
Abstract
In this article, we discuss how medical virtual instruments are used for ambient assisted living technologies. Ambient assisted living technologies enable seniors to age well in the comfort of their homes. Case studies are used to describe some ways that medical virtual instruments are being used to support ambient assisted living in the key disease domains of cardiovascular, neurologic, hormonal and musculoskeletal health. The article also discusses the open research issues and future perspectives relating to the use of medical virtual instruments in these domains.
I. Introduction
Virtual Instruments refer to instruments that integrate much of the functionality of traditional physical “hard” instruments into a hardware/software co-designed platform that takes advantage of the high performance of hardware and the high flexibility of software. This approach leads to advantages such as portability, flexibility, low cost–functionality ratio and increased modularity.
Medical virtual instruments (MVIs) refer to virtual instruments that are used in the medical domain. In this article, we discuss the use of such instruments within the context of ambient assisted living (AAL) technologies for enhancing the health and life of seniors. MVIs can be developed for virtually every disease domain as long as the appropriate modules are used. However, there are some key disease domains that are most relevant to the AAL technologies.
The following disease domains will be discussed:
Cardiovascular;
Neurologic;
Hormonal;
Musculoskeletal.
In subsequent sections, we will discuss these domains and some key algorithms that are used to classify the disease conditions. We will also highlight existing case studies that take advantage of MVIs in their approach.
II. Cardiovascular Domain
This domain covers the monitoring of biosignals that give an insight into the state of the patient’s heart. The biosignals that are used for disease screening in this domain include the electrocardiography (ECG) and oxygen saturation level signals. ECG signals refer to the electrical signals of the brain measured with a non-invasive ECG sensor. Arterial oxyhemoglobin saturation level, otherwise known as SpO2 level, is a measurement of the oxygen saturation of hemoglobin in arterial blood. 1 It utilizes optical sensors: a red and an infrared sensor on one side of the device and a photo detector on the other side. It is based on the principle that the amount of light absorbed by blood is dependent on the level of oxygen saturation of the blood. A photoplethysmograph can be generated from this process, and its period can be used to estimate the heart rate of a patient.
ECG signals give an indication of a wide range of cardiovascular diseases including the following: arrhythmia (irregular or abnormal rhythm of the heart), sleep apnea (cessation of breathing during sleep for certain periods) and the history or propensity for heart attack. It also shows the efficiency of implanted heart devices like the pacemaker. On the other hand, the pulse oximeter can also be used to diagnose heart diseases, but its analysis is not as extensive or as reliable as that of an ECG sensor.2–4
The key algorithms for processing ECG signals include the Hamilton–Tompkins’ algorithm 5 and the Genetic Algorithm. 6 The Hamilton–Tompkins’ algorithm is a refined version of the Pan–Tompkins algorithm and was proposed in the late 1980s but has remained relevant today because its level of simplicity makes it useful for real-time ECG processing. It is a first-derivative method that detects the R-peaks of the ECG signals using thresholding techniques following a series of filter stages that isolates the QRS complex of the ECG signal.
The Billauer peak detection algorithm is a common approach for analyzing SpO2 signals.7,8 Weighted moving averages and frequency transforms like Discrete Cosine Transform and Fast Fourier Transform are also techniques used in processing SpO2 signals.
A summary of some key MVI features for the cardiovascular domain is given in Figure 1 .
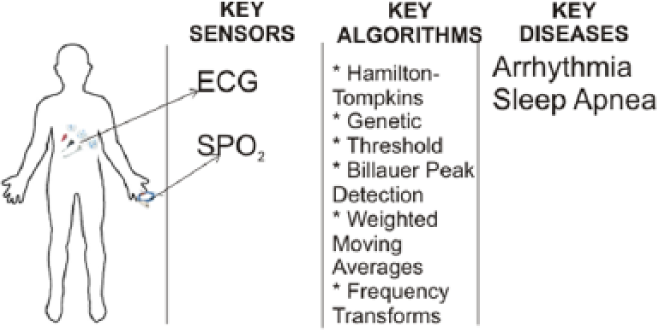
MVI and cardiovascular domain
A. Case studies
The Adaptive Ambient Empowerment for the Elderly (A2E2) project is a good example of a project that uses the concept of MVIs for AAL in the cardiovascular disease domain. 9 It was a 3-year project (2009–2012) sponsored by the European Union (EU) under the Ambient Assisted Living Joint Programme (AAL JP) with six partners across the continent. For the hardware, it utilizes signals harvested from the patient using the following sensors:
Nonin Onyx® II 9560 Pulse oximeter, Zephyr™ HxM;
A&D BPM UA-767PBT-C (automatic blood pressure meter);
GCDC X6-2 and Omron HJ-721IT (pedometer and accelerometer to track health and fitness);
A&D UC-321PBT-C (precision digital scale).
The first two sensors directly focus on the well-being of the heart, while the other two focus on general health and fitness, which in a way are also correlated to the condition of the heart. It uses a touch sensitive screen for its display interface.
To ensure interoperability, all these sensors are Continua certified.10,11 The system also integrates a virtual coach aimed at giving a personalized feel to the monitoring process and making it more acceptable to the seniors.
The details of the processing algorithm used in A2E2 were not provided, but the team stated that there was a connection to a remote processing system that gave a feedback to the patient via the virtual agent based on the results of the biosignal and feedback from the patient.
The Health@Home (H@H) project is another good example of an MVI-based AAL project that focuses on the cardiovascular disease domain. H@H was also sponsored by the EU under the AAL JP. It is used to monitor patients with chronic heart failure. 12 Its hardware is based on wearable ECG, SpO2, weight, blood pressure, chest impedance, respiration and posture sensors. The sensors communicate via Bluetooth with the home gateway which then forwards the aggregated biosignals to a remote server.
A threshold-based algorithm on the gateway processes the gathered data. The gateway is a customized netbook, and it provides data storage, computation and communication with the remote server at the physician’s end. The gateway to server communication is done via public Internet in a way that preserves confidentiality, authenticity and integrity of patient data. Health Level 7 International (HL7) Clinical Document Architecture (CDA) standard blocks are used for this communication. HL7 13 is a standard that addresses health and administrative data between Hospital Information Systems. The processing algorithm is quite accurate with results indicating less than 3% of false negatives and less than 5% of false positives.
III. Neurologic Domain
There is steep rise in the number of patients with neurological disorders across the globe. 14 This trend also affects patients who fall under the age bracket of seniors. According to the World Health Organization (WHO), approximately 15% of seniors have these disorders, and it accounts for 6.6% of the type of diseases they contend with Mental health and older adults. 15 MVIs can help physicians and care givers monitor some of the common neurological disorders, and the key biosignal used for screening for this disorder is captured by the electroencephalography (EEG) sensor. The sensor is placed on the scalp and is used to noninvasively detect the electrical signals that result from the neuronal activity in the brain. EEG signals can be used to screen a number of diseases including schizophrenia, bipolar disorder, depression, sleep disorder and Alzheimer’s.16–19
The galvanic skin response (GSR) sensor is also useful in measuring the stress level of a patient, and this value can be used to infer the neurological state of the patient.20,21
A summary of some key MVI features for the neurologic domain is given in Figure 2 .
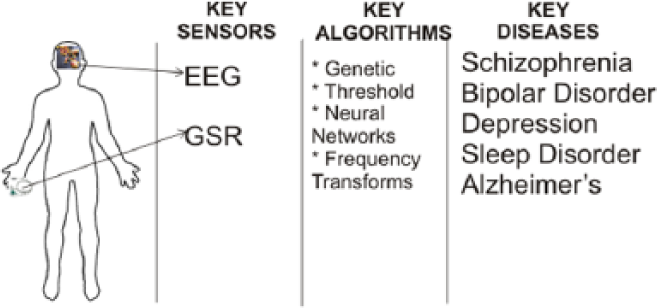
MVI and neurological domain
B. Case studies
MONitoring, treAtment and pRediCtion of bipolAr Disorder Episodes (MONARCA) and Online Predictive Tools for Intervention in Mental Illness (OPTIMI) are two projects that mirror the MVI approach, and they are used to identify neurological disorders.22,23
MONARCA (a 3-year Framework Programme–7 (FP7) project: 2010–2013) focused on bipolar diseases and the system generates a “behavioral profile” of the patient from the data harvested from multiple sensors, including EEG and GSR sensors. The GSR sensor is embedded in a smart sock. The sensors use Bluetooth to connect to the smartphone whose sensors (global positioning system (GPS), accelerometer and magnetometer) are part of the MONARCA system. The smartphone is used as a gateway device to the remote server and runs the threshold-based peak detection and event prevention algorithms. The smart sock contains a secure digital (SD) card used for storage in addition to its use of the memory of the smartphone.
OPTIMI is also a 3-year European Union Framework Programme–7 (EU FP7) project that ended in December 2012. It detects early signs of stress and depression based on readings from EEG and ECG sensors along with voice analysis and cortisol sampling. The sensors forward their data over the web to a remote database server. A query is done on the EEG readings for specific markers based on a neural network algorithm in order to detect the onset of mental illness. This information is used with some form-based data provided by the patients and therapists to determine the patient’s stress level. An appropriate Cognitive Based Therapy (CBT) is then recommended on the basis of the analysis.
IV. Hormonal Domain
The hormonal disease domain refers to a domain where disease screening requires body fluids such as blood. This is because a hormone is defined as a chemical substance produced in an organism and transported using body fluids. Health monitoring in this domain gives a real-time snapshot of the body fluid being monitored, and it provides a useful way for physicians to monitor a patient’s state of health.
Many types of diseases fall under this category. However, the discussion in this paper will focus more on diabetes screening as it is one of the most common diseases in this category. Blood glucose can be measured using a blood stained strip inserted into a glucometer or through an implanted sensor for continuous glucose monitoring. We will focus our discussions on the external glucometers since MVIs have a preference for the least invasive sensing approach.
C. Case studies
The iBGStar is a Food and Drug Administration (FDA) approved glucometer that embraces some of the MVI design approach. It is based on a 9 g device attached to an Apple iPhone or iPod. A blood stained strip is connected to the device, and the glucose level is determined by an algorithm based on a patented Dynamic Electrochemistry® technology.
An iPhone App runs a diabetes management software for keeping track of the glucose levels and alerting the appropriate third parties when the need arises. The iBGStar focuses on a general market but can also be used to support AAL technologies.
ScanaFlo 24 is another MVI-type device that focuses on the hormonal disease domain. It is a disposable platform for urine analysis. Its design allows it to screen for gestational diabetes, urinary tract infection, preeclampsia and other diseases. The device interfaces wirelessly with a smartphone, where the results are processed and displayed. ScanaFlo and its predecessor—Scanadu Scout—use virtual sensing to infer several readings from the measured biosignal.
V. Musculoskeletal Domain
This domain addresses any diseases that affect the muscles, bones or joints. Diseases in this domain are some of the most frequent diseases that affect the elderly. 25 Conditions like frequent falling, arthritis and rheumatism are common. 26
Fall detection and fall risk analysis techniques are usually based on the use of inertial measurement unit (IMU) sensors (especially the accelerometers) and threshold-based algorithms. 27 Other sensors used in the fall detection domain include vision and ambient sensors. 28 The vision sensor approach is based on the image analysis of the patient’s image. The ambient sensor approach analyzes vibrations detected by pressure sensors. Many of the vision and ambient sensor approaches are used with threshold-based algorithms.
A summary of some key MVI features for the musculoskeletal domain is given in Figure 3 .
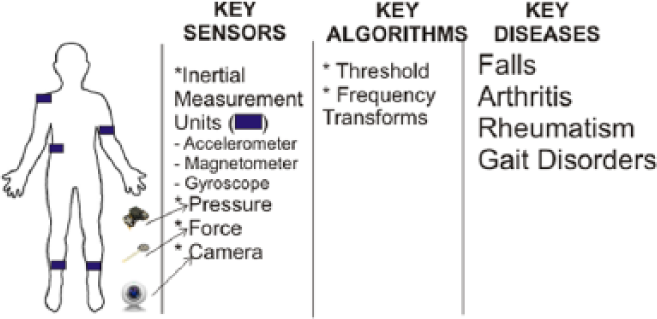
MVI and musculoskeletal domain
D. Case studies
The Ubiquitous Care System to Support Independent Living (CONFIDENCE) is a good example of a project that uses the MVI paradigm in for the musculoskeletal domain. It was a 3-year EU FP7 project that ended in 2011. For sensing, it used a number of “tags,” mainly consisting of IMUs. The tags were wirelessly interfaced with a base-station and a mobile phone. The system does the following:
Identify and localize the tags in order to generate a model of the user and the environment;
Categorize the activities based on a machine learning algorithm;
Notify the care giver or physician in the event of an abnormal activity such as falling.
The device in Pani et al. 29 provides another interesting case study of instruments in the musculoskeletal domain. It is used for hand function evaluation and to monitor the rehabilitation of rheumatic patients either locally or remotely.
It consists of a portable device that contains several sensors that measure statistics like force, temperature, potentiometer, torque and touch response. These statistics are extracted during the exercise sessions of the patients. The exercises include isometric exercises, like hand pinching, hand gripping, finger pinching and rotation. It also includes dynamic exercises like hand extension, rotation and finger tapping. Light emitting diodes (LEDs) and buzzers are used for notification and display.
The statistics are used to evaluate the hand function locally or are transferred to a remote transfer control protocol/Internet protocol (TCP/IP) server via global system for mobile communications/general packet radio service (GSM/GPRS) for deferred remote analysis using threshold-based algorithms.
VI. Open Research Issues and Future Perspectives
The aging of society and the attendant steep increase in the associated healthcare costs have increased the need for and use of MVIs. However, there is still a long way to go before the level of developments in MVI research can compare to the more mature traditional medical instrumentation field. In this section, we highlight some of the key research issues that need to be addressed in order to bridge the gap between these two categories of medical instruments. Addressing these areas will also enable MVIs to become the medical device of choice for patients and physicians. The summary of these key research areas is shown in Figure 4 .

MVI for AAL: key research areas and future perspectives
E. Invasiveness, expansiveness and virtual sensing
There is a strong preference for non-invasive sensors in MVIs, or at least sensors that are minimally invasive. However, the main challenge is that the more detailed medical tests tend to be invasive. For example, a large percentage of diseases can be diagnosed by testing the patient’s blood, 30 and this is an invasive process.
Virtual sensing may be able to help bridge the gap between the minimally invasive MVI sensing that only screens for few diseases and the more invasive traditional medical tests that can screen for a more extensive number of diseases. Researchers need to find a means of accurately mapping the easily accessible biosignals to the more desired but less accessible biosignals.
F. Personalization and reconfigurability
The sequencing of the human genome launched us into an era of personalized medicine, an era that promises to revolutionize healthcare. 31 This era will bring a lot of personalization into most aspects of medicine.
The flexibility of the MVIs makes them a good fit for the personalized medicine era. However, this would require the MVIs to take more details specific to the patients into account. At higher end, this means that the MVIs must be able to run algorithms that take the genotype into account while analyzing the phenotype in the disease screening process. At the lower end, it would require the MVIs to efficiently take the patient’s historical biosignals into account when processing future biosignals. The MVIs then need to support system reconfiguration to reflect the learned knowledge about the patient.
G. Multiparametric testing
Portability is an inherent design paradigm of MVIs, and they are generally designed to be self-contained, “one device” systems. However, there is an increasing need to have them support multiparametric testing. For example, the US$10m Qualcomm Tricoder X-Prize competition 32 seeks to design a portable device that can diagnose 15 diseases.
MVIs of the future will thus need to be able to screen for many diseases, covering a wide range of diagnostic complexity. An increase in the number of diseases that can be screened will lead to greater complexity, size and power requirements for the MVI. These conflicting requirements need to be addressed in future MVI research.
H. Preventive and therapeutic
Current MVI systems are more useful for diagnostic medicine. They have better medical utility value than health and fitness devices, but they still have some way to go before they become the instruments of choice for therapeutic medicine like their traditional medical instruments. Issues like safety and reliability will have to be given more attention before bodies like the FDA and European Medicines Agency (EMA) can approve a large number of therapeutic MVIs.
VII. Conclusion
In this paper, we have discussed the use of MVIs in four main disease domains that relate to AAL technologies. We have identified some case studies of projects in these areas and have also outlined key open research issues and future perspectives of MVIs for AAL.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.