
Abstract
Background:
The current global outbreak caused by COVID-19 has produced a unique situation with severe health and financial consequences. The fast and quick global impact called for an immediate response. A key public health action was the decision to amend the law to allow employees to work from home (WFH) whenever it was possible. In response to public health restrictions to stop the spread of COVID-19, organizations quickly switched to WFH without fully comprehending the effects of continued WFH on mental and physical health. Working from anywhere and at any time has made the separation between business and personal life more difficult. These modifications may cause employees’ workdays to be longer and to experience greater work-life conflict. Overwork and work addiction provide a greater risk to the public’s health and can harm various facets of mental and physical health, such as depression, anxiety, and sleep difficulties. There hasn’t been much research on the underlying processes that link workaholism to poor mental health, especially among Indian academics.
Purpose:
There is a rise in the number of people who are worried about their mental health in academic settings. The primary purpose of this study is to determine whether academicians in India can potentially have a healthy work-family balance, which may mitigate the negative impacts of workaholism and poor mental health especially due to the Work from Home system.
Methodology:
A population-based study was conducted on academicians (n = 456) at private and public universities in Delhi NCR, India. Workaholism, work-family balance, and mental health difficulties were all measured using self-reported scales in the study. By using path analysis, the proposed mediation model was evaluated. The survey responses had an accuracy rate of 80%. Based on the conceptual research framework, PLS-SEM path modeling is used to find the causal connection between the indicators and latent components.
Findings:
The findings indicated that workaholism has been associated with mental health in two different ways: directly and through work-family balance. The path analysis found a statistically significant relationship between work from home and mental health through workaholism and work-family balance. Increased levels of anxiety, depression, stress, headaches, exhaustion, and reduced job satisfaction were some of the mental health consequences of Work from Home.
Practical implication:
This study provides real-world guidance to human resource managers on how to prioritize composite-level interventions at all levels of the university to create highly satisfied employees, provide a good working environment, and improve employees’ mental health.
Originality/value:
Many researches have been done on the relationship between work-from-home and employee mental health, but relatively few have looked at how work-life balance and workaholism play a role in how work-from-home affects employees’ mental health. This study fills a need in the academic and practitioner literature by investigating the relationship between work-from-home from home and employee mental health as well as the mediating function of work-family balance and workaholism with regard to Indian higher education institutions.
Background
With the advent of COVID-19, the way we worked in the workplace changed dramatically. While the work-from-home (WFH) model was implemented as a temporary measure, it lasted longer than expected due to back-to-back COVID waves, and people quickly adapted to working in a digital environment without compromising their performance. People’s ability to work from anywhere and at any time has made work and personal life more complicated (Ng et al., 2007). As a result of these changes, employees had longer workdays and more work-life conflict, which impacted their physical and mental health (Oates, 1971).
Oats used alcoholism as an analogy to define workaholism. Workaholism, defined by Oates in 1971, is a work addiction characterized by persistent thoughts about work when not working, feeling compelled to work due to internal pressures, and working beyond what is expected (Oates, 1971). Although workaholism is motivated by internal pressure, the literature argues that workaholics are motivated by a compulsion to ‘should’ work rather than by a passion or enjoyment of working. Since then, the investigation into workaholism has grown rapidly, and a set of instruments for spotting workaholics have been created. Workaholism can have contradictory psychological, physical, and social effects on the individual exhibiting it and those closest to them. Both internal and external pressures are considered factors in working excessively and obsessively. For the majority of individuals, work is a need that provides numerous benefits, including financial security due to a regular paycheck, a sense of identity, a sense of success, and the capacity to give back to the community.
Workaholism is a phenomenon or behavior related to the job that includes ‘being excessively concerned about work, motivated by an uncontrollable work motivation, and investing so much time and effort in work that impacts other essential life areas’ (Raphael Snir et al., 2013). Workers who are workaholics tend to experience severe health problems and depression symptoms than those who simply put in long hours at their jobs. Because of workaholism, well-being is anticipated to suffer; the individual isn’t provided enough time to rest and feel good. HR professionals and counselors must contribute to career counseling practices to encourage employees to strive toward striking a healthy balance between work and personal time. The research work by Andreassen (2014) provides an in-depth overview of workaholism, examining its stable tendency toward excessive and compulsive working. The study aims to explore various aspects of workaholism, including its definition, prevalence, assessment methods, underlying causes, outcomes on health and well-being, interventions, and proposed future research directions. The target audience for this research includes both researchers and clinicians. The study’s findings are based on a thorough narrative review of the existing literature on workaholism. It indicates that research in this area has grown significantly in recent years. Several screening instruments have been developed to identify workaholics; however, these instruments lack a strong theoretical foundation and show limited convergence with related constructs. Workaholism is found to be linked with impaired health, well-being, and conflicts between work and family life.
The study conducted by Sharma and Sharma (2011) aimed to explore the relationship between personality factors and workaholism among academicians in two universities in the Jammu region of India. The sample comprised 145 participants, and the Dutch Work Addiction Scale was used to assess workaholism. The study found that neuroticism and conscientiousness have a significant negative impact on all three dimensions of workaholism. Salary negatively affected two dimensions of workaholism, while designation positively affected one dimension. The research provides valuable insights into workaholism and its correlates among academicians.
The working environment for university professors is modified due to recent changes in governance and management in institutions. Research shows that over the past few decades, the nature of work has transformed, with an increase in the number of long workdays and a rise in labor intensity in many industries (Mazzetti et al., 2014). Contrary to the widespread public assumption that academics is a low-stress profession, the contemporary working environment for many academicians is significantly different (Leung et al., 2000). Academicians constantly attempt to balance their personal and professional obligations while dealing with the persistent stress of handling expectations in a frequently hypercompetitive atmosphere. There is a constant worry that somebody might mess up, and if that has to happen, they would feel alone and responsible. The system assumes that we are mature, skilled, and resilient enough to handle all the pressure that comes with the work. Although working as an academician at a university might be one of the most respectful careers, it has also evolved as one of the most stressful occupations.
According to some prior studies, the best way to understand workaholism is from the family perspective, where certain types of family dynamics, such as excessive duty, affect individuals within the system (Robinson, 1999). Sometimes the need to support one’s family might result in long work hours that reflect the feeling of carrying too much responsibility. When employees are more involved at work, it becomes harder for them to combine work and family life responsibilities. Due to greater responsibilities, higher workloads, and technological advancements in North America, the number of hours worked has increased, especially among highly educated people. This has created a disparity between work and life (Aziz & Zickar, 2006). Workaholics who fall short of their expectations may feel a loss of resources (a sense of inadequacy), and to make up for it, they could push themselves more aggressively to complete their own set goals (Bakker et al., 2009). The relationship between workaholism and total work-life balance (WLB), or Work-family conflict (WFC), has been the subject of numerous types of research. The workaholic group, those with high levels of work involvement and drive but low levels of job satisfaction, reported a higher level of imbalance between work and life than the other worker types (Aziz, Adkins, et al., 2010; Aziz & Zickar, 2006). In a different study, Aziz, Wuensch, et al. (2010), predicted that workaholism and work-life balance would positively correlate for white workers, but this relationship would not be significant for black workers. However, they discovered that workaholism and work-life imbalance significantly correlated for both groups (Aziz, Wuensch, et al., 2010).
Khilochiya and Patel (2021) conducted a study on Work-Life Balance among women employees in service sectors such as Banking and Financial Services, Hospitals, Hotels, Education, and Telecommunication. They used a validated psychometric instrument developed by Hayman (2005) to measure WLB, adapted from a scale created by Fisher-McAuley et al. (2003). The paper identifies statistically significant relationships between WLB factors and five demographic parameters among women employees. Overall, the study provides valuable insights into the work-life balance experiences of women in the mentioned service sectors and emphasizes the importance of considering spiritual involvement in understanding and promoting work-life balance.
The study conducted by Satyanarayana and Shanker (2012) focuses on work-life balance among 100 employees in the IT Enabled Services sector in India. They collected data using a structured questionnaire and measured work-life balance using a 15-item scale validated by J. Hayman, adapted from Fisher-McAuley et al. (2003). The paper highlights that work-life balance can be achieved through effective time management, open communication, planning, and setting priorities. It suggests that employees can derive satisfaction from each busy day by considering it well-spent and creating a transparent compartment between work and home life. The study emphasizes that employees can seamlessly manage work and home responsibilities with proper effort and time management.
Robinson (1999) examined the relationship between workaholism and mental health (MH) from 1980 to 1998 and found that workaholic behaviors are associated with stress and unfavorable health outcomes (Robinson, 1999). Unbelievably, the number of hours worked was unrelated to the expected health outcome, but the inability to take breaks from work is associated with other harmful health effects such as fatigue and physical complaints (Schaufeli et al., 2008). Studies show that workaholics report relatively high levels of workplace stress and mental health issues to support the claim that workaholism also hurts health (Fassel, 1990). In particular, workaholism may be linked to poor mental health since it causes workaholics to continuously and regularly consider their occupations even when not working. Workaholics may eventually get emotionally or cognitively drained because they may not have enough time or opportunities to recover from their excessive job effort through leisure activities (Burke et al., 2004). In recent years, employers have demonstrated a willingness to develop strategies and programs to increase feelings of belonging to their work to enhance job performance (Böckerman et al., 2012). Although the methods may help companies get a better job done, they may also hurt employees’ mental health. This is due to the potential of workaholism that arises when employees face such demanding conditions and may decide to spend more time at work managing job expectations.
Employees’ mental health may be at risk, which could have detrimental effects (Schaufeli et al., 2009). According to psychological stress theories, common pressures (such as personality traits and stressful situations) can produce depression over the long term or short term. Work addiction and long hours might also make it more difficult to control one’s resources (such as mental capacity, physical stamina, social interactions, and effort). As a result, stress will show up in many areas of life, including sleep disorders (Kubota et al., 2010), interactions between people that are hostile and unhealthy (Scott et al., 1997), and family conflict (Robinson, 1999; Schaufeli et al., 2008). Depressive symptoms could then worsen due to the perceived stress from work and personal duties (Frone et al., 1997). Chronic fatigue is among the conditions that are most frequently linked to overwork and depression. Faintness is a subjective feeling, experience, perception, or awareness that is analogous to extreme exhaustion brought on by mental or physical exertion. People may experience depression, especially if they have obsessive tendencies but are unable to work due to chronic exhaustion. According to a 2017 RAND Europe report, 37% of academic staff have a mental health issue. In the same year, a British study discovered that 43% of the academic studies had symptoms of a mild mental health issue, the most common of which are depression, anxiety, and burnout (Zhang & Gutierrez, 2007). Working from home impacts one’s physical and mental health; spending more time at home makes people feel more worried and sadder overall, frequently prompting changes in routines and eating habits. These alterations in eating behaviors and physical activity patterns may combine with additional pressures associated with working from home to negatively impact physical and mental health (di Renzo, Gualtieri, Pivari, et al., 2020).
Additionally, because they must manage to educate their kids in addition to busier employment with additional distractions, professionals with children are probably more likely to be impacted by these practices. Not all workers have private workstations in their homes, which leads to sharing workspaces with children who must attend school remotely, putting up temporary desks, or working in different locations during the day, such as sofas, beds, and coffee tables (Thompson, 2020). Employees who work from home may also spend more time at their workstations since they don’t have to commute, make fewer business trips, and participate in more online meetings than in-person at various locations. Increased stress brought on by co-workers, lousy body mechanics caused by an unsuitable physical workspace, and prolonged periods of inactivity are just a few of the many causes of increased discomfort and suffering.
Kumaranayake and Srimathi (2016) conducted a study to assess the reliability and factor structure of the General Health Questionnaire (GHQ-28) in a sample of 260 university and college students from South India. The study findings supported the GHQ-28 as a reliable tool with strong internal consistency for evaluating the mental health of the participants. Similarly, Venugopal et al. (2022) conducted a population-based cross-sectional study to examine the mental health status of the general Indian population during the COVID-19 pandemic. They utilized the General Health Questionnaire to evaluate the mental well-being of the participants. The research highlighted the unexpectedly high prevalence of psychological stress among the population. It emphasized the importance of implementing mental health management programs and raising awareness about the pandemic’s impact on mental well-being.
The existing research lacks a comprehensive exploration of how workaholism impacts employees’ mental health within the context of the COVID-19 pandemic and remote work. While some studies have discussed workaholism, its related factors, and the consequences of prolonged remote work, limited research explicitly addresses the link between workaholic tendencies and mental health during the pandemic. The changes in work patterns caused by the pandemic necessitate investigating how workaholism may have intensified in the remote work environment, where the lines between work and personal life are blurred. This situation could lead to longer work hours and increased work-life conflict, potentially harming employees’ mental well-being. Therefore, there is a pressing need for research that specifically examines how workaholism has manifested and evolved in the remote work context and its contribution to mental health issues.
Moreover, research on the specific challenges faced by different occupational groups, such as academicians, concerning remote work and workaholism is limited. Different professions may encounter unique stressors, and work demands that interact differently with workaholic tendencies. Exploring these distinctions can help identify targeted interventions and support systems customized to the needs of specific occupational groups.
An extensive literature review indicates a research gap that requires in-depth studies focusing on the relationship between workaholism and mental health outcomes during the COVID-19 pandemic and remote work. Additionally, investigating effective interventions and understanding the specific challenges faced by different occupational groups can provide valuable insights for organizations and professionals aiming to support their employees’ well-being in the ever-changing work landscape.
By utilizing the scales BWAS, WLB, and GHQ-28, which have been used in previous Indian studies with different respondent groups, this research addresses the gap in the literature by examining workaholism among academicians, making it a pioneering attempt in this direction.
Aims of the study
Numerous studies have looked at the relationship between workaholism and its effects on mental health and work-family balance, but these earlier studies were mainly focused on academicians in India and did not address the relationship between work-from-home and mental health through the mediating role of workaholism and work-family balance, this study attempts to address and fill these knowledge gaps.
The following research questions are developed in light of the hypothesized relationships between the study variables and the research objectives:
RQ1: How do workaholism and mental health relate to one another?
RQ2: What connections can be drawn between work-from-home and workaholism?
RQ3: How do work from home and maintaining a work-family balance connect?
RQ4: What connections exist between work-family balance and mental health?
RQ5: What connections exist between workaholism and work-family balance?
RQ6: What is the relationship between mental health and work from home?
RQ7: How does work-family balance affect the link between workaholism and mental health?
RQ8: How does work from home affect the link between work-family balance and mental health?
Conceptual framework
The theoretical foundations that are used to build the conceptual framework give the overall research direction (Figure 1). The theoretical underpinnings and underlying assumptions of the framework are completely covered in the section on literature reviews. The current study aims to explore the connections between academicians’ Workaholism, Work from Home, work-family balance, and mental health in public and private universities of North India. Given the potential connections between the research variables and the study aims, the following model is designed:
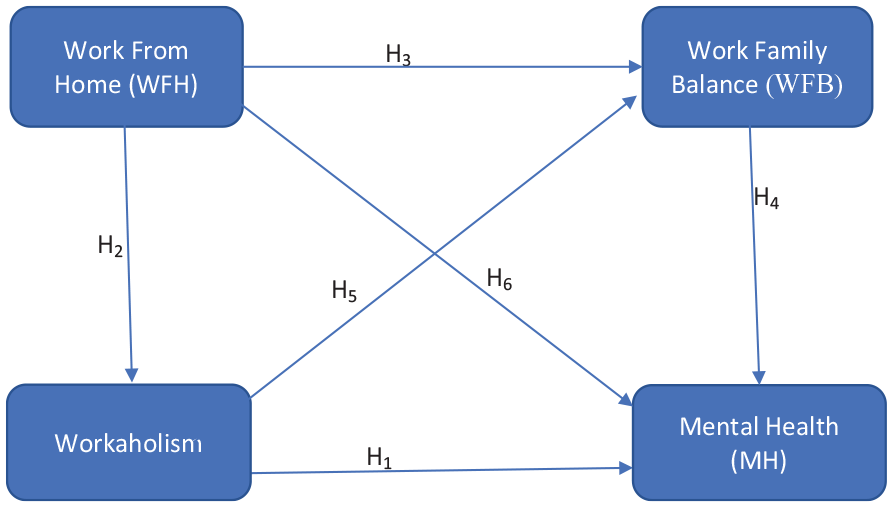
Conceptual framework tested in this study.
H1: Workaholism has a direct and negative impact on mental health.
H2: Work from Home has a direct and negative impact on Workaholism
H3: Work from Home has a direct and negative impact on Work-Family Balance
H4: Work-Family Balance has a negative impact on Mental Health
H5: Workaholism has a negative impact on Work-Family Balance
H6: Work from Home has a negative impact on Mental Health?
H7: Work from Home has a significant impact on Mental Health through Workaholism and Work-Family Balance
H8: Workaholism has a significant and mediating role between Work from Home and Mental Health
H9: Work-Family Balance has a significant and mediating role between Work from Home and Mental Health
H10: Workaholism has a significant and mediating role between Work from Home and Work-Family Balance
H11: Workaholism has a significant and mediating role between Work-Family Balance and Mental Health
Methods
Procedure and participants
The respondents included in this research work are from clinical academic settings; a total of 475 academicians working at a private and public university in Delhi NCR of India were invited to participate in a survey through email and social media platforms. The final size is 456 after removing a few erroneous and ambiguous responses. All information was collected anonymously, and survey participation was entirely voluntary. The selection of specific universities and the number of participants from each institution in the study are influenced by various factors. To begin with, researchers opt for those universities which are known for their expertise and reputation in the medical field. The study includes institutions with a strong track record to ensure that data is collected from knowledgeable and qualified participants, thereby enhancing the study’s credibility and validity. Additionally, the relevance of universities and departments to the research topic is a crucial consideration. Moreover, the number of participants chosen from each university is carefully determined to ensure an adequate sample size for statistical analysis and drawing meaningful conclusions.
The research participants’ demographic information, encompassing gender, age group, and university, is summarized in Table 1, which illustrates the characteristics of the respondents.
Demographic characteristics.
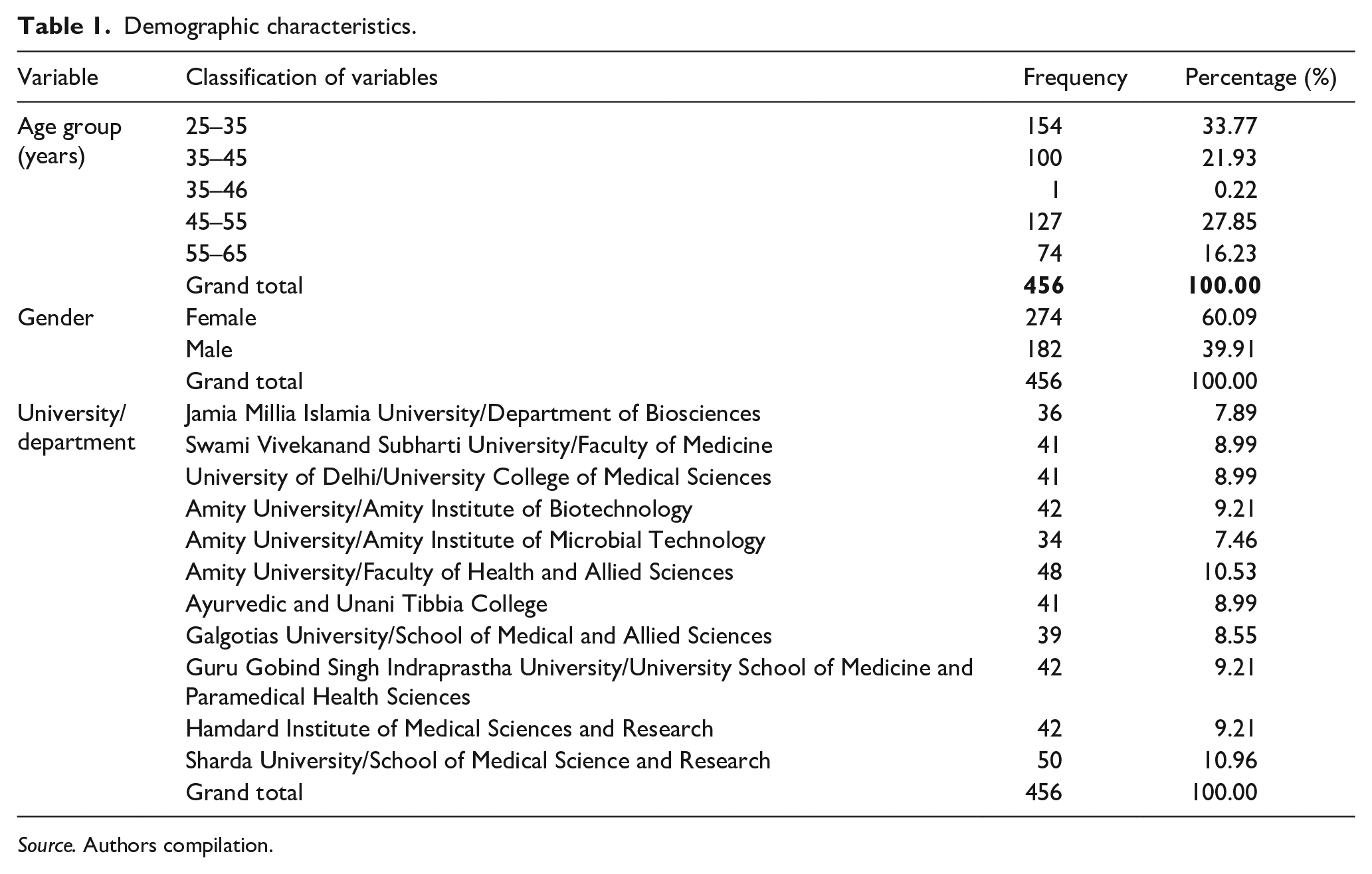
Source. Authors compilation.
The data presented in the frequency and percentage tables summarize the distribution of participants across different categories in the study. In terms of age groups, the majority of participants (33.77%) fall in the 25 to 35 years age range, followed by 21.93% in the 35 to 45 years age group and 27.85% in the 45 to 55 years age group. There is only one participant (0.22%) in the 35 to 46 years age category, which is an outlier. Additionally, 16.23% of participants are aged between 55 to 65 years.
Regarding gender, the study includes a higher percentage of female participants (60.09%) compared to male participants (39.91%). Regarding university/department, the highest number of participants (10.96%) are from Sharda University/ School of Medical Science and Research, and each of the other categories has around 8% to 9% of participants. These findings shed light on the participants’ demographics, which could be crucial for understanding any patterns or trends related to the studied variables.
Measures
The following measures have been incorporated in this study based on the extensive literature review.
Workaholism
Andreassen et al. (2015) conducted a comprehensive examination of various workaholism scales, including DUWAS, WART, and WorkBAT, using an addiction perspective. Nevertheless, they discovered that these scales lacked a robust foundation in addiction theory, leading to a deficiency in face validity. Expressing dissatisfaction with this situation, the researchers designed a novel and more concise scale, aiming to better align it with addiction theory for simpler implementation in clinical settings. This innovative scale, known as the Bergen Work Addiction Scale (BWAS), stands out as the first single-dimensional workaholism scale. The Bergen Work Addiction Scale was created by Andreassen et al. (2015) based on the premise that Work Addiction (WA) measures should be strongly linked to the main components of addiction given the origins of the construct in the field of addiction (Oates, 1971). The BWAS, which consists of seven items and measures a single dimension called Work Addiction, thereby measures each of the essential elements of addiction (Griffiths, 2011). A person with addicted behaviors may also face psychosocial or medical problems. Salience is one of them, along with toleration, mood modification, relapse, withdrawal, conflict, and problems. There are seven items on the scale, one for each of the aforementioned elements. Each item is given a grade on a Likert scale, from a range of 1 (never) to 5 (always).
Work-family balance
People are the most vital connecting link between a business and its success, and work-life balance is concerned with them. When stress experienced at work spills over into the home, employees face family conflict. Hayman 2005 developed a psychometric measure to assess WLB in organizations; the employee perspectives on WLB were gathered using a 15-item scale which was initially designed as a 19-item scale by Fisher-McAuley et al. (2003).
Work from home
A 5-point Likert scale with a range of 1 (much lower) to 5 (much higher) has been used in previous studies to evaluate several aspects of work from home. The same measure is used in the present study to report changes in workload expectations, workplace interruptions, co-worker communication, and workstation differences.
Mental health
Self-report screening tools like the General Health Questionnaire - 28 (GHQ-28) are used to look for potential psychological disorders. The GHQ-28 highlights two key issues: (1) the incapacity to do routine tasks; and (2) the emergence of novel, upsetting circumstances (Goldberg & Hiller, 1979). The scale consists of four dimensions, each represented by seven items: Severe depression (e.g. ‘Feeling that life is completely hopeless’), somatic symptoms (e.g. ‘Feeling that you are ill’), anxiety/insomnia (e.g. ‘Feeling nervous and strung-out all the time’), and social dysfunction (e.g. ‘Feeling that you are playing a useful part in things’). A 5-point Likert scale is used to grade each item, with higher scores indicating more significant issues.
Survey instrument design
This study utilized scales from previous research on work-from-home, mental health, workaholism, and work-family balance. The dimensions of work-life balance were developed by Hayman in 2005, the workaholism scale was adapted from the Bergen Work Addiction Scale (BWAS) by Andreassen et al. (2012), and the GHQ-28, a scale used to assess mental health conditions, was also employed. To validate the construct and reliability of the chosen scales, this research work demonstrated the validity and reliability of each construct, following the guidelines suggested by Fornell and Larcker (1981).
Data collection is started after checking the research instrument’s appearance validity. The research was presented to the six selected subject specialists to establish face validity. The questionnaire was ultimately ready for pre-testing after considering all experts’ suggestions on a five-point Likert scale. Forty surveys were initially distributed to them to determine the intended respondents’ opinions of the ideas’ clarity and comprehensibility. The survey questions were further modified in response to their feedback to ensure everyone could comprehend them. Cronbach’s alpha was used to evaluate the reliability and internal consistency. The results of a pilot test (N = 40) were assessed using structural equation modeling and partial least squares in this study.
Data collection and sampling
A benefit of PLS-SEM is that results are unaffected by a limited sample size. To determine the appropriate sample size, this study used the following statistical approaches:
(a) Tables for calculating sample sizes (Krejcie & Morgan, 1970).
(b) The instrument’s scale design, which indicated that a maximum sample size of 384 is required for a 5-point Likert scale.
(c) The sample size for this investigation was established using G*power’s a-priori power analysis estimation.
The sample size of 475 ought to be sufficient because the highest of the three options has been chosen. The final size is 456 after removing a few erroneous and ambiguous responses. The respondents were given a standardized questionnaire to collect the required information. Employees of universities in the National Capital Region of Delhi responded to the survey. Convenience sampling is used to collect the responses from September 2021 and October 2022.
Non-response bias
The primary issue is non-response bias, which impacts how results are generalized (Michie & Marteau, 2010), therefore, researchers need to address this issue (Ritchie et al., 2013). The systematic distinction between those who responded to a survey and those who were invited but did not respond is known as response bias (Menachemi, 2011). This study has ensured that the problem is resolved by completing all necessary tasks. To conduct wave analysis, the data is divided into two datasets (early respondents vs late respondents). Comparing the responses from early and late responders allowed the study to assess the possibility of non-response bias (Armstrong & Overton, 1977). The results of the t-test, which corroborate the non-response bias and have little relevance to our work, do not demonstrate a statistically significant difference between the early wave (182) and later wave (274) groups (p = .49). In the end, it is determined that 456 surveys could be analyzed.
PLS-SEM
PLS-SEM path modeling is utilized to determine the causal relationship between the indicators and latent components, following the conceptual research framework. This study assesses and expands on the idea that PLS-SEM provides greater flexibility as a modeling tool for research constructs compared to maximum likelihood.
Results
Respondent’s profile
The sample of this study is academicians from public and private universities in the Delhi NCR region of India. Academicians who work in different public and private universities contributed to the study by responding to the questionnaires. About 40% of respondents are male, and 60% of respondents are female. In terms of age, the majority of respondents age 33.77% is between 25 and 35.
Measurement model
The internal consistency of the constructs is assessed using the multi-item reflection scale. It is noteworthy that all constructs exhibit remarkable internal consistency, as indicated by Cronbach’s alpha values surpassing Nunnally’s threshold of 0.7 (Nunnally, 1967). It has been suggested that an AVE (Average Variance Extracted) exceeding .5 offers empirical evidence for convergent validity. This is because the corresponding latent variable explains over 50% of the variance in the related indicators, while other latent variables account for less than 50% (Fornell & Larcker, 1981). All AVE values in this study (.777 and .579) surpass the threshold of .5, confirming convergent validity. Table 2 demonstrates that all research constructs exhibit exceptional levels of internal consistency and reliability, with outer loadings for the items exceeding the minimal threshold value of 0.6.
Reliability and validity.
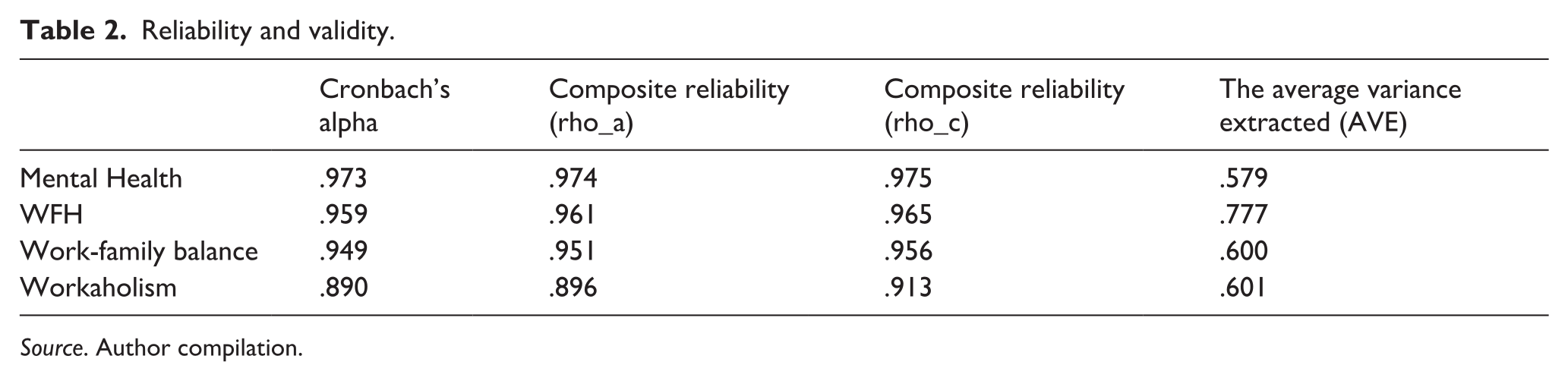
Source. Author compilation.
The study examines the discriminant validity of the constructs using the Fornell and Larcker (1981) criterion. In Table 2, the off-diagonal values demonstrate the relationships between the latent constructs, indicating their discriminant validity. This is further validated in Table 3, where the inter-correlations are compared with the AVE values. The research concludes that the constructs have discriminant validity as the shared variance values are lower than the corresponding AVE values (Fornell & Larcker, 1981).
Analysis of discriminant validity.
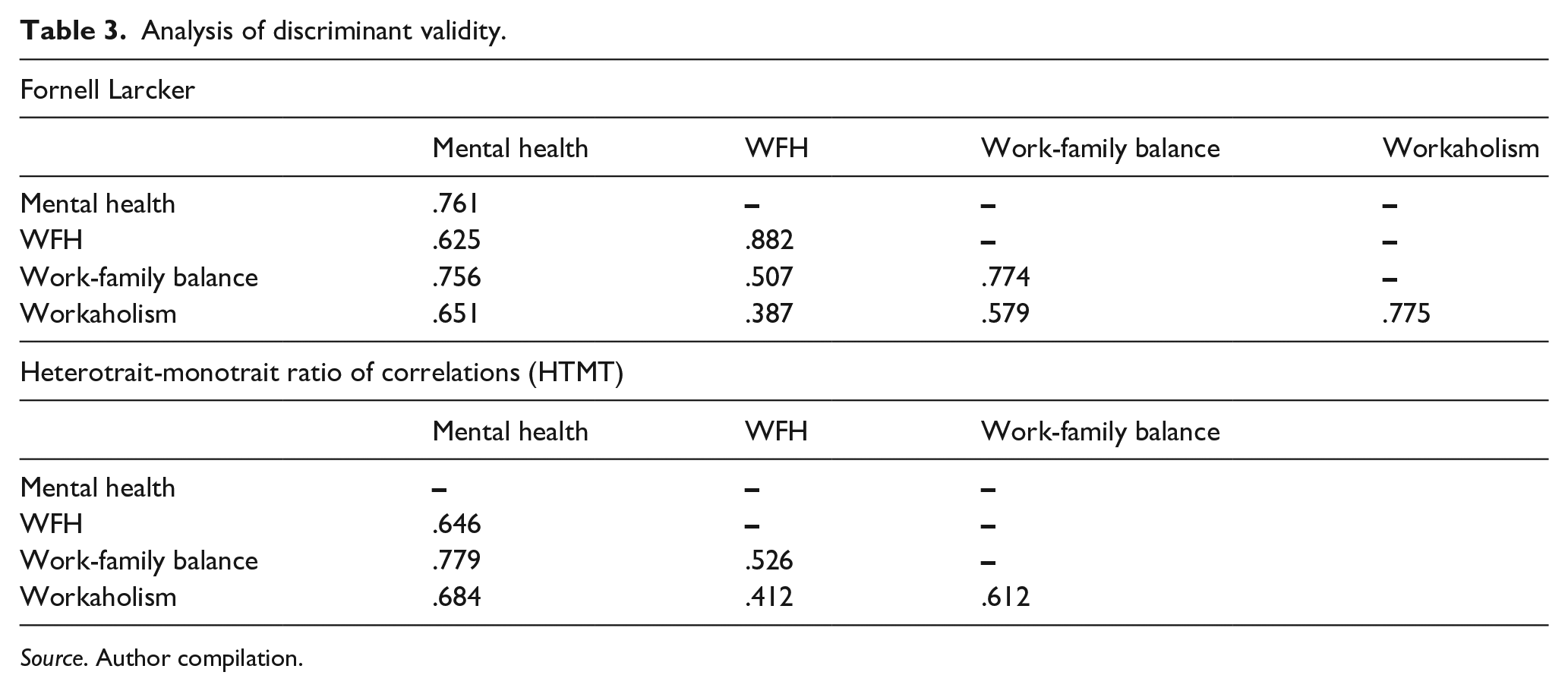
Source. Author compilation.
Two latent variables that are supposed to represent two different theoretical concepts must be statistically sufficiently dissimilar for them to have discriminant validity. To achieve discriminant validity, the heterotrait-monotrait ratio of correlations (HTMT) score must lie between certainty stretch values of −1 and 1 (Henseler et al., 2015). Table 3 reveals that discriminatory validity has been obtained, with all HTMT values falling between −1 and 1.
Structural model
Path analysis is employed using PLS-SEM to evaluate the relationships between the constructs in the structural model. The standardized regression coefficients, representing the estimated path coefficients, are examined for their absolute magnitude and sign. In Figure 2, all the expected linkages within the path model range from 0.269 to 0.431 and are found to be significant at a 5% level of significance, except for the effects of the two control variables, firm size and industry.
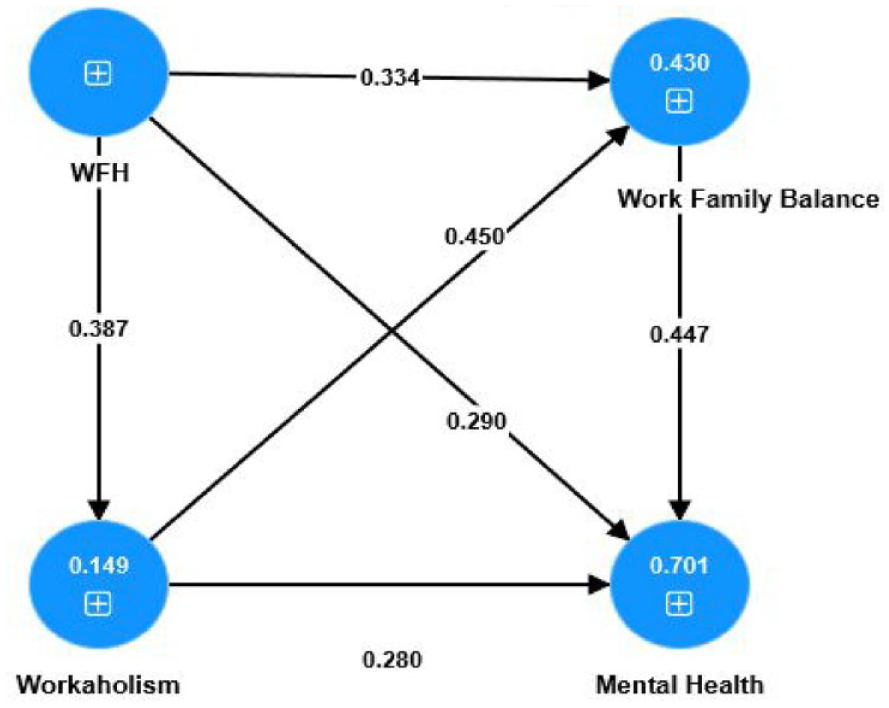
Results of the PLS-SEM model.
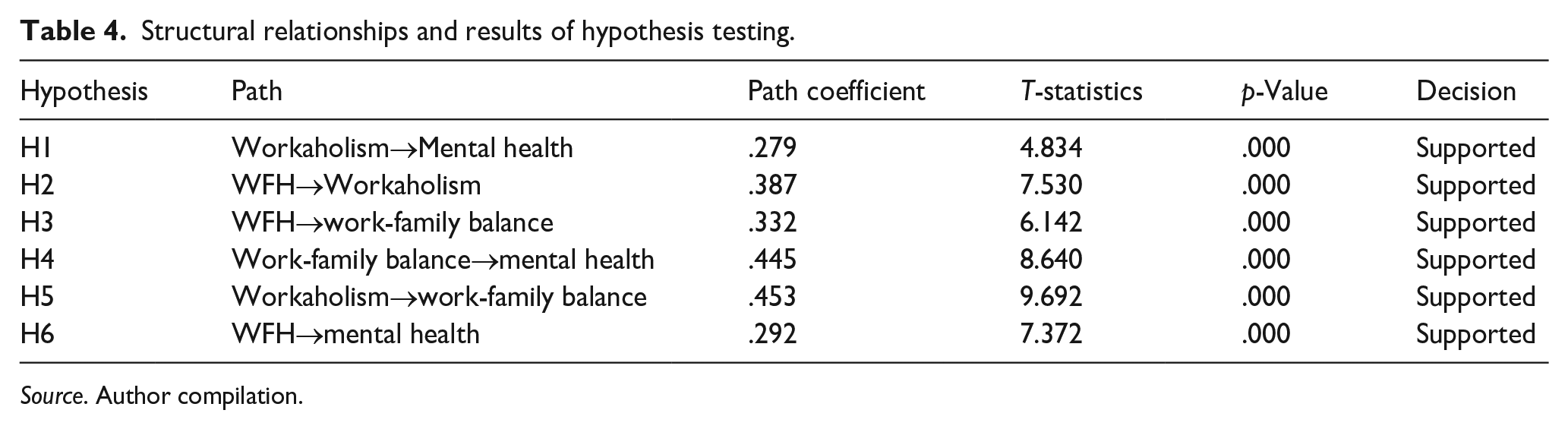
Table 4 and Figure 2 provide a summary of the findings. The findings support the study’s null hypothesis, according to which H1: Workaholism has a direct and detrimental impact on mental health, which is revealed in the result (β = .269, t = 6.999, p = .000). According to the results (β = .387, t = 7.530, p = .000) H2: Work from Home has a direct and negative effect on workaholism. H3: Work from home strongly predicts Work-Family Balance, according to the path analysis results (β = .332, t = 6.142, p = .000); H4 asserts that there is a negative impact of Work-Family Balance and Mental Health, and this relationship is shown in the result (β = .445, t = 8.640, p > .000). H5 shows how Workaholism and Work-Family Balance are associated and have a negative impact, and it is revealed through the results (β = .453, t = 9.692, p = .000). H6 examines the relationship between WFH and Mental Health, and the findings indicate that WFH negatively affects Mental Health (β = .292, t = 7.372, p = .000).
Structural relationships and results of hypothesis testing.
Source. Author compilation.
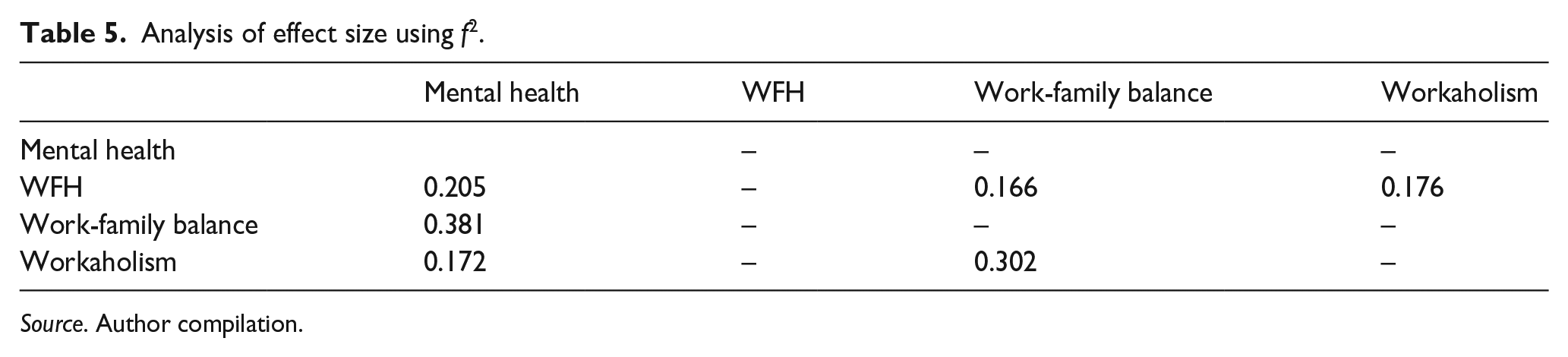
The effect size is calculated by using the f2, which indicates a weak, medium, or large impact size, respectively (⩾0.02 is small; ⩾0.15 is medium; and ⩾0.35 is large). The correlations hypothesized in this study’s f2 values range from 0.166 to 0.381 (medium to large; see Table 5).
Analysis of effect size using f2.
Source. Author compilation.
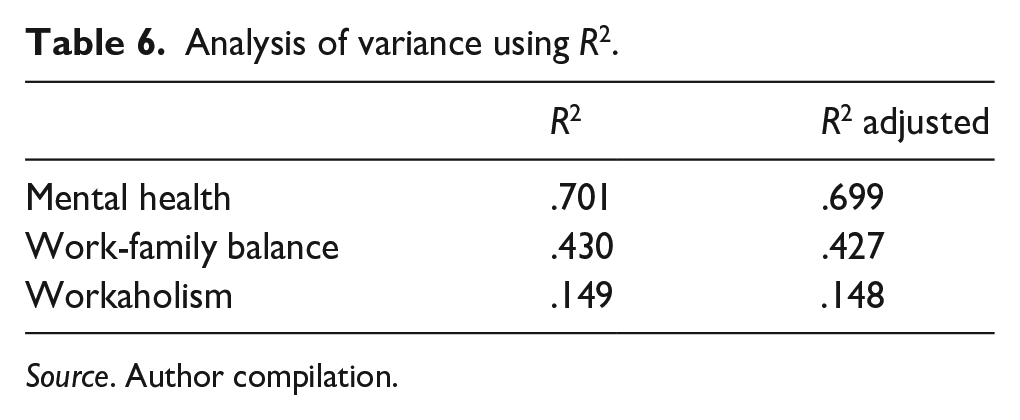
R2 statistics are utilized to indicate the extent to which the exogenous variable influences the variance of the endogenous variable. Following Cohen’s (1988) guidelines, the R2 values for the endogenous latent variables are interpreted as substantial if .26, moderate if .13, and weak if .02. In Table 6 of this study, the R2 values range from .701 to .149, indicating moderate to substantial effects.
Analysis of variance using R2.
Source. Author compilation.
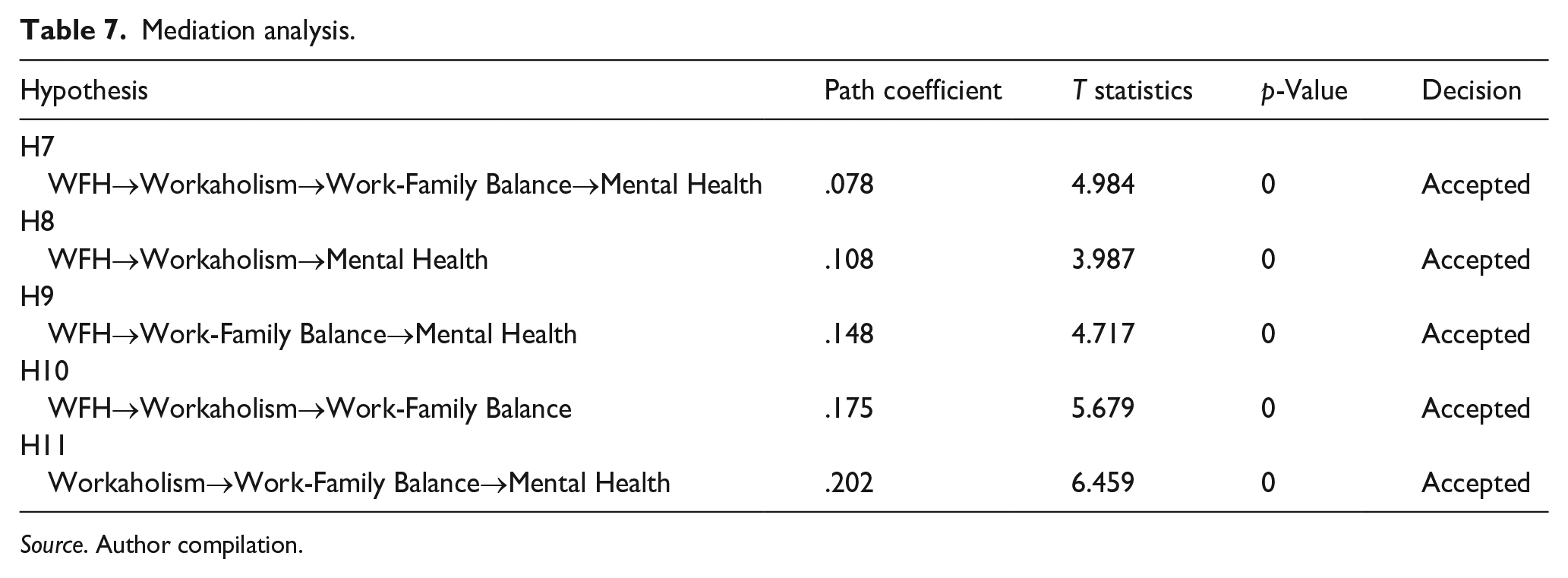
The mediating analysis is performed to assess the role of Workaholism and Work-family balance between work-from-home and mental health. The results, as depicted in Table 7, revealed the path analysis as H7: WFH → Workaholism → Work-Family Balance → Mental Health, which demonstrates the impact of WFH on Mental Health through Workaholism and Work-family balance, it has a significant indirect effect (β = .78, t = 4.984, p < .000) which represents a nested mediation (i.e. mediation within a mediation).
Mediation analysis.
Source. Author compilation.
H8: WFH has a significant indirect effect on Mental Health (β = .108, t = 3.987, p < .000); results indicate that workaholism mediates the relationship between WFH and Mental Health. H9: The relationship between WFH and Mental Health through work-family balance is analyzed, and results show a significant indirect effect (β = .148, t = 4.717, p < .000). H10: The indirect effect path coefficient of the relationship between WFH and Work-Family Balance through Workaholism is also significant (β = .175, t = 5.679, p < .000). H11: Indirect effect between Workaholism and Mental Health through work-family balance is found significant and concluded that work-family balance mediates between workaholism and mental health (β = .202, t = 6.459, p < .000). The result of the analysis concludes that these mediation models suggest that the relationship between WFH and Mental Health was indirect and fully mediated by Workaholism and Work-Family Balance.
Discussion
This discussion will offer evidence for the conclusions drawn from the literature review as a finding summary. Previous investigations have supported the conclusions of this study that workaholism significantly impacts both mental health and work-family balance. Quinones and Griffiths (2015) concluded that workaholism poses a risk to the public’s health and may have a negative impact on employees’ mental health. According to McMillan and O’Driscoll (2004), people who are chronically stressed out are more prone to suffer from conditions like coronary heart disease. Spence & Robbins also demonstrated that workaholics frequently report other physical and mental health difficulties. According to Spence et al. (2010), a person who suffers from workaholic syndrome would be sad, their life would be imbalanced, and they would also report less overall enjoyment and life satisfaction. Additionally, they would be more anxious, idealistic, and prone to health complaints (Spence & Robbins, 2010).
The study discovered that Work from Home directly affects workaholism. Work from home has the potential to exacerbate the murky distinctions between our personal and professional lives by pushing us to devote unsustainable and unhealthy amounts of time and energy to our jobs. According to Burke and McAteer, it has been assumed that technological advancements and flexible work arrangements have increased workloads and responsibilities, leading to an increase in the number of hours worked (Burke & McAteer, 2006).
Additionally, work-from-home arrangements were found to have an impact on mental health. This result was supported by previous studies. Work from home affects one’s mental health; when people spend more time at home, they generally feel more anxious and unhappier, which causes changes in routines and eating habits (di Renzo, Gualtieri, Cinelli, et al., 2020; di Renzo, Gualtieri, Pivari, et al., 2020). The effects on one’s physical and mental health result in increased stress that comes with work from home (Mazza et al., 2020; Ricci et al., 2020). Work from home also impacts work-family balance because individuals accustomed to established working hours find it challenging to manage work and personal commitments. It might be challenging to draw boundaries between work and personal obligations to achieve a work-family balance condition, particularly in the pandemic situation with its numerous limitation rules.
Apart from assessing the direct relationship between the variables, mediation analysis is conducted to examine indirect relationships. The results show a total mediation effect between work-from-home (WFH) and mental health through the mediating factors of workaholism and work-family balance. These findings not only confirm previous research but also highlight a negative relationship between WFH and mental health, which is influenced by the mediating roles of workaholism and work-family balance (Robinson, 1999; Schaufeli et al., 2008). In their study, Ayar et al. (2022) emphasized the significant impact on employees’ lives and behaviors when work-life balance is compromised. The health of employees has been adversely affected by various factors, including inconsistent working hours, shift work, role conflict, inadequate remuneration, lack of occupational safety, job ambiguity, excessive workload, and physical aspects related to the work environment (Ayar et al., 2022). Stress is brought on by an imbalance between work and family life that results from an excessive workload or high expectations at work. This has a detrimental influence on the quality of work and family life as well as on the well-being of the individual (Efeoğlu & Özgen, 2006).
Numerous scientific studies have been published in the literature to support the idea that people who work such long hours have an increased risk of developing depression, burnout syndrome, and myocardial infarction (Aronsson et al., 2017). As a result, it is believed that changing working conditions can offer a solution for preserving and protecting employees’ physical and psychological well-being. Since our study is the first to look into the impacts of work from home, work-life balance, and the extent of workaholism on academicians’ mental health, it will significantly contribute to the literature.
Implications
This research suggests that work-from-home has a detrimental impact on mental health due to excessive workload, distraction at home, noisy environment, house chores, and not having a good working environment which may result in creating a negative environment in the work and family and also resulting to increased levels of stress and poor health. In case such an environment persists, it may change the behavior of the academicians without the realization and directly or indirectly affect their performance. Academicians will avoid taking new initiatives that may result in less innovation in teaching pedagogy which will impact the development of future talent. Our new education policy focuses on academic and industry integration, but the stress and lack of well-being due to work-from-home may not produce the required results in terms of solutions for industry problems and providing future direction.
Work from home in the digital workplace might promote flexibility that unleashes people’s creativity, provided that work-life balance strategies are stretched and successfully implemented by employees with organizational support. Organizations should prioritize composite-level treatments at all levels of higher education to increase employee satisfaction, provide a positive work environment, and enhance mental health. Implementing a mental health program in organizations may play a significant role in increasing productivity and the mental well-being of employees.
To address the nation’s mental health challenges, studies should integrate mental health into primary healthcare, deliver high-quality care, and improve access to care at the societal level, and also, there must be mental health legislation. Effective preventative and therapeutic interventions for mental disorders within the healthcare system should be promoted through mental health policies and programs. Having access to mental healthcare in the community results in improved physical and mental health as well as a good quality of life.
Limitations and future research directions
The data was collected from private and public universities in the Delhi NCR region of India; which limits the coverage of the study to North India only. Future research should expand the scope of their study which may benefit from comparisons between higher education institutions from different countries. Qualitative research could be carried out to corroborate further the study’s findings to gain more insight into each factor. Other sectors that have embraced work-from-home policies outside education include banking and financial services (BFSI), information technology (IT), healthcare, etc. Future studies may examine these industries to see how they affect productivity and the environment. Experimental research may be able to provide a deeper understanding of the phenomenon and its implications on higher education institutions. Future research may also examine how work-from-home environments impact student growth and learning.