
Abstract
Ambient Assisted Living has become a cost-effective option for coping with the rapid aging of society. Personalized health monitoring is an important aspect of Ambient Assisted Living, and it depends on the availability and use of appropriate medical devices. Medical virtual instruments provide a viable option for such devices. They refer to a hardware/software co-design of medical instruments that provides the dependability of hardware as well as the flexibility of software. In this paper, we discuss the concept of medical virtual instruments and their use as an effective option for Ambient Assisted Living. The discussion covers the enablers of this technology, the main challenges, and the hardware, software and connectivity options for such instruments.
I. Introduction
Ambient Assisted Living (AAL) techniques are helping senior citizens spend their golden years at home and in good health. 1 These techniques are based on information and communication technologies (ICTs) that identify, monitor and reverse their health problems in a way that improves their quality of life.
The rapid growth of the population of seniors—those above 65 years—in several developed countries across Europe, America and Asia, along with the dwindling health budgets, has increased the interest of both the government and researchers in AAL.
For example, in Europe, an AAL Joint Program based on a public–private partnership provided 700 million Euros to fund over 150 AAL projects from 2008 to 2013. 2 The success of the first phase has led to the extension of the project to cover another phase from 2013 to 2020.
In the United States, AAL or its counterpart—Independent Living research—is an active area of research in many top universities with funding from the National Science Foundation (NSF), 3 state governments and private funding sources. In the Republic of Korea, close to 40% of the population is expected to be above 65 years by 2050. 4 This has spurred the National Research Foundation into funding a number of AAL and Aging Well projects to ensure that life is as close to normal for these seniors. The 65+ age group is more prone to chronic disease, and there is usually a need to regularly monitor their vital signs and other body signals. However, it has become impractical to provide enough hospital beds and dedicated physicians to look after their well-being in an efficient and economic way. This has prompted physicians to adopt personalized health monitoring (PHM) as a cost-effective way to monitor seniors in the comfort of their homes.
PHM refers to the monitoring of health signals by patients with little or no medical training in non-controlled environments such as their homes. 5 Most times it refers to long-term monitoring of the health signals and is usually the first step in the identification and treatment of disease in seniors.
The geriatric section of the hospital is equipped with a number of devices that are used to support such health monitoring of seniors. A goal of the AAL process is the miniaturization of these devices to such a point that they can be conveniently used for PHM. This need has opened the door for the adoption of virtual instrumentation in AAL.
A. What is a virtual instrument?
A virtual instrument refers to an instrument that is not real in the sense that it does not have all the physical parts available in an equivalent traditional instrument. It utilizes a hardware/software (HW/SW) co-design approach, and a large portion of the instrumentation is implemented in software. 6 HW/SW co-design is an approach that can be used to design high-performance systems that have resource and cost constraints. It takes advantage of the high performance of hardware and the flexibility of software for system design.
The hardware of a virtual instrument consists of three main modules—the sensor, display and memory modules. The sensor module captures all the analog signals of interest and conditions them for further processing. Any instrument is of little use except it allows users to perceive the value of the measurements. The display module addresses this need by providing the user with a visual or non-visual indicator of the measurements. They are usually implemented on liquid crystal displays (LCDs), light emitting diodes (LEDs) or as audio alerts. In some devices, such as those that include tactile sensors, they also enable users to provide a feedback to the system.
There is an interval between signal acquisition and processing, and during this period the signals are stored in the memory module. The size of the signals can grow quickly, and it is important to have a type of memory module that anticipates this size. The module also stores the signals after they have been processed.
The software portion of a virtual instrument is made up of the processing and the interface modules. The processing module represents the core intelligence of the instrument. It implements the appropriate algorithms that govern how the sensed signals are processed. The interface module provides the bus required for intra- and inter-instrument communication.
The intra-instrument communication refers to the communication between the different modules of the instrument, while the inter-instrument communication refers to the communication between two distinct virtual instruments.
Some virtual instruments are implemented as embedded systems in an approach that is referred to as hard virtual instrumentation. This refers to virtual instruments that are implemented on reconfigurable hardware platforms such as a Field Programmable Gate Array (FPGA) ( Figure 1 ).7,8 The software portion is implemented on the FPGA’s soft embedded processor such as Xilinx’s MicroBlaze, 9 Altera’s NIOS, 10 and Actel’s Cortex M1. 11
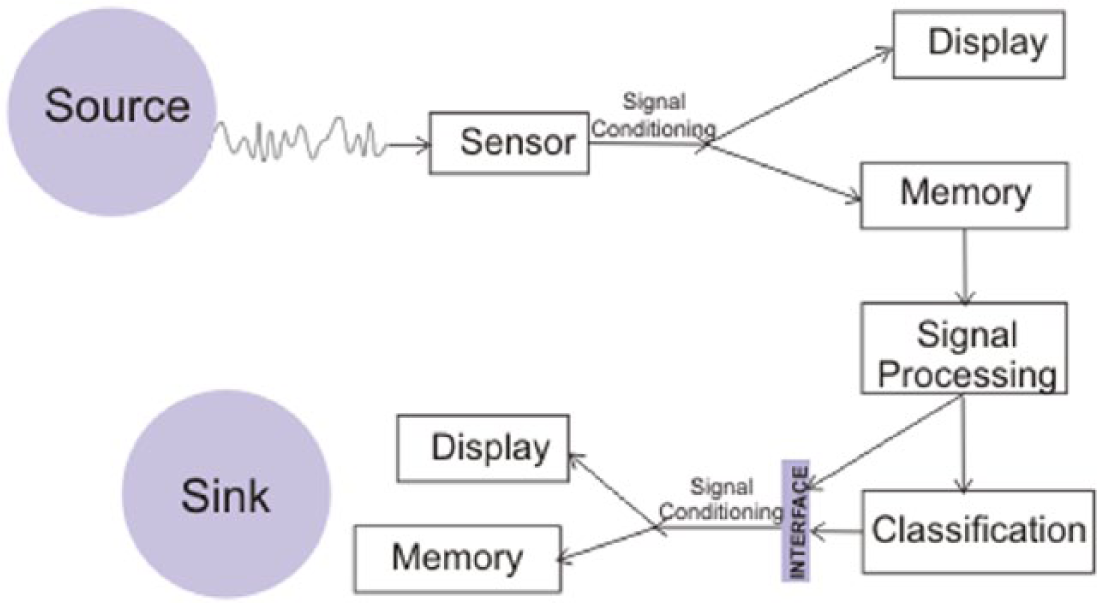
Some modules in a virtual instrument
B. Factors that have influenced the use of virtual instruments
There has been a significant growth in the deployment and use of virtual instruments in the last decade. 12 This can be attributed to some key technological advances in areas such as the sensors, memory, efficient lightweight algorithms, wireless communication and digital signal processing.
Semiconductor technologies such as micro-electro-mechanical systems (MEMSs) and nano-electro-mechanical-systems (NEMSs) have enabled the design of devices with high levels of functionality and miniaturization. As a result of these advances, sensors and actuators have become smaller, cheaper and more sensitive. They have also become less power hungry and include options for wireless communication. 13
In a similar vein, the density of memory devices and the processing capacity of processing devices have steadily increased over the years. In addition to these, the communication pathways between the different modules of virtual instruments now support high data rates. All these factors have played a key role in the development of virtual instrumentation. 14
II. Medical Virtual Instruments
Virtual instruments can be deployed across various industries and in different contexts. The virtual instruments used for AAL can be referred to as medical virtual instruments (MVIs) since they are used to implement the virtual form of the tradition instruments used in the medical domain within the context of AAL.
The source and the sink of MVIs differentiate them from general virtual instruments. 15 The patient is the source of the MVI, and the physician or the caregiver makes the sink of the instrument. As expected, MVIs are more delicate than general virtual instruments as a result of the human subjects at either end of the instrument. The other modules within the instrument are also chosen to reflect the specific measurements to be taken by the instrument.
A. Advantages of MVIs
Virtual instruments have a number of advantages over traditional instruments. In this section, we briefly discuss some of the benefits of MVIs over their traditional counterparts. These benefits have informed the growing use of MVIs in AAL projects.
Unlike the general virtual instruments marketed by some vendors, the MVIs are vendor-agnostic instruments. Also, they are modular and self-contained and thus do not need external PCs to function.
The first advantage of MVIs is their portability. Seniors need instruments that do not restrict their movement and virtual instruments can easily provide such portability and flexibility. Traditional medical instruments used to monitor seniors can be rather bulky, but MVIs are more compact because a large portion of the instrument is implemented as software. This enables them to be used for testing seniors at home—a major motivation for AAL. 16
The next benefit of an MVI is its flexibility. The flexibility of the system makes it easier to modify the parameters in real time to suit the specific needs of the patient or physician. Health monitoring technologies and standards change fairly quickly, and this easily leads to the obsolescence of traditional instruments. However, since a large part of the MVI is software-based, it is easier to ensure that they stay up to date since design changes can be swiftly made with a greater degree of freedom. The flexibility of MVIs also allows parts of a given instrument to be easily modified for use as another type of instrument.
MVIs also have the advantage of a much lower cost to functionality ratio than their traditional instrument counterparts. Virtualization of an instrument already reduces its costs significantly. In some cases, the costs can drop to less than 5% of the cost of the standard instruments.17,18 In addition to lower costs, the MVIs are able to simultaneously provide a number of parallel instruments and functions that further reduce the cost to functionality ratio of the equipment.
MVIs are modular and allow designers to reduce design complexity and allow for greater system integration than traditional medical instruments. Also, unlike traditional instruments, the modules support system re-use and are flexible enough for easy interfacing with compatible third-party devices.
III. MVI Hardware
The hardware of a MVI comprises the more rigid parts of the instrument. They have a greater effect on the performance of the instrument than they do on its flexibility. In this section, we describe the key components of MVI hardware.
A. Sensors
Sensors are one of the most important instruments of the MVI as they determine the quality of the biosignals that are measured from the patient. The type of biosignal to be sensed determines the type of sensor used in the MVI ( Table 1 ). Some of the most useful sensors used in AAL are described in the sections that follow.
MVI sensors
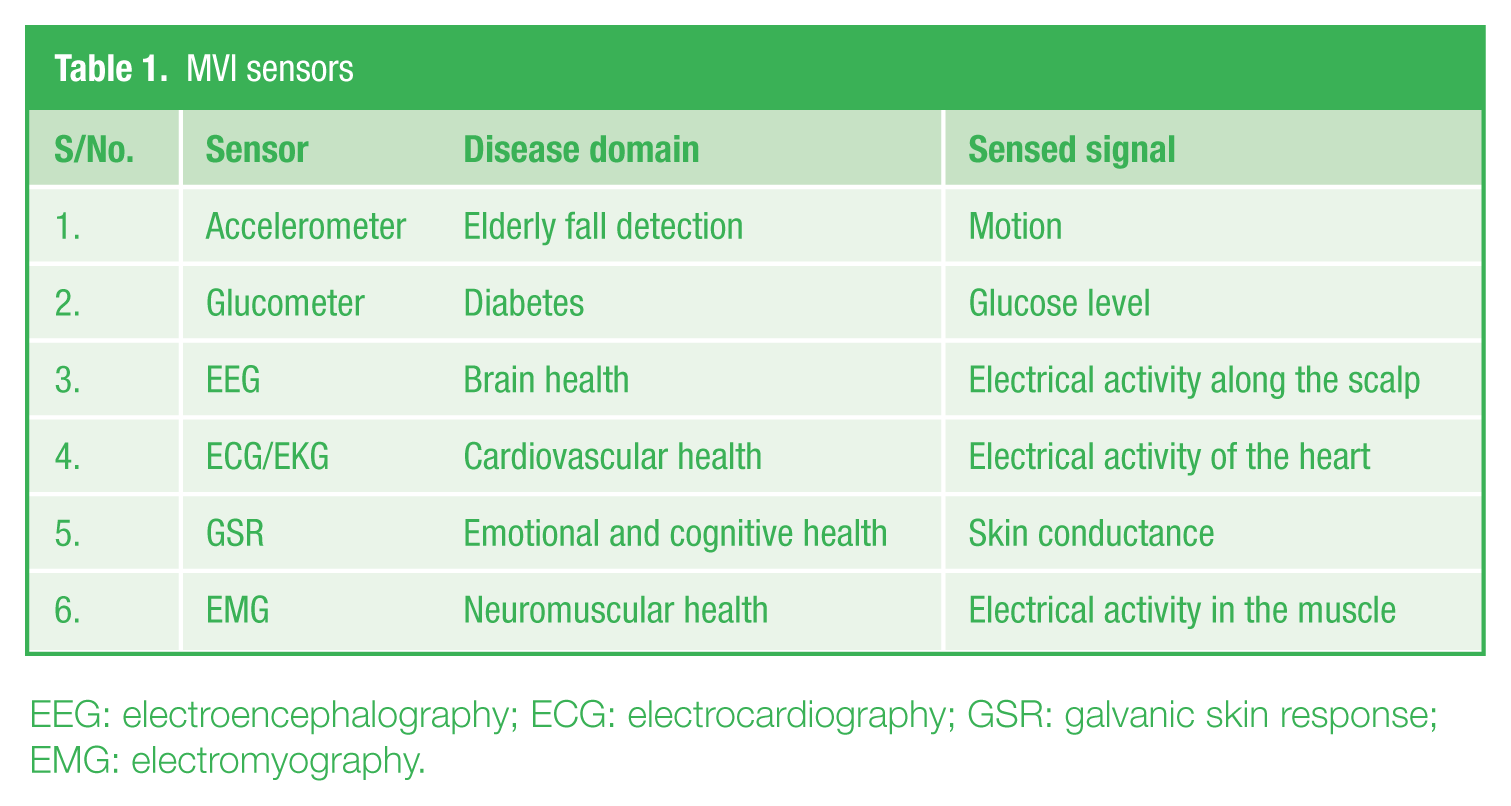
EEG: electroencephalography; ECG: electrocardiography; GSR: galvanic skin response; EMG: electromyography.
B. Accelerometer
A motion sensor is used to analyze the movement of the patient. 19 The accelerometer is the main instrument used for detecting motion and is used to measure the acceleration forces acting on a body and can analyze the movement patterns of a patient. 20 It does not measure the standard acceleration, which is the rate of change in velocity, rather it is used for measuring the acceleration perceived as the weight of the body. 21 It is measured using g-force or “g” units, where 1g represents the standard gravitational acceleration of the earth, 9.81 m/s2. It takes both static and dynamic readings.
A number of systems are based on triaxial accelerometers that measure values along three orthogonal axes, usually the x-, y- and z-axes, to give Ax, Ay and Az readings. Thresholding provides a common and straightforward approach for inferring the condition of the patient from the accelerometer readings. It generally requires obtaining a single value from the readings. This value, known as the resultant value, R, is calculated as shown in equation (1)
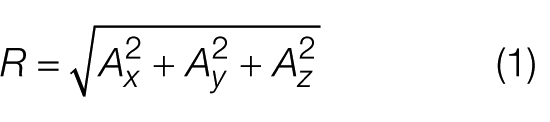
Some of the important specifications for an accelerometer include its sensitivity, sampling rate and maximum swing. 22 Sensitivity refers to the change in measured output for any given unit of change in the measured signal, and it is measured in millivolts per gravity. Generally, the more sensitive the accelerometer, the better it is.
The sampling rate refers to the number of accelerometer readings that can be taken every second and is measured in Hertz. It should be guided by the speed of the intended application. The maximum swing refers to both the lowest and highest values of the readings that can be recorded by the accelerometer. It is the maximum force the device can accommodate on a given axis. Typical values include ±1.5g, 2g and 5g.
Accelerometers used in MVIs are generally used as wearable sensors either as in wristwatches 23 or velcro strapped onto the body. 24 The choice of the positioning depends on the intensity of the activity being monitored. For example, the accelerometers can be strapped to the waist, arm and knee for low-, medium- and high-level activities, respectively. 25
C. Glucose meter
This measures the approximate concentration of glucose in the blood and is very useful for patients suffering from diabetes mellitus. 26 The standard approach involves pricking of the fingertip to obtain a blood sample on a chemically active disposable test-strip. The test-strip is then used as an input to the glucose meter to give the glucose level typically measured in millimoles per liter. Diabetic patients test their glucose levels several times a day. 27
The glucometer derives its reading from the electrochemical reaction between the glucose in the blood and the chemicals in the strips. 28 Modern glucometers are based on strips that use a chemical known as glucose oxidase. 29 It is an enzyme that reacts to the glucose in blood. The electrode in the meter measures the strength of the electric flux generated by the chemical reaction in order to quantify the level of glucose in the blood.
Continuous glucose monitoring (CGM) is another approach that is gaining popularity and is a better fit for health monitoring using MVIs. It involves the use of a biosensor that is placed underneath the skin for a few days to a week. It checks the glucose level in the tissue fluid rather than the blood. 30 This approach is more expensive than the test-strip method. It also has greater latency since the glucose level in tissue fluid lags the glucose in blood by about 5 min. 31 However, although invasive, it is easier to accommodate in automated systems.
Accuracy, sample size and latency are some of the most important considerations when choosing a glucose meter. The accuracy of the meter is very important as it helps the patient to avoid frequent false positives and false negatives because erroneous results can have dire consequences for the patient. Generally, the acceptable margin of error is within 15% of the actual value. 32
The less the amount of the sample size, the better it is as long as the margins of error are not exceeded. This is because the amount of blood or fluid used is proportional to the level of comfort experienced by the patient. The quality of the meter is also determined by the speed of the results. Most meters give an output in less than a minute, while a few provide results in a few seconds. 33
D. Electrocardiography and electroencephalography sensors
Electrocardiography (ECG/EKG) and electroencephalography (EEG) sensors have similar classifications and design considerations. As such, we will discuss them together in this section.
ECG refers to the non-invasive recording of electrical activity that results from the polarization and depolarization of the cardiac tissue. 34 An average ECG signal ranges between 1 and 10 mV, and a typical ECG signal consists of different sections, namely, a P-wave, QRS complex and a T-wave ( Figure 2 ). The cycle-to-cycle characteristics of these sections help physicians to determine the state of the heart and can be used to screen for heart diseases.
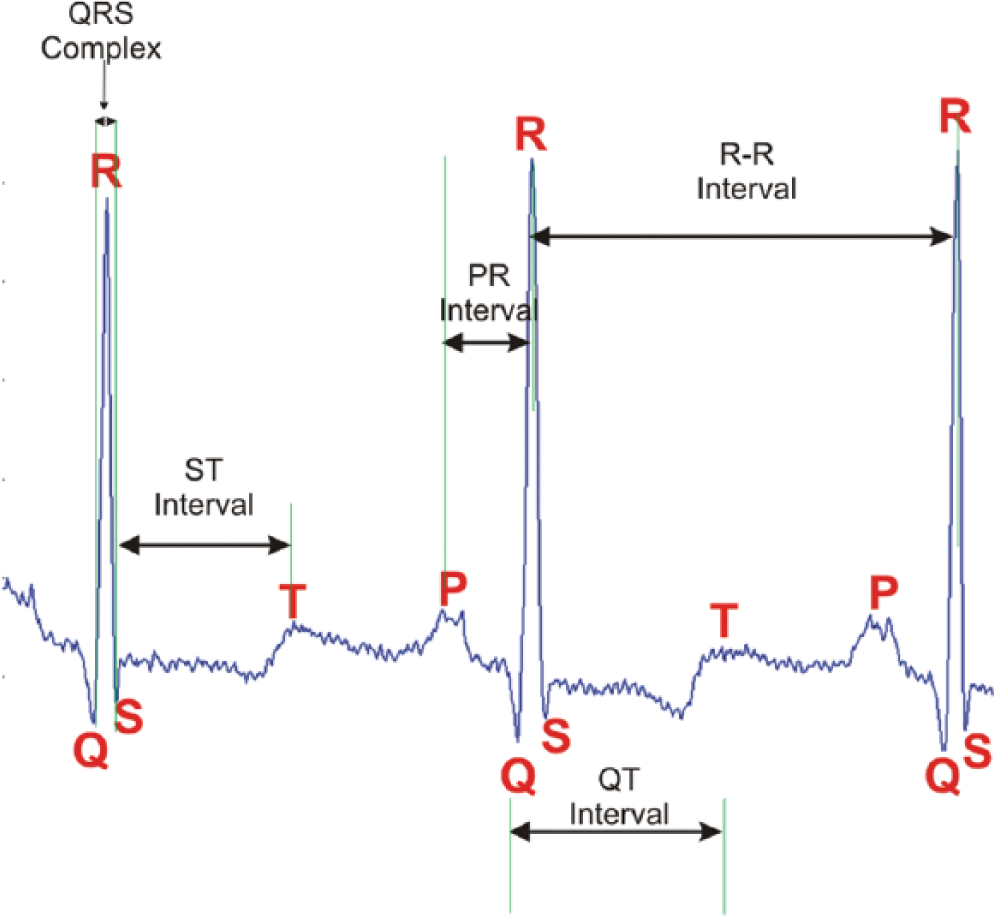
Key segments of an ECG signal
EEG refers to the recording of electrical activity on the scalp resulting from neuronal activity in the brain. The EEG signals range between 10 and 100 µV and are much lower than those of other biosignals.35,36 The positioning of the EEG sensors is usually based on the international 10–20 placement system. 37
The sensors measure the readings of the appropriate signals on the skin. There are two broad groupings of ECG and EEG sensors, each with two types—the wet, dry and noncontact on the one hand and the active and passive on the other. 38 The wet sensors require the use of conductive gels and are usually made up of Ag/AgCl electrodes. Wet sensors have been used for decades and are very accurate. They are the preferred approach for taking readings at the hospital. However, they require skin preparation and can be rather uncomfortable for long-term monitoring.
The dry electrodes make direct contact with the scalp and do not require any skin preparation. They are more comfortable for the patient but tend to provide lower signal levels due to the skin-electrode impedance posed by the unprepared scalp. 38 They also experience greater motion artifacts since they do not use any conductive gel to hold them in place. The noncontact sensor does not make any direct contact with the scalp. It measures the signals through a capacitive coupling of the sensor to the scalp. Of the three types, the noncontact sensor is the most convenient and unobtrusive for the patient as it does not require any skin preparation. However, motion artifacts have the greatest effect on these types of sensors.
The active and passive sensor types are defined based on the use of an external electronic circuitry to amplify the weak EEG signals and suppress noise. 39 The active sensor includes a low noise amplifier with high input impedance. It is used for the suppression of noise, amplification of the signal and reduction in the effect of the high skin-electrode impedance. The passive sensor detects the signals without the aid of any external circuitry. Practical systems are usually of the active type.
Key considerations in the choice of health monitoring ECG/EEG sensors include the sampling rate, sensitivity, noise level and channel size. EEG signals have a high temporal resolution with signals generated in the order of milliseconds. 40 As such, an EEG sensor needs a sampling rate high enough to detect the signals. Typically, the minimum sampling rate should be 500 Hz. 41 The minimum sampling rate for an EEG signal is within the range of 200 Hz. 42
The EEG signal level is very low, and it is important to have a sensor with a high level of sensitivity that can detect small changes while being robust to noise. The ECG signal has less stringent sensitivity requirements due to its higher signal level. The channel size refers to the number of simultaneous signal readings taken by the sensor and is dependent on the number of electrodes on the sensor. The channel size is determined by the type of application and the expected cortical coverage or the conduction system of the heart. Generally, the higher the channel size, the more accurate the readings, but this also leads to a larger sensor with more complex processing.43,44
E. Galvanic skin response sensor
Galvanic skin response (GSR) sensors are used to measure the electric conductance of the skin.45,46 The conductance depends on the sweat-induced moisture of the skin and is a reflection of the physiological and psychological state of the patient. 47 The working principle of the GSR is based on the fact that the skin temporarily becomes a better conductor of electricity when the subject is physiologically aroused. 48 To improve the level of signal detection, the GSR sensors are placed where there is a high density of the eccrine sweat glands. These areas include the palms and the soles of the feet.
Micro Siemens (µS) and arbitrary analog units (Arb) are the measurement units for skin conductance. Key features to determine the quality of a GSR sensor include its sampling rate (Hz), resolution (ns), analog-to-digital converter (ADC) resolution (bits) and its range of operation.
F. Electromyography sensor
Electromyography (EMG) sensors measure the electrical activity in the skeletal muscles. 49 There are two types of EMG sensors, namely, the surface and the intramuscular. 50 Testing with the latter involves the insertion of needles into the muscles, and it requires the supervision of a health expert. As such, for PHM, the surface option is more appropriate. However, the surface EMG sensor is not as specific to the muscle area as the intramuscular EMG sensor. 51
The key issues in surface EMG are signal-to-noise ratio and distortion of the signal. An average EMG signal ranges from 0 to 10 mV, and the dominant frequency range of the signal is 50–150 Hz. 52 The sensors can either be the wet or the dry type, and the characteristics are similar to those discussed for ECG and EEG sensors above.
G. Virtual sensors
In some cases, it is either expensive or impractical to sense the physical quantity of interest. In such instances, it may be possible to use a proxy or surrogate sensing approach. This involves sensing a signal that is easy to sense and using the value to estimate the signal of interest. The sensor used in this approach is known as a virtual sensor since it does not monitor the real signal of interest. The common methods for virtual sensing include the analytical and empirical methods. 53 The analytical method involves the use of equations that show a relationship between the measured signal and the signal of interest. For situations where there is no clear-cut relationship between the entities, approximate models are used.
The empirical method for virtual sensing involves observing historical data of both the measurable quantity and the quantity of interest. A correlation is done between both data, and the healthcare specialist then infers the signal of interest from the current sensor data from the measurable signal.
One example of the use of virtual sensing in PHM is the SpiroSmart. 54 It is based on the audio data recorded on a mobile phone and generated from the full lung exhalation of a patient. It is used to estimate the spirometric measures of lung function with an accuracy of 94.9% when compared to standard tests done with expensive spirometers.
Another virtual instrument based on virtual sensing is discussed in Bukkapatnam et al. 55 It derives hemodynamic signals from ECG and thus obviates the challenge of purchasing expensive equipment for measuring hemodynamic signals.
H. Smartphone-based sensors
Smartphones are fast becoming a useful tool for MVIs due to the number of sensors that have been integrated into them.56,57 For example, a typical smartphone contains the following sensors: accelerometer, magnetometer, gyroscope, ambient light sensor, microphone, GPS location sensor, capacitive touch screen sensors and infrared sensors.58,59
A cursory look suggests that these are not typical sensors of interest for the MVI domain. However, it should be noted that many other standard sensors such as ECG, EEG and glucometer can be interfaced with the smartphone via a Bluetooth connection. Also, virtual sensing techniques can be used to infer signals of interest from signals measured using the smartphone’s embedded or external sensors.
I. Display and storage in the MVI’s hardware
The display and the storage modules complement the sensors as the main components of the MVI’s hardware. LEDs and LCDs are typical display options used in MVIs. Of the two, the LED is a cheaper and more power efficient option. 60 Single LEDs can be used to indicate test results. For example, a set of three LEDs with different colors can be used to qualify the glucose level measured in a glucometer as too low, normal or too high. A seven-segment LED display can be used to display more detailed results that include numbers and letters. LCDs are more efficient and have better brightness and contrast ratios albeit at a more expensive price. Some systems also use audio prompts to inform the patient of health monitoring results.
J. Memory
MVIs require memory modules that can store data during the different stages of processing. The type and size of the memory required depend on the type of computation and its frequency. For example, an MVI used as a glucometer requires far less memory than an MVI used for 16-channel EEG recordings. Memory options include random access memory (RAM) or secure digital (SD) card memory available on the instrument. However, due to large memory requirements in a number of MVIs, developers now use the option of cloud storage. 61
K. Specialized hardware
For some MVIs, there is a need to use specialized hardware along with the standard hardware discussed earlier. Such specialized hardware is used to include features that can enable reconfigurability or can speed up the algorithms used in the MVIs.
Examples of such specialized hardware include FPGAs, Graphics Processing Units (GPUs) and Programmable System on Chips (PSoCs). The FPGAs can support real-time reconfiguration of digital blocks and, depending on application, can provide speed-up values of between 20 and 200 times. 62 GPUs had hitherto been more common in the gaming industry, but in recent times other domains have begun to take advantage of their number- crunching ability to process computationally intensive tasks. Many of such tasks are common in the medical domain. 63 Like the FPGA, the PSoC also supports programmability and reconfigurability. However, unlike the FPGA, they support both analog and digital processing blocks, albeit at a slower processing speed than FPGAs. 64
IV. MVI Software
Flexibility is one of the most important advantages of MVIs, and the software portion of the instrument has a key role in this attribute. It enables the instrument to be customized to suit the requirements of the measurement.
The software portion of the MVI includes modules that are neither part of the hardware nor the connectivity of the instrument. It represents the core portion of the device, and all the signal processing takes place here. It typically includes modules for data analysis, drivers, graphical user interface, error processing, controllers, device drivers, storage, communication and a library of virtual instruments. 65
The software typically runs on a microprocessor attached to the instrument.66,67 For MVIs implemented on mobile phones, the software comes in the form of an app that runs on the phone.68,69 On distributed and network-enabled MVIs, the software portion can also reside on a remote server or on the cloud. 70
We discuss the key components of MVI software in this section.
A. Algorithms for classification
Medical instruments are used to screen for diseases, and in MVIs the algorithms play an important role in the process. 71 The algorithms used in MVIs refer to a step-by-step procedure for diagnosing and classifying a disease using a finite number of steps. The choice of the algorithm used depends on the type of diseases to be diagnosed, type of input parameters available for the process and the available resources for the computation.
Several algorithms can be used with MVIs. A number of the main algorithms used across the various disease domains are either a subset or a combination of the following categories: support vector machine (SVM), genetic algorithm (GA), threshold-based and neural networks (NNs).
An SVM is a supervised learning model that uses data points (support vectors) closest to the decision surface (hyperplane) of the expected diagnosis to classify new data. 72 It provides a deterministic approach to obtaining an accurate classification that is unique and global. However, the algorithm can tend to be complex and have high memory requirements. 73 In Harikumar et al., 74 SVM is used to classify the risk of epilepsy in patients based on their EEG signals.
A GA is a bio-inspired approach that is based on adaptive heuristics. It mimics the process of natural selection in nature and implements the classification using a fitness function. This algorithm is conceptually simple and useful for scenarios where there are several input parameters. The inductive nature of GA means that it can work with internal rules and does not need to know or work with the problem-specific rules. As a result, GAs can be used for several types of problems.
It also has the advantage of being robust to dynamic changes in the system environment but cannot integrate problem-specific information. 75 GA is used to predict the presence of heart disease in Jabbar et al. 76
For many of the biosignals, it is possible to predict the presence or absence of a disease based on a given level in the signal, and this level is known as the threshold. Algorithms based on the thresholds classify the disease based on some pre-specified or adaptive threshold. These types of algorithms provide a heuristic approach that is straightforward and generally simpler to implement than the other types of algorithms. Threshold-based algorithms are used with ECG signals in Kew and Jeong 77 and for fall detection in Wang et al. 78
The NN is a nondeterministic algorithm that was inspired by the interconnection of the neurons in the brain. Its classification is based on simple but highly connected processing elements whose weights are dynamically modified in response to incoming signals based on some learning rule. It is an accurate, robust and highly parallel technique. However, it is comparatively slower than other algorithms and tends to be resource intensive for systems with large input data sets. 79 It is used to screen for heart diseases in Jin et al. 80
B. Evaluation metrics
The choice of the algorithm to use for a given disease domain should depend on the following metrics—accuracy, precision, training time, speed, robustness, scalability, specificity and selectivity.
The accuracy refers to the proximity of the measured value to the actual value. In the field of medicine, the accuracy of the measurement has a greater level of importance as it may well be the difference between life and death for the patient. The accuracy is a ratio of the correct readings (true positives and true negatives) and all the readings taken. Precision refers to the consistency of the results under unchanged conditions. It is the ratio of the true positives to the total number of positives (true and false).
Speed refers to the duration it takes to complete the classification process, and this includes the training process for classifier algorithm. For many medical signals, this training process is needed for proper analysis and classification. The robustness of an algorithm describes how much the performance is independent of the type and distribution of the input signals.
Scalability refers to the ability of the system to maintain its level of performance as the size of the input signal increases. In medical diagnosis, the specificity is the proportion of negative classifications that are correctly made, while the sensitivity refers to the proportion of positive classifications that are correctly made. As such, specificity focuses on correct exclusions, while sensitivity focuses on correct detections.
V. Connectivity Options for MVIs
The measurement and analysis of the biosignals of patients are of little value unless the results are communicated to an appropriate caregiver or medical decision maker in a timely manner. The connectivity options for an MVI allow such communication to take place.
Connectivity basically refers to the process of initiating and maintaining communication for a dataflow between the MVI and a remote instrument or an information system. There is a preference for wireless communication options since MVIs are designed for portability and mobility.
In this section, we describe the salient features of the main protocol standards along with the important considerations for MVI connectivity.
A. Protocol standards
There are four main protocol standards for short-range communication, and they are all used for MVIs. They are Bluetooth, ZigBee and WiFi. They all operate in the Industrial, Scientific and Medical (ISM) frequency range of 2.4 GHz.
The Bluetooth was developed in 1994 as a replacement for the cable. 81 It provides inter-device communication for up to eight simultaneous devices within a radius of about 10 m and has low power requirements (about a third of what mobile phones use). It also has data rates up to 1 Mbps and is popular with the mobile phone and many other portable consumer products. For the MVI, Bluetooth is used to communicate between wearable sensors or mobile phones and the main MVI device on the one hand and the MVI and a communication gateway on the other. 82
The ZigBee protocol was developed in 1998 and can be used to connect around 65,000 simultaneous devices. It has very low power requirements and data transfer rates of up to 250 kbps. Wearable devices can also be connected to the MVI using the ZigBee protocol. The very low power requirement of ZigBee devices increases their appeal for use in MVIs. 83
The WiFi protocol was developed in 1991 and provides long-range inter-device wireless communication of up to 100 m. Unfortunately, it requires much greater power and is more prone to interference from other devices. It can provide data rates of up to 54 Mbps. 84 MVIs mainly use WiFi to connect to the communications gateway that transfers the measured signals to a remote location.
B. Interoperability standards
MVIs can comprise a number of off-the-shelf devices, and it is important that they are interoperable. Interoperability allows these devices to seamlessly share information among themselves. It can be enhanced when the individual devices adhere to the appropriate industry standards.85–87 Some of the main efforts geared toward promoting this interoperability include the Continua Alliance and the Personal Health Data (PHD) standards (ISO/IEEE 11073).
The Continua Alliance is a 240-member group whose goal is to build a system of interoperable personal health solutions. 88 At the moment, it is the only collaborative effort focused on supporting personal telehealth. It focuses on three main areas, namely:
Disease management;
Aging independently/AAL;
Health and fitness.
The Continua products focus on portable devices that utilize wireless protocols, thus making them an ideal fit for MVIs. Continua certifies products that are interoperable with other personal health devices. Medical device developers must design their systems in accordance with appropriate standards in order to obtain the Continua certification. These standards are based on the ISO/IEEE 11073 PHD standards, and they support both Bluetooth and ZigBee protocols.
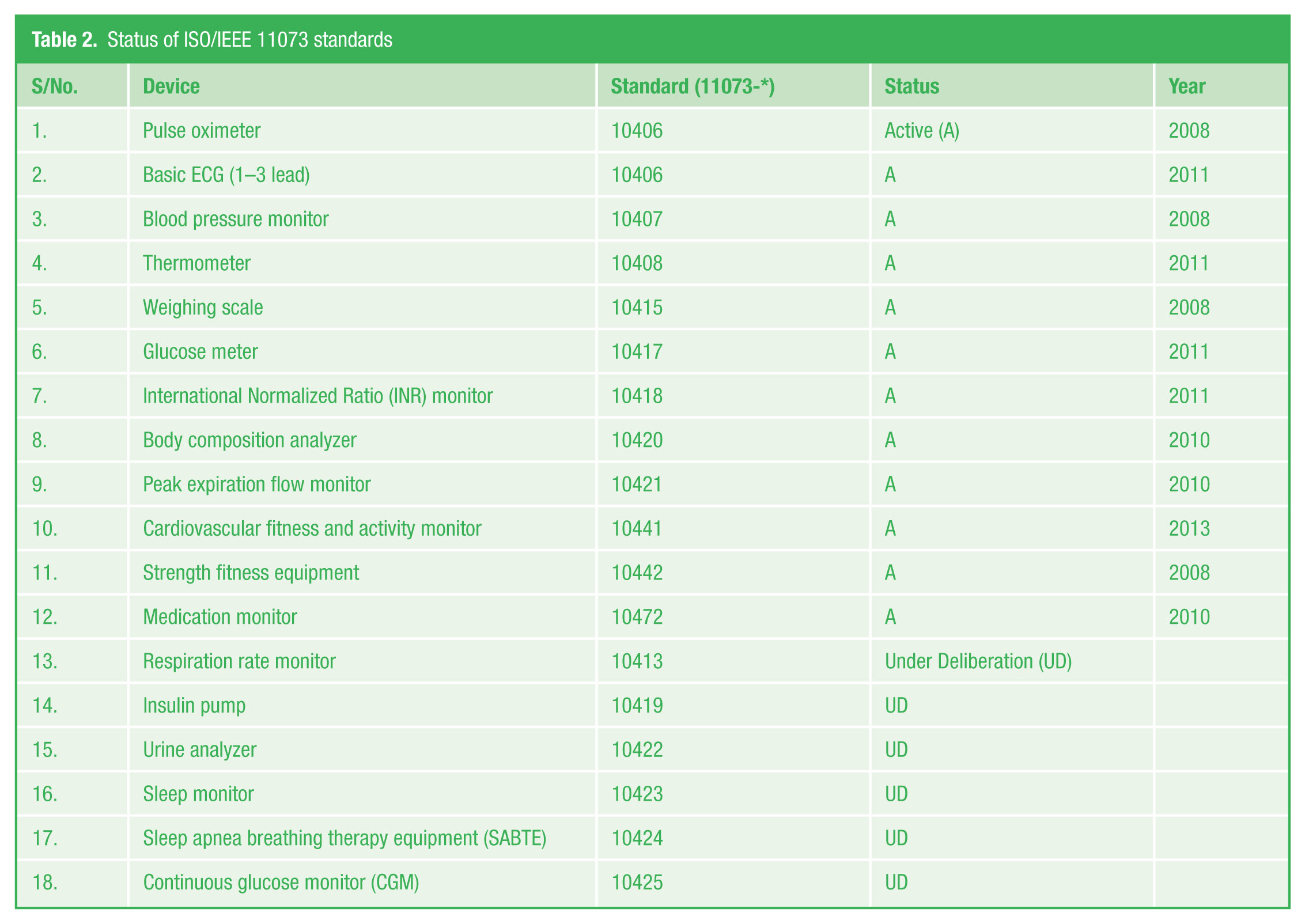
The ISO/IEEE 11073 standards support communication between personal health devices and external devices. Examples of these health devices include glucometers, thermometers, pulse oximeters, blood pressure meters, peak expiration flow monitor, weighing scale and a host of other devices. 89 Table 2 shows a list of the current device standards, their status and the year some of them became active. The standards define the exchange and representation of data exchange as well as the terminology for communicating between personal telehealth devices and compute engines. 88 They also make it easier to interface the devices with the Electronic Medical Records (EMRs) and can potentially reduce charting errors and enable the integration of decision support systems.
Status of ISO/IEEE 11073 standards
Agent, transport and manager are the three terms frequently used in this standard. The agent represents the health device, and the transport refers to the communication interface that facilitates the transfer of data to a remote device known as the manager. 90
C. Privacy and security
Health-related data are considered to be one of the most sensitive types of data. 91 Patients are uneasy about the risk of their online health records, meant to be accessed by a trusted doctor or caregiver, ending up with some stranger or a person with malicious intent. As such, privacy and security are important concerns that need to be addressed in the deployment of MVIs.
Privacy ensures that the data are only accessed by the appropriate people, while security addresses the confidentiality, integrity and availability of the data. One may argue that privacy and security should not be so important with MVIs since they are basically meant for health monitoring for individual patients. However, the fact that the data may need to be transferred over a network to a physician or caregiver makes it an important issue.
A number of implementation options exist with varying ranges of complexity. These include passwords, encryption and biometric access. Privacy and security of personal health data are governed by rules and laws specific to the countries of deployment. 92 For example, the Health Insurance Portability and Accountability Act (HIPAA) is used in the United States, the Data Protection Directive is used in the European Union and the Personal Information and Protection Act (PIPA) is used in Korea.
VI. Conclusion
In this paper, we have described the key elements of MVIs and discussed the important role they can play in medical instrumentation and PHM, especially as it relates to AAL technologies. Key metrics and design parameters that affect the utility of these instruments were also discussed.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.