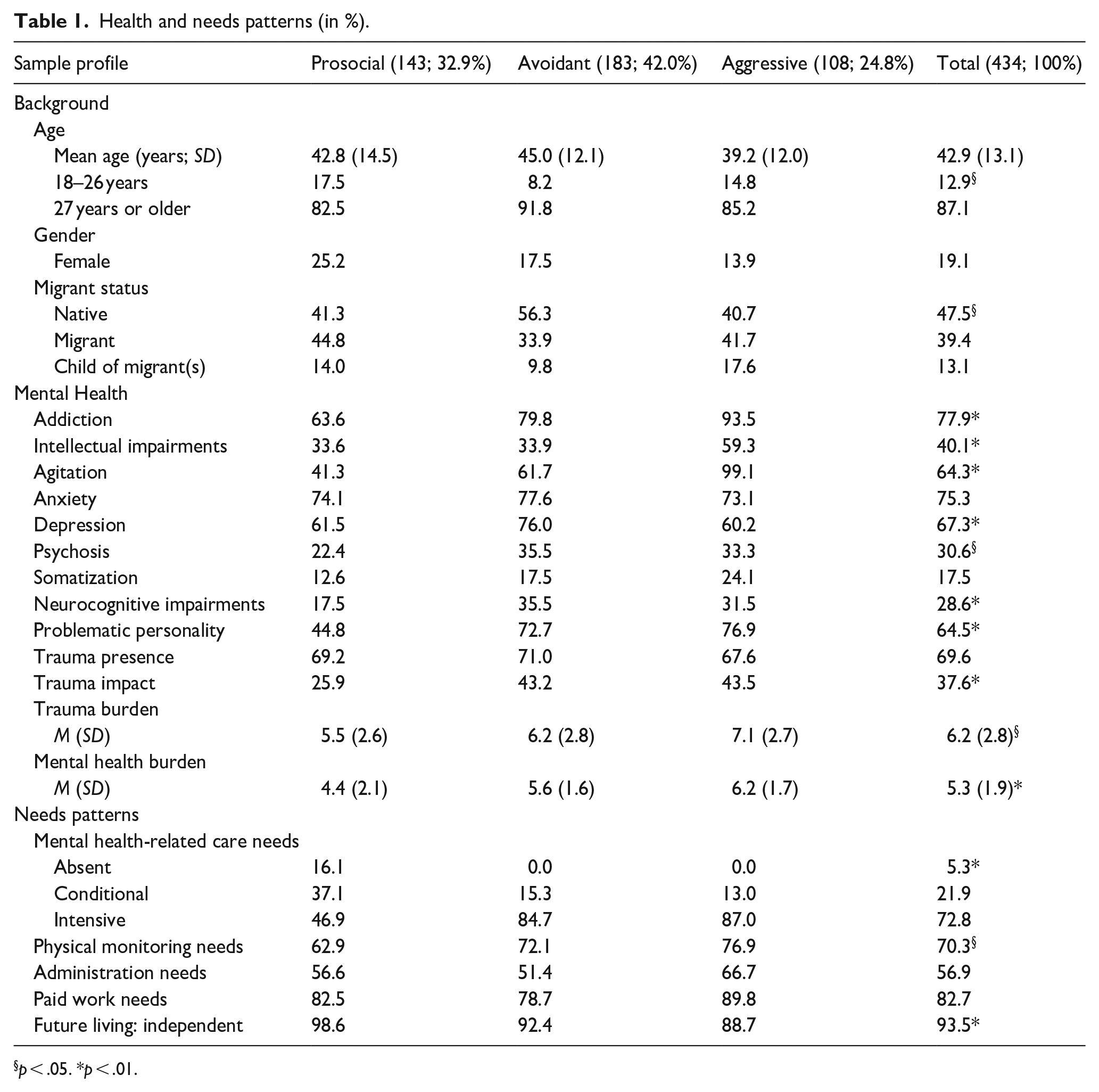
p < .05. *p < .01.
HSU with PRM experience less distress (lower MH-burden, trauma impact, and MHRCN). In the AVM-AGM-groups, the high distress is attended with intensive MHRCN in about 85%. Previous traumas often result in intense fear or safety concerns. Almost all with AGM are addicted and agitated. Intellectual impairments are also frequent. In the AVM-group, depression, anxiety, and addiction are prominent.
The coping groups have similar needs for physical monitoring, administration help, and paid work support. The ‘future living status’ shows that ambulant care suffices to cover needs when the HSU would have a home. Exceptions are cases with 24-7 needs, mostly related to severe physical comorbidity such as terminal liver failure.
Table 2 shows that stress-related perceptions and behaviors are lower in the PRM-group. In top, the self-ratings show greater disease concerns in the AVM-AGM-groups. Below, the substance use consistently increases from PRM to AVM and AGM (AGM is 1.5 times AVM). In the AGM-group, three out of four report physical violence over the last year. Externalizing behavior is prevalent, but regularly combined with internalizing distress. In the AVM-group incidentally violent acts occur but did not reflect a sustained pattern. Accordingly, the dis-ease raises a heterogenous picture of in- and/or externalizing responses.
Individual distress responses (in %).
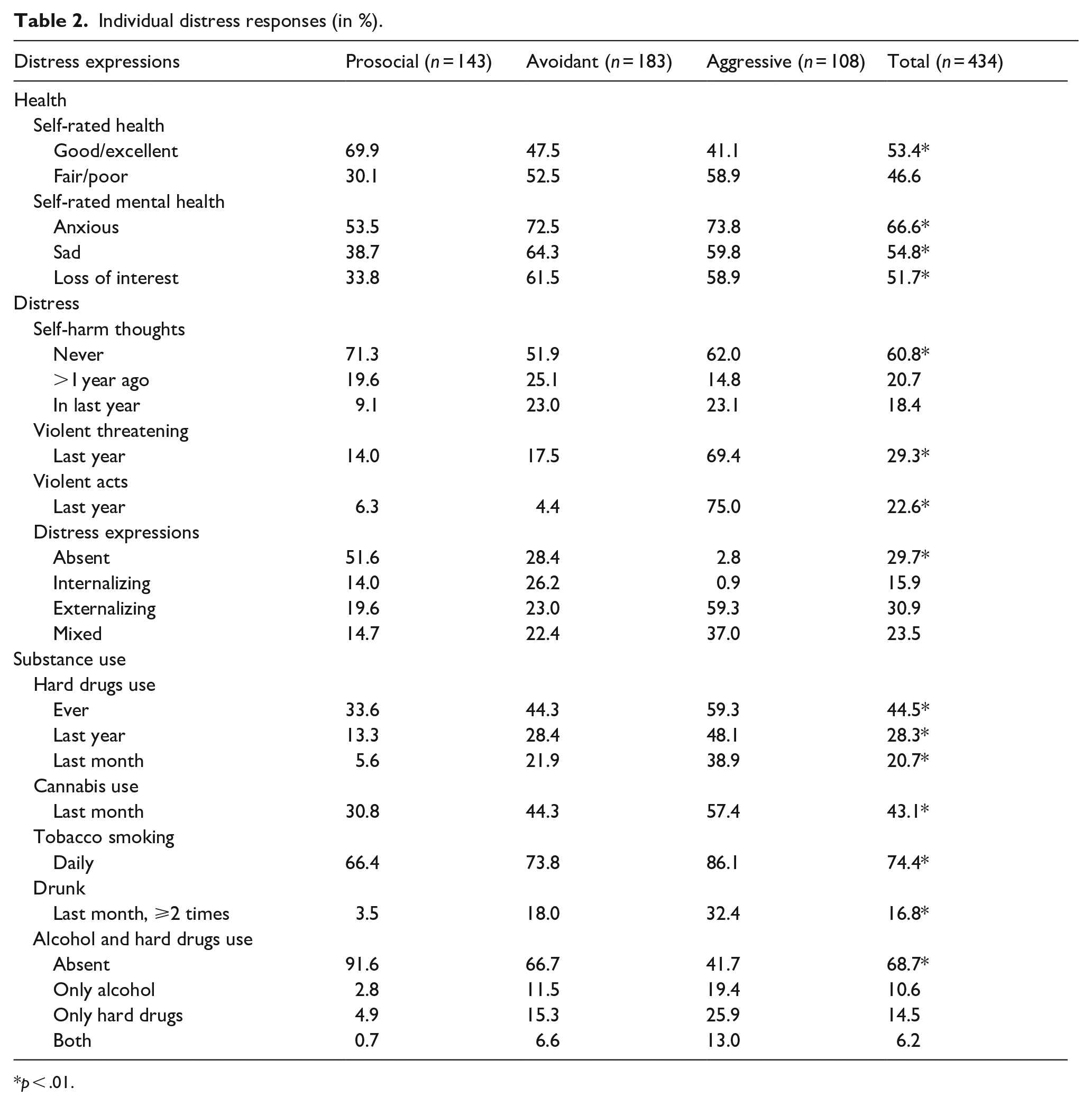
p < .01.
Dis-ease in relations
Table 3 records the distress in relations. The dis-ease is more prominent in the AVM-AGM-groups. Most PRM-copers have a positive outlook. They have concrete plans and keep perspective on future needs. Apparently, they can handle the present distress. Still, many have nobody they implicitly trust. This suggests that some adopt optimism to minimize distress. In all groups, many withdrew actively from social networks, waiting for better times. Many HSU miss family contacts. Often, they have no longstanding contacts anymore.
Distress in relations (in %).
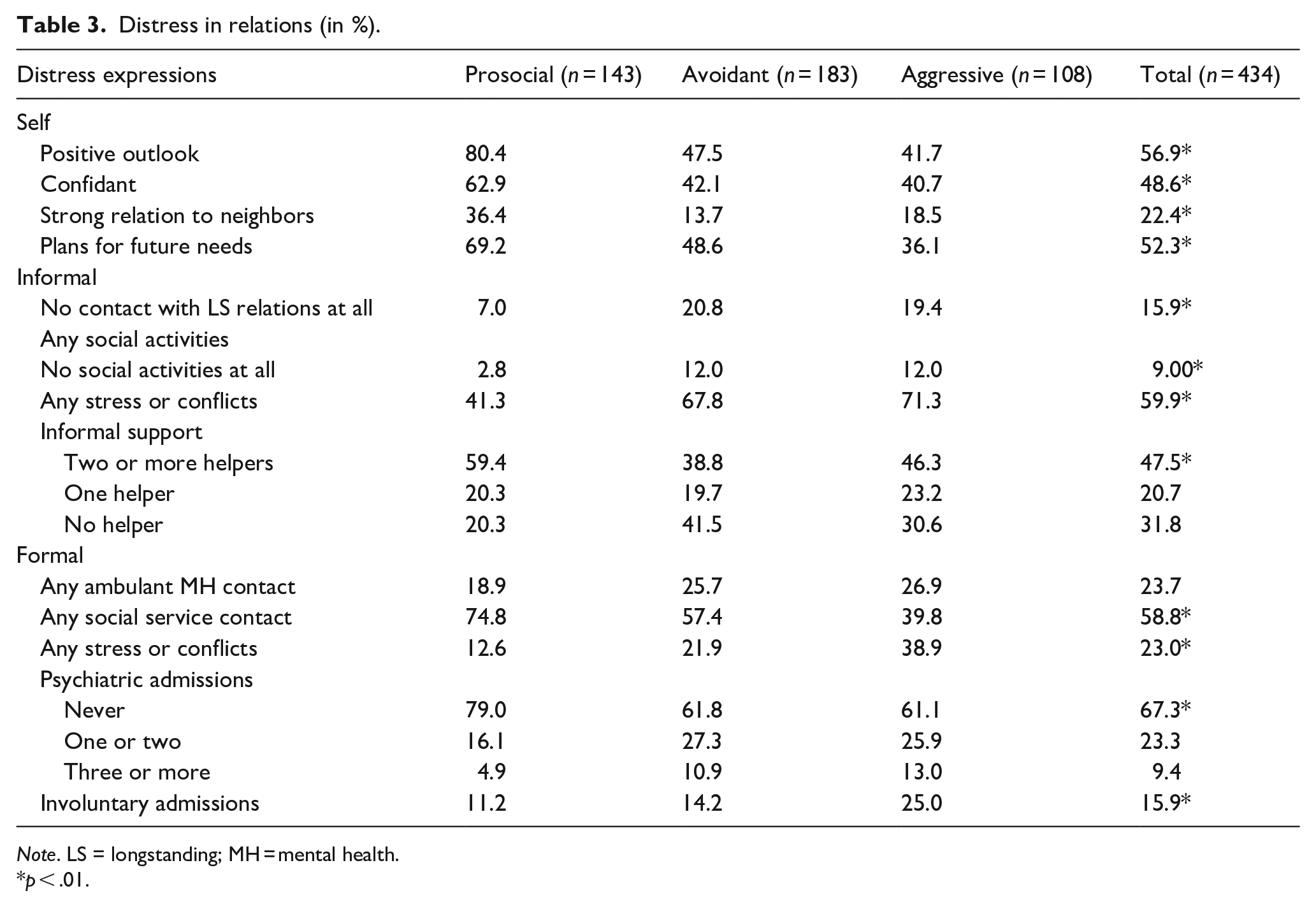
Note. LS = longstanding; MH = mental health.
p < .01.
Distress also elicits conflicts in relations. Closer inspection reveals that stress and conflicts in (in)formal caregiver relations significantly increase with rising externalizing responses (Supplemental Appendix B). Similarly, higher levels of internalizing responses increasingly burden informal caregivers. Accordingly, the resulting informal network is most favorable for the PRM-group. In the AVM-group informal helper relations are completely atrophied.
In formal caregiver relations, stress and conflicts increase to 38.9% in the AGM-group. They are often involuntarily admitted. Compared to the PRM-group, psychiatric admissions in the AVM-AGM-group are doubled.
Conditions for growth and citizenship
Reviewing vital conditions for growth and health at society level, Table 4 depicts the delivered services in relation to present needs. Overall, the servicedness of separate needs is low. Present MHRCN are only serviced in less than 1 out of 10. Paid work needs are less serviced in the AVM-group. Concurrent health and basic needs are hardly matched.
Conditions for growth and citizenship (in %).
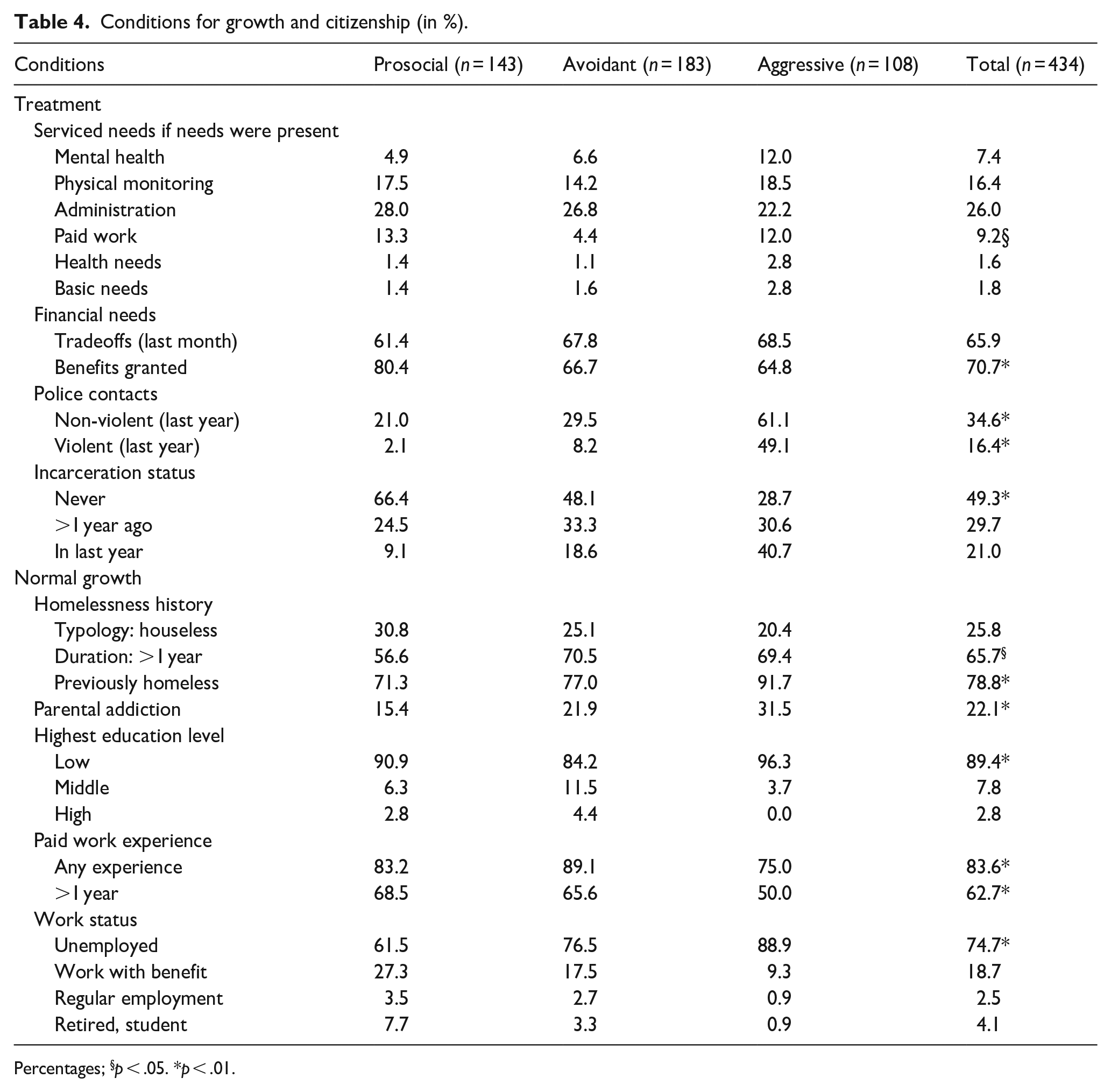
Percentages; §p < .05. *p < .01.
A majority is forced to choose between essential goods such as adequate food, shelter, clothing, or necessary health care. Because the PRM-group has better social service contacts (Table 3), more benefits were granted. Contacts with the police-justice system often occur. The frequency is particularly high in the AGM-group. Closer inspection reveals that all police-justice contacts exactly correlate to the rising externalizing distress expressions (Supplemental Appendix B).
A substantial subgroup becomes homeless after being released from incarceration in the last year.
Not having a home is pervasive. The intermittently homeless are more prevalent in the PRM-group, as lower MH-distress improves prosocial behavior. Then, resilience and relational resources offer opportunities for achieving goals and living outside the homeless services.
The regular addiction among parents is one of many indicators of early unstable conditions for normal growth. Also, life histories of migration, violence, abusive relations, or institutional youth care pointed to disturbed school careers. In all HSU the education level is low. Most experience persistent financial troubles. Most have paid work experience, but job loss rates were high. Some intermittently started in new jobs, often in sheltered positions. Combining sheltered and regular jobs, the working proportion decreases from 30.8% (PRM), to 20.2% (AVM), to 10.2% (AGM). HSU in the AGM-group are most deprived, with parental addiction, previous homelessness, lowest education level, and the poorest work experience.
Discussion
Considering the global challenges to counter health inequity, this paper offers insights into distress-induced dynamics of people deprived of a home. The Dutch HOP-TR study represents a saturated population sample of homeless service-using citizens. Using a rights-based, transdiagnostic, recovery approach, we present a socio-ecological analysis of care pathways. Documenting vital conditions for growth and citizenship, this monitor explores major opportunities to develop ‘fair space for life’. Finally, we discuss the essentials of dynamic care monitoring.
Regarding the research questions, all HSU have vital, interdependent needs. Their natural responses reflect survival strategies to multiple stressors which make up their lives. Under low distress, prosocial behavior is prominent (32.9%). High and protracted distress levels are found with an avoidant (42.0%) or aggressive mode (24.9%). Further, the monitor documents the detrimental repercussions of continuing, increasing distress on the HSU’ well-being and behavior. It exposes the dis-easing effects upon their self-confidence and relations to others. Apparently the PRM-group has a constructive attitude. Conversely, many keep a positive attitude for facing excessive distress. In all groups, the descent in the social hierarchy causes social withdrawal, alienation, and marginalization. Misunderstandings and conflicts end in rejections and stigma. Externalizing distress increasingly impacts (in)formal caregiver relations (Supplemental Appendix B). Likewise, higher degrees of internalizing distress particularly burden informal caregivers.
At the society level, fair conditions for growth and citizenship are challenged by the cumulative impact of distress over their lives. To some degree the health-care system accommodates increasing needs, as appears from the absence of substantial serviced-needs’ differences between the PRM- and AVM-AGM-groups. Needs related to symptom and risk management are more often met, but other needs receive no matching care. This demonstrates the systematic failure of the health-care system to deliver multi-domain integrated care. Consequently, fair conditions to thrive are unavailable.
Unsurprisingly, this puts HSU and their networks at a disadvantage. They complained that the health-care system undermined their autonomy and overruled their resilience. Many HSU preferred to rely on themselves. They often detached due to prior traumas, rejections, and power imbalances. Informal caregivers remained present as long as possible. Besides, formal caregivers struggled with frustrations and loyalty conflicts. Despite rejection by the HSU, they are expected to take responsibility. Accordingly, they expect that implementing evidence-based interventions will fix the needs, hereby overlooking the power imbalances and stress it puts on relations.
The results reflect how care focuses on risk management and consequently on control. Assuming that social withdrawal or radical survival strategies are deliberate choices, results in escalations. Anticipated personal and public safety risks explain why coercive treatment and police-justice contacts increase. Repression and control spiral up with distress levels. The rise of police-justice interactions holds pace to rising externalizing distress manifestations.
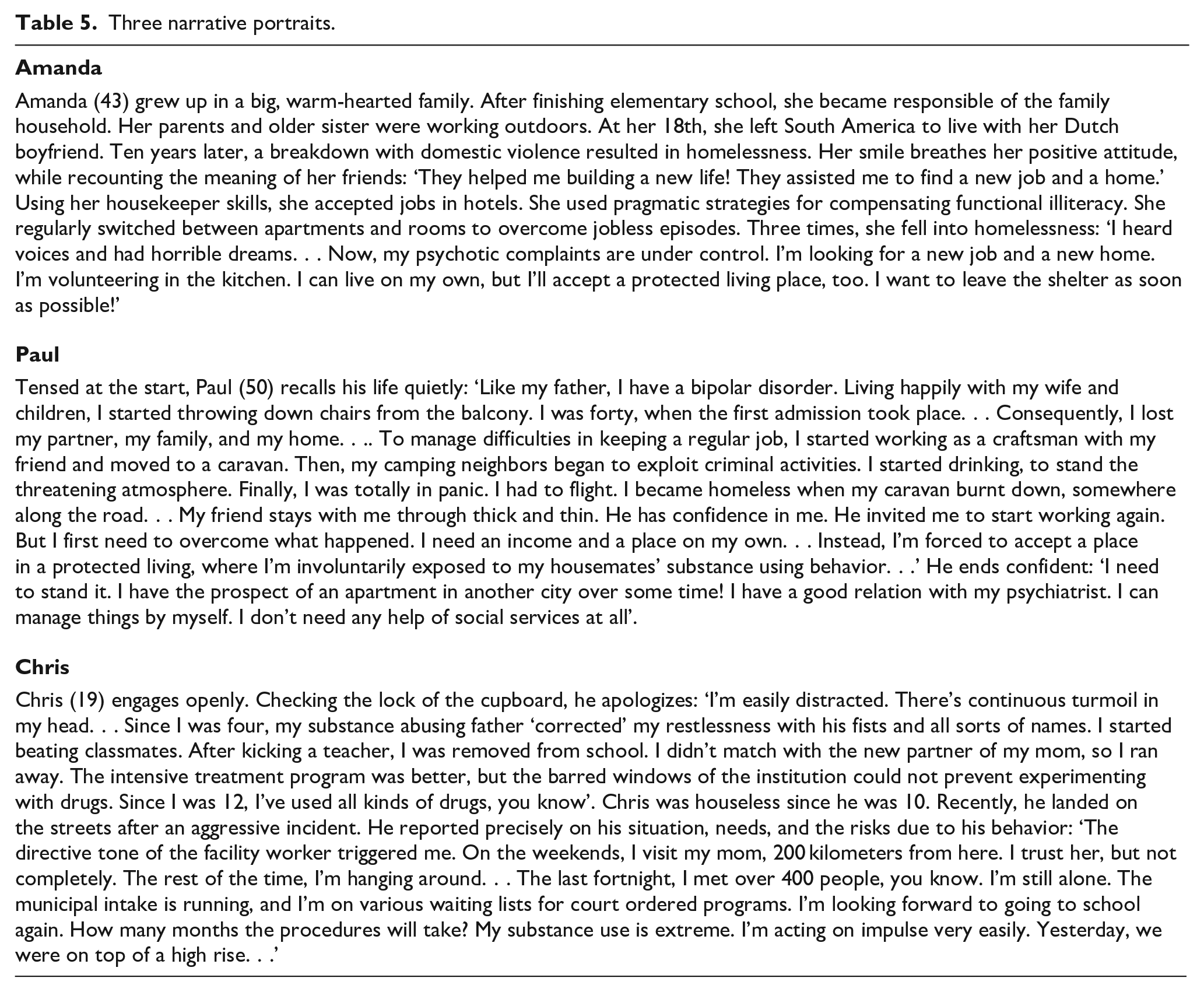
So, this monitor reveals that the survival strategies are ‘understandable’ responses to pervasive neglect. Unfair assumptions hold HSU personally responsible of their situation, disregarding the cumulative impact of environmental conditions on their lives. The detrimental roles of society and the health-care system in the care pathways are overlooked. The diverse sources of unfairness are intrinsic to the health-care system and culture. Therefore, reducing inequity will require profound culture transformations. The narrative portraits in Table 5 show how we can work on that. The voices reveal why the HSU struggle with continual distress. Preserving their autonomy and pro-actively supporting them to access resources, can free the power of creative, meaningful opportunities in the civil society. In Dutch contexts, triadic community care proved successful to acknowledge challenges and diversify care, releasing all community resources (Tjaden et al., 2021; Tjaden, Mulder, et al., 2021). Ethnographic research in a city revealed how normal behavior, lived experience, and personal qualities were vital to establish working relations with ‘deadlocked cases’ (Van Everdingen, Peerenboom, Gras, & Delespaul, 2023). Still, parallel care plans from separate sectors proved insufficient to break the fear of presumed dangerousness, restraints, and recurrent hospitalizations. Active neighbor involvement marked the onset of mutually empowering relations, resulting in a flourishing growth-enabling triadic collaborative approach.
Three narrative portraits.
This monitor underpins the need of triadic strategies. Growth and rehabilitation processes in communities go far beyond the health care system. The interdependent, intensive needs of socially excluded populations deprived of a home require robust, relation-driven, process-oriented, care pathways. Engaging in triadic networks can help find opportunities and keep focus on fair conditions for emergent growth. Besides, metaphors can give space to differences and enable transformative change in multistakeholder networks (Rosen et al., 2020; Van Everdingen, Peerenboom, Gras, & Delespaul, 2023). Open Space Technology practices offer examples, using powerful metaphors such as ‘holding space’ or ‘feeling space’ (Owen, 1995).
Meanwhile, ‘commoning’ is a verb. ‘Recovery’, ‘commonism’ and ‘inclusion health’ are movements, requiring a service, policy, and research agenda (Luchenski et al., 2017; Ragins & Sunkel, 2023; Zielke et al., 2021). When (severe) mental illness is present, the risk of social exclusion is paramount. At present, population health and needs data is mainly descriptive, focusing on individual vulnerabilities and behavior. Real-life data from effect evaluations normally report on positive results, but rarely explores why proven effective interventions do not always work (Volk et al., 2016). People falling out of care trajectories generally disappear from these monitors. Administrative data, displaying the role of structural factors to marginalization, is usually limited to specific domains.
Therefore, we adopted a transdiagnostic mental health approach and explored what happens in interactions. This provides a meaningful context to experienced distress patterns, while exposing the diverse sources of unfairness intrinsic to the health-care system and society. The findings illustrate that the proportion with intensive mental health-related care needs, previous homelessness, and serviced-needs-if-needs-were-present provide important information on the attainment of general or targeted public health strategies in (sub)populations. It confirms that the homelessness figures in a region or country ask for comprehensive consideration with police-justice contacts (Nilsson, Nordentoft, Fazel, & Laursen, 2023). Employing transdiagnostic strategies to health patterns in the general population would reinforce future quality monitoring, while exposing how far services reach people in need.
Given the need for action on health equity and the social determinants of health, this paper provides an example of a dynamic care monitor. In all, it conveys a clear call for action at various ecosystem levels. Starting from the experiences of people deprived of a home at the edge of a modern society, it reveals the costs of the distress-induced dynamics over time. It entices to expand our focus from optimizing personalized care of individuals to enriching opportunities for growth in communities. It asks to make ‘fair space for life’ central in all monitoring over care pathways. It provides hopeful results, as managing environmental causes can recover ‘lost cases’ for society. This empirical data appeals to the readiness of citizens and services for advocacy roles in the civil society, within and outside the health-care system. It also addresses governmental roles. After all, the Dutch municipalities are still responsible of the continuity and the interconnections between various care domains.
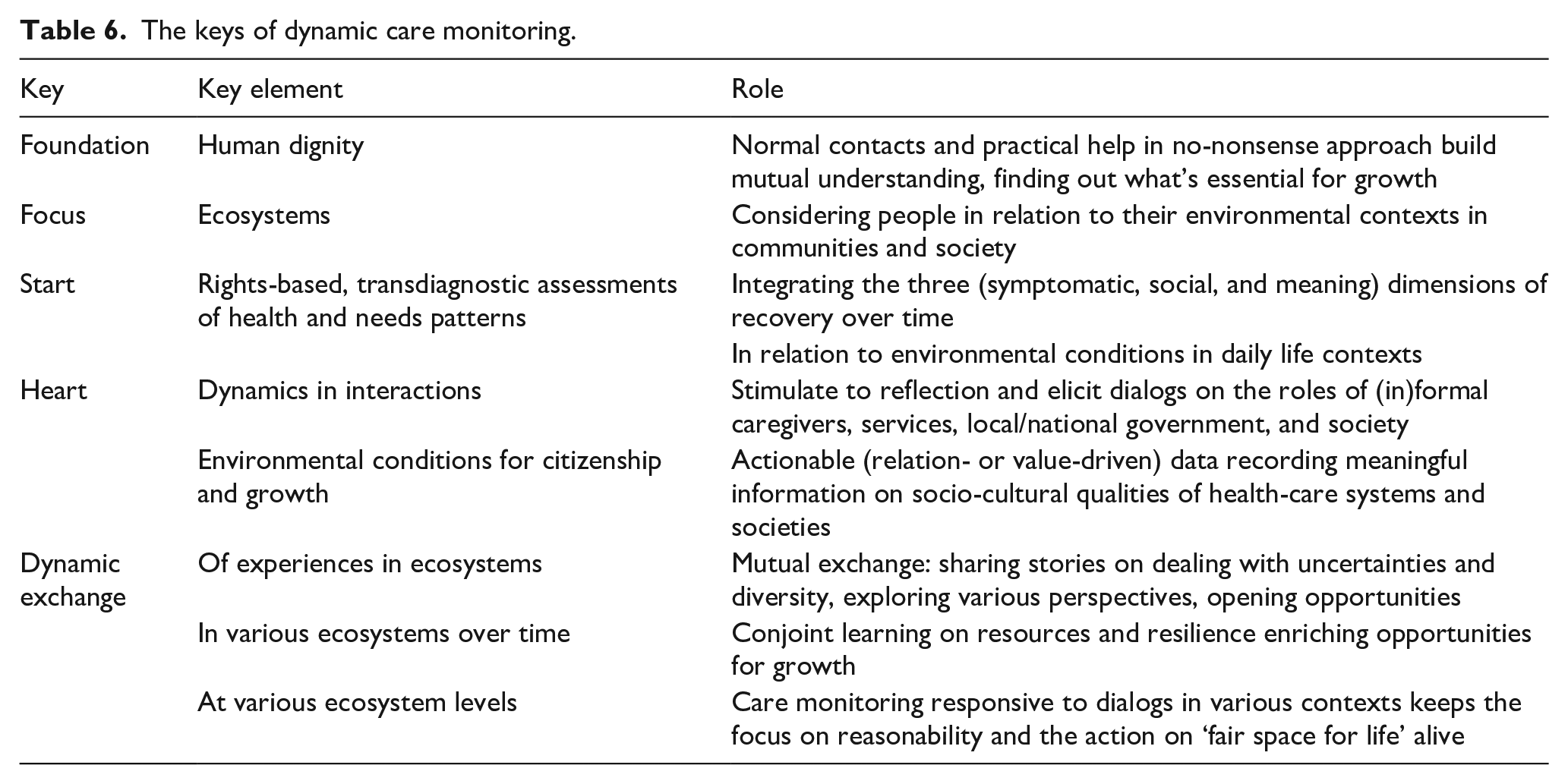
This novel monitoring approach is suitable for all populations with interdependent needs (in or at risk of social exclusion). Taking care transitions as a team sport asks for dynamic, interactive monitoring over care pathways. Table 6 shows the ‘rules of game’ of dynamic care monitoring in an ecosystems approach. Starting from the human dignity of service users, the actionable data naturally invites citizens and services to engage in value- and process-oriented collaborations. The dynamics over time stimulate reflection, while eliciting dialogs on human dignity and fair conditions for growth. Adaptive, responsive monitors can foster conjoint learning processes in networks of citizens and workers in the civil society. Then quantitative value-based care financing data are expanded with meaningful qualitative information on values, power dynamics, and social justice. Such monitors provide content to grasp the multilevel, long-lasting, incremental processes for culture change. An integrating, multidimensional approach, tackling the underlying causes, can improve the conditions for growth over lives and generations. Then shared experiences ease dealing with uncertainties and diversity in communities, while assisting to deconstruct systemic fear, prioritize safety, reduce needless suffering, and move sustainably toward fair space and optimal flourishing for all.
The keys of dynamic care monitoring.
This study has several limitations. The data was collected in single interviews by a single interviewer. Four out of five HSU had not visited a physician in the last 3 months. Medical records were not available, except in one facility. Therefore, a researcher with a MD background collected the data. The data quality is limited to face-to-face encounters during the local reviews.
People without a postal address fall of the governmental radar and are underrepresented in social surveys. Recent Dutch surveys on the health, social capital, and resources of the precariat and socially excluded city dwellers are still based on administrative data of citizens with a postal address (Van Bergen et al., 2021; Vrooman et al., 2024). The single-person assessments in this study might induce bias but offer the best health estimates of a hidden part of the Dutch inhabitants. The transdiagnostic approach yielded robust assessments of health and needs patterns.
The cross-sectional design overrepresented HSU with complex needs who remained in the services for long time. Inherent to the skewed population sample, everything relates to everything. Coping style coding was based on available subject data and can have confused independent and dependent data in the analyses. Regarding the circularity in the data, we focus on the distress patterns and depict changes over time. We documented the sources and operationalization of the data in Supplemental Appendix A.
Supplemental Material
sj-docx-1-isp-10.1177_00207640241264657 – Supplemental material for Fair space for life: A dynamic care monitor working up to growth and flourishing for all
Supplemental material, sj-docx-1-isp-10.1177_00207640241264657 for Fair space for life: A dynamic care monitor working up to growth and flourishing for all by Coline van Everdingen, Peter Bob Peerenboom, Irene van de Giessen, Koos van der Velden and Philippe Delespaul in International Journal of Social Psychiatry
Supplemental Material
sj-docx-2-isp-10.1177_00207640241264657 – Supplemental material for Fair space for life: A dynamic care monitor working up to growth and flourishing for all
Supplemental material, sj-docx-2-isp-10.1177_00207640241264657 for Fair space for life: A dynamic care monitor working up to growth and flourishing for all by Coline van Everdingen, Peter Bob Peerenboom, Irene van de Giessen, Koos van der Velden and Philippe Delespaul in International Journal of Social Psychiatry
Footnotes
Acknowledgements
First: the authors would like to thank all the homeless people who participated in the HOP-TR study by sharing their stories. In addition, we thank the management teams, the staff, and the field professionals of the commissioning organizations for their cooperation.
Author Contributions
C.v.E., P.B.P., I.v.d.G., K.v.d.V., and Ph.D. participated in the conceptual design of the study. C.v.E. drafted the manuscript, collected the data, and performed the analyses. P.B.P. executed the quality control of the survival mode assessments. All the authors critically revised the manuscript and contributed to interpretation of the data. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Municipalities and homeless service organizations commissioned and funded the data collection in the various subsamples and gave permission for scientific use. The data were collected by an independent researcher with total autonomy in the report and interpretation of the data. The Maastricht University and the Radboud University Nijmegen provide core financial support for the scientific use of the management data in the HOP-TR study.
Institutional review board statement
The research ethics committee of the Radboud University Nijmegen Medical Centre approved that our research plan for the scientific use of the management data does not fall within the remit of the Medical Research Involving Human Subjects Act (record number 2018-4463). Therefore, our research plan can be carried out in the Netherlands without approval by an accredited research ethics committee and without the explicit written informed consent of the participants.
Informed consent statement
Consent to participate was obtained. Oral consent is in reports 1 and 2; in addition to the oral consent also written consent is in reports 3 to 7.
Data availability statement
The first author is using the data of the HOP-TR study to make a PhD. When the PhD is finished, the data will become available in a public repository. Until then, we are open to data requests within the scope of collaborative projects.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.