
Abstract
Background:
Soldiers in military service are at risk of exposure to traumatic and stressful experiences, which can lead to symptoms of posttraumatic stress disorder (PTSD) and symptoms of depression. In the context of veterans’ PTSD and depression, social support has been shown to be a very significant resource. However, while general depression has been examined among veterans and although combat soldiers are often men, male depression has been rarely examined. Therefore, the present study aimed to examine the relationships between social support, PTSD symptoms, and male depression among veterans.
Methods:
Five hundred and ninety-five male combat veterans completed a demographic questionnaire and measures of social support, PTSD, and male depression, including the specific symptoms of anger, substance use, social withdrawal, and restricted emotions.
Results:
Structural-equation-model analyses showed that social support was negatively associated with both PTSD symptoms and depression symptoms. Specifically, social support showed lower trends of associations with substance use and anger; whereas there were higher associations with social withdrawal and restricted emotions. PTSD showed the strongest association with anger. Thus, we can see that social support is a key resource for coping with PTSD and different symptoms of male depression.
Conclusion:
Greater attention to social support, PTSD, and aspects of male depression could assist the development of intervention and therapeutic programs and also help to prevent the misdiagnosis of depression among military veterans.
Soldiers in military service are at risk of exposure to traumatic and stressful experiences, such as injury, coming under fire, and witnessing the suffering or death of fellow service members and civilians (Brownlow et al., 2018; Doody et al., 2022; Vinokur et al., 2011). It has long been demonstrated that such exposure can lead to emotional distress and mental-health problems (Hoge et al., 2006; Reijnen et al., 2015; Stevelink et al., 2018). Within this context, posttraumatic stress disorder (PTSD) and depression symptoms have been shown to be the most significant consequences of such exposure (Nichter et al., 2019; Vaughan et al., 2014; Williamson et al., 2018).
PTSD is characterized by a wide array of symptoms following a traumatic event. These symptoms include intrusive trauma-related memories, avoidance of trauma-related cues, negative cognitions and mood, and alterations in arousal (American Psychiatric Association [APA], 2022). A handful of studies have demonstrated the prevalence and severe impact of PTSD symptoms on veterans following their military service (Asnaani et al., 2014; Fulton et al., 2015; Pacella et al., 2013; Sherman et al., 2016). Depression has been shown to be another major emotional state that affects veterans following their military service (Fortney et al., 2016; Trivedi et al., 2015). According to the DSM-5-TR (APA, 2022), depression can include sadness, feelings of emptiness, fatigue, or irritable mood, along with sleeping problems and suicidal ideation, which together with specific cognitive and somatic symptoms lead to significantly impaired functioning (Maina et al., 2016). Taken together, emerging evidence suggests that the co-occurrence of PTSD symptoms and depression symptoms may impose an even greater burden on mental health and well-being than either condition alone (Flory & Yehuda, 2022).
Within the context of depression, gender differences have been demonstrated over the years, such as more common diagnoses and a higher risk of suicide attempts among women and higher rates of suicide completion among men (APA, 2013; Sedlinska et al., 2021). These differences suggest that depression symptoms might manifest differently among men and women, as some of the typical symptoms (such as sadness and the seeking of help) challenge culturally accepted masculine codes of behavior and so are less commonly exhibited by men (Mahalik et al., 2021; Moynihan, 1998). On the other hand, men might exhibit other emotional symptoms following depression that do align with masculine gender norms, such as externalizing behaviors, anxiety, anger, irritability and antisocial behavior, emotional suppression, substance misuse, and risk-seeking (Lynch & Kilmartin, 2013; Sedlinska et al., 2021; Sigurdsson et al., 2015). Notably, women have been shown to report higher levels of depression symptoms substantially more often than men, including in studies of specific populations such as medical students (Dabbagh et al., 2023; Dutta et al., 2023), individuals with diabetes (Anderson et al., 2001), gastroenterology patients (Alosaimi et al., 2014), and university students during the early part of the COVID-19 pandemic (Debowska et al., 2022). This concept might be even more significant in the case of male combat veterans, who were trained during their military service to respond aggressively under stressful conditions and who may experience emotional distress following traumatic experiences they endured during their military service. However, while general depression has been examined among veterans and although combat soldiers are often men, male depression has been rarely examined. This study aimed to fill this gap.
In the context of veterans’ PTSD and depression, social support has been found to be a very significant resource. Extensive trauma research has shown that social support is a significant coping resource (Besser et al., 2014; Brewin et al., 2000; Ozer et al., 2003; Weinberg, 2018), especially among veterans. Among that population, it has been shown to be a paramount resource for coping with PTSD and depression symptoms (Cox et al., 2017; Painter et al., 2016; Pietrzak et al., 2010). Nevertheless, research studies have often focused on general depression symptoms and paid less attention to the relationships between social support and specific manifestations of male depression.
To bridge this gap in our knowledge regarding social support, PTSD symptoms, and male depression among veterans and in accordance with the theoretical framework that views PTSD as the dominant disorder following traumatic events, which drives the development of comorbid depression (Ginzburg et al., 2010; Stander et al., 2014), the present study examined the relationship between social support, PTSD symptoms, and male depression.
Two hypotheses were examined:
Social support will be associated with lower levels of PTSD symptoms and lower levels of male depression.
PTSD symptoms will be associated with higher levels of male depression symptoms.
Within this concept we hypothesized that the subscales of the male depression symptoms will demonstrate different associations and trends with social support and PTSD symptoms. Namely, masculine depressive symptoms will show stronger associations and trends.
Method
Participants
The sample consisted of 595 male combat veterans. The participants ranged in age from 24 to 47 years, with an average age of 31.97 years (SD = 5.20) and their average number of years of education was 12.58 (SD = 2.06). Three hundred and fourteen participants (52.8%) reported a high financial status, 111 (18.7%) reported an average financial status, and 170 (28.6%) reported a low financial status. Among the participants, 198 (33.7%) were married or in a close intimate relationship and 389 (66.3%) were single or divorced. Nearly all of the participants (92.6%) were exposed to a life-threatening event during their military service and 70 (11.8%) participants were injured during their service.
Measures
Demographic and general questionnaire
This questionnaire covered demographic variables such as age, education, financial situation, and personal status, as well as general information regarding military service, such as service in a combat unit, exposure to traumatic life-threatening events during service, and injury during the course of one’s military service.
PTSD symptoms
PTSD symptoms were evaluated using the Posttraumatic Stress Disorder Checklist (PCL-5; Weathers et al., 2013). This is a 20-item questionnaire, corresponding to the diagnostic criteria for PTSD according to the DSM-5 (APA, 2013). The severity of each item is rated on a 5-point Likert scale ranging from 0 (not at all) to 4 (extremely). Higher scores reflect higher levels of PTSD symptoms. The Cronbach’s alpha internal-consistency coefficient for this scale was .96.
Male depression
Male depression was examined using the Men’s Depression Inventory (Fields, 2010). This questionnaire includes 29 items that examine male depression symptoms. The scale relates to four types of male depression symptoms: (1) anger, aggression, and hostility; (2) substance use; (3) social withdrawal; and (4) restricted emotions. Higher scores reflect higher levels of symptoms. For each item, respondents are asked to rate the extent to which they agree with the statements based on how they have felt over the past 2 weeks. The severity of each item is rated on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). In the current study, due to a technical error, two items (Items 12 and 13) were not included. Therefore, the total scale included 27 items. Despite this error, the Cronbach’s alpha internal-consistency coefficient for the total scale was .90. The Cronbach’s alpha internal-consistency coefficients for the different symptoms were as follows: .90 for anger, aggression and hostility; .85 for substance use; .65 for social withdrawal; and .85 for restricted emotions.
Social support
Social support was examined using the Multidimensional Scale of Perceived Social Support (Zimet et al., 1988). This questionnaire relates to three sources of social support (i.e. family, friends, and significant other), with items that are each rated on a 7-point Likert scale ranging from 1 (major disagreement with the item) to 7 (major agreement with the item). Higher scores reflect higher levels of perceived social support. The Cronbach’s alpha internal-consistency coefficient for this scale was .95.
Procedure
Following the approval of the University’s ethics committee (blinded for review), an initial request to take part in the study was distributed by the B’Shvil Hamachar Organization. This organization conducts nature-assisted group interventions for Israeli combat military veterans and is the largest organization in the country that conducts such interventions. Those who took part in a program run by the organization were asked to participate in the study and fill out the study questionnaires. Participation in the study was voluntary and it was clearly stated that those who chose not to participate would not be harmed in any way and that choosing not to participate would not affect anyone’s ability to take part in the organization’s activities. This was also highlighted in the informed-consent form, which also stated that participation in the study was voluntary and that participants could end their participation at any stage. Keeping participants’ safety in mind, the questionnaires were anonymous. Assistance was limited to clarifying instructions. No compensation was offered for participation in this study. Data were collected between February 2021 and December 2022.
Data analysis
In the first stage of the data analysis, we used IBM SPSS Statistics 27 to examine the means of the research variables and their standard deviations, as well as correlations between those variables. In the second stage of our analysis, we conducted structural-equation modeling using AMOS (version 27), to examine how social support, PTSD symptoms, and male depression are associated with one another. First, we ran a general model referring to the total scale of male depression as a general concept. Then, we ran an additional structural-equation model to examine the relationships between social support, PTSD symptoms, and the four different depression symptoms: anger, aggression, and hostility; substance use; social withdrawal; and restricted emotions. In both models, we controlled for age, education, financial status, and injury.
Results
In the first stage of the data analysis, we examined the means of the research variables and their standard deviations, as well as correlations between those variables (Table 1). As shown in Table 1, negative correlations were found between social support and PTSD symptoms (r = −.34; p < .01) and between social support and the total score for male depression (r = −.51; p < .01). In addition, a positive correlation was found between PTSD symptoms and the total score for male depression (r = −.66; p < .01). When we examined the relationship between social support and PTSD in light of the different symptoms of male depression, we found negative correlations between social support and all four of the examined symptoms. Negative correlations were found between social support and anger, aggression, and hostility (r = −.33; p < .01); social support and substance use (r = −.26; p < .01); social support and social withdrawal (r = −.57; p < .01); and social support and restricted emotions (r = −.38; p < .01). Reversed trends were found for the relationships between PTSD symptoms and the different symptoms of male depression. That is, positive correlations were found between PTSD and anger, aggression, and hostility (r = .66; p < .01); PTSD and substance use (r = .39; p < .01); PTSD and social withdrawal (r = .52; p < .01); and PTSD and restricted emotions (r = .44; p < .01).
Means, standard deviations, and correlations between social support; PTSD; male depression; anger, aggression, and hostility; substance use; social withdrawal; and restricted emotions.
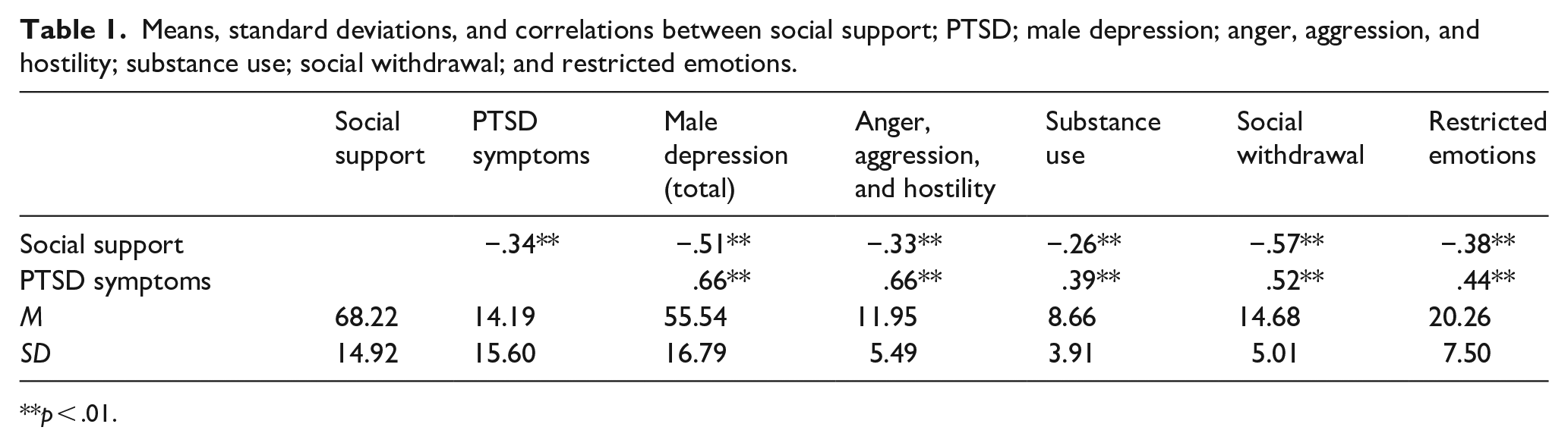
p < .01.
We then used structural-equation modeling to examine how social support, PTSD symptoms, and male depression were associated with one another. First, we ran a general model referring to the total scale of male depression as a general concept (Figure 1). Following that, as we were interested in understanding the relationships between the study variables and the different symptoms of male depression, we ran an additional structural-equation model (Figure 2) to examine the relationships between social support, PTSD symptoms, and the four different symptoms of male depression: anger, aggression, and hostility; substance use; social withdrawal; and restricted emotions. In both models age, education, financial status and injury were controlled as confounding variables but are not presented for the sake of simplicity and readability.
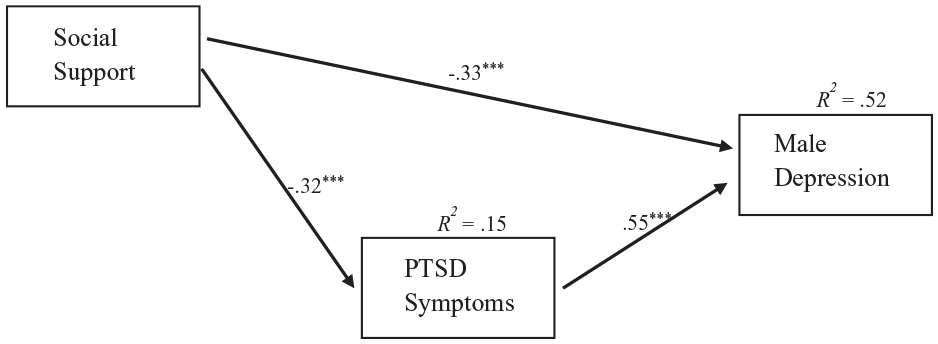
The associations between social support, PTSD symptoms, and male depression.
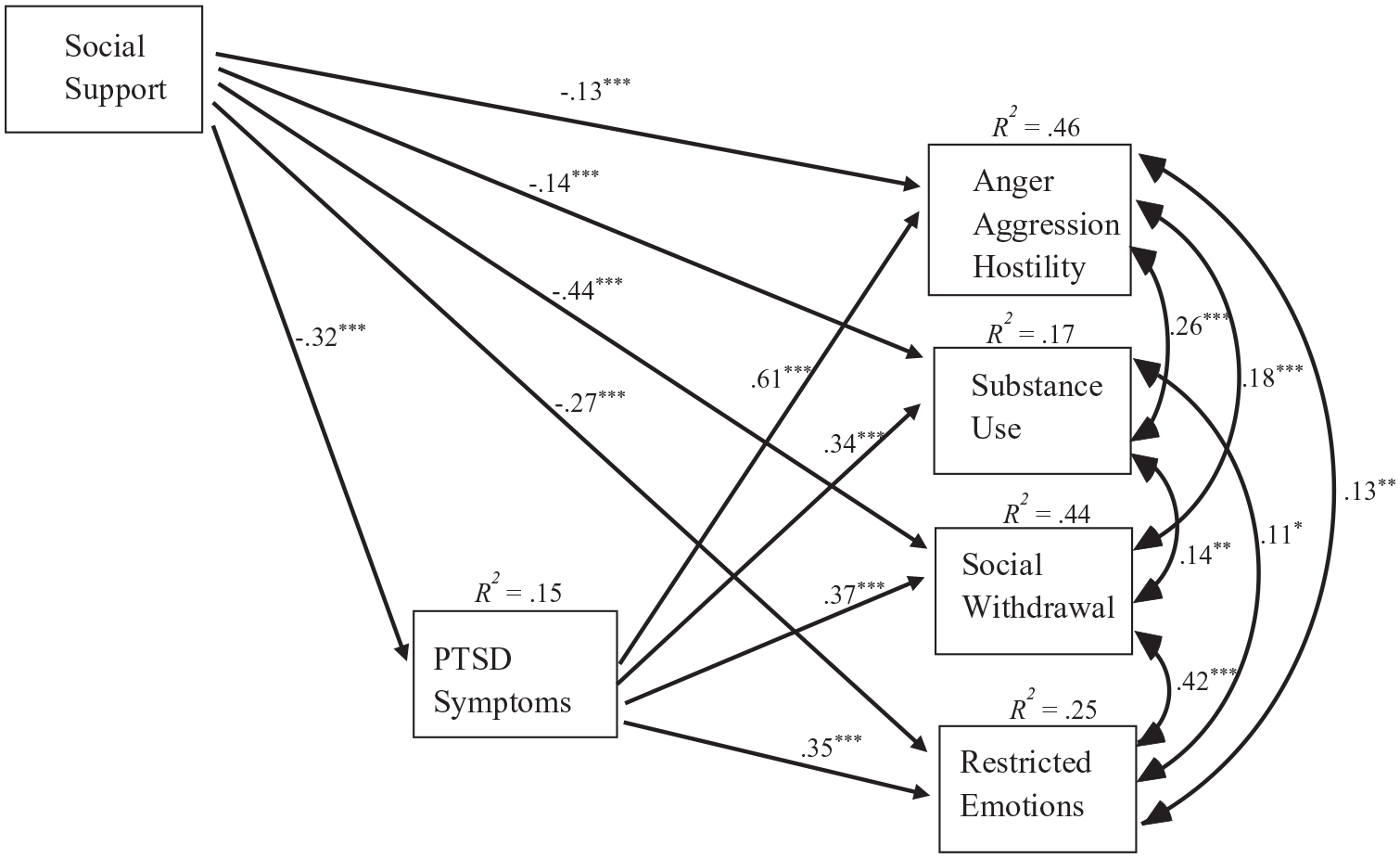
The associations between social support, PTSD symptoms, and symptoms of male depression.
The first model (Figure 1) fit the data well: χ2(13) = 11.121; p = .601; χ2/df = 0.86; NFI = 0.981; CFI = 1.000; and RMSEA = 0.996. The second model (Figure 2) also fit the data well: χ2(23) = 21.633; p = .542; χ2/df = 0.94; NFI = 0.984; CFI = 1.000; and RMSEA = 0.000.
As shown in Figure 1, social support was negatively associated with both PTSD symptoms (β = −.32, p < .001) and male depression symptoms (β = −.33, p < .001). PTSD symptoms were positively associated with male depression (β = .55, p < .001). The study model significantly explained 15% of the variance in PTSD symptoms and 52% of the variance in male depression.
Regarding the second model and the different symptoms of male depression, as shown in Figure 2, social support was negatively associated with anger, aggression, and hostility (β = −.13, p < .001); substance use (β = −.14, p < .001); social withdrawal (β = −.44, p < .001); and restricted emotions (β = −.27, p < .001). PTSD was positively associated with anger, aggression, and hostility (β = .61, p < .001); substance use (β = .34, p < .001); social withdrawal (β = .37, p < .001); and restricted emotions (β = .35, p < .001). The study model significantly explained 46% of the variance in aggression and hostility; 17% of substance use; 44% of social withdrawal; and 25% of restricted emotions.
Discussion
The main goal of this study was to examine the relationships between social support, PTSD symptoms, and male depression among combat veterans. In accordance with our research hypothesis, social support was found to be associated with lower levels of PTSD symptoms and male depression. This finding further emphasizes the importance of social support and its significant relationship with PTSD symptoms and depression following exposure to trauma (Cox et al., 2017; Ozer et al., 2003; Painter et al., 2016; Weinberg, 2018) among combat veterans. Moreover, among veterans, depression has often been examined as a general variable (Cox et al., 2017; Painter et al., 2016; Pietrzak et al., 2010), with less attention paid to unique male gender characteristics of this condition. Thus, the relationship demonstrated between social support and male depression in the present study illuminates the potential importance of social support in the context of specific levels and manifestations of male depression.
Our examination of the second study model (Figure 2) revealed an interesting relationship and trend between social support and the different symptoms of male depression. We observed lower relationships between social support and substance use and between social support and anger, aggression, and hostility, and higher relationships between social support and social withdrawal and between social support and restricted emotions. According to our findings, different symptoms of male depression might interact differently with social support. These findings suggest that male depression reflects additional manifestations of posttraumatic distress, which are aligned with masculine gender norms (Lynch & Kilmartin, 2013; Sedlinska et al., 2021; Sigurdsson et al., 2015). Accordingly, anger, substance use, antisocial, and externalizing behaviors are more congruent with masculine norms than sadness or seeking for help. Therefore, it is possible that while social support is more available in response to classical ‘vulnerability’ or ‘crying out’ for help expressions such as social withdrawal, avoidance, emotional regulation, and restricted emotions are less acceptable. These dimensions of vulnerability might be more compatible with the external social surroundings’ feelings of empathy and a desire to help trauma survivors. On the other hand, masculine or potentially ‘abusive’ symptoms, such as aggression and harmful behavior, substance use and anger, aggression, and hostility might cause individuals in the veterans’ social surroundings to feel less comfortable and more cautious in their interactions with them. This, in turn, would be reflected in a lower trend between social support and masculine depression symptoms.
This concept could also be observed in the context of our second study hypothesis, which examined the relationship between PTSD symptoms and male depression. In the realm of trauma and depression, research has demonstrated a high comorbidity between PTSD and depression, a comorbidity that may impose a great mental-health burden (Flory & Yehuda, 2022). The significant relationships between PTSD and symptoms of male depression demonstrated in the present study further emphasize the importance of understanding the comorbidity of PTSD and male depression. In the examination of the associations between PTSD and the different symptoms of depression, the strongest association was found between PTSD symptoms and anger, aggression, and hostility. This finding might suggest that, among male veterans, PTSD is especially and prominently associated with masculine depressive symptoms, such as aggressive behavior. Awareness of this concept should be integrated into the diagnostic process and therapeutic interventions, to provide more sensitive and focused interventions to address veterans’ emotional distress. Nevertheless, one should bear in mind that the present study was conducted among male veterans. It is possible that the different dimensions of depression are related and inclined to combat military service in general for both men and women regardless of gender rather than only for men. Thus, given the novelty of this study, further investigation is suggested among combat men and women veterans.
Taken together, these findings have important implications. When providing emotional assistance to combat veterans following their military service, it is important to address social support as a key resource for coping with PTSD and male depression symptoms. Therapists should harness and utilize social support with sensitivity relating to the different symptoms of male depression. The relationship between social support and depression symptoms such as social withdrawal and restricted emotions should be preserved and strengthened. While the relationship between social support and the depression symptoms of substance use and anger, aggression, and hostility dimensions, which showed lower trends should be encouraged and empowered for stronger social support. Within this context, therapists as well as policymakers should consider the strong relationship between PTSD symptoms and depression symptoms of anger, aggression, and hostility. Such attention could assist the tailoring of intervention and therapeutic programs and also help to prevent the misdiagnosis of depression among military veterans.
Several limitations of this work should be noted. The relationships between the study variables were supported by a theoretical framework that views PTSD as the dominant disorder that drives depression (Ginzburg et al., 2010; Stander et al., 2014). However, the cross-sectional nature of this study precludes any conclusions regarding causal relationships. In addition, all participants were recruited through the B’Shvil Hamachar Organization. Although this organization offers its programs to all military combat veterans, caution is required when generalizing these findings. Another limitation related to the research sample is the inclusion of only male veterans. It is possible that the different symptoms of depression examined here are associated with combat military service, in general, for people of all genders rather than only for men. Therefore, we suggest that this study be replicated among female veterans as well, to allow for the examination of similarities and differences between men and women. Nevertheless, despite these limitations, this study makes an important theoretical and practical contribution to our understanding of the relationships between social support, PTSD symptoms, and male depression among combat veterans.