
Abstract
Aims:
Most evidence on psychosocial factors in recent-onset psychosis comes from high-income countries in Europe, Australia, Canada and the USA, while these factors are likely to differ under varying sociocultural and economic circumstances. In this study, we aimed to investigate associations of self-stigma, religiosity and perceived social support with symptom severity and psychosocial functioning in an Iranian cohort of people with recent-onset psychosis (i.e. illness duration of <2 years).
Methods:
We used baseline data of 361 participants (N = 286 [74%] male, mean age = 34 years [Standard Deviation = 10.0]) from the Iranian Azeri Recent-onset Acute Phase Psychosis Survey (ARAS). We included assessments of self-stigma (Internalized Stigma of Mental Illness, ISMI), religiosity (based on Stark & Glock), perceived social support (Multidimensional Scale of Perceived Social Support, MSPSS), symptom severity (Positive And Negative Syndrome Scale, PANSS) and psychosocial functioning (clinician-rated Global Assessment of Functioning Scale, GAF, and self-reported World Health Organization Disability Assessment Schedule 2.0, WHODAS 2.0). Descriptive analyses were employed to characterize the study sample. Covariate-adjusted ordinal and multivariable linear regression analyses were performed to investigate cross-sectional associations of baseline ISMI, religiosity and MSPSS with concurrent PANSS, GAF and WHODAS 2.0.
Results:
Higher self-stigma was associated with poorer self-reported functioning (B = 0.375 [95% Confidence Interval (CI): 0.186, 0.564]) and more severe concurrent symptoms (B = 0.436 [95% CI: 0.275, 0.597]). Being more religious was associated with poorer clinician-rated functioning (OR = 0.967 [95% CI: 0.944, 0.991]), but with less severe symptoms (B = −0.258 [95% CI: −0.427, −0.088]). Stronger social support was associated with poorer clinician-rated (OR = 0.956 [95% CI: 0.935, 0.978]) and self-reported functioning (B = 0.337 [95% CI: 0.168, 0.507]).
Conclusion:
This study shows that self-stigma, religiosity and perceived social support were associated with symptom severity and clinician-rated as well as self-reported psychosocial functioning in an Iranian cohort of people with recent-onset psychosis. The findings extend previous evidence on these psychosocial factors to one of the largest countries in the Middle East, and suggest that it may be worthwhile to develop strategies aimed at tackling stigma around psychosis and integrate the role of religiosity and social support in mental ill-health prevention and therapy.
Introduction
Psychotic disorders are caused and influenced by the interplay of neurobiological and psychosocial factors (Owen et al., 2016; Radua et al., 2018). While the latter are likely to depend on a person’s social and cultural environment, availability of cross-cultural evidence is scarce (Burkhard et al., 2021; Maselko, 2017; Myers, 2011; Susser & Martínez-Alés, 2018). In this study, we investigated baseline levels of self-stigma, religiosity and perceived social support and their associations with concurrent symptom severity and psychosocial functioning in a cohort of people with recent-onset psychosis in the Islamic Republic of Iran.
Current evidence on environmental determinants of psychotic disorders is limited, since the vast majority of mental health research is conducted in high-income countries (HICs) in Europe, Australia, Canada and the USA (Burkhard et al., 2021; Maselko, 2017). As a consequence, previously identified environmental risk factors in psychosis may be less relevant to lower- and middle-income countries (LMICs), or may have a different impact under varying geographic, sociocultural and economic circumstances. As such, the lack of studies from diverse settings is not only problematic for local healthcare providers missing an appropriate evidence base, but also limits the general understanding of psychotic disorders.
Recently, the multi-center Azeri Recent-onset Acute Phase Psychosis Survey (ARAS) (Farhang et al., 2021) was initiated to investigate characteristics, determinants and course of recent-onset psychosis in Iran, one of the largest and most populated countries in the Middle East. The current study focuses on psychosocial factors that may differ between the HICs mentioned above and the Middle East, including levels of self-stigma (Semrau et al., 2015), religiosity and perceived social support (Nosheen, 2017).
Stigma has detrimental effects on severe mental illness (SMI), including psychotic disorders (Drapalski et al., 2013; Dubreucq et al., 2021; Kane et al., 2019; Simonsen et al., 2019; Vass et al., 2015). Stigma in mental illness entails discrimination, stereotypes and prejudices by society (i.e. public stigma) and affected individuals themselves (i.e. self-stigma) (Corrigan & Watson, 2002), with the latter usually being a result of the former. A 2021 systematic review of self-stigma in SMI found that higher self-stigma is associated with more severe positive and negative symptoms in schizophrenia, and poorer global functioning in SMI overall (Dubreucq et al., 2021). Although the authors included studies from around the world, only 4.8% of the reviewed articles came from the Middle East, mainly from Turkey (Dubreucq et al., 2021). The only Iranian study showed self-stigma to be high amongst patients with SMI (Ghanean et al., 2011), while another study from Iran showed that people with schizophrenia and their relatives are confronted with social rejection and oppression (Rezayat et al., 2019).
The role of religiosity in psychotic disorders is somewhat ambivalent and seems to depend on the individual context (Lucchetti et al., 2021; Weber & Pargament, 2014). Siddle et al. found recently hospitalized patients with schizophrenia suffering from religious delusions to experience more severe symptoms and poorer functioning levels than other patients (Siddle et al., 2002). Similar associations between religious delusions and symptom severity were observed in a 2018 Indian study (Mishra et al., 2018). Nevertheless, patients with religious delusions do not per se identify as being religious, which makes it difficult to draw conclusions about the role of religiosity.
Religiosity can also positively impact mental health, and psychotic disorders in particular. Especially during the recovery process, religion and spirituality can provide existential meaning, supporting patients in coping with their illness and contributing to feelings of hope and comfort (Huguelet & Koenig, 2009). In addition, being part of a religious community and taking part in religious ceremonies can increase resilience to stressors, for example, by forming a reliable social support net (Huguelet & Koenig, 2009).
To date, most internationally published research on this topic stems from Christian populations in Europe and the Americas (Gearing et al., 2011; Lucchetti et al., 2021; Weber & Pargament, 2014), while religiosity might well have different implications for people with psychosis living in Islamic countries. Moreover, irrespective of the religious denomination, religiosity may play a particular role in Iran, where religion is an integral part of society and where the vast majority of people identify as being religious, though to varying degrees.
Social support is another factor known to play a role in mental illness. It entails practical assistance (e.g. with household activities) or emotional comfort, and is often provided by family, friends or a significant other such as a spouse. With regard to psychosis, lack of social support is related to illness onset (Gayer-Anderson & Morgan, 2013). Moreover, having frequent contact with family and friends was strongly associated with better overall functioning amongst 980 Australian psychosis patients (Evert et al., 2003). A narrative review on schizophrenia in LMICs suggests that a supportive family environment in particular has the potential to improve prognostic outcomes (Asher et al., 2018). Family, including the extended family, is commonly believed to be more important in the Middle East as compared to western Europe, for example. Due to cultural, religious and/or economic reasons, people in the Middle East generally gather with their family more often and live longer at their family home, which are factors that can partially shapes one’s social support system. To our knowledge, the quality or extent of social support perceived by individuals with recent-onset psychosis living in Iran, and how this may relate to symptom severity and social functioning, has not been investigated thus far.
This study aimed to investigate cross-sectional associations of self-stigma, religiosity, and perceived social support with symptom severity and levels of psychosocial functioning in a cohort of people with recent-onset psychosis in Iran. We hypothesized that high levels of self-stigma are associated with more severe symptoms and poorer psychosocial functioning. Conversely, we hypothesized that higher levels of religiosity and perceived social support are associated with less severe symptoms and better functioning.
Methods
Study design and population
Cross-sectional baseline data was obtained from the Azeri Recent-onset Acute Phase Psychosis Survey (ARAS) (Farhang et al., 2021). This is an ongoing prospective cohort study established in 2018. The catchment area comprises approximately 3,900,000 inhabitants of the East Azerbaijan province in north-western Iran, around 950,000 inhabitants of the Kermanshah province and almost 14,000,000 inhabitants of the Tehran province. Islam is the dominant religion in the Iranian general population as well as in the ethnic minority groups included in this study. In East Azerbaijan, participants were recruited at Razi University Hospital (Tabriz, East Azerbaijan) and at collaborating private clinics around Tabriz. Participants in the other two provinces were recruited at Farabi University Hospital (Kermanshah, Kermanshah) and Razi University Hospital (Tehran, Tehran). Note that it is common practice for primary and secondary care providers in Iran to refer patients suspected of having a psychotic disorder to academic psychiatric centers, where admission typically ensues.
For the current study, inclusion took place between September 2018 and September 2020. Eligible diagnoses were schizophrenia, schizophreniform disorder, delusional disorder, brief psychotic disorder, schizotypal personality disorder, schizoaffective disorder and substance induced psychotic disorder as assessed by the 5th version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (American Psychiatric Association, 2015). Patients receiving any of these diagnoses, who had their first sign or symptom within the previous 2 years, were invited by their treating psychiatrist to participate in ARAS. The only exclusion criteria were uncooperative behavior and age below 18 years.
Data was anonymized and collected after obtaining written informed consent by the participant or their legal guardian. This study meets international ethical standards, including the Declaration of Helsinki, and was approved by the Iranian National Ethical Committee (IR.NIMAD.REC.1396.101). ARAS was funded by the Iranian National Institute for Medical Research Development (NIMAD) in 2017. For further details, please consult the protocol publication (Farhang et al., 2021).
Measurements and ratings
Sociodemographic data included age, sex, marital status, educational level, and socioeconomic status (SES). The latter was assessed using a questionnaire tailored to the Iranian context (Abobakri et al., 2015). History and presence of substance abuse were also documented. This included current and past use of alcohol, cannabis or hard drugs (i.e. amphetamine, tramadol, opium, heroin and/or opioids).
Diagnostic and baseline clinical interviews took place at admission to the mental healthcare facility. All assessments were conducted in Farsi by trained psychologists and psychiatrists. For diagnostic assessments, the Structured Clinical Interview for DSM-5 (SCID) (Mitra Hakim et al., 1970; Shooshtari et al., 2007) was used. Patients were re-evaluated at the research site if they had already received a diagnosis by the referring psychiatrist. In case of discrepancy between diagnoses made by the referring psychiatrist and the researcher-administered interview, a third independent psychiatrist was consulted.
Symptom severity was assessed using the Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987). While this tool was initially developed to assess patients diagnosed with schizophrenia, it has been extensively used in people with early psychoses who qualify for other diagnostic categories along the psychosis spectrum.
Psychosocial functioning was assessed within 1 month after admission using the DSM-IV Global Assessment of Functioning (GAF) scale and the WHO Disability Assessment Schedule 2.0 (WHODAS2.0; Rajeziesfahani et al., 2019; Ustun et al., 2010). GAF is a clinician-rated assessment of social, occupational and psychological functioning, with scores ranging from 0 to 100. Due to limited variance in the current sample distribution of GAF scores, we subcategorized those to facilitate analyses: GAF < 30, GAF = 30–40 and GAF > 40. WHODAS2.0 is a self-report tool inquiring about cognition, mobility, selfcare, getting along with other people, daily life activities and participation in society. Total scores range from 36 to 180, with lower scores indicating better functioning.
Self-stigma, religiosity and perceived social support were also assessed within 1 month after admission.
Self-stigma
This was measured with the Internalized Stigma of Mental Illness (ISMI) scale, a self-report questionnaire inquiring about alienation, stereotype endorsement, experience with discrimination, social withdrawal and stigma resistance (Boyd et al. 2014; Jacobsson & Ghanean, 2013; Ritsher et al., 2003). Cronbach’s alpha in this study was .91.
Religiosity
Religiosity was assessed using a 26-item questionnaire based on Stark and Glock’s dimensions of religiosity (Khodayarifard, 2010). This instrument was adapted to Islam and measures dimensions of religious beliefs (e.g. believing in the existence of God), experience (e.g. feeling close to God), practice of rituals (e.g. fasting during Ramadan) and consequences (e.g. abstaining from alcohol). Items are rated on a 4-point Likert scale, with total scores of up to 26 indicating low, 27 to 78 moderate and 79 to 104 high levels of religiosity. Cronbach’s alpha was .84. We evaluated whether people scoring high on internal/personal dimensions of religiosity (i.e. Beliefs and Experience scores above the median) simultaneously had similar levels of external/social religiosity (i.e. Practices and Consequence scores above the median).
Perceived social support
This was measured by the Multidimensional Scale of Perceived Social Support (MSPSS) (Bagherian Sararoudi et al., 2013; Zimet et al., 1988), a tool evaluating social support by a person’s family, friends or significant other. Cronbach’s alpha was .93.
Statistical analyses
First, general sociodemographic and clinical data as well as levels of self-stigma, religiosity, and perceived social support were analyzed using descriptive statistics. In a next step, regression analyses were performed to investigate associations between self-stigma, religiosity, and perceived social support (predictors) with symptom severity and level of functioning (outcomes). Self-stigma, religiosity and perceived social support were each analyzed as independent variables in an ordinal regression model with clinician-rated functioning (GAF) as the dependent variable. The same independent variables were analyzed in multivariable linear regression models with (a) self-reported functioning (WHODAS2.0) and (b) symptom severity (PANSS) as the dependent variable, respectively. In all regression models, we adjusted for age, sex, SES, and substance use (i.e. current use of cannabis or hard drugs). The latter is commonly stigmatized in itself and known to be associated with more severe symptoms of psychosis (Harrison et al., 2008). In the regression analyses with psychosocial functioning as the outcome (GAF, WHODAS2.0), we additionally controlled for symptom severity (PANSS).
Results
Description of the study sample
An overview of sociodemographic details, clinical characteristics and levels of self-stigma, religiosity and perceived social support is shown in Table 1.
Overview of sociodemographic, psychosocial, and clinical baseline characteristics (N = 361).
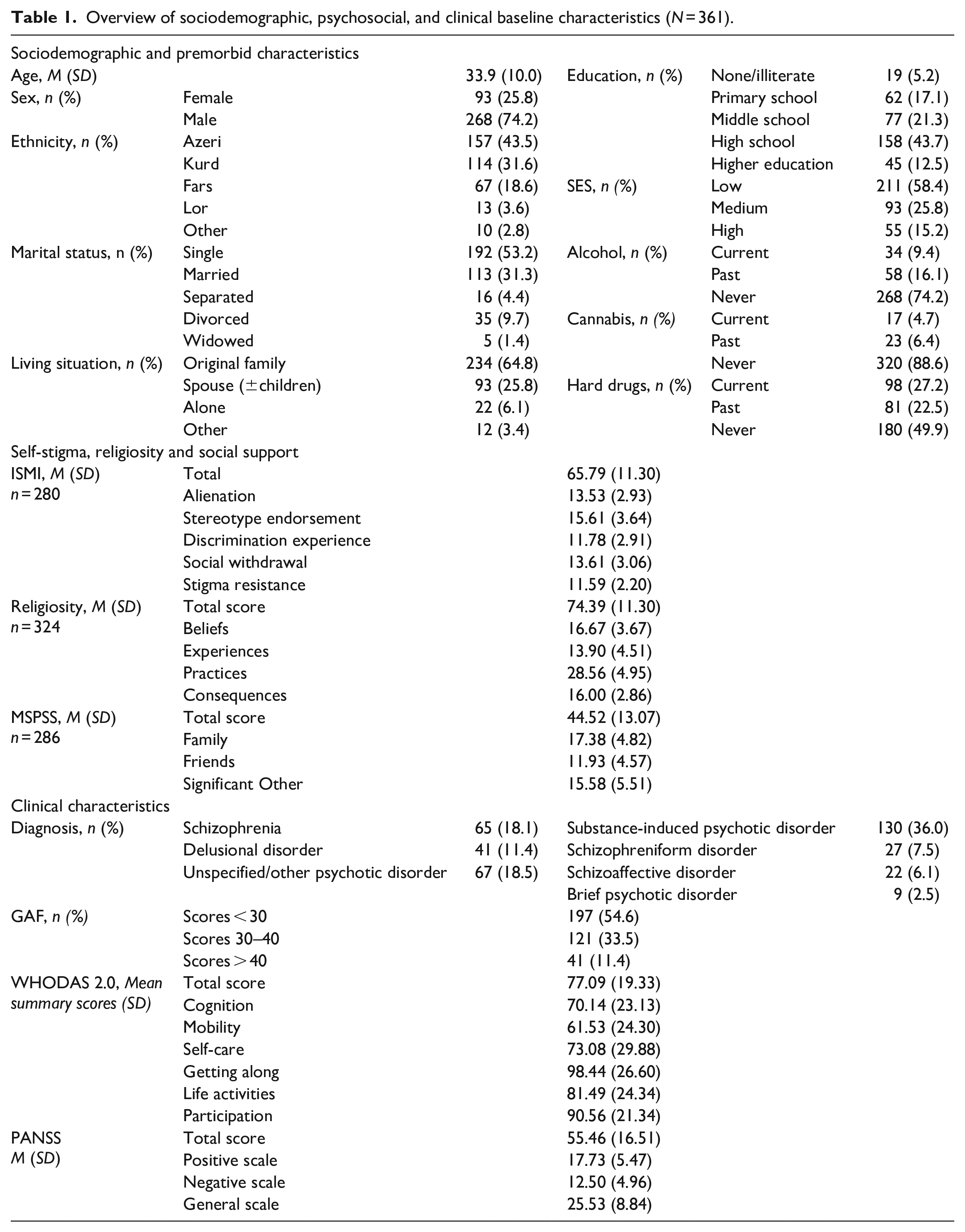
In total, 361 subjects were included in the study, 142 of which were recruited in Tabriz, 123 in Kermanshah and 96 in Tehran. The majority was male (n = 268, 74.2%) and the mean age was 34 years (range 18–68). Most participants lived with their family (n = 234, 64.8%) or spouse and children (n = 93, 25.8%). Less than 10% of the sample reported current use of alcohol (n = 34, 9.4%) or cannabis (n = 17, 4.7%) while 27.2% (n = 98) were using illicit drugs other than cannabis at the time of inclusion. The latter group entailed 69 (19.1%) opium users. The most common diagnoses were substance-induced psychotic disorder (n = 130, 36.0%), schizophrenia (n = 65, 18.1%) and unspecified/other psychotic disorder (n = 67, 18.5%).
Values on all of the psychosocial (predictor) variables were missing in 34 subjects, another 38 missed assessments of ISMI and MSPSS and 9 subjects missed scores only on ISMI. Missing value analyses indicated that the majority of cases lacking information on psychosocial factors were recruited in Tabriz. In the Tehran sample, there were 6 subjects with missing values, and in Kermanshah, there was none.
Regression analyses
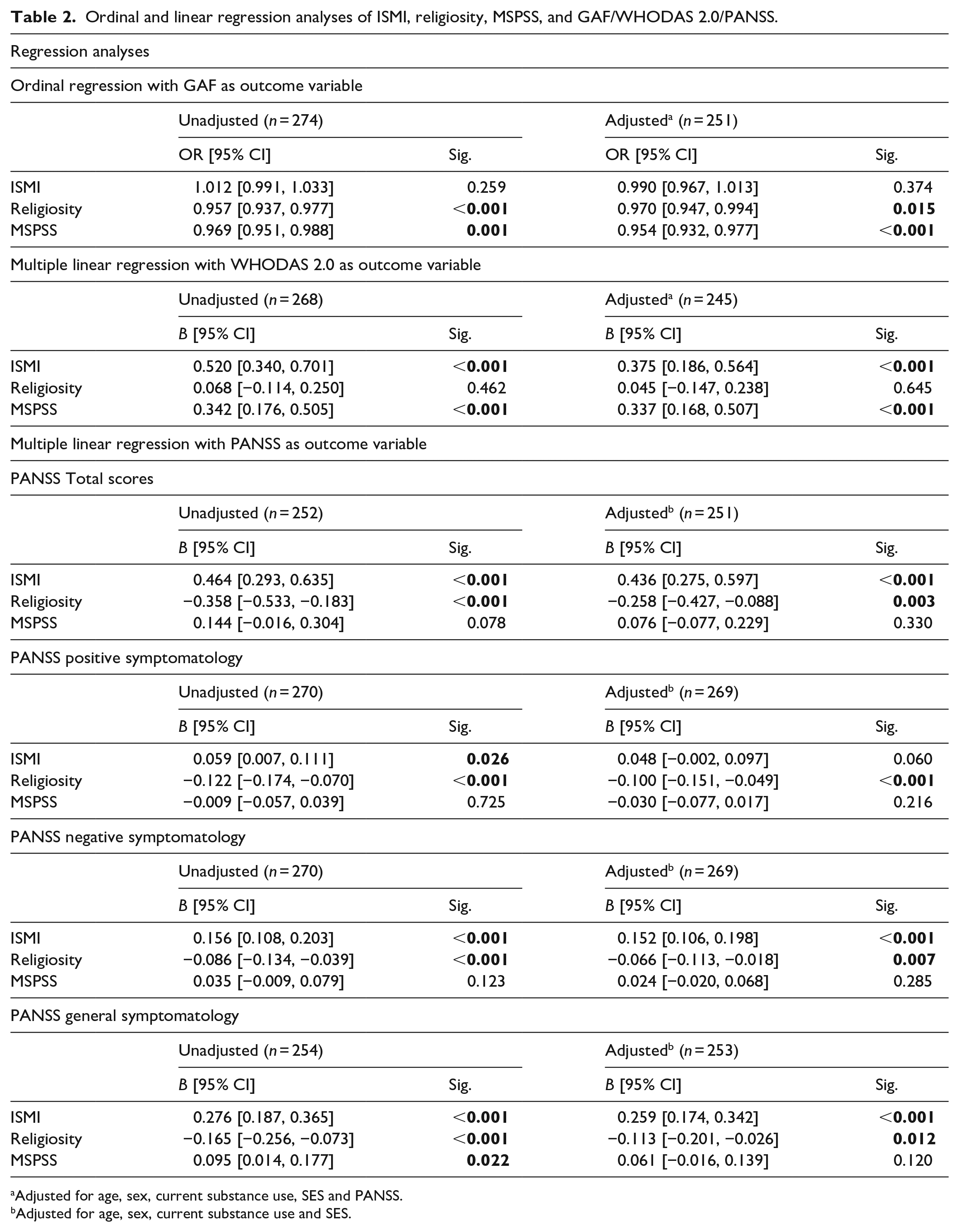
Results of the regression analyses are depicted in Table 2. For each model, we excluded cases with missing values listwise.
Ordinal and linear regression analyses of ISMI, religiosity, MSPSS, and GAF/WHODAS 2.0/PANSS.
Adjusted for age, sex, current substance use, SES and PANSS.
Adjusted for age, sex, current substance use and SES.
Self-stigma
Multivariable linear regression analyses indicated that higher levels of self-stigma were associated with poorer self-reported functioning, B = 0.375 [95% CI: 0.186, 0.564], p < .001, after adjusting for age, sex, SES, current substance use and symptom severity. Furthermore, higher self-stigma was associated with more severe symptoms, B = 0.436 [95% CI: 0.275, 0.597], p < 0.001. This association was found for overall PANSS scores and for the negative and general symptom dimension separately.
Religiosity
There were no significant discrepancies between internal/personal and simultaneous external/social dimensions of religiosity (Appendix 1). Higher scores on the Religiosity scale were associated with a decrease in the odds of having a higher categorized GAF score (i.e. better clinician-rated functioning), with an adjusted odds ratio (OR) of 0.970 [95%CI: 0.947, 0.994], p = .015. Conversely, higher levels of religiosity were associated with less severe symptoms, B = −0.258 [95% CI: −0.427, −0.088], p = .003. This association was found for overall PANSS scores and for every symptom dimension separately.
Perceived social support
An increase on the MSPSS (i.e. stronger social support) was associated with a decrease in the odds of having a higher categorized GAF score (i.e. better clinician-rated functioning), with an adjusted OR of 0.954 [95% CI: 0.932, 0.977], p < .001. Similarly, an increase on the MSPSS was associated with higher WHODAS2.0 scores (i.e. poorer psychosocial functioning), B = 0.337 [95% CI: 0.168, 0.507], p < .001.
Discussion
This cross-sectional study investigated associations of self-stigma, religiosity and perceived social support with symptom severity and levels of psychosocial functioning in 361 people with recent-onset psychosis living in Iran. Higher self-stigma was associated with more severe symptoms and lower levels of self-reported functioning. Being more religious was associated with less severe symptoms but poorer clinician-rated functioning. Perceiving stronger social support was associated with lower levels of self-reported functioning.
General characteristics – comparing ARAS to Western-European cohort
ARAS was designed analogously to the Psychosis Recent-onset Groningen Survey (PROGR-S) from The Netherlands (Liemburg et al., 2014). Here, we briefly discuss the general ARAS sample characteristics in comparison to the Dutch cohort in order to illustrate some of the potentially relevant differences in sociodemographic and clinical parameters.
Almost a third of the Iranian sample was married, while this was the case in 4.9% of PROGR-S participants (Liemburg et al., 2014). Also, 6.1% of ARAS participants were living on their own at the time of study inclusion, while this applied to roughly half of the Dutch sample (Liemburg et al., 2014). These factors may, for example, play a role in the identification, nature and/or progression of social withdrawal behavior, and seem worth to be investigated in future studies. Furthermore, our data indicates differences concerning drug use. Lifetime use of cannabis (a known risk factor for psychosis (Hasan et al., 2020)) and alcohol was relatively common in the Dutch cohort (61.7% and 44.5%, respectively), and only a minority had experience with other substances (2.3%) (Liemburg et al., 2014). In the Iranian sample, however, the majority said they had never used cannabis or alcohol (88.6% and 74.2%, respectively), while lifetime use of hard drugs was comparatively high (49.7%). Of note, opium use accounted for a large share of the latter. It was beyond the scope of the current study to investigate whether the observed differences in drug use, which might merely reflect the general population’s drug use habits, have implications for patients or their care providers. However, our observations underline the need to extend current psychosis research to diverse settings with regards to social, cultural and economic circumstances.
Self-stigma, religiosity, and perceived social support
Self-stigma
In a 2021 systematic review on self-stigma in SMI (Dubreucq et al., 2021), the authors report that levels of self-stigma amongst patients with schizophrenia were higher in the Middle East than in Europe, albeit all of the evidence for that patient population originated from Turkey. In the current study, mean scores on the ISMI appear to be somewhat lower than in a 14-country European survey on self-stigma in patients with schizophrenia (Brohan et al., 2010). This may be explained by the stage of illness, since people with prolonged psychosis seem to experience more self-stigma than patients in the early phases (Firmin et al., 2019). In any way, our numbers ascertain that self-stigma is a considerable issue in people with recent-onset psychosis.
The positive association between self-stigma and symptom severity is in line with results from previous research on people with psychotic disorders in general (Gerlinger et al., 2013), as well as those with recent-onset psychosis (Firmin et al., 2019; Kinson et al., 2018; Simonsen et al., 2019). Low self-esteem (Corrigan & Watson, 2002; Vass et al., 2015) and social stress due to defeat (Selten et al., 2016), social exclusion or minority status (Veling, 2013) are plausible explanations for underlying mechanisms, although self-stigma may not only lead to more severe symptoms but might, reversely, also be caused or aggravated by the symptoms. Next to having more severe symptoms, patients with higher self-stigma also had lower levels of psychosocial functioning, albeit only when assessed with the self-report tool. The fact that functioning levels were not associated with self-stigma when rated by clinicians might indicate that healthcare providers miss insight into the subjective burden of the disorder for the affected individuals, that is, the extent to which patients feel impaired by experiences of being stigmatized in their daily life.
Overall, the results correspond to our hypotheses and underscore the importance of addressing internalized stigma regarding their disorder in people with recent-onset psychosis, as this could ameliorate functioning or alleviate symptoms.
Religiosity
We found that levels of religiosity in our study population were within the moderate reference range (mean = 74.39, ‘moderate’ scores = 27–78). The role of religiosity in psychosis is quite equivocal. Religious delusions have been associated with poorer outcomes of psychotic disorders (Lucchetti et al., 2021; Mishra et al., 2018; Siddle et al., 2002), but religious faith by itself can be a source of strength, meaning and support for many people (Huguelet & Koenig, 2009). While a study using data from a WHO survey across 18 countries suggests that religiosity is related to psychotic experiences (Kovess-Masfety et al., 2018), several studies showed that religiosity is associated with positive outcomes in patients with psychotic disorders (Lucchetti et al., 2021).
Findings from the current study deviate partly from our hypotheses and may seem paradoxical, since being more religious was associated with less severe symptoms on the one hand, but with poorer (clinician-rated) functioning on the other. These somewhat inconsistent observations could be explained by the heterogeneity of what religiosity actually entails, and how different aspects of religiosity might, in turn, relate to outcomes of psychosis. For example, external/social dimensions are thought to be protective in the form of social support, but can also be harmful as a source of enforced social norms and even oppression (Huguelet & Koenig, 2009). Similarly, internal/personal dimensions of religiosity can provide meaning to a person’s life (Huguelet & Koenig, 2009), while a punitive image of God may lead to increased feelings of guilt or emotional distress (Weber & Pargament, 2014). Hence, individual circumstances and differential facets of religiosity might be key in determining whether religiosity plays a protective or harmful role concerning symptoms or psychosocial functioning, respectively. Qualitative research is needed to unravel the relations of specific aspects of religiosity with different symptom dimensions and areas of functioning under varying circumstances. Furthermore, future studies should investigate the discrepant results concerning clinician-rated versus self-reported social functioning levels.
Altogether, this study shows that religiosity is associated with symptom severity and functioning levels in recent-onset psychosis. Healthcare providers may be advised to explore the meaning of religiosity in their patients’ lives and differentially incorporate relevant aspects into individual therapeutic approaches, since addressing them harbors the potential to improve prognostic outcomes.
Perceived social support
Even though there is no specific MSPSS reference data for people with psychosis, perceived social support in our sample appears to have been weaker than in a group of healthy controls as well as psychiatric patients from a validation study of the MSPSS in Turkey (Eker & Arkar, 1995). This is in line with the current body of evidence indicating that social support is quantitatively and qualitatively poorer in people with psychosis (Gayer-Anderson & Morgan, 2013; Palumbo et al., 2015). Both in the current study and in a systematic review of 23 studies (21 of them being from HICs) investigating social networks in psychosis patients (Palumbo et al., 2015), family seems to be the biggest source of social support. However, this may, in fact, not be different from the general population, and should not undermine the importance of other sources of social support, for example, friends (Gayer-Anderson & Morgan, 2013).
Our hypotheses regarding social support have to be rejected: higher levels of perceived social support had no association with symptoms and were actually associated with poorer clinician-rated and self-reported psychosocial functioning. One plausible explanation for the latter is reverse causality. That is, people who were having (increasing) difficulty with functioning in daily life were also receiving – and perceiving – more social support. Another explanation might be that individuals lacking social support try to keep up their duties at work and other social roles longer than people with a social support net, as they cannot afford to withdraw from social roles without getting into financial and social troubles. The finding that perceived social support was not related with symptoms does not correspond to what we expected based on previous longitudinal research, where stronger perceived social support was associated with symptomatic remission in 123 people with early psychosis (Tempier et al., 2013) and with less severe symptoms after 3 years in 113 FEP patients (Norman et al., 2005). Our results could indicate that social support does not determine symptom severity during early disease stages, while it may well become relevant over time, for example, by promoting treatment adherence or when losing touch with friends. However, there has been earlier cross-sectional research showing that perceived social support was associated with less severe concurrent symptoms in 38 FEP patients (Sündermann et al., 2014). There are also suggestions that a decline in social support prior to FEP onset might be more relevant in determining symptom severity than the amount/quality of social support itself (DeVylder & Gearing, 2013). Since current conclusions must remain tentative, further replication studies are needed and should ideally also consider pre-onset and follow-up stages of psychosis.
In sum, this study found that perceived social support in people with recent-onset psychosis in Iran had no relation with concurrent symptom severity, and that social support was stronger in those with low functioning levels – probably as a reaction to the patients’ state rather than being a cause. Even though symptomatic outcomes might not be directly affected, a solid social support system is likely to be essential for adequate psychosocial functioning.
Strengths and limitations
To our knowledge, ARAS is the first large cohort study of people with recent-onset psychosis in Iran. Generalizability of our results is high due to the large sample size, the diverse and geographically broad catchment area, the study design and measures. Even though most participants were hospitalized at the time of inclusion, we believe that the ARAS study population reflects the general patient population of recent-onset psychosis, as it is common for patients suspected of having a psychotic disorder in Iran to be referred for evaluation and treatment to academic psychiatric centers, where admission typically ensues. Furthermore, this study investigated psychosocial factors that have never been researched in this particular setting before, while it is especially those factors that can be expected to differ under different sociocultural and economic circumstances (e.g. (Semrau et al., 2015)). This study thus represents one of the first larger-scale attempts to close the gap in evidence from the Middle East about psychosocial factors in people with psychosis.
There are also some limitations to the current study. First, the cross-sectional study design precludes from drawing conclusions about causality, which complicates the formulation of practical clinical implications. Second, we had to exclude 10% of the sample from the regression analyses due to missing values on key variables, though their sociodemographic data was useful for characterizing the hitherto unresearched patient population. Third, robust evidence concerning cross-cultural validity of our assessment tools in the Iranian context is lacking. Lastly, while most of our assessment tools are widely used and showed high internal reliability, GAF as an instrument to assess psychosocial functioning has some shortcomings, for example, in terms of reliability (Aas, 2010), and had to be subcategorized, which is uncommon and may inconvenience the interpretability of our results.
Conclusion
This study suggests that self-stigma, religiosity and perceived social support are associated with symptom severity and levels of psychosocial functioning in people with recent-onset psychosis living in Iran. Further cross-cultural qualitative and longitudinal research is needed to disentangle the relations between differential aspects of those factors and the respective outcomes. Nevertheless, based on the current findings, clinicians and/or public health professionals need to consider developing strategies to tackle the stigma around psychosis, incorporating aspects of religiosity in management approaches, and integrating the role of social support networks in preventative and therapeutic efforts.
Footnotes
Appendix 1
Acknowledgements
We thank everyone involved in ARAS, in particular the participants and clinical staff, and are grateful for the international collaboration on this project.
Availability of data and materials
Please contact the corresponding author (SF) to submit a data request for the ARAS cohort.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ARAS was funded by the Iranian National Institute for Medical Research Development (NIMAD). MD was funded by an internal research grant of the University Medical Center Groningen (MD-PhD number 21-40).
Ethical approval
ARAS is approved by the National ethical committee of the National Institute for Medical Research Development (NIMAD) in Iran in 2017 (record number: IR.NIMAD.REC.1396.101).