
Abstract
Background:
Refugee groups fleeing war and violence and resettling in the West are one of the population groups that are poorly understood. Understanding their mental health challenges and providing effective and evidence-based interventions continue to be formidable challenges.
Aim:
This study presents a refugee mental health framework [RMHF] that was developed to address the gaps in understanding and responding to the needs of refugee populations by prioritizing their voices, and incorporating lessons learned from working with these refugee communities into the development of the framework.
Method:
A RMHF was developed, presented and refined with input from refugee communities, multiple stakeholders and an expert panel.
Results/conclusions:
This paper presents the process and finalized framework, and discusses its utility as a mapping, planning and intervention tool in supporting refugee communities with their resettlement and promoting mental wellbeing.
Rationale
The world is in a mental health crisis of ‘monumental suffering’, according to the Lancet Commission, a team of 28 global experts who have come together to focus on mental illness and care (Boseley, 2018). The expert commission estimates 13.5 million lives could be saved every year if mental illness is given proper attention.
The ongoing refugee crisis and international displacement, and their impact on mental health, are also part of this bleak picture. According to the United Nations High Commissioner for Refugees (UNHCR), there are more than 65 million people forcibly displaced worldwide, representing a new post-Second World War record (CTC News, June 20, 2017). As a response to the conflict in Syria, which has been termed the worst humanitarian crisis in the world today, Canada resettled 25,000 Syrian refugees between November 2015 and February 2016. Given this context, and the unique issues that refugees face when fleeing from homes torn apart by war and violence, do we have the knowledge base to develop appropriate policies and plans, implement programs and services, and address mental health care and prevention that are constructive to this population?
Healthcare disparities in immigrant and refugee populations have been well-documented, even in affluent countries of the Western world (Wilkinson & Marmot, 2003). Not surprisingly, this pattern of disproportionate impact on racialized communities has also been observed during the current COVID-19 pandemic (Andoh, 2020; Cook et al., 2020; Rimmer, 2020). With an increased awareness of mental health’s place in the overall health of an individual, family, and community, global and national strategies to address mental health are being developed. Such strategies, while improving overall population health, lead to an increased disparity because of higher absorption rates among the advantaged. Williams and Mohammed (2013) therefore argue that the only way to eliminate such disparities is to have rapid improvements in the health of the disadvantaged, compared to the rest of the population. Given the urgency, combined with the well-documented issues in addressing refugee mental health (e.g. Mental Health Commission of Canada, 2016; Pain et al., 2014; Silove et al., 2017) it is imperative that we have an introspective approach entailing creativity and authenticity in working with diaspora communities.
Regrettably, very few from refugee communities lead research in their own communities or in the refugee mental health field in general (Crumlish & O’Rourke, 2010), thus leading to a dearth of contextualized knowledge and experience on the subject matter. Whereas refugee survivors of trauma and torture largely originate from non-Western countries, the planning and implementation of research aimed at understanding these survivors are mainly in the hands of mainstream academia. Moreover, despite the acknowledgment of major challenges in applying diagnostic criteria developed in the West to war and violence, the knowledge experts in developing countries look to the West for ‘gold standard’ treatments, as they lack the necessary resources and optimal circumstances that can facilitate investment in the skills and resilience that is present locally (Somasundaram, 1998). Professionals in the West who work in the field of refugee mental health also rely on models and approaches that are adapted from mainstream models, in an attempt to fit the different and multiple realities of the diverse communities that seek a safe haven in the West. We look for the commonalities and use them as evidence to find universalities in mental illness and suffering. This point is very well illustrated in the DSM-5 (American Psychiatric Association [APA], 2013) which reads, ‘Cultural syndromes and idioms of distress influence the expression of PTSD and the range of comorbid disorders in different cultures. . .’ (p. 278). As such, we err by ignoring the unexplainable unique factors that we may observe in refugee populations as ‘noise’, or label them as varying expressions of a phenomenon familiar in the Western context.
Kleinman has noted in his work as early as 1977, that ‘reification of one culture’s diagnostic categories and their projection onto patients in another culture, where those categories lack coherence and their validity has not been established, is a category fallacy’ (quoted in Kleinman, 1988, p. 15). However, to date, our conceptual understanding of trauma in the West is to approach our understanding of war and violence worldwide and across all circumstances (such as in conflict zones, among internally displaced, in refugee camps, and diaspora communities in the West) through a single lens without nuance. We judge and label the other’s experience from our frame of reference, thereby failing to acknowledge the strength, resilience, and nuances of distress that are present in the different cultural groups to which refugees belong (Pandalangat, 2006). This propensity is seen in the mainstream utilization of generalized labels such as ‘fatalism’ (DSM-5: APA, 2013, p. 277), and ‘passive’ coping (Hassan et al., 2015, p. 17) when addressing traditional non-Western cultures’ world-views and perceptions.
Though the knowledge that is applied today to address refugee mental health is clearly a product of the well-meant efforts of many scholars throughout many years, as the Indigenous author Elliot (n.d.) writes, ‘empathy is not enough’. She says, ‘To truly write from another experience in an authentic way, you need more than empathy’. When your research and application originate from lived experience, there is authenticity, not just empathy. A recent review on refugee mental health concludes: ‘Within the mix, the voice of the refugee communities is vital. Mental health cannot be conferred, it must be regained by the communities that have temporarily lost their equilibrium as a consequence of overwhelming circumstances’ (Silove et al., 2017, p. 137). The core principle of the refugee mental health framework [RMHF] that is being presented here has exactly that in mind.
To date, the evidence is lacking for effective assessment (Campbell, 2007; Hollifield et al., 2002; McColl et al., 2010) and treatment interventions for refugees (Aroche & Coello, 2004; Bernardes et al., 2010; Crumlish & O’Rourke, 2010; Johnson & Thompson, 2008; Tribe et al., 2019). With the main emphasis on randomized controlled trial studies, there are recommendations for first-line treatments for PTSD in the general population, with the best practice being trauma-focused exposure-based approaches. There is also criticism, for example, on the acceptance of cognitive behavioral therapy as best practice, psychology’s reliance on randomized controlled trials, and research which does not reportedly reflect the reality for many trauma victims. Shedler (2017) addresses this in detail in his disapproval of the recent treatment guidelines for trauma, issued by the American Psychological Association.
A psychiatric diagnosis is an interpretation of a person’s experience (Kleinman, 1988). Interpretation always depends on the interpreting professional’s knowledge, orientation and biases. The diagnostic systems that mental health professionals are working with are mainly based on normative experiences among Westerners. In spite of cultural revisions made to the recent Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013), its applicability to diverse cultures remains a major challenge due to the fact that the DSM continues to be based on a universalist/biological model with an isolated rather than integrated cultural component (La Roche et al., 2015). As mental health professionals, we have been trying to adapt our diagnostic methods to better understand, assess, and interpret the refugee experience, and have made progress in terms of best practices, guidelines and models to provide better help (e.g. Kanagaratnam et al., 2017). Even so, we need to move beyond the clinical sphere of diagnosing and stop seeing diagnostic labels as the end product of mental health care. The whole is greater than the sum of its parts; thus, a diagnosis should not prevent us from gaining a more comprehensive insight on refugees and their communities (Andermann et al. (2021). Regardless of proper diagnosis or lack thereof, refugee mental health and wellbeing is an interplay of dynamics at different levels: the individual, the family, the community, and the larger system of which refugees are a part of.
Having an integrated understanding of mental health is key at all these levels. Intervention programs that are designed to utilize resilience factors in a cultural group could create unintended consequences (Grandbois & Sanders, 2012; Kouyoumdjian et al., 2017). Such an example is cited by Williams and Mohammed (2013) in which distribution of casino revenue to Native Americans, though intended to improve health and reduce health disparities, turned out to increase alcohol consumption and obesity, a result which was associated with the distribution of funds. Findings such as these point to the importance of a closer association between the research community and policy makers. Findings from health-related research should be better integrated into healthcare delivery and social policy across the multiple sectors of the society.
In their report to the Mental Health Commission of Canada (2016) write how difficult it is to create a synthesized document for refugee/migrant populations, as existing frameworks to improve mental health services for these populations, though promising, have been developed in different places for different populations. However, mental health programs that specifically target one cultural community are found to be four times more effective when compared to programs designed for heterogeneous populations. Additionally, it has been found that services provided in the patients’ native language are twice as effective (Murray et al., 2010). Thus, when working for the betterment of mental wellbeing in refugee communities, what we need is a common framework of understanding that reflects refugee voices. This has been lacking so far.
Guidelines and models exist that take into account the broader context in addressing the mental health needs of refugee groups. Ecological models have been proposed to work with specific age groups (Ellis et al., 2019), emphasizing many of the environmental stressors that need to be considered when working with this population (Miller & Rasmussen, 2017). Models of service provision addressing challenges (Misra et al., 2006), best practice guidelines for health promotion including protective and risk factors (Centre for Addiction and Mental Health, 2012), and planning multi-level interventions (Im et al., 2021) have also been recommended. The World Health Organization (2018) has put forward refugee mental health guidelines. In Canada, a refugee mental health model has been suggested by the Mental Health Commission of Canada (2016). While these efforts are commendable, the framework that is being presented by the authors of this paper is unique in its aptness of placing the refugee’s life-world at the center of the approach. Moreover, the framework facilitates taking a systematic approach to map, plan and intervene, regardless of where refugee communities are in their path to healthy integration.
Pilot role of Tamil community
The Tamil community has been used as a reference point to develop this refugee mental health framework [RMHF] as it has contributed immensely to the Canadian mosaic in diverse ways, meaning it is well positioned to offer crucial lessons learned in terms of informing the RMHF.
The largest quantitative study on the mental health of the Sri Lankan Tamil Diaspora was undertaken in Toronto. This was a CIHR funded study led by Dr. Morton Beiser, of 1,600 adult Tamils to look at the prevalence of anxiety, depression and PTSD in the Tamil community. Tamil service providers requested the study be undertaken as there was a spate of suicides in the late 1990’s in the Tamil community. The findings emphasized among other factors the importance of looking beyond the index events and incorporating the stresses of passage as well as post-migration linkages, in the healing of refugee trauma (Beiser et al., 2011).
There have been many other studies in Tamil communities through the years. Social functioning is a casualty of the war, and its disruption impacts individuals’ sense of wellbeing profoundly. Research shows that the Sri Lankan Tamil community emphasizes social functioning as the hallmark of health. This has been found with other ethnic communities as well (Pandalangat et al., 2013). There is research evidence indicating that the community holds an integrated notion of health, one that encompasses physical, mental and social components, which is also the case with other non-Western cultures (Weerasinghe & Mitchell, 2007). Mental illness is seen in a continuum but mostly as not dissonant to oneself or to the community unless it manifests itself in socially disruptive behavior (Kanagaratnam et al., 2020).
The Tamil community has built a very strong business and political presence for itself in Canada. The community has a strong advocacy history and also an increasing presence in the media. It is an established, successful community, dealing at the same time with significant struggles and resettlement stressors to date.
Given the unique challenges faced by refugee communities, it is important to look at how the system can be tailored to help enhance the system. The intent is that this framework, developed using one refugee community as a reference point, is unique yet flexible in its applicability to other refugee communities. This is a practical and grounded approach to developing a refugee mental health framework.
Development of the refugee mental health framework
The refugee mental health framework [RMHF] presented in this paper seeks to address many of these gaps in understanding and respond to the needs of refugee populations by prioritizing their voices, and incorporating lessons learned from working with these refugee communities into the development of the framework. Different refugee communities are at different points in their journey in Canada. A refugee mental health framework is important to inform work in all refugee communities and foster advocacy at the federal and provincial levels.
The developers of this framework are a team with experience and expertise in research, practice, international development, and program planning, and have done considerable work with refugee communities. Two of them have lived experience as refugees. The team has developed a mental health framework using the Tamil community as a case study, with community members with lived experience providing input into the framework.
As part of this process, the team led a 1-day workshop with diverse stakeholders on May 17, 2016, where lessons learned and a draft framework were presented. Tamil community members with lived experience were consulted through the process and also presented their valuable insights and experiences at the workshop. There were 65 participants representing a very diverse stakeholder-ship, including but not limited to refugee and family lawyers, mental health counselors, physicians, psychiatrists, researchers, program planners, policy makers and artists, from municipal and provincial levels of government, community organizations serving refugees, hospitals and academic institutions. There was unanimous agreement by all participants that the framework was indeed a very valuable tool for informing our work with refugee communities.
Subsequently, the framework was refined and updated in consultation with an expert panel. All members of the panel had significant expertise in the field of mental health, with many having worked with displaced communities in both local and international contexts (Figure 1).
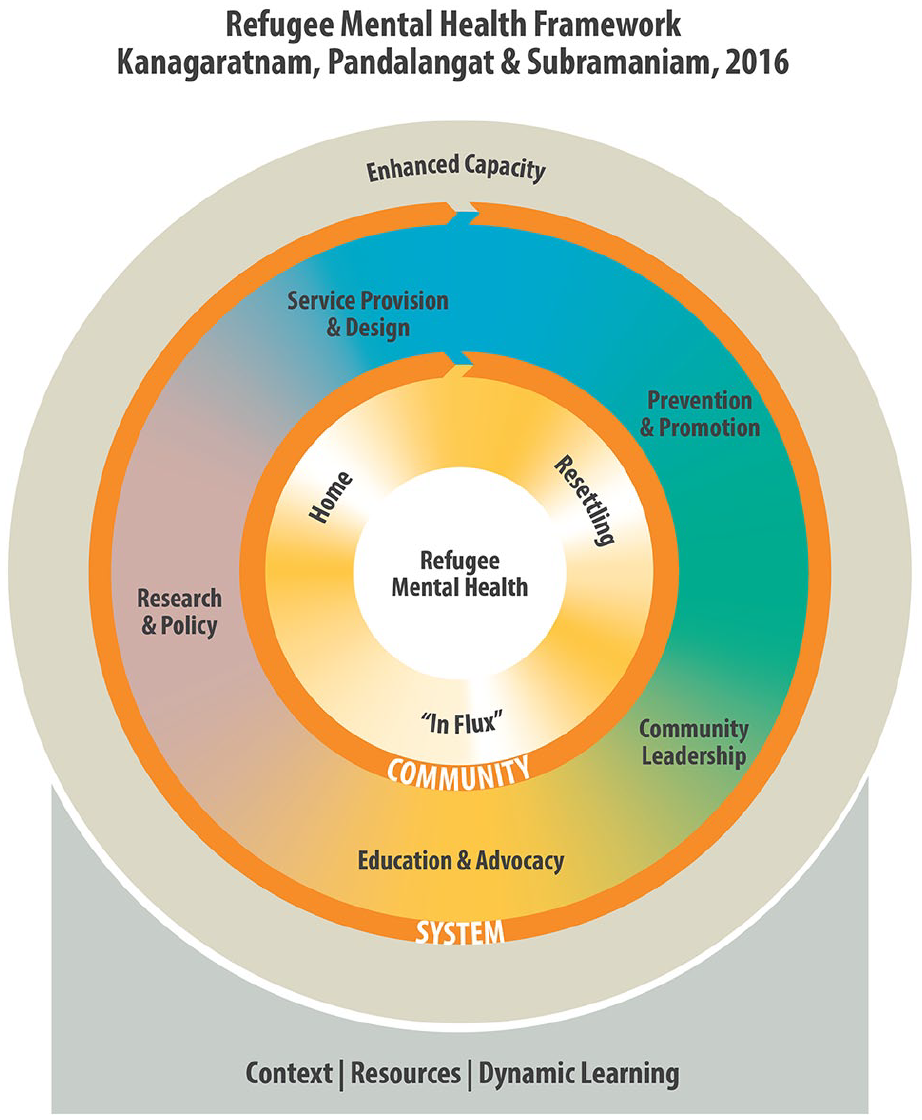
The refugee mental health framework.
Expanding on the dimensions of the framework
Understanding the refugee community is at the core of the framework. This encompasses different facets and experiences of the community – (a) the Home Community refers to the community in its home space, in the country of origin, within its native historical, cultural and social contexts (b) the community In-flux reflects the experiences of the refugee community due to the war and unrest that it experiences – this includes, but is not limited to trauma, torture, losses, detentions, and flights to foreign lands (c) the Resettling Community provides a picture of the community in its current context of resettling into another country, faced with challenges and the necessity to make adaptations. Understanding the different dimensions of The Community is crucial to meeting them where they are at, understanding their challenges and needs, and being respectful of the cultures, contexts, and strengths that they bring with them
The system level dimensions of Service Provision and design, Prevention and Promotion, Research and Policy, Education and Advocacy, and Community Leadership are all interconnected, and are informed and guided by the understanding of the dimension of The Community. For example, how does our understanding of a community, their beliefs with regards to health and wellness, their migration trajectory etc., inform service provision and design. How do we use tools and modalities and stories that they are familiar with in our prevention and promotion, what are the gaps in our understanding of the community, its sub-populations and interventions that work for the community that can be filled through relevant research, what is the policy regarding refugee health and resettlement, has it been different for different refugee communities, how have these differences impacted mental health and well being? How will advocacy help improve the lives of refugee communities, both at the individual and system levels and how can research help build the advocacy? When dimensions start addressing these very pertinent issues, the application of the framework becomes that much more effective and relevant. The Community Leadership sub dimension in the system dimension is extremely important in utilizing and fore fronting the expertise and knowledge and influence of the community, treating it as an invaluable resource that should be part of a systematic, and systemic response to our work with refugee communities.
The utility of the RMHF
The development of the RMHF has significant value as it covers core aspects of refugee mental health that is seen across communities.
The RMHF is a useful tool as it:
Starts from a fundamental understanding of the community values and characteristics, and its experience through migration and settlement;
Considers these different aspects at all levels of service provision, research, program, policy and system design;
Incorporates community leadership as a crucial system factor in enhancing refugee mental health. This moves the notion away from the traditional ‘service to’ frame of reference to the ‘work with’ frame of reference;
Integrates context (the COVID-19 pandemic is a contemporary example), resources and continuous learning so that the framework continues to be a dynamic, evolving entity.
From the perspective of clinical practice, this model is adaptable and can be used effectively in designing appropriate programs and services. It will play a crucial role in influencing government policy around refugee populations, and can be used as an educational tool in training professionals working with refugee communities. While the Canadian government is extending significant goodwill toward certain refugee communities, the application of this evidence-based framework will ascertain a systemic, equitable government response to all refugee communities.
Case study support for the RMHF
The following case study helps illustrate the various components of this framework as it may apply to the Tamil Diaspora:
Sri, a 17-year-old male, arrived in Canada through an agent in 1996. He had no close relatives in Canada but was promised to be taken care of by a distantly related uncle, who resided in Canada. Due to the war schools in Sri Lanka were not functioning, and as a young Tamil boy in the Northern province of Sri Lanka, his parents were forced to send him to the capital city of Colombo when he was 14 years old, out of fear for his safety. Since then, Sri managed on his own in Colombo, renting a room with a family whom he did not know. Though he was initially safe in Colombo and far away from the bombing, shelling and risk of abduction in the North, as a Tamil male living away from family, he was arrested under suspicion that he had links to armed groups, and was at one point also sexually assaulted when in custody by government forces. Sri managed to get out of the country with the help of a lump sum of $15,000 paid to an agent by the uncle in Canada. The travel from Sri Lanka took him almost 2 years as he was detained in a couple of European countries en route to Canada.
Upon arriving in Canada, though relieved to be far away from his war-torn home country, Sri was still longing for his parents and was overwhelmed by the daily challenges of living in a completely unfamiliar environment, and without landed status. Due to the large debt, he owed his uncle, and knowing that he needed to financially support his father back home (who lost his small business due to the war), he knew he had to start making money. His uncle got him a job at a factory owned by a person in the community, and Sri started working as a general laborer. His refugee claim was accepted and he gradually managed to pay his uncle’s debt, and was making enough money by working overtime hours to regularly send money back home to support his family. With experience, he was promoted at work to a machine operator. Feeling obliged due to having received help from his uncle, Sri agreed to marry his uncle’s daughter. Life became significantly stressful for Sri when his arm was amputated due to an accident at work. He was not successful in returning to work, and the relationship difficulties with his spouse escalated when Sri ended up being home with no job, leading to severe depression.
In reviewing the above scenario, it is clear that having an understanding of young newcomers like Sri would have been useful for mental health practitioners to identify the potential challenges he and many other young Tamil men may have faced when resettling in Canada in similar situations. Knowledge about Sri’s home community in the Northern Province of Sri Lanka would have helped practitioners understand the emphasis the Tamil community places on education, the strong connection to one’s village/home town, and the home community’s view on mental health and wellbeing. Sri had lost stability in his life at the young age of 14 when he was removed from his parents and his home community, and arguably before that due to the multiple evacuations he endured when living in the conflict zone. The journey to Canada took him 2 years, even after which his life was in limbo for many years until he obtained landed status. As such, the significance of possible attachment trauma, the incarcerations and sexual assault, and other incidents that were challenging for him comprise the In-flux component of the RMHF. An in-depth understanding of the above could have, for instance, informed us that Sri would most likely not have had the ability to identify and acknowledge his own trauma. As such, he would have not sought help himself, and even if he did, this would have not been through mainstream channels; the focal point of intervention should therefore have been Prevention and Promotion. Acknowledging the home as the core of a Tamil’s life-world, and utilizing existing village groups in the diaspora as collective spaces of healing, could have been effective approaches to mental health treatment. Knowing the attributes of the diaspora, promoting Community Leadership, and utilizing the local media for Education and Advocacy initiatives could have proven to be successful in easing the stressors of resettlement and improving Sri’s adaptability, as well as the community at large. Early initiatives to rectify lost education due to the war in young people like Sri is important to consider within Service Provision and Design. Strengthening education is beneficial in the long run, as it helps individuals like Sri to reach their potential by attaining better language and job skills, which can increase their chances of having safer workplaces and more equitable marital relationships. Relevant research and evaluation could help to test out this hypothesis. The Research and Policy component of the RMHF should value and incorporate local knowledge and expertise with the aim of addressing issues that are meaningful for the community such as, for instance, the therapeutic potential of suggested village groups. Using RMHF as a mapping and intervention tool, as indicated above, will inform policy development that would pave the way for implementation procedures that are common and unique to the different war-affected refugee communities, ultimately leading to Enhanced Capacity of the community.
We believe the above case study illustrates in retrospect how the RMHF could have been applied as a mapping tool with the Tamil diaspora, guiding effective interventions at many levels. Likewise, the observations of this community, made through the different phases of the community’s resettlement, could be extended to better understand the second-generation Tamil diaspora and its strengths and challenges, as well as be applied to other refugee communities.
Limitations and future directions
In presenting, evaluating and finalizing the RMHF, we had clear approval on the framework’s relevance and applicability above and beyond the Tamil community from our participants and the expert panel. Our participants and the expert panel had knowledge of and represented other refugee communities. However, granting that the RMHF has been developed based on one refugee community as a reference point, our next steps will be to pilot it with different ethnic communities that have fled their home countries due to war and violence. Such studies would enable us to understand how the RMHF could be applied as needed to fit the different realities of the various ethnic populations. By strengthening the utility and applicability of the RMHF, the framework could become a valuable tool to systematically map the needs of any newcomer refugee community and plan effective and appropriate interventions at the micro, meso, and macro levels. Furthermore, lessons learned from applying the RMHF to established refugee communities such as the Tamil community could inform its use in other and more recent ethnic groups. As noted above, the RMHF could also be used across generations of a specific community, as an effective evaluation tool of any prevention, promotion, education, advocacy and other service provision initiatives. It would also be interesting to examine the RMHF’s utility in different community organizations that serve this population, and also to subgroups, such as children who had witnessed violence between parents, men with addiction issues, and LGBTQ refugees. In the current context of the worldwide Coronavirus pandemic, the unique needs of refugee populations have been identified by authors Sieffien et al. (2020). As such, the RMHF would be a valuable tool to explore and evaluate how the different refugee communities have coped during and in the aftermath of the pandemic. The lessons learned through this process will help us in identifying how enormous crises differentially affect war-exposed refugee communities, and will better prepare us to mitigate the effects of future disasters on these populations.
Footnotes
Acknowledgements
The authors would like to recognize and thank the expert panel comprising of Dr. Haile Fenta, Dr. Daya Somasundaram, Mr. John Trainor, Dr. Clare Pain, and Dr. Arun Ravindran for their insightful and valuable inputs and feedback into the Refugee Mental Health Framework. Authors Dr. Ivan Silver and Dr. Brenda Toner were also on this panel.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.