
Abstract
Background:
Employment has a therapeutic impact, enhances community integration and improves the quality of life of persons with mental illness (PwMI). Vocational rehabilitation (VR) models must be sensitive to existing needs and resources. Several VR models have been tested in high income countries. Mapping different VR models in India would help both practitioners and policymakers.
Aim:
The study aimed to comprehensively review VR models tested among PwMI in India.
Methods:
We adhered to the Preferred Reporting Items for Systematic Reviews extension for Scoping Reviews. We included interventional studies, case studies and grey literature carried out for the VR of PwMI in India. The search was done in PubMed, PsychInfo, worldwide science and Web of Science. Google Scholar was used to supplement the search. A Boolean search using MeSH terms was carried out for the period January 2000 to December 2022.
Results:
A total of twelve studies (one feasibility study, four case studies, four institute-based intervention studies and two studies reporting NGOs’ role) were included in the final synthesis. The studies included in the review were either quasi-experimental studies or case based. Types of VR included supported employment or place and train or train and place models, case management and prevocational skills training.
Conclusion:
Limited studies exist on VR in PwMI from India. Most studies assessed a restricted set of outcomes. The experiences of NGOs should be published so that practical challenges can be understood. There is a need for public-private partnerships in designing and testing services and should involve all the stakeholders.
Keywords
Introduction
A high proportion of global disability-adjusted life years are attributable to mental illness (Whiteford et al., 2013). Severe mental illnesses (SMI) such as schizophrenia and bipolar disorder cause cognitive and functional decline, leading to disability (Green, 1996; Potkin et al., 2017). Disability leads to social exclusion and limitations in social participation (Burns et al., 2007; Cullinan et al., 2011). Among all disabilities, SMI is associated with the highest unemployment rates (Jagannathan et al., 2020; Jaleel et al., 2015; Suresh et al., 2012).
Employment has a therapeutic impact on symptom reduction, lowers the levels of disability and enhances community integration (Bell et al., 2014; Jagannathan et al., 2020; Michon et al., 2014). Employment is one of the indicators of well-being and quality of life for persons with mental illness (PwMI) (Durgoji et al., 2019). Employment is a critical felt need for PwMI and their caregivers, and a significant proportion of PwMI are willing to work (Khare et al., 2021; Phutane et al., 2012; Waghmare et al., 2016). Barriers such as symptoms and relapse, side effects of medications, low employment expectations, negative attitude, stigma and lack of opportunity for skill training prevent them from engaging in income generation activities and employment (Rangarajan et al., 2020; Thomas et al., 2019). There have been efforts from stakeholders to enhance the employment opportunities for the PwMI in India (Jagannathan et al., 2020; Ministry of Law and Justice, Government of India, 2016; Rangarajan et al., 2020)
In high-income countries (HIC), employment models such as supported employment or transitional employment have been effective for PwMI (Burns et al., 2007; Drake et al., 2012; Michon et al., 2014; Oulvey et al., 2013) however, many of these models are yet to be examined in low resource-settings such as in India. For example, Individualised Placement and Support (IPS) requires considerable financial and human resource investment, imposing limitations for implementation in India. Vocational rehabilitation models must be sensitive to existing needs, resources, health services and economic scenarios. The current scoping review has aimed to provide a comprehensive overview of different vocational rehabilitation (VR) models tested among the PwMI in India.
The rationale of the review
We have aimed to identify VR interventions, types, strategies and outcomes. A scoping review was selected because it allowed exploring the breadth and depth of available evidence for the given population, concept and context (PCC), (The Joanna Briggs Institute, 2015; Peters et al., 2020, 2021). We have included case studies and literature on NGO-based VR to provide a ground reality of VR interventions in India. The review findings will inform the mental health and rehabilitation professionals on various existing models in VR in India, the implications of these models, limitations and future directions.
Materials and methods
Study design
The PCC criteria were used to define the eligibility criteria in the review. The population (P) was persons diagnosed with mental illness based on ICD-10 criteria (World Health Organization [WHO], 1993); we included ICD-10 categories from F20.0 to F48.0 and the caregivers of these individuals. Concept (C) was the vocational rehabilitation/employment-related interventions in both institution/communities based, designed and provided for the population. The context (C) was India, with a prevalence of any mental morbidity of 13.67% (Gururaj, 2016). We have included all the published research between 2000 and 2022 in this review. We have included primary studies of any design that addressed VR intervention for the population.
Search strategy
A preliminary literature search was done from January 1, 2000, to December 31, 2022 using a combination of terms ‘Rehabilitation, Vocational’ OR ‘Occupational Health Services’ OR ‘Employment, Supported’ AND ‘Mental Disorders’ AND ‘India’ using the electronic database of PubMed, PsychInfo, worldwide science and Web of Science. Google Scholar (search engine) was also used to supplement the search. Further, a Boolean search using MeSH terms of keywords was also carried out.
Screening and study selection
The articles were screened through the titles, and abstract and relevant articles were selected based on the following selection criteria. Peer-reviewed original studies published in English language journals were screened for inclusion in the review by the first author, ST. The articles which addressed the research question by reporting on any of the following areas were considered for inclusion in the review (1) psychosocial interventions carried out for employment of PwMI, (2) interventional studies, case studies and grey literature and websites such as ‘Worldwide Science. Org’, and websites of NGOs working in the area carried out for employment of persons with mental illness and (3) interventions assessing the employment-related outcome among the PwMI. In case of any discrepancy, the studies were included in the review if there was consensus amongst all the authors.
Data extraction
Data were extracted from each source using a data extraction form developed by the first author ST and was independently reviewed by the other authors. Extracted data covered the following: author (s), year of publication, aim/purpose, study population and sample size, settings, study design, VR intervention type, VR intervention principles, outcome assessment, significant findings and conclusion. The extracted data was transferred to a spreadsheet, and all the authors reviewed the information.
Results
Characteristics of included sources: A total of 24,411 studies were identified using the databases. Based on the inclusion criteria, twelve studies were included in the review (Figure 1). We have included five intervention studies, four evidence-based case studies and one community-based rehabilitation intervention with VR components. Besides, we have included two studies which mentioned the role of NGOs in VR.
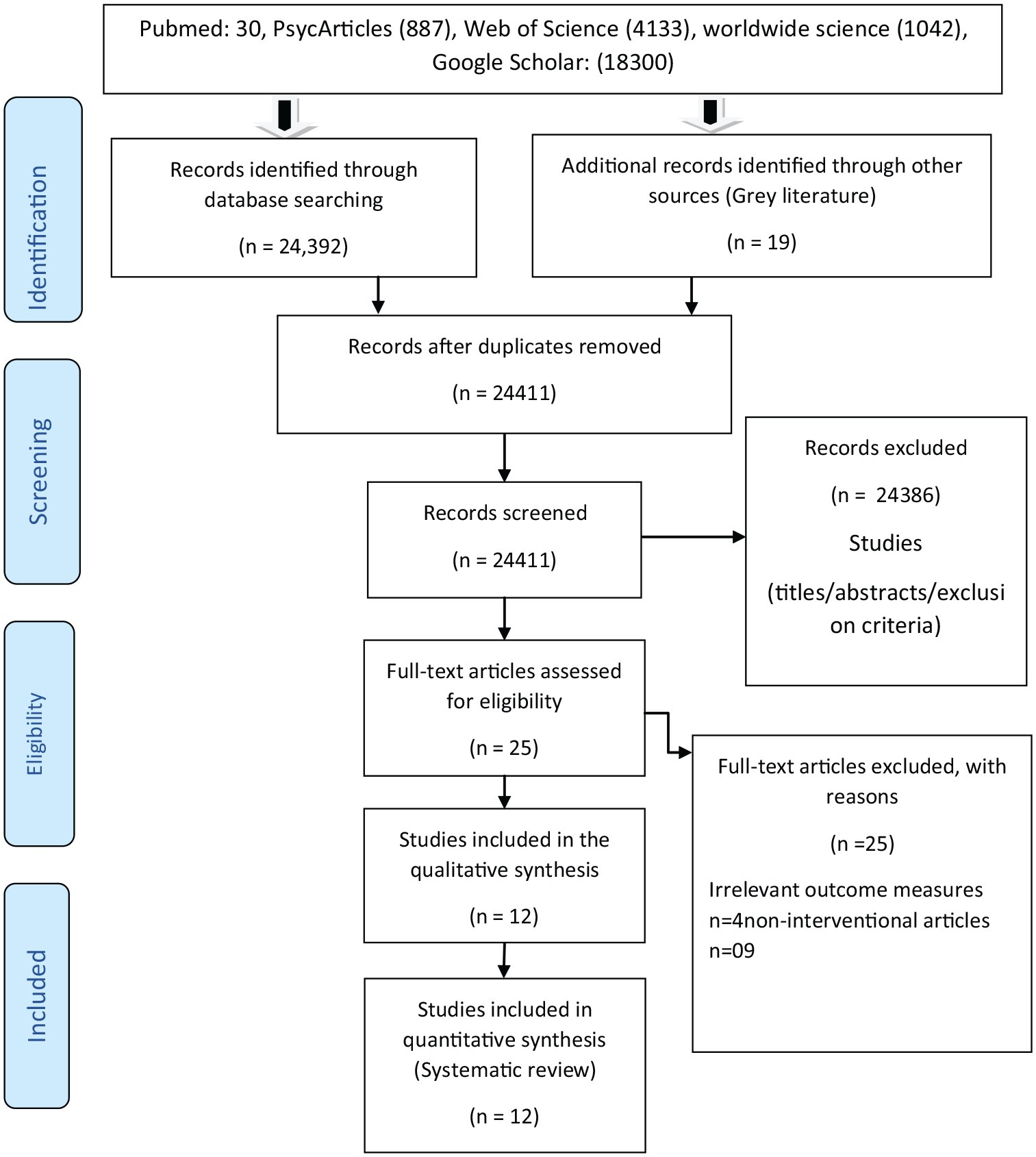
PRISMA flow diagram.
Review findings
The section presents the scoping review findings covering the types of VR or employment models, the population and the settings of the intervention and outcomes. A summary of the review findings has been attached in the online Supplemental File 2.
Evidence-based models of VR in India
Vocational skill training was the most common VR identified along with the supported employment model. All twelve studies were either non-RCTs or case studies. A summary of the review findings is attached in the Supplemental File.
Supported employment models
Only one interventional study reported using a supported employment model in India. The study was conducted in a tertiary care mental health setting to evaluate the feasibility of a supported employment programme for persons with severe mental disorders (SMIs) (Jagannathan et al., 2020). A single group pre and post without control design was used to test the feasibility of the interventions. Sixty-three participants with SMI (Schizophrenia 44 and bipolar affective disorder 19) were recruited for the study. The study included participants with clinical stability, with a minimum of 10th standard education and a minimum 6-month of unemployment. The components of the model were (a) assessment of the vocational potential with a vocational potential assessment scale (Harish et al., 2020) vocational counselling by trained research staff, (b) networking and liaison with various stakeholders/employers working in the private and public sectors, (c) job-related training by using train and place model or place and train model based on individual needs and (d) continuation of support for 6 months. The findings from the study suggest that more than half the participants (50.8%) were placed in competitive employment and 27% of the participants actively attempted the placement, 11.1% of the participants required upskilling and 11.1% of the participants dropped out during the follow-up period. There was an improvement in the socio-occupational functioning of the participants who participated in the intervention and a reduction in their disability. The study also reported that more than five participants continued their education for more than 6 months. Some of the study’s limitations were the lack of a control group to test the influence of other extraneous variables, such as the influence of other psychosocial interventions; the study did not consider self-employment as a type of employment for PwMI in this model.
Evidence based on case studies on supported employment
We identified four case studies and included detailed descriptions of six cases of VR in India. Three case studies used a supported employment approach for persons with schizophrenia, whereas one for obsessive-compulsive disorder (Andrade et al., 2022; Jaleel et al., 2014; John et al., 2017). The supported employment approaches used in these studies were vocational assessment, skill training, rapid job search based on patient choice, vocational placement and integration of mental health services into the workplace by focussing on regular follow-up. The studies found that supported employment approaches helped enhance vocational skills, assisted in vocational placement, job retention and financial independence for more than 1 year. In addition, the studies also reported improvement in the socio-occupational functioning of the participants, thus, leading to reduction in symptoms and disability. The third case study used a family-centric rehabilitation approach by integrating the supported employment intervention with other psychosocial interventions and found improvement in vocational skills, identification of suitable employment and placement, retention of employment for more than 1 year, symptom reduction, functionality improvement and psychosocial well-being of the entire family (Thekkumkara et al., 2020). Besides, the approach mentioned the role of disability welfare benefits such as reservation for employment, reasonable accommodation and other social security schemes based on the Rights of Persons with Disability Act (RPWD) 2016 to ensure the entire family’s welfare. The standard approach used in all the case studies was the case management approach for providing VR services. The services provided by the MHPs were assessments of vocational skills, direct VR interventions, collaboration and coordination with vocational skill training centres, vocational instructors and potential employers in the private and public sectors. The case studies emphasised the need for a case management approach through continuous evaluation and follow-up.
Tertiary care centre-based vocational rehabilitation models
Four studies (Gandhi et al., 2014; Roy et al., 2019; Suresh Kumar, 2008; Xaviour et al., 2022) used a tertiary care centre-based vocational rehabilitation model. The interventions’ settings were day-care-based vocational rehabilitation centres as adjuncts to the psychiatry department. Two of these studies were conducted at the Psychiatric Rehabilitation Services of the National Institute of Mental Health and Neurosciences (NIMHANS), Karnataka, India. The other two included studies were undertaken in the rehabilitation units at the Institute of Mental Health and Neuro Services (IMHANS), Kerala, India. The interventions included vocational skill assessment, prevocational training in various sections of the day-care – candle making, bakery, paper printing, computer basics, green skills, paper cup making, bag and umbrella-making and included other psychosocial interventions from the multidisciplinary team members. The training was provided for both inpatients (for meaningful engagement, symptoms management and pre-vocational skill training) and outpatients as day boarders (as a part of activity scheduling, prevocational skill learning, vocational skill learning and source of behaviour-based incentives). The studies reported improvement in work performance, treatment adherence, self-esteem, quality of life and well-being of the participants (Gandhi et al., 2014; Suresh Kumar, 2008). Moreover, these models depicted improved quality of life and caregivers (Xaviour et al., 2022). In one of the studies (Roy et al., 2019), the vocational rehabilitation model used was Holi colour-making using flowers conducted by collaborating with a non-governmental organisation (NGO). The primary outcome of this model was profit sharing with all the participants based on their performance and contribution.
Community-based rehabilitation models
The community-based rehabilitation models (CBR) have primarily focussed on the elements of the CBR matrix proposed by WHO (2010), focussing on skill training and vocational rehabilitation under the matrix employment. The study conducted to understand the effectiveness of CBR on the disability of persons with schizophrenia in rural community settings in India adopted a randomised control trial design (Chatterjee et al., 2014). The trained lay health workers delivered the interventions on the various components, including ‘Individualised rehabilitation strategies to improve the personal, social and work functioning of participants’. The VR interventions provided were vocational counselling, referral services and skill training (Balaji et al., 2012; Chatterjee et al., 2014).
Vocational rehabilitation interventions initiated by the NGOs
NGOs provide a plethora of VR interventions in institutions and the community. An exploratory study was conducted to understand the income generation programmes for PwMI and the challenges faced, using a mixed methods approach of field visits and qualitative interviews across 13 mental health rehabilitation centres while gathering the details of interventions and challenges (Roy, Jayarajan, & Sivakumar, 2020). The study identified that most NGOs were private, located in urban areas and provided residential and VR interventions. The centres follow a mixed method of vocational training, including vocation-based skill training or transitional employment process, looking at the local resources and viable employment opportunities particular to that community. The vocational/income generation activities included household consumables, paper products, textile products, handicrafts, food products, animal husbandry, jute products, horticulture and running the shops. The VR activities were reported to be a collaboration between the PwMI, caregivers, NGOs and other stakeholders. The personnel involved in most of the NGOs were vocational instructors, mental health professionals and other NGO staff. The study has detailed descriptions of NGOs’ vocational/income generation activities. Another study conducted to understand the human resources and models of mental healthcare integration into primary and community care in India recorded the VR initiatives by NGOs such as Chellamuthu trust, The Volunteers for Community Mental Health (VOLCOMH) outreach programme at Mizoram, Medico Pastoral Association, Enable India and the Richmond Fellowship Society of India (Chowdury, Dharitri, Kalyanasundaram, & Suryanarayana Rao, 2011; Jaleel et al., 2014; Rajeev & Shinde, 2022; van Ginneken et al., 2013).
Discussion
In India, the employment needs of PwMI have been explored, and the importance of VR interventions for improving employment outcomes among PwMI has been recognised (Durgoji et al., 2019; Jagannathan et al., 2020; Samuel & Jacob, 2020; Waghmare et al., 2016). The current review shows that only limited evidence exists for VR in India. Our review has highlighted the benefits of the existing models of VR, the approaches and outcomes specific to India. Many tertiary care centres have psychiatry units that provide VR services as part of the various psychosocial interventions, yet only twelve published studies could be identified. The studies identified were either case studies or quasi-experimental research designs, emphasising the need for more experimental studies. Though one RCT on CBR was included in the review, the results of the study did not explicitly report the VR process. The reasons for the limited literature maybe because most of the VR services are provided by NGOs who may not necessarily engage in evidence-based research. Another reason could be that compared to the number of organisations providing VR in HIC, there is lack of a systematised VR service in India. The paucity of funds allocated to the mental health and disability sector could be the reason for limited research in the area (Math et al., 2019; Vashist et al., 2022). Rehabilitation may be construed as not related to the health sector directly and to be dealt by the social justice and empowerment sector. Intersectoral coordination may be challenging.
Supported employment is the best evidence-based practice in VR from HIC (Kinoshita et al., 2013). Only one study had tested the feasibility of the model in India (Harish et al., 2020; Jagannathan et al., 2020). Placement status, job retention and impact of employment on disability rates and functionality have been regarded as essential outcome variables in the studies conducted in HIC and the study conducted in India also reported outcomes on these variables (Michon et al., 2014; Wallace & Tauber, 2004). Further, the study recorded participants’ experience while availing of the supported employment services. The model was tested after the Rights of Persons with Disabilities Act (RPWD), 2016 (Ministry of Law and Justice, Government of India, 2016). It incorporated some of the critical provisions of the Act, such as reasonable accommodation and recognising high support needs. A study conducted in India has elucidated the importance and nature of reasonable accommodation in employment for persons with psychiatric disabilities (Rangarajan et al., 2020). The study highlights the need to upscale the model with more rigorous research methods like RCTs.
The other studies in the review were case studies that used various components of the supported employment model. The case studies included in the review consistently reported improvement in psychopathology, global functioning and reduction in overall disability levels, similar to findings with supported employment outcomes as reported in a systematic review (Burns et al., 2007). The included studies have emphasised a multidisciplinary approach to delivering the services, which includes psychiatric social workers, psychiatrists, clinical psychologists, psychiatric nurses and vocational instructors (Dobbins et al., 2016; Liberman et al., 2001).
The review highlights the role of tertiary care centre-based day care centres in providing VR services. Tertiary care centres-based VR models are often considered a traditional model of rehabilitation (Murthy et al., 2017; Waghmare et al., 2016) that serve many purposes such as engagement in meaningful activities, a multitude of opportunities for graded exposure to work, prevocational and vocational skill training and transition to employment. Some centres have moved to a concept called profit sharing (Roy et al., 2019). Most of these centres employ inpatients and outpatients in tertiary care centres (Chandrasekaran et al., 2022; Roy et al., 2020; Thekkumkara et al., 2020; Xaviour et al., 2022). However, these centres are not restricted to persons with psychiatric disabilities and have reported outcomes in persons with intellectual developmental disabilities and other physical and neurological disabilities (Chandrasekaran et al., 2022; Roy et al., 2019). Studies show improvement in caregiver’s burden, enhanced well-being and coping apart from improved patient-related outcomes secondary to the VR (Chandrasekaran et al., 2022; Thekkumkara et al., 2020; Xaviour et al., 2022). A national survey conducted to understand the conditions of mental health centres across the country with special reference to the women with mental illness found that out of 26 tertiary care mental health centres, 18 provided VR interventions (National Commission for Women, 2019). The survey indicated that in most tertiary care centres, the training provided needed to be more adequately utilised as a means for recovery and as a source of income for the PwMI (National Commission for Women, 2019). In addition, the survey found that these skills are all conventional with limited market value and offer a minimal scope for a treated PwMI to become economically self-reliant. A few institutions have adopted skills training that may be contemporarily relevant in the Indian context, such as mobile cover making, gift packing, screen printing, handicrafts, leather toy making, painting, craftwork, music, gardening and goat rearing (National Commission for Women, 2019).
The review has identified that either train and place or place and train models were used in the studies. The train and place model focusses on generic work skills and personal development training in such areas as confidence building, assertiveness, communication skills, activities of daily living skills and stress management (Danley & Anthony, 1987). In this model, the participants must learn pre-vocational and work readiness skills before they are placed in work settings which are often sheltered workshops under the supervision of mental health professionals or owned by hospitals or rehabilitation agencies (Rinaldi & Perkins, 2007). In contrast, the place and train models focus on placing the person in competitive employment by liaising and then training the person in a set of skills necessary for work (Kinoshita et al., 2013).
Based on the principle of empowerment and recovery and through a partnership of the MHPs and the PwMI, the clubhouse model of VR can be an alternative that needs to be explored in VR. Systematic reviews have reported the effectiveness of the model in improving the quality of life, employment outcomes and reducing the rates of relapse and hospitalisation of PwMI. Though these models were tested in the 1950s in HIC no published literature was found that used the clubhouse model in India (Battin et al., 2016). SEVAC, based in Kolkata, India is probably the only clubhouse in the country that is recognised by the Clubhouse International (Battin et al., 2016; Sevac, n.d.)
NGOs play a vital role in providing rehabilitation services in India (Thara & Patel, 2010). The role of NGOs in delivering VR has been recognised (Jaleel et al., 2015; Thara & Patel, 2010), yet there is a shortage of published literature on VR interventions provided by NGOs. Many NGOs provide VR-based intervention in institutional and community rehabilitation settings but limited scientific reporting can lead to constraints in replicating these models in other centres (Chowdury et al., 2011; Jaleel et al., 2014; Rajeev & Shinde, 2022; Sahu et al., 2014). There are government institutions such as Lokapriya Gopinath Bordoloi Regional Institute of Mental Health (LGBRMH), Tezpur and NIMHANS, Bengaluru, that have initiated a partnership with NGOs for VR interventions (Roy et al., 2019). Most NGOs are in urban areas, and there is a requirement for rural-based VR opportunities. To overcome these challenges, the Government of India’s flagship programmes, such as the Skill India programme (Thekkumkara et al., 2021), other government-initiated skill training programmes such as ‘Manasadhara’ day care centres ( Government of Karanataka, n.d.), regional vocational skill training centres for women (Ministry of Skill Development and Entrepreneurship, Government of India, n.d.), and the locally available microfinance self-help groups, can be utilised (Nair et al., 2018; Ravilla et al., 2019).
Considering the population in rural areas, CBR can significantly contribute to the VR of the persons residing in rural Indian communities (Balaji et al., 2012; Chatterjee et al., 2009; Sivakumar, 2019). The advantages of such intervention include understanding the local situations, community needs, local resources and employment demands and providing VR interventions based on the prevailing needs (Ravilla et al., 2019). Based on the CBR models, studies have been conducted in the community, and vocational components were included in the interventions; however, a detailed description of the specific VR provided, and process have not been explicitly recorded (Chatterjee et al., 2009; Patel et al., 2011). The components of CBR, such as self-help groups, can be explored for its viability for persons and caregivers with mental illness in the community (Nair et al., 2018). Assertive Community Treatment has been tested and reported effective in HIC (Gold et al., 2006; Waynor & Dolce, 2015). ACT model has been explored rarely in the Indian context except for one published report. However, it did not record employment outcomes (Arahanthabailu et al., 2022).
In India, while considering the employment/VR interventions for PwMI, the approaches must be designed by understanding the ground realities. The requirements ensured under the RPWD, 2016 for persons with disabilities must be incorporated carefully (Ministry of Law and Justice, Government of India, 2016). The provisions, such as reasonable accommodations and higher support needs, would encourage a PwMI to engage in competitive employment and may also enhance recovery. MHPs must advocate for ensuring workplace reservations and reasonable accommodations for PwMI. A minimum of four percentage of public sector employment has been reserved for persons with disabilities, including one per cent for persons with disabilities due to mental health conditions and multiple disabilities (Philip et al., 2022). Assistance by MHPs to the PwMI in registering with the special employment exchange or the government-initiated online services such as Swarajability would enable them to identify employment fairs and may increase the chances of employment (India, n.d.; Ramasubramanian et al., 2016). PwMI as persons with disabilities have been included in the Mahatma Gandhi National Rural Employment Guarantee Act (MNREGA) programmes (Ehmke, 2016), which guarantees minimum employment and wages for PwMI and the National Handicapped Finance and Development Corporation (Department of Empowerment of Persons with Disabilities, n.d.) provides subsidised loans for various microfinance self-employment programmes.
Partnerships between NGOs and tertiary care centres would provide a platform for adapting and developing some VR approaches among the PwMI (Patil, Patil, Tekkalaki, Chate, & Patil, 2022). For designing and implementing any model of VR, human resources (occupational therapists, placement officers, vocational instructors) who can integrate with mental health services are essential. The existing mental health care centres should focus on enhancing human resources and ensuring the provision of VR services to mental health service users. The upcoming National Institute of Mental Health Rehabilitation at Sehore (Ministry of Social Justice & Empowerment, Government of India, n.d.) can play a vital role in developing, testing and implementing the models of VR for the PwMI so that the District Mental Health Programme, NGO and other tertiary mental health care centres can deliver VR services for PwMI.
Strengths
The selection of studies was not restricted to a particular model of VR, and we have included all the available literature, including case studies. While reporting, we have adhered to the JBI scoping review method and PRISMA-ScR guidelines for writing scoping reviews.
Limitations
The review identified a small number of studies overall and included case studies. We have only included VR interventions relevant to psychiatric disabilities and have not focussed on IDD or other developmental disabilities. Many VR interventions could be common with PwMI and there could be several needs that may need to be individualised.
Conclusions
A limited number of studies have been published on VR for PwMI from India. Most studies are either feasibility studies or case studies assessing only a few outcome variables. Indigenous models and adaptations of successful models reported elsewhere (e.g. supported employment) must be developed and tested through rigorous experimental studies. The experiences of NGOs need to be published so that practical challenges can be understood. There is a need for more public and private partnerships in designing and testing services involving all the stakeholders.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231183920 – Supplemental material for Vocational rehabilitation in persons with mental illness in India: A scoping review
Supplemental material, sj-docx-1-isp-10.1177_00207640231183920 for Vocational rehabilitation in persons with mental illness in India: A scoping review by Sreekanth Thekkumkara, Vikram Singh Rawat, Aarti Jagannathan and Krishna Prasad Muliyala in International Journal of Social Psychiatry
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval Ethical clearance for this study was not required as secondary data were used.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.