
Abstract
This article utilizes cross-national datasets to build and test a theoretical framework that emphasizes the interactive relationship between political freedom and inequality regimes in explaining the spread and control of COVID-19. First, we construct a theoretical framework to analyze the dilemmas faced by liberal democratic regimes in managing both the economy and virus control. Next, we incorporate another framework to conceptualize the capacity of welfare states to support economically vulnerable populations and pandemic victims. To test our hypotheses, we employ multivariate OLS regression analyses on confirmed case rates, focusing on 4-month intervals during the first year of the COVID-19 crisis. The findings provide sufficient support for our claim that, at higher levels of inequality, political freedom is positively associated with the spread of COVID-19. Conversely, at lower levels of inequality, political freedom is negatively associated with the spread. This study underscores the inherent vulnerability of democratic freedom to infectious diseases and highlights the importance of social welfare provisions and healthcare systems in responding to large-scale disasters such as the COVID-19 pandemic
Introduction
Throughout 2020, coronaviruses (SARS-CoV-2, COVID-19, or coronavirus hereafter) pervaded worldwide, resulting in massive death tolls and economic recession in many countries. Similar to other disasters, the coronavirus unwittingly revealed the social inequalities underlying each society. The bare everyday realities of inequality disclosed by the pandemic are disproportionately concentrated in the lower socioeconomic strata of societies. Particularly notable is how precarious jobs in the labor market lack social protection, leading to massive unemployment and economic strain. However, from a cross-national perspective, the pandemic’s impact, as measured by confirmed cases, seems inconsistent across countries. Why do some developed or developing societies cope better with the coronavirus? Which societies or countries have managed the coronavirus pandemic more effectively, and why? We aim to explore the structural patterns of COVID-19 diffusion from a macro perspective.
We can assume that economic status and political competence are key factors that explain how well a society controls confirmed COVID-19 cases and the associated death toll. It seems plausible that a country with a developed economy and a well-functioning political system would be better equipped to minimize the pandemic’s infection rates and death toll, as such countries are often presumed to have more advanced bureaucratic resources and policy measures (Kaufmann et al., 2009) to protect their citizens from unexpected disasters. However, what we have encountered in diverse media outlets is contrary to our expectation; many economically developed societies in the Western hemisphere, such as the United States (US), the United Kingdom (UK), and other European countries, have struggled with massive infection rates and enormous death tolls. In contrast, countries in East Asia, such as South Korea, Taiwan, Laos, and even Vietnam, as well as some island nations in the Pacific, such as New Zealand and Australia, are regarded as having controlled the pandemic more effectively. To illustrate, as of 27 December 2020, the US reported over 18 million confirmed cases and 342,920 deaths, the UK reported more than 2 million confirmed cases and 90,475 deaths, while Japan reported 217,312 confirmed cases and 3,213 deaths, and Australia reported 28,296 cases and 920 deaths (WHO, 2024). This apparent discrepancy challenges conventional assumptions and warrants a deeper investigation into the sociopolitical factors influencing pandemic outcomes across diverse global contexts.
Why is the COVID-19 infection rate greater in some industrialized countries that are expected to have more capacity to deal effectively with epidemics? In the realm of social science, how can we understand and explain those unexpected situations? To investigate this issue, we focus on the inequality ingrained in societies and propose discovering the relationship between sociopolitical institutions and the structural inequality causing the damage from the pandemic. To be specific, we aim to achieve the following goals: (1) understanding how each country’s sociopolitical structure impacts responses to coronavirus pandemics; and (2) understanding how existing sociopolitical institutions and inequality structures enable the state/society to better cope with disasters and crises, particularly in the initial stage. This study aims to investigate how socioeconomic structures influence the spread of coronavirus as measured by confirmed case rates, using diverse macro-level cross-national data, thereby advancing the discussion on the relationship between inequality and social disasters.
Theoretical discussion
Previous studies on the politics of disasters and coronavirus pandemics
Until recently, the students of disaster studies have mainly focused on how inequality is revealed and handled in immense natural disasters such as hurricanes, earthquakes, floods, and so on (Kahn, 2005; Reininger et al., 2013). Individuals in developing nations or regions characterized by limited infrastructure are the primary victims of natural disasters. It is often assumed that their insufficient income and low social capital are associated with their inferior living environments and vulnerability to unexpected natural events (Donner and Rodríguez, 2008; Fothergill and Peek, 2004; Reininger et al., 2013; Tselios and Tompkins, 2019). Nonetheless, the COVID-19 infection has distinctive features from conventional natural disasters due to distinctive features in both the virus’s initial stages and societal responses to mitigate its impact. First, in the incipient coronavirus, measures to control the movement of the general population, such as mandatory mask-wearing and restrictions on social gatherings, are considered crucial since the spread of the virus is susceptible to physical proximity during social and economic activities (DeFranza et al., 2021). Second, when assessing the impact of the virus, we can assume that alleviating the disaster is closely aligned with each nation’s socioeconomic structure. This includes an examination of how inequality is ingrained within a society and an evaluation of the implementation of social politics, such as inclusive social care. Hence, we can expect that, in general, the spread of COVID-19 is intricately affiliated with citizens’ lifestyles, shaped by the extent of political freedom and the social and economic structure of damage mitigation efforts in each country.
In the inception of COVID-19, a group of developed nations has faced challenges in contending with the virus (Khafaie and Rahim, 2020). Within the cohort of wealthy countries, distinctive policy responses to the virus have emerged, reflecting different political governance backgrounds and socioeconomic structures. Notably, the divergent approaches taken by the US (Bergguist et al., 2020) and New Zealand (Jamieson, 2020) in containing the pandemic exemplify the marked variations in government actions.
Nevertheless, it is difficult to find studies investigating how democratic institutions and inequality systems respond to disasters, especially the 2020 coronavirus pandemic. Limited research within the social sciences has partially explored the impact of COVID-19 on democratic regimes and existing inequalities. The crisis, given its highly contagious nature, has posed challenges to mass collective action and thus has threatened democratic institutions in some countries. Amat et al. (2020) point out that the COVID-19 crisis provokes dilemmas concerning the relationship between public health and civil liberties. As citizens’ economic and civic activities face restrictions, there is a tendency toward strong expert leadership wielding centralized power to control the pandemic, potentially sidelining democratic governance (Ballard-Rosa et al., 2018).
Moreover, some studies on COVID-19 reveal its unjust impact, especially on those with low socioeconomic status (Patel et al., 2020). For instance, Schmitt-Grohe et al. (2020) reported that residents in low-income areas are more likely to test positive for COVID-19 than residents in New York City’s wealthiest neighborhoods. McLaren (2021) shows a strong correlation between the minority population and COVID-19 deaths in the US. Moreover, Blundell et al. (2020) suggest that COVID-19 has exacerbated various forms of labor market inequality. In the UK, workers in shutdown industries are more likely to be low income, female, young (aged <25 years), and from marginalized ethnicity, while workers who can work from home are relatively safe from the risk of infection.
Viral pandemics pose new challenges to existing political–economic regimes. Viruses disrupt the essential ingredients of the market and procedural democracy operations—individual freedom and human interaction—both of which are indispensable to daily production and transactional activities. Furthermore, such pandemics disproportionately impact the weaker dimensions of an existing political economy (Blundell et al., 2020; Dorn et al., 2020)—specifically, the socially and economically vulnerable. The state bureaucracy may struggle to reach this population, even when stringent control measures are crucial to managing the infection rate among them. Therefore, navigating the unusual circumstances requires a nuanced consideration of both economic and social dimensions. How can a regime effectively manage the simultaneous and conflicting risks inherent in these two dimensions? Can a government protect both the vulnerable and individual rights while facing the unprecedented scale of a viral pandemic? We delve into these questions by revisiting the core elements of democracy and inequality literature. Subsequently, we put forth new theoretical propositions and hypotheses to examine the interplay of political freedom and income inequality within the context of the COVID-19 situation.
Dilemmas of liberal democracy in disease control
In democratic regimes where the rule of law protects citizens’ freedom of religious and political association, participation in cultural and hobby clubs, protection of private lives and associated information, as well as property rights, citizens have been comfortable with the “self-restraining” state (Schedler et al., 1999) that does not interfere in citizens’ everyday lives and is legally accountable. From the citizens’ perspective, restriction of these diverse dimensions of freedom incurs higher psychological and economic costs, leading to significant resistance from civil society. In this context, we posit that disease control governance tends to be less effective in democratic regimes.
In a well-established democracy, a pre-existing consensus between the government and the public regarding potential encroachments on private rights (access to private information) constrains discretionary prevention measures. These measures might otherwise impede the viral spread, for example, through the utilization of technologies that can identify individuals’ locations via a cellular phone application—an approach covertly or explicitly employed by the Chinese and South Korean governments (Moradi and Vaezi, 2020). On the government side, existing health and social welfare institutions will step forward in the form of government disease prevention and control agencies, which force disease control to be modestly applied even though it is needed at the highest possible level.
In this environment, some political leaders find room to disseminate rhetoric and policy that advocates for centralized, stricter government control. Research on “negative economic shocks,” which are similar to natural disasters in their impacts on citizens’ lives, reports that macro-level economic crises tend to increase political polarization as citizens increasingly support non-mainstream, extremist parties (Author et al. Forthcoming). Furthermore, voters often exhibit a tendency to endorse authoritarian leaders amid such circumstances (Ballard-Rosa et al., 2018).
In this regard, we build the first hypothesis to examine whether institutional protection of individual freedom paradoxically encourages viruses to spread in the private sphere. In this scenario, societies in which citizens preserve their rights to participate in informal and formal civic association freely and actively without intervention or constraint by higher authorities, such as the state (Paxton, 2002; Putnam, 1997), are more likely to be exposed to the COVID-19 pandemic. The vibrant civic culture underpinned by democratic institutions creates a vast reservoir that the state cannot fully monitor to deter the spread of viruses. Therefore, well-established democratic norms to protect individual freedom interact with associational activities, including freely congregating for political and religious reasons.
Inequality and disaster response
Social vulnerability conceptualizes a society’s level of readiness to manage a spectrum of disasters, ranging from natural occurrences to political and economic crises. Some societies and their governments proactively prepare for diverse disasters during periods of normalcy, resulting in ordered, disciplined, and organized responses to one or multiple disasters. In contrast, others remain unprepared and resort to improvisation when an unexpected disaster strikes. Prepared societies minimize the number of victims affected by disasters, while unprepared societies expose their members to the maximum impacts of disasters without adequate buffers and safety nets. Particularly, those most vulnerable to such “unmitigated” disasters are individuals at the bottom of the social strata, including the poor, outsiders, the precariat, the socially isolated (often older people) (Klinenberg, 2003; Wisner et al., 2004), and the critically ill (Fink, 2013). Outsiders and the precariat face unemployment risks in a long-term economic depression following a disaster. The socially isolated and the critically ill are often ignored by authorities in situations requiring urgent rescue (Klinenberg, 1999). Consequently, disaster victims in unprepared societies are disproportionately concentrated in these “socio-economically weak” groups (Blundell et al., 2020; Patel et al., 2020; Schmitt-Grohé et al., 2020).
Some societies, usually those that have prepared for disasters in an organized manner, promptly take actions following disasters, including the quick repair of broken roads and bridges, immediate welfare provision for severely affected individuals, the implementation of “economic stimulus packages” to rejuvenate the economy, and efforts to pacify the social and political unrest. Conversely, other societies, which have normally been unprepared to handle disasters’ aftermath, respond to them without specific plans. Their leaders deflect blame from civil society by attributing disasters to particular groups or external forces (Klinenberg, 1999). We posit that these two phases of responses of society “before” and “after” disasters are primarily driven by pre-existing “inequality regimes” as follows: (Already) equal societies will provide more resources to the lower classes and those socially isolated in the bottom social strata, which may persist during the disasters. Additionally, equal societies with well-developed social welfare systems will restore their “pervious equilibrium” at a lower cost, thanks to their pre-existing social welfare system.
More equal societies with well-developed social welfare systems have institutionalized social policies by which those experiencing various social and economic risks can lead their lives “without relying on the market” (Esping-Andersen 1990, 1999). This occurs despite personal disasters and accidents, including aging, sickness, industrial accidents, unemployment, and even childbirth. In these societies, disasters imply that a much larger population is exposed to a larger scale of risks, which requires a welfare system of even greater magnitude to buffer such a vulnerable population. Mobilizing resources is more straightforward in more developed welfare states, where civil society has already achieved necessary social consensus and trust, and social welfare systems have penetrated the vulnerable population. In these societies, the socially isolated, especially the elderly, are more likely to be reached by the state. Information on disasters is more likely to be shared with such populations through the public alert system. Most importantly, rescue packages may be more readily delivered to those who most need them. Therefore, more equal societies with more egalitarian and universal welfare systems are likely to recover more quickly from disasters than other societies employing less universal and more limited welfare systems.
Unequal societies without well-developed social welfare systems will incur higher costs in caring for the lower classes and the elderly population. They have also not institutionalized state apparatuses that enable the bureaucracy to penetrate and reach the socially marginalized when disasters occur. Without social consensus on rescue costs and without pre-existing resources and institutions that are immanently needed to rescue those at the bottom and the margin, these societies are more likely to leave the most vulnerable exposed to disaster hazards.
Finally, in more equal societies with comprehensive social welfare systems, health as a “public good” or “the commons” (Ostrom, 1990) may have been prioritized, leading to the development of more efficient public healthcare systems. In such societies, vulnerable populations, such as the elderly and the socially marginalized, are likely to have easier access to the public healthcare system during social and economic crises like pandemics. There is a possibility that the trust and solidarity fostered by universal healthcare systems may also lead citizens to accept temporary sacrifices of their individual rights during public health crises. In contrast, unequal societies with selective social welfare provisions may exhibit indifference toward their vulnerable populations or lack the necessary medical capacities to address monumental healthcare crises such as COVID-19.
Based on the discussion on inequality and welfare regimes, we hypothesize that inequality and lack of welfare state institutions to reduce the inequality will amplify the diffusion of pandemic disease in a society. In a more equal, equality-pursuing society, citizens have built “common goods” in the form of social welfare to protect them from risks they may experience during their lifetimes, such as unemployment, disease, industrial accidents, and aging. In addition, the governments are more likely to cultivate the capacity to assess the national vulnerability and formulate strategies for rare events, such as global pandemics. In addition, the development of national information channels would mitigate the impacts of virus diffusion by informing citizens about the disease and infection (Qazi et al., 2021). Different societies have institutionalized diverse welfare regimes to mediate between ruthless market mechanisms and individual citizens’ misfortunes (Esping-Andersen 1990, 1999). In more unequal societies, citizens with limited access to social safety nets because of eligibility and means-testing criteria must find their own solutions when facing unemployment, poverty, and disease. In non-Western societies, existing welfare institutions often produce “a second layer of inequality” in which those who are excluded from market remuneration are also excluded from social safety nets (Huber and Stephens, 2012; Lipton, 1977).
We expect that these different levels of protective management of citizens’ risks generate diverse environments for virus diffusion. First, in more unequal, poverty-laden societies whose citizens are minimally protected from various socioeconomic risks, viruses may attack those exposed to poor working conditions and unhealthily congested residential areas—poor neighborhoods. Second, those engaged in precarious labor such as delivery services and personal care services may be exposed to a higher probability of virus infection, which may turn them into virus spreaders. Most importantly, in more unequal societies in which social welfare policies protect citizens unevenly and disproportionately, poor citizens will be alienated from the existing healthcare provision, thereby being at higher risk of either being infected or infecting others. Limited access to information channels and low health literacy disproportionately impact poor populations who lack access to health services in pandemic situations (Ahmed et al., 2020; Pirisi, 2000). From these scenarios, we build the second hypothesis: In unequal societies, in which individuals suffer from lower social safety net coverage and the state makes less effort to reduce inequality, COVID-19 confirmed cases will be higher (than in more egalitarian countries with better social welfare provisions).
Inequality, political freedom, and pandemic
We construct a more complex situation in which inequality regimes and democratic norms of freedom interact, producing diverse environments and contexts of virus infection, detection, and extermination. Our previous discussion of political freedom and inequality regimes suggests that there could be four hypothetical, ideal-type societies, as illustrated in Table 1. The four categorizations are derived from three datasets, which will be explained further in the “Data” section. 1 First, in the upper cells (Cells 1 and 2) of the following two-by-two tables in Table 1, a high degree of political and religious freedom provides individuals with more room for social and political gathering and organizing capacities, which serve as a reservoir for virus contagion. However, depending upon the inequality-management regime, such risks will be mitigated at a tolerable level or amplified to an uncontrollable level.
A framework of pandemic risk and response according to inequality and political freedom regimes.
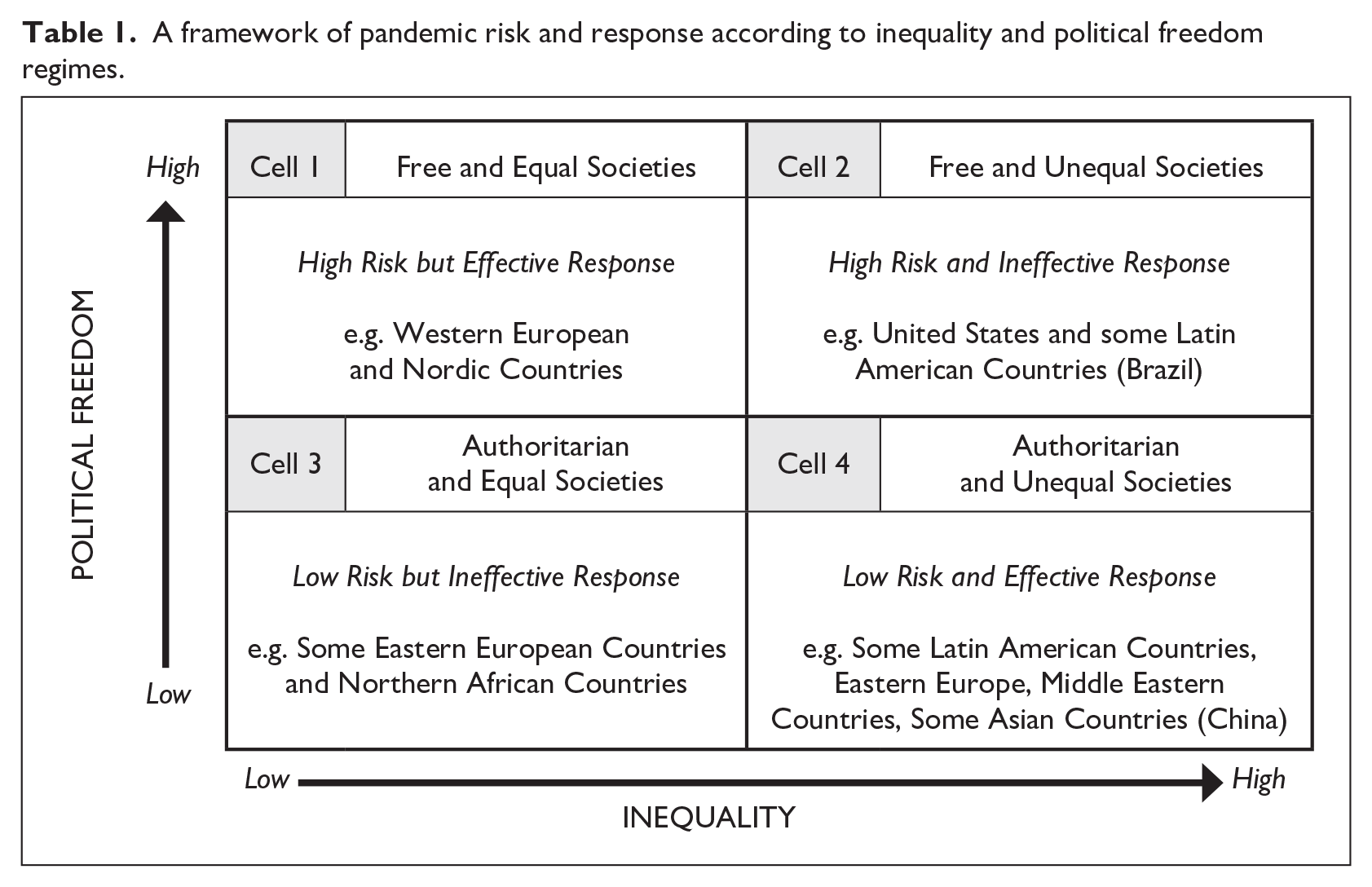
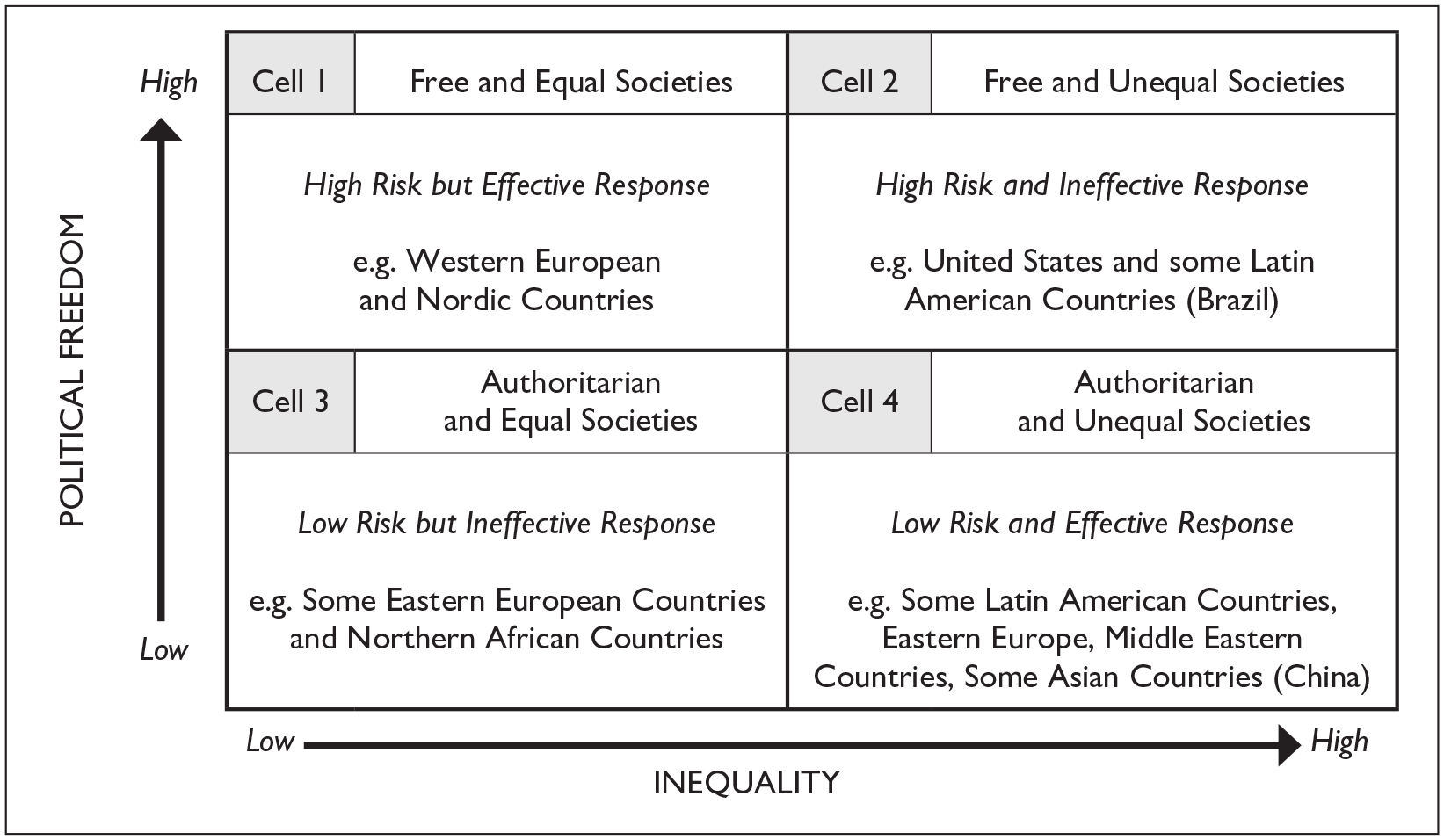
In Cell 1, in which generous welfare institutions have developed and implemented policies, implicit knowledge, and access points for the socially and economically vulnerable, potential COVID-19 victims are likely to receive effective care through existing welfare institutions, including public or publicly guided/coordinated medical care providers. Therefore, although political freedom may expose citizens to high risks, the robust efforts of the welfare state will effectively manage and mitigate the impact on victims. In this society, more freedom does not necessarily lead to higher confirmed cases in the long term. 2
Next, Cell 2 of Table 1 depicts that when less generous welfare states are not interested in protecting the vulnerable at society’s margins, the higher level of political freedom (high risks of virus spread) will translate into a higher number of confirmed cases due to the ineffectiveness of initial state responses. When contrasting this scenario with Cell 1, we can assume that among the countries with a high level of political freedom, the underdevelopment of welfare states may serve as a key component contributing to the escalation of COVID-19 cases.
In contrast, Cell 3, in which relatively equal societies coexist with low political freedom, is well illustrated by some East European countries such as the Russian Federation, Belarus, Azerbaijan, and Kazakhstan, namely, the countries from former Soviet Union. Even if inequality is regarded as low in these societies, it reflects low levels of development in which citizens conform to the lack of political freedom and are not properly taken care of by the existing state welfare. At the same time, post-Soviet states are heavily challenged by their unsettled economy and decentralizing healthcare systems (Issanov et al., 2020). In these societies, the coronavirus pandemic risk could become more severe over time, as government response is relatively ineffective.
In Cell 4, in which unequal societies, often coupled with authoritarian regimes (prevalent in Asia, Africa, and the Middle East), it is possible that unequal and unfree societies, such as China, produce the best performance outcomes regarding the prevention of coronavirus pandemics. These competitive authoritarian regimes may also seek rapid economic growth strategies—like the Chinese government does—by enabling big businesses and urban formal sectors (Lipton, 1977) to disproportionately accumulate income and wealth. There is a possibility that these regimes may develop strong and harsh coercive state apparatuses to monitor and suppress citizens’ desires for more equal distribution (Acemoglu and Robinson, 2006), despite high suppression costs. Therefore, a competitive authoritarian government, which quells any free association and speech desires effectively, may simultaneously utilize their state policing systems for detecting and tracking viruses. They may implement policies tracing citizens using its penetration devices within civil society. The MENA (Middle East and North African) region has been known for proactive efforts in addressing the COVID-19 crisis from its inception, imposing quarantine and curfew measures coupled with severe penalties for non-compliance. The pandemic has catalyzed substantial investments in the healthcare sector across MENA countries (OECD, 2020). Countries on the Arabian Peninsula, which rely heavily on oil revenues, have identified COVID-19 as a major threat due to the sudden plunge in global oil demand, which led them to adopt measures such as border closures to prevent the proliferation of the virus (Saleh, 2022). Under these situations, autocratic regimes with high inequality may paradoxically perform better than autocracies with low inequality (as in Cell 3). 3 Consequently, we build the third hypothesis: In more unequal societies, greater political freedom will be associated with higher COVID-19 confirmed cases, while in more equal societies greater political freedom will be associated with lower COVID-19 cases. However, the impact of COVID-19 diffusion is not solely determined by the sociopolitical environment of a society but is also shaped by the inherent nature of the virus and its mechanisms for infiltrating a society. Therefore, we will deliberately estimate the effects of political freedom and income inequality on the COVID-19 situation in 4-month intervals within the initial year of the infection. By considering the time variance during the early stages of the COVID-19 infection, we aim to catch the deliberate mechanisms of the interrelationship between political freedom, income inequality, and a global pandemic by examining these effects over distinct intervals.
Data
We use multiple data sources to examine the association between political and economic structure and pandemic. These sources include Daily COVID-19 cases and deaths by date reported to the World Health Organization (WHO), Standardized World Income Inequality Database (SWIID), Freedom in the World Index from Freedom House, and World Development Indicators of the World Bank. The overall dataset comprises 126 nations that have reported their pandemic situation to the WHO. As our analysis focuses on the initial stage of COVID-19 infection, we use the year 2020 as the primary period of interest. Furthermore, we divide this focal year into 4-month intervals to capture the transitions in international and national responses to the newly emerged disease. The number of observations in the overall dataset is detailed in Appendix 1. The correlations between the variables are presented in Appendix 2, and the countries included in the dataset are listed in Appendix 3. Due to the missing data for various measures, the sample sizes vary among the estimated models, contingent on the inclusion of specific independent and dependent variables.
Dependent variables
Confirmed COVID-19 case rate
This study sets “cumulative confirmed cases per 1 million people” as the dependent variable, corresponding to the hypothesis that the main independent variables such as inequality (Gini index) and democracy (extent of political freedom) are highly associated with the spread of coronavirus. However, this variable could reflect a compounded effect (the more there are tests, the more there are confirmed cases) if we account for each nation’s diverse coronavirus testing pattern. 4 A major problem for cross-national comparisons of COVID-19 is the underreporting of cases and deaths. Low-income countries with poor governance and welfare institutions may have lower capacities to collect reliable data. Autocratic regimes are very likely to underreport the confirmed cases and deaths. This issue also pertains to some democratic countries that tried to underreport to show off the government’s COVID-19 responsiveness.
To remedy these systematic biases, we employ two strategies: For COVID-19 confirmed case rates, we include “COVID-19 testing” as one of the covariates, which represents the total number of tests run per 1000 people, sourced from COVID-19 Testing by Our World in Data (Hasell et al., 2020). For COVID-19-related deaths, we utilize corrected estimates of COVID-19 deaths provided by the Institute for Health Metrics and Evaluation (IHME). IHME calculated estimates of underreporting by comparing reported COVID-19 deaths to excess mortality (Wang, 2021).
We use data on the COVID-19 situation obtained from the WHO, limited to the period between 3 January 2020, and 15 December 2020. This timeframe was chosen because vaccines became available from mid-December in some advanced countries, significantly altering the pandemic’s dynamics. The final sample comprises 126 countries after listwise deletion. We excluded a dozen (mostly island) countries with populations smaller than 1 million and several other countries for which social protection data were unavailable. 5
Independent variables
Net Gini and reduced inequality
To measure income inequality, we used the Gini index from the SWIID (Solt, 2020). This database integrates inequality data drawn from national statistical offices worldwide, including sources such as the Luxembourg Income Study (LIS), the OECD Income Distribution Database, the World Bank, and Eurostat. SWIID provides the most comprehensive comparable Gini indices for 192 countries by minimizing reliance on problematic assumptions, thereby enabling optimal cross-national inequality comparison (Solt, 2020).
This study employs two measures to denote income inequality: net income inequality and reduced inequality. Net income inequality is represented by the Gini coefficient of post-tax and transfers inequality, which is calculated based on equivalized household disposable income. In this study, we define net income inequality as net Gini. In addition, reduced inequality follows the measure proposed by Bradley et al. (2003), which assesses the state’s effect on inequality reduction through taxes and transfers. The equation for reduced inequality is provided below:

where market income Gini refers to the pre-tax and transfer Gini calculations based on market income, which includes the total income from wages, self-employment income, private pension income, and other similar sources. By subtracting net income inequality from market income inequality, we calculate the reduction in inequality achieved through taxes and transfers. Dividing this reduced inequality by market income inequality allows us to measure the proportional reduction in income inequality. This measure captures the degree of the government’s redistributive effort to reduce inequality through taxation and government transfers.
Political freedom
To assess the extent of political freedom in each nation, this study uses the “Freedom in the World” Index provided by Freedom House. 6 This index scores countries on a scale of 0–100 points, based on 10 political rights indicators and 15 civil liberties indicators, each ranging from 0 to 4. Essential indicators include the electoral process, political pluralism and participation, government functioning, freedom of expression and belief, associational and organizational rights, the rule of law, personal autonomy, and individual rights (Freedom House, 2020).
The Freedom House index is widely used in studies exploring various dimensions of freedom, such as press freedom and freedom of expression (Sandoval and Collins, 2016), as well as political background and democracy (Giannone, 2010; Steiner, 2014). It is considered ideal for measuring civic and political freedom because it comprehensively covers the institutional aspects of democracy and individual freedoms pertaining to civil society’s social and organizational matters.
The individual and social rights manifested in organized gatherings and activities can serve as an incubator for virus diffusion through human interactions. This risk is exacerbated in non-conforming civil societies due to political and religious extremism and non-compliance with government orders. Moreover, democratic political processes and political pluralism not only preserve civil rights but also encourage social and organizational gatherings based on individual and social rights. This dynamic is particularly evident when partisan politics intersect with religious organizations, as observed in countries like the US and South Korea during the COVID-19 pandemic.
Therefore, we utilized the global measure from Freedom House as the primary indicator of the extent of social and political freedom in civil societies, in preference to other popular measures of democracy (e.g. Polity IV series, which focuses more on institutional constraints of democracy). 7
Control variables
Population, population density, and health system capacity
The major mechanism of COVID-19 infection is rapid human-to-human transfer (Shereen et al., 2020). An infected individual can spread the virus through coughing, respiratory droplets, sneezing, or aerosols. People who come into contact with these aerosols can become infected if they inhale them through their nose or mouth (Phan et al., 2020; Riou and Althaus, 2020). Consequently, both the total population and its density are crucial factors in explaining the COVID-19 situation. Therefore, we control for total population and population density (Hamidi et al., 2020; Wong and Li, 2020), averaged over the period from 2009 to 2018, to enable a comparative study across countries. 8
In addition, research has indicated that older adults face increased fatality rates from COVID-19 (CDC COVID-19 Response Team et al., 2020). This heightened vulnerability suggests that the demographic structure of a country may influence the impact of COVID-19 (Bonanad et al., 2020; Jordan et al., 2020; Promislow, 2020). To account for this, we include the proportion of the elderly population in our analysis. We also incorporate the total number of hospital beds per 1000 people to assess the capacity of medical institutions to manage the pandemic (Ghisolfi et al., 2020). Despite the strong correlation between the elderly population and hospital beds per 1000 people (r = 0.69, p < .001), both variables are included due to their theoretical importance in understanding COVID-19 diffusion mechanisms (Sen-Crowe et al., 2021).
Finally, we control for the proportion of young people (aged 15–24 years), who are generally more active in social gatherings and thus more likely to contribute to virus spread (Park et al., 2020).
Economic growth indicators and geography
Gross domestic product (GDP) is a common indicator of the state’s economic growth (Brinkman and Brinkman, 2011 ; Fedderke and Klitgaard, 1998). The level of economic development can reflect a country’s capacity for managing COVID-19, including the ability to conduct testing and implement control measures. Therefore, we include the average GDP per capita from 2009 to 2018 to account for the effect of economic growth on the COVID-19 situation. This allows us to assess how variations in economic development may influence the pandemic’s effects across different countries.
Furthermore, economic openness represents a country’s level of globalization, facilitating the international exchange of economic and human capital. Given that COVID-19 spreads through human-to-human transmission, a country’s participation in the global market could influence the pandemic’s dispersion. Braudel (1992), in his opus on civilization and materialism, noted that in the fifteenth and sixteenth centuries, epidemics proliferated along the global Europe trade routes. Thus, we include total trade volume (exports plus imports of goods and services as a percentage of GDP), averaged over 10 years, as an alternative indicator of globalization and economic openness, sourced from the World Bank.
Finally, we introduce a dummy variable for island nations and a categorical variable representing continental regions to control the geographical factors that may contribute to divergent experiences with COVID-19 across countries. Island nations are advantageous in rapidly implementing and enforcing lockdown measures, which can result in more effective protection of their citizens compared with subnational islands or countries facing borders with other countries (Craig et al., 2020; Murphy et al., 2020; Sindico et al., 2020). Also, Zahid and Perna (2021) reported the substantial variation in COVID-19 mortality rates across continents, highlighting that Europe exhibits the highest mortality rates, while Africa registers the lowest. To control these regional differences, we categorize countries into six continental groups: North America & Europe, Latin America & Caribbean, East Asia & Pacific, Central & South Asia, sub-Saharan Africa, and Middle East & North Africa.
Method
Our dataset contains the latest 10-year (2009–2018) average indicators of inequality, political freedom, social protection, and demographic information for 126 countries, which were merged from various sources. As our analysis involves a relatively small cross-sectional dataset (n ⩽ 250), we employ an ordinary lease squares (OLS) regression model with a heteroskedasticity consistent covariance matrix (HCCM) known as HC3 (Long and Ervin, 2000). 9 Our main regression equation was

where Yi refers to the Confirmed Case Rate in each model. Xi indicates our independent variables, which are Net Income-based Gini or Reduced Inequality. Fi refers to Political Freedom, making XiFi an interaction term between the two independent variables with Political Freedom. Ci included control variables.
We analyze both cumulative data and change-score data across three time points. For cumulative data, we consider January–April (Wave 1), January–August (Wave 2), and January–December (Wave 3), while we employ the change-score calculated from May to August and from September to December. During the first period, WHO activated the initial responses to alarm the escalating pandemic situation and conducted research on COVID-19 while the COVID-19 infection was under the government’s limited tracking capacity on the regional level. The second period served as an interim period that WHO issued guidance on contact tracing and large-scale movement restrictions. Numerous countries imposed international travel bans during this time. In the third period, advancements in COVID-19 testing, particularly the approval and use of rapid diagnostic tests, significantly improved the government’s capacity for case detection. For cumulative data, each period encompasses confirmed cases or deaths from previous periods. However, in the change-score data, each period includes only the newly added cases or deaths specific to that time point.
Results
Multivariate regression analysis
Table 2 tests the hypotheses mentioned above regarding the proposed relationships between confirmed COVID-19 case rates, inequality (or efforts to mitigate inequality), and the extent of freedom in each country. In Table 2, we investigate whether our democracy–inequality interaction models account for the different phases of COVID-19 pandemics by sub-dividing pandemic periods into three conjunctures: an initial impact period (from January 2020 to April 2020), a middle adjustment period (from May 2020 to August 2020), and a greatly diverging period (from September 2020 to December 2020). Each dependent variable measures the cumulative confirmed case rate since 3 January 2020. First, we employ ordinary least squares (OLS) models (using HC3) without any interaction terms to investigate each variable’s main effect on confirmed COVID-19 case rates (Models 1, 3, 5). Following baseline models, we included interaction terms to explore the dynamics between inequality and political freedom (Models 2, 4, 6) in Table 2.
Multivariate linear regression (using HC3) of cumulative confirmed case rates at three time points: interaction models of political freedom and inequality.

Note: All variables except Political freedom and Island nations are in logarithmic form. Confirmed cases is the log transformation of cumulative confirmed cases per 1 million people. t statistics in parentheses.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
Model 1 in Table 2 demonstrates that, of the various control variables, GDP per capita and population density are positively associated with the level of confirmed case rates. This suggests that countries with higher economic affluence and larger population concentrations are more susceptible to COVID-19 exposure due to its nature, which makes its incidence prone to a high volume of social and economic activities. The number of hospital beds has a marginal significance in reducing the COVID-19 infection. Our primary independent variables of interest, political freedom and net Gini, are both statistically significant. While a higher level of political freedom increases COVID-19 infections, the more unequal nations are less exposed to the pandemic in Wave 1. This finding supports our first hypothesis that countries with more political freedom will see increased COVID-19 infections within a society. However, countries that are relatively more unequal experienced a weaker impact from COVID-19 infections in Wave 1, which rejects our second hypothesis. In Models 3 and 5, political freedom does not significantly affect confirmed case rates, but net Gini shows a marginally significant positive effect on confirmed case rates in Model 3. This result suggests that while initially equal societies may face higher exposure to COVID-19, inequality may become a crucial factor in understanding the virus’s longer-term diffusion.
Models 2, 4, and 6 introduce the interaction terms between net Gini and political freedom to scrutinize the main hypothesis of this study. Although independent variables and their interaction term are not significant in Wave 1 (Model 2), they are significant in all subsequent models. The results in Models 4 and 6 affirm our third hypothesis, indicating that, in more unequal societies, greater political rights will be associated with higher COVID-19 confirmed case rates, while in more equal societies, greater political rights will lead to a lower number of coronavirus cases (per 1 million people). These findings suggest that liberal democracy may indeed serve as a reservoir for pandemics when coupled with highly unequal distributional structures within such institutional environments.
Table 3 tests the same framework against alternative dependent variables. In Models 1–4, we test “change scores” of confirmed case rates between three time points. Model 3 reveals a positive association between net Gini and the increment in newly reported case rates observed from April to August 2020. This finding suggests that higher level of income inequality correspond to an increased vulnerability to COVID-19 risks during Wave 2. In Models 5 and 6, we test IHME estimates to ameliorate concerns regarding underreported cases in authoritarian and underdeveloped countries. The interaction terms are statistically significant for all models, and the patterns of coefficients are also nearly identical with the results in Table 2. Overall, two contrasting trends of democracy-confirmed case rate under low and high inequality are robust between actual reported cases and estimated IHME cases.
Multivariate linear regression (using HC3) of changes in confirmed case rates at two time points and IHME estimates: interaction models of political freedom and inequality.

Note: All variables except Political freedom and Island nations are in logarithmic form. Newly added cases is the log transformation of cumulative confirmed cases per 1 million people between two time points. IHME Estimates refers the logarithmic form of COVID-19 death toll estimates, aiming to account for underreporting as corrected by the IHME. t statistics in parentheses.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
Figure 1, built based on Model 6 in Table 2, displays how the slope of political freedom varies depending on the level of net Gini. 10 The results suggest that, at lower values of net income inequality, the effects of political freedom are negative, implying that in equal societies, freedom tends to reduce the COVID-19 confirmed case rate. However, at the mean value of income inequality, such a relationship became flattened, while at a higher level of income inequality, political freedom clearly increases the confirmed case rate. That is to say, at the lowest level of inequality (logged net Gini = −1.4, at the 1st percentile), the 1 unit increase of freedom in Model 6 decreases (natural logged) confirmed case rate by 0.0214(−0.0214 = 0.05 + 0.051*(−1.4)), but at the highest level of inequality (logged net Gini = −0.46, at the 99th percentile), the same 1 unit increase in freedom increases (natural logged) confirmed case rate by 0.07346 (0.07346 = 0.05 + 0.051*(−0.46)).
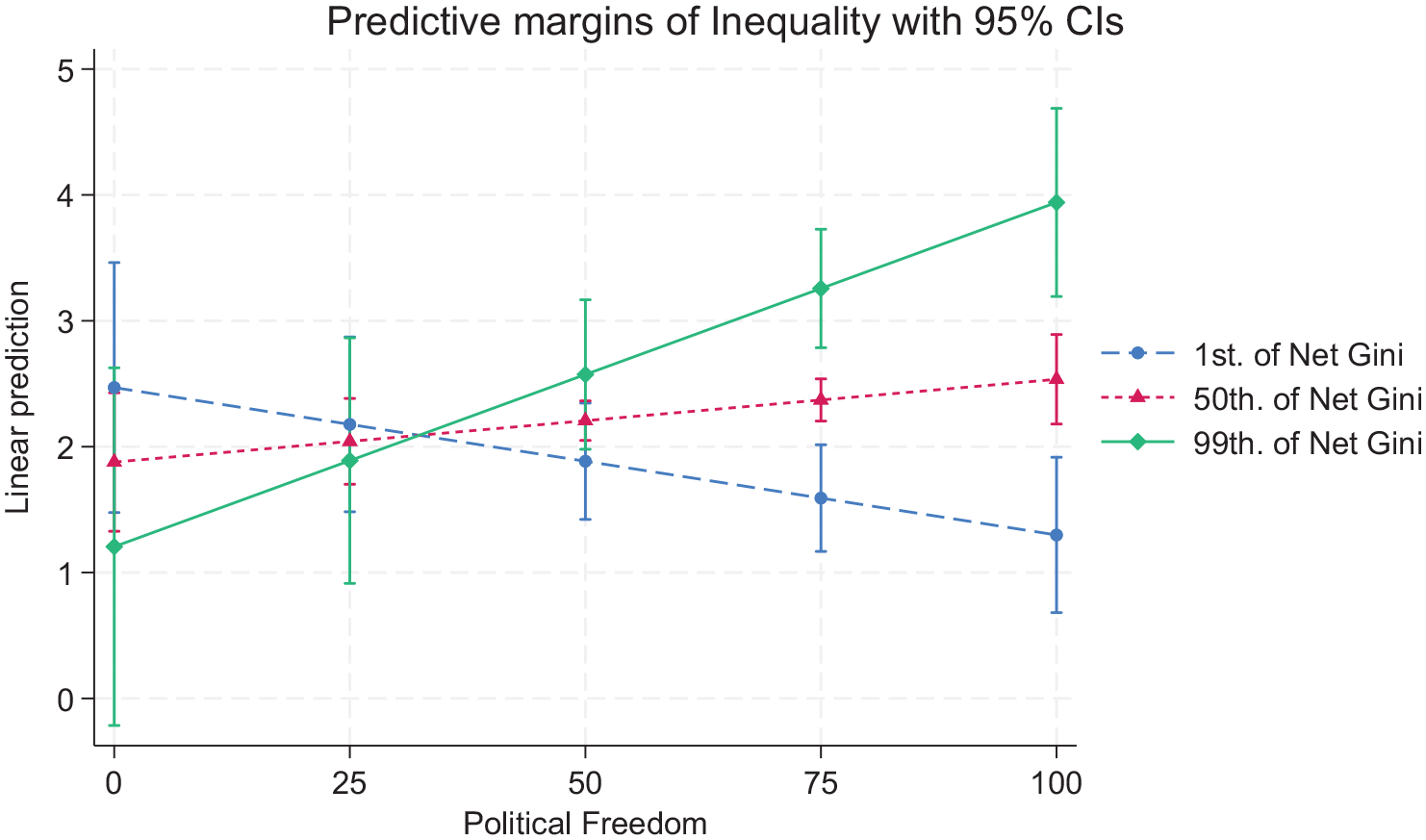
Presentation of political freedom–inequality interaction effects in Wave 3 (15 Dec 2020) [Model 6 in Table 2].
Then, when does the marginal effect prevail (statistically)? Figure 2 displays the marginal effects of political freedom on IHME estimates of COVID-19 death cases as measures of inequality change from a 1st percentile to a 99th percentile value (1%, 10%, 25%, 50%, 75%, 90%, and 99%). Bars in panel in Figure 2 are the histogram and the vertical line on the right side indicates the percentage of observations. The panel in Figure 2 illustrates that the marginal effect with its confidence intervals (Brambor et al., 2006) of political freedom is statistically different from zero when net income Gini is greater than 0.38 (equivalent to −0.96 on the natural logged net Gini scale). Thereby, the graph demonstrates that the size of the freedom effect on COVID-19 death cases increases as net income inequality increases.
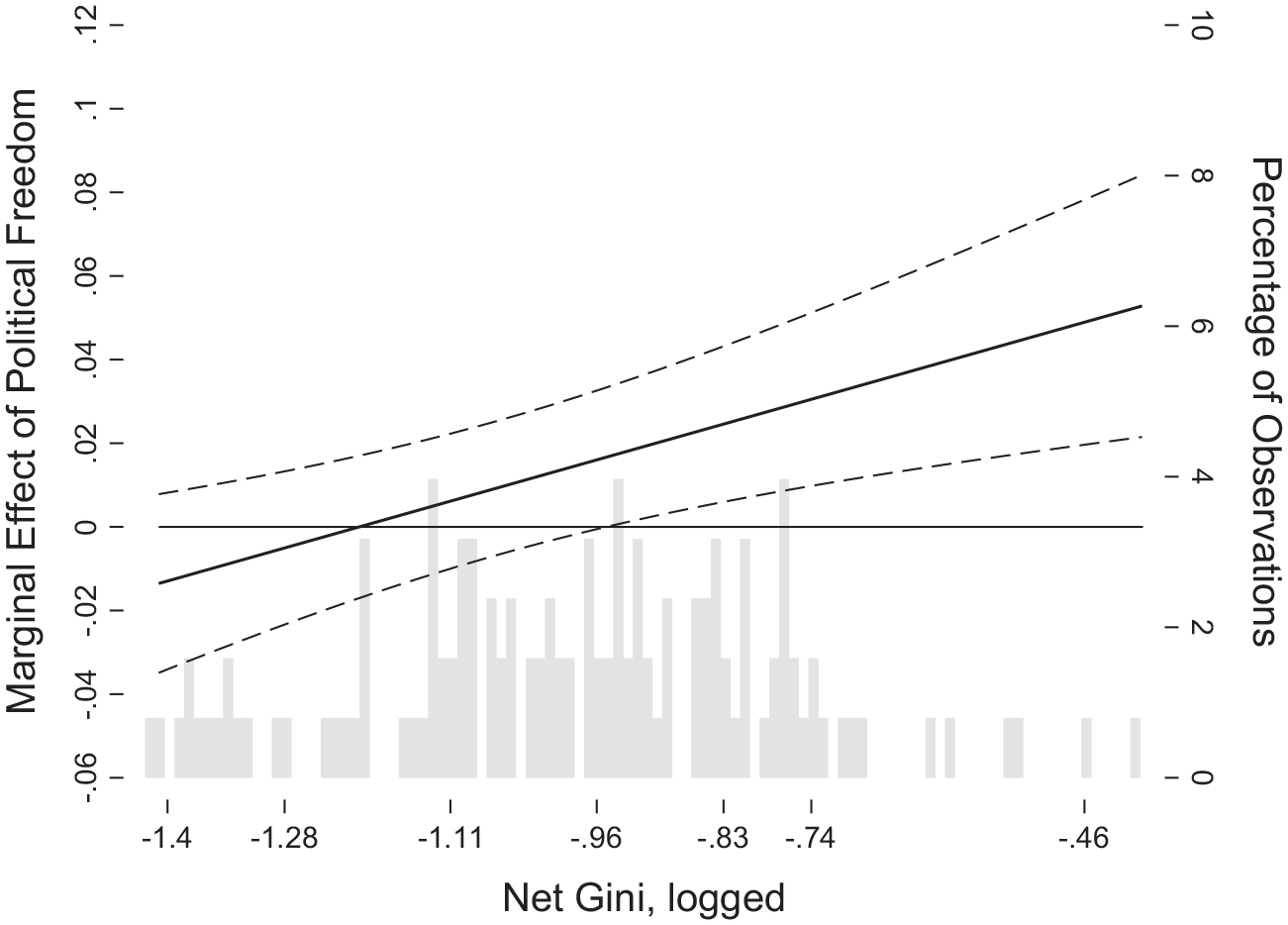
Average marginal effects of political freedom on IHEM estimates of COVID-19 death tolls with 95% intervals conditional on net Gini (with controls).
Table 4 introduces six region-based dummy variables to account for unobserved region-specific cultural, geopolitical, and genetic inheritance factors. Comparative to North America and Europe, all other regions show significantly lower confirmed case rates in Waves 1 and 3. In addition, the effects of political freedom and net Gini become insignificant in Model 1 when continental regions are controlled. However, income inequality is positively associated with the COVID-19 confirmed case rates in Models 3 and 5. These results confirm our second hypothesis, suggesting that COVID-19 confirmed cases will be higher in unequal societies. The findings also indicate that, despite the relatively delayed exposure to COVID-19, unequal societies may undergo rapid diffusion of the virus. This can be attributed to socially and economically marginalized individuals facing higher risks, stemming from inadequate social safety nets, limited medical assistance, and fragile social coordination within such societies. The significant effects of the interaction models have been reduced, but they remain statistically significant at alpha = 0.01 level, implying that political freedom × inequality interaction models account for variations in confirmed case rates within each continental region. Table 5 tests alternative measures of dependent variables as we did in Table 3. For the change scores of confirmed cases and the IHME estimates, our main interaction models are consistently significant and robust, even after controlling for region-specific dummy variables.
Multivariate linear regression (using HC3) of cumulative confirmed case rates at three time points: interaction models of political freedom and inequality including region dummies.
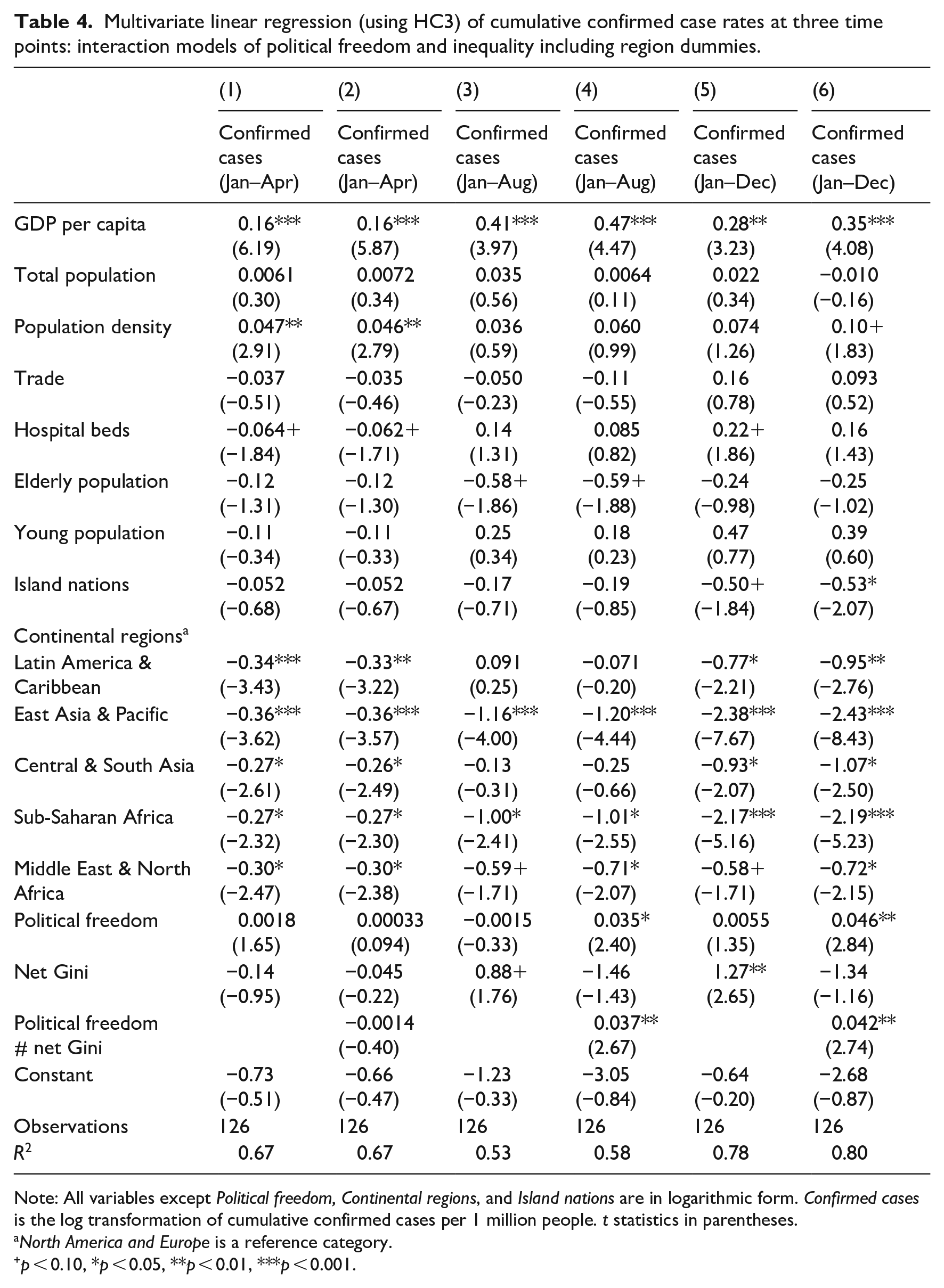
Note: All variables except Political freedom, Continental regions, and Island nations are in logarithmic form. Confirmed cases is the log transformation of cumulative confirmed cases per 1 million people. t statistics in parentheses.
North America and Europe is a reference category.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
Multivariate linear regression (using HC3) of changes in confirmed cases at two time points and IHME estimates: interaction models of political freedom and inequality including region dummies.

Note: All variables except Political freedom, Continental regions, and Island nations are in logarithmic form. Newly added cases is the log transformation of cumulative confirmed cases per 1 million people between two time points. IHME Estimates refers the logarithmic form of COVID-19 death toll estimates, aiming to account for underreporting as corrected by the IHME. t statistics in parentheses.
North America and Europe is a reference category.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
Furthermore, we conducted supplementary analyses using the 2023 Inglehart-Welzel World Cultural Map (Inglehart and Welzel, 2005) instead of continental dummies. Researchers have highlighted that societal culture is significantly associated with COVID-19 outcomes, including morbidity and mortality (Gokmen et al., 2021; Kumar, 2021). Mayer et al. (2020) argue that the degree of political freedom is not linked with COVID-19 infection; however. countries with Confucian and South Asian cultural backgrounds showed a temporary superiority in disease response. Despite these insights, the results of the supplementary analyses align with our primary findings (see Appendix 5).
Models in Table 6 control for the number of national lockdowns for confirmed case rates until 15 December 2020. The models purport to test whether the government’s unyielding policy choice contributes to reducing confirmed cases. The results show that countries employing national lockdown policies do not significantly differ from other countries in their counts of COVID-19 victims. Countries that adopt national lockdowns must have used them as the final resort, facing the uncontrollable spread of the disease, which incurs an endogeneity concern. 11 Overall, however, the variable does not affect the main outcome of this study: with or without this variable, our primary freedom–inequality interaction model is robust.
Multivariate linear regression (using HC3) controlling lockdown effects and COVID-19 testing (15 Dec 2020).
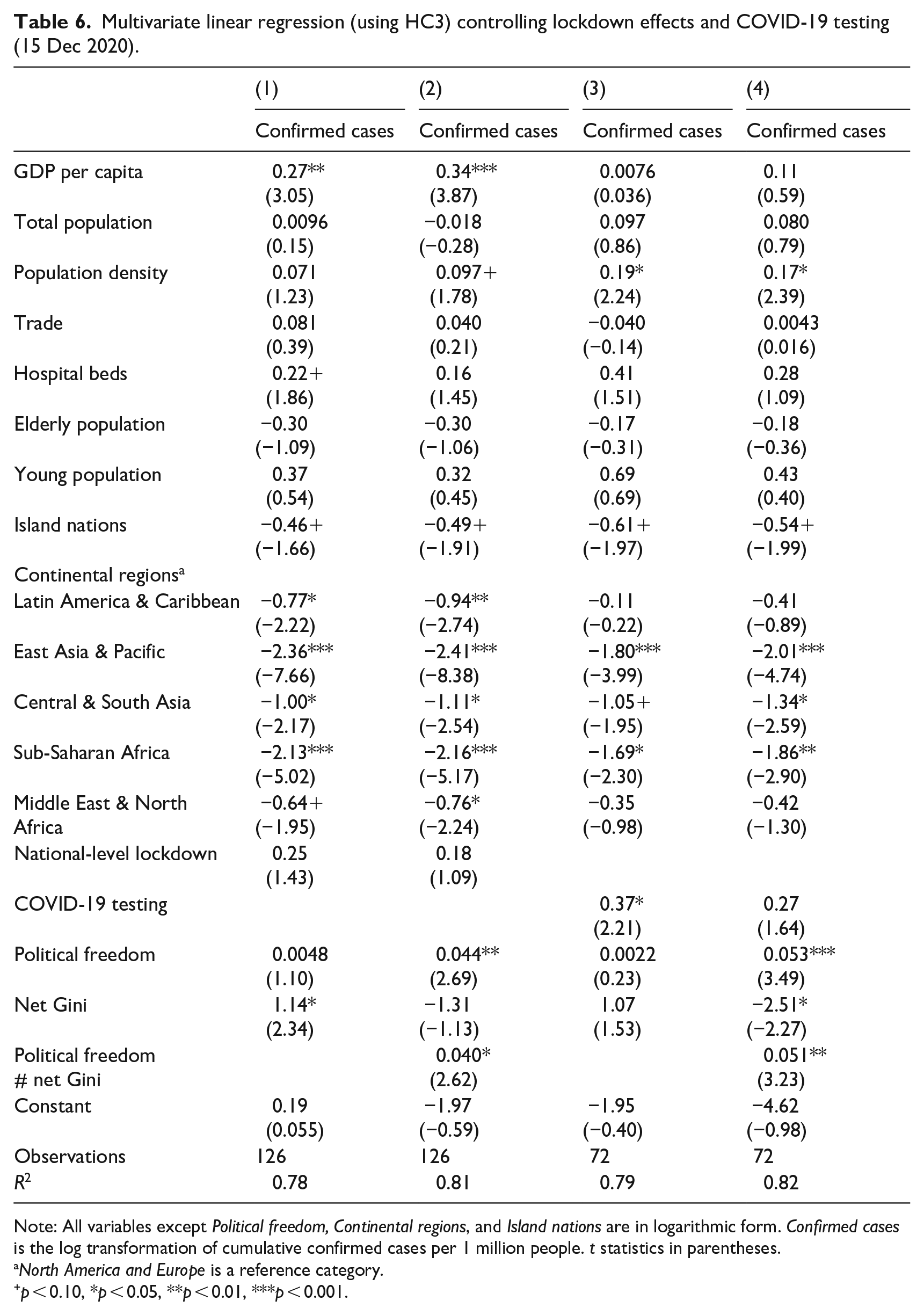
Note: All variables except Political freedom, Continental regions, and Island nations are in logarithmic form. Confirmed cases is the log transformation of cumulative confirmed cases per 1 million people. t statistics in parentheses.
North America and Europe is a reference category.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
Models 3 and 4 in Table 6 introduce an important control variable: test cases. If some countries have more medical and administrative capacity to conduct COVID-19 tests, then they will naturally have higher confirmed case rates. In Model 3, with the COVID-19 testing variable, GDP per capita became nonsignificant, suggesting that there exists collinearity between two variables. As more affluent countries have greater administrative capacity to conduct tests, it is not surprising. When our main interaction term is introduced in Model 4, our independent variables are significant. While net Gini and political freedom are significant at alpha = 0.05 and 0.01, respectively, the interaction term of them is highly significant at alpha = 0.001 level. This implies that, with the same level test numbers (per 1000 people), the proposed democracy × inequality interactive relationship gets even stronger.
In Table 7, we test whether the welfare state’s efforts to reduce inequality affect the political freedom–coronavirus linkage, utilizing measures of inequality-(reduction) other than the net Gini. As in Table 2, we initially explore whether political freedom, which indicates institutionalized political participation and pluralism, paradoxically contributes to the spread of COVID-19 (addressing Hypothesis 1). Then, we test the effects of an interaction term between political freedom and reduced inequality on confirmed COVID-19 case rates to determine if the welfare state’s reduction in inequality ameliorates the positive associations between inequality and COVID-19 spread.
Multivariate linear regression (using HC3) of cumulative confirmed case rates at three time points: interaction models of political freedom and reduced inequality, including region dummies.

Note: All variables except Political freedom, Reduced inequality, Continental regions, and Island nations are in logarithmic form. Confirmed cases is the log transformation of cumulative confirmed cases per 1 million people. t statistics in parentheses.
North America and Europe is a reference category.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
The results in Models 4 and 6 in Table 7 support our hypothesis that, at a lower level of the welfare state efforts to mitigate the inequality through taxation and transfers, a higher degree of political freedom contributes to a greater COVID-19 infection rate. Conversely, the relationship is reversed under more egalitarian welfare state efforts with high levels of taxation and transfers; higher political freedom is conducive to decreasing the COVID-19 infection rate at these high levels of welfare state efforts. The interaction term is highly significant at alpha = 0.01 in Model 4 and alpha = 0.001 in Model 6. These findings may support the assertion that politically liberal societies with severe inequality suffer greater partisan political polarization, as Thomas Piketty has recently observed in his opus (Piketty, 2020). This polarization may, in turn, result in the malfunction of virus control policies implemented by partisan incumbents. In societies where democratic partisan politics have failed to ameliorate socioeconomic inequality, a significant portion of either Left or Right partisan adherents may not align with the incumbent government’s efforts to control pandemics, as witnessed in some North American and Western European countries during the COVID-19 situation.
These findings are depicted in Figures 3 and 4. Figure 3, corresponding to Model 6 in Table 7, indicates that higher political freedom correlates with higher confirmed case rates in the presence of low levels of reduced inequality (reduced inequality = −12.4, at the first percentile), as illustrated by the blue short-dashed line. 12 Conversely, greater political freedom results in lower confirmed case rates under conditions of high levels of welfare state efforts (reduced inequality = 47.5, at the 99th percentile), as illustrated by the green solid line.
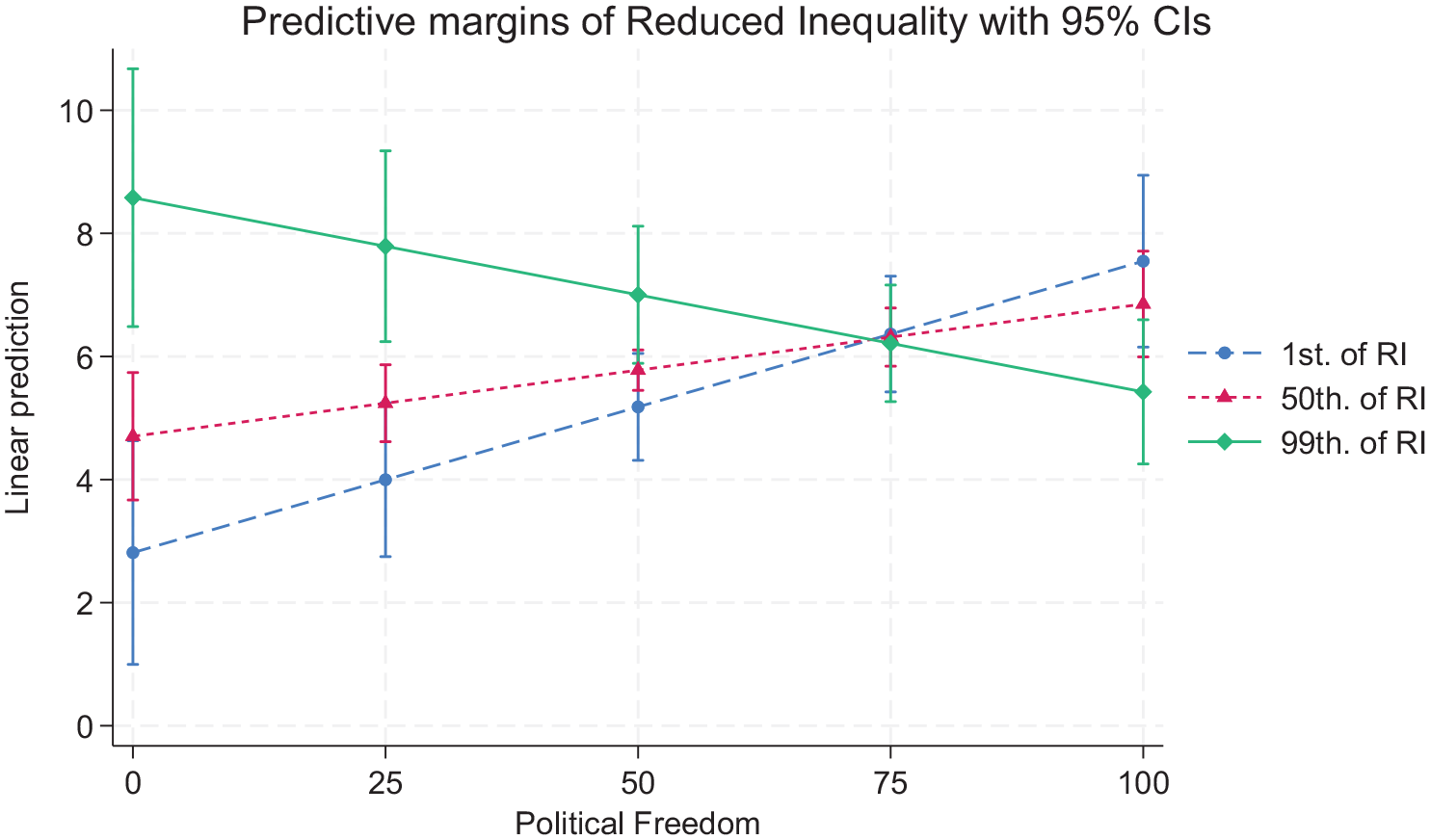
Presentation of political freedom-reduced inequality interaction effects in Wave 3 (Dec 15, 2020) [Model 6 in Table 7].
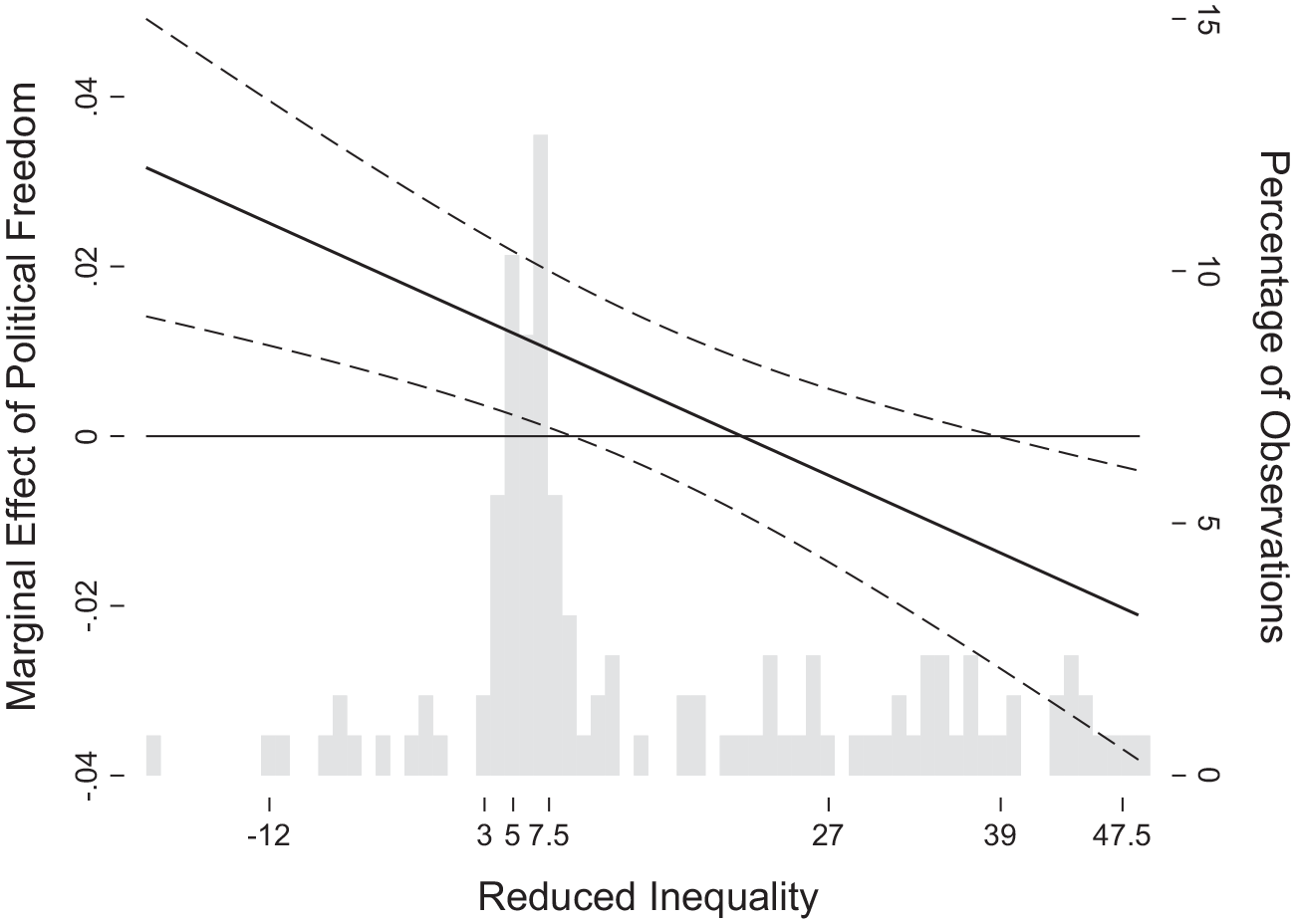
Average marginal effects of political freedom on COVID 19-confirmed cases with 95% intervals conditional on reduced inequality (welfare state efforts) with controls in Wave 3 (Dec 15) [Model 6 in Table 7].
Figure 4 illustrates how the marginal effects of political freedom on COVID-19 confirmed case rates vary conditional on reduced inequality—the welfare state efforts. At lower levels of reduced inequality, the marginal effects are positive, but at higher level of reduced inequality, the marginal effects become negative. In short, the divergent responses of democratic political mechanisms to the COVID-19 pandemic crisis were not evident when the pandemic first arrived in the early months of 2020. However, liberal democracy’s vulnerability to and resilience in the face of the pandemics emerged in subsequent period and continued to exert its influence. Our findings suggest that democratic governance responds to the crisis in markedly different ways depending on its inequality regime. In more equal societies, welfare states provide sufficient administrative efficiency and well-established medical systems to combat the viruses, enabling citizens and the state to participate in viral control and treat infected individuals. Such societies are more resilient in recovering from a pandemic, and the solidaristic institutions compensate for the cost of freedom and liberty. However, in more unequal societies, the lack of the public provision of universal social welfare and access to medical systems exposes citizens of lower socioeconomic status to a higher risk of infection from pandemics. In such societies, the cost of freedom and liberty is concentrated on the socially marginalized.
Discussion and conclusion
The primary finding of this study is that when higher levels of inequality exist, liberal democracy, as measured by political freedom, is positively associated with the spread of COVID-19. In comparison, at lower levels of inequality, political freedom is negatively related to the spread. Our central argument is that political freedom provides a potential reservoir for lethal infectious diseases, but this tendency is contingent upon previously institutionalized welfare regime efforts and inequality outcomes. An inequality-reducing regime will help all its constituents fight against the pandemic, while an inequality-increasing/perpetuating regime will leave its outsiders relegated to be victims of viruses. This study highlights the significance of pre-existing social protection systems when they support the lower classes and deter the spread of infectious disease. Motivated by recent studies on inequality and disasters (Kahn, 2005; Reininger et al., 2013) as well as previous literature on welfare states and democracy (Esping-Andersen 1990; Huber and Stephens, 2001; Przeworski, 1986, 1991, 1995), we underscore the importance of pre-existing welfare regimes in accounting for variations in COVID-19 confirmed rates. Such a focus is linked to our ultimate assumption that a regime with a record of protecting its citizens universally will do its best to protect them during a pandemic. In contrast, a regime nonchalant about its economically and socially disadvantaged citizens will demonstrate the same indifference to the vulnerable.
The surprising finding that inequality and liberal democracy closely interact with each other in explaining the spread and impact of COVID-19 highlights the importance of the antagonism between liberal democracy and disease control. We initially draw our attention to the dilemma faced by partisan incumbents between liberal democracy and bureaucratic control of citizens’ private spaces, which hampers deeper penetration of authorities into citizens’ everyday lives. We examine this bleak scenario in which political freedom fosters the spread of viruses under competitive electoral systems.
Finally, we simultaneously bring in the notion of social vulnerability. We propose that more equal societies, with their well-developed social welfare systems, allocate more resources to the socially isolated, thereby recovering equilibrium more quickly and at a lower cost. With this social vulnerability hypothesis, we also examine an optimistic scenario in which equality mitigates the pandemic’s negative impact on the vulnerable. Our interactive framework connects democracy and inequality to account for COVID-19’s spread and impact, integrating these two scenarios into a single model.
This study’s findings relate to an important theoretical issue in comparative political economy: the relationship between welfare states and virus control. Grounded in the framework of welfare state scholarship (Esping-Andersen 1990; Huber and Stephens, 2002; Korpi, 1983), this study posits that more egalitarian political regimes incorporating universal and generous welfare states may respond to pandemics more effectively than their liberal counterparts. However, at least among rich democracies, such as the US, the initial impact of the pandemic was severe. In societies with high freedom and high inequality, the socially and economically marginalized are unprotected by existing medical programs and facilities, and liberal government traditions fail to monitor and control those infected and conduct contact tracing. As a result, confirmed cases and deaths soared nearly exponentially. Similar phenomena were observed in Latin America, where societies have enjoyed liberty through recent democratization but remain deeply segmented by economic inequality.
Societies in southern continental Europe, such as Italy and Spain, have also suffered significantly from the deep penetration of viruses into civil society. In these societies, rich and dense civic networks with religious foundations, which remain largely intact from government influence, have served as reservoirs for virus infection. In contrast, Nordic countries (except for Sweden), Germany and its surrounding neighbors, and two other liberal countries, New Zealand and Australia, have performed quite well in controlling the spread and aftermath of COVID-19. With some variations, the latter countries typically have well-institutionalized medical and social welfare programs that support the socioeconomic lower classes.
In developing societies, some competitive authoritarian leaders (Brinks et al., 2019) may protect their relatively servile citizens more competently during this era of mass disasters. Societies where democratic traditions have not fully developed and that have therefore performed relatively well in disease control may face severe economic challenges and potentially more suppressive and harshly authoritarian governments after the pandemic. This is due to the highly concentrated and deeply penetrating state power granted by citizens during the crisis, as vividly illustrated by the Chinese case.
The politics of disasters in democratic regimes may, therefore, increase internal tensions. Cross-national and comparative evidence of variations in COVID-19 prevention and control suggests that current liberal democratic governments are not only vulnerable to attacks from viruses and other disasters but also to threats from diverse authoritarian and populist politics. As most liberal democratic regimes have not established an emergency contract between the state and civil society regarding citizens’ political and religious freedoms and private everyday lives, they are inherently susceptible to deadly viruses. Furthermore, since some liberal democratic societies lack the institutional capacity to reach marginalized citizens during large-scale disasters and pandemics, entire or partial populations become fundamentally vulnerable to the effects of charismatic (often authoritarian) leadership that resorts to populist or even totalitarian politics.
The global COVID-19 crisis and the findings from this study teach us that, in more egalitarian societies, the government established during stable times is better equipped to respond to citizen needs during crises. In contrast, in inegalitarian societies, where the government was minimized by citizens during settled times, there is insufficient capacity to meet citizen needs during unsettled ones. Therefore, how societies establish their approach to dealing with large-scale disasters will shape the social contract between the state and society in the aftermath.
Although this research makes theoretical and empirical contributions, there are some limitations. As we primarily focus on broad measure of political freedom and income inequality, future research will need to explore more in-depth mechanisms through which democratic institutions and aspects of social inequality—such as population composition, living conditions, and education—are associated with the successful control and management of disease infections. Future research will also need to examine the influence of the welfare system on managing disasters and recovery by using alternative measures of the welfare state’s capacity. In addition, apart from the welfare state, future research should investigate the roles of civil society in protecting populations marginalized by social safety nets. For example, social organizations might reveal the lack of aid to marginalized individuals, support them as supplementary welfare agencies, or pressure the government and private corporations to respond more actively. Consequently, further research that delves deeper into the mechanisms underlying the relationships identified in this study and the roles of civil society in enhancing the protection of the vulnerable during crises will contribute to a more comprehensive understanding of the dynamics of disease diffusion in potential pandemic crises.
Footnotes
Appendix
Supplementary analysis with regional dummy variables from the 2023 Inglehart-Wezel cultural map.

| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | |
|---|---|---|---|---|---|---|---|---|
| Confirmed cases |
Confirmed cases |
Confirmed cases |
Confirmed cases |
Confirmed cases |
Confirmed cases |
IHME estimates | IHME estimates | |
| GDP per capita | 0.15***
(3.80) |
0.15***
(3.83) |
0.55***
(3.69) |
0.58***
(4.05) |
0.65***
(4.29) |
0.67***
(4.74) |
0.31 (1.17) |
0.35 (1.37) |
| Total population | −0.019 (−0.73) |
−0.024 (−0.85) |
0.052 (0.66) |
0.019 (0.24) |
0.0081 (0.079) |
−0.021 (−0.22) |
0.13 (0.70) |
0.083 (0.47) |
| Population density | 0.086**
(2.75) |
0.089**
(2.97) |
0.12 (1.40) |
0.14+
(1.73) |
0.22*
(2.31) |
0.24**
(2.68) |
0.10 (0.74) |
0.13 (1.00) |
| Trade | −0.15 (−1.56) |
−0.15 (−1.58) |
−0.19 (−0.65) |
−0.22 (−0.81) |
0.018 (0.055) |
−0.013 (−0.041) |
−0.26 (−0.38) |
−0.31 (−0.45) |
| Hospital beds | −0.0033 (−0.065) |
−0.014 (−0.28) |
0.35
+
(1.71) |
0.27 (1.41) |
0.35
+
(1.96) |
0.28
+
(1.69) |
0.57
+
(1.98) |
0.47
+
(1.74) |
| Old population | −0.13 (−1.59) |
−0.14 (−1.54) |
−0.60 (−1.37) |
−0.66
+
(−1.97) |
0.063 (0.13) |
0.0048 (0.012) |
0.92 (1.66) |
0.84
+
(1.80) |
| Young population | −0.36 (−0.75) |
−0.37 (−0.77) |
0.60 (0.41) |
0.52 (0.40) |
2.01 (1.32) |
1.93 (1.43) |
2.18 (0.89) |
2.08 (0.92) |
| Island nations | −0.28**
(−2.88) |
−0.28**
(−2.91) |
−0.65
+
(−1.93) |
−0.60
+
(−1.98) |
−1.13**
(−2.84) |
−1.09**
(−2.89) |
−1.23 (−1.60) |
−1.16 (−1.49) |
| Cultural map a | ||||||||
| African-Islamic | −0.42*
(−2.25) |
−0.47*
(−2.46) |
−0.00089 (−0.0015) |
−0.34 (−0.61) |
0.55 (0.68) |
0.26 (0.32) |
1.99 (1.30) |
1.53 (1.00) |
| Catholic Europe | −0.067 (−0.32) |
−0.039 (−0.19) |
−0.20 (−0.35) |
−0.0072 (−0.014) |
0.89 (1.11) |
1.06 (1.42) |
1.62 (1.19) |
1.89 (1.43) |
| Confucian | −0.57
+
(−1.85) |
−0.56
+
(−1.89) |
−1.42*
(−2.24) |
−1.35*
(−2.38) |
−1.80
+
(−1.93) |
−1.73
+
−1.98) |
−2.23 (−1.23) |
−2.13 (−1.19) |
| Latin America | −0.44*
(−2.59) |
−0.49**
(−2.78) |
0.59 (1.00) |
0.25 (0.46) |
0.67 (0.85) |
0.37 (0.47) |
1.72 (1.18) |
1.26 (0.85) |
| Orthodox Europe | −0.30 (−1.45) |
−0.33 (−1.57) |
0.79 (1.16) |
0.59 (0.93) |
1.64
+
(1.83) |
1.46
+
(1.76) |
2.39 (1.57) |
2.11 (1.46) |
| Protestant Europe | 0.065 (0.39) |
0.13 (0.69) |
−0.24 (−0.45) |
0.17 (0.36) |
−0.16 (−0.20) |
0.21 (0.28) |
0.28 (0.21) |
0.85 (0.66) |
| West & South Asia | −0.39
+
(−1.77) |
−0.44
+
(−1.99) |
−0.24 (−0.36) |
−0.57 (−0.91) |
−0.39 (−0.41) |
−0.68 (−0.74) |
−0.92 (−0.50) |
−1.37 (−0.76) |
| Political freedom | −0.00010 (−0.059) |
0.0065 (0.96) |
0.0030 (0.66) |
0.048**
(2.87) |
0.0072 (1.28) |
0.047*
(2.22) |
0.013 (1.12) |
0.075*
(2.41) |
| Net Gini | 0.13 (0.66) |
−0.24 (−0.83) |
0.67 (1.22) |
−1.91 (−1.67) |
0.30 (0.54) |
−1.97 (−1.49) |
0.25 (0.24) |
−3.33 (−1.66) |
| Political freedom # Net Gini |
0.0069 |
0.047**
|
0.041
+
|
0.065*
|
||||
| Constant | 1.33 |
1.12 |
−4.50 |
−5.93 |
−11.0
+
|
−12.3*
|
−8.25 |
−10.4 |
| Observations | 92 | 92 | 92 | 92 | 92 | 92 | 91 | 91 |
| R 2 | 0.69 | 0.69 | 0.52 | 0.57 | 0.71 | 0.73 | 0.63 | 0.65 |
Note: Cultural map is a categorization of countries according to the degree of cultural values related to secularity and quality of life (Inglehart and Welzel, 2005). All variables except Political freedom, Cultural map, and Island nations are in logarithmic form. t statistics in parentheses.
English-Speaking is a reference category.
p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Education, Republic of Korea, NRF-2021S1A5B1096737.