
Abstract
Background:
The Health of the Nation Outcomes Scales for people with Learning Disabilities (HoNOS-LD) is an 18-item measure which provides a structured and standardized approach to rating various clinical and psychosocial outcomes and has been in use nationally since 2002.
Aims:
To revise and improve the HoNOS-LD’s utility in contemporary intellectual disability (ID) services whilst retaining its original objectives and five-point severity ratings.
Method:
ID clinicians were invited to complete an online survey, rating each item on the existing measure for being fit for purpose, identifying issues and suggesting improvements based on their experience of using the HoNOS-LD in practice. Scales were then assessed and revised sequentially; survey responses were used to inform discussion and revisions to the HoNOS-LD by the Advisory Board.
Results:
A total of 75 individuals replied. Respondents had used HoNOS-LD for an average of 8.0 years (S.D. 5.28 years) and 88% found the scale to be useful in their practice. On average, respondents used HoNOS-LD ratings to inform care 42.4% of the time (S.D. 33.5%). For each scale there was a significant negative correlation between the percentage of positive/very positive respondent ratings and the number of changes proposed. Common changes included simplifying terms, reducing ambiguity and replacing anachronistic language.
Conclusion:
The changes outlined in this paper are based on the advisory group’s expert consensus. These changes are intended to improve reliability and validity but now need empirical testing as well as review by service users.
Introduction
Intellectual disability
Intellectual disability (ID) describes ‘a condition of arrested or incomplete development of the mind, which is especially characterised by impairment of skills manifested during the developmental period, which contribute to the overall level of intelligence, including cognitive, language, motor and social abilities’ (WHO, 2019). In the United Kingdom however, the term learning disability (LD) is the preferred term (Cluley, 2018) This article refers to clinical tools from the 1990s as well as contemporary clinical practice hence both terms are used interchangeably according to the timepoint in question.
The Health of the Nation Outcome Scales (HoNOS) and the HoNOS-LD
The HoNOS is a 12-item outcome measure intended for use with adults of working age experiencing severe mental conditions (Wing et al., 1999). It was developed and refined through field tests with 2,706 patients and 492 clinicians (including psychologists, nurses, occupational therapists, psychiatrists, speech and language therapists and support workers) before the final version was validated with 197 psychiatric patients (Wing et al., 1998).
Testing of HoNOS with people with intellectual disabilities (PwID) found limitations in key clinical areas such as communication skills and movement disorders (Ashaye et al., 1997). This resulted in the development of the HoNOS-LD, an 18-item measure, which was tested against other established measures with 372 PwID. This was shown to have good reliability and validity, providing a structured and standardized approach to measure various clinical and psychosocial outcomes (Roy et al., 2002).
Like the HoNOS, the HoNOS-LD was intended to be holistic, suitable for routine use and hence acceptable to a range of professions in a variety of settings (Wing et al., 1998). It was also designed to have good reliability (both inter-rater and internal consistency), sensitivity to change over a 3 month period and have a positive correlation to more established scales such as the Aberrant Behaviour Checklist (Roy et al., 2002; Tenneij et al., 2009).
Since its development, the HoNOS-LD has been translated into other languages including French (Straccia et al., 2022) and Spanish (Esteba-Castillo et al., 2018). It is used in clinical practice in England, where it forms part of outcome data collected nationally (NHS Digital, 2022) and New Zealand, where its use is mandated (Te Pou, 2021). It has shown to be useful in measuring outcomes and guiding treatment in a range of settings (Hillier et al., 2010).
The aim of this study was to review and improve the HoNOS-LD’s utility in contemporary intellectual disability services whilst retaining its original objectives and five-point severity ratings. This paper outlines the scope, process, issues identified and resulting revisions (subsequently renamed HoNOS-Intellectual Disabilities or HoNOS-ID).
Method
Study design
An Advisory Board (chaired by the RCPsych’s National HoNOS Advisor) was convened by canvassing professional networks for representatives from England and New Zealand with extensive experience in either: HoNOS-LD staff training; its use in clinical practice; using aggregated HoNOS-LD data for service, professional or governmental level oversight. The eight Board members represented psychiatry, psychology, mental health and ID nursing, nurse educators and information analysts from England and New Zealand (see Supplemental Information 1).
Members of this board oversaw the development of an online survey tool and identified relevant professional stakeholder networks (including the UK’s: Royal College of Psychiatrists, the British Psychological Society, Learning Disability Senate, Intellectual Disability Research Network and New Zealand’s: Programme for the Integration of Mental Health Data and the HoNOS Trainer’s Group), where the survey link was subsequently circulated. Finally, Board member JP collated and analysed the survey responses before using them to inform the Board’s revisions to the HoNOS-LD.
Measures
With reference to the project’s aims and objectives, the bespoke questionnaire was developed using Qualtrics (Qualtrics XM, 2022), an online survey platform. The international membership of the working group ensured the phrasing of questions was generalizable to clinicians working both in the UK and New Zealand where different terminology is used. The final version of the survey was estimated to take approximately 30 min to complete which was deemed the optimum time to balance response engagement and gain the minimum required information to draw meaningful conclusions.
The online cross-sectional survey used an exponential and non-discriminatory snowballing technique (Etikan, 2016). This involved commencing with key contacts in professional organizations of the authors in different participating countries and requesting they forward the request and link within their own professional networks. This should be considered non-probability sampling.
The introductory section specified that the survey was aimed at clinicians working primarily with PwID before gathering some generic information about the respondents. Subsequent sections guided participating healthcare professionals to reflect on their experience of using the HoNOS-LD in routine practice, to identify issues and to suggest any revisions they felt the Advisory Board should consider making. Finally, for the overarching HoNOS-LD instruction page, and each of the subsequent 18 scales, the original text was presented followed by four questions:
(i) What could be changed to simplify this part of the tool?
(ii) What could be changed to reduce ambiguity in this part of the tool?
(iii) Is there any language in this section that is now outdated in the context of contemporary practice?
(iv) Overall, this section is fit for purpose (a five-point Likert scale from ‘strongly disagree’ – ‘strongly agree’).
The survey was available online throughout July and August 2020 with a reminder to encourage participation sent at the midpoint. The survey template is provided in Supplemental Information 2.
Process
To ensure consistency with the previous reviews of HoNOS (James, Painter, et al., 2018) and HoNOS65+ (James, Buckingham, et al., 2018), the same criteria were used to judge the survey responses. These were that, for a change to be supported, it needed to result in a tangible improvement (e.g. simplification/clarification/removal of anachronisms) and:
maintain the original instrument’s integrity as far as possible.
maximize comparability with existing individual and aggregated data.
support the use of HoNOS-LD as a summary of clinical assessment(s).
adhere to the HoNOS-LD ‘core rules’: each item is a behaviourally anchored five-point scale. items are sequentially rated (1–18). all available information is used to make a rating. information already rated in an earlier item is disregarded. the most severe problem/worst manifestation from the preceding 4 weeks is rated. problems are rated according to the degree of distress caused and/or its impact on behaviour. must be rated by a mental health professional trained in clinical assessment. problems are rated regardless of cause.
Ethics and governance
All participants were advised at the start of the study that participation was voluntary, that no participant identifiable data would be collected and their replies would be anonymized and pooled prior to analysis. Further, it was specified that informed consent from these healthcare professionals would be presumed if participants submitted the survey. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were ethically approved by Sheffield Hallam University (Review ID: ER21994638).
Analysis
Anonymized responses to the survey were downloaded into Microsoft Excel for data cleaning and analysis. Fixed-response variables were categorical or ordinal, thus analysis consisted of frequencies and cross tabulations. A Spearman’s rank correlation was calculated to assess the relationship between the percentage of positive/very positive fitness-for-purpose ratings and the number of changes proposed for each scale.
Free-text replies were grouped for analysis by author (MM) before authors (JP and MJ) applied the agreed criteria to categorize each suggestion as potentially in/out of scope according to the magnitude and significance of the change that would be required. In conjunction with the Likert scale ratings for each HoNOS-LD scale (Table 2), this helped to structure the Advisory Board’s monthly online meetings. Scales were assessed and revised sequentially before the revised tool was reviewed in its entirety to ensure:
No changes had breached the a priori project criteria.
Consistency of language.
The gradation of severity ratings remained in keeping with the original scales.
All survey responses had either been actioned or rejected with the group’s decision recorded for transparency.
Upon completion of their discussions, the Board agreed the final draft of the revised tool which is presented in this paper.
Results
The 75 respondents that completed the survey had worked in the field of ID for an average of 16.8 years (S.D. 10.1 years) and used HoNOS-LD for an average of 8.0 years (S.D. 5.28 years). Further participant details can be seen in Table 1.
Participant attributes.
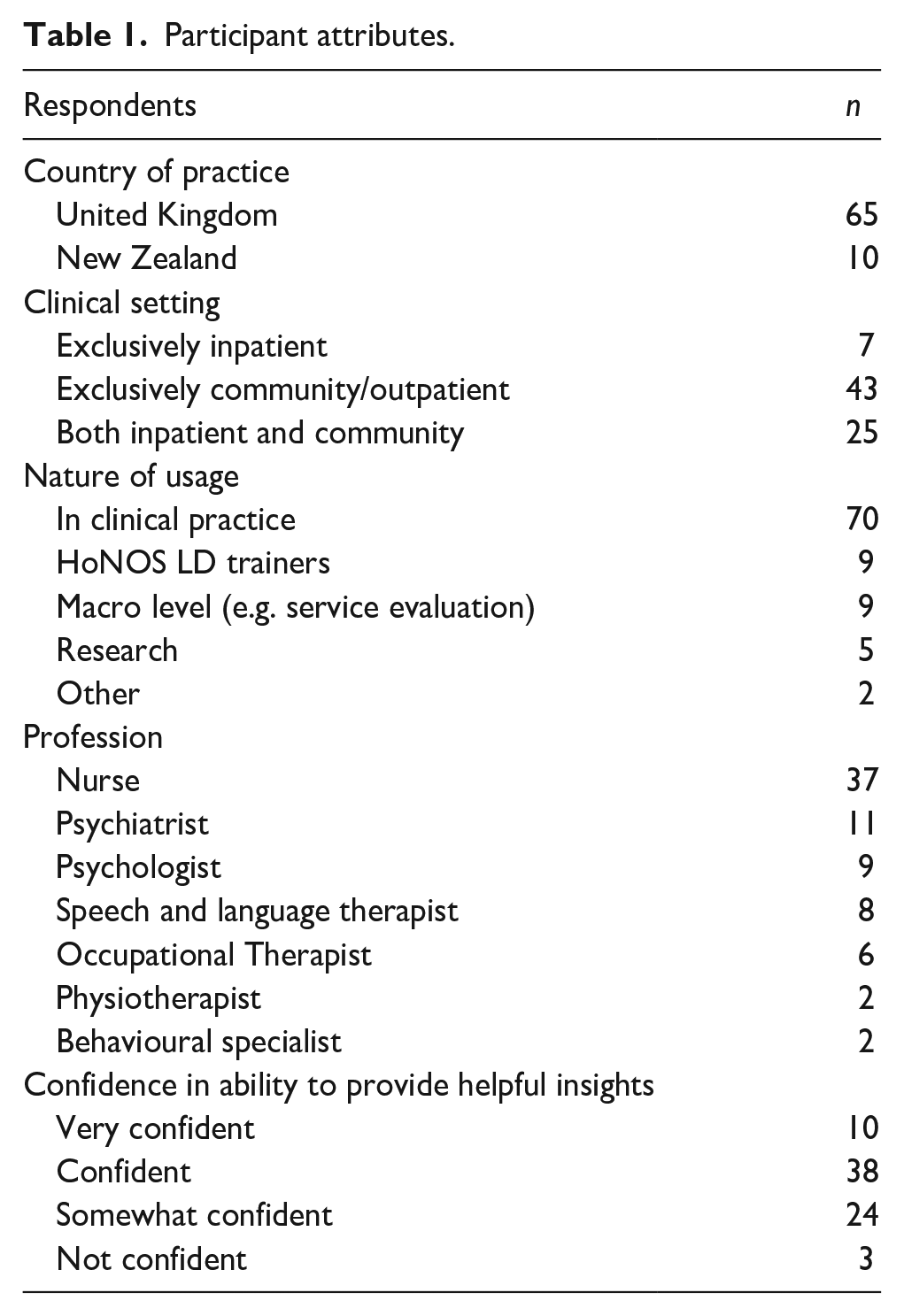
Nine survey respondents (12%) reportedly found HoNOS-LD extremely/very useful in their practice, 57 (76%) found it moderately/slightly useful and nine (12%) did not find it useful. On average, respondents used HoNOS-LD ratings to inform care 42.4% of the time one was completed (S.D. 33.5%). Their fitness for purpose ratings can be seen below in Table 2 where scale 10 (Problems with sleeping) and 13 (Seizures) were rated most favourably and scales 3 (Other mental and behavioural problems) and 15 (Activities of daily living outside the home) rated notably lower than the remainder. For each scale there was a significant negative correlation between the percentage of positive/very positive respondent ratings and the number of changes they proposed (r[17] = −.57, p = .016). However, there was no association between fitness for purpose and the actual number of changes made. In part this is due to the varying proportions of these suggestions that were deemed to be out of scope changes.
Survey responses to questions i–iv for each HoNOS-LD item.
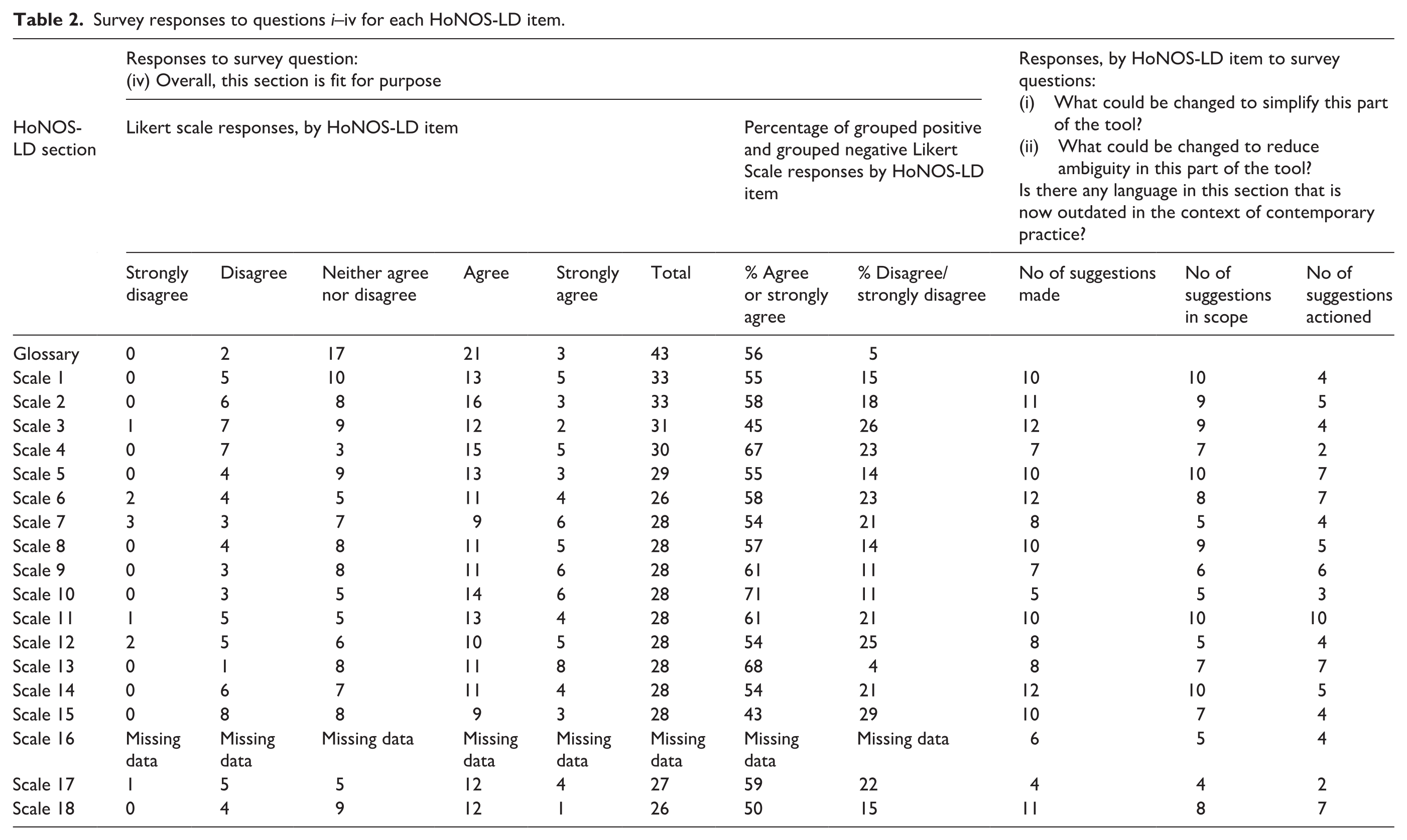
This information, together with the scale-by-scale qualitative feedback was used to inform the Advisory Board’s deliberations which, ultimately resulted in the changes outlined in Supplemental Information 3 (original HoNOS-LD wording included to aid comparison with the new HoNOS-ID). The Advisory Board meetings took place monthly of which there were 12 in total over the course of the review.
Discussion
This publication follows the review of the original (working age) HoNOS (James, Painter, et al., 2018) and HoNOS65+ (James, Buckingham, et al., 2018). These reviews were informed by each other prior to each version of the tool being finalized. However, the HoNOS-LD has some distinct and separate features and so, whilst some of the changes made to the HoNOS and the HoNOS 65+ were considered, the majority of the review was independent of previous changes.
The first survey question asked participants to identify areas of the tool requiring
In contrast, and perhaps as a result of this same brevity, numerous areas of
Survey respondents were also asked to identify
To further aid this, bullet points from the HoNOS 2018s over-arching instructions were utilized. (James, Painter, et al., 2018) Firstly, that the glossary contains examples of behaviours to be rated, rather than exhaustive lists. Secondly that ratings of 0 and 1 are generally not clinically significant, requiring no specific action other than possible monitoring for change, whereas ratings of two and above are regarded as clinically significant. Finally, that the person’s culture must be taken into account when rating all scales.
Limitations
Although the Advisory Board were purposively recruited for their significant expertise in the use of HoNOS-LD, and the survey respondents were drawn from a representative range of professional backgrounds that was more diverse than Roy et al.’s original study, (Roy et al., 2002) the overall sample size (n = 75) is limited in terms of the combined ID workforce of England and New Zealand. Also, because the online survey link was circulated via professional networks the response rate is unknown. However, there was a large amount of descriptive, open text responses from the survey which was sufficient to make significant changes across the scales.
As with the review of HoNOS (James, Painter, et al., 2018) and HoNOS65+ (James, Buckingham, et al., 2018), several potentially useful improvements were identified but ultimately rejected for falling outside the project’s scope. This was because they were deemed to constitute substantial changes, that would have resulted in a completely new instrument. Perhaps the most notable example of this was the implicit assumption in the tool that physical (restraint) interventions are always used appropriately.
The changes outlined in this paper are based on expert consensus alone. Given the original tool was designed as a Clinician Rated Outcome Measure (CROM) this is an acceptable first step however, as with the updated versions of HoNOS and HoNOS 65+, they now require empirical testing and to form part of a meaningful consultation with service users. However, undertaking such studies would require funding and preferably involvement from all countries that have heavily invested in the existing HoNOS-LD to date. This issue is being actively pursued by members of the Advisory Board. Furthermore, although these changes are intended to improve reliability and validity, they do not obviate the continued need for training in the use of the scales.
Conclusion
The HoNOS LD was found to have continued clinical utility but was in need of updating. The resulting HoNOS-ID addresses many of the participants’ suggestions, creating a measure more in keeping with contemporary ID practice. Service user consultation and further research (with a focus on practical application within different clinical settings) is now required to test these changes in preparation for introduction into the national datasets of England and New Zealand.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231175773 – Supplemental material for Review and update of the Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD)
Supplemental material, sj-docx-1-isp-10.1177_00207640231175773 for Review and update of the Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD) by Jon Painter, Nicola Adams, Barry Ingham, Michael James, Madiha Majid, Ashok Roy, Rohit Shankar and Mark Smith in International Journal of Social Psychiatry
Supplemental Material
sj-docx-2-isp-10.1177_00207640231175773 – Supplemental material for Review and update of the Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD)
Supplemental material, sj-docx-2-isp-10.1177_00207640231175773 for Review and update of the Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD) by Jon Painter, Nicola Adams, Barry Ingham, Michael James, Madiha Majid, Ashok Roy, Rohit Shankar and Mark Smith in International Journal of Social Psychiatry
Supplemental Material
sj-docx-3-isp-10.1177_00207640231175773 – Supplemental material for Review and update of the Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD)
Supplemental material, sj-docx-3-isp-10.1177_00207640231175773 for Review and update of the Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD) by Jon Painter, Nicola Adams, Barry Ingham, Michael James, Madiha Majid, Ashok Roy, Rohit Shankar and Mark Smith in International Journal of Social Psychiatry
Footnotes
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: All authors were members of the project’s Expert Advisory Board. AR is the original developer of the HoNOS LD. RS has received institutional and research support from LivaNova, GW pharma, UCB, Eisai, Veriton pharma, Averelle and Destin outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: MJ’s time on the project was funded by the Royal College of Psychiatrists.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.