
Abstract
Background:
Caregivers are responsible for the home care of family members with severe mental illnesses (SMIs) and their lives are often subject to changes that can create stress and burden. The purpose of this study was to explore the current state of family disease burden and its correlation with social support among family caregivers of SMIs patients.
Methods:
Using a random sampling method, a total of 1,108 family caregivers of SMIs patients in community health service centers were selected. A general information questionnaire of family caregivers and patients, the Family Disease Burden Scale, and the Social Support Rating Scale were used.
Results:
The score of the Family Disease Burden Scale of 1108 family caregivers was 16.57 ± 10.65. Family disease burden was negatively correlated with social support (p < .05). The main influencing factors of family disease burden were average annual family income, duration of illness, distance to medical care, risk of unpredictable behavior, social support, caregiver-patient relationship, gender, and comorbid chronic conditions (p < .05).
Conclusion:
Family caregivers of SMIs patients have a relatively low level of caregiver-perceived social support. Interventions to enhance perceived social support could help maintain the health of family caregivers and improve the quality of family care.
Statement of clinical relevance
Our findings provide information on the relationship between the family burden of illness and social support among primary caregivers of patients with severe mental disorders, as well as factors influencing the family burden of disease. This information can help the government or hospital authorities to take the necessary measures to provide strategic support and interventions to benefit the physical and mental health of family caregivers and the mental recovery of patients.
Limitations
As a cross-sectional study, it is not possible to infer causal relationships between social support and family disease burden. Second, this study was conducted in regional mental health centers, and insufficient attention was paid to family caregivers of patients with SMIs who lacked motivation to seek care, which to some extent led to insufficient comprehensiveness of sample coverage. Therefore, more detailed sociodemographic characteristics among primary caregivers should be considered in future studies, and studies using longitudinal data may expand our understanding of the causal relationship between family burden of illness and social support.
Introduction
Severe mental illnesses (SMIs) are frequently chronic and relapsing disorders in which the illness’s symptoms are so severe that they substantially limit a person’s ability to adapt to social situations and perform other tasks (Ruggeri et al., 2000). An estimated 970 million individuals globally encountered mental disorders in 2019 (Dattani et al., 2021). In China, the six most widespread SMIs are schizophrenia, schizoaffective disorder, paranoid psychosis, bipolar disorder, epilepsy-related mental disorders, and intellectual disability with mental disorders (China, 2018). It has been estimated that as many as 6.43 million people living in China were suffering from SMIs in 2020 (Wufang et al., 2022). Mental disorders ranked second in terms of Years Lived with Disabilities (YLDs) in 2017 and currently account for roughly 20% of the total disease burden in China (Zhou et al., 2019).
Family burden of illness refers to the patient’s problems, difficulties, or adverse effects of the patient on his or her family and related members (or caregivers), and includes both objective burden and subjective burden (Alzahrani et al., 2017). Caring for a person with mental illness entails disturbance of daily routines, stigma and blame, discontent with family and relatives, financial concerns, physical loads, difficulties with patient adherence to treatment, and challenges with health services and government support (Evensen et al., 2017). In general terms, routine inpatient care was moved to community care facilities during the second part of the 20th century through the process of deinstitutionalization (Thompson & Doll, 1982). This trend has extended the detrimental impact of serious mental illnesses not only to the individual patient, but also to caregivers and families. Family caregivers of people with SMIs are often overwhelmed by the burden of caring for people with SMIs at home who had severely impaired social functioning, are in a prolonged state of illness, and are under physical, psychological, and financial pressure (Shiraishi & Reilly, 2019). At the same time, due to the associated stigma, family caregivers of people with SMIs are often too ashamed or reluctant to seek social support, or are even socially isolated, which further increases their caregiving burden (Chen et al., 2019).
Social support is the help that an individual gets through social relationships to reduce psychological stress, alleviate mental disorders, and enhance social activities, where the range of social relationships includes community, organization, team, colleagues, relatives, friends, and family (Langford et al., 1997). Studies have shown that providing adequate subjective and objective social support to family caregivers of people with SMIs and increasing their use of social support, can help reduce their caregiving burden, promote the recovery of people with SMIs, and enhance the sense of access for vulnerable families (Alyafei et al., 2021).
It was not until after the mid-1950s that the experiences of informal family caregivers of persons with mental illnesses came to the attention of researchers (Maurin & Boyd, 1990). However, there is a paucity of research on the burden of SMIs, with the limited available research focusing on persons with schizophrenia and less on other illnesses and family caregivers. Moreover, the influence of social support on family caregiver burden is not completely understood. Thus, this study investigated the current state of family disease burden and its correlation with social support in the families of caregivers of patients with SMIs, with the aim of providing a clinical and theoretical reference for the promotion of community mental health services.
Materials and methods
Participants
A cross-sectional design was used in this study, and all study participants were recruited from January to July 2022 at 23 community health service centers in Nanjing, Jiangsu Province, China, using a random number table method. Fifty family caregivers of patients attending outpatient visits were randomly selected in each community, and the final sample included in the analysis was 1,108 cases due to some missing data. Trained researchers used a structured questionnaire to collect data through face-to-face interviews. The study was approved by the ethics committee of Nanjing Medical University, and all subjects signed an informed consent form.
The diagnosis of SMIs was based on the diagnostic criteria of the Chinese Classification and Diagnostic Criteria of Mental Disorders (Chen, 2002). The inclusion criteria for the caregiver were as follows: (1) caring for the patient for more than 3 months; (2) at least 18-years-old; (3) able to understand, speak, and read Mandarin Chinese; (4) willing to sign informed consent after being provided with a complete explanation; and (5) not suffering from cognitive or psychiatric disorders or serious organic diseases.
Instruments
The general conditions of patients and family caregivers were surveyed by a self-administered questionnaire. The survey included the family caregiver’s gender, age, relationship with the patient, occupation, marital status, average annual household income, duration of care, and education level. Information related to the patient’s illness included the duration of illness, type of illness, risk of unpredictable behavior, and whether there was a family history of mental illness.
The risk assessment grading is divided into 0 to 5 levels according to the management and treatment specifications for severe mental disorders issued by the National Health and Wellness Commission of China (China, 2018; Qi et al., 2016), from mild to severe, as follows: Level 0: no behavior on any of the following levels 1 to 5; Level 1: verbal threats, shouting, but no vandalism; Level 2: appears to be vandalism but is limited to the home, is directed solely at the property, and can be persuaded to stop; Level 3: appears to be visibly vandalizing, is not confined to the home, is directed solely at the property, and refuses to stop; Level 4: appears to be persistently vandalizing, regardless of the occasion, against property or people, and cannot be persuaded to stop, including self-inflicted injury or suicide; Level 5: any act of violence against a person with a controlled dangerous weapon, or arson, explosion, and so on, whether in the home or in a public place. It is generally accepted that the risk of perpetration is low for levels 0 to 2, and high for levels 3 to 5 which require special attention.
Pai.S., an Indian scholar, developed the Family Burden of Disease Scale (FBS) to comprehensively and systematically understand the family burden of patients (Pai & Kapur, 1981). This study used the Chinese version of the Family Burden of Disease Scale to assess (Huang et al., 2021). It consists of 24 items in 6 dimensions: family financial burden (6 items), family daily activities (5 items), family entertainment activities (4 items), family relationships (5 items), physical health of family members (2 items), and mental health of family members (2 items). The higher the total score, the more severe the burden. Each dimension score is divided by the number of items in that dimension to obtain a standardized score. A positive response with a standardized score of greater than or equal to 1 indicates a moderate or higher burden. The percentage of positive responses is the rate of positive responses. Cronbach’s α was .916.
The Social Support Rating Scale (SSRS) was originally developed in China by Xiao (Shuiyuan, 1994). It consists of 10 items in 3 dimensions, namely objective support, subjective support, and use of social support. A higher overall SSRS score indicates a higher level of social support for family caregivers of persons with severe mental illnesses. The total social support score can be classified into low social support (scores of 12–22), moderate support (scores of 23–44), and high support (scores of 45–66). Cronbach’s α was .764 for the scale.
Statistical analysis
The statistical software IBM SPSS 26.0 was used to analyze the data. Count data were expressed as numbers of cases and percentages, and measurement data were expressed as mean±standard deviation. One-way analyses of variance (ANOVAs), t-tests, and Pearson correlation analysis were used to indicate statistically significant differences at p < .05. The regression analysis of family burden of disease was performed by stepwise regression with multiple linear regression.
Results
Family caregivers’ scores on the Family Burden of Disease Scale
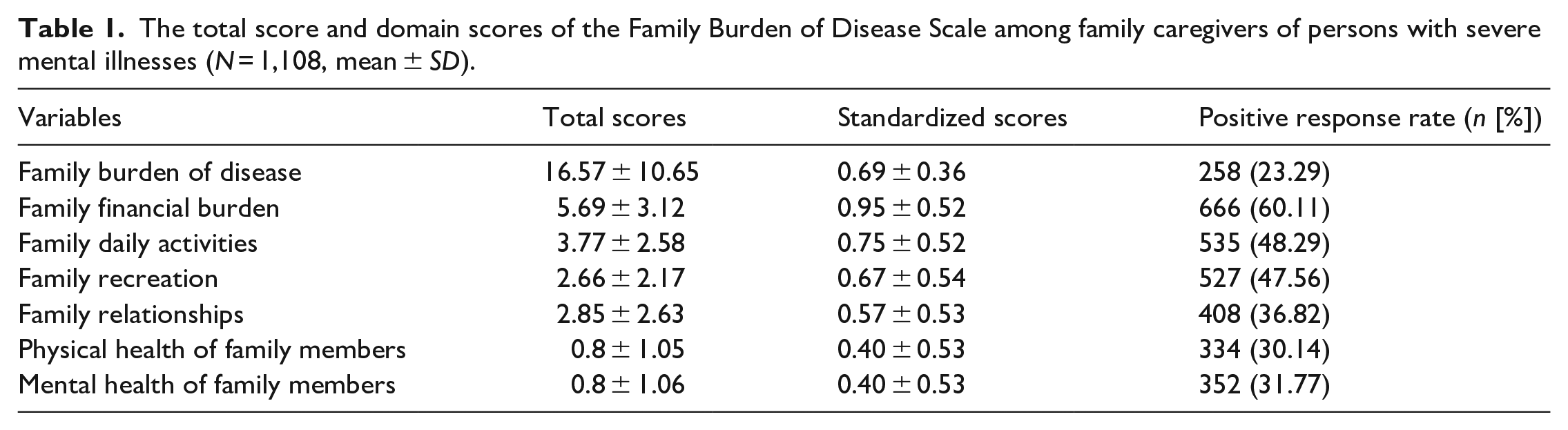
A total of 1,108 valid questionnaires were returned for this study, with 719 male and 389 female family caregivers aged 56.81 years (SD = 12.98). The mean scores for the family burden of disease entry for the patients’ family caregivers were 16.57 (SD = 10.65), and the positive response rates for each dimension of moderate or higher burden were, in descending order, family financial burden, family daily activities, family recreation, family relationships, family mental health, and family physical health (Table 1).
The total score and domain scores of the Family Burden of Disease Scale among family caregivers of persons with severe mental illnesses (N = 1,108, mean ± SD).
The differences in the scores of gender, age, education, occupation, relationship with the patient, duration of care, average annual family income, and marital status of the family caregivers were statistically significant (p < .05) (Table 2).
Family burden of disease scores for family caregivers with different socio-demographic characteristics (N = 1,108, mean ± SD).
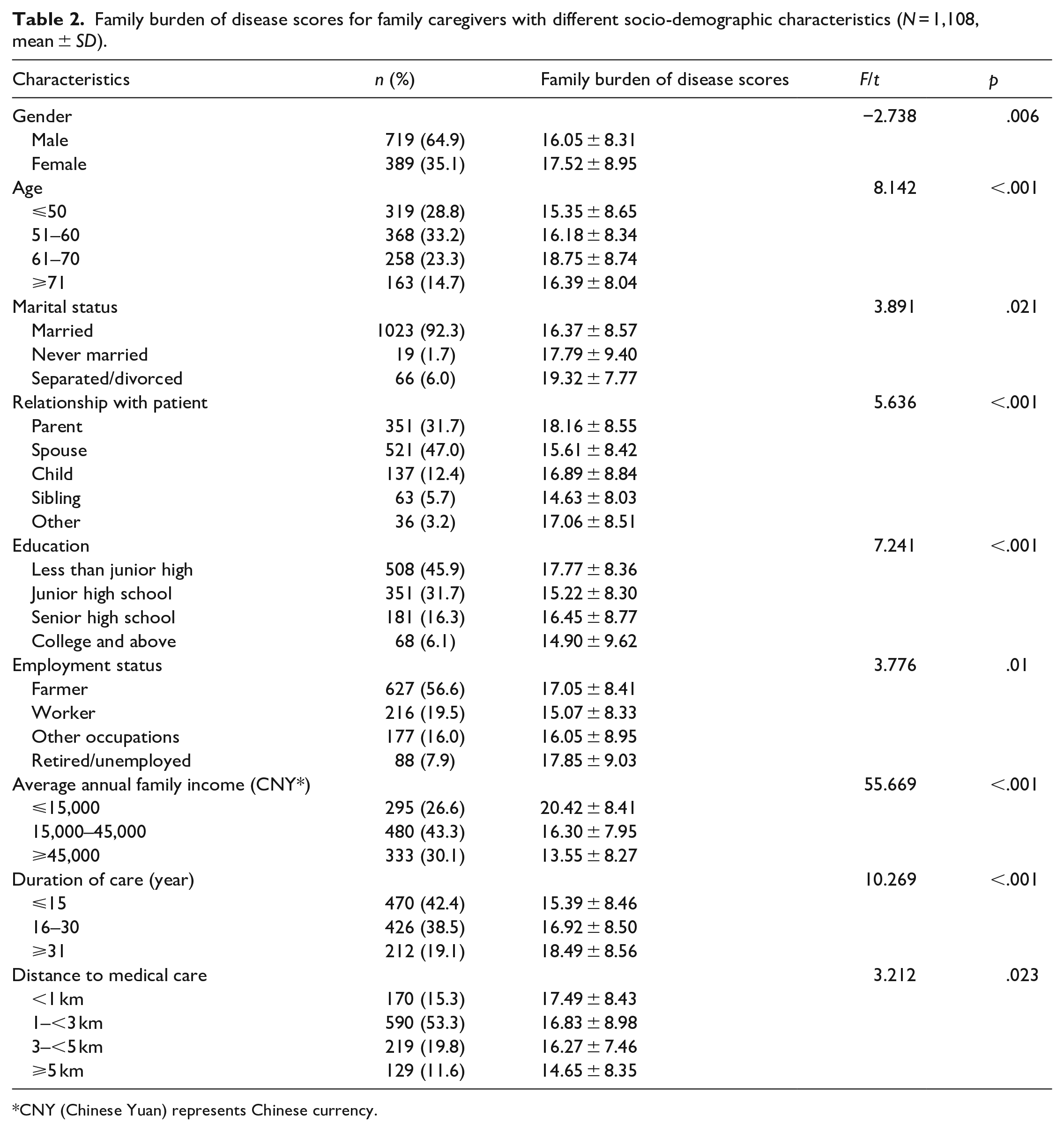
CNY (Chinese Yuan) represents Chinese currency.
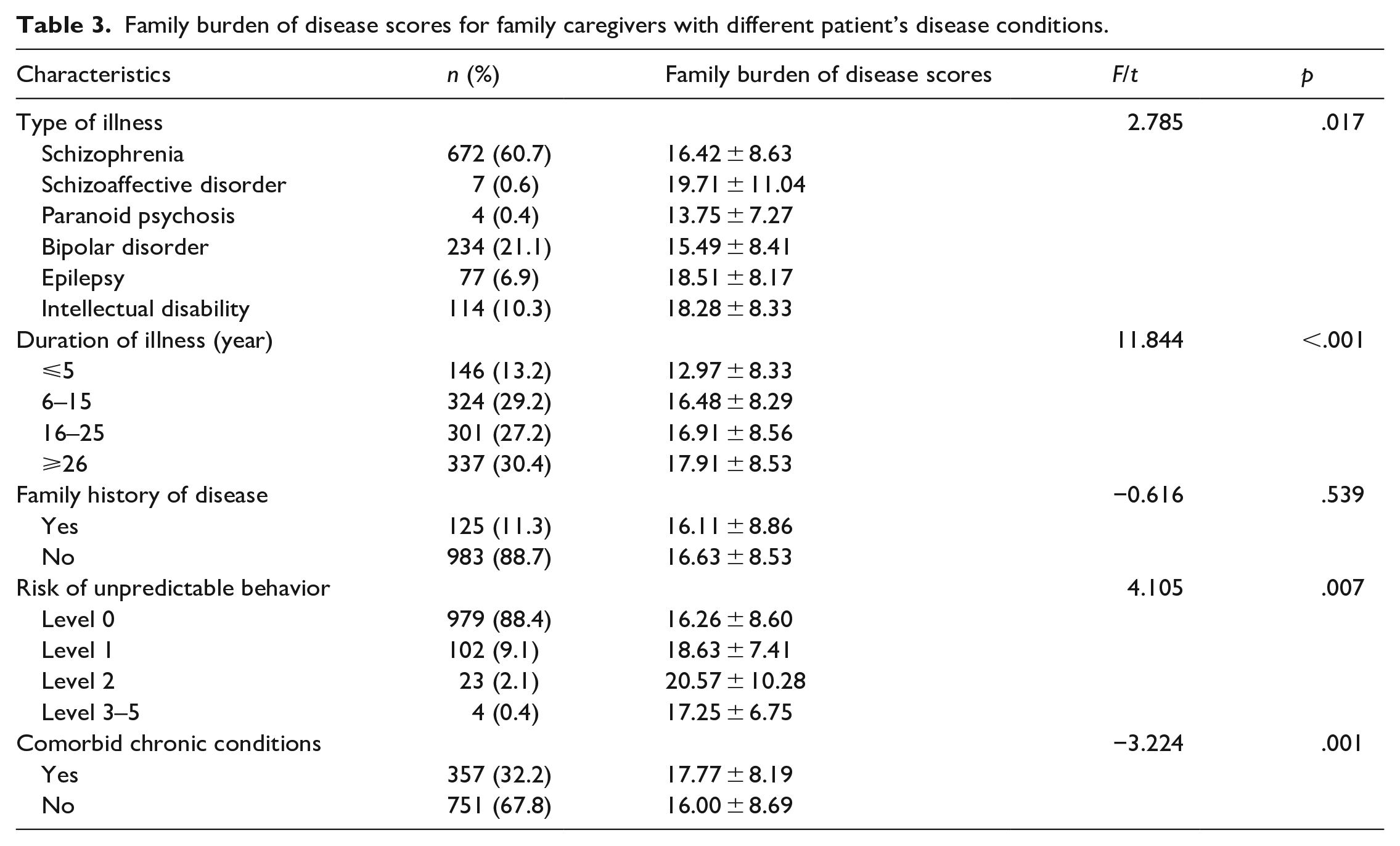
A total of 1108 patients were included in the analyses, 438 of them male and 670 of them female. Their age range was 17 to 89 years (50.66 ± 13.70). Table 3 showed the impact of the patient’s illness on the caregiver’s family burden of disease scores. There were significant differences in the family burden of disease scores for different illness types, duration of illness, risk of unpredictable behavior, and whether there were other chronic diseases (p < .05).
Family burden of disease scores for family caregivers with different patient’s disease conditions.
Correlation analysis of caregivers’ family burden of disease and social support
The average score of social support for family caregivers of people with SMIs was 37.64 (SD = 6.45), which was at an intermediate level. Pearson’s correlation was used to assess the relationship between the change in family burden of disease and the change in levels of social support. Table 4 indicated that the family burden of disease was negatively correlated with social support (r = −0.069, p < .05), objective support (r = −0.087, p < .01), and use of social support (r = −0.083, p < .01).
Correlation analysis of caregivers’ family burden of disease and social support.
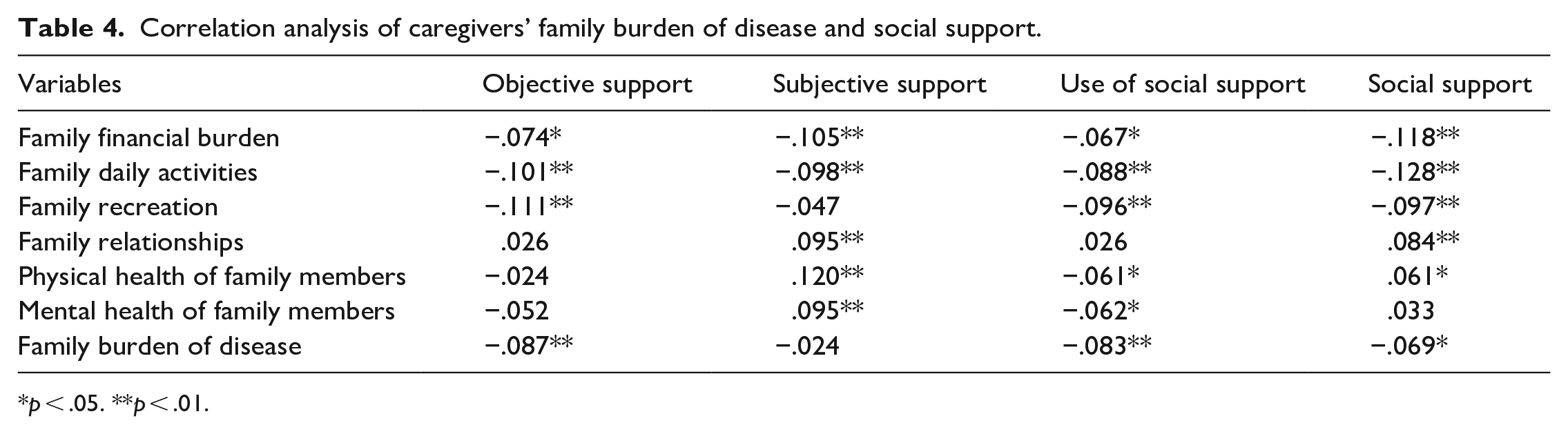
p < .05. **p < .01.
Multiple linear regression analysis of factors influencing caregivers’ family burden of disease
The total family burden of disease score was used as the dependent variable in a multiple linear regression analysis. The independent variables were social support and the statistically significant variables of univariate analysis (Entry level was 0.05, deletion level was 0.10). According to the results, the independent variables in the family burden of disease regression equation were average annual family income, duration of illness, distance to medical care, risk of unpredictable behavior, social support, caregiver-patient relationship, gender, and chronic diseases in turn (F = 25.064, p < .001) (Table 5).
Multiple linear regression analysis of factors influencing caregivers’ family burden of disease.
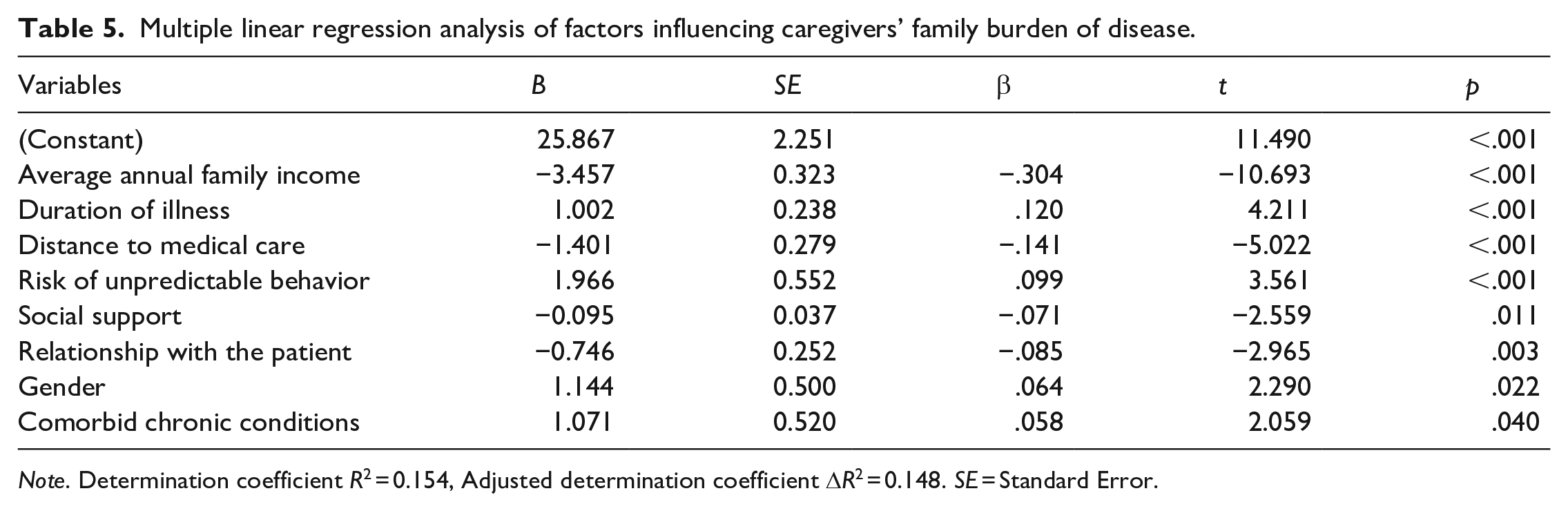
Note. Determination coefficient R2 = 0.154, Adjusted determination coefficient ΔR2 = 0.148. SE = Standard Error.
Discussion
The current family burden of disease situation
This survey revealed that the caregivers’ family burden of disease was at the mild to medium level, which was generally consistent with the results of most of the studies reported in the literature (Di Lorenzo et al., 2021). The majority of family caregivers (70%) were over 50 years old and either the parents (31.7%) or spouses (47%) of the person for whom they were caring. More than half of the family caregivers survey had been caring for the patient for more than 15 years, suggesting that most family members of persons with SMIs were long-term caregivers. As can be seen from the scores of the six dimensions of the family burden of disease, the positive rate of economic burden was the highest among the medium and above burdens, accounting for 60.1%, which may be related to the characteristics of the disease itself. SMIs are chronic long-term conditions with high disability and low employment rates (Shiraishi & Reilly, 2019). The costs of visits to a restructured hospital doctor, long-term anti-psychotic medication, accident and emergency, intermediate and long-term care services and productivity losses tend to be much higher in those with mental disorders than in those without (Abdin et al., 2021). Consequently, tremendous pressure, a longer duration of illness, disease stigma, and limited health care coverage probably are responsible for the high level of family burden of disease for caregivers (de Filippis et al., 2022). In clinical work, we should not only focus on the diseases and their therapies, but also on the health status and illness burden of the patient’s caregivers, which is directly related to the quality of care and recovery.
Analysis of the influencing factors of family burden of disease
Average annual family income
The results indicated that the burden of mental illness is greater for those with lower incomes and less wealth, which was consistent with the results of previous studies (Peng et al., 2019). The reason for this may be related to the medical costs associated with treating SMIs as chronic conditions (Shiraishi & Reilly, 2019). The annual household income directly affects the caregiver’s ability to pay for the patient’s medical expenses. Therefore, establishing a sound medical insurance system and increasing the proportion of medical insurance for mental diseases is of significance when it comes to reducing the burden on patients’ families (McAlpine & Mechanic, 2000).
Duration of illness
This study showed that the longer the duration of the patient’s disease, the higher the disease burden. Researchers have previously discovered that the caregiving burden inversely correlates with caregiving length (Crespo-Facorro et al., 2021; Peng et al., 2022). It is possible that the greater the duration of disease and treatment, the less likely family caregivers are unable to handle emergencies in a timely and accurate manner (Rahmani et al., 2022). The delay in the recovery of the patient’s disease and the caregivers’ fear that the disease will lead to a decrease in the patient’s ability to assume roles both within and outside of the family are likely to increase the psychological burden on family caregivers and should be given full clinical attention.
Distance to medical care
The results of the regression analysis revealed that the distance to medical care was a statistically significant factor influencing the burden of caregiving. However, this was contrary to the findings of other studies that the farther the distance, the heavier the burden (Billi et al., 2007; Nic et al., 2015). This may be related to the fact that the patients in this study participated in a free treatment program or that some patients were hospitalized.
Risk of unpredictable behavior
According to multiple linear regression analysis, patients with risk level 2 had the highest disease burden on caregivers’ families. Patients with SMIs may develop unpredictable and dangerous behaviors under the influence of the disease, even resulting in vicious incidents that cause casualties, property damage, heavy family burdens, and affect social security and operational order (Smith et al., 2018; Yamamoto et al., 2009). Patients should adhere to long-term medication treatment and regular review to help stabilize disease symptoms and restore social function, thereby reducing or even avoiding risky behaviors and relieving the burden of disease on the family caregivers (Wan & Wong, 2019).
Social support
Family disease burden was negatively correlated with social support, and regression analyses also showed that social support for family caregivers was a statistically significant factor influencing caregiving burden. These results are consistent with other studies that suggest that caregivers with higher levels of social support experience lower levels of burden (Tay et al., 2022), which may be attributable to the influence of stereotypes and the specificity of disease symptoms. Patients’ families often adopt an active avoidance attitude toward exogenous support after discharge and during community family therapy, which eventually leads to social withdrawal and family self-isolation (Lei & Kantor, 2021). Policymakers should precisely identify priority populations in need of social support among family caregivers of people with SMIs, leverage limited community resources to enhance social support for this vulnerable group, and promote interventions to reduce the burden of care (Sun et al., 2019).
Relationship with the patient
The regression analysis results also showed that the family caregiver’s relationship with the patient was a statistically significant factor affecting the caregiving burden, especially for parental caregivers. The reason may be that patients with SMIs differ significantly from their parents in terms of communication, emotional involvement and response, behavioral control, intimacy, and adaptability compared with ordinary families (Mendenhall & Mount, 2011). In addition, they must complete family tasks and manage matters arising from caregiving needs on their own, and the lack of appropriate support adds to their burden (Banerjee et al., 2016). They need to be supported by health care providers to develop strategies to adjust to their situation and maintain health and well-being.
Gender
What can be clearly seen in Table 2 is that the family burden of disease is higher for female family caregivers than for male family caregivers. This discrepancy could be attributed to the fact that in the Chinese cultural context, women are subjected to the dual pressure of family and work. Especially a married woman with children, not only to worry about family matters but also to care about the education of children. Another possible explanation for this is that women are more likely to suffer from common negative emotions and lower quality of life, such as depression and anxiety (Kiely et al., 2019). There is an urgent need for interventions to support caregivers, especially women who provide unpaid care work (Bhan et al., 2020).
Comorbid chronic conditions
According to the study’s findings, individuals with SMIs who also had co-occurring chronic diseases scored higher for the family burden of illness than those who did not. Diabetes, hypertension, cardiovascular disease, chronic obstructive pulmonary disease, and other chronic diseases are common in the study population. These patients face higher rates of disability and more complex symptoms, which require more specialized care from the family caregivers, thus increasing their disease burden (Correll et al., 2017; Vancampfort et al., 2015). The need to enhance all aspects of ancillary testing and the use of medications with fewer adverse effects allows for the timely detection of symptoms and reduces the burden on family caregivers.
Conclusion
In general, the family burden of illness and social support of the family caregivers of patients with SMIs in this study were at a moderate level. Findings indicated that social support and other predictors were significantly associated with family disease burden. Further research should be undertaken to investigate the effectiveness and feasibility of intervention strategies and psychosocial measures for burden reduction for people with SMIs and their family caregivers. In particular, such strategies can be targeted first at parental caregivers with low social support and the patients with SMIs who have a longer duration of illness and comorbid chronic conditions.
Limitations
As a cross-sectional study, it is not possible to infer causal relationships between social support and family disease burden. Second, this study was conducted in regional mental health centers, and insufficient attention was paid to family caregivers of patients with SMIs who lacked motivation to seek care, which to some extent led to insufficient comprehensiveness of sample coverage. Therefore, more detailed sociodemographic characteristics among primary caregivers should be considered in future studies, and studies using longitudinal data may expand our understanding of the causal relationship between family burden of illness and social support.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (Grant No.72374109) and the 2022 China Medical Board Open Competition Program (No. 22-475). The funders had no role in the design and conduct of the study, data collection, analysis, and interpretation; writing of the manuscript; or the decision to submit the article for publication.
Ethical approval
The study was approved by the Ethics Committee of Nanjing Medical University, and informed consent was required from all patients and family caregivers included.