
Abstract
Background:
Health disparity and under-utilization of health services is prevalent among Asian refugees and migrants in Western countries and can profoundly impact health outcomes. Cambodians who survived extreme physical and emotional trauma during the genocides enacted by the Khmer Rouge regime in the 1970’s are particularly vulnerable to poor mental health outcomes decades later. Understanding the experiences of help-seeking and service use by displaced Cambodians in Western countries may help to design more effective and culturally safe healthcare services.
Aims:
To identify characteristics or factors associated with help seeking behaviours and service utilization of displaced Cambodians with mental health issues living in Western countries.
Methods:
This review followed the Arksey & O’Malley methodological framework for scoping reviews. Articles for review were identified through searches of nine electronic databases and manual searches. Relevant articles were selected, and data was extracted and synthesized into key themes.
Results:
This review included 15 articles. Most of the studies were conducted in the USA (n = 13) with one each conducted in Canada and New Zealand. Seven studies used qualitative interviews, five used a cross-sectional survey approach, two used a mixed-methods approach and one was a narrative review and case series. Key findings highlighted the impact of Cambodian cultural beliefs about mental health (guilt, shame and help-seeking stigma) on service utilization and the disconnect between Western models of service provision and preferred Cambodian ways of receiving support.
Conclusion:
Mental health services in Western countries are likely to be under-utilized by Cambodians due to a mismatch between health beliefs and Western models of care. Further investigation of the association between health beliefs and barriers to service utilization among adult Cambodian refugees is warranted.
Introduction
Many Cambodians who survived extreme physical and emotional trauma during the genocides enacted by the Khmer Rouge regime in the 1970’s may have poor mental health outcomes decades after (Marshall, 2005; Ostrander et al., 2017). During this regime, millions of Cambodians – specifically the elite and educated citizens – were executed, resulting in waves of displaced Cambodians arriving in western countries seeking refuge; most were highly vulnerable to depression, post-traumatic stress disorders (PTSD), anxiety and other mental health issues. There is evidence that the devastating impacts of war horrors continue to afflict Cambodian survivors and their families over the generations (Figge et al., 2020).
Health disparity and under-utilization of health services is prevalent among Asian refugees and migrants in Western countries and can profoundly impact health outcomes. There are pervasive myths that refugees and migrants are highly resilient peoples (Minas et al., 2013) and inconclusive studies depicting Southeast Asians as healthier than the mainstream populace (Fozdar & Salter, 2019) leading to potentially inadequate mental health service design and delivery models. Previous research has shown that despite high rates of psychopathology (e.g. depression, PTSD, anxiety and other mental health issues), adult Southeast Asians face disparities in health care access that interfere with timely help-seeking in Western countries (Mollica et al., 1990; Porter & Markham, 2012; Priebe et al., 2016). This is particularly concerning as estimates of PTSD in displaced Cambodians can be as high as 28.4% for Khmer Rouge survivors (De Jong, 2001; Sonis et al., 2009). It is thought that Cambodians are unable or unwilling to access mental health services due to their cultural and historical experiences (Lambert et al., 2014) thus creating a vicious circle of disparity that potentially impacts their quality of life and intention to take action.
Given this combination of extreme trauma, high rates of psychopathology and under-utilization of mental health services, it is important to understand drivers of and barriers to help-seeking behaviours and mental health service utilization of displaced Cambodians and their families in Western countries. This scoping review synthesizes the evidence on the mental health service utilization and help-seeking behaviours of displaced adult Cambodians in Western countries. The review defines displaced people as those who were born outside of their county of residence and reside in those countries on permanent and temporary visas. This definition includes those who voluntarily migrated in search of economic activities, study or to reunite with family (Tribe, 2005). This review maps relevant literature in terms of volume, nature and characteristics to answer the following question: What are the characteristics or factors associated with mental health help-seeking behaviours and service utilization of adult Cambodians in Western countries?
Materials and methods
A scoping review methodology was used to map and synthesize relevant literature related to the research question (Daudt et al., 2013; Munn et al., 2022; Pham et al., 2014). Arksey and O’Malley’s (2005) scoping review framework, updated by Levac et al. (2010) guided this review. The process was reinforced by the 2020 Joanna Briggs Institute PRISMA = ScR checklist for conducting scoping studies (Tricco et al., 2018).
This scoping review was completed through the following steps (Arksey & O’Malley, 2005):
Identifying the research question
Searching for relevant studies
Selecting studies
Charting the data
Collating, Summarizing and Reporting the results
Identifying the research question
Using the Population, Content, Context (PCC) framework (Tricco et al., 2018), we formulated the scoping review question as follows: What are the characteristics or factors associated with mental health help-seeking behaviours and service utilization of Cambodians in Western countries? Rickwood et al. (2005) defined help-seeking as a persons’ ability to recognize that he or she has a problem, and they need help. It also includes the person’s ability to clearly articulate his/her awareness of the problem.
Search strategy
We started with an iterative broad search through Google Scholar to guide development of the search terms (keywords and index terms) to use in databases, as follows (with all strings combined using the Boolean operator ‘AND’):
Cambodia* OR asia*, Migrat* OR migrant* OR refuge*
Mental* OR psychiat* OR Psycho* OR depress* OR anxi* OR distress* OR traum*
servic* OR engag* OR help* OR involv* OR discrim* OR access* OR social* OR interven*
experience* OR perspective* OR view*.
Articles were identified through searches of electronic databases including Pubmed, PsycNet (PsycInfo and PsycArticles), Medline, Academic Search Complete, CINAHL Complete, Health Source: Nursing,/Academic Edition, Psychology and Behavioral Sciences Collection, Social Work Abstracts, SocINDEX; completed in November, 2022. Additionally, we hand searched key journals and the reference lists of included articles for additional sources that may have been missed from the database search. The search strategy was conceived with the help and guidance of the Swinburne University librarians.
Eligibility
Peer-reviewed studies were included if they were written in English, described one or more of the common mental disorders such as depression, anxiety, PTSD and other mental health disorders; and reported on help seeking and/or service utilization among adult (>18 years old) Cambodians in Western countries. Published theses and book chapters that reported original research were also eligible for inclusion.
Study/source of evidence selection
The screening process was done by collating and uploading the identified citations into the Covidence citation management programme. A total of 294 studies were imported for screening and 95 duplicates were removed. Two authors (VT and ND) screened the titles and abstracts of the identified citations for eligibility and a further 95 were discarded as irrelevant. Another author (LO) resolved any disagreements via discussion until consensus was reached. All authors then conducted full-text reviews of the remaining 104 studies and assessed their eligibility. In this phase, 89 studies were excluded for the following reasons: did not address the theme of mental health help-seeking behaviour (n = 49), population other than adult Cambodians with mental health issues (n = 34), conducted in non-Western country (n = 4), not available in English (n = 2).
In total, 15 studies were included for this review. The Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping review (PRISMA-ScR) flow diagram (Page et al., 2021) (Figure 1) displays the screening process.
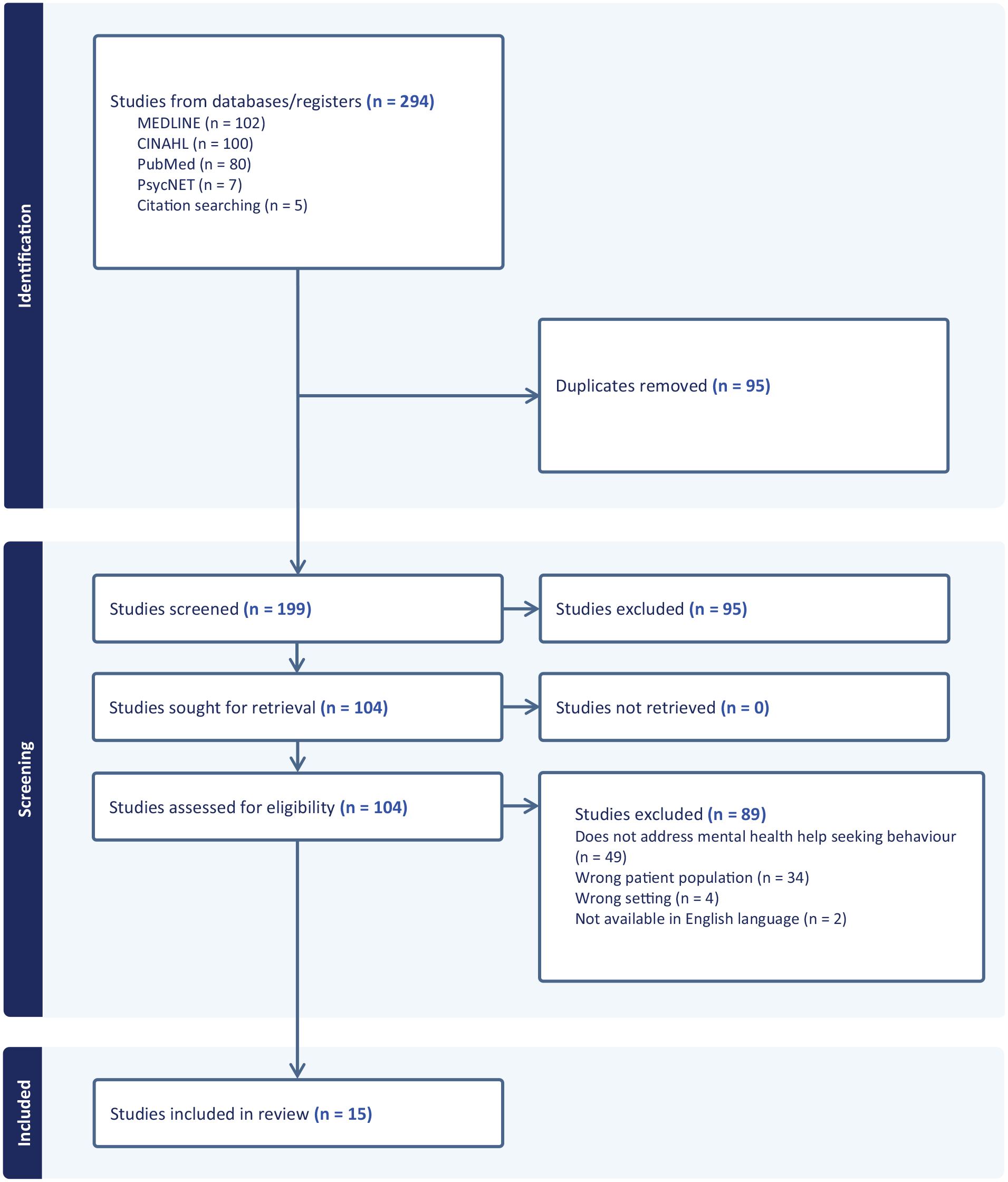
Experiences and help seeking behaviours of adult SE Asian immigrants of mental health services in Western countries.
Data charting/extraction
An excel data charting form was collectively developed by authors to extract the following information from each study: article citation, location and setting, participants, aim(s), study design, intervention or experience, data collection tools, data analysis method and key findings.
Data analysis and synthesis
The included studies were published between 1990 and 2020. Most of the studies were conducted in the USA (n = 13), with one each from Canada and New Zealand. Seven studies used qualitative interviews to explore the help-seeking behaviours or experiences with services, five used a cross-sectional survey approach, two used a mixed-methods approach and one was a narrative review and case series. The number of participants per study ranged from 6 to 490. Most studies (n = 12) included both male and female participants, two included only women and one only man. Common mental health distress and stress-related issues identified in the studies included PTSD, sometimes described using the Cambodian term koucharang (or ‘thinking too much’: a state of rumination over and preoccupation with intrusive thoughts and memories), somatization (including headaches, chest pain and excessive sleeping), social phobia, panic disorder, anger, suicidal ideation, anxiety and depression. Characteristics of included studies are summarized in Table 1.
Characteristics of Included Studies
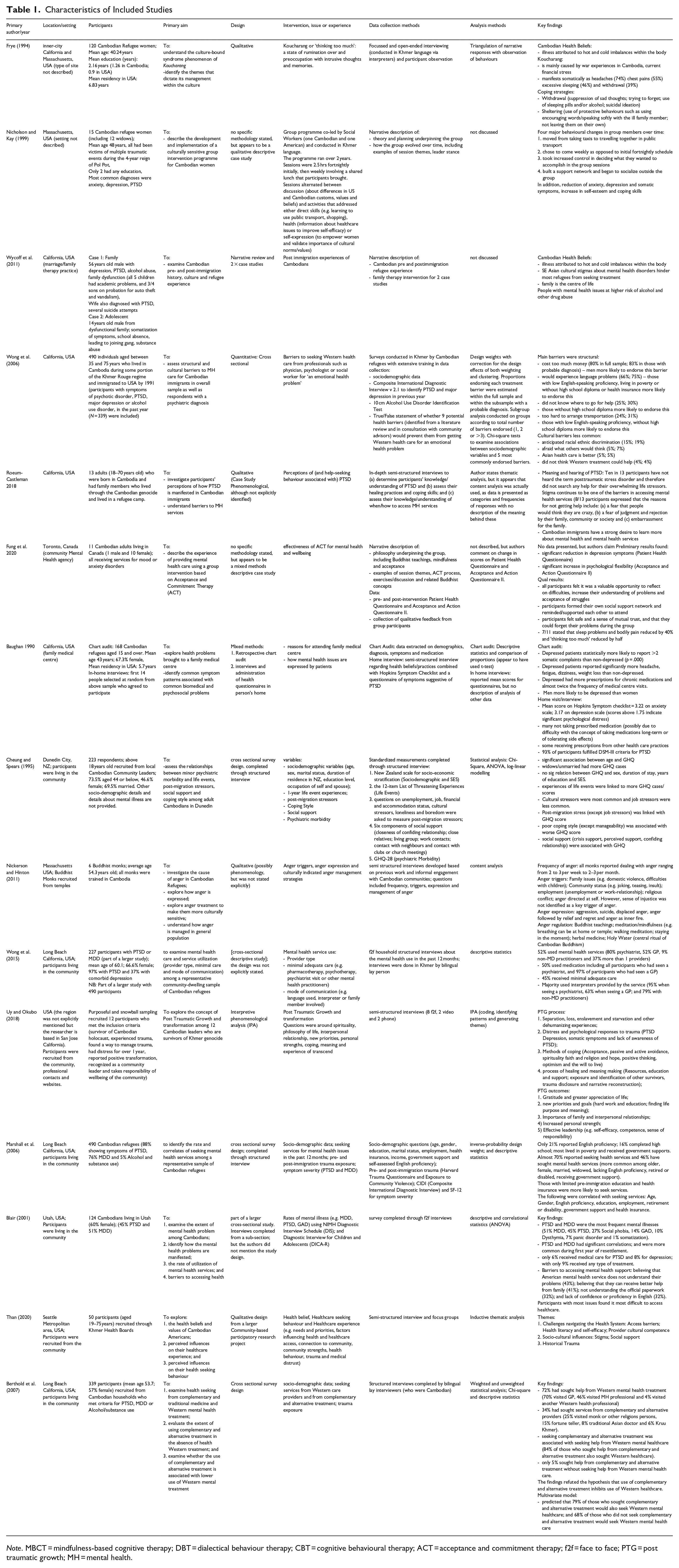
Note. MBCT = mindfulness-based cognitive therapy; DBT = dialectical behaviour therapy; CBT = cognitive behavioural therapy; ACT = acceptance and commitment therapy; f2f = face to face; PTG = post traumatic growth; MH = mental health.
Identification of common constructs
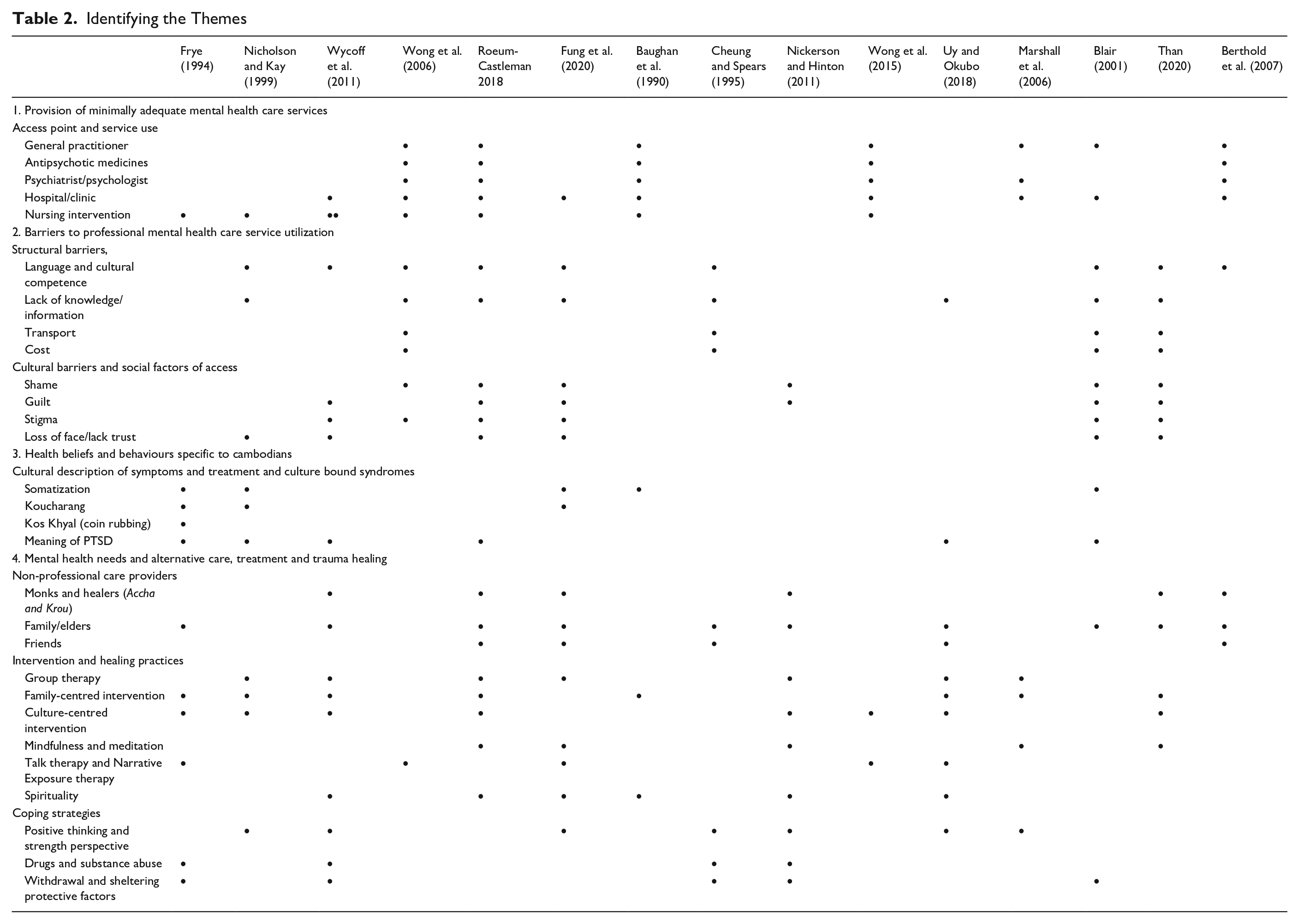
After charting the data, authors colour-coded the findings to identify similarities and differences and to identify common patterns. The tentative themes were merged and compared with the reviewed studies through an iterative process. Four major themes were identified, each with multiple sub-themes: provision of minimally adequate mental health care services; barriers to professional mental health service utilization; health beliefs and behaviours specific to Cambodians; and mental health needs, treatment and trauma healing (Table 2).
Identifying the Themes
Findings
Theme 1: Provision of mental health care services
Access point and service use
We first sought to establish rates of help-seeking and utilization for common mental health illnesses. In three cross-sectional studies, all involving community-dwelling Cambodians living in California, help-seeking was greater than expected (Berthold et al., 2007; Marshall et al., 2006; Wong et al., 2015). Wong et al. (2015) found that 52% of participants used mental health services (with 80% of these seeing a psychiatrist, 52% General Practitioner (GP), 9% non-medical practitioners and 37% more than one provider), while 50% used medication including all participants who had seen a psychiatrist and 97% of participants who had seen a GP. Marshall et al. (2006) found almost 70% of participants were in contact with a Western healthcare provider and had benefitted from nursing intervention and 46% had sought mental health services (more common among older, female, married, widowed, lacking English proficiency, retired or disabled, receiving government support). Interestingly, only 21% reported English proficiency and 16% had completed high school. Similarly, Berthold et al. (2007) found that 72% had sought help from Western mental health treatment (Majority visited a GP or MH professional; 70% and 46%; and 4% visited another Western health professional) while 34% had sought services from complementary and alternative providers (25% visited a monk or other religious person, 15% fortune teller, 8% traditional Asian doctor and 6% Kruu Khmer, who are practitioners of traditional Cambodian medicine).
In contrast, Blair’s (2001) investigation of utilization of health and mental health services in Utah found that, despite the high rates of major depressive disorder and PTSD, only 8% of respondents received mental health care for PTSD, 6% for major depressive disorder and 10% for other mental health problems. Less stigma due to acculturation may have contributed to higher rates of service seeking in California (Marshall et al., 2006). Also, participants in the Californian studies had access to interpreters provided by the service providers (95% when seeing a psychiatrist, 63% when seeing a GP; and 79% with non-medical practitioners). It was noted, therefore, that participants in these studies received adequate mental health care, described in Wong et al. (2015) as having received adequate pharmacotherapy (>2 months of antidepressants) or psychotherapy (>8 visits with a psychiatric) by obtaining treatment from the GP and psychiatrists at twice the rate of individuals with depression or PTSD in the general population in the USA.
Theme 2: Barriers to professional mental health care utilization
Structural barriers
Wong et al. (2006) used a survey to identify the potential barriers to accessing Western health care for emotional health problems. They found that structural issues, such as the high cost of health care (80%) and language barriers (60%) were the most common barriers to mental health care, followed by difficulties finding the right services (25%), transport logistics (24%) and discrimination (15%). Similarly, Than (2020) included poor health literacy, health insurance coverage and provider cultural competence as additional barriers.
Using the General Health Questionnaire (GHQ), Cheung and Spears (1995) conducted community surveys in New Zealand and found that perceived post-migration and cultural stressors (72.6%) were the most common barriers to accessing health services. Experiences of life events (such as serious illness or injury, death of parent, child or spouse, death of close friend, becoming unemployed and major financial crisis), however, were significantly related to higher GHQ scores. This potentially explains the high prevalence of help-seeking and utilization for common mental health illnesses.
Cultural barriers and social factors of access
Socio-cultural influences, such as shame, guilt, stigma and unavailability of social support, can influence the decision to seek help. Blair (2001) attributed low rates of help-seeking to cultural barriers, with 43% of the participants indicating that American care providers did not understand the needs of Cambodian people, 41% stating that they receive better services from their family and Buddhist monks, 32% not understanding the official paperwork and 32% lacking confidence or proficiency in English (32%). Participants with more significant-issues may have found it most difficult to access healthcare owing to the negative perception about and a lack of recognition of PTSD symptoms. In Roeum-Castleman (2018), over half of participants identified fear of being judged and embarrassment for their family as barriers to seeking help. Than (2020) found that prevailing silence and avoidance of the topic prevented people from openly discussing their mental health in the community.
Wong et al. (2006), however, found the opposite: cultural barriers such as lack of confidence in Western medicine and stigma (4%), anticipated ethnic discrimination (15%), fears about what others would think (5%), attitudes that Asian health care is better (5%) and thinking Western treatment would not help (4%) were the lowest rated impediments to navigating western health care systems.
Theme 3: Health beliefs and behaviours specific to Cambodians
Cultural description of symptoms of mental health distress and culture-bound syndromes
Somatization
Health beliefs and behaviours specific to Cambodian culture were reported in six of the included studies. Baughan et al. (1990) examined somatic complaints among displaced Cambodians living in California and found that 80% of the patients diagnosed with depression also had at least two nonspecific complaints of backache, chest pain, headache, abdominal discomfort, fatigue or dizziness. These patients also had more prescriptions for chronic medications and almost twice the frequency of medical centre visits.
‘Koucharang’
Frye and D’Avanzo (1994) described Koucharang, as ‘a state of rumination over and the preoccupation with intrusive thoughts and memories’ (p. 89). Koucharang is caused by historical factors such as war experiences in Cambodia and pre-migration stressors and current stressors such as financial challenges and was described by the adult Cambodian women as substantially distressing. They stated that this culture bound syndrome manifests somatically as headaches (74%) chest pains (55%) excessive sleeping 46% and withdrawal (39%).
‘Kos Khyal’ (coin rubbing)
Two studies described the Cambodian definition of illness as disequilibrium that arise from a cultural state of being ‘cold’ or ‘hot’ or internal state of imbalance described as ‘wind illness’ (Frye & D’Avanzo, 1994; Wycoff et al., 2011). Illnesses that are caused by bad wind are purged by kos khyal or coin rubbing, a traditional practice that involves rubbing the skin with tree oil and scraping it with a heated coin for the bad wind to escape, enabling the body to resume a state of balance (Wycoff et al., 2011).
Meaning of PTSD
Three studies found that some mental health terminologies such as post-traumatic stress disorder have different meanings in the Khmer language or are non-existent (Marshall, 2005; Roeum-Castleman, 2018; Uy & Okubo, 2018). In one study, 10 out of 13 participants responded with ‘I don’t know what PTSD is. . .’ and ‘I have never heard of the term’ (Roeum-Castleman, 2018, p.51). The participants in these studies had not heard the term PTSD but when the symptoms were described to them, they were more open to sharing their experience of it (Uy & Okubo, 2018). Notable descriptions given included worry, anger, thinking too much, sadness and stress all the time (Marshall, 2005; Roeum-Castleman, 2018).
Theme 4: Mental health needs and alternative care, treatment and trauma healing
Non-professional care providers
Cambodian people may view indigenous forms of treatment as complementary to Western mental health care in addressing psychiatric problems. Berthold et al. (2007) found that most participants had sought help from Western mental health services, but 34% had also accessed complementary and alternative providers (25% visited a monk or other religions person, 15% fortune teller, 8% traditional Asian doctor and 6% Kruu Khmer). Berthold et al. (2007) concluded that seeking complementary and alternative treatment was associated with seeking help from Western mental healthcare service providers as 84% of those who sought help from complementary and alternative treatment also sought Western healthcare, while only 5% sought help from complementary and alternative treatment alone, thus disproving the hypothesis that use of complementary and alternative treatment inhibits the use of Western healthcare.
Intervention and healing practice
Two studies (Fung et al., 2020; Nicholson & Kay, 1999) explored strength-based approaches to enhance feelings of safety and security in group therapy. Nicholson and Kay (1999) implemented a group programme in Khmer language for over 2 years with 2.5 hours sessions fortnightly that alternated between discussions about differences in US and Cambodian cultural values and activities that addressed direct skills to improve self-esteem, self-efficacy regarding healthcare issues and self-expression by empowering women and validating the importance of cultural norms. After the programme, participants were more comfortable with using public transport, had increased control over decisions and created a social network outside the group. Further, there was a reduction in anxiety, depression and somatic symptoms. Fung et al (2020) described a group intervention for people with mood or anxiety disorders based on Acceptance and Commitment Therapy (ACT) which is congruent with Buddhist philosophy of mindfulness.
Three papers explored group and family oriented interventional approaches (Nickerson & Hinton, 2011; Uy & Okubo, 2018; Wycoff et al., 2011). Wycoff et al (2011) explored the impact of family therapy via case studies, concluding that therapists and care providers must have an understanding of the events during the Cambodian civil war, such as forced signing of confessions, to better identify the needs and concerns of Cambodian people. They also found that displaced Cambodians appreciated the need for trained bilingual paraprofessional interpreters and therapists who have spent time interacting with the community before and during therapy. They recommended insight-oriented therapies such as cognitive behavioural and strength-based approaches that reinforce respect for Cambodian cultural values, traditions and family hierarchy and highlighted the need to address unresolved grief and loss, teach behavioural and communication skills and encourage connection and interaction at family level.
Uy and Okubo (2018) studied Posttraumatic Growth (PTG) among 12 Cambodian community leaders who survived the Khmer Rouge genocide and had demonstrated ‘positive transformation’. The PTG process incorporated methods of coping (acceptance, passive and active avoidance, spirituality faith and religion, hope, positive thinking, optimism and the will to live) and the process of healing and meaning making. Outcomes were: gratitude and greater appreciation of life; new priorities and goals (hard work and education; finding life purpose and meaning); and increased personal strength.
Nickerson and Hinton (2011) investigated the causes and appropriate intervention strategies for anger among the Cambodians by exploring the perspectives of Buddhist monks living in Massachusetts. In qualitative interviews, all monks reported dealing with anger ranging from two to three cases per week. Anger triggers were identified as: family issues (e.g. domestic violence and difficulties with children); community status (e.g. joking, teasing and insult); employment (unemployment or work-relationship); religious conflict; and anger directed at self. The authors suggested education on the Buddhist doctrines of mindfulness as the most effective strategy for anger regulation. Participants used meditation therapy, herbal medicines and holy water to ‘put out the internal fire’ (p. 406). The authors also found that meditation practices such as compassion and kindness lowered arousal and facilitated a focus on the present moment.
Coping strategies
Positive thinking and strength perspective
Fung et al (2020)’s Acceptance and Commitment Therapy (ACT) group intervention encouraged positive thinking in line with Buddhist teachings. Whilst no data was presented, the authors reported increased resilience in participants, significant reduction in depression symptoms (as measured by the Patient Health Questionnaire) and a significant increase in psychological flexibility (Acceptance and Action Questionnaire II) after receiving the six sessions. Moreover, the majority of the participants stated that sleep problems and bodily pain were reduced by 40% and ‘thinking too much’ reduced by half (Fung et al., 2020, p. 196).
Withdrawal and sheltering behaviours
Two papers (Frye & D’Avanzo, 1994; Wycoff et al., 2011) described culturally acceptable management of distress: Withdrawal and Sheltering. Wycoff et al. (2011) reported higher risk of alcohol and other drug abuse in people experiencing distress, and Frye and D’Avanzo (1994)’s qualitative study of 120 Cambodian Refugee categorized the following as withdrawal: suppression of sad thoughts (56% of the participants); trying to forget; use of sleeping pills and/or alcohol to block emotions (58%). One participant explained ‘it is very important to forget. . . I get a headache’ (p. 92) after using sleeping pills. They also identified sheltering or protective behaviours (such as encouraging words/speaking softly with the ill family member, and not leaving them alone) towards family members with koucharang. About 54% felt that koucharang could be alleviated using laughter, positive vibes and family members being available to support the affected person. Consequently, Frye and D’Avanzo (1994) proposed strategies that used culturally sensitive intervention approaches for Cambodian refugee women struggling with koucharang while focussing on the quest for equilibrium, a tenet of Cambodian worldview.
Discussion
This scoping review synthesized the literature on Cambodian adults’ mental health service utilization and help seeking behaviours in Western countries. We found that displaced Cambodians’ cultural values, beliefs and meaning making potentially affect their capacity to navigate the Western health system for diagnosis and treatment of common mental health illnesses. For example, adult Cambodians are taught to endure pain and to overcome mental health challenges and may not be open addressing their challenges (Nicholson & Kay, 1999). Most included studies reported cultural barriers to accessing health care systems in western countries, such as guilt and shame and the lack of culturally competent personnel to serve the population. This is consistent with studies of mental health utilization among African immigrants is South Australia (Fauk et al., 2022) and Asian refugees in Europe (Satinsky et al., 2019) which found stigma, guilt and shame as major access barriers.
To bridge this gap, some authors recommended family-oriented care and group therapy, which is fitting given the need to address issues of guilt and shame. Group therapy has strong empirical support in Western treatment models (Slobodin & De Jong, 2014; Zehetmair et al., 2018), and has shown substantial treatment outcomes for displaced citizens who have experienced violence and torture (Bunn et al., 2018). Another common theme was the preference amongst Cambodians to receive both mental health services and complementary and alternative medicine. Most relied more on professional services, a finding that is consistent with a study that showed Filipino Americans utilized Western care more than alternative medicine (Gong et al., 2003).
Generally, the studies contradicted perceptions that displaced Cambodians do not utilize mental health services in Western countries. This finding is surprising given that some terms such as PTSD do not exist in the Cambodian language. It is notable, however, that these findings came from studies involving community-dwelling Cambodians living in California where trained bilingual paraprofessionals from the community worked with clinics to improve service utilization, and this may not be true of other settings.
Implications for practice
Adult Cambodians associate emotional, affective, cognitive and somatic problems with traumatic events. This review identified cultural explanations of mental health distress that align with symptomatic and etiological conceptualizations of typical symptoms of trauma such as anger, fearfulness and functional impairment. This conceptualization is a necessary component of culturally safe care for Western mental health service providers working with Cambodians.
Hinton et al. (2013) proposed a somatic-focussed treatment model for traumatized refugees that may inform assessment and coordination of care. They designed the Cambodian Symptoms and Syndrome Inventory (C-SSI) to capture culturally salient somatic symptoms and cultural syndromes for mental health distress. Individual, family and group Interventions should be contextually sensitive to Cambodian populations and should address trauma experiences. Mental health service models should also integrate the spiritual aspect of meditation and incorporate spiritual leaders and family members in the treatment plan to affirm cultural values and explanations of mental illnesses.
Limitations
This scoping review did not include studies on young Cambodians, other Southeast Asian refugees in Western countries and second and third generation Cambodians living in Western countries. The pervasive impact of intergenerational trauma, mental health outcomes, service-utilization and help seeking behaviour among offspring remains an important topic for future explorations. Despite the thorough screening process in this review, this review did not include a quality appraisal which may potentially impact the accuracy of findings. The review considered various study designs, thus there were inconsistencies in the quality and methodology that may impact generalizability of the findings.
Conclusion
Survivors of trauma and momentous loss during war may struggle to navigate unfamiliar health care systems. Traumatic experiences leave indelible marks on survivors, therefore it is important to consider their sociocultural perspectives, such as the understanding and perception of mental health, so that needs are addressed congruently with recipients’ values and belief systems. Cambodian cultural beliefs about conventional medicine and spiritual life should augment and inform provision of mental health services in Western countries to increase service uptake.
Future research should explore the relationship between Cambodian cultural values and use of Western mental health services and the capacity of contemporary Western mental health care systems to meet their unaddressed needs. This should also incorporate the MH needs and help seeking behaviours of second and third generation Cambodians to fully understand their current service utilization of in Western countries.