
Abstract
Background:
According to federal and cantonal law, persons with an acute mental illness can be admitted to a psychiatric hospital or another suitable institution against their will, when other therapeutic options are not available or have been exhausted. In the canton of Basel-Stadt, this is the responsibility of public health officers employed by the division of Social Medicine of the cantonal Health Department.
Aims:
This study aims to elucidate which factors influence the decision-making of public health officers regarding compulsory admissions over the period from September 2013 to April 2022 in the canton of Basel-Stadt.
Method:
Leveraging comprehensive clinical data from the health department of the canton Basel-Stadt (N = 5,′550), we estimated a mixed effects logistic regression model to identify factors contributing to the decision of public-health officers to compulsorily admit patients, while controlling for potential clustering effects among public health officers.
Results:
The risk for compulsory admissions was most strongly predicted by the presence of potential self-harm. In comparison, while being a strong predictor, potential harm to others played a considerably lesser role. Furthermore, psychiatric syndrome, previous compulsory admissions, and the specific context of evaluation were significant predictors. Finally, we found no meaningful personal bias among public health officers.
Conclusion:
The results suggest that public health officers’ decision-making regarding compulsory admissions focuses on preventing self-harm and, to a lesser degree, harm to others. This indicates that such measures are only used as a measure of last resort, which is in line with current evidence regarding the detrimental effects of compulsory measures on treatment outcomes in psychiatry. Our findings suggest that all relevant stakeholders, including the police, share this perspective. Decision-making regarding compulsory admissions was mostly free of personal biases, suggesting adherence to shared professional standards by public health officers.
Introduction
Potentially harmful effects of compulsory measures in psychiatry are well known and described in the literature, namely increased stigmatization (Sowislo, Gonet-Wirz et al., 2017; Sowislo, Lange et al., 2017), trauma (Steinert et al., 2013), poorer patient-therapist relationships (Theodoridou et al., 2012) and adherence to therapy (Deutschenbaur et al., 2014). Given the coercive nature of compulsory admissions, they should be used only as a last resort when less severe measures (i.e. voluntary admission to a suitable institution or outpatient treatment) have been exhausted and have not yielded the desired outcome. In Switzerland, the criteria for issuing a compulsory admission are laid down in federal civil law (articles 426–439 of the Swiss Civil Code) (Swiss Confederation, 1907) as well as in cantonal laws (in the canton of Basel-Stadt in the Law for the Protection of Children and Adults (Kanton Basel-Stadt, 2012) and the Psychiatry Law (Kanton Basel-Stadt, 1996)). Art. 426 of the Swiss Civil Code defines the preconditions for issuing compulsory admissions: the presence of a mental disorder or mental disability or severe neglect, the existence of an appropriate institution, and no other means of care. In addition, the burden that the patient places on family members and third parties and their protection must be taken into account (Swiss Confederation, 1907). Although not explicitly mentioned in the law as a precondition for compulsory admissions, additional criteria are applied in the assessment for or against compulsory admission. These criteria are self-endangering behavior and behavior endangering others (Gesundheitsdepartment des Kantons Basel-Stadt, 2022).
The regulations on compulsory admissions vary considerably from canton to canton: in some cantons, all physicians with a professional license may order compulsory admissions, while in other cantons, this authority is restricted to certain physicians (Hermann et al., 2018) or held by the cantonal child and adult protection authority (KESB). This could partially explain the high variability in cantonal admission rates (Christen & Christen, 2005; Kuhl, 2008; Schuler et al., 2018, 2020). Basel-Stadt is the only canton where admissions for persons 18 or older are exclusively ordered by the public health officers employed by the division of Social Medicine of the cantonal Health Department, based on an in-person assessment. The compulsory admission to a psychiatric institution is valid for 6 weeks. However, the psychiatric institution may suspend it as soon as the patient no longer poses a danger to himself or others. Compulsory hospitalization beyond this period (e.g. persons with long-term placement in a nursing home) must be ordered by the cantonal child and adult protection authority (KESB) (Kanton Basel-Stadt, 1996, 2012).
Several studies examined risk factors associated with compulsory admissions, showing a heterogeneous picture: while some studies found an association with male gender (Cougnard et al., 2004; Riecher et al., 1991; Umama-Agada et al., 2018), increasing age (Hotzy et al., 2019; Hustoft et al., 2013; Juckel & Haußleiter, 2015) and being married (Umama-Agada et al., 2018; van der Post et al., 2012), other studies found female, younger (Chang et al., 2013; Eytan et al., 2013) and unmarried patients (Juckel & Haußleiter, 2015) to be at higher risk for compulsory admissions. Presence of schizophrenia or psychotic disorders (Cougnard et al., 2004; Hotzy et al., 2019; Juckel & Haußleiter, 2015; Riecher et al., 1991; Silva et al., 2018; Umama-Agada et al., 2018), previous involuntary admissions (Lay et al., 2019; Oliva et al., 2019; Silva et al., 2018; van der Post et al., 2009), ethnicity (Davies et al., 1996; de Wit et al., 2012; Hustoft et al., 2013; Terhune et al., 2022) and admittance during nighttime or weekend hours (Arnold et al., 2019; Hustoft et al., 2013; Juckel & Haußleiter, 2015) were more consistent risk factors across several studies. However, a recent systematic review and meta-analysis examining compulsory admissions in the UK and internationally showed higher risks for BAME (Black, Asian, and minority ethnic groups) and migrant groups to be compulsorily admitted compared to white ethnic groups, with odds ratios ranging from 2.53 for Black Caribbean patients to 1.33 for South Asian patients (Barnett et al., 2019). Another recent systematic review and meta-analysis by Walker et al. (2019) examining clinical and social factors associated with compulsory admissions showed the most substantial risks for the presence of a psychotic disorder and previous compulsory admissions (odds ratios > 2) and moderate risks for male gender, single marital status, presence of a bipolar disorder, unemployment and receiving welfare benefits (odds ratios ranging from 1.23 to 1.71). While not included in the meta-analysis, police involvement in admission and perceived risk to others were suggested as risk factors using narrative synthesis (Walker et al., 2019).
This study leverages a unique representative sample, covering all assessments by public health officers regarding compulsory admissions from September 2013 to April 2022 in the canton of Basel-Stadt. In contrast to the available literature, this also includes persons who did not meet the threshold for admission against their will and subsequently did not enter inpatient treatment. This allows us to directly study the factors governing public health officers’ decision-making regarding compulsory admission instead of relying on group comparisons from hospital records based on treatment status (voluntary vs. involuntary). Furthermore, by employing a mixed-effects logistic regression model, our study can also capture the extent to which personal biases might affect decision-making.
Methods
Data
For every assessment for compulsory admission, the responsible public health officer collects the following information: personal data (first and last name, date of birth), gender, responsible public health officer, and other persons involved during the evaluation (e.g. emergency psychiatrist, police officer, or social services of the police), date and duration of the evaluation, suspected syndrome category at the time of admission (dementia or organic disease, depressive syndrome, manic syndrome, personality disorder, schizophrenia or other psychotic disorder, addictive disorder), the decision by public health officer (compulsory admission, voluntary admission, no admission, consultation only), justification for the decision (self-endangering behavior or behavior endangering others, intolerable behavior to others, state of neglect), place of evaluation (e.g. hospital, police station, apartment, etc.). Public health officers could state more than one justification per case. Comprehensive electronic records of the abovementioned information have been available since September 2013. Public health officers come from various medical backgrounds other than psychiatry and do not make a formal mental-health diagnosis during their assessment. Instead, they categorize each case into broader syndrome categories.
The electronic records of the Health Department comprised 7,467 entries. We included on-site evaluations by public health officers for patients 18 years or older in our descriptive analyses. We therefore excluded telephone inquiries (n = 1,817), consultations only (n = 59), and persons younger than 18 years (n = 9). The final dataset for descriptive analyses thus consisted of 5,582 entries. For logistic regression modeling, we further excluded cases with missing information regarding age (n = 12), place of evaluation (n = 19) and duration of evaluation (n = 1). The final dataset for logistic regression analyses thus comprised 5,550 entries. Cases were divided into two groups: compulsory admission versus no compulsory admission (i.e. no subsequent in-patient treatment). The compulsory admission group also includes patients who formally entered the psychiatric clinic voluntarily after evaluation by a public health officer for compulsory admission. Even though, strictly speaking, these cases do not represent compulsory admissions, we believe it is appropriate to combine these two groups since we cannot rule out that their decision to receive in-patient care was influenced by the evaluation and could be seen as the effect of informal coercion.
The local ethics committee approved this study (Ethikkommission Nordwest- und Zentralschweiz, EKNZ 287-13/PB_2020_00029).
Statistical analysis
All statistical analyses were conducted using the R statistical package (version 4.1.2) (R Core Team, 2021) and the Integrated Development Environment (IDE) for R, RStudio (version 2021.09.0) (Studio Team, 2021).
We used descriptive statistics using the gtsummary package (Sjoberg et al., 2021) for comparing the groups with and without compulsory admissions. We performed univariate analyses using Pearson’s Chi-squared test for categorical variables and the Wilcoxon rank sum test for the continuous variable age.
Further, we estimated a mixed-effects logistic regression model to identify factors associated with the decision of public health officers to admit patients to psychiatric care against their will. Compulsory admission (yes vs. no) was the binary response variable. Syndrome, sex, age group, self-endangering behavior, behavior endangering others, intolerable behavior to others, state of neglect, number of previous compulsory admissions, place of evaluation, presence of police, presence of police social services, presence of a physician, presence of emergency psychiatrist, presence of psychiatrist other than the emergency psychiatrist, canton of residence, duration and time of evaluation were the predictors. Notably, the estimation of a mixed-effects logistic regression model includes random effects estimates for the evaluating public health officers. This allows us to measure to which degree decision-making might have been impacted by personal biases toward admission against the patient’s will. This part of the analysis was performed with the glmer function from the lme4 package (Bates et al., 2015) and the tidy function from the broom.mixed package (Bolker & Robinson, 2022) for computing confidence intervals and p-values. Goodness-of-fit was calculated using the r2_nakagawa function (as described by Nakagawa and Schielzeth (2013)) from the performance package (Lüdecke et al., 2021) and the icc_function (intraclass correlation) from the same package (Lüdecke et al., 2021) to test for clustering among public health officers.
Finally, to ensure the robustness of our findings, we performed sensitivity analyses. First, we repeated the above-described analysis but excluded the 243 cases who formally were voluntarily admitted after evaluation. Second, we performed a fixed-effects logistic regression with the same data. The level of statistical significance was set at p ⩽ .05.
Results
Descriptive analyses of on-site evaluations and compulsory admissions over time
The baseline characteristics are shown in Table 1. Of the 5,582 cases in our study, 4,409 were admitted against their will (79%). They were more often female (52%) and slightly older (median age 50 years) than patients who were not admitted to an institution (47% female, median age 48 years). In addition, they presented more often with the following syndromes: schizophrenia and psychotic disorders (40% vs. 21%) and dementia and organic disorders (19% vs. 12%). In contrast, personality disorders, addictive disorders, and affective disorders were more frequent in the group with no compulsory admissions (18% vs. 9%, 13% vs. 9%, and 20% vs. 19%, respectively). Self-endangering behavior was almost always present in compulsorily admitted patients (94%), whereas this proportion was still 54% in the group with no compulsory admissions. The criteria behavior endangering others, intolerable behavior toward others and state of neglect were all more frequently documented in compulsorily admitted patients (37% vs. 18%, 32% vs. 19%, and 11% vs. 6%, respectively). Further factors associated with compulsory admissions compared to the group with no admissions were increasing numbers of previous compulsory admissions and the presence of a psychiatrist or physician. Interestingly, longer duration of evaluations and evaluations outside office hours were more often represented in the group in which no compulsory admission was ordered. In univariate analyses, differences in all the variables mentioned above were statistically significant (Table 1).
Baseline characteristics, compulsorily admitted patients versus patients with no admission, September 2013 to April 2022.
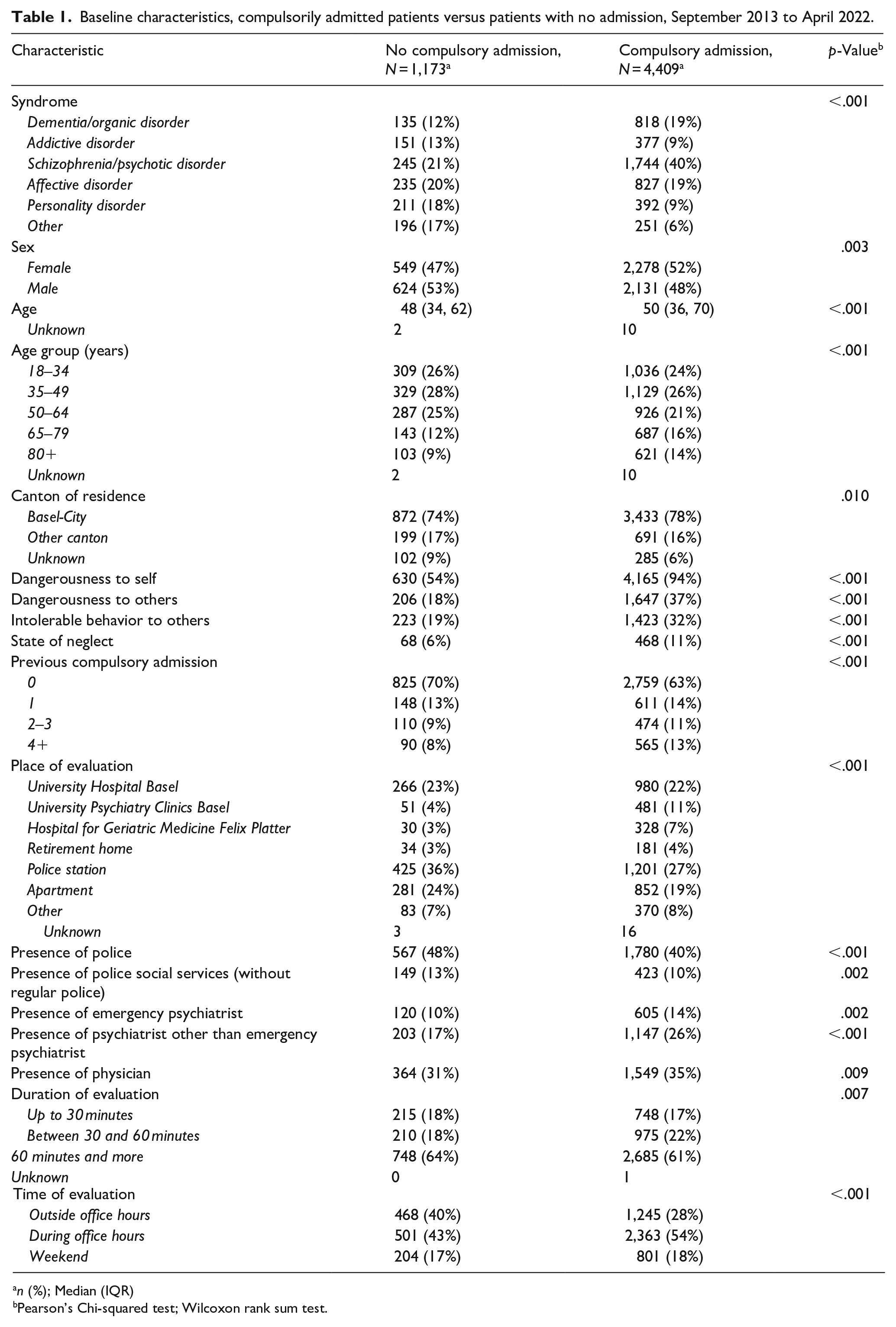
n (%); Median (IQR)
Pearson’s Chi-squared test; Wilcoxon rank sum test.
Logistic regression modeling
The results of the mixed-effects logistic regression analysis from September 2013 to April 2022 are presented in Table 2. This model explained 49.9% of the variance regarding the decision for or against compulsory admissions (conditional Nakagawa R2 = 0.499).
Mixed-effects logistic regression (random intercepts), considering the period September 2013 to April 2022. Individual public health officers performing the assessment were included as random effects.
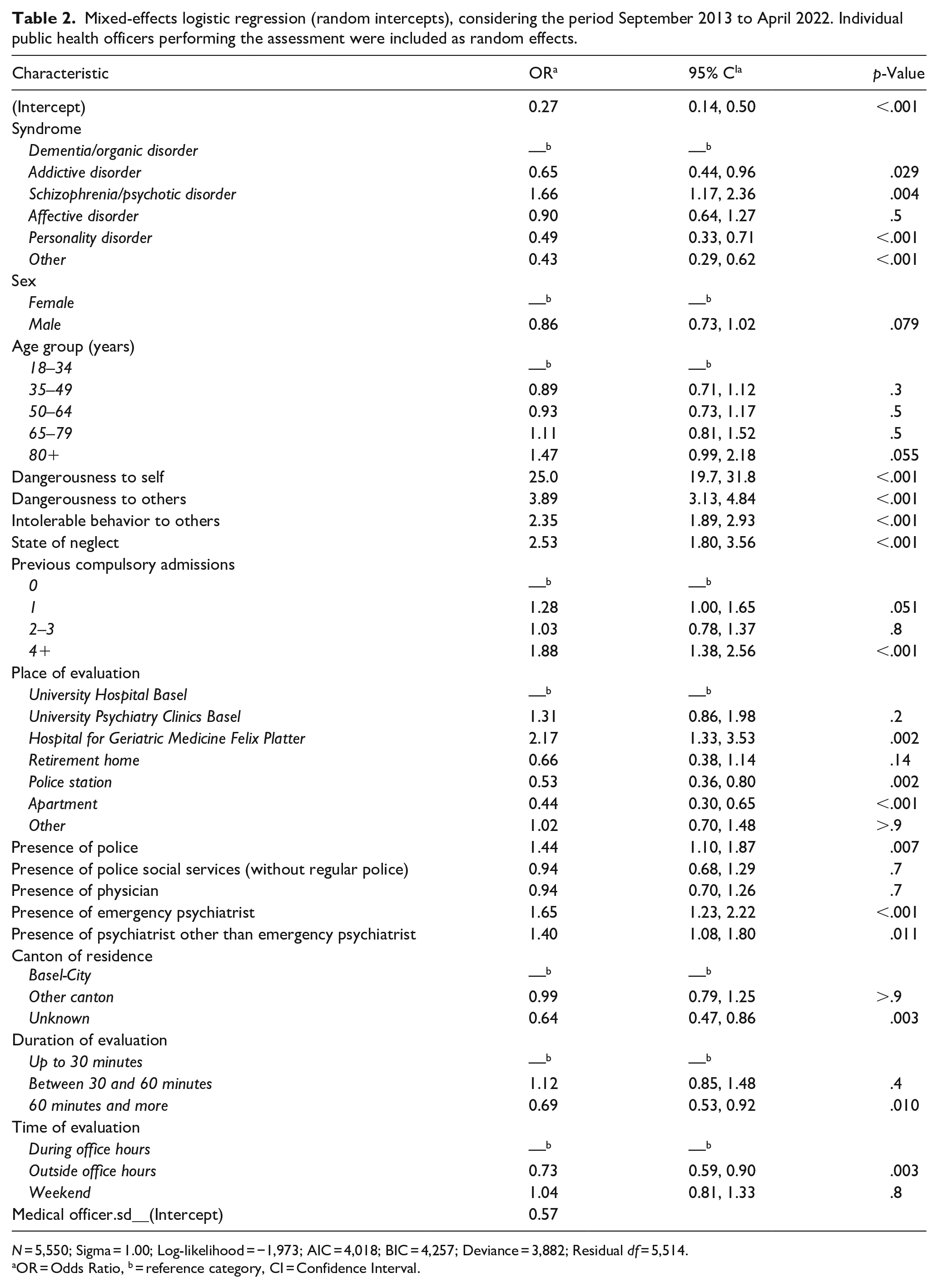
N = 5,550; Sigma = 1.00; Log-likelihood = −1,973; AIC = 4,018; BIC = 4,257; Deviance = 3,882; Residual df = 5,514.
OR = Odds Ratio, b = reference category, CI = Confidence Interval.
Self-endangering behavior was the factor most strongly associated with the decision for compulsory admissions, followed by behavior endangering others, a state of neglect, and intolerable behavior toward others. In terms of underlying syndromes, compared to the reference category of dementia and organic disorders, schizophrenia and psychotic disorders were associated with a higher likelihood of compulsory admission, whereas the opposite was true for the remaining syndromes. Regarding the place of evaluation, the setting of a geriatric hospital was the most critical risk factor for compulsory admissions, followed by other clinical settings (compared to the reference category of University Hospital Basel). In addition, a history of multiple compulsory admissions was linked with an increased risk of readmissions.
Although the presence of police was significantly positively associated with the risk for compulsory admission, evaluation at the police station was associated with a considerably reduced risk. Taken together, the risk for compulsory admission was not elevated (combined OR for the place of evaluation and presence of police <1), except for police involvement outside the police station, which comprises only around 15% of cases.
Moreover, involvement of the social service unit of the police force (not uniformed) was not associated with an increased risk for compulsory admission, even in community settings. While the presence of psychiatrists showed a higher likelihood of compulsory admissions, no such effect could be seen for the presence of physicians. Interestingly, evaluations outside office hours and evaluation duration longer than 60 minutes were associated with a lower likelihood of being compulsorily admitted. Furthermore, we found no statistically significant effects for age and gender.
To account for potential personal biases of individual public health officers on the decision to admit a patient to a psychiatric institution involuntarily, the public health officers conducting the assessment were entered as random effects in the mixed-effects logistic regression model. The intraclass coefficient of 5% (ICC = 0.050) suggests only minor clustering effects by public health officers.
Results were mainly unaffected by excluding cases voluntarily admitted after evaluation (Table S1, Supplemental Material), except for increasing age and gender being statistically significant in this model. Furthermore, the intraclass coefficient of 4.8% (ICC = 0.048) was very similar to the primary model. Finally, a fixed-effects-only model without random effects (Table S2, Supplemental Material) showed very similar results compared to the primary model, apart from an attenuated effect for self-harming behavior and the presence of a psychiatrist other than an emergency psychiatrist.
Discussion
This study leverages a large (n = 5,550) and representative consecutive longitudinal sample of patients assessed for compulsory admissions throughout the canton of Basel-Stadt from January 2013 to April 2022. By also including persons who did not meet the criteria for involuntary hospitalization, it identifies the risk factors that govern the decision-making of public health officers concerning compulsory admission to psychiatric care. Another strength of this study is that by employing a mixed-effects logistic regression model, we can measure the degree to which public health officers’ personal biases may impact decision-making.
The risk of self-endangering behavior appeared to be the most crucial determinant for compulsory admission. However, self-endangering behavior was also present in 54% of patients who were not admitted to a psychiatric institution against their will, indicating that public health officers followed a broad concept of danger-to-self that goes far beyond imminent danger-to-self.
While a systematic review and meta-analysis by Walker et al. (2019) suggest that the perceived or actual risk of harm to self or others is critical in professionals’ decisions about compulsory admissions, a comparison with existing literature is difficult since behavior endangering self or others is usually not available as an explicit predictor regarding the decision for or against compulsory admissions, as implemented in our logistic regression models, but seems rather implicitly assumed according to the underlying diagnosis.
The cantonal health service in Basel-Stadt exclusively entrusts public health officers – recruited from a wide range of medical specialties other than psychiatry –- with decision-making power regarding compulsory admissions, possibly benefiting from an effect first-described by Eytan et al. (2013), who suggested, based on data from Geneva, that limiting the right to order compulsory admissions to specific professional groups, might help reduce compulsory admission rates.
Our results appear to be in line with the public attitude in the canton of Basel-Stadt toward the approval of coercive measures in psychiatry, as shown by a recent study by Steiger et al. (2022), where respondents showed more tolerance toward behavior that implied danger to others as compared to behavior endangering oneself. Hence, one could argue that this particular setup serves its political purpose of aligning the decision-making regarding a critical liberal rights issue with the existing public attitudes toward this issue.
This is further supported by the aggregate compulsory admission rates published by the Swiss Health Observatory Obsan (Swiss Health Observatory, 2021) for each canton. The rates of involuntary hospitalizations in the canton of Basel-Stadt have been within the national average range in recent years. However, Basel-Stadt, with almost 90% of its population residing in the country’s third largest city, is by far the most densely populated canton in Switzerland (Federal Statistical Office, 2021). Given the higher prevalence of risk factors associated with poorer mental health in cities like low socio-economic status, low social support, migration status, schizophrenia prevalence, etc. (Gruebner et al., 2017; Peen et al., 2010; Vassos et al., 2012), we might therefore expect particularly high compulsory admission rates for Basel-Stadt, especially compared to other cantons with large metropolitan areas (e.g. Zurich, Geneva). Instead, both of these cantons show significantly higher rates.
In contrast to Walker et al. (2019), police involvement is only associated with an increased risk for compulsory admission under very limited circumstances but with an equal or reduced risk in most contexts. This suggests that the police, like other major stakeholders (e.g. physicians, public health officers, University Psychiatric Clinics Basel), share the concern for the potentially harmful effects of compulsory measures (Deutschenbaur et al., 2014; Sowislo, Gonet-Wirz et al., 2017; Sowislo, Lange et al., 2017; Steinert et al., 2013; Theodoridou et al., 2012) and therefore considers them only as a measure of last resort.
In that light, the positive association with the presence of a psychiatrist or emergency psychiatrist might seem surprising. However, we believe this indicates selection bias since the involvement of a psychiatrist or emergency psychiatrist is typically a predefined intermediate step for most significant stakeholders (e.g. University Hospital Basel, police officers, etc.) before the formal involvement of a public health officer.
Interestingly, although lack of decision-making capacity is not a prerequisite for ordering a compulsory admission and is therefore not systematically assessed during the evaluation of public health officers, syndromes that are typically associated with lack of insight or reduced decision-making capacity (e.g. schizophrenia, dementia) were more strongly associated with compulsory admissions, even after controlling for risk-to-self or others, suggesting that public health officers might implicitly consider lack of decision-making capacity in their assessment.
We found little evidence for clustering effects among public health officers, suggesting that the decision to admit persons compulsorily is widely free of personal biases and follows shared professional standards. Moreover, it appears to be independent of regular office hours, suggesting consistent evaluation standards during all times of the day, including weekends.
Focusing on studies from Switzerland, organic psychotic disorders, or schizophrenia spectrum disorders were the most consistent risk factor associated with compulsory admissions (Arnold et al., 2019; Eytan et al., 2013; Hotzy et al., 2019), whereas the association of age and gender was inconclusive in the studies mentioned above. Aggressive behavior (Silva et al., 2019) and admission during nighttime or on weekends (Arnold et al., 2019) were also associated with compulsory admissions. Furthermore, a history of previous compulsory admissions was associated with an increased risk of re-admissions (Lay et al., 2019; Silva et al., 2018).
With regards to the international literature, the factors mentioned above as well as additional risk factors could be confirmed by our findings: self-endangering behavior (Lebenbaum et al., 2018; Rodrigues et al., 2019; Schmitz-Buhl et al., 2019), behavior endangering others (Hustoft et al., 2013; Walker et al., 2019), the presence of schizophrenia or psychotic disorders (Cougnard et al., 2004; Juckel & Haußleiter, 2015; Riecher et al., 1991; Umama-Agada et al., 2018; Walker et al., 2019), and previous compulsory admissions (Oliva et al., 2019; van der Post et al., 2009; Walker et al., 2019). Our sensitivity analysis also implicated an association with increasing age (Hustoft et al., 2013; Juckel & Haußleiter, 2015). Interestingly, unlike in several other international studies (Cougnard et al., 2004; Riecher et al., 1991; Umama-Agada et al., 2018), male gender was not associated with an increased likelihood of compulsory admissions. Furthermore, an increase in compulsory admissions during nighttime or on weekends, as shown in Swiss and international literature (Arnold et al., 2019; Hustoft et al., 2013; Juckel & Haußleiter, 2015), could not be supported by our data suggesting the consistently high quality of evaluations by public health officers and actors involved in compulsory admissions at all times.
The present study has several limitations. First, no definitive diagnosis can be made during the on-site evaluation by public health officers since the time for the patient interview is usually very limited, and no further diagnostic clarifications can be initiated. Thus, the diagnostic groups presented here only represent tentative diagnoses and were broadly classified as syndromes. In addition, the data routinely collected during on-site evaluations by public health officers are limited. Several factors associated with compulsory admissions that have been described in the literature are not recorded in the cantonal data set, for example, country of origin or ethnic background (Davies et al., 1996; de Wit et al., 2012; Hustoft et al., 2013; Terhune et al., 2022; Walker et al., 2019), marital status (Juckel & Haußleiter, 2015; Umama-Agada et al., 2018; van der Post et al., 2012), educational status (Hustoft et al., 2013) or engagement to outpatient services (Oliva et al., 2019). Therefore, while we provide evidence that the impact of personal biases on individual public health officers’ decision-making is minimal, we cannot rule out systematic bias regarding migration status or ethnic background. Furthermore, patients living in Basel-Stadt but being evaluated in another canton are not recorded in our dataset, since the canton in which the person is evaluated is responsible for initiating a compulsory admission. Due to the local characteristics of Basel-Stadt (e.g. legal system, demographics), the results of this study are not easily generalizable to other cantons or the whole of Switzerland.
Conclusion
In conclusion, in the canton of Basel-Stadt, the decision-making of public health officers regarding compulsory admissions is primarily driven by preventing self-harm and, to a lesser degree, by harm to others. This suggests that compulsory admissions are only used as a measure of last resort, in line with current evidence regarding the detrimental effects of compulsory measures on treatment outcomes in psychiatry. This view appears to be shared by all major stakeholders in the system, including the police. It is reflective of public attitudes toward compulsory measures, suggesting that the current system serves its politically assigned role. Moreover, public health officers’ decision-making seems to be widely free of personal biases. It is independent of the assessment time, indicating a consistent quality of assessment that follows shared professional standards.
Supplemental Material
sj-docx-1-isp-10.1177_00207640221141020 – Supplemental material for Compulsory psychiatric admissions in the canton of Basel-Stadt between September 2013 and April 2022: Analysis of the cantonal database of the Health Department of Basel-Stadt
Supplemental material, sj-docx-1-isp-10.1177_00207640221141020 for Compulsory psychiatric admissions in the canton of Basel-Stadt between September 2013 and April 2022: Analysis of the cantonal database of the Health Department of Basel-Stadt by Michael Schneider, , Moritz Back, Jana S Krückl, Julian Moeller, Undine E Lang and Christian G Huber in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The authors want to thank Marie-Louise van Aubel, Lisa Hochstrasser, Simon Fuchs, Thomas Bart, and Ruth Spieler Denz for their work leading up to this study.
Author contributions
MS, MB, JK, JM, UL and CGH designed the study. MB collected and analyzed the data, MB and MS interpreted the data. MB wrote the initial draft of the paper. MS, JK, JM, UL and CGH critically revised the manuscript for important intellectual content. MB had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors have contributed to read and approved the final version of the manuscript.
Availability of data
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is unavailable.
Conflict of interest
The authors report no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
The local Ethics Committee approved this study (Ethikkommission Nordwest- und Zentralschweiz, 287-13/PB_2020_00029).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.