
Abstract
Background:
A range of evidence for the effectiveness of one-to-one peer support in mental health services is emerging. Levels of engagement with peer support vary with limited studies showing few individual participant characteristics predicting engagement. Implementation factors that might predict engagement have not been considered.
Methods:
Data were analysed from the intervention arm of the ENRICH trial of one-to-one peer support for discharge from acute psychiatric inpatient care. Two outcomes were considered: (1) a measure of ‘engaged with peer worker’; (2) number of face-to-face contacts with peer worker post-discharge. Two sets of independent variables were analysed against each outcome: (1) pre-randomisation participant characteristics; (2) implementation factors measured pre-discharge. Analyses used logistic and zero-inflated negative binomial regression models according to outcome structure.
Results:
Data were analysed for 265 participants randomised to peer support who had a known peer worker. Non-heterosexual participants had increased odds of engaging with peer support compared to heterosexual participants, OR = 4.38 (95% CI: 1.13, 16.9, p = .032). Longer duration of first contact with peer worker (OR = 1.03, 95% CI: 1.00, 1.04, p < .001) and more relationship building activities in the first contact (OR = 1.4, 95% CI: 1.13, 1.85, p = .004) were associated with greater odds of engaging with peer support. Analysis of number of contacts post-discharge showed consistent findings.
Conclusions:
Implementation of peer support should include a focus on relationship building in the first session of peer support. The potential for peer support to break down barriers to accessing mental health services experienced by people from marginalised communities warrants further investigation.
Introduction
Peer support in state funded or regulated mental health services is often delivered one-to-one by peer workers; people with personal experiences of using mental health services, employed and trained to offer support to others receiving care for similar mental health difficulties. Qualitative research has consistently reported positive experiences of the impacts of peer support (Gidugu et al., 2015; Walker & Bryant, 2013). Evidence is mounting for the effectiveness of one-to-one peer support in mental health services, with a recent systematic review indicating that peer support can lead to modest but significant improvements in personal recovery (Standardised Mean Difference (SMD) of 0.22, 95% Confidence Internal (CI) (0.01, 0.42), based on 593 participants from three trials) and empowerment (SMD = 0.23, 95% CI 0.04, 0.42, 519 participants from four trials) (White, Foster et al., 2020). However, no significant effects were observed for hospitalisation, psychiatric symptoms, quality of life, satisfaction with services, social functioning, social network support or working alliance, and numbers of studies remain small and of variable quality (White, Foster et al., 2020). This mixed picture lacks clarity for policy makers and as a guide to implementing peer support into mental health services.
Data from recent trials have indicated a range of rates of engagement with peer support. In two trials of peer support for people at discharge from psychiatric hospital, 45.8% (22 of 48) (O’Connell et al., 2018) and 63% (40/63) (Rogers et al., 2016) of participants respectively took up a minimum of one session of peer support. In studies of community-based peer support, 72.4% (160/221) of participants took up at least three of the peer support sessions on offer in one trial (Johnson et al., 2018), with 75.4% (86/114) of participants taking up a least four sessions in another (Mahlke et al., 2017). Average number of sessions attended per participant as a proportion of maximum or target number of sessions on offer also varies, from 15.4% (mean of 6 out of a maximum of 39 on offer) in one of the hospital discharge trials (Rogers et al., 2016), to 46.9% (mean of 12.2/26) (Mahlke et al., 2017) and 70% (median of 7/10) (Johnson et al., 2018) in the community-based trials. With studies not reporting further analysis of these data, this variation alone warrants investigation.
There is limited literature exploring levels of engagement with peer support and outcome. In an analysis of service use data from people attending a peer-based recovery service for people with a diagnosis of substance use disorder, a positive association was observed between number of peer- supported follow-up sessions attended and recovery capital score (Ashford et al., 2021). A per-protocol analysis from a trial of a peer specialist intervention for people with mental illness and substance use disorders indicated that participants with high engagement with peer support (12 contacts or more) were more likely than control group participants to show positive change in psychiatric symptoms compared to participants with low engagement (Chinman et al., 2018). A small amount of research to date has explored factors that might predict levels of engagement with peer support. A study of peer support among homeless veterans with mental health conditions and substance use histories found that neither participant socio-demographic characteristics nor mental health and substance use severity were predictive of engagement (Ellison et al., 2016). In a randomised controlled trial of peer specialist services, also for homeless veterans, higher hope for the future, shorter period spent homeless prior to being offered peer support, higher severity of self-reported substance use symptoms and higher level of mental health service use were all associated with engagement with peer support (Chinman et al., 2019). These studies did not explore any association between how peer support was delivered and engagement.
Literature on the values and principles underpinning peer support is clear that choice and control over engaging with peer support is core to the distinctive nature of the peer support relationship (Gillard et al., 2017). If people choose not to engage or continue with peer support once they have been offered it, there remains a need to better understand how peer support might be offered in a way which is more engaging and therefore potentially more effective. This echoes a wider mental health literature indicating how strength of therapeutic relationship is predictive of the effectiveness of many mental health therapies and interventions (Goldsmith et al., 2015; Priebe & Mccabe, 2008). In addition, it has been argued that the peer-to-peer relationship should also be grounded in shared experiences of marginalisation related to community (including gender, ethnicity, sexual orientation, age and religion), especially where people are excluded from mental health services (Faulkner & Kalathil, 2012; Hope & Ali, 2019). Questions about potential association between outcomes and this ‘matching’ of peer workers and participants (Pfeiffer et al., 2011) remain unanswered.
Our study aims to address these questions in order to optimise engagement and, potentially, the outcomes of one-to-one peer support in mental health services.
Methods
We conducted a multisite, individually randomised controlled trial (ENRICH) of peer support for discharge from inpatient to community mental health care, with the full methods described elsewhere (Gillard et al., 2020). The trial recruited 590 participants who were currently psychiatric inpatients with a previous recent admission, randomising half (n = 294) to one-to-one peer support for discharge in addition to care as usual (CAU; follow-up from community mental health services post-discharge), and half (n = 296) to CAU only. Participants allocated to peer support were offered at least one face-to-face contact with a designated peer worker while still in hospital, and then 10 weekly contacts followed by three fortnightly contacts post-discharge. Peer workers had all completed manualised training and provided flexible support focused on building individual strengths and connection to community (Gillard et al., 2020; Marks et al., 2021).
Participants offered peer support were no less likely to be readmitted to inpatient care in the year post-discharge – the primary outcome – compared to those in the CAU group (relative risk (RR) 0.97 95% CI 0.82, 1.14; p = .68) (Gillard et al., 2022). A Complier Average Causal Effect (CACE) analysis (Dunn et al., 2015) compared participants who had had at least two contacts with their peer worker, at least one of which was in the community post-discharge, with a subgroup of similar participants in the CAU group (identified using all baseline participant data). These criteria were developed with the study’s Lived Experience Advisory Panel – people with direct experience of peer support – and reflected the principle of choice in peer support (i.e. choosing to meet away from the restrictive environment of the ward) (Goldsmith et al., 2019). We found that participants who met these criteria were significantly less likely to be readmitted in the year post-discharge than similar participants not offered peer support (RR 0.88 95% CI 0.76, 0.99) (Gillard et al., 2022).
This association between amount of contact with peer support and outcome emphasises the importance of better understanding the process of engagement with peer support. We also found that Black participants who were offered peer support had lower odds of being admitted to hospital compared to control (odds ratio (OR) 0.40 (95% CI 0.17, 0.94)) than were participants of any other ethnicity (OR 1.12 (95% CI 0.77, 1.63)); interaction p = .031) (Gillard et al., 2022). While we did not match participants to peer workers by ethnicity, it is of interest to explore whether incidental matching was predictive of engagement. This paper reports two analyses which aim to identify pre-randomisation and pre-discharge predictors of engagement with peer support.
The ENRICH study was approved by the UK National Research Ethics Service, Research Ethics Committee London - London Bridge on 10 May 2016, reference number 16/LO/0470.
Participants
Our sample were all participants in the ENRICH trial randomised to peer support who had a known allocated peer worker.
Data
Two dependent variables were examined: (1) ‘engaged with peer worker’, defined in the CACE analysis (Gillard et al., 2022) as having had at least two contacts with the allocated peer worker, one of which was in the community following discharge; (2) number of face-to-face contacts with peer worker post-discharge. Data were attained from structured questionnaires and standardised measures collected at a baseline interview prior to randomisation, electronic patient record extracted by site information management personnel for the 12 months pre-index admission, and a contact log completed by peer workers using an online survey after each attempted contact.
At baseline socio-demographic data for each participant were collected, and standardised assessments made of social inclusion using the Social Outcomes Index (SIX) (Priebe et al., 2008), severity of symptoms using the Brief Psychiatric Rating Scale (BPRS) (Overall & Gorham, 1962), hope for the future using the Herth Hope Index (Herth, 1992), treatment stigma using the stigma subscale of the Barriers to Care Evaluation (BACE-3) (Clement et al., 2012), and internalised stigma using the Questionnaire on Anticipated Discrimination (QUAD) (Gabbidon et al., 2013). The QUAD scale produces two measures of anticipated stigma, severity (mean of all items) and count of life areas where stigma has been anticipated. Number of psychiatric admissions in the year prior to index admission, and type of index admission were extracted from patient records. Using the contact log, peer workers indicated which of a list of activities were covered in each contact. Based on our theoretical model (Gillard et al., 2015), we calculated a variable ‘relationship building’ as a count of the activities ‘using your own lived experience’, ‘learning from the lived experience of the person you are supporting’, ‘negotiating (or renegotiating) the boundaries in your relationship’, ‘accompanying or being alongside the person you are supporting’ and ‘using active listening skills’ recorded as having taken place in the first peer support contact (range of 0–5).
Pre-randomisation predictor variables were; index admission type (compulsory/voluntary), sexual orientation (heterosexual/not heterosexual/declined to answer), gender (male/female), diagnostic group (psychosis/personality disorder/other non-psychotic), ethnicity (Black/Other), age (years), social inclusion (SIX), severity of symptoms (BPRS), hope (HHI), number of admissions in year prior to index admission, treatment stigma (BACE-3), severity of anticipated stigma and count of life areas of stigma (QUAD). Ethnicity data were dichotomised as any Black ethnicity and any other ethnicity because being of Black ethnicity has been shown to be a significant predictor of psychiatric readmission (Halvorsrud et al., 2018) (our primary outcome) and because, as noted above, Black participants offered peer support were significantly less likely to be readmitted compared to control than participants of any other ethnicity (Gillard et al., 2022).
Pre-discharge predictor variables were: same gender, same age (within 18–35, 36+ age groups), same ethnicity (within Asian, Black, White, other ethnic groups) and same diagnosis (within diagnostic groups as above) as allocated peer worker; relationship building at first contact with peer worker (equal to 0 if no contact with peer worker); length of first contact with peer worker (minutes, equal to 0 if no contact with peer worker); days between recruitment and discharge; whether the participant had two or more peer worker contacts pre-discharge.
Statistical analysis
Logistic regression was used to model the relationship between the two groups of predictor variables and the ‘engaged with peer support’ dependent variable. Results are reported with odds ratios (OR) and 95% confidence interval. Zero-inflated negative binomial (ZINB) regression was used to model the relationship between the two groups of predictor variables and the number of face-to-face contacts post-discharge. The dependent variable had a high proportion of zero values (zero-inflated) – participants who, for a range of reasons, might have either chosen or been unable to continue to meet their peer worker post-discharge – and a skewed distribution with a few very high values (over-dispersed). ZINB regression models the two parts of the distribution using two linked models; the first estimates the odds of a zero count (zero face-to-face contacts post-discharge) using logistic regression reported with ORs (odds of zero contacts), the second estimates the non-zero counts (number of face-to-face contacts post-discharge) using negative binomial regression reported by incidence rate ratios (IRR), both with 95% bootstrapped percentile confidence limits (BPCL).
A sensitivity analysis was conducted for the pre-randomisation predictors models due to missing data and a high correlation between two of the predictors. Six was removed as this variable had the most missing data, and the count of life areas QUAD variable was removed as the two versions of the scale, mean and count of life areas were highly correlated, r = .73. Analysis was conducted using R v4.10.2 (SAMHSA, 2021).
Results
Five hundred ninety participants were randomised into the ENRICH trial of whom 294 were allocated to peer support. Three of these participants withdrew their data. Of the remainder, 265 had a known peer worker. The 26 participants allocated to peer support for whom peer worker was not known were largely at one study site where reporting was incomplete.
Descriptive data
Summary statistics of the sample are reported in Table 1. In brief, the sample had a mean age of 39.7 years (SD = 14.0) ranging from 18 to 74. There were similar numbers of male (125, 48.3%) and female (133, 51.4%) participants, one identifying as transgender. Most of the sample were White, 144/257 (56%), 43/257 (16.7%) were Black. Two hundred seventeen participants (81.9%) were heterosexual. The most common diagnosis was psychosis, with 118 participants (44.5%). Approximately half of participants (126, 47.5%) had been admitted compulsorily under the Mental Health Act. In the year prior to index admission participants had a median of one psychiatric admission and 18 community mental health team contacts
Sample descriptive statistics.
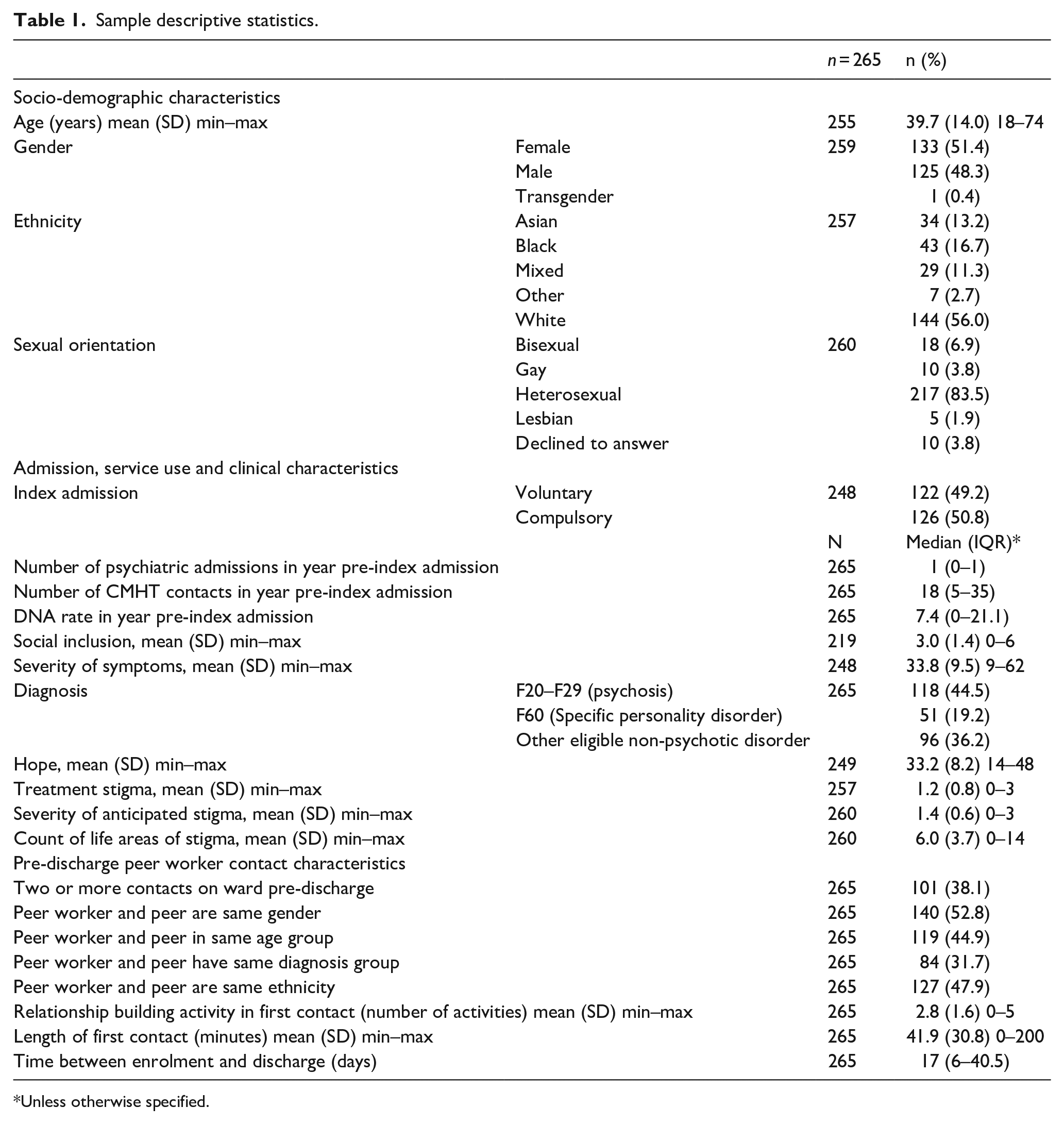
Unless otherwise specified.
The median duration between recruitment and discharge was 17 days (IQR 6–40.5). One hundred one participants (38.1%) had at least two peer worker contacts on the ward. The mean length of the first contact was 42 minutes ranging from 0 to 200 minutes. Variation in the number of relationship-building activities conducted in the first contact is evident. The extent to which participants and peer workers had the same demographic characteristics ranged from 31.7% to 52.8% across characteristics.
Engagement with peer support
Sixty-two percent, 163/265 of participants received peer support as defined as having had at least two peer worker meetings, at least one of which was in the community following discharge. The mean number of face-to-face contacts was 6.2 (median = 5.0, SD = 5.3, IQR = 1.0–10.5) and ranged from 0 to 22 contacts. For the 163 who engaged with peer support their mean number of face-to-face contacts was 9.1 (median = 9; SD = 4.7) ranging from 2 to 22. Post-discharge they had a mean of 7.1 face-to-face contacts (median = 7; SD = 4.0; IQR = 1–14) ranging from 1 to 15. Ninety-one participants (34.3% of the sample) had zero face-to-face contacts post-discharge. The mean number of face-to-face contacts post-discharge for those with at least one was 6.7 (median = 7.0; SD = 4.1; IQR = 3–10).
Pre-randomisation predictors of engagement
The only demographic characteristic significantly predictive of engaging with peer working was sexual orientation (seeTable 2), non-heterosexual participants having 4.4 times the odds of engaging with peer support than heterosexual participants, OR = 4.38 (95% CI: 1.13, 16.9, p = .032). There was weaker evidence that sexual orientation was also associated with not having any contacts post-discharge, OR = 0.72 (95% CI: 0.00, 25.00, p = .062), non-heterosexual participants having lower odds of having zero contacts post-discharge than heterosexual participants. Sexual orientation was not associated with the number of contacts post-discharge assuming participants had at least one contact. There was a non-significant finding that Black participants had lower odds of engaging with their peer worker, OR = 0.5 (95% CI: 0.23, 1.22, p = .134). There was weak evidence regarding age, p = .074, that for those participants who had at least one contact post-discharge that older age was associated with more contacts, IRR = 1.01 (95% CI: 1.00, 1.02).
Pre-randomisation predictors of engagement.
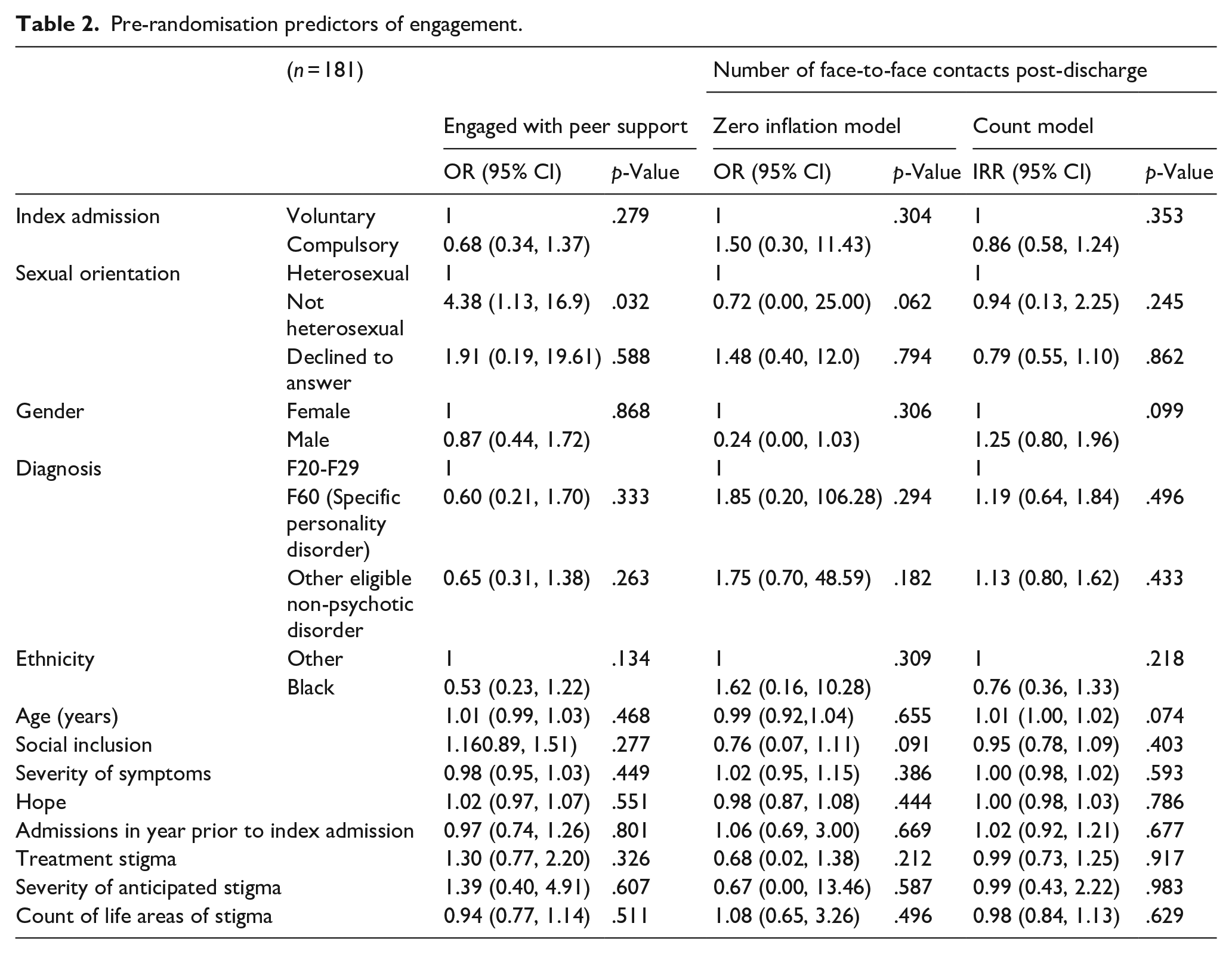
The models in Table 2 were refitted without SIX and count of life areas of stigma (QUAD) in line with pre-specified sensitivity analyses. This increased the sample size to 211 participants. Results were consistent with the reported models in Table 2. Little’s test was non-significant, χ2 = 91.9, p = .981, indicating that there was no evidence that missing data were not missing completely at random and therefore complete-case analysis is appropriate.
Pre-discharge predictors of engagement
Table 3 reports the results of the regression models exploring predictors relevant to the beginning of the peer support relationship. A shorter time between recruitment and discharge (OR = 0.99, 95% CI: 0.99, 1.00, p = .002), a longer duration of first contact with peer worker (OR = 1.03, 95% CI: 1.00, 1.04, p < .001) and more relationship building activities in the first contact (OR = 1.4, 95% CI: 1.13, 1.85, p = .004) were all associated with greater odds of ‘engaging with peer support’.
Pre-discharge predictors of engagement.
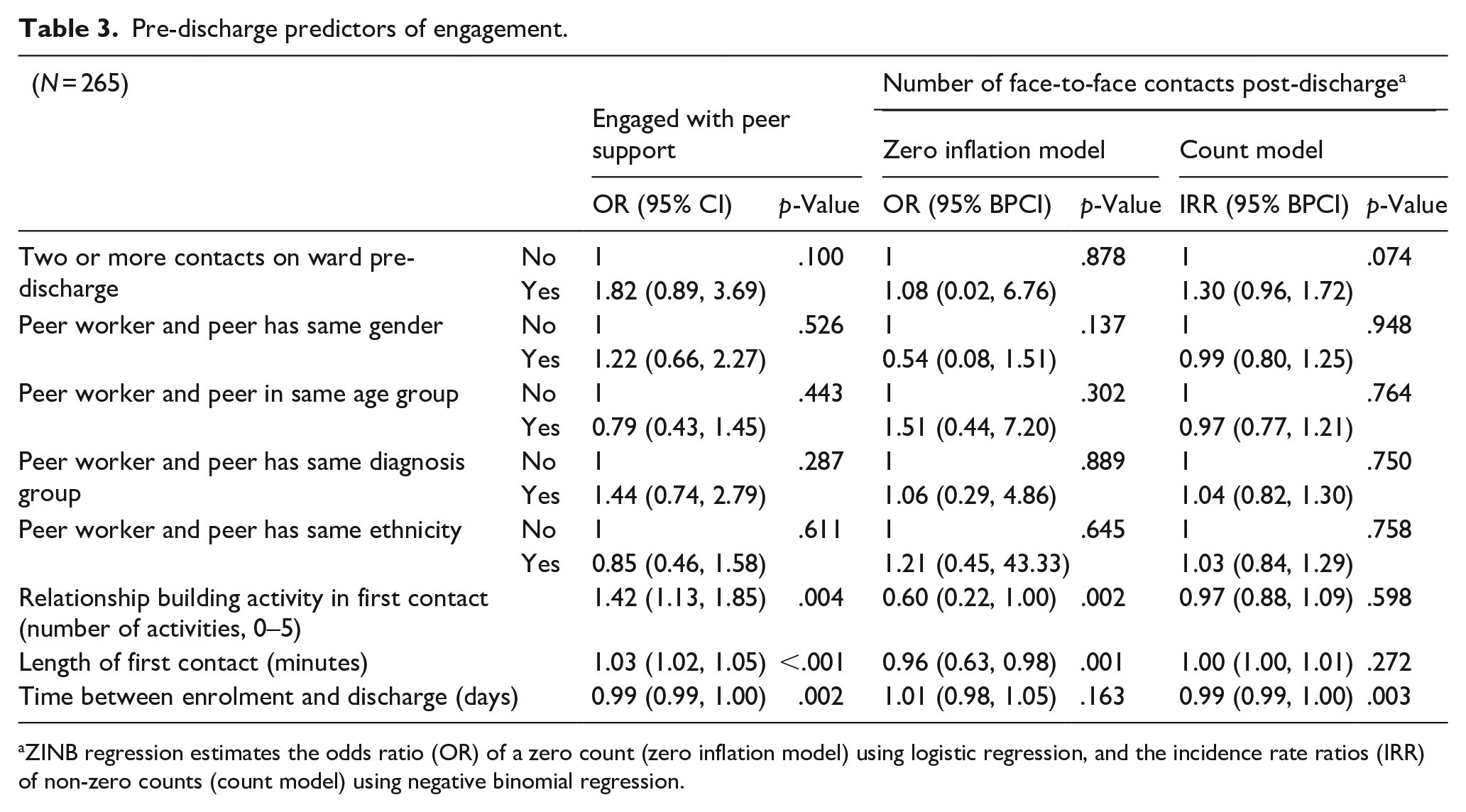
ZINB regression estimates the odds ratio (OR) of a zero count (zero inflation model) using logistic regression, and the incidence rate ratios (IRR) of non-zero counts (count model) using negative binomial regression.
The two parts of the ZINB regression model indicated complementary results. More activities based on relationship building during the first contact and a longer length of first contact were associated with lower odds of having zero contacts post-discharge, OR = 0.59 (95% BPCI: 0.07, 1.09, p = .001) and OR = 0.96 (95% BPCI: 0.01, 0.98, p = .001) respectively. For those participants with at least one contact, having had more days between recruitment and discharge was associated with a lower number of face-to-face contact post-discharge, IRR = 0.99 (95% BPCI: 0.99, 1.00, p = .003).
Discussion
This study aimed to identify whether pre-randomisation (participant characteristic) or pre-discharge variables (peer support characteristics) were predictive of either ongoing engagement with peer support or number of peer support sessions post-discharge. We observed little association between participant characteristics and engagement with peer support. Participants who identified as non-heterosexual had significantly higher odds of engaging with peer support post-discharge than heterosexual participants. Notwithstanding low numbers of participants in this group, we note a lack of research explicitly exploring mental health peer support among LGBTQ+ people (Faulkner & Kalathil, 2012). Other research has indicated that people who identify as LGBTQ+ are reluctant to disclose their sexual orientation to healthcare providers (including primary care and mental healthcare providers), with evidence suggesting that LGBTQ+ people can continue to feel pathologised because of their sexuality (Bachmann & Gooch, 2018), and as a result are less likely than heterosexual people to access care that meets their needs (Durso & Meyer, 2013; Salway et al., 2018). We also note that Black participants might have been less likely to engage with peer support, while still benefitting more from the intervention than people of other ethnicity (Gillard et al., 2022). This could reflect heterogeneity resulting from grouping together Black ethnicities, but suggests a need to investigate further the experiences and understandings of peer support in different cultural contexts. Other research has indicated that peer support offers a different sort of relationship to a typical patient-clinician relationship, enabling disclosure more generally (Gillard et al., 2015). As such our findings raise the possibility that people who experience marginalisation in mental health care might find it easier to engage with, and/or open up to peer workers than to other mental healthcare providers.
Findings from elsewhere that higher baseline hope scores were associated with a greater level of subsequent engagement in peer support (Chinman et al., 2019) were not replicated in our study. Research has indicated a positive association between hope and intention to seek both informal and formal psychological help (McDermott et al., 2017). We note that mean values for hope were lower in the inpatient population in our study than they were for participants in Chinman et al. (2019) community-based study, that relative lack of optimism in our sample perhaps accounting for some lack of enthusiasm for peer support, possibly indicating that the timing of the offer of peer support was challenging for this group of people.
We observed more associations between pre-discharge characteristics of peer support, and engagement with peer support post-discharge. Longer first contact with peer worker was associated with engagement with peer support and, correspondingly, with less likelihood of having no contacts post-discharge. A higher number of relationship-building activities in that first contact was similarly associated with ongoing engagement with peer support, suggesting that a first session of peer support with a clear focus on relationship building may lead to improved engagement and potentially better outcomes. Our earlier research was indicative of the importance of relationship building as a peer support mechanism (Gillard et al., 2015, 2017). This informed an emphasis on relationship work in peer worker training and in the supervision of peer workers by an experienced peer, as specified in the intervention handbook for the trial (Marks et al., 2021). The importance of role specific training for peer workers has been widely noted (Simpson et al., 2014; Tse et al., 2014).
Interestingly, we found no association between having multiple contacts with the peer worker pre-discharge and ongoing engagement, while a longer duration between recruitment into the study and discharge was associated with lower odds of remaining engaged with peer support and fewer contacts in total post-discharge. This felt counter-intuitive as more opportunities to meet with the peer worker before discharge might be assumed to enhance relationship building. It is possible that this longer length of stay on the ward reflected a frustrating period of delayed discharge, or a prolonged period of acute mental distress for those individuals, with associated challenges to building a relationship with the peer worker.
We also found no association between matching of participant to peer worker (incidental rather than planned in our study) – in terms of either age, gender, ethnicity or diagnostic group – and engagement with peer support. This is despite research suggesting that peer identification in mental health encapsulates wider aspects of shared identity beyond experiences of mental distress (Faulkner & Kalathil, 2012; Hope & Ali, 2019), and studies reporting peer support targetting specific clinical groups (Chien et al., 2019; Pfeiffer et al., 2011). As such we saw people engaging in peer support ‘across difference’, again raising the possibility that there is something about the quality of the peer-to-peer relationship – perhaps in contrast to the patient-clinician relationship – that encourages ongoing engagement independent of the identities of the individuals involved.
Strengths and limitations
Strengths of this study were our a priori identification of potential predictor variables grounded in empirical and theoretical research in the field, and our ‘engaged in peer support’ criteria we developed with our lived experience advisory group. Confidence in our findings was enhanced by the complementarity of our analyses; pre-discharge predictors of being engaged with peer support were all supported by either the zero-inflation or count model of number of peer support contacts post-discharge.
Missing data in some baseline variables was a potential weakness of the study, although sensitivity analysis indicated that findings remained robust when measures with missing and highly correlated variables were removed. Low numbers of participants in some groups, particularly, for example, participants identifying as lesbian, gay, or bisexual, suggest that some of our estimates should be treated with caution and seen as avenues for further study, rather than definitive findings. We also note that the socio-demographic categorisation we used for sexual orientation and ethnicity were incomplete and limited our analyses. Incomplete contact logs by peer workers at one site also potentially undermined reliability of findings. Finally, this was a quantitative study; qualitative research exploring people’s experiences and views on engaging with peer support would help interpret these findings.
Implications for practice
Given our findings around an association between length and quality of first peer support contact and ongoing engagement with peer support, a focus on relationship building in peer worker training, supervision and guidance for the crucial first session should inform peer support practice in mental health services going forward. However, our findings also suggest that leaving inpatient care might be a difficult time for people to build and sustain a new relationship. The approach to peer support we developed was very flexible, encouraging peer worker and participant to agree how they worked together, choosing from a range of tools (Gillard et al., 2020; Marks et al., 2021). It is possible that people might have benefitted from a more structured and explicitly supportive approach, including a more structured first session to support relationship building, introducing flexibility as the relationship developed.
In addition, our findings with respect to sexual orientation, ethnicity and the lack of association between incidental matching and engagement suggest that peer support has the potential to work ‘across difference’ (limitations in our data notwithstanding). These findings raise the possibility that peer support might offer additional benefits to people who may feel marginalised, unheard or discriminated against by mental health services. Mental health services struggle to address inequalities in access, experience and outcomes of care for people from marginalised communities (Halvorsrud et al., 2018), and as such, support and training for peer workers to work with diversity and break down barriers to communication and relationship building in mental health care would seem to offer an opportunity to address, at least in part, historic inequities in care.
Footnotes
Correction (February 2023):
This article has been updated with the new author Mike Lucock in the author’s list since its original publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the UK National Institute for Health Research (NIHR), Programme Grants for Applied Research funding programme (grant number RP-PG-1212-20019). This paper presents independent research funded by NIHR. The views expressed are those of the authors and not necessarily those of the UK National Health Service (NHS), the NIHR or the Department of Health and Social Care.