
Abstract
Background:
Healthcare workers (HCW) are at high risk to develop mental health problems during the COVID-19 pandemic because of additional work load, perceived stress, and exposure to patients with COVID-19. Currently, there are few studies on change over time in the prevalence of depressive symptoms during pandemic start among HCW. Thus, the aims of the current study were to examine whether depressive symptoms increased during the pandemic and were associated with perceived stress and own COVID-19 infection and workplace exposure to virus-infected patients.
Methods:
The cohort study used longitudinal data from HCW collected monthly (July 2020 till December 2020) during the first year of the pandemic before vaccination became available. The sample of n = 166 was drawn from a German hospital and included medical (e.g. nurses, therapists, and physicians) and administrative staff. Using multilevel models, we analyzed the change in depressive symptoms [assessed with General Depression Scale (GDS), a validated German version of the Center for Epidemiological Studies Depression Scale (CES-D)] and its association with perceived stress across the study period. Laboratory-confirmed own infection was tested as a potential moderator in this context. Subscales of the GDS were used to examine change over time of depressive symptom modalities (e.g. emotional, somatic, and social interactions (β, 95% confidence interval).
Results:
Depression scores increased significantly during the study period (β = .03, 95% CI [0.02, 0.05]). Perceived stress was associated with depressive symptoms (β = .12, 95% CI [0.10, 0.14]) but did not change over time. Exposure to COVID-19 infection was associated with a higher increase of depressive symptoms (β = .12, 95% CI [0.10, .14]). Somatic symptoms of depression increased among medical HCW with workplace exposure to COVID-19 (β = .25, 95% CI [0.13, 0.38]), but not in administrators (β = .03, 95% CI [−0.04, 0.11]).
Conclusion:
Research is needed to identify factors that promote the reduction of depressive symptoms in medical HCW with exposition to COVID-19 patients. Awareness of infection protection measures should be increased.
Introduction
Coronavirus 2019 disease (COVID-19) has spread internationally over the past 2 years.
Since 2020, there have been waves of COVID-19 (i.e. increase of new COVID-19 cases followed by decline), the causative agent of which is ‘severe acute respiratory syndrome coronavirus 2’ (SARS-CoV-2). By this account, people faced new virus variant strains (e.g. delta variant and omicron variant) with virus-specific severity and symptoms (El-Shabasy et al., 2022). The first two peaks of coronavirus incidence had high rates of virus-related mortality (El-Shabasy et al., 2022), indicating more severe disease courses compared with the third wave. The increase in confirmed COVID-19 cases in the general population resulted in an increasing number of individuals hospitalized for COVID-19 (e.g. United States: April 20th 2020: 50 per 100,000; October 24th 2020: 202 per 100,000; COVID-Net, 2020-2021). Public health responses to contain the spread of SARS-CoV-2 included self-isolation, quarantine, school closures, curfews, and full lockdowns (Kunzler et al., 2021), which may be associated with poor mental health in individuals, and in the general public (Galea et al., 2020; Kunzler et al., 2021; Moreno et al., 2020).
Mental health can be defined as ‘a dynamic state of internal equilibrium which enables individuals to use their abilities [. . .] to cope with adverse life events and function in social roles’ (Galderisi et al., 2015). Health care workers (HCW) may be particularly vulnerable to poor mental health during the pandemic due to their working conditions and work-related distress associated with the pandemic. To date, several studies have been published on the mental health of HCW during the COVID-19 pandemic (de Kock et al., 2021; de Sousa, Tavares, et al., 2021; Marvaldi et al., 2021; Muller et al., 2020; Spoorthy et al., 2020). Previous studies operationalized mental health among HCW along with COVID-19 predominantly by outcomes related to sleep disturbance, anxiety, and depression. For example, Marvaldi et al. (2021) indicated a burden of depression and depressive symptoms, with a pooled prevalence of 31 % among 68,030 HCW. de Kock et al. (2021) summarized the findings of studies with a prevalence of depressive symptoms ranging from 9 to 50 %.
To examine protective and risk determinants that may contribute to depressive symptoms among HCW, socio-ecological predictors are discussed in the literature (Hennein et al., 2021). Briefly, socio-ecological theories attempt to explain health in the context of multiple influences at different levels, each with resources and burdens for health (Bronfenbrenner, 1979). In case of the COVID-19 pandemic, previous studies suggest that determinants at the individual and the institutional levels may contribute to depressive symptoms among HCW. For example, at an individual level young age, female sex and an own COVID-19 infection are associated with depressive symptoms (de Kock et al., 2021; Magnúsdóttir et al., 2022; Mazza et al., 2020). de Kock et al. (2021) found that medical HCW (e.g. physicians and nurses) have a higher burden of depressive symptoms than nonmedical HCW (institutional level). In addition, HCW who have job-related exposure to virus-infected patients are thought to be at risk for mental health burdens, due to their workload, inadequate personal protective equipment, or decisions to triage COVID-19 patients (de Kock et al., 2021; Giang et al., 2020; Lu et al., 2020; Moreno et al., 2020; Nicolaou et al., 2021; Zhang et al., 2020). As such, institutional organization may contribute to concerns about own infection (Cai et al., 2020) and psychological distress at an individual level (Muller et al., 2020) that, in turn, contribute to depressive symptoms (de Sousa, Vargas, et al., 2021).
Mental health impairment in HCW is widely recognized as an important public health and health care challenge in the pandemic, as it is associated with both immediate and long-term consequences in individuals and for health care. For example, poor mental health contribute to sick absence from work (Spoorthy et al., 2020), medical errors and turnover rates (Marvaldi et al., 2021), as well as to severity of an acute own COVID-19 infection (Magnúsdóttir et al., 2022; Xie et al., 2022) with elevated levels of mental sequelae (Zeng et al., 2022). Promoting health of HCW is considered critical in pandemic management to health and to continuity of healthcare provision (Adams & Walls, 2020; Sahu et al., 2020; World Health Organisation [WHO], 2020, 2022).
The current literature is insufficient to comprehensively assess the impact of the pandemic on depressive symptoms in HCW and associated determinants for several reasons. First, recent findings on the prevalence of depressive symptoms in HCW are contradictory (de Kock et al., 2021; Marvaldi et al., 2021), which may depend on the operationalization of the outcome, the sample characteristics, and/or measurement instruments. Second, existing studies on depressive symptoms at the beginning of the pandemic among HCW contain few longitudinal data of outcomes or determinants (Jordan et al., 2023). Third, determinants or moderating factors of depressive symptoms over time that account for actual workplace exposure to COVID-19 were not examined.
The aim of the current study was to evaluate a change in the prevalence of depressive symptoms in HCW during the pandemic. According to the ecological theory mentioned above, perceived stress and healthcare workers’ own infection status (individual level), as well as workplace exposure to virus-infected patients (institutional level) were considered to explore the following research questions:
RQ1: Was there a change in depressive symptoms among HCW during the first wave of the COVID-19 pandemic, and was this change associated with perceived stress?
RQ2: Is change in depressive symptoms moderated by HCW’s own COVID-19 infection and/or workplace exposure to COVID-19 patients?
RQ3: Do depressive symptom modalities differ by workplace exposure to COVID-19 patients?
Methods
Data from a prospective cohort study
We used data from a prospective cohort study conducted in a standard care hospital at the primary healthcare level in the German federal state of Brandenburg. The aim of this study was to examine (i) the seroprevalence of antibodies against SARS-CoV-2 among HCW and (ii) self-reported exposure to COVID-19 patients at the job, as well as (iii) subjective physical and mental health. For this purpose, we recruited n = 166 participants from different hospital wards (i.e. emergency department, intensive care unit, cardiology, geriatrics, pediatrics, laboratory, radiology, and administration). To avoid possible selection bias, all persons currently working in the hospital wards concerned were to be recruited. The wards were selected according to suspected exposure to COVID-19 patients. This strategy made it possible to include the majority of eligible staff in the sample, who were predominantly female and on average 45 years old. This is consistent with German hospitals 2021 (about 80% female; age <34 years (35.2%), >35 to 44 years (20.8%), >45 to 54 years (21.7%), >55 years (22.4%; Fuchs & Weyh, 2023; Wasem & Blase, 2023)). Blood samples for laboratory analyses and questionnaires were collected monthly from July 2020 to December 2020. Thus, the data reflected the first two peaks of coronavirus incidence in the basic population in Brandenburg, when licensed vaccines were not yet available and the ‘sense of vulnerability’ was increasing among people, in part due to rising mortality rates (El-Shabasy et al., 2022).
Further study information (e.g. participation rates) and results of serological analysis were previously published (Hoffmann et al., 2021). Our study was ethically approved according to German ethical guidelines and informed consent was obtained by participants.
Measures
Main dependent variable: Repeatedly measured mean continuous depression scores (GDS mean scores)
Our main outcome of interest was self-reported mental health, operationalized by depressive symptoms. We administered the validated General Depression Scale (GDS, reliability (Cronbach’s alpha) = .89–.92, convergent validity e.g. with Becks inventory for measuring depression = .88 (Beck et al., 1961; Hautzinger et al., 2012; Shafer, 2006), which is the German version of the ‘Center for Epidemiological Studies Depression Scale’ (Carleton et al., 2013; Radloff, 1977). The GDS comprises 20 items of self-descriptive statements of oneself, each in relation to the last week and each on a 4-point scale (0: less than 1 day, 1: 1–2 days, 2: 3–4 days, and 3: 5–7 days). GDS mean scores were calculated for all participants with three or fewer missing items at each survey timepoint, in line with previous studies (Kleih et al., 2022). Higher mean scores indicated more depressive symptoms, with a range of values of 0.00 to 2.30 in this study (GDS range of values: 0.00–3.00).
Second dependent variable: Repeatedly measured continuous scores of GDS subscales
Depressive symptoms manifest in different modalities (e.g. emotional, somatic, and interactional). In order to evaluate temporal effects, we computed five subscales based on all GDS items (n = 20) that have been previously confirmed in factor analytic studies (Hautzinger et al., 2012):
(1) Emotional symptoms: item numbers 1, 3, 6, 10, 12, 14, and 18 (n = 7)
(2) Motivation symptoms: item numbers 7 and 20 (n = 2)
(3) Cognitive symptoms: item numbers 4, 5, 8, 9, and 16 (n = 5)
(4) Somatic symptoms: item numbers 2, 11, and 17 (n = 3)
(5) Interactional symptoms: item numbers 13, 15, and 19 (n = 3)
Predictor variables (independent variables)
a. Linear time
The variable time specified whether the depression scores were collected at baseline (July 2020), ‘Time 1’ (August 2020), ‘Time 2’ (September 2020), ‘Time 3’ (October 2020), ‘Time 4’ (November 2020), or at ‘Time 5’ (December 2020). Since we collected data at more than three timepoints, we tested time as a linear predictor variable (Twisk, 2006).
b. Previous own infection among HCW
A previous own infection with SARS-CoV-2 among HCW was confirmed by laboratory analysis with serological testing of total Ig antibodies against SARS-CoV-2. Briefly, a nucleocapsid antigen from a SARS-CoV-2 assay was applied, resulting in a cut-off index on a continuous scale (99.5% sensitivity and 99.8% specificity). Further information on applied laboratory analytics were previously published (Hoffmann et al., 2021).
We converted the values to a dichotomous variable, with a cut-off index (COI) ⩾1.00 interpreted as positive for SARS-CoV-2 antibodies (i.e. confirmed own infection).
c. Perceived stress among HCW
We assessed self-rated stress among HCW using the 4-item version of the validated Perceived Stress Scale (Cohen et al., 1983; PSS). This involves a critical appraisal of one’s life in the last month according to the extent of and control over stressful situations, with each item rated on a 5-point scale (0 – never, 1 – almost never, 2 – sometimes, 3 – fairly often, and 4 – very often). The scores of the individual items were summed, yielding a range of values from 0 to 16, with higher scores indicating a higher amount of perceived stress.
We tested a correlation of PSS4 sum scores with symptoms of depression for each survey timepoint. Furthermore, we examined a linear time trend in PSS4 sum scores, and they neither increase nor decrease (i.e. remain stable) over time among participants. The Supplemental Material presents corresponding data (Supplemental Tables 4 and 5). Therefore, for analysis, mean stress scores were computed using PSS4 for participants for whom the complete scale items were collected at a minimum of 3 timepoints. Accordingly, this variable (stress) reflects an average of PSS scores across the entire study period.
Covariates
Sociodemographic data, including information on sex [female/male] and age [year of birth], was collected using a questionnaire that participants completed at baseline.
We clustered participants into four groups according to which hospital ward they were working at: 1 – emergency department; intensive care unit; 2 – cardiology, geriatrics, pediatrics; 3 – laboratory, radiology; and 4 – administration (Hoffmann et al., 2021). We then built a dichotomous variable ‘group’ [administrative/medical staff] indicating exposure to workplace contact with COVID-19 patients, presuming that medical staff have more frequent contact than administrative staff.
Statistical analyses
All analyses were performed using R (version 4.0.3 2022). All tests were considered significant at p < .05 and were stratified by ‘group’ (i.e. indicating varying degrees of workplace exposure to COVID-19 patients).
In order to perform a ‘complete case analysis’ (Lewin et al., 2018), we created an analytic dataset with missing values omitted for each variable used (i.e. scores of depressive symptoms at all timepoints, age, sex, COI value, and average PSS scores). Differences between medical and administrative staff in workplace exposure to COVID-19 patients were tested using Fisher’s exact test (Kim, 2017).
Step 1: Confirmation of a linear time trend in depressive symptoms and a predictive value of perceived stress
In the first step, we attempted to confirm a linear time trend in the change in depressive symptoms. We ran three (M0–M2) linear multilevel models with repeatedly measured mean depression scores as the dependent variable by using lme() function in R (Laird & Ware, 1982; Pinheiro et al., 2022). In these models, we included time as a linear predictor by using it as a fixed effect, which specifies whether mean depression scores were measured at baseline (July 2020), ‘Time 1’ (August 2020), ‘Time 2’ (September 2020), ‘Time 3’ (October 2020), ‘Time 4’ (November 2020), or at ‘Time 5’ (December 2020). To account for differences in the dependent variable both within level (level 1: data at different timepoints) and between levels (level 2: individuals), we used ‘subject’ as a random effect. The variable ‘subject’ indicated whether data belong to the same person. Since we analyzed repeatedly measured data, we accounted for residual autocorrelation of the data between survey timepoints by extending the models through the introduction of a covariance structure. We used the predefined first-order autoregressive structure (AR1) as recommended by Horváth et al. (2014) for linear time series data analysis.
We used the following equation to predict repeatedly measured scores of depressive symptoms by time and stress, while adjusting for age and sex:

Using ANOVA, we investigated differences in the model fit by comparison of the Akaike information criterion (AIC value; Wagenmakers & Farrell, 2004)):
- Model M0: random intercept (level 2: ‘subject’)
- Model M1: random intercept, with time’ and stress as predictors (level 1: time, stress, level 2: ‘subject’)
- Model M2: random intercept with first-order autoregressive covariance structure (AR1), with time and stress as predictors (level 1: time, stress, level 2: ‘subject’)
Testing for multicollinearity (Lüdecke et al., 2021): We found no evidence for significant multicollinearity with variance inflation factors (VIF) below 1.07 for all predictors and covariates (time, age, sex, stress). Furthermore, for all variables the average VIF was <1.1 and tolerance statistics were >.93 (Bowerman, 2000).
Testing for heterogeneity biased estimates and inferential statistics (Bell & Jones, 2015): Using the function ‘check_heterogeneity_bias’ (performance package; (Lüdecke et al., 2021)), we found no evidence for significant correlation of age, sex, and stress, each with the random effect (‘subject’).
Step 2: Differences in the linear time trend in depressive symptoms by own infection and/or by workplace exposure to COVID-19 patients?
As described above, theories about the pathways through which mental health may be affected suggest that a previously confirmed viral infection may contribute to poorer outcomes (Mazza et al., 2020). Thus, we evaluated whether a previously confirmed own virus infection predicts mean depression scores over time. We extended Model M2 with an interaction term time × infection for Model M3, where infection indicates whether a SARS-CoV-2 infection could be newly confirmed at a survey timepoint among HCW.
We repeated Model M2 and Model M3 stratified by workplace exposure to COVID-19 patients. Significant interactions are graphically depicted (see Figure 1).
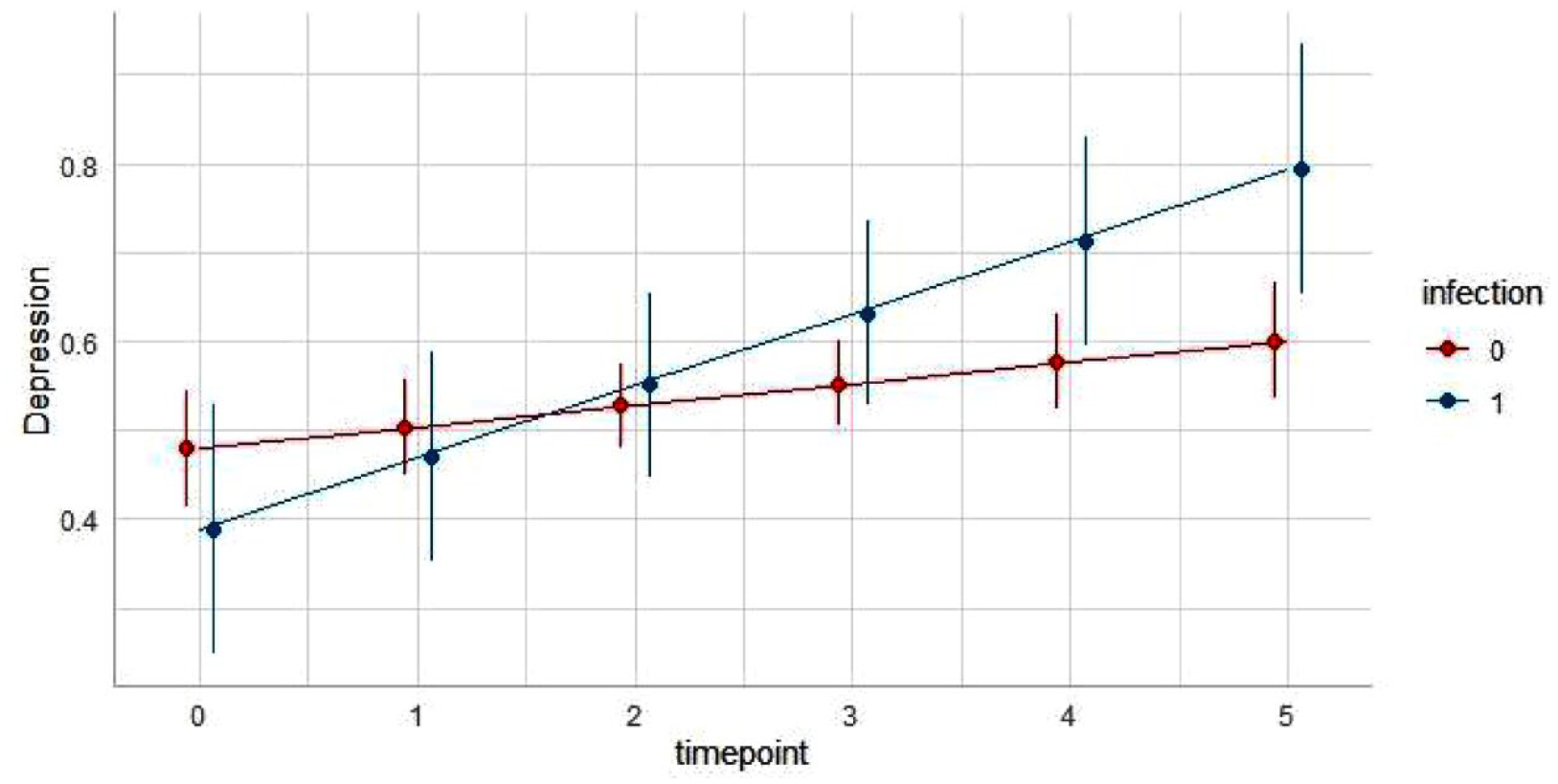
Predicted values of depressive symptoms by laboratory-confirmed infection status among overall sample (infection 0 = no, 1 = yes).
Step 3: Differences in the linear time trend in depressive modalities by presumed workplace exposure to COVID-19 patients
Recent literature suggests mental health burden (e.g. anxiety, depression, sleep problems, and distress; Muller et al., 2020) varies by workplace exposure to COVID-19 patients (Muller et al., 2020). To evaluate a temporal change in modalities, we reran the above Model M2, with fitting each of the GDS subscales as dependent variables to the linear multilevel models.
Results
Of n = 166 healthcare workers recruited, a total of n = 91 had complete data on mean depression scores and own infection status at each survey timepoint as well as baseline information (i.e. age, sex, and hospital ward group). In addition, these HCW had complete PSS data at a minimum of three survey timepoints.
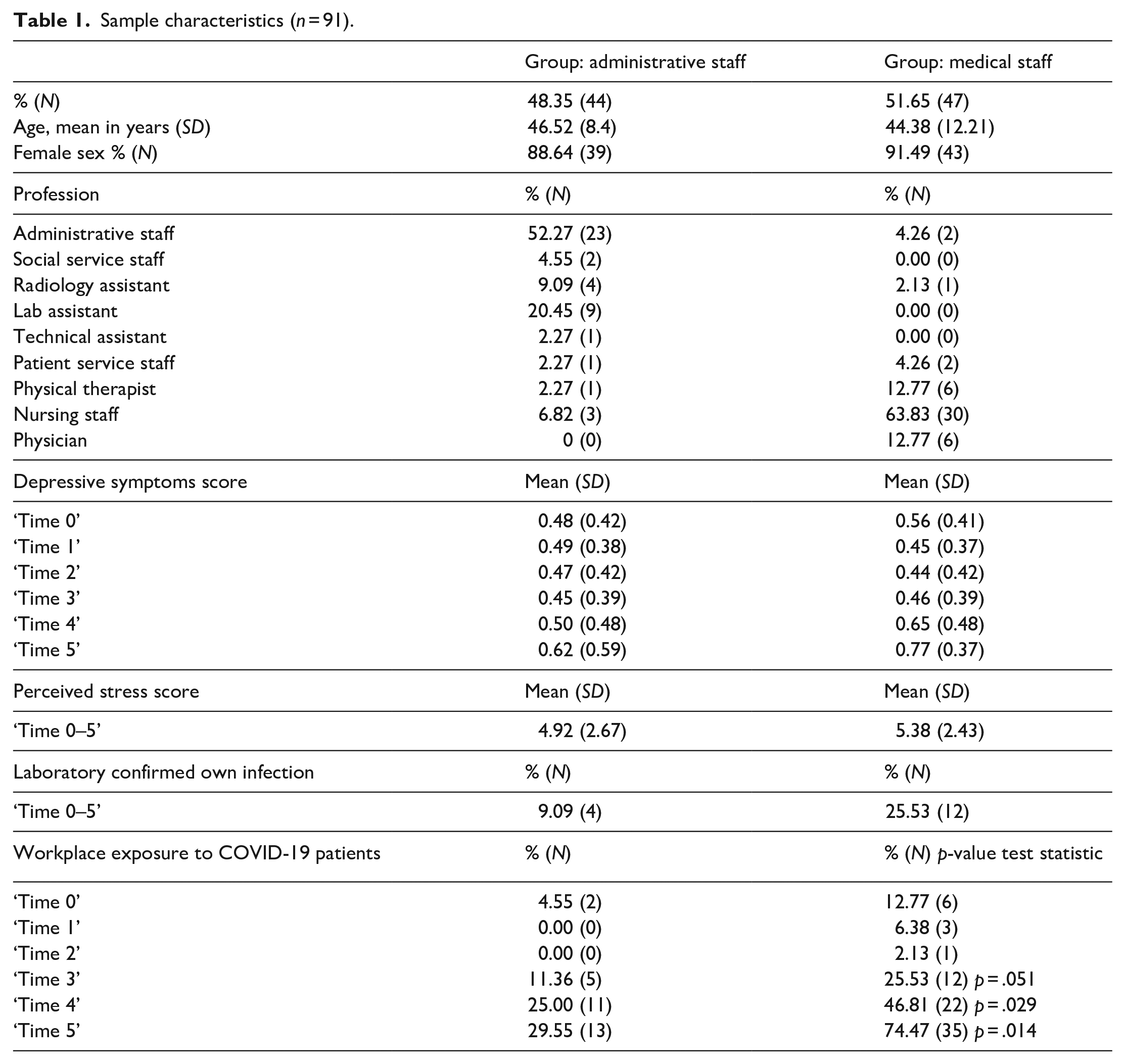
Sample characteristics of these n = 91 participants are displayed in Table 1. Administrative staff mainly reflect individuals with administrative and laboratory jobs (about 72%), while those for medical staff refer to nurses, physicians, and physical therapists (about 90%). While among medical HCW, 74.47% (n = 35) reported workplace exposure to COVID-19 patients at time 5, this proportion was 29.55% (n = 13) among administrative staff. The more frequent exposure among medical HCW was statistically significant (p = .014).
Sample characteristics (n = 91).
Step 1: Confirmation of a predictive value of both time and stress on depressive symptoms
Model M0 in Table 2 shows 62% explained variance (ICC) by ‘subject’, indicating significant between-level variation requiring multilevel analyses.
Linear time and stress as predictors of mean depression scores among healthcare workers.
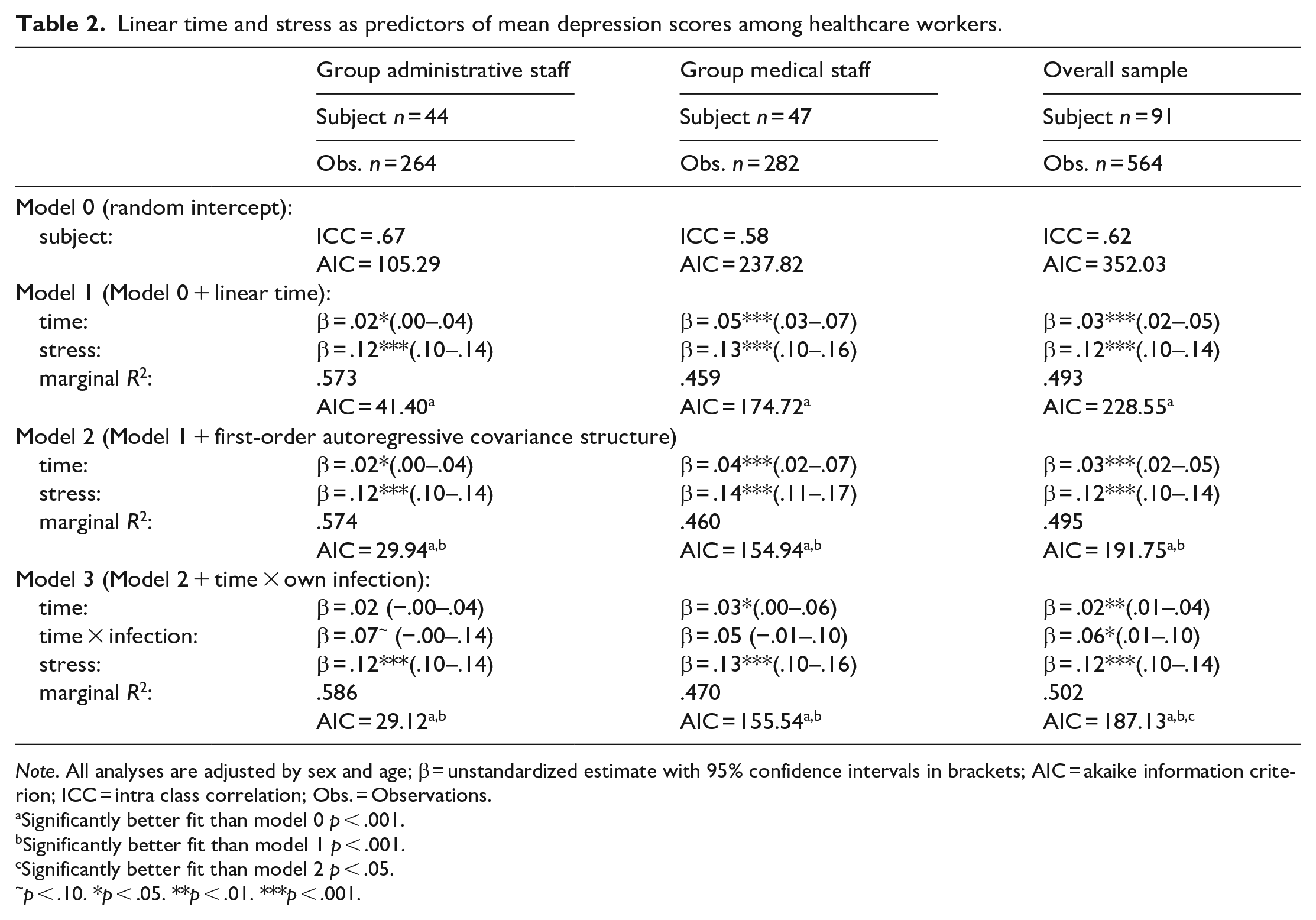
Note. All analyses are adjusted by sex and age; β = unstandardized estimate with 95% confidence intervals in brackets; AIC = akaike information criterion; ICC = intra class correlation; Obs. = Observations.
Significantly better fit than model 0 p < .001.
Significantly better fit than model 1 p < .001.
Significantly better fit than model 2 p < .05.
p < .10. *p < .05. **p < .01. ***p < .001.
Time was significantly associated with mean depression scores in Model M1. Similarly, model fit improved significantly compared to Model M0. Adding a first-order autoregressive covariance structure to Model M1 resulted in a further significant improvement of Model M2. The prediction of mean depression scores by time (β = .03) was significant (95% CI [0.02, 0.05]), indicating an increase of depressive symptoms over time in the overall sample. In Model M2, stress significantly predicted repeatedly measured depressive symptoms (β = .12, 95% CI [0.10, 0.14]).
Step 2: Differences in the linear time trend in repeatedly measured depressive symptoms by own COVID-19 infection among HCW and/or by workplace exposure to COVID-19 patients
Model M3 showed a significant interaction with a laboratory-confirmed own infection among overall sample and, likewise, had a better model fit than Model M0, Model M1, and Model M2 (see Table 2).
Figure 1 depicts the significant interaction between a linear time predictor in mean depression scores and an infection status among overall sample. Among individuals with confirmed infection status, there was a stronger positive relationship between time and depressive symptom scores.
When stratified by workplace exposure to COVID-19 patients, Model M2 maintained a predictive value of time for depressive symptoms among medical HCW (β = .04, 95% CI [0.02, 0.07]), and a marginal effect among administration staff (β = .02, 95% CI [0.00, 0.04]). Similarly, model fit of Model M2 improved compared to Model M0 and Model M1 for both groups. Additionally, Model M2 retained a predictive value of stress on depressive symptoms among medical HCW (β = .14, 95% CI [0.11, 0.17) and administration staff (β = .12, 95% CI [0.10, 0.14]). Model M3 did not maintain an interaction effect among health care worker groups. Accordingly, Model M3 did not show improved model fit in the analysis of stratified sample data.
Step 3: Differences in the linear time trend in repeatedly measured modalities by workplace exposure to COVID-19 patients
Of the analysis sample (n = 91), 71 participants answered all items in each GDS subscale at each survey timepoint, which was considered valid for computing the subscale scores.
Table 3 shows a replication of Model M2 with repeatedly measured sums in the GDS subscales as dependent variables. A predictive value of time maintained for emotional symptoms among both administrative (β = .31, 95% CI [0.14, 0.49]) and medical HCW (β = .42, 95% CI [0.14, 0.70]). Somatic symptoms increased significantly over time among medical HCW (β = .25, 95% CI [0.13, 0.38]), but not among administrative staff (β = .03, 95% CI [−0.04, 0.11]). Model M2 retained a marginal effect of time for motivational (β = .06, 95% CI [0.00, 0.13]) and interactional symptoms (β = .10, 95% CI [0.00, 0.12]) among administrative staff, but not among medical HCW.
Linear time and stress as predictors of depressive modalities among healthcare workers by workplace exposure to COVID-19 patients.
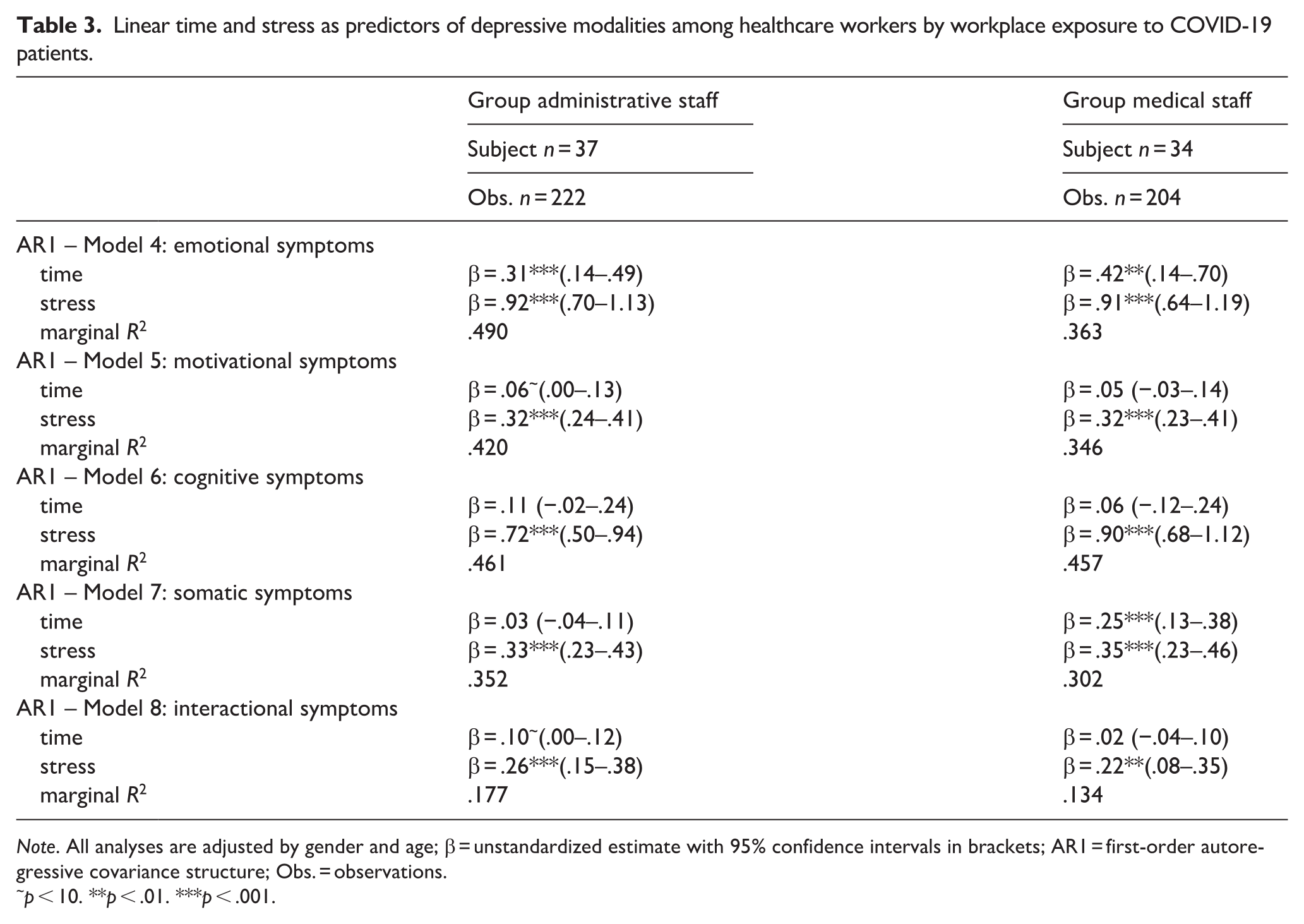
Note. All analyses are adjusted by gender and age; β = unstandardized estimate with 95% confidence intervals in brackets; AR1 = first-order autoregressive covariance structure; Obs. = observations.
p < 10. **p < .01. ***p < .001.
Perceived stress predicted the scores for each repeatedly measured depressive symptom modality and in each HCW group.
Discussion
The present study examined longitudinal changes in depressive symptoms and the predictive value of perceived stress among healthcare workers in 2020, taking into account both workplace exposure to COVID-19 patients and laboratory-confirmed infection status. Analyses were based on data collected at a general primary care hospital during the first two peaks of coronavirus incidence in the population in the German federal state of Brandenburg, when no licensed vaccine was available yet.
RQ1: Temporal increase in mean values of depressive symptoms and predictive value of perceived stress during the first wave of the COVID-19 pandemic
Multilevel models showed a temporal increase in depressive symptoms among healthcare workers. These results are in line with previous findings of the population-based ‘Gesundheit in Deutschland aktuell’ study (GEDA for short; engl. ‘Health in Germany up-to-date study’) conducted in 2014/2015 by the Robert Koch-Institute on the prevalence of depressive symptoms in the general population of 10.1 %, even beyond clinical diagnoses (Bretschneider et al., 2017). The temporal trend in the increase of depressive symptoms is partially consistent with studies showing an increase in the prevalence of self-reported clinical diagnoses of depression according to the past 12 months in recent years (Thom et al., 2017). However, these findings are comparable to a limited extent as Thom et al. (2017) did refer to a different operationalization of depressiveness (‘ever medically diagnosed’ vs. here: GDS, continuous measure of depressive symptomatology). By contrast, Damerow et al. (2022) confirmed a temporal decrease of depressive symptoms in the period from April to August 2020 in the general German population based on GEDA data, which have been collected in cross-section in 2019/2020. The authors argue that the COVID-19 pandemic did not contribute to an increase in depressive symptoms in 2020 (Damerow et al., 2022). However, comparability of results is limited due to both the study population (here: HCW) and the data (here: longitudinal).
Multilevel models showed an additional predictive value of perceived stress on changes in depressive symptoms, an association that confirms findings from previous studies on stress and depression in HCW during the pandemic (Li et al., 2022) and that has been discussed in a recent narrative review (de Sousa, Vargas, et al., 2021).
RQ 2: Own infection exacerbates temporal increase in mean depressive symptoms, regardless of workplace exposure to COVID-19 patients
When stratified by workplace exposure to COVID-19 patients, time and stress additively predicted mean depression scores, but without significant differences between HCW groups. By analyzing the moderating effect of a previous infection, we found an additional interaction effect between time and infection in the overall sample, but not when stratified by workplace exposure to COVID-19 patients, suggesting a steaper increase in depression symptom scores over time among individuals who were infected with SARS-CoV-2 and those who were not infected. The recent study confirms previous findings on mental health burden in individuals with COVID-19. However, previous studies on the association between mental health and COVID-19 were mainly descriptive in nature or reflect retrospective case control or cohort study designs (de Kock et al., 2021; WHO, 2022). Briefly, poor mental health in individuals may both predispose them to severe COVID-19 disease (WHO, 2022) and be associated with mental health symptoms as a consequence of a COVID-19 diagnosis (Magnúsdóttir et al., 2022; Xie et al., 2022). Our findings based on longitudinal data extend previous findings by suggesting a directed association between infection and poor mental health (here: depressive symptoms). Hence, our findings support previous results of cross-sectional data analyses indicating COVID-19 to be associated with the onset of mental disorders (e.g. anxiety, depression, and stress) after an acute illness (Magnúsdóttir et al., 2022; Xie et al., 2022).
Our results support the following suggestions about mechanisms by which COVID-19 infections influence depression symptoms. First, previous studies pointed to psychological effects resulting from, among other things, social isolation due to one’s infection. For example, Pancani et al. (2021) found physical separation to be associated with depression. Second, studies pointed to inflammatory processes as a biological mechanism underlying the onset of depression (Mazza et al., 2020; Miller & Raison, 2016). In line with this, we found that scores for depressive symptoms were higher over time when an infection was previously confirmed. Consequently, risk for depression in the post-disease phase could be affected by infection-related demands on the immune system (Mazza et al., 2020; Miller & Raison, 2016).
RQ 3: Workplace exposure to COVID-19 patients affects temporal increase in somatic depressive symptoms
Multilevel models showed an increase in depressive symptom modalities according to workplace exposition to COVID-19 patients. In both HCW groups, emotional symptoms (i.e. feelings of worry, gloom, dejection, anxiety, loneliness, and sadness) increased over time. Studies of mental health determinants among HCW at the beginning of the pandemic suggest that they may be concerned about infecting themselves or their families with COVID-19 or about rising mortality rates (Cai et al., 2020; El-Shabasy et al., 2022) or they may increasingly experienced infections by their own or infections and deaths in relatives and acquaintances.
In particular, medical staff with increasing patient contact showed increasing scores for depression-related somatic symptoms (i.e. fatigue, sleep disturbance, and weepiness), whereas this was not the case for administrative staff. These findings are in line with evidence demonstrating associations between hospital working ward and mental health among HCW. For instance, Lai et al. (2020) found that HCW involved in the frontline diagnosis, treatment, and care of patients with COVID-19 are at higher risk of developing depression compared to administration staff. Sagherian et al. (2020) indicated that hospital nursing staff suffered from poor sleep and fatigue during the COVID-19 pandemic. Our findings revealed an additively predictive value of perceived stress on somatic and emotional symptoms. This finding points to individual and institutional determinants of depressive symptoms and, thus, supports the above ecological theory. For example, Sagherian et al. (2020) refered to an institutional level by pointing to decreased intershift recovery or avoiding breaks during healthcare provision in the first wave of the pandemic that, in turn, are associated with quality of sleep (Xiao et al., 2020) and perceived stress on an individual level (Spoorthy et al., 2020; Xiao et al., 2020).
Strength and limitations
To the best of our knowledge, this study is one of the first to use longitudinal data analysis to examine the change in depressive symptoms recorded repeatedly over a 6-month period at the beginning of the pandemic. Our main outcome was assessed using the GDS, a validated measure of depressive symptoms. In addition, previous infection with SARS-CoV-2 was confirmed by laboratory analysis and included in our analysis. A further strength of the study is that it was conducted during the early phase of the pandemic when vaccines were not yet available, thus findings are not confounded by vaccination status.
Our study has several limitations. First, due to item nonresponse across all survey timepoints, we were only able to include n = 564 observations from 91 participants. However, this subsample was similar in age and sex compared the original sample. Eight participants with an infection with SARS-CoV-2 dropped from the recruited sample due to missing data (Hoffmann et al., 2021). The current analysis is based on data collected at six time points in 2020 from HCW at a primary care hospital. Further research could consider longitudinal research on mental health among HCW in different healthcare settings (e.g. university hospitals, rehabilitation hospitals, or outpatient care) or at different points during the pandemic (de Kock et al., 2021). Finally, we were unable to include additional potential sources for psychological stress (e.g. social isolation; Brooks et al., 2020) due to missing responses in the questionnaires or a lack of variance in the data. Since recent findings suggested that socio-ecological factors are helpful to examine health among HCW (Hennein et al., 2021), such factors (e.g. team cohesion and hospital politics) should be considered in future longitudinal studies of HCW’s mental health.
Conclusion
In the present study, the prevalence of depressive symptoms in healthcare workers was found to increase between the first two incidences peaks of COVID-19 cases in 2020. Our study revealed that newly confirmed own infection contributed to the temporal increase of depressive symptoms among healthcare workers during the study period, regardless of the workplace exposition to COVID-19 patients. In addition, depression-related somatic symptoms increased over time among HCW that provided direct care to COVID-19 patients, but not among administrative staff. We conclude that job-related contact with COVID-19 and an own infection predict deterioration of mental health and related symptoms among HCW over time. Our findings could help to improve the mental health of HCW by emphasizing both the need for personal protective measures against infectious diseases and workplace health promotion in clinical settings. Further research is needed to identify protective factors that promote the reduction of depressive symptoms in medical HCW with exposition to COVID-19 patients, including stress-related determinants.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231196737 – Supplemental material for Did the prevalence of depressive symptoms change during the COVID-19 pandemic? A multilevel analysis on longitudinal data from healthcare workers
Supplemental material, sj-docx-1-isp-10.1177_00207640231196737 for Did the prevalence of depressive symptoms change during the COVID-19 pandemic? A multilevel analysis on longitudinal data from healthcare workers by Stephanie Hoffmann, Susanne Schulze, Antje Löffler, Juliane Becker, Frank Hufert, Heinz-Detlef Gremmels, Christine Holmberg, Michael A Rapp, Sonja Entringer and Jacob Spallek in International Journal of Social Psychiatry
Footnotes
Author contributions
Conceptualization: JS, SH, JB, FH, HDG, and SE; Data collection: JB and SH; Methodology: SH, JS, and SE; Data curation: SH and SS; Formal analysis: SH; Writing – original draft: SH; Writing – review and editing: SH, SE, SS, JB, JS, HDG, AL, CH, MR, and FH; Supervision: JS.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the Brandenburg University of Technology Cottbus-Senftenberg (EK2020-8) gave ethical approval for complete study. Written, informed consent for participation in this study was obtained from all participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.