
Abstract
Background:
At the beginning of the COVID-19 pandemic, concerns arose about a possible rise in alcohol consumption. Early surveys, however, more commonly pointed towards a decrease of alcohol use. But studies based on self-reports may underestimate alcohol use. They also depend on the population sampled. Because of border closures and gastronomy restrictions, countries with centralised alcohol sales provided a unique opportunity to study total domestic consumption during the pandemic without influence of private import or reliance on self-reports.
Aims:
We examined the correlation between alcohol sales and national COVID-19 restrictions in three such countries, Finland, Norway and Sweden.
Method:
We conducted this study as a mirror image study, comparing alcohol sales during the first 2 years of the COVID-19 pandemic with the two preceding years. We explored hours of daylight/season as potential confounders.
Results:
We found no relevant change in alcohol sales during the pandemic years for Finland or Sweden. For Norway, there was a level-change in sales, which could be explained by decreased imports. Sales followed a seasonal pattern. In all three countries, the initial pandemic increase in alcohol sales coincided with an underlying annually recurring seasonal variation.
Conclusions:
The COVID-19 pandemic had less of an impact on alcohol consumption in the three Nordic countries than could intuitively be expected. The increase of alcohol sales at the beginning of the COVID-19 pandemic coincided with a seasonal rise following a pre-pandemic pattern. Therefore, caution should be exercised with drawing conclusions from data with a short time perspective to avoid attribution bias.
Introduction
The COVID-19 pandemic brought fundamental changes and challenges to countries worldwide. As restrictions and lockdowns were widely implemented, concerns arose about the impact of these on public mental health and welfare (Werneke et al., 2022). Right from the beginning of the pandemic, concerns were voiced about an increase in alcohol consumption and alcohol-related harm (Ramalho, 2020). The impact of the pandemic on mental health in general and alcohol consumption in particular remains unclear. Two opposing theories exist regarding the impact of a crisis, such as the COVID-19 pandemic, on alcohol consumption. Consumption may either increase due to heightened levels of anxiety or decrease due to strained personal finances and fewer opportunities for social drinking (Leifman et al., 2022; Rehm et al., 2020). A simulation study from the US showed that if alcohol consumption was to increase during the pandemic, alcohol-related health costs could be expected to increase substantially during the following years (Barbosa et al., 2023). Studies based on cross-sectional surveys of self-reported use or sales data for the first few months or the first year of the pandemic have mostly suggested a decrease of alcohol use in the Nordic countries (Jääskeläinen et al., 2022; Kilian et al., 2021; Leifman et al., 2022; Mäkelä et al., 2021; Trolldal & Åström, 2021).
The currently available research on alcohol consumption focuses on the beginning of the pandemic. Less is known about how alcohol consumption developed during the full course of the pandemic. However, a longer time perspective is important. Direct adverse effects of the pandemic, such as COVID-19 related mortality and lockdowns, decrease over time. Indirect detrimental effects of the pandemic, such as economic fallout, increase over time. In Nordic countries that exert an alcohol monopoly, sales data are published quarterly. Due to border closures during the pandemic virtually eliminating private imports, and serving restrictions in the gastronomy sector, domestic sales data from countries with alcohol monopoly roughly represent total consumption. This presents a unique opportunity to study the effects of COVID-19 lockdown measures on alcohol consumption in such countries over a longer period.
Aim
We aimed at comparing alcohol consumption in relation to restriction measures in three Nordic countries, Norway, Sweden and Finland, during the first 2 years of the COVID-19 pandemic with the two previous, pre-pandemic, years. Specifically, we tested three hypotheses:
For all three countries alcohol retail sales (a) increased, (b) varied in relation to social distancing recommendations and (c) varied with national economic development.
Material and methods
Study design
We conducted a mirror-image study of the pandemic years 2020–2021 for Finland, Norway and Sweden using the two previous years as control (Figure 1). Using this mirror image design, we compared trends in alcohol sales as a proxy for alcohol consumption before and after the start of the COVID-19 pandemic.

Mirror-image study design.
Selection of countries
We included all Nordic countries that (a) exert an alcohol monopoly and (b) publish sales data in the public domain. Three Nordic countries, Finland, Norway and Sweden fulfilled these inclusion criteria (Figure 2). All three countries employ the practice of monopolised alcohol retail (alcohol monopoly) and publish the alcohol sales data publicly online. The other two Nordic countries, Iceland and Denmark including the Faroe Islands and Greenland, were excluded. The alcohol monopoly in Iceland does not provide raw sales data in the public domain. Denmark, including the autonomous island of Greenland, does not exert any alcohol monopoly. While alcohol monopoly is present locally in the Faroe Islands, data for 2021 was not published at the time of writing.
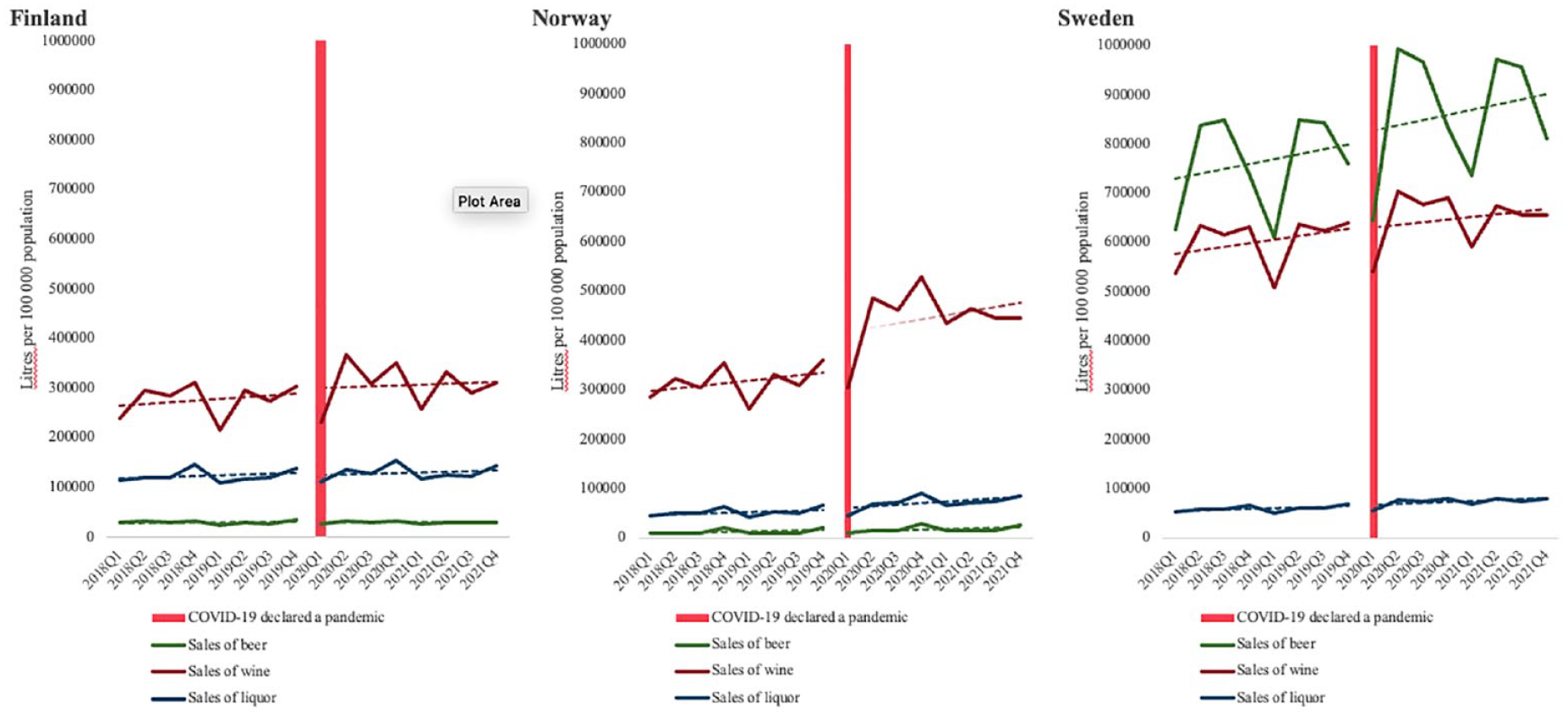
Alcohol sales per country, quarterly 2018–2021.
Data collation
Data for alcohol sales, COVID-19 restrictions, national economic development, hours of daylight, COVID-background data, social distancing measures concerning the gastronomy sector, and border closures, size of population, and – in the case of Sweden – public opinion was collated from relevant publicly available sources (Table 1).
Information sources from the public domain a .
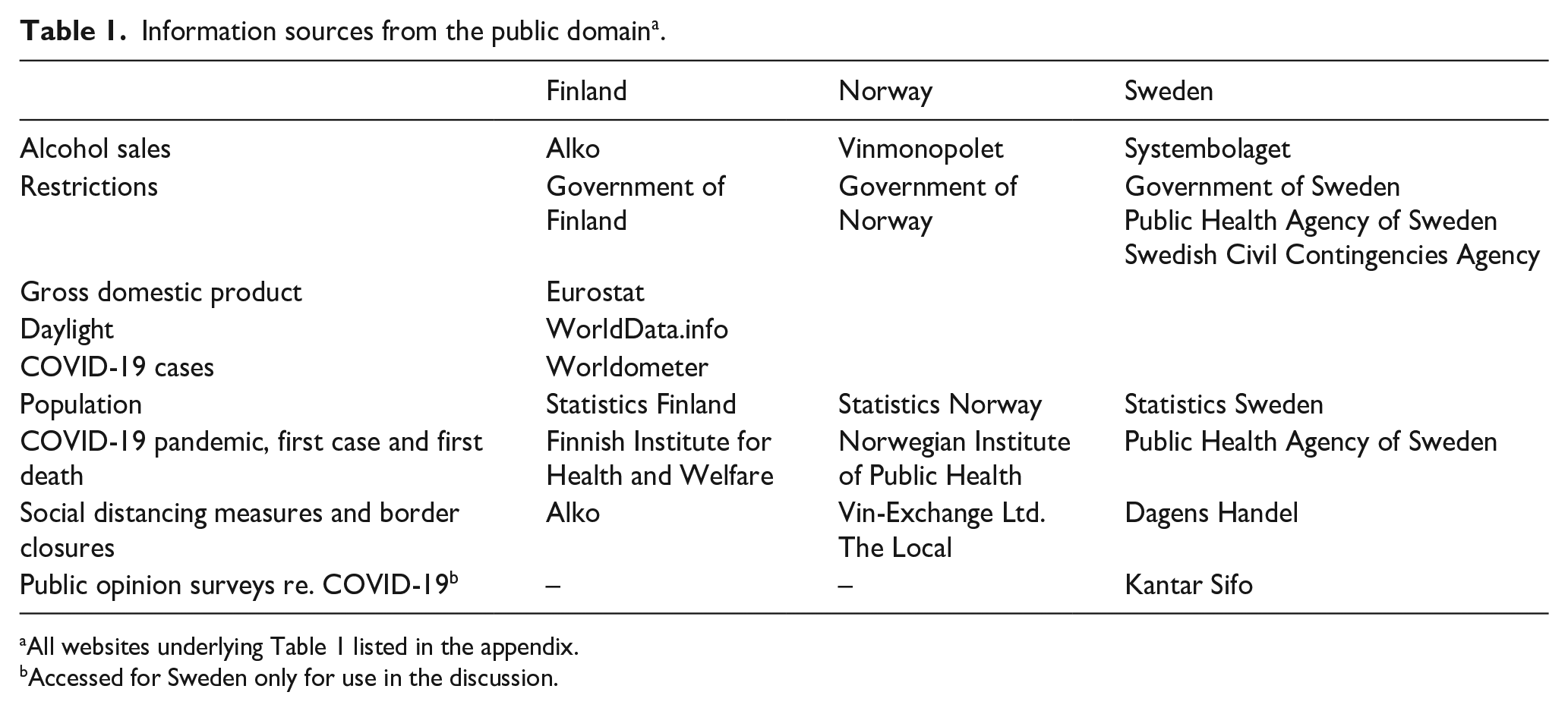
All websites underlying Table 1 listed in the appendix.
Accessed for Sweden only for use in the discussion.
Alcohol sales
Data for sale volumes were acquired in the categories of beer, wine and liquor (i.e., distilled spirits), using monthly or quarterly sales reports from the alcohol monopoly in respective countries. All three countries differ in regard to their respective alcohol by volume (ABV) limits, above which alcohol must be sold through the state monopolies. The ABV limit is 5.5% in Finland, 4.7% in Norway and 3.5% in Sweden. Extrapolated data in terms of units of ‘pure’ alcohol sold were available for Finland and Sweden but not for Norway. Instead, for Norway, the category wine, which accounted for 81–85% of total alcohol sales by volume, was used. Sales statistics from the three alcohol monopolies concerned direct private sales. Data was expressed in sales per 100,000 population aged 15 years or older.
COVID-19 restrictions
Information regarding social distancing measures and border closures was collected from government press releases. For Sweden, data was complemented by information from the Public Health Agency of Sweden (Folkhälsomyndigheten) published online. Restrictions relating to gastronomy in general and alcohol serving in particular were translated into to quarterly milestones for each country. These milestones were then expressed as either (a) restaurant lockdown or ban on serving alcohol, (b) restrictions, but no ban, on alcohol serving, or (c) no restrictions. For continually updated and overwritten webpages, we used captures from Wayback Machine, a research tool published by Internet Archive allowing for webpage snapshots frozen in time (appendix).
National economic development
To estimate national economic development, gross domestic product (GDP) per capita was used. Data was collected from EuroStat for the indicator GDP Euro per capita as quarterly exit values (Table 1).
Hours of daylight
To evaluate seasonal effects as a potential confounder, we explored the variance of alcohol sales with hours of daylight per sales quarter. We used the capital cities in each country, that is Helsinki, Oslo, and Stockholm as reference points. We chose the capitals for two reasons, (a) they lie on similar latitudes and (b) their metropolitan areas cover about one quarter of the respective total population (appendix).
Statistics
Quarterly alcohol sales for each country were plotted for the 4 years under study using 1 January 2020 as the mirror point. Alcohol sales data was then plotted against general COVID-19 restrictions, restrictions in the gastronomy sector, national economic development and hours of daylight. Concerning the economic development, a quotient was calculated using quarterly pure alcohol consumption, or for Norway wine consumption, and GDP. Two-tailed t-tests were performed using OpenEPI (appendix), comparing the mean quotients for the two pre-pandemic and the two pandemic years. As the study was based on the total available data and not just a sample of the available data, we did not conduct any further significance testing.
Ethics
This study was exclusively based on anonymous summary statistics available in the public domain. Therefore, no ethical approval was necessary.
Results
The COVID-19 pandemic in the three countries
The first COVID-19 case was recorded 29 January 2020 in Finland, 31 January 2020 in Sweden and 26 February 2020 in Norway. The first COVID-19 associated death was recorded 7 March 2020 in Finland, 11 March 2020 in Sweden and 12 March in Norway. On 31 December 2021, the endpoint of our study, the following COVID-19 associated death rates were recorded: 311 deaths/million population in Finland, 247 deaths/million population in Norway and 1462 deaths/million population in Sweden.
Social distancing measures and border closures
Whereas Finland and Norway had strict social distancing measures with restaurants and bars being closed for several months, Sweden imposed substantially fewer restrictions. In Sweden, restaurants and bars remained open throughout the entire pandemic, albeit with varying opening hours. In all three countries, the alcohol monopolies remained open for the entirety of the pandemic. However, there were some regional variations and slightly differing operating hours depending on epidemic situation. Although Sweden had not closed its borders to Finland and Norway, Finland and Norway had closed their borders to Sweden. Therefore, for most of the time during the pandemic, borders between the three Nordic countries were only open to commuters. External borders were mainly closed. They were gradually reopened to external vaccinated travellers during the second half of 2021 (appendix).
Pre-pandemic and pandemic alcohol sales
Pre-pandemic and pandemic quarterly alcohol sales are summarised in Table 2 and in more detail in the appendix.
Pre- and pandemic quarterly alcohol sales in Finland, Norway and Sweden.
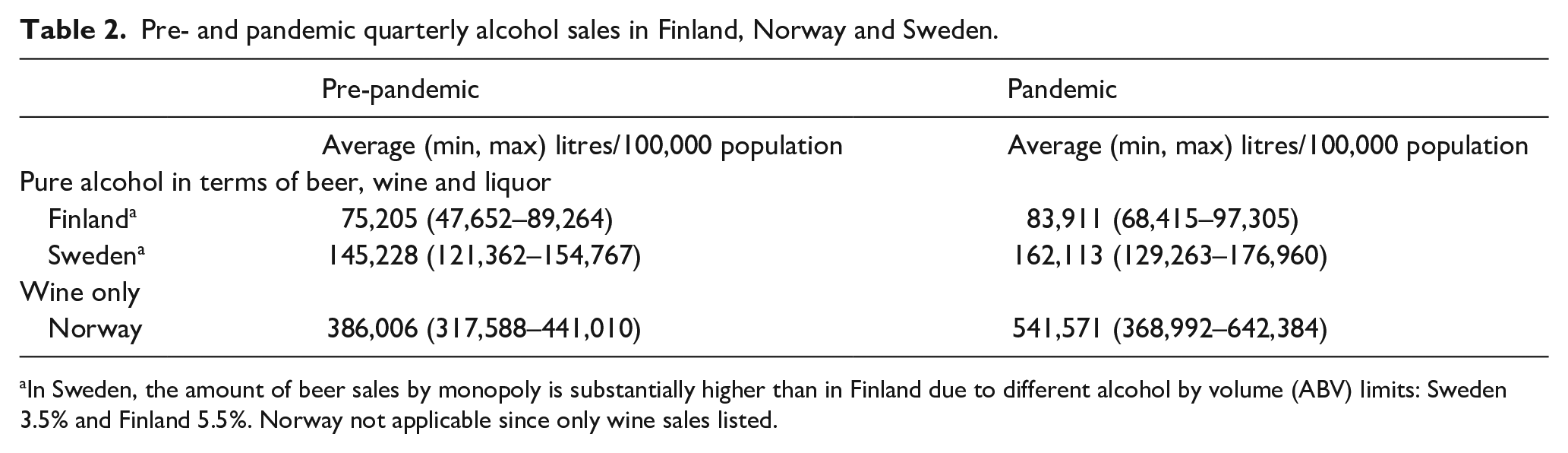
In Sweden, the amount of beer sales by monopoly is substantially higher than in Finland due to different alcohol by volume (ABV) limits: Sweden 3.5% and Finland 5.5%. Norway not applicable since only wine sales listed.
All three countries demonstrated increased alcohol sales between the first and second quarter of 2020, that is at the beginning of the COVID-19 pandemic. However, when comparing the two pandemic years with the two pre-pandemic years, there was only a slight increase in mean sales for Finland and Sweden following the underlying trend. For Norway, sales levels increased markedly during the two pandemic years. Despite this level change, the trend remained unchanged in the pandemic years (Figure 2).
On visual inspection, alcohol sales did not vary with social distancing measures limiting public gatherings (Figure 3). Nor did alcohol sales vary with restrictions specific to the gastronomy sector (Figure 4). For Norway, wine sales showed apparent correlation with closure of restaurants following the first quarter of 2020. However, no increase was seen during later lockdown periods for any of the three countries when social distancing measures were tightened further (Figure 4). The alcohol sales-GDP quotient (Figure 5) increased significantly between pre-pandemic and pandemic average for Norway. (p = .0013). The quotient did not differ significantly for Finland (p = 0.1640) or Sweden (p = 0.2575).
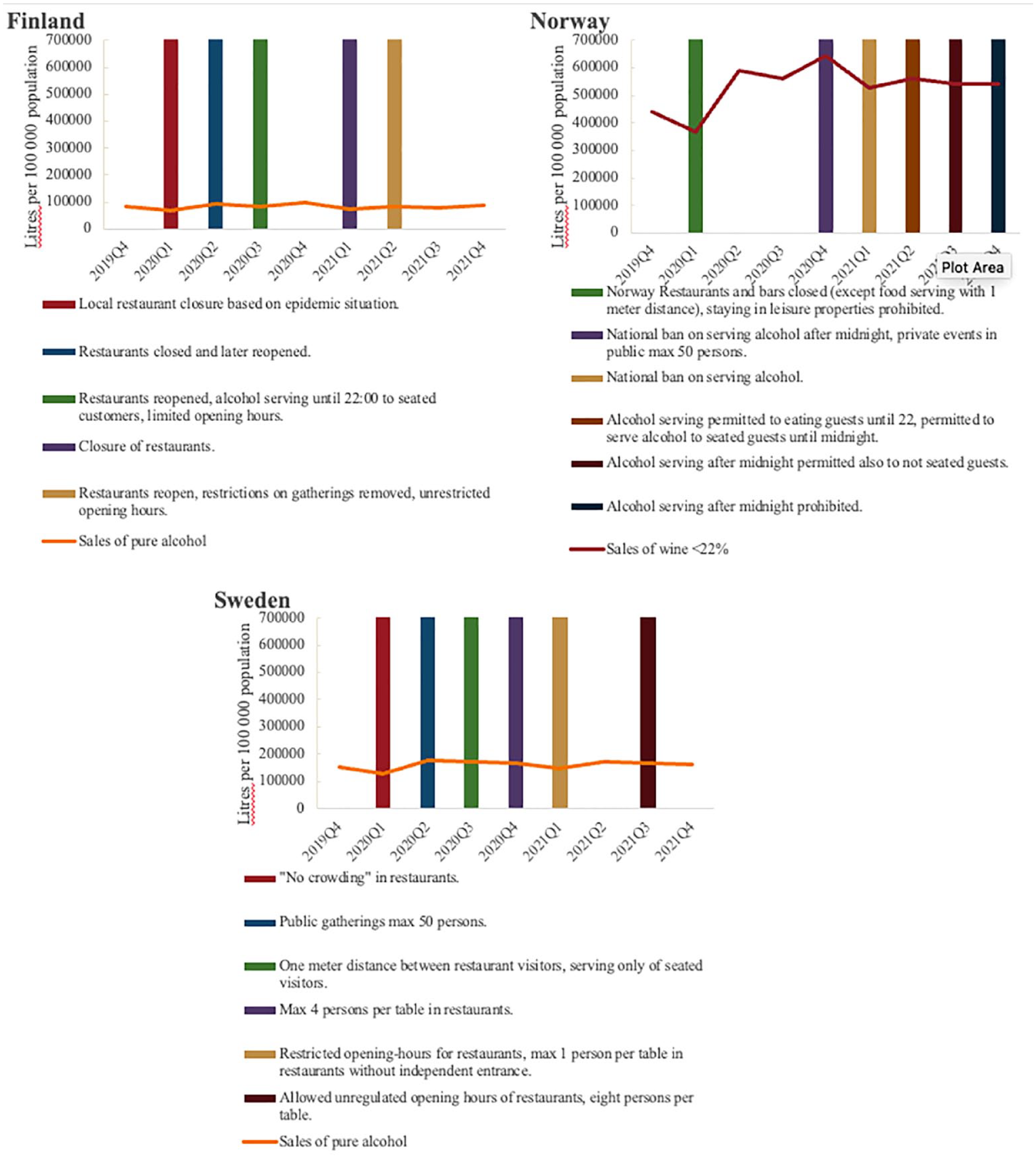
Alcohol sales and national restrictions, quarterly 2019Q4–2022.
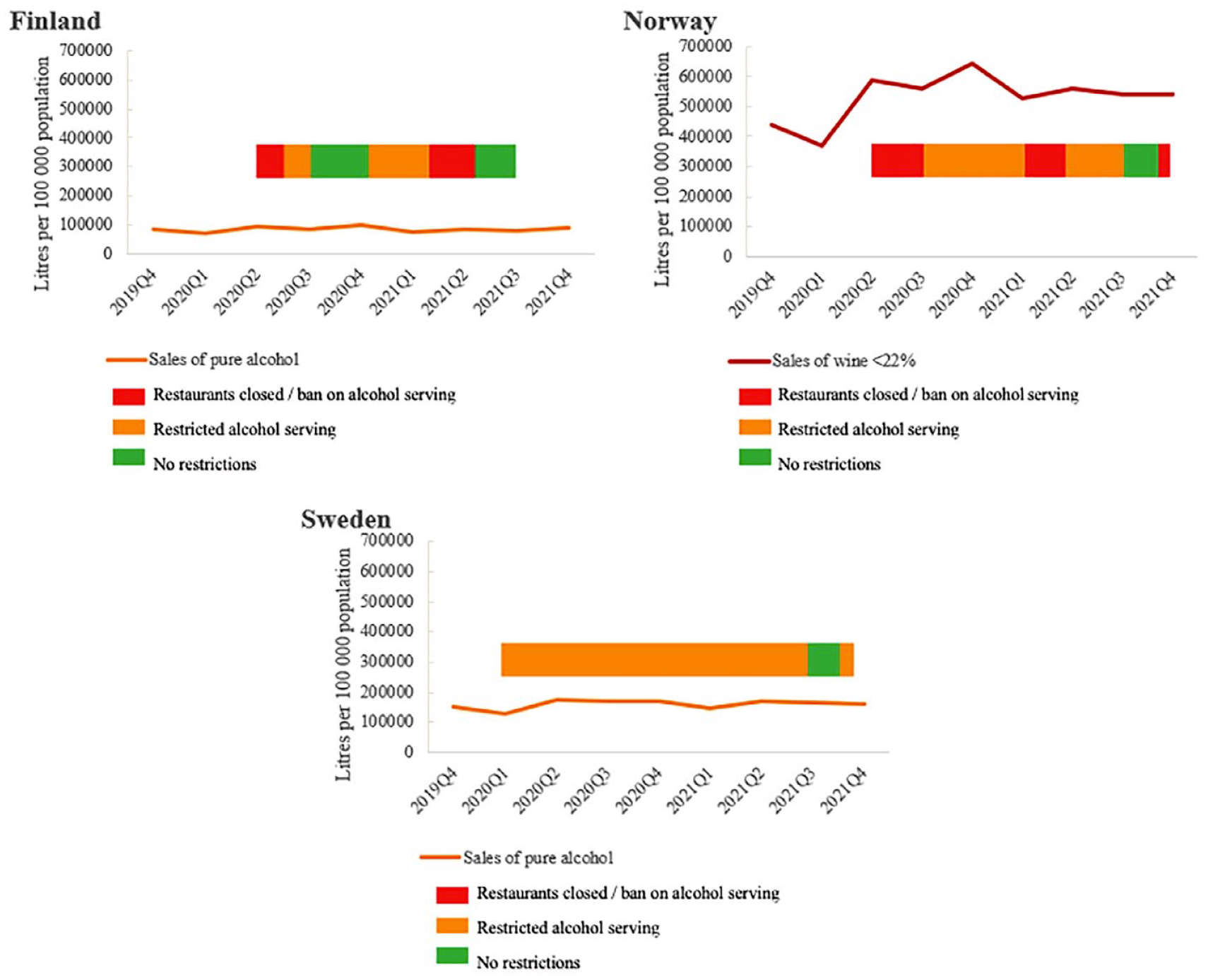
Alcohol sales and restrictions stringency in the gastronomy sector, quarterly 2018–2021.
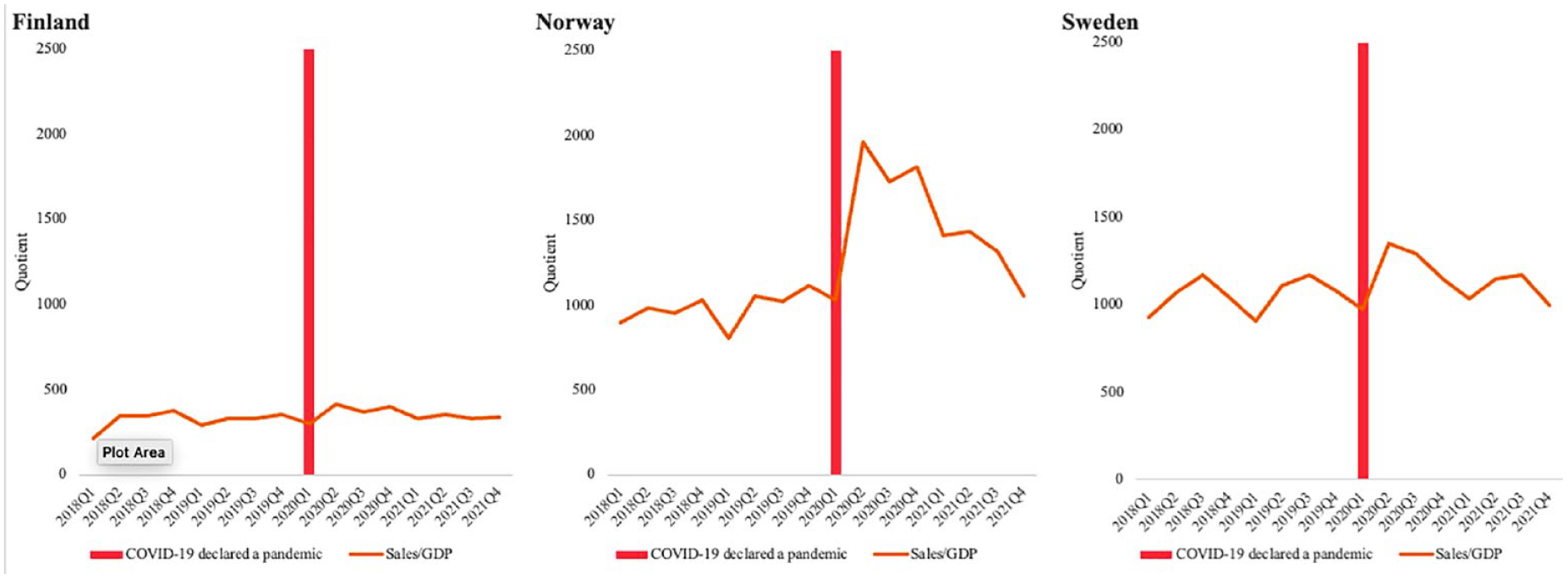
Alcohol sales/gross domestic product-quotient, quarterly 2018–2021.
For all countries, there was seasonal variation of alcohol sales. In Sweden, beer sales correlated with hours of daylight, being highest in summer and lowest in winter (Figure 6). For Finland and Norway, where beer with higher ABV is available in supermarkets, data was not available. For all three countries, wine sales were higher both during the second and fourth quarter of each year, coinciding with the midsummer and Christmas season. This seasonal pattern did not change during the pandemic years.
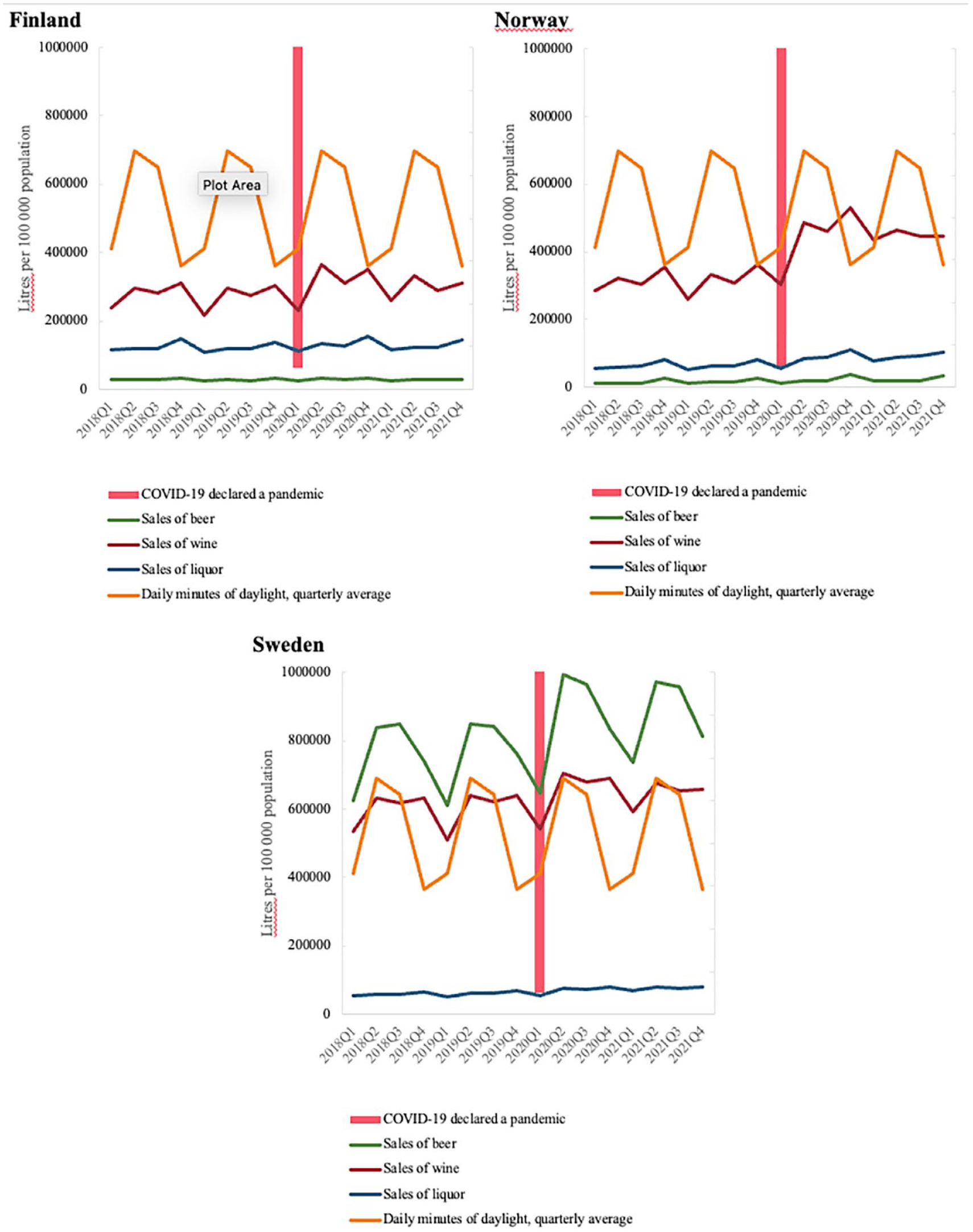
Alcohol sales and hours of daylight, quarterly 2018–20.
Discussion
In this study, we found no change in alcohol sales during the pandemic years for Finland or Sweden, but a level-change in sales for Norway. However, compared to the pre-pandemic period, there was no indication of an altered sales trend for any of the three countries. We did not see any clear correlation between restrictions on leisure or gastronomy sectors and alcohol sales for any of the three countries. The relationship between alcohol sales and GDP changed significantly only in Norway. In all three countries, sales during the pandemic largely followed the pre-pandemic pattern.
Our findings raised the question why alcohol sales had increased in Norway but not in Finland or Sweden. It was implausible that Norwegians should be less emotionally resilient that their neighbours. Strictness of lockdown could not either explain the increase of alcohol sales seen in Norway; Finland employed similarly strict lock-down measures. Therefore, we explored import figures as a possible alternative explanation. Pre-pandemic alcohol sales per capita had been higher in Finland and Sweden than in Norway. Due to higher taxation on alcohol in Norway, alcohol had widely been imported during the pre-pandemic years. In 2018, according to Norwegian sources, 77,000 litres pure alcohol per 100,000 population were imported. Of these imports, 38,000 litres of pure alcohol stemmed from tax-free sales at Norwegian airports and 25,000 litres from cross-border with Sweden (Guttormsson et al., 2022). In 2020, when pandemic restrictions were in place, only 7,000 litres pure alcohol per 100,000 population were imported via tax-free sales at Norwegian airports. According to Swedish sources, cross-border sales from Sweden to Norway dropped from a total of 2.6 million litres pure alcohol in 2019 to 647,000 litres in 2020. This corresponds to 59,000 litres of pure alcohol per 100,000 population in 2019, and 14,700 litres per 100,000 population in 2020. Here, we note a discrepancy between data from Norwegian registered imports and Swedish sales data. If the decrease of imports was factored in, there would be a level decrease rather than a level increase of alcohol consumption in Norway. For Sweden and Finland, we lack comprehensive import data. Contrary to Norway, Finland and Sweden share borders with countries that do not run an alcohol monopoly. One study addressed beer sales in Germany, comparing the two states of Schleswig-Holstein and Hamburg with the rest of the country. Schleswig Holstein was singled out due to it close connection to Sweden and Denmark. Hamburg was included because the relevant statistics report both states together. This study showed that in these two states, between 2019 and 2020, beer sales dropped by 22%. In the rest of Germany, beer sales dropped by only 5.8%.
The same study suggested for Finland that a decrease in cross-border purchases was only partially replaced by domestic purchases (Leifman et al., 2022). Therefore, if a drop of cross-border sales is taken into accounts, alcohol consumption most likely also decreased in Finland and Sweden.
A similar compensatory mechanism was observed in the UK. There, a survey compared household shopping trends from 2020 with trends from 2015 and 2019. This survey reported an increase in alcohol purchase of 37.5% between 23 March to 15 July 2020 compared with the reference periods. This increase in alcohol purchases coincided with the lockdown. However, when the investigators factored in alcohol purchases foregone due to closures in the gastronomy sector (pubs, bars, restaurants), there was no change in the overall amount of alcohol that households had purchased (Anderson et al., 2022).
Social distancing measures may increase anxiety levels, particularly at the beginning of their implementation (Brooks et al., 2020; Prati & Mancini, 2021; Robinson et al., 2022). For Sweden,
Kantar Sifo, a company conducting market and opinion surveys, monitored anxieties and concerns during the COVID-19 pandemic in a representative sample of the Swedish population. The surveys showed stable and low levels of worrying during 2021 (Table 1), although Sweden had higher COVID-19 associated mortality than Finland and Norway at the time. These low levels of worrying may have been due to the avoidance of lockdowns for any duration of the pandemic, which was unique to Sweden. But again, Finland had equally strict restriction measures as Norway with no change in alcohol sales.
Economic uncertainty coupled with a feeling of being trapped and loss of control has been highlighted as a factor that could ‘contribute to a sense of helplessness and hopelessness where people may see suicide as a way out’ (Brenner & Bhugra, 2020). Economic hardship could therefore also increase alcohol consumption due to psychological distress. One survey conducted with 14,899 residents from 105 countries suggested that job losses and lost or reduced wages may have increased alcohol consumption (Quadri et al., 2023). But in many countries, alcohol consumption during the first months of the pandemic seemed to have decreased rather than increased (Kilian et al., 2021). In one UK survey, low income was associated with decreased alcohol use (Garnett et al., 2021). Neither do our own results support a relation between alcohol consumption and economic development at macrolevel. Increased governmental economic support may have exerted a protective effect on both personal finances and finance-related distress. But it remains unclear how big such effects were compared to decreased affordability. At the same time, an interaction between high income, financial distress and alcohol consumption has been shown (Kilian et al., 2021). Possibly, members of high-income groups felt that they had more to lose during the pandemic.
Even if alcohol consumption did not increase at macrolevel, there may have been effects at microlevel. Particularly vulnerable groups may have been more prone to increasing alcohol intake than the general population. This may have resulted in a polarisation of alcohol consumption towards drastic reduction on the one hand and drastic increase on the other. Pre-pandemic factors, such as pre-existing drinking motives, may have played a role in alcohol consumption during the pandemic. Surveys suggest that pre-pandemic high or hazardous use of alcohol may have predisposed to further increase of alcohol intake during the pandemic (Kilian et al., 2022; Matone et al., 2022; Rossow, Bartak, et al., 2021; Rossow, Bye, et al., 2021). Young age, psychiatric problems including depression, female sex, work-related stressors were identified as further risk factors (Garnett et al., 2021; Jacob et al., 2021; Oksanen et al., 2021). Decreased access to addiction care may also have driven alcohol consumption up (Quadri et al., 2023).
The marked increase in sales between first and second quarter of 2020 for alcohol in all three countries may largely reflect pre-pandemic seasonality. Some cross-sectional surveys from other countries, such as Germany (Koopmann et al., 2021), the UK (Oldham et al., 2022) and the US (Barbosa et al., 2021; Castaldelli-Maia et al., 2021) also reported an increase of drinking during spring 2020. These surveys, may, to a degree, have picked up similar seasonal effects. Therefore, seasonality needs to be taken into account to avoid drawing premature conclusions from limited data at the onset of a health crisis, which, in the case of the COVID-19 pandemic, coincided with an underlying seasonal spike of alcohol consumption.
It remains unclear how accurately survey data reflects national alcohol consumption. One study of alcohol consumption in 23 European countries concluded that across all countries, alcohol consumption was underestimated when derived from survey data. Survey results may also depend on type of alcohol consumed and drinking pattern (Kilian et al., 2020). Ultimately, survey results may reflect attitudes towards and acceptability of drinking rather than real consumption (Kilian et al., 2021). For instance, conservative alcohol culture in some countries may lead to underreporting. If sampling is biased to more vulnerable parts of the population, there may be overreporting. (Kilian et al., 2021; Naimi et al., 2017). If data is pooled from many countries, data may become heterogenous and possibly non-representative if the number of participants per country is low. For instance, in the survey by Quadri et al. (2023), the average number of participants per country was 142. Pooled data may also become difficult to interpret when number of participants varies greatly between countries. In the survey by Kilian et al. (2021), 31,964 adults were sampled from 21 countries. However, 15,686 (49.1%) of respondents came from Norway. Although results were weighted, weights may not fully compensate for country-specific biases. The COVID-19 pandemic with border closures and gastronomy sector restrictions brought a unique opportunity to record total alcohol sales without the uncertainty of undeclared private import and the subjectivity of self-reports. Such data, along with a single central sales source for each country, allowed us to analyse objective trends in alcohol consumption for the duration of the pandemic. This, we consider a major strength of our study.
National sales data, such as ours, does not allow determination of changes in alcohol within subpopulations. In that sense, survey studies have an advantage. They can explore potential polarisation of consumption based on vulnerability. We adjusted for hours of daylight/season as a potential major confounder. Adjusting for more confounders was beyond the scope of our study. Sales data regarding beer was difficult to compare between the three countries due to different ABV regulations. Beer is much more freely available in Norway and Finland than in Sweden. Finally, we could not assess alcohol sales in the gastronomy sector. But since alcohol sales in the gastronomy sector were restricted or in part totally stopped, our results could only overestimate but not underestimate alcohol consumption.
Conclusion
Our study suggests that the COVID-19 pandemic had less of an impact on alcohol consumption in the three Nordic countries than could intuitively be expected. A level increase in alcohol sale in Norway was explained by decreased import. The increase of alcohol sales at the beginning of the COVID-19 pandemic coincided with a seasonal rise following a pre-pandemic pattern. Caution should be exercised with drawing conclusions from data with a short time perspective, for instance at the beginning of a major public health crisis, to avoid attribution bias.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231194486 – Supplemental material for Alcohol consumption under lockdown measures during the COVID-19 pandemic in three Nordic countries
Supplemental material, sj-docx-1-isp-10.1177_00207640231194486 for Alcohol consumption under lockdown measures during the COVID-19 pandemic in three Nordic countries by Oscar Gunnerlind, Robert Lundqvist, Michael Ott and Ursula Werneke in International Journal of Social Psychiatry
Footnotes
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: U.W. has received funding for educational activities on behalf of Region Norrbotten, Sweden (Masterclass Psychiatry Programme 2014-2018, EAPM 2016 Luleå, Sweden): Astra Zeneca, Janssen, Eli Lilly, Novartis, Otsuka/Lundbeck, Servier, Shire and Sunovion. U.W. has received lecture honoraria from Lundbeck and Janssen and has served/serves on scientific committees for Janssen, receiving honoraria for these activities. U.W. is a shareholder of Novo Nordisk. M.O. has been scientific advisory board member for AstraZeneca AB, Sweden 2018 – 2020. OG and RL declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was conducted in the framework of thesis for a MSc Medical Sciences (OG) at Umeå University, Umeå, Sweden.
Ethical approval
No ethical approval was necessary since all data used was available in the public domain.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.