
Abstract
The commercial determinants of health (CDoH) describe the adverse health effects associated with for-profit actors and their actions. Despite efforts to advance the definition, conceptualization, and empirical analyses of CDoH, the term's practical application to mitigate these effects requires the capacity to measure the influences of specific components of CDoH and the cumulative impacts of CDoH on the health and well-being of specific populations. Building on the Global Burden of Disease Study, we begin by conceptualizing CDoH as risk factor exposures that span agency and structural influences. We identify 6 components of these influences and propose an initial set of indicators and datasets to rank exposures as high, medium, or low. These are combined into a commercial determinants of health index (CDoHi) and illustrated by 3 countries. Although now a proof of concept, comparative analysis of CDoH exposures by population, over time and space, and their associated health outcomes will become possible with further development of indicators and datasets. Expansion of the CDoHi and application to varied populations groups will enable finer targeting of interventions to reduce health harms. The measurement of improvements to health and wellness from such interventions will, in turn, inform overall efforts to address the CDoH.
Introduction
Over the past decade, the commercial determinants of health (CDoH) have attracted increasing attention in public health research, policy, and practice. While much of the CDoH scholarship to date is focused on “unhealthy commodity industries” (such as tobacco, alcohol, and ultra-processed food) and their impact on the rapid rise of noncommunicable diseases (NCDs) worldwide,1,2 recent analyses have broadened to other industries (such as motor vehicles, pharmaceuticals, and gambling) and their wider health impacts.3–5 Reviews of the expanding CDoH literature support locating commercial influences in historical and contemporary contexts, as well as closer integration of this growing body of work across industries, geographies, levels of analyses, and disease outcomes.6–8 From our conceptual review of this literature, within the context of historical and contemporary capitalism, we define CDoH as “the ways in which actors (through market and nonmarket strategies) and structures (stratification, systems, organization, culture, and regulatory frameworks and governance) operate to generate profit, and thereby influence patterns of health, disease, injury, disability, and death within and across populations.” 9
The purposes of this article are to further enhance the analytical and practical value of this term and to support the deeper development of “concepts, theories, frameworks, and methods for the study of CDoH.” 2 As de Lacy-Vawdon and Livingstone observe, “social, political, commercial, and economic structures and relations of CDoH are under-theorized.” 6 Moreover, there is a need to apply expanded theorizing to more fully assess the practices of commercial actors, alongside the “deeper societal factors” 10 that sustain and promote these practices. For this purpose, some scholars have linked CDoH to wider concepts of power11,12 and complex systems thinking. 7
As a contribution to this growing scholarship, we begin by arguing that traditional public health approaches lead to a narrow conceptualization of CDoH focused on the production and consumption of specific unhealthy products. This body of work tends to cast CDoH largely as a subset of social determinants of health (SDoH), 6 leading to resignation that the pathways between CDoH and health outcomes are too diffuse and complex to understand, let alone address, with targeted interventions.
In this article, we propose an alternative approach that seeks to assess CDoH as exposures within a given society encompassing proximal and distal health determinants. We identify 6 key components of CDoH and, for illustrative purposes, provide examples of potential indicators and datasets to rank each component for a given country. We argue that these rankings can then be combined to measure aggregate exposures to CDoH. We conclude that this approach encourages a more integrated understanding of the influences of CDoH through agency and structure. This approach, in turn, can serve as a starting point for comparative analyses across countries to explain how varying levels of exposure to CDoH might explain different patterns of health and disease. Finally, identification of exposures to specific CDoH components can inform the targeting of strategies and interventions to mitigate them. 13
CDoH as Proximal and Distal
The Global Burden of Disease (GBD) study was the first to combine mortality and morbidity statistics into a single summary measure of population health for the world. The ability to compare across countries and regions, and to understand patterns and trends over time, was previously hindered by a lack of standardized definitions, measures, and data. The lack of comparable and longitudinal data across all countries, in turn, posed challenges for setting priorities. 14 The disability-adjusted life year as a unit of measure, defined as “years of life lost from premature death and years of life lived in less than full health,” 15 filled this critical gap. The result was increased attention to conditions that impact morbidity (healthy years lost), including hitherto neglected conditions such as mental health and injuries.
A key contribution of the GBD study is the association of different categories of risk factors with health outcomes. A risk factor is defined by the World Health Organization (WHO) as “a factor that raises the probability of adverse health outcomes.” 16 Over time, the number of risk factors identified by the GBD study has increased, from 22 (organized into 6 categories) in 1993 17 to 87 (organized into 4 levels) in 2020.18,19 Recognizing that potentially countless risk factors could be identified, the GBD study has focused on “selected risk factors which have global spread, for which data are available to estimate population exposures or distributions, and for which the means to reduce them are known.” 16 Risk factors are defined as proximal determinants of health (Figure 1) because they have a more direct (or downstream) impact on disease/injury and death. Proximal risk factors relate to biology (eg, hypertension) and behaviors (eg, smoking), along with relatively direct exposures (eg, air pollution). Distal causes, by contrast, refer to the socioeconomic and environmental determinants that shape proximal risk factors. Bringing together globally comparable data on “the relative contributions of different diseases, injuries, and risk factors to overall population health,” 20 and their association with proximal risk factors and distal determinants, the goal of the GBD study is “to support policy decisions in the allocation of resources for prevention, health care, and research.” 20
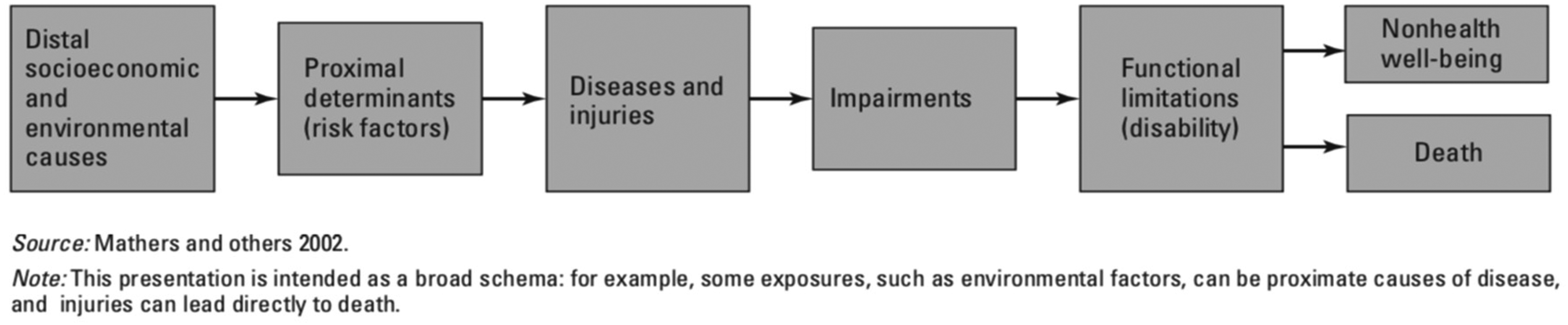
Overview of global burden of disease framework.
The GBD study drew important attention to the steady rise in NCDs since the 1990s. Between 1990 and 2019, NCDs are estimated to have increased from 43% to 54% of the GBD. 21 NCDs now account for 71% of total deaths worldwide, with 81% of those deaths caused by 4 disease types (cardiovascular diseases, diabetes, cancers, and chronic respiratory diseases). This is expected to rise to more than 85% by 2030. 22 Efforts to address the growing global burden of NCDs have included the WHO Framework Convention on Tobacco Control (FCTC) (2003), United Nations Political Declaration on NCDs (2011), and follow-up WHO Global Action Plan for the Prevention and Control of NCDs (2013), together with numerous regional initiatives. 23
While increased attention to this epidemiological transition in many countries was much needed, understanding of the causal factors and development of appropriate interventions to address this shift have been circumscribed by dominant biomedical paradigms in health education and practice. The GBD focus on proximal risk factors, in particular, has led to an emphasis on modifiable behavioral (tobacco, alcohol and drug use, diet) and metabolic (eg, hypertension, hyperlipidemia) risk factors, including global efforts to address NCDs. 24 WHO and global initiatives have focused on promoting “healthy lifestyles and choices.” 25 Despite accumulating evidence of the influences of commercial actors, mainstream public health approaches remained focused on changing “risky” (ie, unhealthy) individual behaviors. Efforts to challenge this perspective, by drawing attention to the CDoH, have thus come up against their relegation to the distal. Most importantly, perhaps, public health actions to effectively reduce the global burden from NCDs have struggled accordingly. As Horton observes, “progress has been inadequate and disappointingly slow….An advocacy strategy based on four diseases [cardiovascular diseases, cancer, chronic respiratory diseases, diabetes] and four risk factors [tobacco use, harmful alcohol use, unhealthy diet, and physical inactivity] seems increasingly out of touch….We need a different approach.” 26
Commercial Determinants of Health as Agency and Structure
We propose a different approach to the understanding of CDoH as risk factors by connecting the proximal and distal. We argue that the growing scholarship on CDoH provides important explanations of population-level health outcomes associated with health-harming products and the pathways by which these products are produced, distributed, marketed/promoted, regulated and taxed (or not), and ultimately consumed. In this way, much of CDoH scholarship is aligned with the work of Nancy Krieger, who argues that the upstream-downstream analogy obscures the simultaneity of proximal and distal factors, as well as the 2-way flow of causality between them. 27
At the same time, as currently conceptualized, the study of CDoH is hindered by “a wide range of specific and nonspecific” representations in conceptual frameworks for the SDoH. As Maani and colleagues write, “consideration of commercial actors is frequently understated, not made explicit, or simply missing in many of the most influential conceptual frameworks addressing the SDoH.” 28 In general, when CDoH are included, these frameworks either reduce them to unhealthy behaviors as proximal risk factors, or conceptualize corporate activity as distal “general environmental “influences” 28 or even “determinants of determinants.” For this reason, conceptualizing the CDoH as a subset of SDoH is not especially helpful for linking the distal and proximal.
An alternative for advancing “a more explicit and systematic focus” 28 is through approaches that span structure and agency. 29 In social theory, agency concerns “the capacity of individuals to perceive their situation, reason about it, consciously monitor their action, form motives,” 30 make independent choices, and ultimately act. Agency, in the context of CDoH, includes individual or organizational choices and behaviors that result in the production and consumption of commercial products that have health-related consequences. The CDoH, therefore, concern the practices or conduct of commercial (eg, firms, trade associations, chambers of commerce) and allied actors (eg, politicians, public officials, lawyers, scientists) that seek to generate profits and other financial benefits that have relevance to health risks. 31 As such, the study of international political economy organizes these practices into 2 broad strategies: market and nonmarket. Market strategies concern practices taken to position commercial actors to be competitive in a marketplace and capable of taking advantage of market opportunities. Nonmarket strategies concern “how business organizations respond to, and influence, their broader political and social environment.” 32 The ways in which different forms of power are exercised by commercial actors, in pursuit of such strategies, is receiving growing attention. 33
Structure concerns the relatively stable and enduring institutions of a society that shape (and are shaped by) relationships between people and groups. Social structures shape human agency by influencing the opportunities and choices available.
34
It is now widely recognized that “many of the most powerful influences on health are “structural” in nature; that is, they derive from the social, economic, and political structures and are beyond the control of most (if not all) individuals.”
35
On obesity, for example, Walls and colleagues argue that a: focus solely on individuals—be it on their knowledge, willpower, or decision-making ability—will not be successful in reversing our society's body weight trajectory. We need measures aimed at changing the context, not the individual. Rather than simply encouraging consumers to make healthier choices, we must recast the environment so that healthy options are far more accessible, available, and desirable than unhealthy alternatives.
36
Scholars in the social sciences have categorized social structures in different ways. For example, anthropologist Melford Spiro applies 8 institutional variables: economy, settlement pattern, family, household, marriage, descent, social stratification, and government.
37
Sociologists traditionally categorize social structures into levels (micro, meso, macro, and increasingly global), with ongoing debate about the relationships and interactions among these levels.
38
For the purposes of this article, to advance measurement of CDoH, we build on methodological and theoretical debates in medical sociology since the early 21st century to explain health inequalities. In a 2003 review of these debates, Williams describes: new thinking that draws on some very old sociological arguments about the need to theorise what people do as something more than either an individual lifestyle-choice or the one-way outcome of structural determinants which are themselves produced in some under theorised way by capitalism, post-industrialism or globalism. What is missing from this work is an analysis of the relative determination of different sorts of structures… .
39
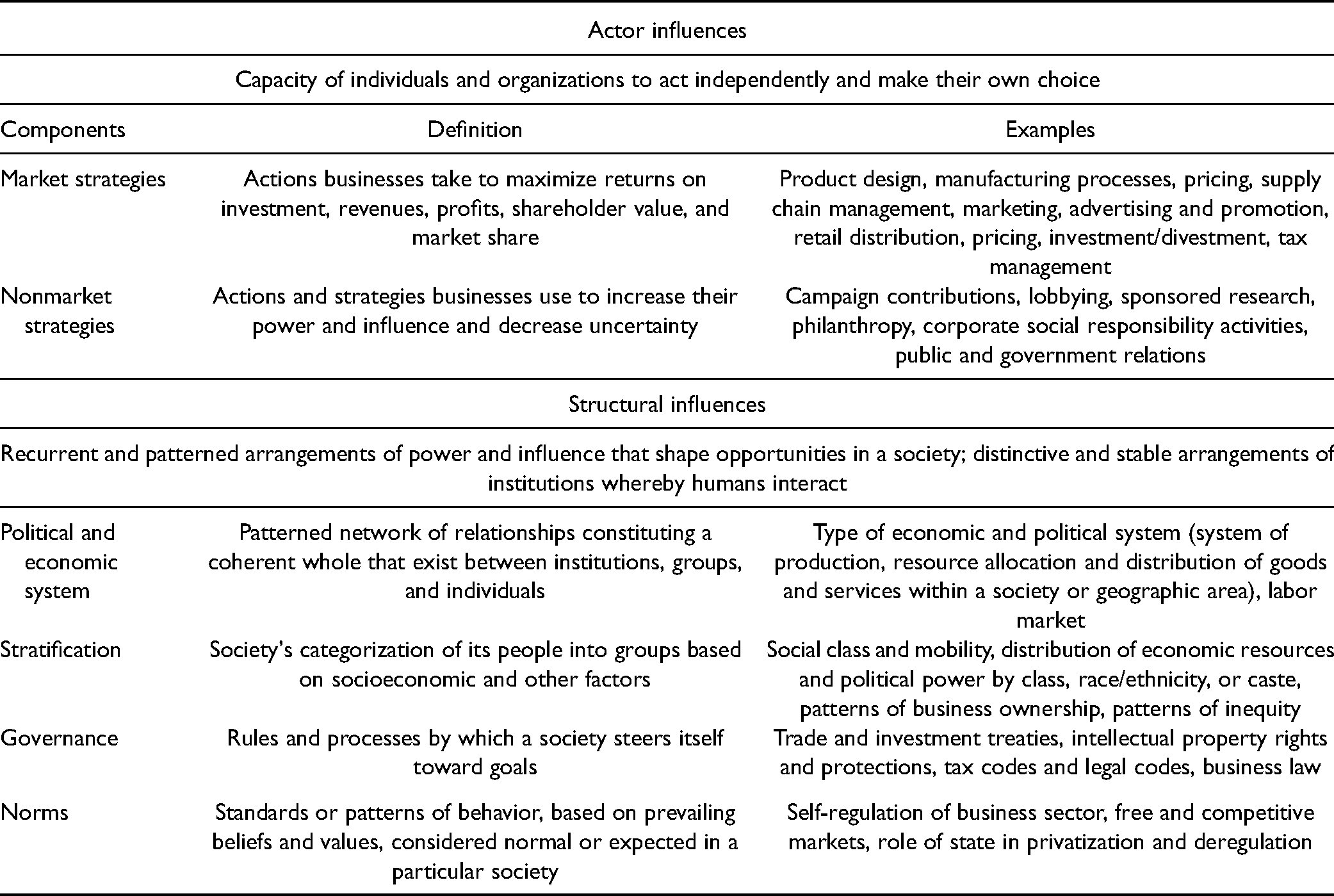
In addition to 2 agency components, we set out 4 structural components identified in these debates that are most relevant to CDoH at a national level: (a) political and economic system, (b) stratification, (c) governance, and (d) norms. 10 We focus on the country level because of the wider availability of data compared to other levels. We argue that these structures shape the nature, form, and degree of power available to, and exerted by, actors within a given country.
In social theory, the weight given to agency (individual free will) versus structure (social determinism) remains an enduring scholarly debate. It is not our intent to reconcile these influences but rather to encourage empirical analyses that recognize their dual importance, mutual interaction, 40 and, ultimately, combined influences as CDoH. We seek to remedy what Williams describes as “a lack of attention to the development of concepts which will help explain why individuals and groups behave the way they do in the context of wider social structures—to link agency and structure.” 39 On structure, Crammond and Carey describe the “need to consider more structure in public health, particularly those structures more proximal to the individual who is making behavioral choices.” 35 For example, Wood and colleagues identify 6 market strategies used by processed food manufacturers “to reduce intense competition with large rivals and maintain market dominance over smaller rivals.” 41 Similarly, US tobacco companies engaged in nonmarket strategies (eg, lobbying of US trade representative) to open Asian markets dominated by national monopolies from the late 1980s 42 and to shape taxes and tariffs in their favor within the Central American Common Market. 43 Conversely, agency via market and nonmarket strategies shape the social structures that enable or disable CDoH. For example, transnational corporations have consistently lobbied for economic policies that structure economies worldwide in particular ways, such as through taxation, competition, and trade protections, hence safeguarding and perpetuating their interests. A broad range of powerful commercial actors have also actively fostered public debate supporting “sensible” or “better” regulation, along with other ways to limit the role and size of the public sector.44,45 Agency and structure, in other words, should be recognized as both distinct and inseparable when analyzing the CDoH. Table 1 sets out definitions and examples for the 6 components of CDoH as agency and structural influences.
A Conceptual Framework for the Study of Commercial Determinants of Health.
Measuring CDoH as Exposures to Agency and Structural Components
Most efforts to date to measure the association between commerce and social (including health) impacts have been from a for-profit business perspective.46,47 These analyses seek to measure the “business value” accruing to firms from, for instance, their involvement in corporate social responsibility initiatives. For example, Evans and Siesfeld set out how “measurement techniques and data analytics … enable organizations to measure the business value of social impact … along six key drivers of value creation [emphasis added] from corporate social activity—brand differentiation, talent attraction and retention, innovation, operational efficiency, risk mitigation, and capital access and market valuation.” 48
By contrast, efforts to measure the impacts of commerce from a public health perspective have been limited. One example is a corporate health impact assessment (CHIA) framework by Baum and colleagues as “an overarching analytical framework and systematic methodology … to assess the impacts of TNC [transnational corporation] practices on populations within countries from a health equity perspective.” 49 Applying mixed methods such as document analysis, media analysis, semi-structured interviews, and geographic information systems, the framework also provides the potential to identify population groups particularly subject to health risks and benefits and to understand “the impact of different national regulatory structures on the ways in which corporations operate” through cross-national comparisons. In another example, Madureira Lima and Galea adopt a quantitative approach in developing a corporate permeation index (CPI). Corporate permeation is defined as “the extent to which corporations are embedded in the political, legal, social, economic, and cultural fabric of a country.” 50 Recognizing that “commercial interests deploy myriad tactics to promote their products,” the authors select 25 composite indicators of “corporate practices that influence the health of populations.” The CPI advances measurement of CDoH by providing a tool for quantifying corporate power exerted in diverse guises. Like the CHIA framework, it also provides a standardized framework for comparative analysis across countries.
We build on these 2 useful approaches by, first, conceptualizing commercial actors as more than corporations. A corporation is a particular form of economic organization that has become dominant during the 20th century in national economies. 51 The CHIA framework focuses on the agency of transnational corporations—large corporations operating across national jurisdictions—that manufacture unhealthy products. 52 We propose that measurement of CDoH should extend to a fuller range of public and private (and hybrid) actors that sustain and promote commercial practices, such as advertising firms, investors, private consultants, trade associations, and think tanks. Second, while Madureira Lima and Galea rightfully integrate both market and nonmarket (political) practices into the CPI, and locate these practices within political, legal, and extra-legal (illicit) environments, measurement of the structural components remains needed. 53
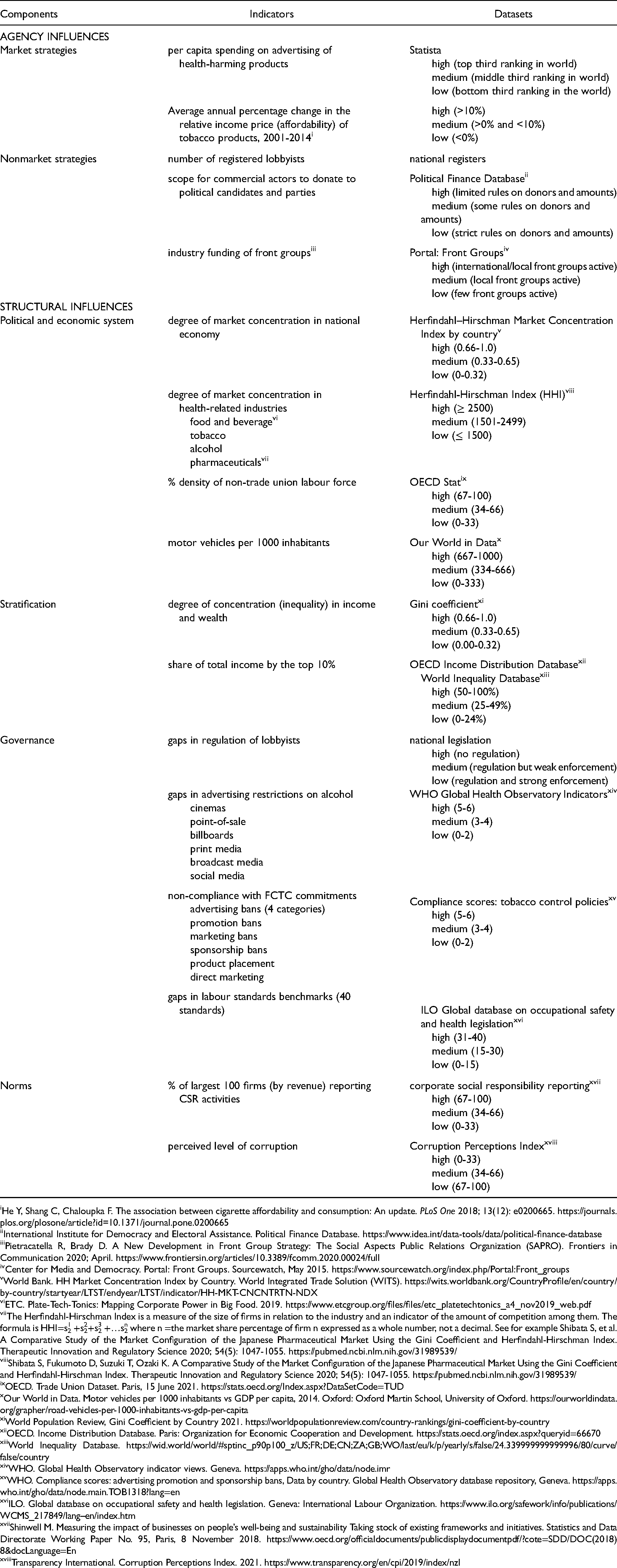
For this purpose, as a proof of concept, using the 6 agency-structure components shown in Table 1, we identify illustrative examples of indicators and existing datasets that can be used to rank degree of CDoH exposure (Table 2). The selection of indicators is determined by current availability of national (macro-level) data identified through online searches of data sources including the United Nations, World Bank and regional development banks, International Monetary Fund, and Organization for Economic Co-operation and Development. Given limitations in available data, a strict quantitative approach is not possible, although additional indicators may be added in future as new datasets become available (and/or are identified). Where possible, we provide quantifiable indicators to enable assessment of varying levels of exposure. The indicators for each component result in an evaluative rating (high, medium, low) to indicate relative level of exposure, with higher exposure associated with greater health harms. For example, higher per capita spending on advertising of health-harming products is ranked as a higher level of exposure. For each indicator, there is existing evidence of its association with health harms. We then combine these ratings into a composite Commercial Determinants of Health Index (CDoHi) as a measure of a country's aggregate exposure. The application of CDoHi to different countries offers the potential to assess relative aggregate exposure and thus cross-national and regional comparisons.
Example indicators and datasets to measure CDoH risk exposures
He Y, Shang C, Chaloupka F. The association between cigarette affordability and consumption: An update. PLoS One 2018; 13(12): e0200665. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0200665
International Institute for Democracy and Electoral Assistance. Political Finance Database. https://www.idea.int/data-tools/data/political-finance-database
Pietracatella R, Brady D. A New Development in Front Group Strategy: The Social Aspects Public Relations Organization (SAPRO). Frontiers in Communication 2020; April. https://www.frontiersin.org/articles/10.3389/fcomm.2020.00024/full
Center for Media and Democracy. Portal: Front Groups. Sourcewatch, May 2015. https://www.sourcewatch.org/index.php/Portal:Front_groups
World Bank. HH Market Concentration Index by Country. World Integrated Trade Solution (WITS). https://wits.worldbank.org/CountryProfile/en/country/by-country/startyear/LTST/endyear/LTST/indicator/HH-MKT-CNCNTRTN-NDX
ETC. Plate-Tech-Tonics: Mapping Corporate Power in Big Food. 2019. https://www.etcgroup.org/files/files/etc_platetechtonics_a4_nov2019_web.pdf
The Herfindahl-Hirschman Index is a measure of the size of firms in relation to the industry and an indicator of the amount of competition among them. The formula is HHI=s12 +s22+s32 +…sn2 where n =the market share percentage of firm n expressed as a whole number, not a decimal. See for example Shibata S, et al. A Comparative Study of the Market Configuration of the Japanese Pharmaceutical Market Using the Gini Coefficient and Herfindahl-Hirschman Index. Therapeutic Innovation and Regulatory Science 2020; 54(5): 1047-1055. https://pubmed.ncbi.nlm.nih.gov/31989539/
Shibata S, Fukumoto D, Suzuki T, Ozaki K. A Comparative Study of the Market Configuration of the Japanese Pharmaceutical Market Using the Gini Coefficient and Herfindahl-Hirschman Index. Therapeutic Innovation and Regulatory Science 2020; 54(5): 1047-1055. https://pubmed.ncbi.nlm.nih.gov/31989539/
OECD. Trade Union Dataset. Paris, 15 June 2021. https://stats.oecd.org/Index.aspx?DataSetCode=TUD
Our World in Data. Motor vehicles per 1000 inhabitants vs GDP per capita, 2014. Oxford: Oxford Martin School, University of Oxford. https://ourworldindata.org/grapher/road-vehicles-per-1000-inhabitants-vs-gdp-per-capita
World Population Review, Gini Coefficient by Country 2021. https://worldpopulationreview.com/country-rankings/gini-coefficient-by-country
OECD. Income Distribution Database. Paris: Organization for Economic Cooperation and Development. https://stats.oecd.org/index.aspx?queryid=66670
World Inequality Database. https://wid.world/world/#sptinc_p90p100_z/US;FR;DE;CN;ZA;GB;WO/last/eu/k/p/yearly/s/false/24.339999999999996/80/curve/false/country
WHO. Global Health Observatory indicator views. Geneva. https://apps.who.int/gho/data/node.imr
WHO. Compliance scores: advertising promotion and sponsorship bans, Data by country. Global Health Observatory database repository, Geneva. https://apps.who.int/gho/data/node.main.TOB1318?lang=en
ILO. Global database on occupational safety and health legislation. Geneva: International Labour Organization. https://www.ilo.org/safework/info/publications/WCMS_217849/lang--en/index.htm
Shinwell M. Measuring the impact of businesses on people’s well-being and sustainability Taking stock of existing frameworks and initiatives. Statistics and Data Directorate Working Paper No. 95, Paris, 8 November 2018. https://www.oecd.org/officialdocuments/publicdisplaydocumentpdf/?cote=SDD/DOC(2018)8&docLanguage=En
Transparency International. Corruption Perceptions Index. 2021. https://www.transparency.org/en/cpi/2019/index/nzl
Initial Application of CDoHi to 3 Countries
To illustrate how this index could be used, as a proof of concept, we assembled relevant indicators for 3 countries: the United Kingdom, Mexico, and Nigeria. These countries are chosen to provide diversity in wealth, size of population, and basic health indicators (Table 3). They are also chosen because of the availability of national-level data using a sample of the indicators and datasets shown in Table 2.
Basic Profiles of Selected Countries.
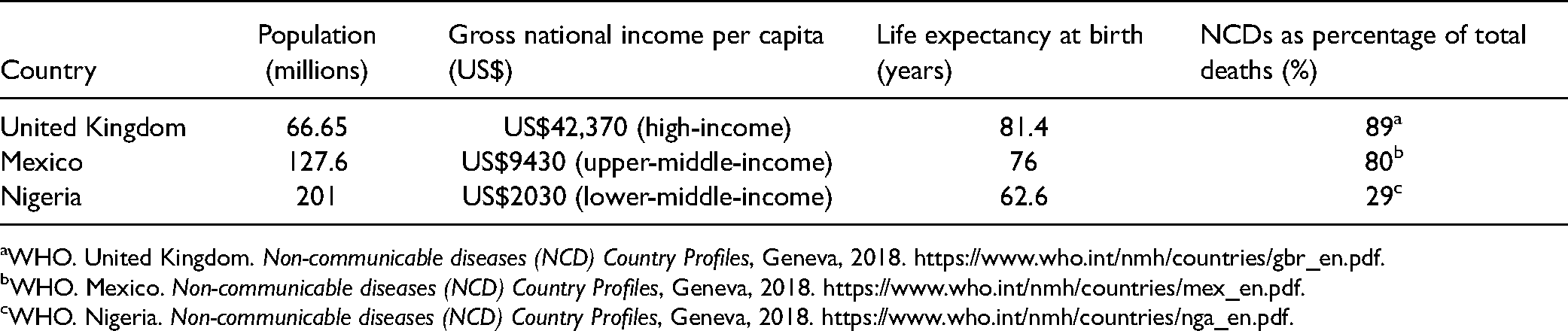
WHO. United Kingdom. Non-communicable diseases (NCD) Country Profiles, Geneva, 2018. https://www.who.int/nmh/countries/gbr_en.pdf.
WHO. Mexico. Non-communicable diseases (NCD) Country Profiles, Geneva, 2018. https://www.who.int/nmh/countries/mex_en.pdf.
WHO. Nigeria. Non-communicable diseases (NCD) Country Profiles, Geneva, 2018. https://www.who.int/nmh/countries/nga_en.pdf.
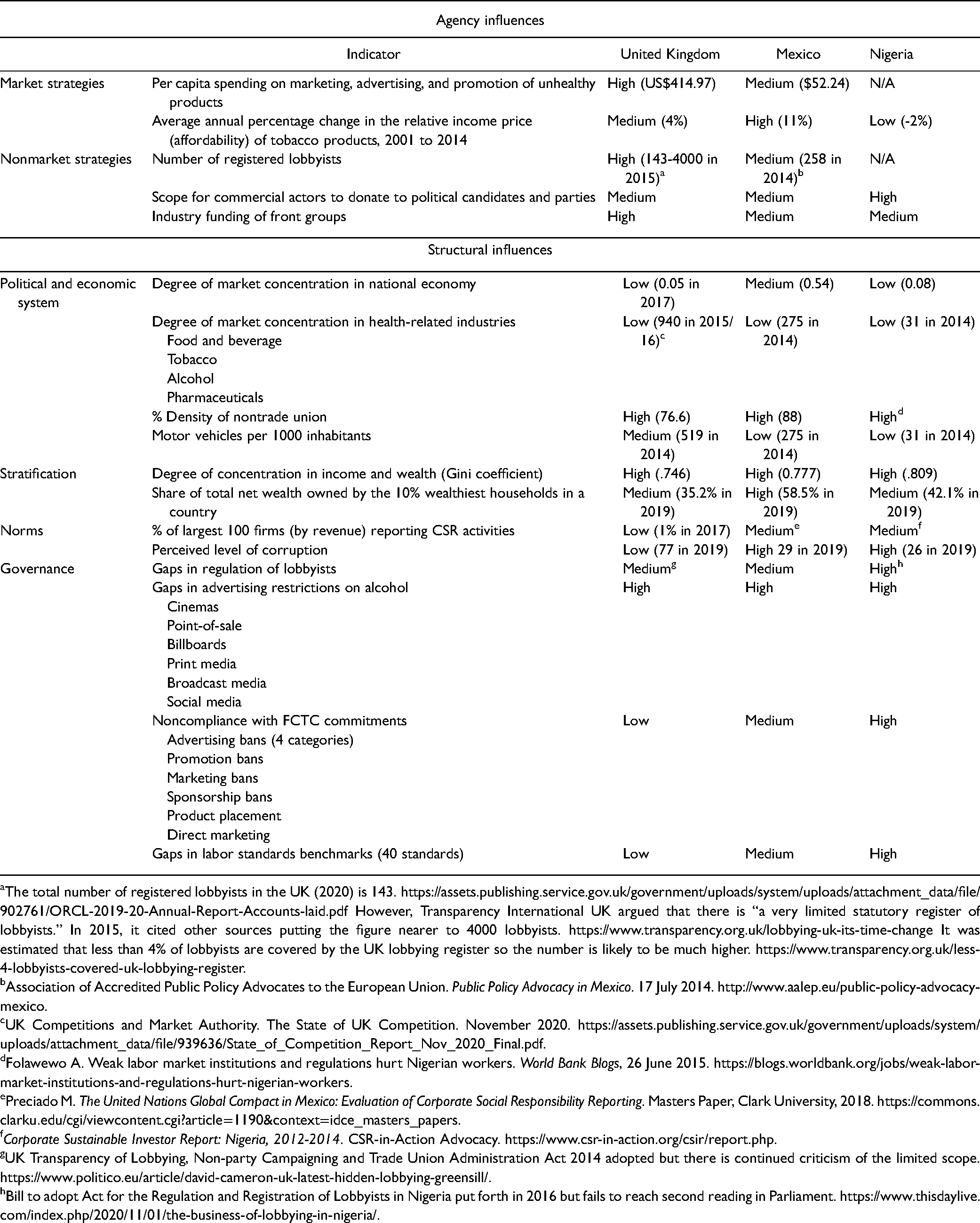
Table 4 presents the rankings for each indicator as an initial assessment of the varied nature of exposures to CDoH in each country. Further development of this approach should seek to add additional indicators under each component, based on emerging research on the CDoH, toward identifying the most useful for explanatory purposes. For these 3 examples, we can begin to identify opportunities for mitigating exposures such as wealth inequities and gaps in advertising restrictions for alcohol products. We can also begin to identify associations between high levels of exposure to market and nonmarket strategies, together with rankings for structural influences that enable those exposures. For example, a weak system of regulating lobbyists is expected to be consistent with a high level of government exposure to lobbyists and their lobbying. In the United Kingdom, there are 143 officially registered lobbyists (2020) under existing regulations. 54 However, Transparency International UK estimates that fewer than 4% of lobbyists are covered by the UK lobbying register. 55 Similarly, a high level of noncompliance with FCTC commitments to increasing tobacco taxation is expected to be consistent with higher affordability of products, as illustrated by Mexico.
Risk Exposures to CDoH in 3 Countries.
The total number of registered lobbyists in the UK (2020) is 143. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/902761/ORCL-2019-20-Annual-Report-Accounts-laid.pdf However, Transparency International UK argued that there is “a very limited statutory register of lobbyists.” In 2015, it cited other sources putting the figure nearer to 4000 lobbyists. https://www.transparency.org.uk/lobbying-uk-its-time-change It was estimated that less than 4% of lobbyists are covered by the UK lobbying register so the number is likely to be much higher. https://www.transparency.org.uk/less-4-lobbyists-covered-uk-lobbying-register.
Association of Accredited Public Policy Advocates to the European Union. Public Policy Advocacy in Mexico. 17 July 2014. http://www.aalep.eu/public-policy-advocacy-mexico.
UK Competitions and Market Authority. The State of UK Competition. November 2020. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/939636/State_of_Competition_Report_Nov_2020_Final.pdf.
Folawewo A. Weak labor market institutions and regulations hurt Nigerian workers. World Bank Blogs, 26 June 2015. https://blogs.worldbank.org/jobs/weak-labor-market-institutions-and-regulations-hurt-nigerian-workers.
Preciado M. The United Nations Global Compact in Mexico: Evaluation of Corporate Social Responsibility Reporting. Masters Paper, Clark University, 2018. https://commons.clarku.edu/cgi/viewcontent.cgi?article=1190&context=idce_masters_papers.
Corporate Sustainable Investor Report: Nigeria, 2012-2014. CSR-in-Action Advocacy. https://www.csr-in-action.org/csir/report.php.
UK Transparency of Lobbying, Non-party Campaigning and Trade Union Administration Act 2014 adopted but there is continued criticism of the limited scope. https://www.politico.eu/article/david-cameron-uk-latest-hidden-lobbying-greensill/.
Bill to adopt Act for the Regulation and Registration of Lobbyists in Nigeria put forth in 2016 but fails to reach second reading in Parliament. https://www.thisdaylive.com/index.php/2020/11/01/the-business-of-lobbying-in-nigeria/.
In addition, this approach provides a potential method for aggregating risk exposures to CDoH. The United Kingdom, Mexico, and Nigeria (for indicators with available data) rank medium/high for 11/17 (65%), 15/17 (88%), and 11/15 (73%) indicators, respectively. These 3 countries appear to demonstrate relatively high exposure. An additional range of indicators and their application to more countries will provide the basis of comparative analysis of relative exposure by country. Importantly, what relative level of exposure to CDoH means for explaining health outcomes such as burden of NCDs requires further analysis. For the United Kingdom and Mexico, the high exposure to CDoH may help explain the high proportion of deaths from NCDs. For Nigeria, the association is less clear, with 29% of deaths from NCDs, a reflection perhaps of state of development and associated stage in epidemiological transition. This does not mean that the CDoH have lesser influence, but rather different points of influence, such as access to clean water, health care, and housing. The refinement of this approach using longitudinal data, to identify trends in exposures and health outcomes, will be an important advance to this initial analysis.
Discussion
The proposed CDoHi seeks to achieve 3 analytical advances. First, it seeks to overcome conceptualizations of CDoH that limit understanding of the range and extent of their influence. Their relegation to the realm of upstream distal factors, and even further afield as “general environmental “influences” 28 or “determinants of determinants,” contributes to their neglect amid a strong public health focus on addressing proximal risk factors. Similarly, the CDoH focus to date on health-harming products, and the industries that produce and market them, has overlooked the ways in which commercial determinants are structurally embedded in societies and shape health in myriad ways. Our aim is to encourage fuller conceptualization of CDoH, as agency and structural influences, and to more fully assess these influences as risk factor exposures.
Second, a standardized method of assessing CDoH exposures provides the potential for comparative analysis across different populations. To date, the study of CDoH has produced useful case studies describing the activities of particular industries, health-harming products, or populations affected. With the fuller development and expanded application of this proposed approach, it may be possible to understand differential levels of exposure by specific populations or by the same population over time and place. To the extent that we can associate relatively high (and rising) exposures to CDoH and associated adverse health outcomes, as discussed below, we can identify populations at higher risk.
Third, a fuller appreciation of CDoH influences enhances the capacity to develop more and wider-ranging interventions to prevent identified exposures and thus reduce adverse population health outcomes. The escalating cost of treating NCDs (eg, health care costs for cardiovascular diseases in the European Union totaled €111 billion [US$121 billion] in 2015), 56 for example, has shifted attention to improving prevention strategies. The rising rates of NCDs in low- and middle-income countries and among the poor, 57 and the link between NCDs as preexisting conditions for COVID-19, further highlights the importance of improved upstream mitigation of risk.58,59 By identifying aggregate levels of exposure, along with key indicators of specific exposures, the CDoHi could support the targeting of priority interventions. For example, in a country with relatively high exposure to nonmarket strategies, regulatory requirements could be introduced to improving transparency of lobbying activity.
In developing the CDoHi, we acknowledge several caveats. Limitations in existing/available data restrict the types of indicators that can be presently used and the level of analysis at which they can be applied. We have focused on selected indicators and national level data at this time, but hope that future research will develop new datasets that allow fuller assessment of CDoH exposures and at other jurisdictional or population levels. For example, WHO might be scored as exposed to the agency influence of corporations, with the recent creation of the WHO Foundation and increased funding from the commercial sector. 60
We acknowledge the CDoHi needs further development and testing in other settings and sectors. In this article, our aim is to set out a proof of concept that will need to be refined over time. Indeed, the nature of data collected to enable improved measurement and monitoring of CDoH urgently needs expansion. This includes data across time and place, at different units of analysis, and across a wider range of commercial sectors. 61 In this illustration, the CDoHi provides a snapshot in time of current and recent exposures. Conducting assessments over time to understand changes to, and causes of, levels of exposure (eg, public health interventions, commercial actors) could help to link exposures to health outcomes. At the same time, we recognize the many constraints to wider use of the CDoHi, including dose/risk exposure associations and time lags from exposure to impact. Ultimately, this approach seeks to encourage new research and policy initiatives that spark fuller data generation, collection, and analysis efforts, as well as improved transparency of commercial influences to inform policy interventions.
Finally, an additional limitation is our primary focus on the adverse health impacts of CDoH. Certain exposures are likely to be associated with positive health outcomes. For-profit entities may introduce bicycle-sharing plans, organic fresh fruits and vegetables, and exercise facilities, which all have positive effects on population health. A fuller assessment of the CDoH should derive a rating based on the balance of positive and negative health impacts. For example, the growing, preparing, and selling of fresh fruits and vegetables as a commercial activity promote dietary health. However, if production involves exposure of agricultural workers to harmful pesticides and other workplace hazards, contributes to local pollution, or widens health inequities because of lack of affordability, the rating for exposures to CDoH should also reflect these negative externalities.
Conclusion
While the recent growth of attention to the CDoH marks a critical advance in public health research and policy, the full potential for this concept has yet to be realized. In this article, we set out a proposed approach to measuring CDoH as population-level risk exposures spanning agency and structural components. This is an initial starting point for advancing an alternative to still-dominant approaches focused on modifiable behaviors and metabolic risk factors. We conclude that, with further refinement and additions to these indicators, data sources, and application to different populations over time, the CDoHi can support a fuller understanding of the nature and significance of commercial influences on health and well-being. For more than 30 years, the GBD study has advanced data to inform public health research, policy, and practice. As the CDoH have dramatically expanded in their importance to human and planetary health, it is time to advance better ways to measure these exposures and to apply these assessments to inform more effective public health action.
Footnotes
Acknowledgments
The authors wish to acknowledge the support of Samantha Goulding in the initial literature and data scoping process. The authors also thank Julianne Piper, Jeff Collin, and Meghan Winters for their comments and participation in 2 meetings related to this project.
Author Contributions
Kelley Lee contributed to conceptualization, methodology, formal analysis, data curation, writing—original draft, writing—review & editing, funding acquisition. Nicholas Freudenberg contributed to conceptualization, methodology, formal analysis, data curation, writing—review & editing. Marco Zenone contributed to data curation, writing—review & editing. Julia Smith, Melissa Mialon, Robert Marten, Joana Madureira Lima, Sharon Friel, Daniel Eisenkraft Klein, Eric Crosbie, Kent Buse contributed to conceptualization, writing—review & editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Canadian Institutes of Health Research Planning Grant Number 429653. The funder played no role in the study design, the collection, analysis and interpretation of data; in the writing of the article; and in the decision to submit it for publication.