
Abstract
Many of the simple and low-cost child diarrhea morbidities interventions, such as adequate home care, access to health care services, and improved sanitation and hygiene practices, are far beyond the reach of many households in developing countries, and Namibia is not an exception to this. In this study, a quantitative cross-sectional study design using a multivariable log-binomial model was used to examine the effect of household demographic characteristics on diarrhea morbidity in children aged zero to 48 months using data collected from the 2013 Namibia Demographic and Health Survey. Household demographic characteristics such as household's wealth index and main language spoken at home had lower risks on child diarrhea morbidity, while characteristics such as age of household head, toilet facilities shared with other households, current age of child, residency of the child, and child vaccination status had higher risks. The Namibian government, together with nongovernmental organizations, should make necessary vaccines interventions compulsory to prevent diarrheal diseases during the first few years of the child's life and continuously enhance initiatives that invest in good sanitation and hygiene infrastructure within Rukwangali- and Lozi-speaking communities in the country.
Diarrhea in children under age five remains one of the significant public health concerns in developing countries and an important cause of morbidity and mortality among children in these countries. Even with much progress made in the reduction of diarrhea burden, especially among children younger than five years, diarrhea morbidity still remains a leading cause of death and morbidity among these children. 1 Even though diarrhea is the body's way of ridding itself of germs, with most episodes lasting a few days to a week, 2 its diseases account for one in nine child deaths worldwide, making diarrhea the second leading cause of death among children under the age of five. 3 In 2017, diarrhea accounted for approximately 8 percent of all deaths among children under age five worldwide, which translated to more than 1,400 young children dying each day or approximately 525,000 children per year. 4 Despite the availability of simple, effective treatments, diarrhea disease is still a major cause of mortality in children under age five in developing countries, contributing to up to 21 percent of deaths. 5 In most high-income countries in Europe and Asia regions, the diarrhea morbidities in children were reportedly below one per 100,000 cases per year, while in low-income countries, the death rate was estimated to be higher than 300 per 100,000 cases per year, especially among the poorest countries with few resources and less robust health infrastructure systems, such as Madagascar, Chad, and the Central African Republic. 6 Approximately 90 percent of the global diarrhea deaths reported occurred in South Asia, Southeast Asia, and Sub-Saharan Africa, with more than one-quarter occurring among children younger than five years. 1 In Namibia, the national prevalence of diarrhea morbidity stood at 17 percent, with 40.2 per 1,000 live births, and it was responsible for 5 percent of all deaths in children under five, making it the second leading cause of child death in the country.4,7
Various studies have indicated that epidemiologic factors that contribute to the occurrence of diarrhea morbidity in children were complex in nature. These included factors such as residential area, household structure, unemployment, household income, mother's/caregiver's age, number of people per household, access to information, type of toilet facilities, access to safe drinking water, child immunization status, nutritional status, and number of sleeping rooms in the household, as illustrated in Figure 1. Moreover, diarrhea morbidities in children are treatable and preventable through simple measures such as vaccination; adequate home care; access to health care services; improved water, sanitation, and hygiene practices; and better nutrition. 8 However, many of these simple and low-cost interventions are far beyond the reach of many households in developing countries, and Namibia is not an exception to this. Hence, the main objective of this study was to examine the effect of household demographic characteristics on diarrhea morbidity in children aged 0 to 48 months in Namibia. Findings from this study will provide useful insights for evidence-based health policies and programs on diarrhea morbidity among children in the country, thereby further aiding in the effective allocation and utilization of public health programs and resources in the prevention of diarrhea mortality among children within the country.
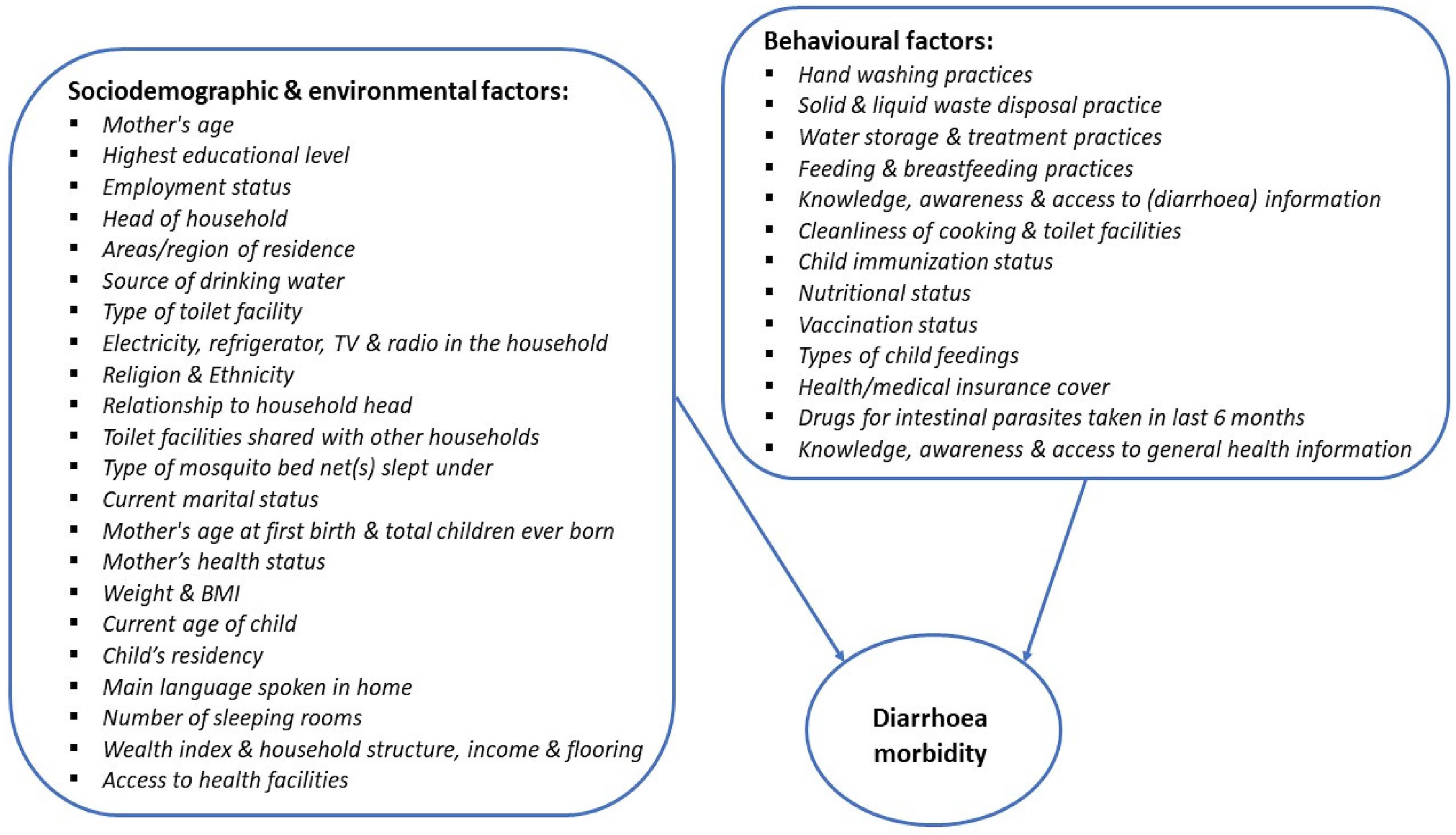
Theoretical model for some of the factors contributing to child diarrheal prevalence.
Material and Methods
The data used in this study were obtained from the 2013 Namibia Demographic and Health Survey (NDHS). The Demographic and Health Survey (DHS), funded by the U.S. Agency for International Development, is part of the worldwide measure DHS programs designed to collect information on fertility, family planning, infant and child mortality, maternal and child health, nutrition, domestic violence, and knowledge and prevalence of Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) and other noncommunicable diseases, which allows monitoring progress through time with respect to these issues and provides an international database that can be used by researchers investigating topics related to population, health, and nutrition. 9 The 2013 NDHS is the fourth and latest comprehensive, national-level population and health survey conducted in Namibia in collaboration with the Ministry of Health and Social Services as part of the global DHS program, with the study initiated in April 2012 and the data collection aspect carried out from May to September 2013. 9
The sampling design used in the 2013 NDHS was designed to provide estimates of most key variables for all of the then-13 administrative regions in Namibia. 9 Currently, Namibia has 14 administrative and official regions, after the Kavango region was split into Kavango East and Kavango West. More detailed information about the sampling methods and the entire survey can be found in the 2013–2014 NDHS report, freely available online on the DHS website. Furthermore, the 2013 NDHS data were obtained after the author of this study completed the mandatory user's agreement of the DHS program online, via the DHS website. No separate permission was required for the DHS data usage and resulting study publications. The inclusion criteria for this study were all children aged 0 to 48 months whose mothers participated and provided information for them in the 2013 NDHS. Children with incomplete, non-response, or missing information were excluded from this study.
Descriptive Analysis
The household demographic characteristics considered in this study were the age of household head, toilet facilities shared with other households, household's wealth index, current age of child, residency of the child, child vaccination status, and main language spoken at home. The individual children considered in this study were identified from the NDHS as per the inclusion criteria for this study. The responses to question such as “Has (NAME) had diarrhea in the last two weeks?” as captured in the NDHS data were used to determine the children's diarrhea morbidity status in this study. Similarly, the responses to the “Did you ever have a vaccination card for (NAME)?”, “Do you have a card where (NAME)'s vaccinations are written down?”, “Has (NAME) had any vaccinations that are not recorded on this card, including vaccinations given in a national immunization day campaign?”, and “Did (NAME) ever have any vaccinations to prevent him/her from getting diseases, including vaccinations received in a national immunization day campaign?” questions as captured in the NDHS data were used to determine the children's vaccination status in this study. More detailed information about these demographic characteristics and the remaining characteristics considered in this study can be found in the 2013–2014 NDHS report, freely available online on the DHS website.
Statistical Analysis
Pearson's chi-square test was performed to examine the association between the household demographic characteristics and diarrhea morbidity among children aged 0 to 48 months. Moreover, the effect of the household demographic characteristics on child diarrhea morbidity was determined using a multivariable log-binomial model. This model uses a log-link function to connect a set of predictor variables
Results
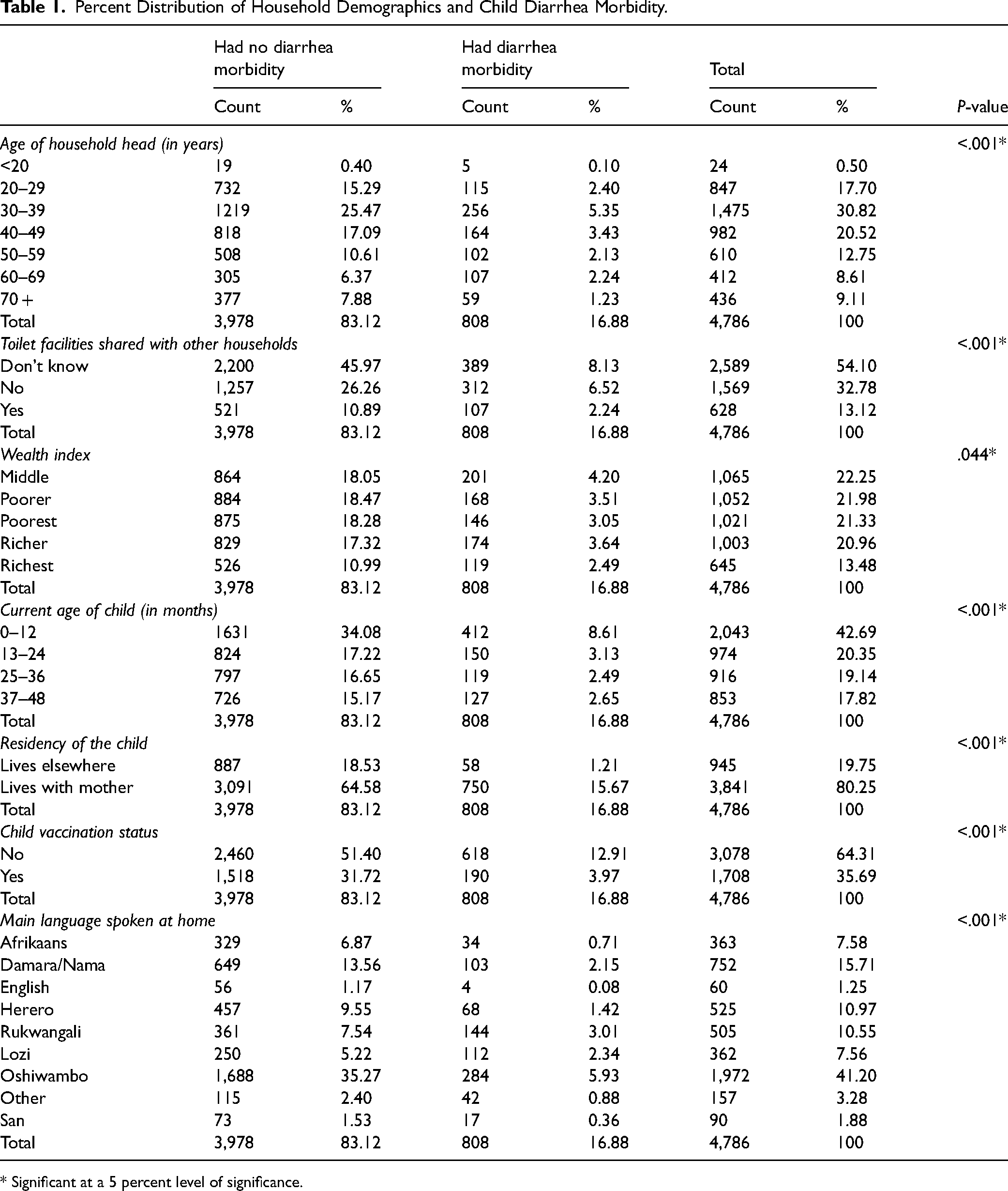
As per the inclusion criteria of this study, a total of 4,786 children aged 0 to 48 months old were considered, out of whom 808 (16.88%) had diarrhea morbidity and 3,978 (83.12%) did not have diarrhea morbidity, as shown in Table 1. With respect to household demographic characteristics, out of the 808 children who had diarrhea morbidity, the majority were aged 0 to 12 months old, were not vaccinated, and lived with their mothers in middle wealth-indexed households headed by persons who were 30 to 39 years old. Likewise, the majority were from households that did not know if they shared toilet facilities with other households and spoke Oshiwambo as their main language in their respective homes.
Percent Distribution of Household Demographics and Child Diarrhea Morbidity.
* Significant at a 5 percent level of significance.
Associations Examination
From Table 1, at a 5 percent level of significance, the age of household head (P-value <.001), toilet facilities shared with other households (P-value <.001), wealth index (P-value = .044), current age of child (P-value <.001), residency of the child (P-value <.001), child vaccination status (P-value <.001), and main language spoken at home (P-value <.001) can be concluded to have a significant association with diarrhea morbidity among children aged 0 to 48 months old. All these characteristics with significant associations were included in the fitted multivariable log-binomial model, with the subsequent results shown in Table 2.
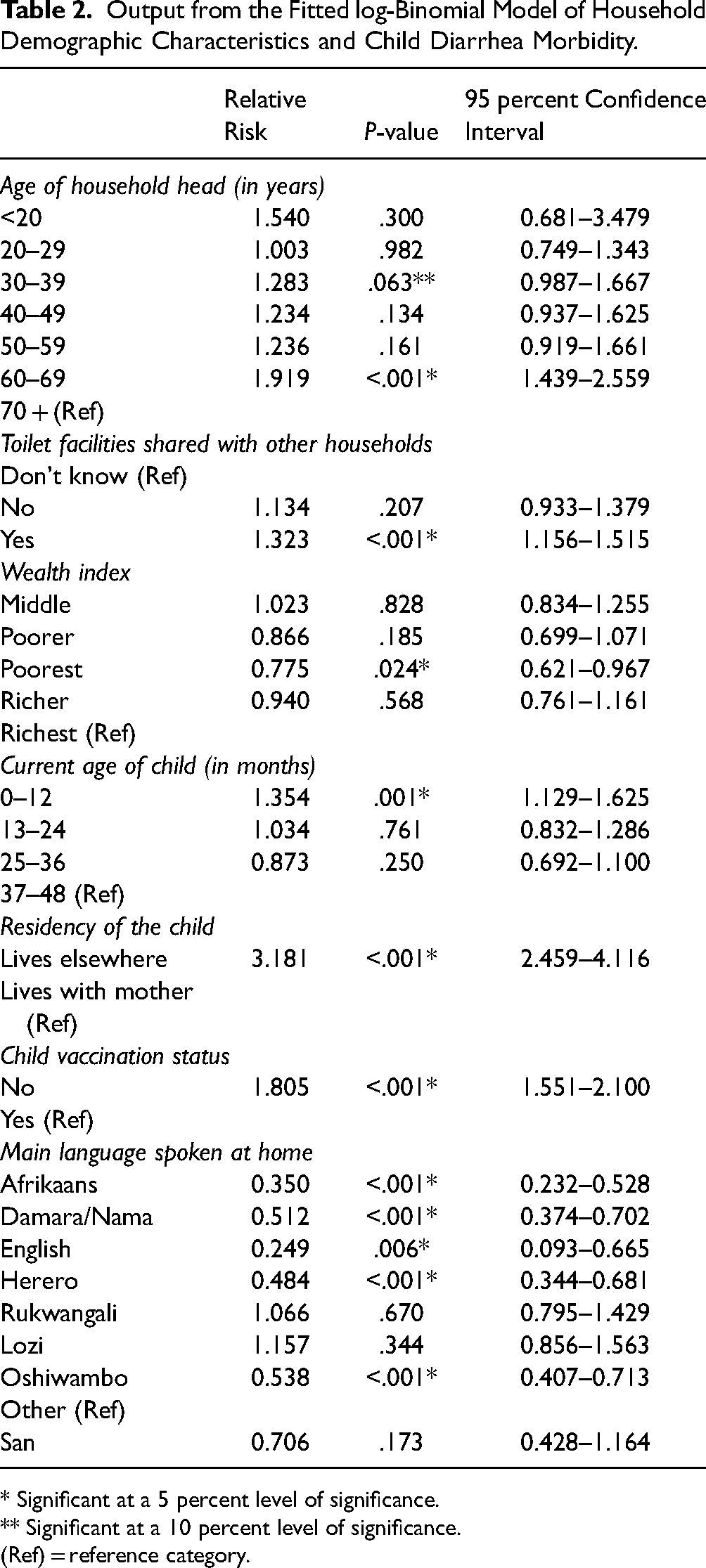
Output from the Fitted log-Binomial Model of Household Demographic Characteristics and Child Diarrhea Morbidity.
* Significant at a 5 percent level of significance.
** Significant at a 10 percent level of significance.
(Ref) = reference category.
Effect on Child Diarrhea Morbidity
From Table 2, with a significant P-value at a 5 percent to 10 percent level of significance, it can be concluded that the risk of diarrhea morbidity for a child living in a household headed by a 30- to 39-year-old person (RR = 1.283; P-value = .063; 95% CI:0.987–1.667) and a 60 to 69 years old person (RR = 1.919; P-value <.001; 95% CI:1.439–2.559) was between 1.28 and 1.92 times higher compared to the risk for a child living in a household headed by a 70 + years old person. Likewise, the risk for a child living in a household that shares its toilet facilities with other households (RR = 1.323; P-value <.001; 95% CI:1.156–1.515) was 1.32 times higher compared to the risk for a child living in a household that does not know if they shared their toilet facilities, while the risk for a child aged 0 to 12 months (RR = 1.354; P-value = .001; 95% CI:1.129–1.625) was 1.35 times higher compared to the risk for a child aged 37 to 48 months.
Moreover, the risk of diarrhea morbidity for a child living in a poorest wealth-indexed household (RR = 0.775; P-value = .024; 95% CI:0.621–0.967) was 0.78 times lower compared to the risk for a child living in a richest wealth-indexed household, while the risk for child living in a household whose main language spoken in the house was English (RR = 0.249; P-value = .006; 95% CI:0.093–0.665), Afrikaans (RR = 0.350; P-value <.001; 95% CI:0.232–0.528), Herero (RR = 0.484; P-value <.001; 95% CI:0.344–0.681), Damara/Nama (RR = 0.512; P-value <.001; 95% CI:0.374–0.702), or Oshiwambo (RR = 0.538; P-value <.001; 95% CI:0.407–0.713) was between 0.25 and 0.54 times lower compared to the risk of diarrhea morbidity for a child living in a household who spoke other languages, as shown in Table 2. However, the risk for a child who did not live with his/her mother (RR = 3.181; P-value <.001; 95% CI:2.459–4.116) was 3.18 times higher compared to the risk for a child who lived with his/her mother, while the risk for a child who had not been vaccinated (RR = 1.805; P-value <.001; 95% CI:1.551–2.100) was 1.81 times higher compared to the risk for a child who had been vaccinated.
Discussion
In this study, the effect of household demographic characteristics on diarrhea morbidity in children aged 0 to 48 months in Namibia was estimated using a multivariable log-binomial model. The majority of the children who had diarrhea morbidity were aged 0 to 12 months old, were not vaccinated, and lived with their mothers in middle wealth-indexed households headed by persons who were 30 to 39 years old and spoke Oshiwambo as their main language in their homes. Diarrhea morbidity was more likely to occur in children who were living in households headed by persons 30 to 39 years old and by persons 60 to 69 years old who share toilet facilities with other households. Likewise, the morbidity was more likely to occur in children aged 0 to 12 months who did not live with their mothers and had not been vaccinated. However, the morbidity was less likely to occur in children who were living in poorest wealth-indexed households and whose main languages spoken in the house were English, Afrikaans, Herero, Damara/Nama, or Oshiwambo.
These findings are not surprising. Children with older mothers/caretakers/guardians are often associated with higher likelihoods of diarrhea morbidity than their young(er) counterparts due to the fact that as the mothers/caretakers/guardians get older, they are more prone to contracting adult-related health illnesses or diseases such as diabetes, high blood pressure, and hypertension (to mention a few), thereby affecting their immune system and weakening their abilities to properly care for the child(ren) under their care. 11 This also agrees with Omona and colleagues, 5 whose findings showed that children whose caretakers were older had 12 to 14 times higher odds of diarrhea morbidity than their younger counterparts. In addition, it is well-known that facilities such as toilet, bathroom, and kitchen areas shared by several households of different family sizes tend to have reduced cleanliness, thus increasing the risk of diarrhea morbidity. This also concurs with Omona and colleagues, 5 who revealed that a high number of individuals in a household sharing the same facilities potentially compromises hygiene and sanitation, thereby making the children living in such households more prone to contacting diarrheal pathogens and morbidities.
Furthermore, the high risk of diarrhea morbidity in children aged 0 to 12 months can be attributed to the fact that most of them were primarily being fed breastmilk, which contains antibodies that helps protect against many common childhood illnesses while providing all the energy and nutrients that the children need, especially, for the first months of their lives. 12 However, the current health statuses and underlying illnesses of the breastfeeding mothers can contaminate the quality of the breastmilk during feeding, especially mothers living with infectious illnesses such as HIV, hepatitis B virus, hepatitis C virus, cytomegalovirus, West Nile virus, and human T-cell lymphotropic virus, thereby making the children more prone to contacting diarrheal morbidities. Similarly, previous diarrheal diseases-related studies such as those by Dadonaite 6 and the World Health Organization, 8 showed that vaccination was another way of preventing and protecting children against diarrheal-related diseases and mortality, with Dadonaite 6 concluding that vaccination combined with other sanitary measures was a more cost-effective means of protecting children against diarrhea morbidity.
Moreover, the low risk of diarrhea morbidity in children living in households whose main languages spoken in the house were English, Afrikaans, Herero, Damara/Nama, or Oshiwambo can be attributed to the fact that the majority of the sponsored health information meant to raise awareness on healthy societal issues were most often written and translated in these languages, which were already familiar to and popular in most communities in Namibia, especially for mothers/caretakers/guardians in some of these communities, who are less educated and do not know how to read or write even in their own local languages. This finding further agrees with Omona and colleagues, 5 who concluded that less informed people were less likely to take their own and their children's hygiene and sanitation seriously.
Conclusion
With household demographic characteristics such as age of household head, toilet facilities shared with other households, current age of child, residency of the child, and child vaccination status creating more risks of child diarrhea morbidity, while characteristics such as household's wealth index and main language spoken at home had fewer risks, together with continual assistance from nongovernmental organizations, health care providers, and clinical facilities, it can be recommended that the Namibian government: (a) provide and make necessary vaccines interventions (such as rotavirus vaccines and cholera vaccines) compulsory to prevent diarrheal morbidities and diseases during the child's first few years, (b) increase the adoption of proven measures against diarrhea morbidity (such as vaccination, exclusive breastfeeding, oral rehydration therapy, and household and community sanitation systems), (c) continuously enhance initiatives that invest in good sanitation and hygiene infrastructure in communities, especially in the Lozi- and Rukwangali-speaking communities, and (d) continually educate (low-income) households on the importance of good sanitation and hygiene, especially in the country's unpopular and indigenous spoken languages, such as Lozi and Rukwangali. This can easily be achieved through constant engagements and collaborations with community-based organizations such as churches, traditional authorities, community leaders, local authorities, and regional councils for assistance when needed. Moreover, further studies on this topic are recommended using data from the next NDHS, pending available funding from the sponsors.
Limitations
The majority of the questions in the 2013 NDHS questionnaire relied heavily on memory recall of the participating mothers, which could have led to the possibilities of systematic under-reporting of some family sociodemographic characteristics and information. In addition, the NDHS information on the diarrheal history of the children was obtained based on the self-reported responses from mothers’ recollection of the diarrheal history of their children within the last two weeks preceding the interview day(s) of the mothers. As such, children who had multiple diarrhea morbidities prior to the last two weeks preceding the interview day(s) of their mothers would have been classified as having no diarrhea morbidity in the NDHS. Moreover, although the NDHS had some questions centered around health care services, drinking water, types of feeding, toilet structure, and so on, it did not specifically cater to diarrhea-specific treatment therapies. Thus, separating diarrhea morbidity between children from households that could afford diarrhea treatment therapies and those that could not afford them would have been ideal to study; however, doing so from the NDHS data was not feasible.
Footnotes
Acknowledgments
The U.S. Agency for International Development is thanked for availing the 2013 NDHS data.
Author Contributions
OO initiated the study, acquired, and analyzed the data; reviewed the literature; carried out the statistical and data interpretation and contextual writing at all stages of the manuscript writing; and wrote the manuscript. OO also read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethical Clearance
Ethical clearance for this study was obtained from the University of Namibia Ethics Committee in accordance with the University of Namibia's Research Ethics Policy and Guidelines. The 2013 NDHS data that were used in this study are freely available on a public domain and downloadable from the DHS website, after the completion of a user's agreement and the granting of access. No separate permission is required for data usage and publication. Additionally, this study followed all ethical standards for research without direct contact with human or animal subjects as there were no names of persons or household addresses recorded in the DHS data.