
Abstract
This article critically examines the use of national border closures at the outset of the COVID-19 pandemic. After explaining why targeted border closures generally do not work and how they violated international law at the time, we examine the unprecedented case of total border closures. Positing that since the current instruments and institutions of global health governance did not anticipate this phenomenon, the legality of total border closures rests on less certain grounds. Then, after asking why nearly every government implemented some form of border closure in March 2020 if neither science nor law provided adequate motivation for their use, we conclude that in the face of a global health emergency, border closures represent an opportunity for political leaders to show determined action, redirect blame to other jurisdictions, and reinforce nationalism. We proceed to argue that both targeted and total border closures have profound legal, epidemiological, and political significance as performances that contradict global realities while undermining notions of global solidarity. Such political theatre means that citizens must weigh these consequences against any perceived benefits of border closures as they would any other politically driven government action, and contest and challenge them appropriately. Citizens must not unduly defer to scientists or lawyers on early COVID-19 border closures because these were primarily political—not scientific or legal—decisions. In this vein, we conclude with some guiding political considerations for scrutinizing government decisions to close borders and observations for the future of global health cooperation during infectious disease outbreaks.
Keywords
With infectious disease outbreaks come pressure on national governments to restrict international travel from affected countries. Many governments give way to this pressure, even when such measures are not rooted in public health guidance or scientific evidence. Controls on international travel from high-risk regions, implemented by dozens of countries within the first 2 months of the COVID-19 outbreak (see Figure 1) and after the discoveries of its variants of concern, isolated vulnerable communities, devastated fragile economies, and disincentivized affected governments from reporting new cases of disease.
1
Such measures, referred to in this paper as “targeted border closures” (see Table 1), are also considered in many instances to be infringements of the International Health Regulations (IHR)—the legally binding instrument administered by the World Health Organization (WHO) that governs how nearly all the world’s countries respond to public health emergencies of international concern (PHEIC) like COVID-19.
2
In turn, targeted border closures undermine our system of cooperation on global public health and the rules-based world order on which we depend
3
(Figure 2). International travel restrictions as of 18 March 2020.
4
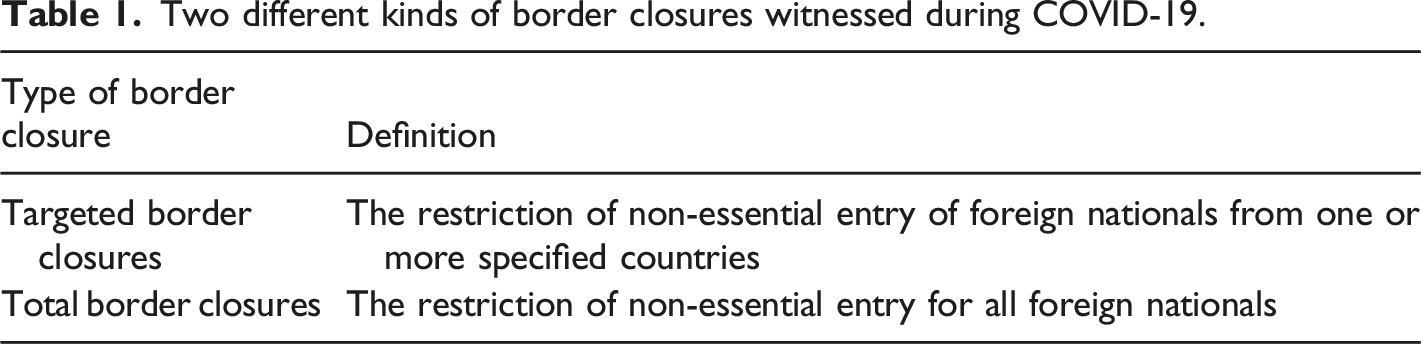
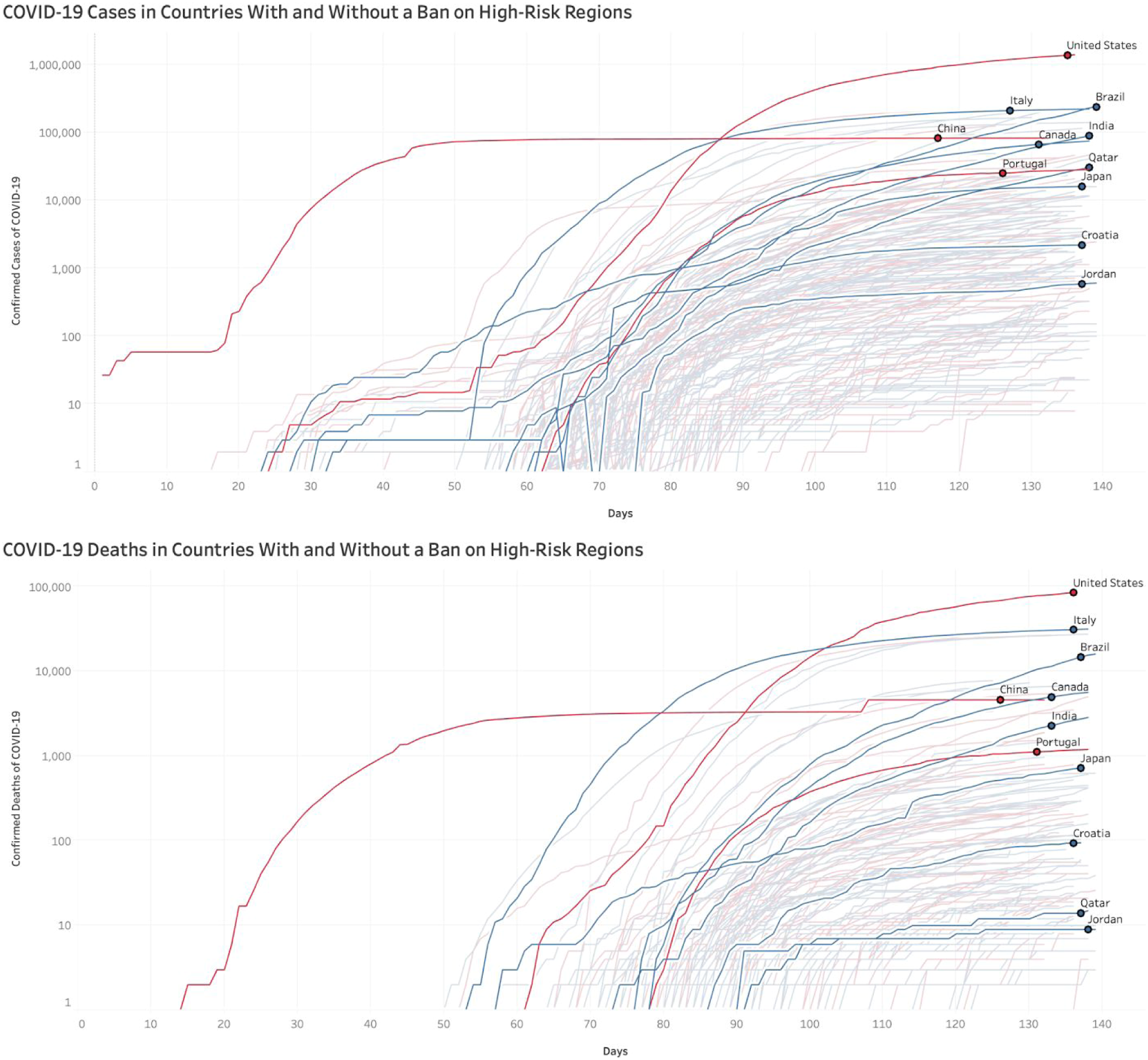
As early as 18 March 2020, 18 countries had mandated quarantines for incoming travellers from high-risk regions like China, 55 countries had imposed bans against travel from high-risk regions, and 37 countries had enacted total border closures. 18 March 2020 was chosen as the map’s date of reference because several countries enacted total border closures on this day, including Canada, Georgia, Oman, Venezuela, and Somalia. Two months later, on 18 May 2020, 14 countries had quarantines for travellers from high-risk regions, 29 countries had bans against travel from these regions, and 113 countries had total border closures. Two different kinds of border closures witnessed during COVID-19. COVID-19 cases and deaths in countries with and without targeted border closures against high-risk regions.
5
Countries with targeted border closures against incoming travellers from high-risk regions (red) have fared no better than countries without targeted border closures (blue).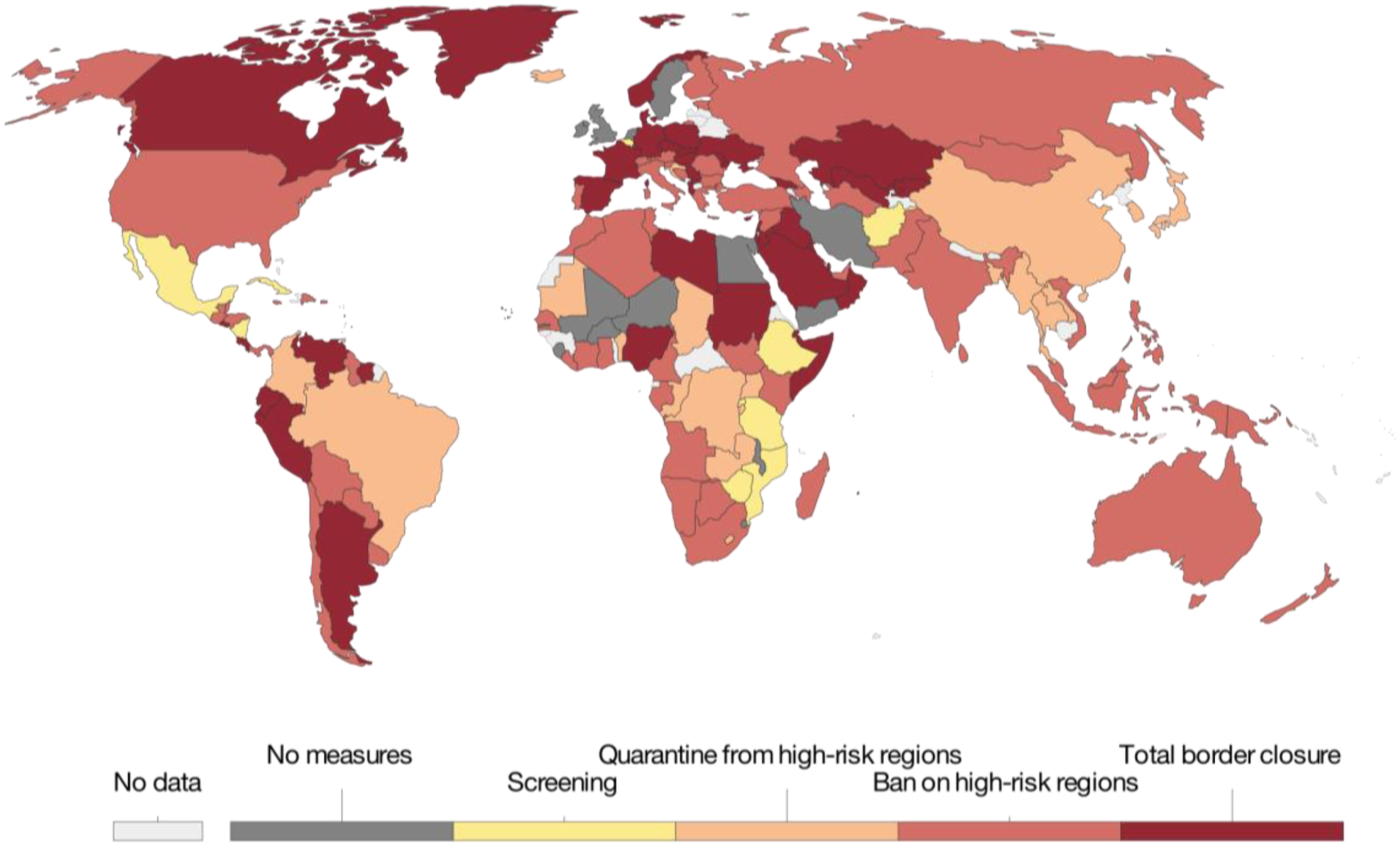
This article critically examines the use of targeted border closures and, to a lesser extent, the unprecedented case of total border closures at the outset of the novel coronavirus (now SARS-CoV-2) outbreak. In the first part of the article, we challenge the narrative that border closures deployed at the onset of the COVID-19 pandemic were justifiable by science and law. We argue that border closures at the onset of the COVID-19 pandemic were adopted for chiefly political reasons and, in some cases, were exploited to advance other political gains. In the second part of the article, we evaluate the epidemiological, legal, and political consequences of border closures and discuss how new developments in our understanding of border closures may affect the future of global health cooperation. Specifically, in the context of a prevailing global tension between integration and fragmentation, we argue that it is not necessary that borders always remain open in the face of an emerging infectious disease outbreak; however, it remains vitally important that global cooperation is sustained. Any attempt to embrace coordinated border closures as a form of global cooperation will need to find strategies that maximize their effectiveness while mitigating their negative effects. However, the feasibility of this path is unclear, especially considering the many political reasons why border closures are so often adopted in the first place. 4
To make this case, we begin by examining the epidemiology and legality of targeted border closures, explaining why they generally do not work and how they can contravene international law. We go on to argue that since the current institutions of global health governance did not anticipate total border closures, the epidemiology and legality of this latter phenomenon rested on less certain ground when they were adopted in March 2020. Then, after asking why nearly every government implemented some form of border closure in early 2020 if neither science nor law provided adequate motivation for these measures, we posit that in the face of a global health emergency of unknown scale and intensity, border closures represent an opportunity for political leaders to garner domestic support by complying with public opinion, delaying or avoiding scrutiny on underfunded public health systems, appearing thorough, diverting blame, and becoming champions of national security, all while simultaneously reinforcing nationalistic narratives and legitimizing the use of borders as a form of foreign policy response. We proceed to argue that both targeted and total border closures have profound legal, epidemiological, and political significance as performances that contradict global realities while undermining international cooperation and global solidarity. Such political theatre means that citizens must not unduly defer to scientists or lawyers on early COVID-19 border closures because these were primarily political—not scientific or legal—decisions. Finally, we conclude with some observations for the future of global health cooperation around border closures during infectious disease outbreaks.
1. Targeted border closures are ineffective
In theory, targeted border closures are intended to prevent all incoming travel by people who might have been exposed to a pathogen in a particular area, who might be carrying it, and who might transmit that pathogen to others in the place of destination. If people from affected areas are not permitted to enter other countries, then it is reasoned that those countries will be safe from the pathogen as there are no human vectors through which the pathogen can travel.
Unfortunately, implementing targeted border closures is not so simple. In general, people will find a way to travel to their destination if they really need or want to do so, either by first travelling to a third country or by travelling through unofficial channels. The former increases global risk by increasing the distance and segments of travel. The latter makes it more difficult to identify individuals who have acquired the pathogen and to trace those with whom they came into contact. There is also usually a gap between the time when governments announce border closures and when they can be implemented, which can provoke an immediate surge in travel and thereby increase the risk of infectious disease transmission alongside the chaos that comes with sudden stampedes of travellers. 6
Furthermore, and despite the scientific uncertainty that is present during any early response to emerging diseases like COVID-19 and its mutated variants of concern, the best available empirical research in March 2020 indicated that targeted border closures were likely to be ineffective in preventing the spread of disease across borders. 7 Temporary flight bans in the United States after the 11 September 2001 terrorist attacks, for example, did not stop or diminish that season’s influenza outbreak. 8 Meanwhile, even though travel restrictions imposed by several countries against Mexico during the 2009 H1N1 influenza outbreak reduced travel by 40% these measures only delayed the virus’s arrival in other countries by less than 3 days. 9 Epidemiologic simulations of H5N1 avian influenza further found that even a 90% reduction in travel through border closures would have merely slow that virus’s spread by a few days to weeks in the implementing country. 10
2. Targeted border closures are illegal
In part due to this demonstrated lack of effectiveness, targeted border closures also tend to be violations of the revised IHR that is legally binding on 196 states parties. 11 The IHR is the product of over 150 years of multilateral efforts to contain the international spread of infectious diseases while preserving economic activities such as international trade and travel. 12 Its precursors, a series of political agreements and conventions between 1851 and 1938, saw European powers agree to standardize international quarantine regulations against the spread of specific diseases such as cholera, plague, and yellow fever, while minimizing the impact on trade among states. 13 Although the raison d’être of these early attempts was protection against public health threats, 14 the minimization of disruptions to trade relations and economies during public health crises remains a key concern for parties to the IHR today. 15 Indeed, as outlined in Article 2, the contemporary IHR aims to “prevent, protect against, control and provide a public health response to the international spread of disease” while avoiding “unnecessary interference with international traffic and trade.” 16
Article 43 of the IHR is central to achieving this balance. It allows states parties to exercise their sovereign right to respond to public health threats and implement health measures that achieve the same or a greater level of health protection than WHO recommendations would. But, importantly, these additional health measures must adhere to a set of conditions that are established in Article 43 (Box 1), intended to protect people and economies from needless harm and to avoid disincentivizing governments from alerting the WHO to new public health risks when first identified within their territory.
17
The article stipulates that additional health measures must (1) be otherwise consistent with the IHR; (2) not be more restrictive of international traffic and not more invasive or intrusive to persons than reasonably available alternatives that would achieve the appropriate level of health protection; (3) accord with the state party’s relevant national laws and its obligations under international law, including its obligations under international human rights law; and (4) be based on scientific principles, available scientific evidence, and available specific guidance or advice from the WHO.
18
Where scientific evidence is insufficient or unavailable, Article 43 notes that additional health measures may also be informed by other available information, including from the WHO and other competent intergovernmental organizations and bodies.
19
These Regulations shall not preclude States Parties from implementing health measures, in accordance with their relevant national law and obligations under international law, in response to specific public health risks or public health emergencies of international concern, which: a. achieve the same or greater level of health protection than WHO recommendations; or b. are otherwise prohibited under Article 25, Article 26, paragraphs 1 and 2 of Article 28, Article 30, paragraph 1(c) of Article 31 and Article 33, provided such measures are otherwise consistent with these Regulations. Such measures shall not be more restrictive of international traffic and not more invasive or intrusive to persons than reasonably available alternatives that would achieve the appropriate level of health protection. In determining whether to implement the health measures referred to in paragraph 1 of this Article or additional health measures under paragraph 2 of Article 23, paragraph 1 of Article 27, paragraph 2 of Article 28 and paragraph 2(c) of Article 31, States Parties shall base their determinations upon: a. scientific principles; b. available scientific evidence of a risk to human health, or where such evidence is insufficient, the available information including from WHO and other relevant intergovernmental organizations and international bodies; and c. any available specific guidance or advice from WHO. A State Party implementing additional health measures referred to in paragraph 1 of this Article which significantly interfere with international traffic shall provide to WHO the public health rationale and relevant scientific information for it. WHO shall share this information with other States Parties and shall share information regarding the health measures implemented. For the purpose of this Article, significant interference generally means refusal of entry or departure of international travellers, baggage, cargo, containers, conveyances, goods, and the like, or their delay, for more than 24 hours. After assessing information provided pursuant to paragraph 3 and 5 of this Article and other relevant information, WHO may request that the State Party concerned reconsider the application of the measures. A State Party implementing additional health measures referred to in paragraphs 1 and 2 of this Article that significantly interfere with international traffic shall inform WHO, within 48 hours of implementation, of such measures and their health rationale unless these are covered by a temporary or standing recommendation.
It must be acknowledged that many of the practical implementation challenges posed by Article 43, as well as other provisions of the IHR more broadly, may be explained by a range of normative deficiencies within the agreement, such as the absence of compliance-inducing and enforcement mechanisms (e.g., targeted sanctions for egregious non-compliance), 20 and the lack of an effective dispute resolution mechanism to resolve divergent interests between states parties in the application of the provision. 21 While possible future IHR reforms are further discussed in Section 7 of this article, the absence of such mechanisms may, in turn, be attributed to the WHO’s general reluctance to exercise its founding normative authority. As the specialized UN agency for health, the WHO has expansive international law-making powers, including the ability to “propose conventions, agreements and regulations.” 22 It has used these powers sparingly, 23 however, opting to wield non-binding normative instruments, such as action plans, codes, and political declarations, to build consensus and coordinate action incrementally on global health issues among its 194 member states while respecting state sovereignty. 24
Article 43’s weak normativity may therefore be symptomatic of the WHO’s perennial “crisis of identity,” characterized by an uncomfortable tension between its medical, scientific, and technical mandate on one hand, and its political and law-making authority on the other. 25 Notwithstanding these deficiencies, however, the fact remains that Article 43 is part and parcel of a legally binding agreement between nations, and as such, its terms must be adhered to subject to the rules of treaty interpretation under the Vienna Convention on the Law of Treaties (the Vienna Convention). 26
In this regard, the provision that countries may enact additional measures pursuant to Article 43 does not immediately sanction the use of targeted border closures witnessed during COVID-19. As the Oxford Government Responses Tracker demonstrates, countries began implementing targeted border closures as early as 28 January 2020, days before the WHO director-general declared a PHEIC pursuant to the IHR. 27 In the ensuing weeks and until mid-March 2020, border closures primarily targeting travellers from affected countries were enacted around the world. As described above, there was no shortage of research on the use of targeted travel restrictions during previous infectious disease epidemics—and the scientific consensus in early 2020 pointed against their long-term effectiveness as a public health response. Scientific evidence generated from the early days of this pandemic strengthened these observations and indicated that border closures at the outset of the COVID-19 pandemic only delayed, and did not prevent, the arrival of the virus. 28 In many cases, early government responses to the pandemic were out of step with the local epidemiological progression of the pandemic, suggesting that government policies were primarily informed by the plight of neighbouring countries or news of events abroad. 29
Furthermore, targeted border closures often lead to violations of international human rights obligations. For some, border closures deny the individual freedom to leave any country or to enter one’s own country of nationality; for others, border closures deny the right to seek asylum; and for others still, border closures deny the right to be free from unlawful interference with family—all of which are enshrined in international law. 30 Border closures may also have deleterious downstream effects on other enshrined rights and freedoms where the supply chain of medical equipment and personnel is disrupted or even blocked, such as the general obligation to assist other countries in implementing social and economic rights under the International Covenant of Social, Economic, and Cultural Rights and the specific duty to protect the right to health of patients and healthcare workers. 31 The appalling scale of disruptions to the conveyance of necessary medical supply and personnel during the 2014–2016 Ebola outbreak in West Africa, for example, led the United Nations (UN) Security Council to call on “Member States ... to lift general travel and border restrictions ... that contribute to the further isolation of affected countries and undermine efforts to respond to the Ebola outbreak.” 32 Similarly, targeted border closures in the early stages of COVID-19 disrupted, among other things, the equitable distribution of personal protective equipment and the availability of essential workers. 33
It is generally understood that international human rights obligations may be limited or derogated from in times of public health emergency, provided such actions are stringently legitimate, necessary, enacted for a short period of time, and proportionate to the public health risk at hand. By intentional analogy, Article 43 of the IHR also explicitly limits the ability of states parties to implement additional health measures to cases where they are “no more restrictive of international traffic and not more invasive or intrusive to persons than reasonably available alternatives that would achieve the appropriate level of health protection.” 34 Arguably, in place of targeted border closures, there were several reasonably available, and more effective, alternative measures for governments to implement during COVID-19, including contact tracing, community surveillance, widespread testing, quarantine, and public communication. 35 Several empirical and policy monitoring studies have considered the limited effectiveness of targeted travel restrictions in the early days of the pandemic. For instance, in their seminal piece describing the chronological trajectory of COVID-19, experts from the Secretariat of the Independent Panel for Pandemic Preparedness (IPPPR) note that limited early screening criteria which focused primarily on direct travel history from Wuhan hampered the accuracy of estimates on the true extent of the virus’s national and international spread. 36
The resort to targeted border closures was likely not the least restrictive measure at the disposal of states parties under Article 43 of the IHR. Soon, however, the vast majority of states would resort to an unprecedented variation of border closures to control COVID-19 at their frontiers. We consider the epidemiology and legality of this variation of border closures in the sections that follow.
3. Total border closures were unprecedented for scientists, lawyers, and politicians alike
Whereas targeted border closures limit the entry of travellers from countries perceived as high-risk, total border closures ban inbound travellers from all countries. In theory, total border closures work via the same logic as targeted border closures, but with the added benefit of stopping all travel of people and microbes, thereby preventing circumvention through third countries and unofficial channels.
Total border closures make intuitive sense—no travel means no human vectors through which the pathogen can travel. But, like targeted border closures, implementing them is not so simple. For instance, no border closure is completely total, in the sense that even the most stringently implemented ones generally still permit the return of national citizens and make exemptions for essential work and necessary travel on the basis of compassionate grounds.
Additionally, at the time that decisions were made to fully close borders, no evidence of their effectiveness really existed. Early evidence that did emerge on their potential effectiveness derived largely from mathematical modelling studies, not empirically driven ones. 37 The lack of empirical evidence was partly due to the unprecedented nature of the global public health threat. Prior to 2020, there were no opportunities to generate evidence because total border closures had previously never been implemented on such a widespread scale. Decision-makers, therefore, could not have possibly based their decision to totally close borders on rigorous empirical evidence, as required under the IHR.
4. Total border closures are possibly legal depending on the outbreak
While there is a consensus among global health legal scholars that targeted border closures violate the IHR, the legal status of the total border closures enacted by over 100 countries is uncertain. 38
At first glance, total border closures are even more restrictive than targeted border closures, such that they should be similarly found to contravene obligations under Article 43 of the IHR. Yet where the text of a treaty is silent on certain matters, the Vienna Convention takes precedence. It mandates states parties to interpret the legal instrument in “good faith” and in light of its “object and purpose.” 39 The purpose of Article 43’s limitations on travel restrictions is to avoid unnecessarily amplifying the economic and social consequences of public health risks in affected countries, and to avoid disincentivizing countries from reporting risks when they appear. 40 Indeed, countries are naturally less likely to report a new infectious disease outbreak in their jurisdiction if they are worried about facing border closures that cripple their economies and expose their outbound travellers to discrimination and human rights abuses. But total border closures do not primarily or only punish specific affected countries; rather, most costs from total border closures are borne by the residents and economies of the countries that enact them. And in that respect, total border closures present an unprecedented situation which the drafters and signatories of the IHR neither anticipated, nor prepared for. Indeed, the 196 states parties to the instrument may not have intended to prevent total border closures if a time came when such closures were desired.
Even if this purposive and interpretive argument does not pass muster, countries enacting total border closures could still have pointed to the absence of opposing scientific evidence on the effectiveness of total border closures at the outset of the pandemic, noting that previous studies have evaluated targeted border closures and not border closures that shut out most of the world. The argument is strengthened when considering the WHO’s lack of reprimand (but notably also lack of support) for these measures once border closures reached critical mass across the globe. But even in the absence of available scientific evidence and advice or guidance from the WHO, states parties are still required to implement measures in accordance with scientific principles—defined in the IHR as “the accepted fundamental laws and facts of nature known through the methods of science [emphasis added].” 41 In the case of total border closures, a government could potentially argue that the constrained travel environment during the COVID-19 outbreak meant that the likelihood of incoming travel via third countries and unofficial channels would be much reduced.
Besides, while it makes good sense for an instrument like the IHR to prevent countries from punishing others with unjustifiable targeted border closures, the international legal principle of sovereignty mitigates in favour of the ability of countries to close their borders. 42 Article 43’s limitation on additional health measures in the IHR must then be read more narrowly to only prevent countries from enacting border closures when they have discriminatory effects on other countries. This means that non-discriminatory total border closures could be legal under international law even when the less restrictive but discriminatory targeted border closures are clearly illegal.
All of that being said, if total border closures are enacted for public health reasons, then, according to Article 43.1 of the IHR, countries must still ensure that “such measures shall not be more restrictive of international traffic and not more invasive or intrusive to persons than reasonably available alternatives that would achieve the appropriate level of health protection.” 43 This provision means that countries are obliged to deploy less restrictive border measures if they are available and if they would attain comparable health protection in a non-discriminatory way. It also means that when travel bans are employed, they must be accompanied by essential domestic and community-based public health strategies to limit transmission. Countries that do not deploy less restrictive measures, such as mandatory quarantine, when they are able to effectively do so would, therefore, still be violating international law.
5. Border closures are enacted for political reasons
If targeted border closures were unsupported by the available scientific evidence at the time and known to often contravene the IHR, and if total border closures were, at the time that they were implemented, only hypothetically effective and only possibly legal, then why did over 140 countries implement these measures and close their borders in some way or another?
Political science offers several possible explanations. Drawing on observations from this and previous pandemic outbreaks, we present six interrelated explanations from political science as well as some conceptual tools to understand how they relate to each other. Taken together, these factors indicate that political decisions to implement both targeted and total border closures are fuelled by the need to act under uncertainty, threat, and time-constraints 44 in a way that balances both international and domestic pressures. 45 Under these conditions, border closures are attractive policy options because they are potentially supported by public opinion, are potentially cheaper than the public health alternative, and potentially prolong or prevent the exposure of internal failures to invest in public health infrastructure. They also provide political cover by way of a decisive and quick action that demonstrates that governments and leaders are exhausting all possibilities in the name of national security, while also externalizing the threat and redirecting blame outside of national jurisdictions. 46 Overall, these bordering practices fall into a broader historical trend in which enacting borders has become a legitimate way to respond to threats, to the continued detriment of international commitments to cooperation and openness. 47
When explaining why governments closed borders during the early days of the COVID-19 pandemic, it is important to note that these decisions were made in conditions that were far from normal. COVID-19 represents a crisis, which means leaders have had to, make decisions under strained conditions of threat, uncertainty, and urgency. 48 In making these decisions, leaders had to weigh domestic preferences and agendas, including the relative importance of public health alongside other social and economic considerations, with the country’s international commitments.
Robert Putnam’s two-level model is helpful to consider how leaders balance costs, benefits, and pressures associated with foreign policy against those associated with domestic politics. Foreign policy exists at the intersection of international and domestic political realms and can be exploited by leaders who use it to align, project, or reflect the values and interests of the domestic population. 49 Indeed, politicians often use foreign policy responses to crises such as COVID-19 to advance domestic political gains. Through foreign policy, domestic leaders often navigate the international realm in a way that maximizes the interests of domestic actors, balancing them against, and sometimes even prioritizing them over, international pressures.
For each of the following six political explanations, we unpack the underlying motivations that may compel leaders to adopt border closures. The reasons we provide are neither mutually exclusive nor exhaustive. Instead, by analyzing the various factors below, situating those decisions within the context of emergency politics, and using Putnam’s two-level model, this section demonstrates how political factors interact with each other and often displace concerns for science and international law in decision-making contexts.
A. Border closures are supported by domestic publics
The first explanation is that governments impose border restrictions and forgo their international commitments because they anticipate that border closures will align with what their domestic publics want. In other words, the anticipated domestic benefits gained by appeasing citizen demands to close borders outweigh the anticipated international costs of reneging on commitments to openness.
Democratic countries may be more inclined than authoritarian ones to consider public opinion when making decisions, but no form of government is completely insulated from it. When considering public opinion in normal times, governments, particularly in democratic countries, will either act in a certain way because they already know that they have public support, or they will act in a certain way because they anticipate public support. 50 The uncertainty present during crises means that decision-makers do not definitively know the severity of the threat nor what their publics want, and time constraints are likely to prevent them from gathering robust assessments of either prior to deciding. Therefore, in crises like COVID-19, it is more likely that if public opinion was considered as a factor for border closures, then it was considered in anticipation. And that anticipation may have proven correct: when surveys emerged, there was widespread support for keeping borders closed in many countries, including Canada. 51 For example, one Canadian survey conducted in December 2021 found that 82% of respondents were in favour of closing the border to travellers coming from countries where the Omicron variant was present. 52 If domestic publics appear to support these measures, public opinion cannot be ruled out as a driving force behind the continued use of border closures around the world, even if science and law point against their use.
B. Border closures are easier and less expensive to enact than the public health alternative
A second explanation for why border closures appear attractive to decision-makers is that they are potentially less expensive than the alternative of mounting a robust domestic public health response. 53 In this explanation, the costs associated with reneging on international commitments to openness are dwarfed by the costs of mounting a response that is veritably driven by epidemiology.
Border closures represent a simple, externally focused means of responding to health threats. They present the opportunity to prevent or prolong the need to mount a public health response, which is internally focused and potentially more expensive and disruptive to daily life for citizens. On its own, this explanation makes more sense for targeted border closures, since the targeted country, not the enacting country, bears the cost of this measure. In isolation, this explanation makes less sense for total border closures since, in these instances, the enacting country bears most of the costs.
But this explanation could make sense for total border closures when put into a longer-term perspective. Border closures are a reactionary response, whereas implementing internal public health measures requires proactive investment in critical public health infrastructure and sustainable supply chains. Border closures, targeted and total, may present as the only attractive policy option when the alternative is to mount a public health response that will inevitably reveal a lack of internal investment in public health preparedness. Even if total closures are more expensive in the short run, they may still make sense as a reactionary policy where there has been a failure to invest in public health infrastructure over the long-term. This would mean that the domestic costs associated with revealing an internal failure to invest in public health and, subsequently, having to compensate for that failure outweigh the costs of reneging on international commitments.
C. Border closures give the appearance of thoroughness
A third explanation is that politicians will enact border closures to cover all their bases in an attempt to prevent backlash. 54 To avoid blame during a crisis response, politicians need to appear as though they have exhausted every possible option. Put differently, the costs associated with losing face internationally for closing borders and potential economic losses due to border closures may be outweighed by potential costs associated with losing face domestically for failing to close borders.
This explanation suggests that even if governments know the science and international law of border closures, they will still feel compelled to enact them because of intense pressure from powerful domestic political actors who might otherwise blame them for not taking every possible action. Such criticism could come from opposition parties, sub-national governments, civil society organizations, academics, and/or journalists, depending on the political institutions of a society and how they give voice to and structure criticism. For example, political pressure to enact border closures may be particularly intense in those countries with federal structures, wherein sub-national governments may look for opportunities to assign blame to the federal government as it controls national borders. Another Canadian example helps to illustrate this point: in May 2021, Ontario premier Doug Ford criticized the federal government’s handling of border control measures by claiming that the province’s third wave was largely driven by porous national borders. 55 Directing criticism toward the federal government, Ford stated that “not enough is being done to keep these deadly variants out of Canada” and that “as long as ... massive loopholes exist we’re not safe.” 56 The same logic is true for countries with multi-party systems and freedom of the press. The ruling party may feel pressure to implement border closures to deny their political adversaries and the media the opportunity to criticize them, particularly during an election year. Even more pressure would be faced by national leaders with all three political institutions—a federal structure, multi-party system, and press freedoms—like Canada, which was indeed one of the earlier countries to enact a total border closure on 18 March 2020 (see Figure 1). 57
D. Border closures divert blame
A fourth reason why countries implement border closures is that border closures externalize the problem and implicitly redirect blame away from the country. Border closures have this effect by projecting the existence of a safe national entity in relation to an unsafe external threat, implying that the problem exists as an external danger threatening the safety of the nation.
While all nation-building performances seek to produce a common notion of national identity for political purposes, the act of enforcing borders during COVID-19 forms identity in a particular way. By creating a boundary between the safe inside and the unsafe outside, border closures create a national identity contingent upon protection from outside threats: the nation is something that must be protected. 58 Targeted and total border closures both do this, but in different ways. Targeted border closures specifically identify other nations as entities from which the domestic population must be protected. Total border closures, while perhaps less discriminatory, still work as a process of othering, but instead of constructing nationhood in relation to another nationality, they construct it in relation to all other nationalities by positing everything inside the nation’s boundaries as safe, and everything outside of them as unsafe.
In this way, exclusionary bordering practices have the additional political effect of re-assigning blame for the health emergency to people or governments outside of one’s country. They discourage citizens from reflecting on the frailty of their own country’s public health infrastructure or holding their elected government to account for past policy choices, such as neglecting to invest not only in domestic public health capacities, 59 but also the capacities of under-resourced countries. 60 Such symbolic acts are ever more instrumental—and politically valuable—in circumstances where a government feels it has insufficient knowledge, tools, or options to address the actual problem.
E. Border closures allow leaders to become champions of national security
A fifth explanation is that the chance to use foreign policy to convey good intentions and take credit for swift action, especially when public attention is high, is too good of an opportunity for politicians to give up. One way that political leaders have exploited foreign policy during COVID-19 to advance their political interests is by virtue signalling. Many politicians appear to be using symbolic actions in the international realm to emphasize positive aspects of their character, including by playing into and reinforcing nationalistic sentiments. 61 In doing so, they emphasize how their leadership in the international space embodies values that are desirable for domestic audiences. In relation to the idea of generating a particular sense of national identity, border closures enacted in the name of public safety signal that the leader is taking the safety of the nation as their primary concern, by securing the nation from foreign threats. Furthermore, by emphasizing that border closures are enacted “out of an abundance of caution” with “the population’s health and safety as their number one priority,” leaders project themselves as gallant protectors and champions of public safety, even when their actions are not supported by scientific evidence or law.
One overt example serves to directly illustrate how today’s political leaders can divert blame while also presenting themselves as defenders of national security through the use of border closures: in a 2 April 2020 press conference discussing border closures, former US president Donald Trump said, “If we didn’t cut off China, we would be in some big trouble. ... We’re the ones that kept China out of here,” directly equating danger from COVID-19 with China as a national entity. 62 Not only does this convey racist undertones, but it in many ways also serves as a political tool to reinforce ideational and material boundaries between the United States and China, while lending perceived credence to the former president’s claim that he was acting to protect and secure the safety of the country. While former president Trump’s remarks directly referred to China as a danger to the United States, all border closures enacted in the name of COVID-19 implicitly do the same thing by presenting the act of closing the border as a form of protection against a foreign danger.
The five political explanations thus far have not sought to explain the underlying causes for the mechanisms of support for border closures. That is, they explain the support for border closures, but they do not explain what garners this support. Some questions that would direct us to these deeper analyses include why publics around the world demand border closures in the first place; why, regardless of direct political support, nationalistic actions like border closures are received favourably; or why it is so virtuous for political leaders to portray themselves as the champions of public safety through bordering practices. There are many determinants of domestic attention to specific international issues like border closures. In fact, there is much room for debating why and when the public cares about foreign policy and the mechanisms by which public opinion affects foreign policy. However, disentangling the complex mechanisms that determine these forces is beyond the ambit of this article. For the sake of this analysis, we can situate these forces in what can be identified as a larger trend where societies around the world have become increasingly focused on borders—what Michael Kenwick and Beth Simmons call “border orientation.” In their analysis, they show how, domestic publics have become more amenable to bordering practices, and many politicians find it easy to oblige (though it is equally possible that political decisions are driving public support). In their words, border orientation refers to “the extent to which the State is committed to filtering the movement of goods and people into and out of its territory.” 63
F. Border closures fit in with long term practices of border orientation
A sixth explanation is that states enact border closures because they fit with their ongoing border orientation policies. Border orientation is a political trend where border controls are increasingly viewed as legitimate responses to threats. With border orientation on the rise, more and more governments are enacting border controls to protect national security from “external threats”—prominently seen with regards to migration and anti-terrorism policies, but equally important to note during pandemics. Kenwick and Simmons found that, on average, border orientation has increased over the last two decades, and countries with higher border orientation scores were more likely to implement border closures during COVID-19. 64
Border closures and bordering practices during COVID-19, therefore, can be seen as the most recent iteration of a particular kind of foreign policy that aims to create material and ideational boundaries as a means of legitimizing political power. Such bordering practices unify a group under an idea (the nation) and justify the exercise of extraordinary power in the name of protecting it. Such acts consolidate power to control the internal domestic space in the face of the threatening external world, 65 satisfying the need to act decisively and quickly while preserving images of foreign dangers and a secure domestic space provided by a competent state. In this sense, whether border closures are backed by science or law is peripheral and mostly irrelevant to the pursuit of other political interests.
6. Border closures have legal, epidemiologic, and political consequences
Regardless of whether a country adopts a targeted or total border closure, border closures divide, contradict, and “other”—with downstream consequences for the global response to this and future pandemics. Specifically, these acts undermine the legitimacy and effectiveness of international law, produce counterproductive incentive structures that hamper epidemiological responses, and contradict modern-day realities of interconnectedness, further entrenching the vulnerability of all countries to infectious disease. 66 In turn, by forming a sense of national identity as something that needs to be secured in relation to other national identities, border closures produce ways of thinking that reinforce nationalistic tendencies 67 and erode global solidarity. 68 Global solidarity, cooperation around epidemiologically driven global public health measures, and an effective rules-based international system are required for achieving an effective and coordinated response to COVID-19 and future global health threats. 69 These nationalistic ideas also prime the public and test their tolerance for securitizing acts, including the use of border closures as potential responses to other ongoing and future challenges, such as climate and war refugees and migrants. 70
A. Legal consequences
At a fundamental level, border closures express a level of ambivalence for the purpose of the IHR, and thereby undermine the rules-based world order in which we live. International treaties are integral to world peace and security, but their effectiveness hinges upon the good faith cooperation of all parties. In the words of former president of the UN General Assembly, Vuk Jeremić, “to strengthen trust between nations, ... respect for accepted norms and standards cannot be ambiguous or selective.” 71 Where rules are deemed insufficient, inadequate, or no longer fit-for-purpose, the appropriate international response is to negotiate new or amended rules to reflect evolving international legal (and, in the case of the IHR, scientific) consensus. Mass non-compliance with agreed-upon rules risks collapsing an international legal regime that was negotiated in the prescient wake of crisis and reckoning.
B. Epidemiological consequences
More pragmatically, border closures produce counterproductive incentive structures that inhibit scientifically informed responses, while contradicting the ethos of global public health. The IHR sought to fill crucial voids in the coordination of the international response to disease outbreaks. Striking a delicate balance between public health reporting and cooperation, Article 43, in particular, is rooted in the understanding that disease outbreaks may arise anywhere in the world. 72 When they do, their emergence elicits often exaggerated and fear-based responses from the broader community of nations. In turn, these fear-based responses inadvertently condition countries to evince reluctance in sounding the global alarm when it is their soil that has harboured the most recent outbreak. We need only look to the selective border control measures taken in response to newer, more transmissible, and lethal variants of SARS-CoV-2, such as the Alpha variant that emerged in the UK, to understand how quickly the eschewer may become the eschewed. In this scenario, the UK actively contributed to the global public good by mounting a testing strategy based on good epidemiology. They tested cases well enough to identify and document the spread of a mutated virus, and promptly notified the global community of its potential dangers. As a direct result of the UK’s efforts, the global community was better off because it could prepare for a more contagious and deadly virus. But by targeting the UK with restrictive border closures, the global community actively disincentivized future cooperation by reprimanding rapid reporting. Ironically, China continues to be chastised for not reporting their initial outbreak fast enough, but so too are countries chastised for reporting new outbreaks in real-time.
C. Political consequences
Border closures divide the world in a manner that belies the interdependence and vulnerabilities shared by all countries in today’s globalized world—vulnerabilities that have been palpably exposed during this pandemic. By appealing to notions of distinct and sovereign powers, border closures represent political performances that reify a world of individual, self-contained states. While states contribute to this process of globalization, and while this process indeed occurs in a system of self-contained states, the continued cross-national flow of people, products, ideas, and microbes—even under these unprecedented restrictions—indicates that the world is interconnected in a way that transcends physical borders, also evidenced by lengthy exemption lists noted on travel restriction orders. 73 And while there are some instances of deepening global connectedness in the response to COVID-19, such as in research and data sharing, 74 the act of closing borders creates boundaries in material reality that run counter to these processes.
Relatedly, border closures undermine global solidarity. Border closures are identity-creating political performances that operate to construct the nation as a natural entity. Political identities are important because they are foundational for how individuals understand the political world. The act of enforcing stringent borders and dividing the world into countries is identity constructing insofar as it delineates the domestic inside from the foreign outside, projecting the existence of a national political community. 75 Nations, as imagined communities, are fragile and tenuous ideational constructs that require constant productive and reproductive acts to sustain them, 76 and responding to global crises by invoking borders precisely achieves this. For example, all border closures enacted during COVID-19 identified locations and identities as “foreign” and “alien” in relation to their home country, and barred travel from these places while exempting their own citizens and residents. 77 These kinds of political acts both depend upon and create an understanding of national belonging tied to citizenship and space as “natural” in relation to unfamiliar “aliens.” 78 Such divisions simultaneously produce and naturalize notions of nationalism in that they unify a people with a common identity—in this case, individuals benefitting from certain rights in a territorially defined nation—while undermining notions of global solidarity. In these ways, the act of closing borders works not only to create material boundaries, but also ideational ones that are politically significant insofar as they divide the world, galvanize territorial identities, contradict physical realities, and serve as a process of othering. 79
These securitizing narratives create a national identity dependent upon a notion of a community threatened by foreign outsiders, and essentialize the existence of nations as political communities threatened by openness. 80 In this way, border closures for COVID-19 are also a way for governments to prime their publics for future border closures against other “threats” however defined. Border closures gauge public tolerance for these kinds of nationalistic responses to other future global events and pave the way for public acquiescence to other problematic border practices.
7. Conclusion
At the time they were implemented in response to COVID-19, targeted border closures were known to be illegal and ineffective for preventing the spread of pathogens. With regards to total border closures, neither evidence on their effectiveness nor interpretations of their legality existed when they were implemented to an unprecedented degree in early-to-mid 2020. One possible justification for the enactment of border closures is that although they do not prevent the arrival of pathogens, they can postpone it, which could in turn buy valuable time for a country to shore up its public health response capacity. But too many border closures were inconsistently applied (undermining their effectiveness and this potential justification), and many prominent examples squandered the temporary opportunity to increase domestic public health capacities offered by border closures. The absence of an empirically supported legal and public health rationale in March 2020 leads us to conclude that under conditions of urgency, uncertainty, and threat, border closures were enacted for political reasons with profound legal, epidemiological, and social consequences.
Since then, the unprecedented nature of border closures has been matched by the unprecedented and extraordinary global mobilization of energy and money to advance our understanding of the pandemic. These efforts have produced several rapid changes to the science of COVID-19, including to our understanding of the potential effectiveness of total border closures.
81
In turn, changes to the science of border closures have potentially transformed their international legal status. Yet while the science and law relating to border closures have changed since March 2020, the political motivations underlying their enactment have not. In this context, we conclude with a few observations and recommendations for policy, starting with one recommendation for domestic policy before discussing another three for global health policy. 1) Accountability, transparency, and deliberation on border closures must still occur
The challenge we have seen in the ongoing pandemic is that governments have justified their border closures by citing expert advice apparently received from epidemiologists and legal counsel.
82
Essentially, political leaders have sought public support for their exclusionary bordering practices by asking citizens to defer to government scientists and lawyers. But, of course, these decisions are not based only on science or law. They are political. And as a result, citizens must not acquiesce. Deferring to government leaders and other authorities on border closures, even in a pandemic emergency, undermines the systems of political accountability on which democracies depend. Citizens owe it to themselves to be critical of governments when they take action with the potential for significant collateral damage. Although time constraints may have prevented the essential process of democratic deliberation before the adoption of border closures, democratic debates over border closures can and must still occur after the fact. 2) Global cooperation through sensible governance, not necessarily opened borders, is crucial
Importantly, when considering how to create effective global strategies for responding to pandemics, we are not arguing that borders must be kept open no matter what, but rather, that it is a fundamental matter of global governance that countries do not break the rules designed to govern the world’s responses to global challenges. The widescale rule-breaking signals that something is wrong with the strategies we set in place to govern pandemics. To be sure, there are epidemiological reasons for not resorting to border closures, including the counterproductive incentives that such responses create. But the fact that so many countries reneged on their commitment to follow the rules set out in the IHR suggests that countries are not confident in the rules, that the rules are not fit-for-purpose, or both. New evidence that border closures may prevent the virus and ongoing public support for this response, despite its many consequences, may mean that the best way forward is to find a way to embrace border closures as a norm of cooperation, which would require finding ways to exploit their benefits while mitigating their potentially negative side effects. It is not sensible for countries to commit to openness but then close their borders. And in response to the trend that we witnessed during COVID-19, there are two possible ways that global policy can react to re-establish sensible governance: either find new ways to change country-level behaviour to meet the established norm of openness, or change the norm in order to meet the ongoing behaviour. The latter would amount to a qualitative shift in our understanding of what it means to cooperate in the face of pandemic emergencies, and there are many additional implications to consider with this approach, including its practicality, feasibility, and desirability. 3) Strategies exist to mitigate the harms of border closures
If border closures are here to stay, which they very well might be, several strategies could be considered to mitigate their harm.
83
Under Article 43 of the IHR, states retain the sovereign right to close their borders, but certain norms and established procedures (in addition to the rules and principles of the IHR) may influence their decision and enable better, more just, and accurate use of border closures. For example, it may be useful to standardize a protocol that coordinates border closures and openings, so that the decision to close borders is not only guided by the whims of domestic policymakers acting unilaterally or individually. Additionally, in concert with the IHR, the WHO could consider formalizing a global exemption list and quarantining practices to mitigate interferences with human rights. Yet, realizing and enforcing these initiatives would depend on the availability of more robust data, raising another challenge for pursuing this route. 4) A combination of sticks and carrots is needed to ensure global health cooperation
Irrespective of the normative approach(es) chosen—whether they may be cooperation through openness or coordinated closures—the widescale sidestepping of IHR obligations during COVID-19 revealed a longstanding weakness in global health governance surrounding the question of how to mobilize and sustain country-level compliance with international law in the face of infectious disease threats. 84 As we consider alternative normative approaches to balancing international travel and a robust and coordinated global response to infectious disease threats, we must also examine the crucial need to craft mechanisms that foster collaboration and shared objectives in the governance of global health security beyond those that depend on effective enforcement and dispute resolution mechanisms as discussed in Section 2. 85
Indeed, a combination of sticks, carrots, and mechanisms for the continuous evaluation of the rules for cooperation is essential for sustaining global governance on enduring challenges like pandemics. These can work to mitigate the individual cost of cooperation, more directly link individual benefit to the collective benefit, or both while enabling the creation of cooperation-supporting norms of fairness. 86 To this end, beyond reforming the IHR to integrate more effective mechanisms of enforcement and dispute resolution, 87 IHR states parties must consider how interpretations of Article 43 should evolve in light of recommendations by the IPPPR to integrate a more precautionary approach to unknown public health risks as well as adopt a new international legal instrument on pandemic preparedness and response. 88 There is also growing recognition among scholars of global health law that a changing landscape of public health knowledge and evidence beckons further adaption of international law as well. 89 Primordial in this regard are the strengthening of data infrastructure at national, regional, and global levels, as well as establishing built-in mechanisms of state peer review on IHR performance, such as the Universal Health and Preparedness Review (UHPR) first proposed by the WHO secretariat in late 2020. 90
Despite these extensive calls for normative reform, it must also be noted that other independent mechanisms of expert review have advised against reopening the IHR for negotiations, finding that much of what is written in the IHR is “well-considered, appropriate and meaningful in any public health emergency.” 91 International treatymaking is a delicate art requiring near-serendipitous geopolitical and economic conditions, and a union of wills among different heads of state. In the absence of such a meeting of diplomatic minds, any foray into IHR reform may pose more risk than opportunity for global health security. 92
Areas for future research
A critical reflection on the reasons for, and effects of, implementing border closures invites questions regarding the source and drivers of public appetite for border closures as legitimate responses to threat. These questions are especially salient in the context of the broader trend toward border orientation.
Finally, any future research on, or plans for, responding to global health challenges, not just border closures, must seek to unify perspectives to discern fair, feasible, effective, and sustainable solutions. There is an urgent need to not limit our focus or isolate our attention to only the legality of actions, virus transmission patterns, or how actions fit within broader social contexts. Instead, legal, health, and political investigations must address the ways that these domains overlap and interact with each other in potentially destructive and constructive ways.
Footnotes
Acknowledgements
We thank Patrick Fafard for sharing his insights on an earlier version of this manuscript and Safaa Yaseen for her research assistance.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SJH serves as vice-president for Data & Surveillance at the Public Health Agency of Canada (PHAC). The academic views and opinions expressed in this article are those of the authors and do not necessarily reflect those of PHAC, CIHR, or the Government of Canada.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Government of Canada, Canadian Institutes of Health Research (CIHR).