
Abstract
Background and aims:
Interferential care differs from the current community-based care programs in that it targets a larger, heterogeneous group and combines brokerage and full service elements in a multi-organizational care team. The team provides all the services itself, but with the aim to prepare clients within a few months for referral to regular (ambulant) healthcare services. The aim of this study was to assess the effectiveness of interferential care.
Methods:
In a multisite, pretest–posttest design, 523 patients of three interferential care teams were followed. Quality of life, problem severity, problems with referral and engagement were assessed at baseline, at referral and again after 6 months. Analyses were performed using linear mixed modeling.
Results:
Interferential care showed moderate to strong effects on quality of life and problem severity. These effects persisted (quality of life) or further improved (problem severity) until follow-up 6 months after referral to regular services. There were also small effects on both engagement and problems with referral.
Conclusion:
Interferential care offers significant improvements in quality of life and problem severity in persons who have severe problems on several life areas and who are currently not reached by healthcare services. It is a promising community-based care program for healthcare systems in which regular care already contains many elements of home-based practice.
Introduction
Since the deinstitutionalization in the 1960s and 1970s, several community-based care services have been developed for persons with severe mental health problems, such as Assertive Community Treatment (ACT), brokerage and clinical and strengths case management (Bedell, Cohen, & Sullivan, 2000; Burns, 2001; Holloway & Carson, 2001; Rosen, Mueser, & Teesson, 2007). These programs are homogeneous in terms of home treatment function and outreach, but are relatively heterogeneous in other components, such as the amount of services that are brokered or directly provided, and type of services provided (Burns et al., 2001; Rapp, 1998; Test & Stein, 2000; Wingerson & Ries, 1999).
Several studies showed that community-based care improves the living circumstances of individuals with severe mental health problems. The strongest evidence is for the ACT program (Coldwel & Bender, 2007; Marshall & Lockwood, 2011; Rosen et al., 2007). According to a recent Cochrane review, those receiving ACT services were more likely to remain in contact, spent less time in the hospital and had better accommodation, employment status and client satisfaction in comparison to those receiving standard community-based care; no differences were found with regard to mental state and social functioning (Marshall & Lockwood, 2011). However, two problems remain. First, there are indications that in a number of European countries, ACT does not have advantages over care as usual (Burns & Catty, 2002; Burns et al., 2001; Holloway, Oliver, Collins, & Carson, 1995; Kent & Burns, 2005; Killaspy et al., 2006, 2009; Sytema, Wunderink, Bloemers, Roorda, & Wiersma, 2007). Some authors relate this to program fidelity (van Vugt et al., 2011). Others suggest that ACT is just not as effective in Europe as ‘standard’ care already contains many elements of home-based practice. They suggest that different programs are needed in these countries (Burns & Catty, 2002; Burns et al., 2001; Nordén, Malm, & Norlander, 2012). Second, there are concerns about the reach of the current services which are developed by the mental health care and are primarily aiming at persons with severe psychiatric disorders. In the Netherlands, it was estimated that only around a third of the persons that were not reached has severe psychiatric disorders. The others are suffering from severe problems on other areas, like substance use, social isolation and/or homelessness (Lourens, Scholten, van der Werf, & Ziegelaar, 2002; Wolf & Planije, 2004).
Therefore, in the Netherlands a special program fitting better with the context and using broader inclusion criteria was developed: interferential care (bemoeizorg in Dutch; Henselmans, 1993; Kroon, 1996), also referred to as Public Mental Health Care, assertive outreach or intensive community-based care (Roeg, van de Goor, & Garretsen, 2004, 2008; Schout, de Jong, & Zeelen, 2011). Interferential care teams are multidisciplinary and include staff from several organizations, that is, mental health care, addiction care, welfare work, general healthcare services, centers for the homeless and care for the mentally disabled. Staff members include (psychiatric) nurses, social workers, social pedagogical workers and a psychiatrist; in addition, physicians are sometimes involved. Clients do not enroll themselves but are introduced to the team by family members, healthcare institutions, housing corporations and others. Services primarily consist of practical support, such as solving financial, housing, hygiene and social problems. Interferential care differs from the current community-based programs in that it targets a larger group (i.e. not only including persons with severe psychiatric disorders, but also persons with their main problems on other life areas such as mental abilities, social life or housing) and combines elements of the brokerage and full service models in that the multi-organizational care team provides all the services itself, but with the aim to prepare clients within a few months for referral to regular (ambulant) healthcare services. This may address the need for more efficient and effective provision of community-based care in the European context. Interferential care has existed in the Netherlands for over 25 years now, but has not previously been studied longitudinally.
This study investigates the effects of interferential care on problem severity, quality of life and problems with referral and engagement. Also explored are the active ingredients of interferential care by looking at the differences in characteristics and effects between three sites. Finally tested was the influence on the effects of the individual characteristics of the clients, the referring person/organization and the problem areas.
Methods
Study design
A multisite pretest–posttest design was used. Three organizationally independent interferential care teams from different regions in the province of North Brabant in the Netherlands were included: Tilburg, Northeast Brabant and Eindhoven. All clients that entered these interferential care teams between November 2008 and April 2011 were included in the study (n = 523). Outcome measures were quality of life, problem severity, engagement and problems with referral. At baseline, in each team, the coordinator and staff members together filled out the Intensive Community-Based Care Program Components Questionnaire (ICPC) (Roeg et al., 2008). This instrument includes multi-item scales of characteristics found by service providers/managers from different types of programs to be the most important elements of intensive community-based care (Roeg et al., 2008). The results of the ICPC were used to understand what elements contributed to the observed effects, as recommended by a number of authors (Cousins, Aubry, Fowler, & Smith, 2004; Dewa, Horgan, Russell, & Keates, 2001; Hargreaves, Jerrell, Lawless, & Unick, 2007; Rapp, 1998; Rush, Norman, Kirsh, & Wild, 1999).
Intervention
When clients were referred to the interferential care teams, the staff first contacted the nearby healthcare organizations to check whether these clients were already receiving any services. If so, the responsible healthcare provider was contacted. If not, a first inventory of the client’s problems was made and when necessary, a care trajectory was started. Team members shared responsibility for the clients and visited them (often in couples) in their own environment. Considerable attention was paid to making and retaining contact and establishing a bond. Together with the clients, a decision was made regarding what actions were needed. Although staff members could use the power of persuasion, the care was voluntary. The services dealt mainly with practical support, such as help with financial/housing problems, support with hygiene/cleaning, negotiation with the authorities or help with social contacts and/or daily activities. Although clients were not treated by the team, a psychiatrist could be consulted. Clients received support for several months in order to prepare them for referral to regular healthcare services. Because all staff members worked at different healthcare organizations and were deployed at the interferential care team, they had easy access to those regular services. When a client was successfully referred or was able to cope on his own again (with or without help from the personal network), the client was discharged.
Data collection
Data of clients were collected at baseline, at discharge and at 6-months follow-up. These measurements were part of the routine outcome monitoring of the teams. For this study, measurements between the teams were synchronized and a researcher visited the teams monthly to administratively support the data collection. Teams received a small incentive for every complete dataset; in addition, gift vouchers were raffled among the clients. Problem severity and quality of life were assessed on all three occasions, whereas engagement and problems with referral were assessed at baseline and discharge only since they were only applicable during interferential care.
Because data collection was part of the routine outcome monitoring and clients received the services they would normally receive, according to the central commission for human research (CCMO), no medical ethical approval was required for this study. At discharge, clients were notified by their service provider about this study, and they were given the opportunity to refuse to allow their data to be used for this purpose by returning a reply card.
Problem severity was measured with the Health of the Nation Outcome Scales (HoNOS), a 12-item instrument including items on behavioral problems, impairment, symptomatic problems and social problems on a 5-point scale from 0 (no problem) to 4 (severe to very severe problem) (Mulder et al., 2004; Wing et al., 1998). Items are scored by the staff after routine assessment. As recommended, all relevant staff received a 4-hour training from an official HoNOS instructor at the start of the study and again after 6 months (Brooks, 2000). The internal consistency of the HoNOS is moderately high (Cronbach’s alpha = .59–.76) (Mulder et al., 2004).
Engagement with interferential care was measured with the 11-item Engagement Measure. The items included appointment keeping, client–therapist interaction, communication/openness, clients’ perceived usefulness of treatment and compliance with medication; each item was rated by the staff members on a 5-point response scale. The Engagement Measure has demonstrated good internal consistency (alpha = .89), inter-rater reliability (alpha = .95) and test–retest reliability (alpha = .90) (Hall, Meaden, Smith, & Jones, 2001).
Problems with referral were measured on a 3-item scale especially developed for this study; on a 5-point scale, staff members rated whether problems were experienced that (might) cause problems with the linkage to regular services during interferential care. Items included clients’ willingness, and obstacles caused by the healthcare and other organizations. Overall scores range from 0 (no problem) to 12 (severe problem). This new scale showed a satisfactory Cronbach’s alpha of .89 in this study.
Quality of life was measured with the Mansa; this includes 12 items related to obtaining satisfaction on different life domains. The instrument was rated by the client himself on a 7-point response scale ranging from 1 (can’t be worse) to 7 (can’t be better). The Mansa has demonstrated satisfactory internal consistency (Cronbach’s alpha of .74) (Priebe, Huxley, Knight, & Evans, 1999).
Analyses
Differences between teams in client characteristics, referring person/organization and problem areas were tested using analysis of variance (ANOVA) for continuous variables and independence tests for nominal variables. For all three teams, means and standard deviations (SDs) were calculated for the four outcome measures at baseline, discharge and follow-up. Cohen’s d (1988) was calculated using change scores from baseline as effect size measure for each team. Values of Cohen’s d at discharge in a preliminary dataset (n = 27) ranged from .55 for problems with referral to .93 for quality of life. Power analysis using these effect size estimates revealed that 26 (quality of life) to 71 clients (problems with referral) were required per team to obtain a power of .90 to detect an effect of the interferential care. The inclusion period was adapted in order to achieve the required sample sizes in all teams at all moments.
The effects of interferential care on the outcome measures were estimated using linear mixed modeling (Singer & Willett, 2003). Hypotheses were tested using maximum likelihood of the procedure MIXED of SPSS 17.0. In all analyses, an unstructured covariance matrix for the dependence structure was estimated.
Our main hypotheses were tested in three steps. First, the main effect of interferential care on the outcome measures was tested, controlled for team. Second, we assessed whether the effect of interferential care was similar across teams by incorporating the intervention × team interaction in the model. Then, in three separate analyses, we assessed whether different types of predictors explained the outcome measures: (1) client characteristics (age, gender, ethnicity, having children and having a partner), (2) referring person/organization and (3) problem areas. The effect of addiction severity was tested with the corresponding HoNOS item for all outcome measures except for the HoNOS itself. In the third step, only predictors that improved the prediction of the outcome measures were added to the final model. We also tested differences between the three teams with respect to the three types of predictors.
Results
Active ingredients of interferential care
Table 1 shows the characteristics of the three teams as measured using the ICPC. The shared characteristics are printed in bold (i.e. scales on which all three teams score >2 on a scale from 0 to 4). All three teams score relatively high on the following: e.g. objectives: making and remaining contact, client satisfaction and social support; organization: defined service package, staff members are generalistic and being known; staff: personal characteristics and methodological independence; healthcare process: personal (client relation), practical support, problem assessment and linking and care coordination.
Team characteristics of the three interferential care teams measured and compared using the ICPC.

ICPC: Intensive Community-Based Care Program Components Questionnaire; T: Tilburg; N: Northeast Brabant; E: Eindhoven; SD standard deviation.
Scores are scale means per team and indicate whether or not the component is characteristic for that team. Scores range from 0 (not at all characteristic) to 4 (extremely characteristic). Shared scales on which all three teams score of >2 are printed bold and show the characteristics that might be the most active elements of interferential care.
Participant characteristics
The participants had a mean age of 45.7 years and 66.1% of them were male (Table 2). Most clients were Dutch, about 40% had children and 17.7% had a partner. Most common were financial, psychiatric and addiction problems. Clients received on average 7.07 (SD = 5.06) months guidance from the interferential care teams. Table 2 summarizes the results of testing the differences on predictor scores across teams. No association was found between team and referring person/organization (χ2(6) = 7.24, p = .30). Differences across teams were observed for the total number of problem areas (most for team Eindhoven, least for team Tilburg), psychiatric problems (most for team Eindhoven), filthiness/neglect (most for team Eindhoven), social problems (least for team Tilburg) and homelessness (most for team Eindhoven).
Demographic characteristics, referring agents and problem areas of the participants at intake.
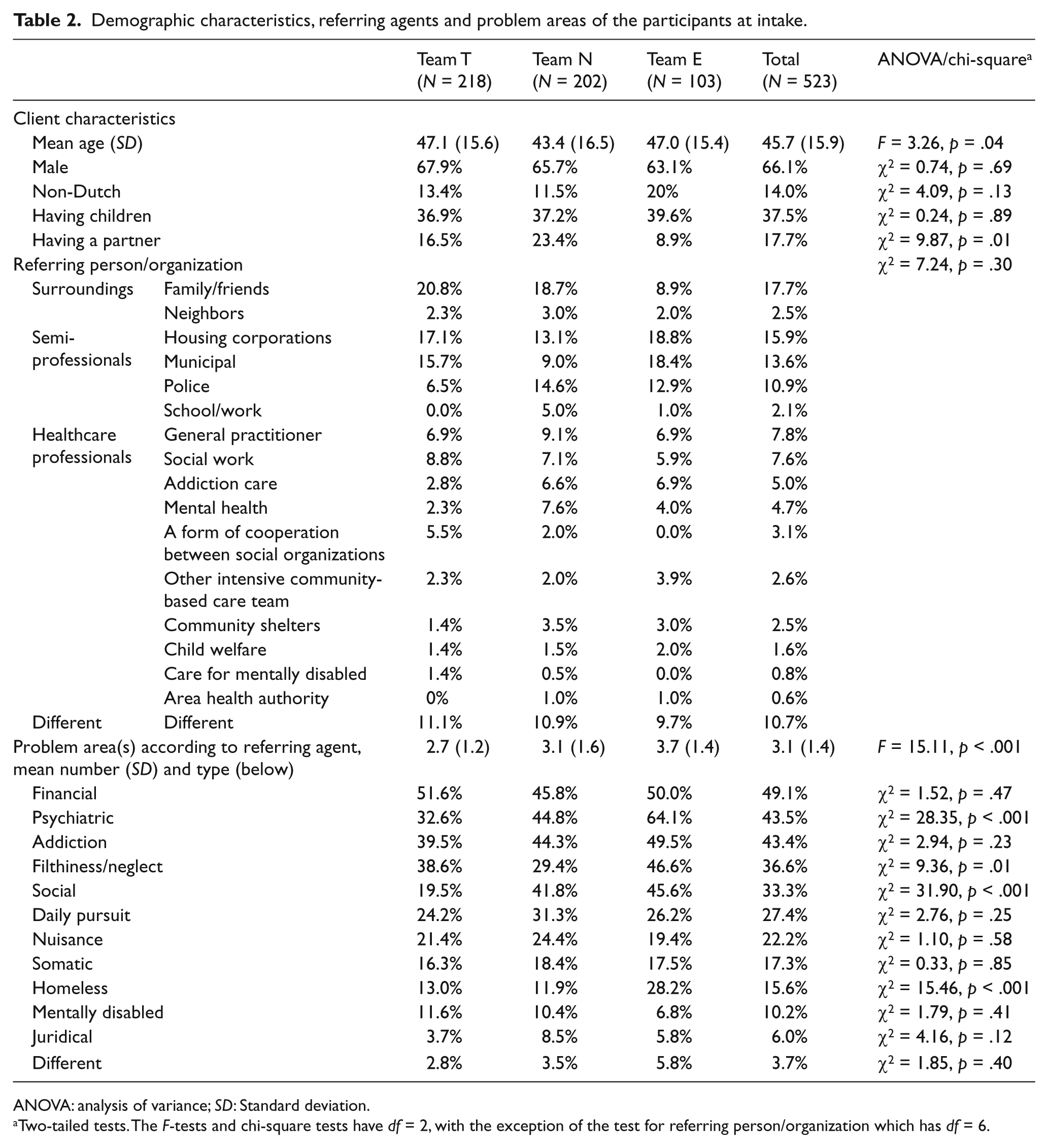
ANOVA: analysis of variance; SD: Standard deviation.
Two-tailed tests. The F-tests and chi-square tests have df = 2, with the exception of the test for referring person/organization which has df = 6.
Table 3 presents the means, SDs and values of effect size measure Cohen’s d for each of the four outcome measures at each time point across all teams and for each team separately. The overall Cohen’s d values indicate moderate effects of interferential care on problem severity at discharge (d = 0.53) and at follow-up (d = 0.72), and strong effects (d = 0.81) on quality of life both at discharge and at follow-up (d = 0.81 and d = 0.92). Furthermore, the results show small effects on both engagement (d = 0.16) and problems with referral (d = 0.18) at discharge.
Means, SD and values of Cohen’s d for each of the four outcome measures at each time point across all teams and for each team separately.
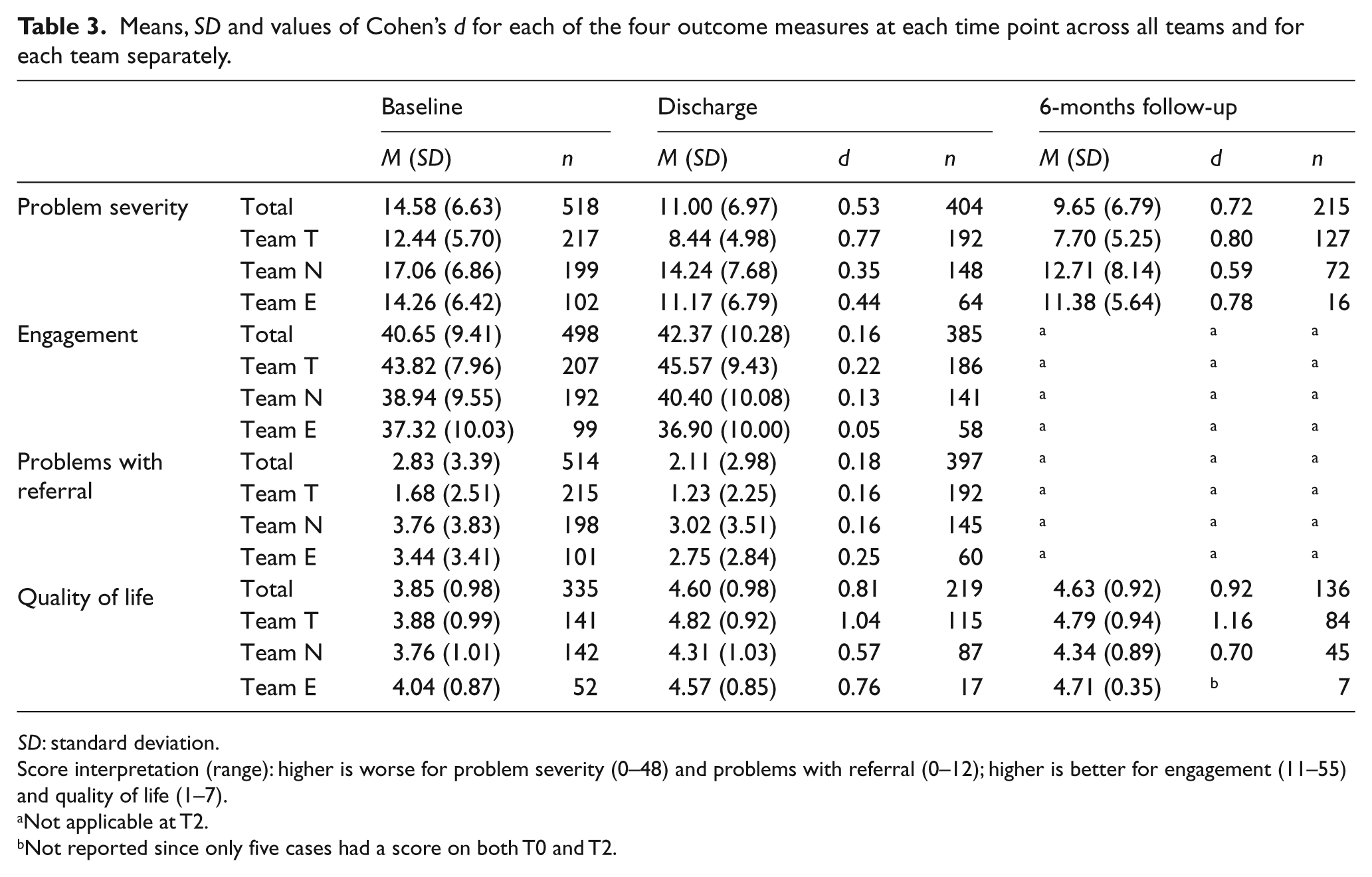
SD: standard deviation.
Score interpretation (range): higher is worse for problem severity (0–48) and problems with referral (0–12); higher is better for engagement (11–55) and quality of life (1–7).
Not applicable at T2.
Not reported since only five cases had a score on both T0 and T2.
Problems with referral, and engagement
After controlling for team, problems with referral were on average 0.57 lower (less problems; t(435.2) = −3.88, p < .001) and engagement 1.30 higher (better engaged; t(392.9) = 2.97, p = .003) at discharge than at baseline. The differences between discharge and baseline did not differ across the three teams for problems with referral and for engagement. The results of the three models with different types of predictors revealed no effect of any client characteristic and no effect of referring person/organization. Effects were found for psychiatric and nuisance problems, addiction severity for problems with referral and engagement and of being homeless for problems with referral only. The final model included the main effects of time and team together, with the effect of the above-mentioned problem areas. The most important results of the final model are summarized in Table 4, showing that after controlling for the effect of the problem areas, problems with referral were .47 lower (p = .002) and engagement 1.14 higher (p = .011) at discharge. Problems with referral were highest for team Northeast Brabant (p = .035), intermediate for team Eindhoven and lowest for team Tilburg (p = .003), whereas engagement was highest for team Tilburg (p < .001) and showed no difference between team Northeast Brabant and team Eindhoven (p = .15) at discharge. Psychiatric problems (p < .001), being homeless (b = .84, p = .01), nuisance problems (b = 0.74, p = .008) problems and addiction severity (p < .001) all increased problems with referral, whereas psychiatric and nuisance (b = −3.42, p < .001) decreased engagement but addiction severity did not (p = .071).
Results of the final model of the linear mixed modeling analyses measuring the effects of interferential care on the outcome measures. a
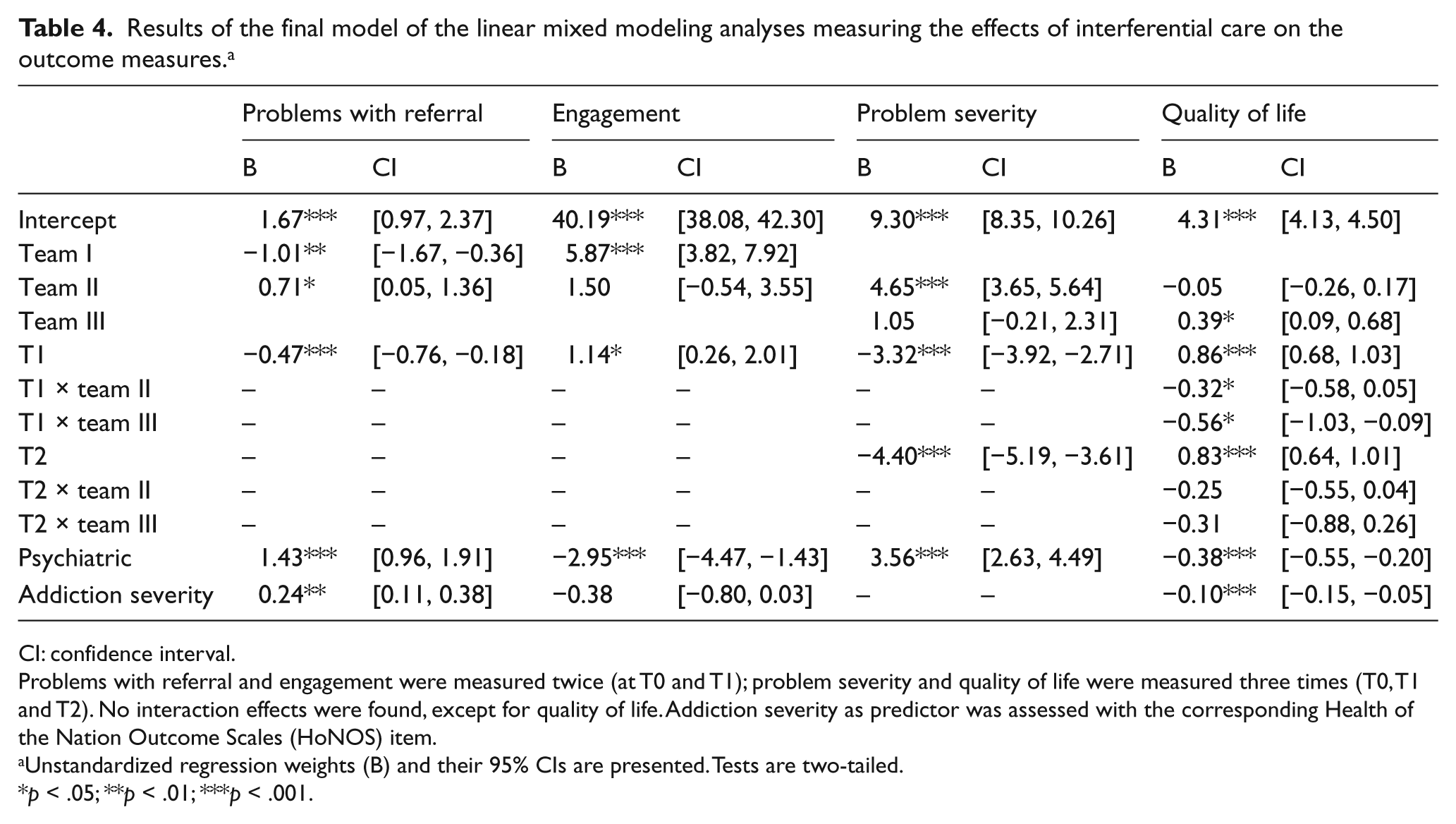
CI: confidence interval.
Problems with referral and engagement were measured twice (at T0 and T1); problem severity and quality of life were measured three times (T0, T1 and T2). No interaction effects were found, except for quality of life. Addiction severity as predictor was assessed with the corresponding Health of the Nation Outcome Scales (HoNOS) item.
Unstandardized regression weights (B) and their 95% CIs are presented. Tests are two-tailed.
p < .05; **p < .01; ***p < .001.
Problem severity
After controlling for team, problem severity was 3.37 lower at discharge than at baseline (t(436.4) = −10.92, p < .001) and 1.02 lower at follow-up than at discharge (t(236.1) = −2.83, p = .005). The intervention × team interaction was not significant (χ2(4) = 4.16, p = .38) indicating that the changes in problem severity over time were equal for all teams. Client characteristics had no effect (all p-values > .05), the effect of referring person/organization was only just significant (χ2(3) = 8.10, p = .04), and an effect was observed for problem areas psychiatric, somatic, mentally disabled, filthiness/neglect, daily pursuit and juridical (p-values < .05). The final model included the main effects of time and team together with the significant problem areas, with the most important results shown in Table 4. These show that after controlling for the effect of the problem areas, problem severity was 3.32 lower at discharge than at baseline (p < .001) and 1.08 lower at follow-up than at discharge (p = .003). Problem severity was highest for team Northeast Brabant, but there was no significant difference between teams Tilburg and Eindhoven (p = .10). Problem areas psychiatric (p < .001), somatic (b = 2.09, p < .001), mentally disabled (b = 2.54, p < .001), filthiness/neglect (b = 1.52, p = .002), daily pursuit (b = 1.36, p = .008) and juridical (b = 2.29, p = .02) all increased the scores on problem severity at all times.
Quality of life
Across teams, quality of life was on average .74 higher at discharge than at baseline (t(248.6) = 11.47, p < .001), whereas at follow-up (.76), it was not different from discharge (t(150.6) = 0.26, p = .80). However, the effect of the interferential care varied across teams (χ2(4) = 10.48, p = .03). The difference in improvement of quality of life between participants of team Tilburg and team Northeast Brabant was significant in favor of team Tilburg both at discharge (b = .41, t(248.1) = 3.05, p = .003) and at follow-up (b = 0.30, t(206.3) = 2.02, p = .04). The difference in improvement of team Tilburg and Eindhoven was similar in size but not significant at discharge (b = 0.43, t(282.9) = 1.82, p = .07) or at follow-up (b = 0.25, t(200.4) = 0.86, p = .39) due to the lower number of participants in team Eindhoven. Of the client characteristics only ethnicity had an effect, that is, non-Dutch participants scored lower. Referring person/organization had no effect (χ2(3) = 3.48, p = .32), whereas problem areas psychiatric, somatic, daily pursuit and addiction severity did (all p-values < .05). The final model estimated included the main effects of both the intervention and the team, their interaction and the above-mentioned significant predictors. The estimates in Table 4 reveal that after controlling for the other predictors, quality of life was .39 higher at baseline in team Eindhoven than in team Tilburg (p = .01). Improvement in quality of life at discharge was .56 lower in team Eindhoven (p = .02) and .32 lower in team Northeast Brabant (p = .02), but not significantly lower at follow-up in both teams. Non-Dutch participants scored .46 lower (p = .001), and negative effects were observed of psychiatric (p < .001), somatic (b = −0.24, p = .03), daily pursuit (b = −0.26, p = .008) problems and addiction severity (p < .001).
Analysis showed no differences between responders and nonresponders, at both discharge and follow-up, for age, problem severity and quality of life. Small to very small differences were found for engagement and problems with referral (η2 = .008–.01).
Discussion
In this study, interferential care had a significant effect on all outcomes assessed: problem severity, quality of life, problems with referral and engagement. This finding is encouraging. The observed improvements are especially relevant as the baseline situation of the clients with regard to their quality of life and problem severity showed to be poor compared with other ambulatory and intensive community-based clients, both in the Netherlands and the United Kingdom (Killaspy et al., 2006; Mulder et al., 2004; Priebe et al., 1999; Sytema et al., 2007).
The effects of interferential care on problem severity and quality of life were relatively high (medium to strong), and they persisted (quality of life) or even improved further (problem severity) after referral to regular services. Comparable improvements on problem severity at discharge were seen in the United Kingdom in programs for psychiatric patients: both in an ACT team and in a community mental health team (CMHT) (Killaspy et al., 2006). A Dutch study on ACT for persons with early psychosis also showed some smaller, but nevertheless moderate, effects. This indicates that with regard to problem severity, interferential care has comparable results as do the programs for psychiatric patients studied in the United Kingdom and the Netherlands.
The increase in quality of life is noteworthy because no improvement in quality of life was reported earlier in ACT or CMHT, either in the United Kingdom (Killaspy et al., 2006) or in the Netherlands (Sytema et al., 2007). Small effects on quality of life were previously found in an ACT program for persons with early psychosis (Verhaegh, Bongers, Kroon, & Garretsen, 2007) and moderate to large effects in a client-based community-based care program for psychiatric patients (Nordén et al., 2012).
The effects of interferential care on engagement and problems with referral were also significant, but had a smaller effect size. At baseline, the clients showed progressively good engagement, indicating that as soon as they were in contact, they were willing to cooperate with the team members. This could not be explained by selection bias as all clients entering the interferential care teams were included in the study. The findings therefore suggest that these clients are not as care-avoiding as thought, but that there are other reasons why they are not making use of the available services, for example, too difficult to get or stay in (e.g. due to waiting lists, administration, keeping appointments and get to the office), or services are not adjusted to their problems (multiple in nature), as was suggested by Schout et al. (2011).
The effects on all outcomes were almost the same for all three teams: the one difference found (i.e. improvement of quality of life was larger in one team than in the other two teams at discharge) had disappeared at follow-up. No comparison could be made to a control group, so it is unknown whether interferential care shows better results than alternatives. However, the fact that three organizationally separate interferential care teams show the same results on four different outcome measures is promising and supports the idea that this type of community-based care helps realize improvements in the living circumstances of individuals that are currently not reached by healthcare services. The multisite design also provides us with first indications about the components of interferential care that are likely to have contributed to the effects. These are the components assessed with the ICPC that are shared by all three teams. These components might be the most active ingredients of interferential care.
The finding that neither the client characteristics nor the referring person/organization influenced the effects on the four measures indicates that the approach and service package used can be the same for all clients within the team. There was one exception: being non-Dutch negatively influenced the quality of life. For this variable, investigation of the mechanism behind this relation might offer a solution for this difference in the future. Most problem areas as measured at baseline had a detrimental effect on one or more of the clients’ outcomes, with the exception of financial and social problems. This indicates that it might be relevant for team members to adapt their working strategy to the type of problems that specific clients are referred for.
Study limitations
Effects were measured with a pretest–posttest design without a control group. Therefore, it should be taken into account that the effects found may (partially) be the result of statistical regression to the mean. To compensate, natural selection for sampling was used which is known to reduce the risk of regression to the mean (Barnett, van der Pols, & Dobson, 2004). Second, although staff-rated measures on clients’ clinical situation have long been accepted as outcomes in effect studies, we recognize that these measures might be subject to (sub)conscious bias. It seems unlikely, however, that this influenced the present findings as there were relatively large differences in effect size between the three staff-rated measures (problem severity, problems with referral and engagement). Furthermore, not only staff-rated but also client-rated outcomes were included, and both improved. Third, there were differences in dropout rates, that is, the follow-up response rate in team Eindhoven was low. This should be taken into account when comparing the three teams on their effects. The response rates in the other two teams, however, were good as well as their overall response rate, supporting the overall findings.
Conclusion
The findings of this study suggest the effectiveness of interferential care as a model for community-based care developed for European healthcare systems in which the regular care already contains many elements of home-based practice. The findings imply that interferential care contributes to improvements on both quality of life and reduction of problem severity. These effects remain at least till 6 months after referral to regular services. Small improvements on engagement and problems with referral also emerged.
Footnotes
Funding
This work was supported by ZonMw, The Netherlands Organisation for Health Research and Development (grant number 31160001).