
Abstract
Medicine regulators rely on pivotal clinical trials to make decisions about approving a new drug, but little is known about how they judge whether pivotal trials justify the approval of new drugs. We explore this issue by looking at the positions of 3 major regulators: the European Medicines Agency, Food and Drug Administration, and Health Canada. Here we report their views and the implications of those views for the approval process. On various points, the 3 regulators are ambiguous, consistent, and demonstrate flexibility. The range of views may well reflect different regulatory cultures. Although clinical trial information from pivotal trials is becoming more available, regulators are still reluctant to provide detailed information about how that information is interpreted. As medicines and vaccines come up for approval for treatment of COVID-19, transparency in how pivotal trials are interpreted will be critical in determining how these treatments should be used.
Keywords
Pivotal clinical trials are key in the regulatory approval of medicines and vaccines, and how regulatory agencies interpret these trials can ultimately influence whether their decisions are accepted by the general public. According to Health Canada, pivotal trials have “high scientific quality, which provide the basic evidence to determine the efficacy, properties, and conditions of use of the drug.” 1 The U.S. Food and Drug Administration (FDA) definition is similar. 2
Regulatory agencies rely on “pivotal trials” to provide evidence of a product’s effectiveness and harm/benefit, but scant research exists on how regulators interpret and use such trials in their final decisions and how their decisions reflect regulatory culture. For example, regulation from the European Parliament outlining procedures for the authorization of medicinal products and establishing the European Medicines Agency (EMA) makes no mention of the term pivotal trials. 3 Yet, variable interpretation by regulatory agencies of the evidence in pivotal trials is evident. For example, 12 of 37 medicines with novel mechanisms of action approved first in Europe and/or Canada had their initial FDA submissions rejected for safety reasons. 4
As a group concerned about regulatory policy—how it is developed and applied—we were concerned by our inability to understand the relationship between regulatory agencies and the pharmaceutical industry when it came to pivotal trials and how the agencies negotiated the use of these trials. We were particularly interested in questions of how decisions were made about the designation of pivotal trials and how evidence from them was used in the regulatory process. Despite an extensive search of the websites of 3 major regulators—the EMA, the FDA, and Health Canada—we were unable to find any policy documents that dealt with these issues.
In the absence of any policy literature about pivotal trials, we contacted the EMA, FDA, and Health Canada by email to obtain their points of view on 4 specific questions: Who designates a clinical trial as pivotal? When is the designation made? How do they use the term “failed trial”? and How are decisions made when trials are positive and negative? The regulatory practices of these 3 agencies carry global implications; their decisions about whether pivotal trial data justify approving a new drug are often relied upon by the three-quarters of the World Health Organization membership with resource-challenged regulatory systems. 5 Health Canada was contacted through its Therapeutic Products Directorate, the branch that approves traditional small molecules. The FDA was contacted through its Office of Media Affairs and the EMA through its Media and Public Relations Service. We did not seek ethical approval because we were contacting the agencies themselves and not specific individuals within the agencies.
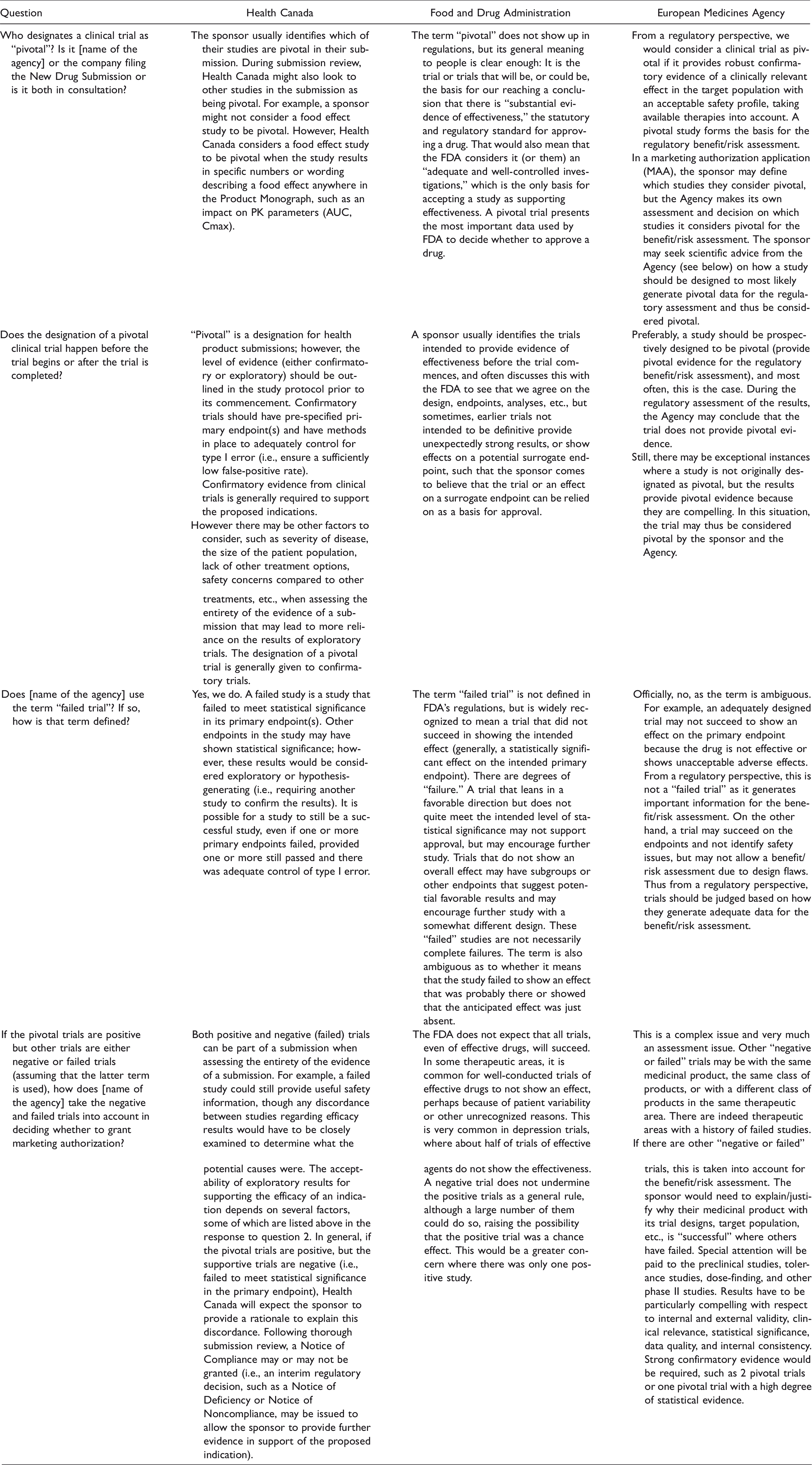
Here we discuss the positions they take and what those positions mean for drug regulation. Table 1 provides the complete verbatim replies from each agency.
Regulators’ Answers to Questions About Pivotal Clinical Trials.
Regulators’ Positions on Pivotal Trials
The Designation of a Clinical Trial as Pivotal
In theory, regulators should have no predetermined economic interest as to which trial should be considered pivotal, whereas the company sponsoring the trial does. If companies make the designation, they are incentivized to maximize the chance of positive results through trial design, collection of data, and its final analysis, leading to results and conclusions that more likely favor the sponsor. 6
Health Canada’s position is that the company usually designates a trial as pivotal in its regulatory submission. Under certain circumstances, the agency can determine that a trial is pivotal without a designation from the company. The EMA takes essentially the same position as Health Canada. The FDA emphasized that the term “pivotal trial” is not present in its regulations, but that it can be understood to refer to one or more trials that form the basis of its conclusion of substantial evidence of effectiveness. However, it is not clear if the FDA or the company makes the decision about which trials are pivotal.
The Timing of Making the Decision About Whether a Trial Is Pivotal
The designation of a trial as pivotal should be made in the protocol before the trial begins in order to remove any regulatory ambiguity about the timing of results that are generated. This a priori decision may be particularly relevant in the case of urgent research during emergencies such as the COVID-19 pandemic. For example, it is unclear how the early termination of the National Institutes of Health-sponsored study on remdesivir before there was definitive data on its effect on mortality 7 affected its presumptive designation as a pivotal trial. 8
Health Canada differentiates between exploratory and confirmatory trials and believes that the level of evidence should be outlined in the protocol prior to commencement of the study—that is, that the decision should be made a priori. It equates pivotal studies with confirmatory ones, but allows that other factors may lead to more reliance on the results of exploratory trials.
The EMA’s position is also that a trial should prospectively be designated as pivotal and that this designation is typically made by the company sponsoring the trial, although the company’s decision may be made after meetings between the agency and the company. Like Health Canada, its position is that in exceptional instances, trials not originally identified as pivotal may provide compelling evidence or alternatively that trials that were initially considered pivotal could be downgraded in status during the evaluation process.
The FDA’s position is also that the sponsor usually identifies the trials intended to provide evidence of effectiveness before the trial commences, and the trial is often designed based on discussions between the company and the FDA. According to the FDA, effects on surrogate endpoints in earlier trials can sometimes provide strong enough evidence for approval—that is, these trials can achieve pivotal status.
Failed Trials
A “failed trial” is usually interpreted as one whose results fail to show that the drug is efficacious due to some failure of assay sensitivity—for example, a flaw in sample selection, outcome assessment, or clinician adherence. 9 It is important to understand how regulators distinguish between failed and negative trials. If regulators decide that a trial failed, the results can be discounted, whereas a decision that a trial was negative may mean that the drug will not be approved.
According to Health Canada, a “failed study” is one where the primary endpoint(s) does not achieve statistical significance. Although other endpoints might show statistical significance, results are considered exploratory or hypothesis-generating and need to be confirmed in a subsequent study. The EMA does not use the term and considers it “ambiguous.” In its view, even an adequately designed trial may not show efficacy if there are unacceptable side effects or no clinical benefits. In either case, the EMA does not necessarily consider this a failed trial if it has generated useful information.
The FDA’s position is that the term “failed trial” is not defined in its regulations, but that it is commonly understood to mean a trial that did not succeed in showing the intended effect. It also considers the term ambiguous because it could mean that the study failed to show an effect that was probably there or it showed that the anticipated effect was just absent. Like the other 2 regulators, the FDA felt that so-called failed trials could generate useful information.
Decision-Making When Some Pivotal Trials Are Positive and Others Are Negative
Typically, regulators require 2 positive pivotal trials to approve a new drug, although that requirement has been somewhat eroded. Between 1995 to 2017, the proportion of new drugs and biologics approved by the FDA using 2 pivotal trials declined from 81% to 53%. 10 This trend in the decline of using 2 pivotal trials as the basis for approval is not unique to the FDA. A 2019 study documented the approval of 23 novel therapeutic drugs between 2012 and 2016 by both the FDA and the EMA based on a single pivotal trial. 11
There is no legislative requirement in the United States regarding what percentage of trials need to be positive. According to a legal analysis, “in theory, a drug sponsor could simply run clinical trials in sequence, stopping only after 2 positive trials have been accumulated.” 12 Using those 2 trials, the FDA could satisfy the criterion of substantial evidence of efficacy, notwithstanding the other negative trials. Negative trials appear not to hinder approval; about half of the antidepressant trials submitted to the FDA between 1987 and 2004 for regulatory approval of 12 drugs were negative. 13 Similarly, in Canada, companies only have to submit “substantial evidence of the clinical effectiveness of the new drug,” with no minimum number of trials specified and no mention of negative trials. 14
The position of Health Canada is that it would expect the sponsor to provide an explanation if the pivotal trials were positive but the supportive (exploratory) trials were negative, and it may require further supportive information. The EMA calls this situation a complex assessment issue; it requires the sponsor to explain the discrepancy in the results and strong confirmatory evidence would be necessary for approval. According to the FDA, not all trials are expected to be positive. The FDA takes the position that, as a general rule, a negative trial does not undermine the positive trials, although a large number of them could do so, raising the possibility that the positive trial was a chance effect.
Regulators, Pivotal Trials, and Drug Regulation
The positions of the regulators about pivotal trials provide valuable insights into their views on drug regulation in general.
Ambiguity
The 3 regulators often take ambiguous positions, creating a discretionary space. This ambiguity may be an artifact of regulators’ historical aversion to disclose information used in decision-making. Until relatively recently, both the EMA and Health Canada were unwilling to make public clinical trial reports filed by drug companies, and the FDA still does not do so. 15
Similarities
The positions taken by all 3 regulators were similar in many respects. Again, this should not be surprising. All 3 are members of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use, an alliance of regulatory authorities and pharmaceutical industry associations that together participate in the development and implementation of the council’s standards. There are also substantial interconnections among the 3 regulators based on Mutual Recognition Agreements. 16
Distinct Therapeutic Cultures
The positions may well reflect distinct therapeutic cultures in the different regions. These “therapeutic cultures arise from networks of actors that produce regulatory policy, determine testing standards, and ultimately decide on market access for new drugs.” 17 Variations in these networks can be seen in the different ways that agencies compose their advisory committees, how they structure their interactions with industry, and the extent to which they integrate patients into their processes.18–20 Two comparisons of how the FDA and the EMA make decisions on oncology drugs found that the 2 manage uncertainty differently. The conclusion from one study was that the FDA is “more open to take risks and base approval on less robust data in order to guarantee quicker access to anticancer medications.” 21 The second study did not find any data showing that the FDA took more risks, but did conclude that the 2 agencies approached risk differently. 22 Both studies illustrate that informal factors, while secondary to the data in driving decisions, play an important role in the drug-regulation process.
Flexibility and Transparency
Finally, drug regulators are flexible in how they interpret clinical evidence—that is, in their use of discretionary power. Flexibility is desirable and necessary because the data require interpretation and the balance between benefit and harm can be hard to determine. 23 However, how this flexibility is expressed should be transparent and justified so that both health care providers and the public understand the rationale for the decisions regulators make. Yet, recent changes to the FDA’s review process—replacing individual scientific reviews that often contain a wealth of information that is not available elsewhere, as well as conflicting interpretations of the evidence, 24 with one “integrated review”—stand to further obscure regulatory decision-making. 25
The onset of the COVID-19 crisis has seen conflicting advice from the FDA. On March 28, 2020, it issued an emergency use authorization, based on case series data, giving doctors permission to prescribe hydroxychloroquine off-label for patients with COVID-19. 26 Less than a month later, the FDA qualified that authorization and said the drug should only be prescribed to patients who are in the hospital or enrolled in a clinical trial. 27
Differences between regulatory agencies are also apparent during the COVID pandemic, despite mutual agreements. For example, the EMA did not authorize the use of hydroxychloroquine for unapproved indications. 28 Different regulatory instruments within the 3 agencies result in different mechanisms to approve remdesivir “conditionally” (Health Canada) or pre-approval as an emergency use authorization (FDA). 29 Most recently, the FDA took extra due diligence in examining safety data, restarting the Phase III Oxford-Astra Zeneca COVID vaccine clinical trial AZD1222 fully 6 weeks later in the United States (October 23) compared to the United Kingdom (September 14) after it was stopped on September 6 due to an adverse event following immunization. 30
Conclusion
The decision to approve a new drug by a regulatory agency is a hybrid of the scientific evidence in pivotal trials and cultural practices that reflect national values and structures. To be fully accountable to the public, regulators must help us understand how they integrate the two. Taking steps to disclose judgment calls about why a trial is considered pivotal and how the evidence from the trial is interpreted would markedly improve public understanding of regulatory decision-making and enhance transparency and accountability.
Footnotes
Acknowledgments
The authors thank Sharon Batt, Peter Doshi, Katherine Fierlbeck, and Nav Persaud for comments on earlier versions of the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joel Lexchin received payments for writing a brief in an action for side effects of a drug for Michael F. Smith, Lawyer, and a second brief on the role of promotion in generating prescriptions for Goodmans LLP. He is a member of the Foundation Board of Health Action International and receives royalties from University of Toronto Press and James Lorimer & Co. Ltd. for books he has written. Janice Graham has no conflicts to declare. Matthew Herder receives honoraria for his work as a member of the Patented Medicine Prices Review Board. Tom Jefferson was in receipt of a Cochrane Methods Innovations Fund grant to develop guidance on the use of regulatory data in Cochrane reviews (2015-018). In 2014–2016, TJ was a member of 3 advisory boards for Boehringer Ingelheim. TJ was a member of an independent data monitoring committee for a Sanofi Pasteur clinical trial on an influenza vaccine. TJ is occasionally interviewed by market research companies about Phase I or II pharmaceutical products, for which he receives fees (current). TJ was a member of 3 advisory boards for Boehringer Ingelheim (2014–2016). TJ was a member of an independent data monitoring committee for a Sanofi Pasteur clinical trial on an influenza vaccine (2015–2017). TJ is a relator in a False Claims Act lawsuit on behalf of the United States that involves sales of Tamiflu for pandemic stockpiling. If resolved in the United States’ favor, he would be entitled to a percentage of the recovery. TJ is coholder of a Laura and John Arnold Foundation grant for development of a RIAT support center (2017–2020) and a Jean Monnet Network Grant (2017–2020) for the Jean Monnet Health Law and Policy Network. TJ is an unpaid collaborator to the project Beyond Transparency in Pharmaceutical Research and Regulation, led by Dalhousie University and funded by the Canadian Institutes of Health Research (2018–2022). TJ consults for Illumina LLC on next-generation gene sequencing (2019–). TJ was the consultant scientific coordinator for the HTA Medical Technology program of the Agenzia per i Serivizi Sanitari Nazionali (AGENAS) of the Italian Ministry of Health (2007–2019). TJ is director of medical affairs for BC Solutions, a market access company for medical devices in Europe. Trudo Lemmens has no conflicts to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.