
Abstract
Objective:
Informal caregivers are often placed in a better position to understand and advocate for the vocational needs of young persons with mental health conditions. However, their opinions are largely ignored in the planning of vocational outcomes. This qualitative study had two broad aims: to explore (1) the perceptions of caregivers of young adults with mental health conditions on issues of paid employment and (2) their views and expectations of employment support services.
Methods:
A total of 30 semi-structured interviews were conducted. Caregivers were 45 years old on average, the majority were women (73%) and were of Chinese ethnicity (53%). Most participants (60%) were parents of the young persons with psychotic disorders (57%), or affective and mood disorders, such as depression or anxiety disorders (43%).
Results:
Thematic analyses of data revealed three superordinate themes: (1) caregiving roles, (2) caregivers’ expectations and hopes, and (3) barriers to employmentof young persons with mental health conditions.
Conclusions and implications for practice:
Caregivers strongly believed that employment support services should prioritise and advocate for recovery while securing employment. Local mental health employment support services should incorporate the views and expectations of caregivers of young persons with mental health conditions to foster better coordination between stakeholders, and enhance support for successful employment, reintegration into the community, and ultimately recovery for these individuals.
Introduction
Mental health conditions are highly pervasive among young adults. According to the National Comorbidity Survey-Replication (NCS-R) study, in the United States, the lifetime prevalence of any mental health condition is approximately 52% among young adults between 18 and 29 years old (Kessler et al., 2005). Another epidemiological survey found that young adults had the highest prevalence, with approximately 26% of those aged between 18 and 25 years experiencing a mental illness during a 12-month period (Bose, 2018). Similar to global patterns, the prevalence of mental health conditions in Singapore is the highest among young adults. Approximately 22% of them between 18 and 34 years old report having a mental health condition in their lifetime (Subramaniam et al., 2019).
Mental health conditions are responsible for a growing proportion of disability and economic burden worldwide (James et al., 2018; Jurewicz, 2015), with unemployment being a major concern (Birnbaum et al., 2010; Luciano & Meara, 2014). At the workplace, mental health conditions have been associated with productivity losses, and absenteeism, among other short- and long-term losses (Dewa et al., 2004). Unlike adults above the age of 50 years, younger adults with mental health conditions are not likely to exit the workforce due to stigma and discrimination by employers, implying that there are windows of opportunities for vocational recovery in young adulthood as opposed to later adulthood (Jurewicz, 2015; Luciano & Meara, 2014). Thus, it becomes vital for individuals with mental health conditions to be engaged in vocational rehabilitation and recovery as early as possible.
Yet, securing employment is particularly stressful for young adults with mental health conditions as they face a different set of vocational challenges that require a unique set of solutions (Bassett et al., 2001). This is because a substantial proportion of young adults with mental health conditions transition into emerging adulthood (Arnett et al., 2014) with an already compromised school education (Goulding et al., 2010; Hjorth et al., 2016) and marked difficulties returning to school (Annapally et al., 2019), that severely limits their capacities for vocational and career growth at the onset.
With a lack of capacity to manage these vocational challenges on their own, informal caregivers, especially family members, become a vital source of support for young adults with mental health conditions. Aside from providing day-to-day care, caregivers play an active role in engaging service providers or finding jobs for their loved ones (Sin et al., 2012). Similar to persons with mental health conditions, caregivers too believe that employment is an integral part of recovery for mental health conditions (Balaji et al., 2012), however, they may hold dissimilar views concerning job choices and employment expectations, which can lead to immense stress, conflict, helplessness and frustration between the two parties (Jagannathan et al., 2011; Martin et al., 2005). This is because, according to the family systems perspective, career choices of young adults are not only influenced by personal traits or interests, but also by the expectations and hopes of the family (Larson, 1995; Splete & Freeman-George, 1985). This is particularly emphasised in families of collectivistic cultures that value familialism, where day-to-day, medical (including psychological treatment and rehabilitation) and career decisions are often shared and shaped by the family, and highly influenced by parents or caregivers (Akosah-Twumasi et al., 2018; Chen & Fan, 2010; Fouad et al., 2016; Samsi & Manthorpe, 2013). Family is also an integral support system for the recovery of mental health conditions (Chadda & Deb, 2013). It is therefore not surprising that help-seeking behaviours for mental health conditions are contingent on the beliefs of the family (Connor et al., 2016). In Singapore, 88% of homes have intergenerational living arrangements (Asis et al., 1995), and thus, the family is the most proximate to the needs of family members. As a family unit, the majority of individuals believe that the family is very much capable of providing help for mental health conditions (Ng et al., 2008).
To promote optimal levels of social and vocational functioning for individuals with mental illness, it is therefore vital to have a multidisciplinary approach between service providers and caregivers in a well-coordinated operationalisation of recovery that is also patient-centred (Escorpizo et al., 2011; Liberman et al., 2001). This approach had been practiced in a supported employment model developed in India which included joint-sessions with family members to discuss employment expectations and preferences with the client, and the study had shown promising outcomes (Jagannathan et al., 2020). Unlike in India, most vocational initiatives in Singapore, emphasise on working with the individuals to address their needs and employability, and with employers, and co-workers to improve the working environment. However, there is less focus on working with caregivers as stakeholders in the given framework. Informal caregivers, who often feel they are placed in a better position to understand and advocate for the vocational needs of persons and young persons with mental health conditions (Weinberg et al., 2007), are often not involved in the process of planning of vocational outcomes between employment support providers and persons with mental health conditions. Given the present gaps, this qualitative study had two broad aims: to explore (1) the perceptions of caregivers of young adults with mental health conditions on issues of paid employment and (2) their views and expectations of employment support services in Singapore.
Method
Procedure
We recruited caregivers with purposive sampling methods. Caregivers were initially referred to the research team by clinicians, case managers or by young persons with mental health conditions themselves. The eligibility criteria were: individuals aged 21 and above, who were Singapore citizens or Permanent Residents involved in providing social, physical and financial support to young persons (aged 18–35 years) living in the community with mental health conditions on a regular, personal basis. Recruitment was conducted in the Institute of Mental Health (IMH), a tertiary psychiatric hospital in Singapore.
Written informed consent was taken before the semi-structured interviews, which were conducted primarily in English. Participants were encouraged to speak in their mother tongue languages (Mandarin, Malay, Tamil) if they felt more comfortable doing so. One interview was conducted primarily in Chinese. Trained researchers utilised an interview schedule to guide the semi-structured interviews and provided appropriate probes in order to encourage richer responses. Interviews were audio-recorded and transcribed verbatim. The interview that was conducted in Chinese was transcribed in Chinese and translated into English in the same transcript. Socio-demographic information of the informal caregivers was collected before the start of interviews. Recruitment of participants stopped when data reached saturation, or when no new themes emerged from the interviews. This was determined through several discussions between the members of the research team after the interviews. The data used in this current study is based on a larger mixed-methods study that investigated the perspectives of multiple stakeholders on individuals with mental health conditions. The larger mixed-methods study received ethics approval from the relevant institutional committees: Institutional Research Review Committee of the IMH and the Domain Specific Review Board (DSRB) of the National Healthcare Group.
Participants
Semi-structured interviews were conducted among 30 informal caregivers who were 45 years old on average, majority were women (73%), and of Chinese ethnicity (53%). Majority (60%) were parents of the young persons who had psychotic disorders (57%) or affective disorders, such as depression or anxiety disorders (43%). Informal caregivers were defined as caregivers providing social, physical and financial support to the young person. The full details of the participants are summarised in Table 1.
Sociodemographic information of caregivers and young adults with mental health conditions.
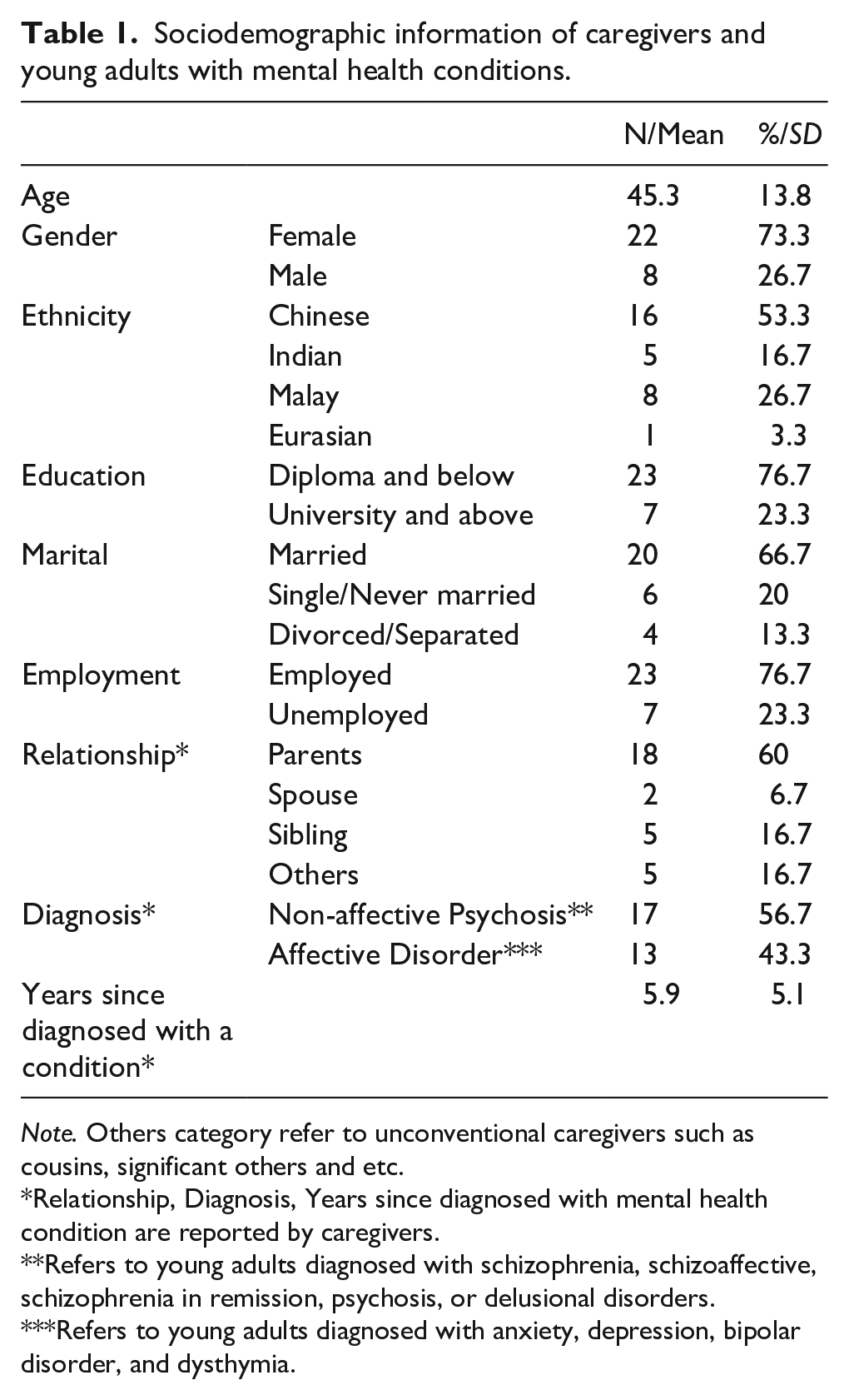
Note. Others category refer to unconventional caregivers such as cousins, significant others and etc.
Relationship, Diagnosis, Years since diagnosed with mental health condition are reported by caregivers.
Refers to young adults diagnosed with schizophrenia, schizoaffective, schizophrenia in remission, psychosis, or delusional disorders.
Refers to young adults diagnosed with anxiety, depression, bipolar disorder, and dysthymia.
Data analysis
With the written consent of participants, interviews were audio-recorded and were transcribed verbatim. Subsequently, the transcripts were analysed using thematic analysis that is guided by the framework by Fereday and Muir-Cochrane (Fereday & Muir-Cochrane, 2006). Important information was recognised, identified and clustered into codes through an inductive coding process. A codebook which consisted of the discussed codes were revised extensively and iteratively through multiple meetings between four coders (WLT, JV, JG and KR). New codes were also highlighted and discussed in the meetings. After the codebook was finalised, the coders coded the same transcript using the NVivo (v.11) software. The process was repeated and the codebook was reviewed until aninter-rater reliability Kappa coefficient of 0.76 was achieved between all coders. This was followed by the coding of the remaining transcripts by all coders.
Results
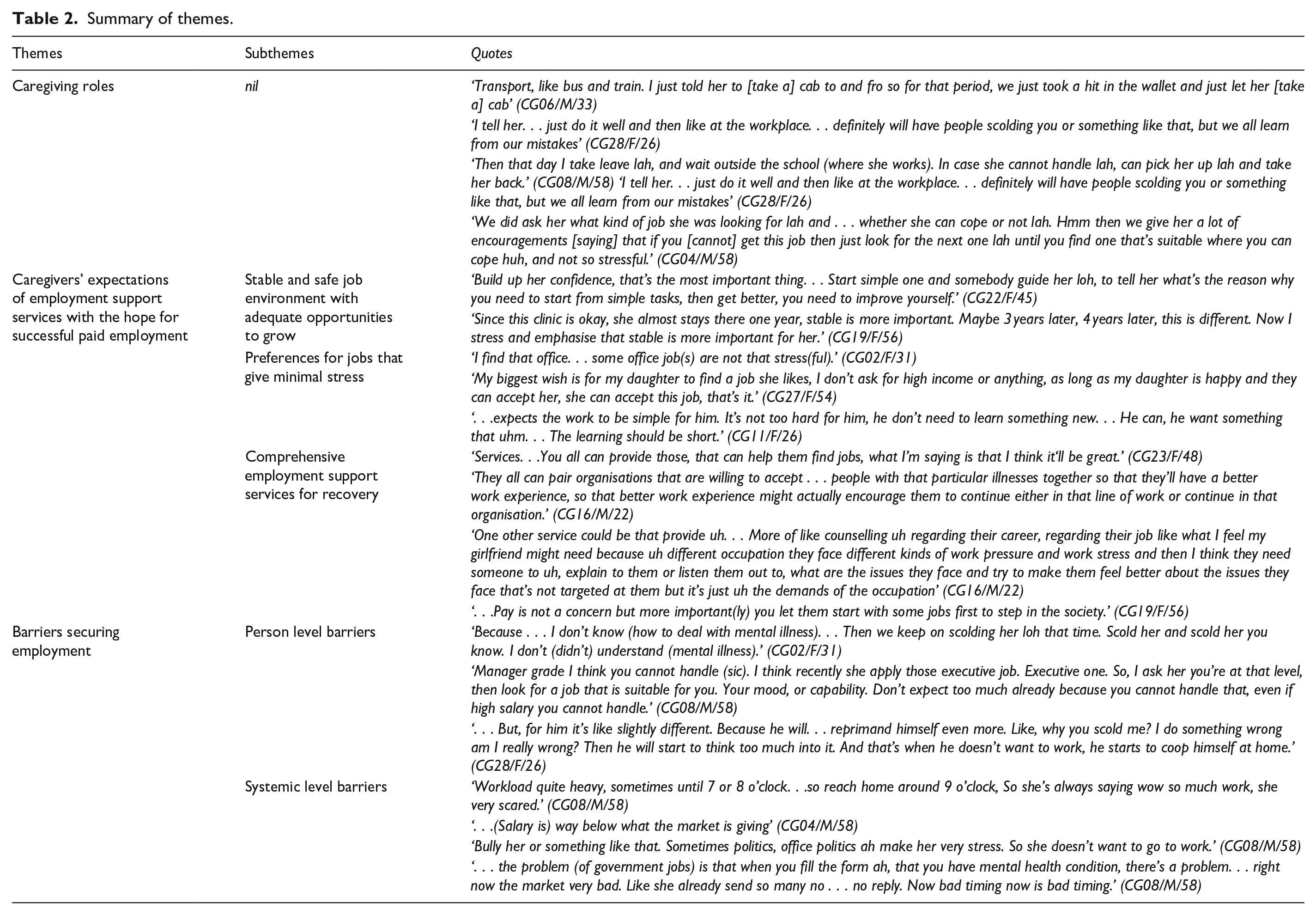
This study aimed to understand informal caregivers’ perceptions of paid employment among young persons with a diverse range of mental health conditions. Thematic analyses of data revealed three superordinate themes: (1) caregiving roles, (2) caregivers’ expectations of employment support services with the hope for successful paid employment and (3) barriers securing employment. The summary of the themes, subthemes and quotes are presented in Table 2.
Summary of themes.
Caregiving roles
Caregivers assumed multiple roles, assisting and supporting young persons’ search for employment. As young adults were generally inexperienced in the area of employment, caregivers provided guidance on what to look out for in a job. This theme was predominantly seen among parental caregivers who felt they understood the young person, and believed that they were able to provide relevant guidance and active care which took into account the young persons’ strengths, skills and their mental state. Some parents made special efforts to accompany their wards to their workplaces and waited around to ensure that they stayed at work and returned home safely. Additionally, the work advice given by caregivers were pragmatic in nature, such as advising ways to control their symptoms at work, adapting to the work environment, getting along with colleagues, presenting a good attitude and to accept criticism. People skills, skills on coping, adapting to a new environment and providing money for transport were some other examples of the myriad support given.
Caregivers’ expectations of employment support services with the hope for successful paid employment
Caregivers discussed important expectations of employment support services and their hopes for career progression and stability. This theme consists of three subthemes: (1) a stable and safe job environment with adequate opportunities to grow, (2) preferences for jobs that give minimal stress and (3) comprehensive support for recovery.
Stable job environment with adequate opportunities to grow
While caregivers strongly believed that employment can support recovery, they also felt that employment can be harmful under certain conditions. To avoid workplace-related harm, they stressed the importance of a conducive work environment, such as having a discrimination-free work experience, limited stress and allowing more time and help for the young persons with mental health conditions to adjust into places of work, particularly for those with schizophrenia and other psychosis.
Having a ‘stable job’ or being ‘stable in a job’ emerged as a recurrent theme throughout the interviews. Given the frequent job hopping or ‘giving up’on their jobs, majority of the caregivers expressed their desires for young persons with mental health conditions to have job stability. Once young persons with mental health conditions found stability in the job, caregivers expect that they should be provided opportunities to progress further in their careers, with opportunities that are appropriate to the young persons’ education level and potential.
Preferences for jobs that give minimal stress
Additionally, caregivers had in their minds specific job characteristics that were deemed as more conducive or preferred by the young adults themselves. These included clerical work and jobs that involved working with children, as these jobs were considered to be less stress inducing. They opposed jobs that involved customer care services where the interaction with people can be a source of great stress. Other preferences included jobs that have fixed work hours (as opposed to those that frequently go overtime), a place that provided internship to learn and earn at the same time, a younger work environment to mingle with other younger individuals (as opposed to older adults) as they are perceived to be more accepting of mental conditions, and jobs that have relevant on-the-job training and coaching so that young persons with mental health conditions can settle in their jobs more quickly.
Comprehensive support for recovery
When caregivers were asked what employment support services should entail, caregivers believed that there should be a comprehensive platform to secure and sustain employment, and operate with the intention to support recovery for all who have mental health conditions. If they engaged employment support services, they would expect employment specialists to work closely with the young persons through (1) securing and sustaining employment and (2) ensuring that employment compliments recovery.
Securing and sustaining employment
The majority of the caregivers believed that employment support services should function like employment resource centres where young persons with mental health conditions can seek assistance and information for jobs. These centres should also have specialists helping to secure and sustain employment for young persons with mental health conditions by finding and matching jobs, providing training workshops, and on-the-job support. Apart from matching jobs based on young persons’ personal interests, caregivers expressed a need to match jobs based on illness type, possibly to encourage peer support and social networking which they had stressed were important for socialisation at work. Most caregivers at the point of interview, felt that more could be done to address the lack of coping skills of the young to deal with the stress on the job.
Employment compliments recovery
Although employment for recovery was not articulated by the majority of participants, it can be inferred from the narratives. Some caregivers mentioned the need to be in jobs that are not stressful, as a first step to recovery, to return to society and normalcy. There should also be counselling services available to support young persons with mental health conditions on the job as well.
Barriers of employment
Caregivers voiced out important barriers to employment, which were characterised into two broad themes of (1) person and (2) systemic levels.
Person level barriers
At the person level, caregivers felt ill-equipped to address the care needs of young persons and they worried about relapse. These concerns came from the lack of knowledge about and stigma against mental illness in general, which in turn lead to a lack of informed involvement in supporting young persons through their illness. Caregivers worried about the possibility of relapse due to stress from work. Besides illness symptoms, caregivers mentioned that certain dispositional traits, such as shyness, being soft-spoken and the lack of social skills, acted as barriers to employment as well. The most prominent feature was the inability to socialised which not only isolated these young persons at work but also reduced their career opportunities. Due to the fears of relapse, and being ill-equipped to address the care needs of those with mental illness, the majority of the caregivers had very low job and career expectations of young persons.
Systemic level barriers
Factors at the systemic level included societal barriers which were often articulated as forces beyond their control, such as an unconducive work environment and an undesirable job economy. Heavy job demands, stigma and discrimination were also key elements to this theme. Other barriers identified were the risk of bullying, stigma and discrimination at the workplace. Disclosing mental health conditions at the workplace had also created difficulties in adjusting into the company. Caregivers expressed that industry restrictions, such as declaring mental illness in application forms, made it harder for the young persons with mental health conditions to apply for positions. Financial instability and disincentives were also cited as important barriers. For instance, a caregiver described some companies as paying salaries that were below the market rate, making it difficult to encourage and motivate young persons to sustain employment.
Discussion
In accordance with previous literature, employment was strongly perceived by most caregivers as a necessary step in the recovery process of young persons with mental health conditions. The advantages are manifold, in terms of reintegrating and engaging with the society, gaining skills, confidence, a sense of achievement and a sustained and fulfilling livelihood (Dunn et al., 2008; Krupa, 2004).
The caregiving process regarding employment for young people with mental health conditions is a complex one. Maintaining hope for the future is an important source of motivation and coping for informal caregivers of people with severe mental illness (McCann et al., 2011). On the contrary, losing hope can drastically affect coping outcomes and eventually patient outcomes (Chadda, 2014). Caregivers, in particular parents and spouses, mentioned instances where young persons with mental health conditions as well as their family were motivated, and expressed happiness that the young persons with mental health conditions were able to work after an episode of relapse. Caregivers’ concerns relating to young persons with mental health conditions’ future were to some extent allayed when they saw them keeping their jobs and becoming independent. This, in itself, was a major reason for increasing access and support for young persons with mental health conditions’ employment. It is noted from our findings that informal caregivers – particularly family members (e.g. parents, siblings), play a crucial role in the decision-making process. They were closely involved in all aspects of employment; from making and supporting the difficult choice between relapse prevention and taking the risk to promote recovery. This is unsurprising as shared decision making is common in collectivistic cultures (Chadda & Deb, 2013; Hsu, 1983; McLaughlin & Braun, 1998). Understanding caregivers’ experiences of securing employment for their relatives is therefore necessary in assessing the kind of support and resources that are needed. However, it must be acknowledged that many caregivers, including family members or spouses, may lack the expertise to support young persons with mental health conditions adequately. This in turn could lead to their views being ill-informed, hampering employment opportunities for young persons with mental health conditions. To avoid such situations, caregivers must be enabled by providing them availability and accessibility of employment support services, appropriate information and psychoeducation regarding illness and management of psychosocial issues related to the young person’s illness to empower them and facilitate the employment process. Past research had shown that when mothers enter brief psychoeducation programmes to improve social skills, their negative attitudes towards schizophrenia were significantly reduced (Kim & Mueser, 2011). In a separate study involving caregivers in similar programmes, self-esteem, satisfaction and perceived family burden improved for caregivers (Chan et al., 2009). Similarly, empowering caregivers with social skills to care for young adults with mental health conditions can facilitate the recovery process.
According to the Relational Coordination Theory by Gittell, having shared goals, knowledge and mutual respect and communication between clients, formal service providers and caregivers can strengthen support for recovery (Gittell & Suchmann, 2013). Underlying recovery is thus seen as a social process that is determined by the roles played by different actors (the individual, family, professionals and the community; (Price-Robertson et al., 2017). Thus, we propose a conceptual model and key variables to serve as an organising framework for guiding supportive interventions for informal caregivers, to facilitate sustained employment for young persons with mental health conditions as presented in Figure 1. In summary, as illustrated, although caregivers assume multiple caregiving roles, they feel that the support they give is inadequate or ineffective due to a lack of understanding of the care needs of young persons with mental health conditions. With hopes for illness recovery and a better future for the young persons, they expressed the desire to access and seek support from professionals, and had certain expectations that they hoped employment support services could meet for the young persons.
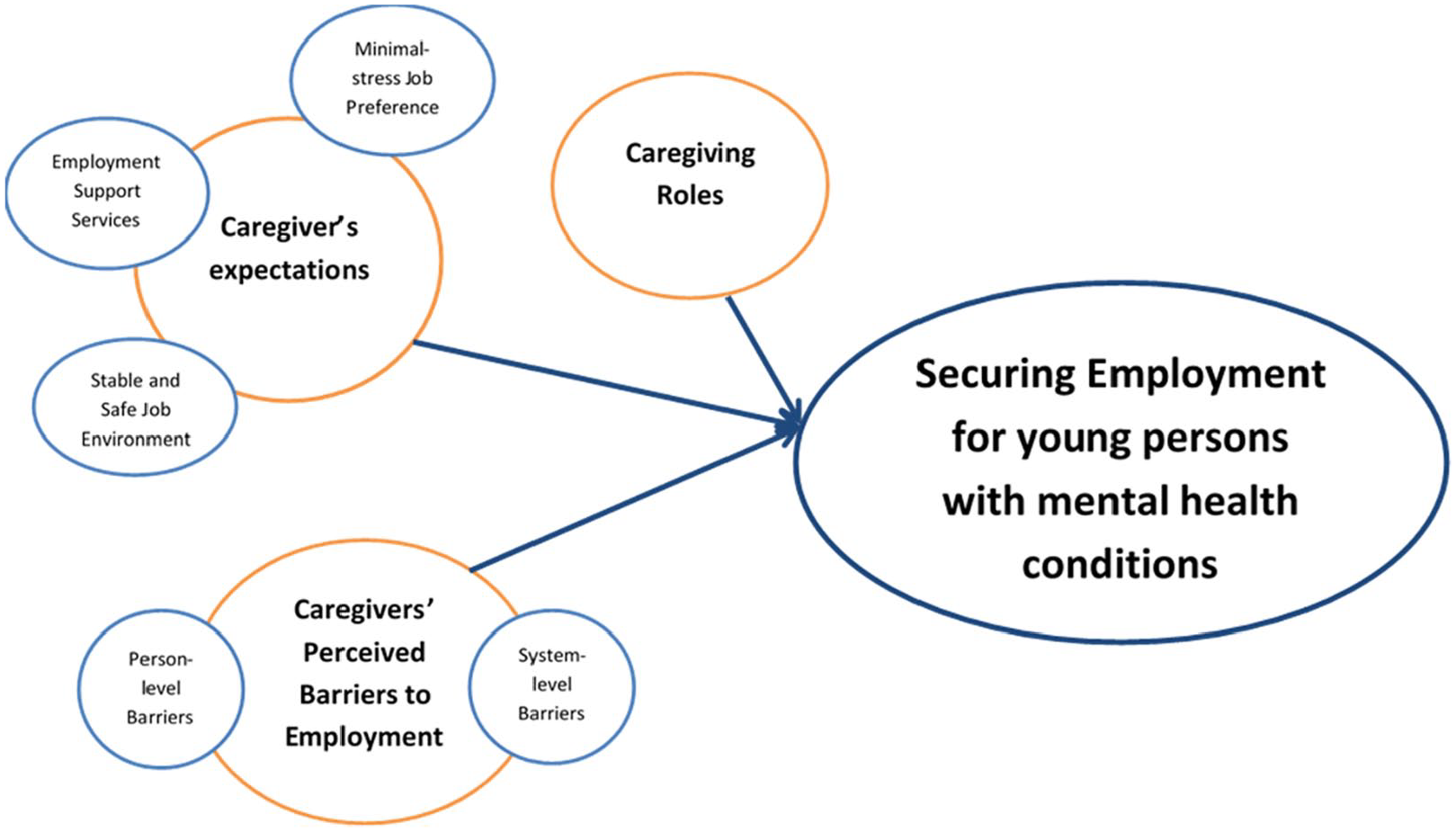
Conceptual model of caregivers’ perceptions of employment for young persons with mental health conditions.
Given the psychological and financial impact of young persons’ illness and dependence on the caregivers, naturally, several expectations from services were expressed. Firstly, caregivers hoped that the available opportunities would meet the young persons’ preferences and strengths to ensure higher job satisfaction and retention. This highlights the importance of appropriate job matching at the entry level. Secondly, concerns regarding the wellbeing and workplace discrimination was evident from caregivers’ narratives. There is a need to provide ‘mentally healthy workplaces’ and conducive environments for young persons with mental health conditions. Suggestions included being in jobs where they had more open and accepting employees or opportunities for ‘job trials’. These suggestions were made due to the underlying concerns that work stress can contribute to relapse (Mazzola et al., 2011). Lastly, societal-level acceptance of mental health conditions was widely expressed as an important factor in fair employment opportunities and practices for young persons with mental health conditions. They highlighted the importance of the need to have concerted efforts to bring about the de-stigmatisation of mental health conditions and/or legal obligations onto employers to foster inclusivity.
Limitations
There are some limitations to this study. First, as the majority caregivers were approached at the psychiatric hospital with their young adult children, these findings may reflect views of caregivers who were supportive of their care-recipient’s needs. In addition to the nature of qualitative research which involves purposive sampling, our findings may not be generalisable to all caregivers of young persons with mental health conditions, as our recruitment was limited to caregivers of those seeking help in a tertiary psychiatric institution.
Conclusion
Informal caregivers assumed multiple roles to assist in securing and sustaining employment and strongly influenced the decisions made by young persons with mental health conditions, thus making them important stakeholders to engage for recovery. In the context of securing employment, caregivers voiced their hopes, expectations and barriers of employment. Local formal mental health employment support services should incorporate the views and expectations of caregivers to foster better coordination with the respective stakeholders, and enhance support for employment and recovery for these individuals.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the National Council of Social Services (NCSS) for the research of this article.