
Abstract
Based on case studies in 12 nursing homes in the United Kingdom, the authors illustrate how financial cutbacks affect job quality and the quality of care. The dimensions of job quality that suffered most were those directly related to the ability of workers to provide care: reductions in staffing, longer working hours, and work intensification. Cuts to labor costs eroded the quality of workers’ jobs in all 12 homes but with two differential outcomes: in seven homes, care quality was maintained, and in five homes, it deteriorated. Care quality was maintained in homes where a patient-centered care approach and remaining job quality allowed workers to develop work-arounds to protect residents from spillover effects. Care quality declined in homes where custodial approaches to care and low job quality did not provide workers the time or resources to protect residents or to maintain prior levels of care. A tipping point was reached, leading to a spillover into impoverished care.
Worries about the quality of residential elder care are a global concern (OECD 2013). As the number of residents in nursing homes 1 has increased dramatically in recent decades—and will double in the next 40 years (European Commission 2008)—a key challenge is the provision of affordable high-quality residential care. The financial crisis of 2008 led to greater concerns about the quality of care because of declines in public funding.
Research on the nursing home industry has focused on two dominant themes: the poor quality of care that many residents receive and the poor quality of jobs of the care workers. These are often viewed as distinct problems and investigated separately by scholars (Eaton 2000). Considering job quality and care quality separately can gloss over the more complex picture of how they relate, particularly in times of declines in public funding. We use data collected in the wake of the financial crisis from 12 UK nursing homes in 2009 to 2012 to investigate whether job quality and care quality are linked in a systematic way. We analyze how ongoing and accelerated cost pressures differentially affect the quality of jobs and care in nursing homes that use different approaches to care: person-centered and custodial. We investigate how cost-saving measures affect the job quality of workers. We show that reductions in labor costs were common across all the homes in the study—including pay, benefits, and staffing levels—in addition to changes in shift patterns and skill mix. Yet the effect on care quality varied across homes. In seeking to account for this variation, we examined how and under what circumstances the approach to care provided the necessary support for care workers to protect residents from the adverse effects of cost cutting and under what circumstances they did not, leading to a spillover from the poor quality of the jobs to impoverished care. For each outcome—maintained care quality and spillover into poor care—we first examined the changes in job quality at each nursing home, mapping the ownership type to the care approach and the changes introduced into care workers’ jobs. Second, we examined patterns in the ways that deterioration in the quality of the jobs affected workers’ ability to provide care. We contribute to the literature by showing the relationship between the quality of jobs and the quality of care, demonstrating that the two cannot be understood separately.
Connecting Job Quality and Care Quality
Increasing attention has been paid to the concept of job quality in the literature because strong evidence shows a “good job” is better for workers’ health, life expectancy, and life chances than a “bad job” (e.g., Coats and Lehki 2008); in addition, significant shifts in how work is organized continue to raise concerns about working conditions and the erosion of job quality (Osterman 2013). The effect of the financial crisis in 2008, for instance, has increased financial pressures on organizations, and their need to address budget deficits has led management to demand more of people at work, as organizations look to their workers to do more with less (e.g., Overell et al. 2010).
Job quality is defined as a “set of features that help to meet jobholders’ needs from work” (Green et al. 2013: 754). It encapsulates material and intrinsic benefits for workers (Iskander and Lowe 2013): compensation, the degree of work intensification, the employment contract, task diversity, and the level of autonomy (Findlay, Kalleberg and Warhust 2013; Holman 2013; Osterman 2013). Care-work jobs are typically portrayed as bad jobs with poor quality, in that they are characterized by low wages, low benefits, hard physical work, and low levels of autonomy (Appelbaum, Bernhardt, and Murnane 2003; Lloyd, Mason, and Mayhew 2008). Nevertheless, job quality across nursing homes varies widely. Some homes offer far better compensation, benefits, training, and opportunities for advancement than others (Hunter 2000). Because labor is the largest cost component in services such as nursing homes, it is a major target for cuts during times of ongoing and accelerated cost pressures. Cuts in labor costs can lead to lower job quality, including lower pay and worse conditions, fewer resources, less discretion, and fewer opportunities at work. The focus of most of the literature has been on workers, which is important but does not link job quality to organizational outcomes such as the quality of care.
Research into care quality has tended to look at care in isolation from job quality. Interest is now increasing, however, in how care approaches affect care-quality outcomes. Two alternative approaches to conceptualizing care can be found in the literature: person-centered and custodial. Person-centered care is guided by the individual needs and preferences of residents (Avgar, Givan, and Liu 2011) and assumes that residents will be active participants in shaping how their care is managed. In custodial care, the focus is on providing a safe physical environment and meeting the immediate physical needs of residents. Custodial care assumes residents are not capable of determining how their care is provided; instead, residents tend to be viewed as passive recipients of routine assistance (Culley and Courtney 1993). Nursing homes providing custodial care are more likely to be viewed as being in need of changing to adopt a person-centered care approach (Zimmerman, Shier, and Saliba 2014).
Person-centered care typically includes enough flexibility in the system of care to meet the complex, changing, and distinct individual needs of residents (see, e.g., Institute of Medicine 2001; Edvardsson, Winblad, and Sandman 2008; Banaszak-Holl, Castle, Lin, and Spreitzer 2013). Such care quality is difficult to define, but the concept of person-centered care typically includes the following characteristics: is tailored to meet individual needs, takes place in suitable premises with equipment that is clean and in working order, provides residents with enough food and drink, affords residents dignity and respect, gains a resident’s consent before treatment is given, ensures residents’ safety and protects residents from abuse, and supports the discretion for residents to complain about their care (Care Quality Commission [CQC] 2014a). Nursing homes adopting person-centered care are identified as more likely to provide residents with opportunities to exercise choice and control over their care (Eaton 2000). What is missing in studies of care quality is how job quality constrains or supports the ability of staff to provide person-centered care (Zimmerman et al. 2014).
Scholars have linked the capacity of a nursing home to provide person-centered care (Lucas et al. 2007), appropriately trained and consistent staff, and individualized services (Castle 2002) to the availability of financial resources. Koren (2010) demonstrated, for example, how workforce regulations and lower-than-expected reimbursement of fees limited the potential of person-centered care initiatives to improve the care given to residents. Scholars have tended to assume that for-profit nursing homes offer a lower standard of care because their managerial objective to provide returns to investors results in a stronger incentive to minimize expenditures than do nonprofit facilities. Some researchers argued, for example, that extracting revenue from a nursing home to distribute profits to shareholders influences the organizational priorities and spending decisions away from care, sacrificing quality and resident safety in the interests of maintaining efficiency (e.g., Harrington et al. 2001; O’Neill, Harrington, Kitchener, and Saliba 2003; Pear 2008). A systematic review and meta-analysis of observational studies and randomized controlled trials investigating the quality of care in for-profit compared with nonprofit nursing homes found more, or higher-quality staffing, in nonprofit homes (which, on average, offered 0.42 more staff hours per resident each day than did for-profit homes) (Comondore et al. 2009). In contrast, single studies (prior to pooling the findings) showed little difference in the actual care-quality outcomes (measured using numbers of deficiency ratings). Poor care and deficiencies in the quality of care occur in nonprofit nursing homes as well. The simple association between profit status and care quality does not provide sufficient information about the nature of the relationship between the level of resources available to a nursing home and care quality. What is missing from these studies is an examination of the resources available to the nursing homes to organize work processes and of the care outcomes they achieve.
Our research brings together these two strands of research—job quality and care quality—to examine how they relate. Labor scholars have researched the link between the organization of work processes and care quality (Eaton 2000; Ochsner, Leana, and Appelbaum 2009; Avgar et al. 2011; Grabowski, Stevenson, and Cornell 2012; Lin 2014). They identified systems of staff recruitment and selection and training as key factors in shaping how care is provided (Hunter 2000; Castle and Enberg 2007; Yallowitz and Hofland 2008; Hyer et al. 2011; CQC 2014a). Except for a small number of exceptions, the relationships between job quality and care quality—and in particular the conditions under which job quality affects care provision—are less well documented. Eaton (2000) identified the mechanism that leads from a particular work-process design to specific quality outcomes for residents, highlighting that approaches to care in operation within the home are a factor affecting care quality. Cost-saving measures such as decreased staffing levels intensify workloads and affect staff capacity to provide quality care (Currie, Farsi, and MacLeod 2005). Eaton (2000) recommended what she named “bundled HR practices” (e.g., job security and team working) combined with person-centered care approaches as a combination likely to yield better care outcomes. She also cautioned that strong institutional forces resulting in low-wage, low-skill work systems are often directed against this combination. The bundle approach indicates the cumulative impact of overlapping factors, but it does not identify which dimensions of job quality may be crucial and in which context, and whether retaining particular components of job quality may compensate for the loss of others. Through our examination of the erosion to job quality in nursing homes using person-centered and custodial approaches to care, we map the relationship between the care culture and job quality to identify how and why these matter for care quality.
Our premise is that at a general level external financial cuts lead to cuts in labor costs. Because labor is the largest cost component in services such as nursing homes, it is a major target. These cuts lead to lower job quality because workers bear the brunt of the cutbacks. Lower job quality includes a) reduced rewards in the form of pay and benefits and b) fewer resources (reductions in staffing, longer working hours, and work intensification), less discretion, and fewer opportunities at work to provide decent care. Hence, lower job quality leads to poorer care because particular dimensions of job quality allow workers to provide better care.
Research Design
We undertook qualitative field research to develop a theoretical understanding of why care quality varied across nursing homes. We wanted to understand the mechanisms linking financial pressures from the external environment to the quality of jobs and the quality of care.
The context for this study was the post-financial crisis period when the UK government made major cuts in payments to nursing homes. From 2010, £1.17 billion was cut from grants paid by the government to local authorities (LAs) (Department for Communities and Local Government 2011). Approximately 49% of beds in nursing homes are publicly funded through LAs (Laing and Buisson 2014), and because of the cuts, the LAs reduced their funding of nursing homes by 5% in real terms, to a rate below the cost of providing care. This had a destabilizing effect on the UK nursing home market, leading many providers to seek ways to rapidly reduce their labor costs to remain viable (Laing and Buisson 2014). By 2014, 20 to 22% of nursing homes in England had insufficient staff on duty and falling quality of care (CQC 2014b). This can be viewed as an exogenous financial shock that all nursing homes faced, providing us with the opportunity to observe the variation in organizational responses.
From 2009 to 2012, we conducted fieldwork at 12 UK nursing homes providing long-term care for elderly people. 2 Nursing homes in the UK are registered to provide residential care, nursing care, or a mix of the two. The 12 nursing homes varied according to level of care (eight residential and four nursing), size (from 10- to 65-bed facilities), region, and ownership (for-profit and nonprofit care homes and chains) (Table 1). 3 None of these nursing homes had union contracts, and individual employee union membership was extremely low. In the UK care sector, the privatization and fragmentation of employment (because of the large number of workplaces, which are geographically dispersed and employ small numbers of people who work shifts) have posed increasing problems for trade union organizing, and membership over recent decades has diminished (Hardy, Eldring, and Schulten 2012).
Case Study Details
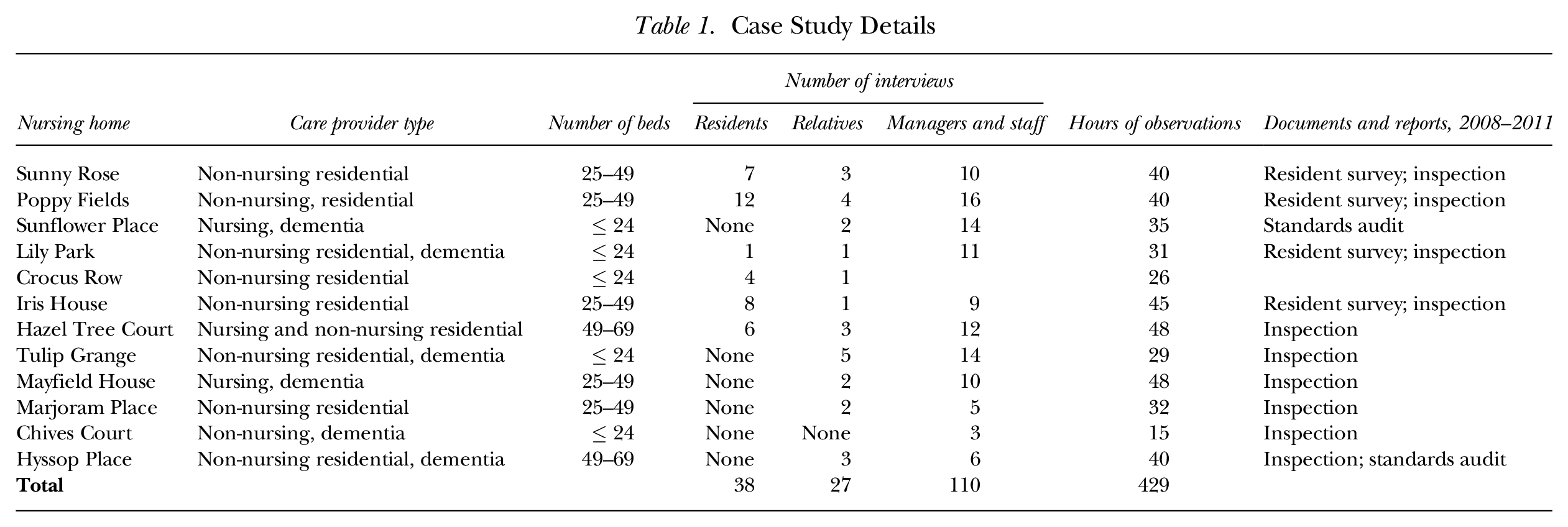
Our field research included repeated site visits to each home, interviews, and observation of daily activities. The visits to each home took place over four to six weeks. We completed 429 hours of observation of everyday activities, experiences, and practices during day and night shifts, both on weekdays and weekends. We conducted a total of 175 interviews: 110 with managers, registered nurses (RNs), and care assistants (CAs); 38 with residents; and 27 with relatives (Table 1). The interviews typically lasted between 30 and 60 minutes. Interviews with managers, RNs, and CAs asked about the nursing home’s approach to the provision of care, employees’ ability to carry out their work, and issues concerning the quality of care. Interviews with residents and relatives explored their experiences in the home and the quality of care. Secondary data, such as reports of annual resident surveys and copies of the national regulator’s annual inspection reports of care quality, were also analyzed. Our case studies focused on establishing an understanding of the relationship among the approach to care, job quality, and care quality.
To develop a theoretical understanding of the factors driving variations in care quality and the relationship between job and care quality, we drew on Eisenhardt and Graebnor’s (2007) method of systematic recursive cycling. We examined data from each nursing home to identify patterns in job and care quality, and followed this with comparative analysis across case data sets to generate a theory about the conditions under which job quality affects care quality.
Findings
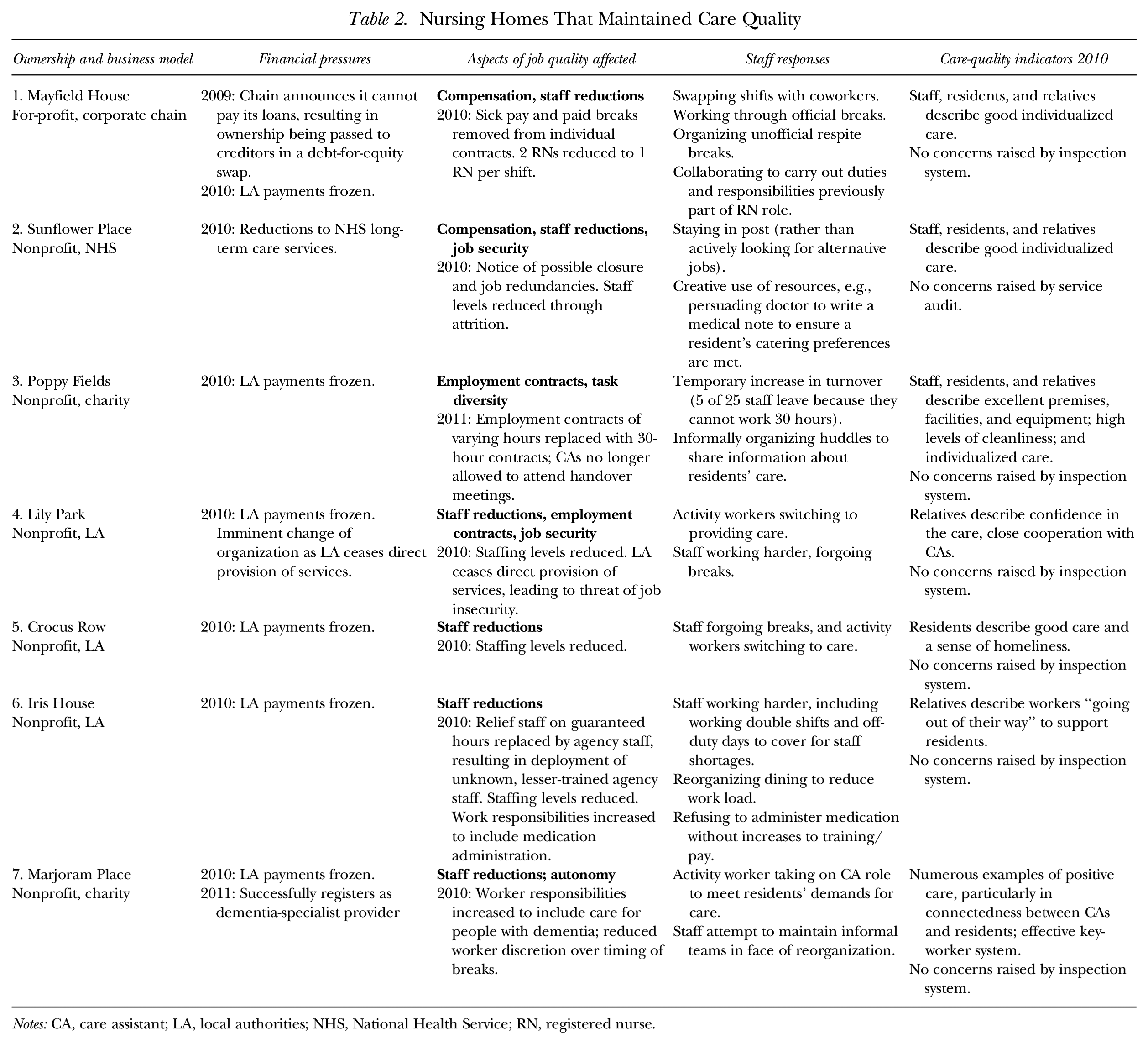
According to our findings, all 12 nursing homes faced ongoing and increasing financial pressures during the time of our study attributable to real term reductions in the LA payments, higher operating costs (rental payments, food, fuel, and a rise in minimum wage rates), and reductions in income because of falling occupancy rates. In response, all 12 nursing homes introduced broadly similar cost-saving measures (without involving union negotiations), including lower pay, fewer benefits, less provision of training, lower staffing levels, and changes in individual employment contracts and the skill mix. The majority of changes in employee contracts increased the number of working hours (e.g., changing 8-hour shifts to 12-hour shifts and/or increasing the weekly number of hours staff worked from fewer than 30 to 35 hours or more). Changes in skill mix included halving the number of RNs on duty during day shifts and replacing them with a senior CA. Although the changes introduced were similar across nursing homes, the care quality varied. Tables 2 and 3 summarize the relationship between job quality and care quality across the full sample of 12 cases. We argue that cost-saving measures negatively affected workers in all the nursing homes in that the quality of their jobs eroded; however, in seven homes, the care quality was maintained, and in five homes, it deteriorated. These effects were consistent with two contrasting patterns. Homes that were able to maintain quality care had adopted a person-centered approach to care, allowing workers the support they needed to maintain care quality despite the erosion in the quality of their jobs. By contrast, the homes in which care quality deteriorated had adopted a custodial approach to care that did not provide support to workers to maintain care quality as the quality of their jobs eroded.
Nursing Homes That Maintained Care Quality
Notes: CA, care assistant; LA, local authorities; NHS, National Health Service; RN, registered nurse.
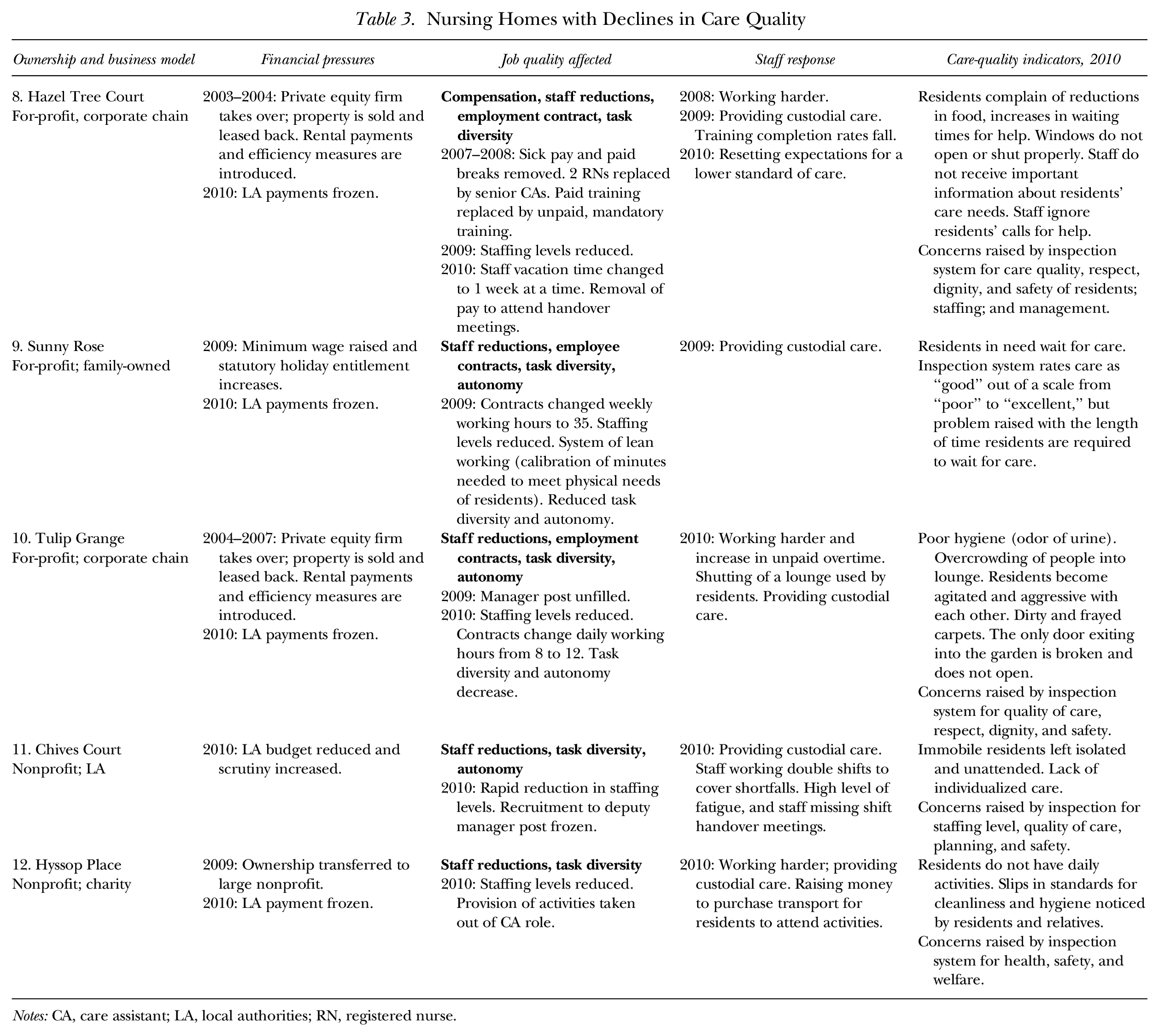
Nursing Homes with Declines in Care Quality
Notes: CA, care assistant; LA, local authorities; RN, registered nurse.
Maintaining Care Quality during Cutbacks
All seven homes in which the care quality was maintained had adopted a person-centered approach to care. One of these homes was for-profit and six were nonprofit (i.e., they were required only to break even rather than to make a profit). These nonprofit homes could draw down additional funding if financial shortfalls were predicted (e.g., for the charity-owned homes, through voluntary donations from the charity or for the LA-owned homes, from additional public funds to hire temporary agency workers to cover for regular staff who call in sick), but the for-profit home did not have this option. That this for-profit home was able to maintain care while increasing efficiency and cost savings suggests that a for-profit status alone is not an adequate explanation for poor care quality. In homes in which the care indicators (derived from regulator reports, interviews, and observations) confirm care quality was maintained, the introduction of cost-saving measures affected the RNs and CAs, but the staff responses to the changes protected the residents from the immediate effects of the cutbacks. Table 2 presents the details of the seven homes in which care quality was maintained, the financial pressures they faced, the components of job quality affected, the RNs’ and CAs’ responses to these changes, and the outcomes for residents’ care in these homes.
Cost-saving measures affected the employment contracts of RNs and CAs, reducing levels of compensation, intensifying staff workloads (as the staffing levels and/or skill mix was reduced), and introducing cheaper staff training (a shift from in-work classroom-based training to e-learning). In these homes, workers sought to protect residents from the effects of the eroded job quality. They reorganized work practices and routines, for example, by swapping shifts to cover for coworkers who were unable to work because of short-term illness or who needed short periods away from work to look after their children. They switched job roles (e.g., activity workers would switch to CA roles, and a receptionist would switch to provide residents with activities). They also worked through meal breaks, continued to work after their contracted hours were completed (a frequent occurrence), and arranged ways to share information (e.g., outside of the handover meetings 4 ). In these work-arounds, the care workers absorbed the effects of the erosion in job quality and protected residents from its adverse effects.
These nursing homes had several things in common. Person-centered care approaches were evident, and the homes were able to direct funds inward toward supporting the delivery of person-centered care. The person-centered care approach asserts the human value of residents, their individuality, and their unique personality and life experiences. It places importance on the perspectives and preferences of the residents and their relationships and interactions with others (Brooker 2004; Killett et al. 2016). Although the workers in these homes experienced reduced pay and/or increased workloads, other dimensions of job quality less related to labor costs were maintained, such as the ability of staff to voice their concerns, work flexibly, and have some control over how they carried out their jobs. Mayfield House is illustrative of this pattern, both in terms of the erosion in job quality and in workers’ responses.
In common with most UK nursing homes, Mayfield House faced ongoing and increasing financial pressures. This for-profit chain introduced cost-saving measures in 2009 to 2010. It reduced the skill mix (replacing one RN post on the day shift with a senior CA role) and made changes to individual employment contracts (removing sick pay and paid rest breaks) that reduced employee pay. For instance, previously wages included payment for breaks to compensate for breaks that were frequently shortened or were not taken to meet the needs of residents: They have changed a lot of things from when I started until now, there’s a difference. They used to pay for staff break times. A lot of companies are still paying for staff breaks. So that has meant salaries went down. Lots of things here are coming down, falling away. (Robin, RN)
Cuts in staffing and higher staff turnover intensified workloads for those who remained. Increases in staff turnover in 2010 (possibly in response to contractual changes regarding paid breaks and sick pay) reduced the pool of care workers available to work shifts. Consequently, staff worked longer shifts and more shifts at short notice or without notice: The work is hard. I am knackered. Sometimes, I go home, I have a shower, I’m in bed, and that’s my day. I get up again at 6 a.m. come back to work, go home, have a shower, go to bed. I do four shifts a week, 44 hours a week. But last week I did six days on the trot. Somebody was messing about with the rotations again, didn’t tell me what they’d done, and just left it to me to do them. Six days on the trot. I was not amused. I’ve been known to go home from here at 8 o’clock, one of the night shift haven’t turned in and they’ve rang me at 9 o’clock to come in and do a night shift as well. I didn’t do it, did I hell. I said “No way.” (Jane, CA)
Regardless of the direct effects that changes to pay and the intensification of workloads had for staff, the prospect of letting the changes to job quality “overlap into care” was unacceptable: But thankfully, in this setting it doesn’t affect our care towards our residents, you know. Because the minute it starts doing that you might as well walk out of your job because it isn’t their fault that “management,” shall we say, think it’s alright to treat their staff in this way and not respect or recognize what you’re doing. But the minute you start letting anything bother you, overlap into how you care, forget it, walk out the door, turn around and leave it because it’s not their fault. (Maureen, CA)
The high value workers placed on shielding residents from the effects of the cost-saving measures and the erosion of job quality is evident in the actions they took to protect residents. Informal arrangements were made to swap shifts with other coworkers, enabling workers to use their days off to recover from illness—a practice one CA identified as a person-centered way of treating each other: We treat each other in a PCC [person-centered care] way too. Someone is allowed to have set days off because they look after their grandkids on a Monday and Tuesday. We swap round shifts because someone’s kid is in a football match and your kid wants you there to watch them. If you are ill at the beginning of the week, someone will swap their shifts with you to later in the week, if it doesn’t upset the unit. (Maureen, CA)
As a result of these arrangements, on-duty staffing levels were unaffected (because absences were prevented) and staff did not lose any pay. An informal system to manage unexpected domestic emergencies enabled staff to leave the nursing home for short periods of time to attend to the needs of their children. Immediate temporary backup to care was provided by the office staff (receptionist, nursing home manager, and housekeeping) switching job roles. The response ensured that the number of staff available to provide direct care to residents was unaffected while also allowing in-job flexibility for staff to manage home and work demands.
Although the removal of pay for meal breaks affected pay levels, staff continued to work through their formal break times to ensure residents’ needs were met, as Jo, a CA, pointed out, “they stopped paying us for breaks, we don’t get paid for lunch yet we work through our breaks all the time.” Informal arrangements were also made for staff to stop working and leave the nursing home for short periods of respite: I formally have half an hour break. It’s up to me when I want to do it. But like today, I’ve had only 10 minutes because it’s so busy. There’s always something. But then I might need to take a breather away from care. I’ll just turn round and say “oh I need to go out.” And that’s a good thing as well, if any one of us feels that feeling of being overwhelmed, we’ll just say “oh can you just step in a minute, I just need a few minutes.” Everybody says “yeah, go on, get out.” (Julie, CA)
Although changes to the employment contracts and staffing levels directly affected pay and intensified workloads, staff were able to retain some control over how they cared for residents. Staff continued to be paid to come into work 15 minutes early for the handover meetings. Moreover, the particular approach used by management in structuring the handover meetings enabled CAs to participate in discussions about the care needs of residents and their care planning: Staff come in for 15 minutes before shift for a handover, and this is paid time. We go through every single resident, and there are 5, 6, 7 members of staff at the handover, all throwing ideas around on how to do things for each of the residents. . . . A resident on pain relieving medication was very unsettled, walking around a lot, which in turn seemed to be contributing to more pain. The doctor had advised that the pain relieving medication could cause physical agitation, so I took this to the handover and the team discussed it, deciding to reduce the medication to see if this would reduce the unsettled behavior. (Mayfield manager)
Listening to others, informing, discussing, and taking action were common practices undertaken throughout the home. An independent inspection of the services at this home in 2010 rated the quality of care as “Excellent” (on a rating scale from “Poor” to “Excellent”): Staff and residents/relatives would be confident that their concerns would be listened to and acted upon. Staff know their responsibilities in passing on any concerns which affect the safety and vulnerability of people. It was evident that the manager takes positive action to improve the quality of life of people who live at the home, often as a result of listening to what people who use the service have to say. (Extract from National Regulator’s Inspection Report 2010)
In addition, family members remarked on the highly individualized and tailored care residents received in the home: One thing that I like, and I’ve been involved with on two occasions is using the hoist. So that’s involved four care assistants and on both occasions they were informing Arthur all the time what they were doing and how it would feel, and constantly reassuring him that he was safe. Instead of just saying “right that’s it, you’re on” which is very important. . . . Just the ambience and the sense of care, and the friendship, and you never get a sense from anybody at all that they’re only doing a job. I mean Patrick, he’s a senior cleaner. He knows all the residents by name, he talks to them, knows their interests. He doesn’t have to do that he could just come in and do that cleaning job. He doesn’t, and none of the staff do. (Pauline, resident’s wife) I think the care is excellent. They’re kept clean, they’re changed regularly, they are very well fed. They give them a good quality of life as best as possible. My husband loves a bath and they bathe him regularly because they said he enjoys it so much. I don’t think he could get any better to be honest. (Michele, resident’s wife)
Notwithstanding the effects of cutbacks on employment contracts, compensation, and workload, the remaining job quality, namely autonomy and flexibility, enabled workers to create work-arounds to protect residents and help stabilize the provision of service during a difficult period.
The pattern of staff using their creativity to overcome declining job quality and prevent spillover to residents’ care was evident in all seven of these nursing homes. Staff in each nursing home collaborated to absorb the effects of job-quality erosion and limit the spillover into care using various strategies. For example, to ensure that feeding and nutrition needs were met during periods of reduced staffing, CAs at Iris House arranged for residents not to go to the designated dining room because it was deemed as potentially unsafe to take them. Instead, they gave residents individually prepared trays of food in their private room or in one of the lounge areas, a practice staff referred to as “residents’ lap tea.” At Sunflower Place, cutbacks had reduced the availability of food at the hospital where the unit was located, leading to a limited choice and concerns about one resident who was not eating enough food. In response, workers persuaded the doctor overseeing the unit to write a medical note to the catering manager requiring that the resident be provided with food he liked, in this case, sausages. In another instance, CAs at Poppy Fields were no longer allowed to attend the handover meetings, and they realized that their knowledge about the individual needs of residents was not reaching decision makers. In response they employed a strategy of huddling together to share information and to discuss which parts of the workload each would do. At Lily Park, when staffing levels were unexpectedly low, CAs worked through their official meal breaks and switched job roles. People contracted to provide residents with activities switched to the CA role. In these homes, enough job quality remained to enable staff to arrange work-arounds and protect residents. In contrast to the patterns found in these seven homes, in the other nursing homes, the effects of cutbacks spilled over into care.
Falling Care Quality during Cutbacks
The deterioration in job quality spilled over into poorer care in five of the nursing homes that we studied (three for-profit and two nonprofit). These homes experienced greater exposures to the effects of cuts in LA payments (i.e., a fall in real income), and they operated without the benefit of additional income streams (this includes both the charity and LA homes). Although similar components of job quality were affected in these five homes as in the previous seven homes, workers did not maintain the prior level of care; rather, they made adjustments that undermined the quality of care, with detrimental effects for residents. For example, care practices shifted toward meeting only the physical needs of the residents, becoming increasingly custodial or omitting care altogether. In each case, care workers responded to the poor working conditions and the reduced staffing levels by cutting back on care. Table 3 provides the details for the five nursing homes in which care quality fell, the financial pressures they faced, the components of job quality affected, RNs’ and CAs’ responses to these changes, and the care outcomes for residents.
The homes in which care quality fell had several things in common. A custodial approach to care was evident in these homes, and management prioritized financial cutbacks over individualized care. At these homes, workers tended to approach care as a series of tasks to be completed. A lack of spending on maintenance and other facilities was visible in some of these homes: broken equipment (wheelchairs and hoists), windows and doors that would either not open or not shut, and frayed and dirty carpeting. We argue the combination of the erosion in job quality, a custodial approach to care, and the lack of spending on essential maintenance and upkeep impeded the ability of workers to provide quality care. In the homes in which financial cutbacks had severely eroded job quality, workers were less able to voice their concerns or to arrange ways to work around the cutbacks. Instead, the cutbacks spilled over into poor care as workers reduced the time they spent with each resident and the amount of care they provided. Hazel Tree Court is illustrative of this pattern in terms of the erosion in job quality, how workers responded to these changes, and the effects on residents.
Hazel Tree Court faced prolonged and intense financial pressures following the freezing of the care payments by the LA and the increases to the cost of running the home. The company owning the chain had been sold to a private equity firm in 2003–2004, which immediately sold the home’s real estate and required the home to lease back the property the chain once owned. Private equity firms typically buy out a company and use various financial strategies, including sale–lease back and cutbacks in spending, to extract value and cash from the business and to pay themselves and their investors large dividends (Appelbaum and Batt 2014). Indeed, the private equity firm owning the nursing home reported spending the profits from sale–lease back deals to expand the business rather than reinvesting them in the nursing homes. At the time of our research in 2010, high rental fees coupled with the freeze in the level of income from the LA had further intensified the financial pressures facing Hazel Tree Court, and management had introduced cutbacks in the catering, maintenance, and staffing budgets. The number of staff available per resident fell from a ratio of 8:30 (2 RNs and 6 CAs) in 2008 to 4:30 (1 RN and 3 CAs) in 2010. Researchers’ observations confirmed that staffing levels frequently fell below the official ratio claimed by the home to 3:30 (1 RN and 2 CAs); consequently, staff regularly “worked short staffed”: We’ve worked short staffed, on many occasions. We’ve got through it but it’s been very hard. When it’s been snowing and staff can’t get into work, I’ve stayed overnight to help and then done a day shift on top. Well we’ve got to because there’s nobody to work. I could have just gone if I wanted but I didn’t. When the home has been short I can do 5, 6, 7 twelve-hour shifts at a time. (Janice, CA)
Further cutbacks froze workers’ pay, and managers were under pressure not to hire temporary agency workers to cover staff shortages: This year we got the notice that nobody was getting a pay raise. Yesterday we had to have an agency care assistant because I’ve got two people off sick. The company never directly say no to get an agency worker in. But then you get shouted at, you are asked why you are over your budget by this much? Why have you had to have this and what are you doing about it? (Hazel Tree Court Manager)
The severity of cutbacks to staffing levels and skill mix (2 RNs were replaced with 2 senior CAs) affected the way in which the RNs and CAs carried out their jobs. As a consequence of halving the number of RNs, the RN role intensified to include the responsibilities and duties normally undertaken by 2 RNs, with detrimental consequences for the supervision of care workers and the safety of residents: Before with the other company there would be one nurse who would do the medication and the doctor’s appointments; and the other nurse would work with the CAs. They would look after the CAs and oversee what they are doing. During that time there was fewer mistakes with the drugs. Now the nurses make mistakes with the drugs. We wear a red apron that says do not disturb. But people do. (Andrew, RN)
RNs attempted to manage the effects of the cutbacks, particularly the reduction in time available to supervise CAs, by organizing the staff rotations to make sure experienced care workers were on each shift. This was not always possible, however, leaving “a weak team,” that could not care properly for residents: As a trained nurse I supervise the CAs, I want a skill-mix on a shift but it is not always possible to plan for this in the staff rotation. Sometimes, I’ve got a weak team and I have to keep an eye on them and check their care. If there is a weak team you’ve got to be alert. I wouldn’t say abused, but I would say it is easy for them to miss out on care. (Rachael, RN)
In common with all the nursing homes, measures were introduced to end paid time for meal breaks, even though staff did not take formal breaks: The other company that owned the home had to pay us for our break times and for handover report time. This company took that away. I have a contract from the old company on-going here. They don’t pay me the handover time but they have kept my pay for breaks. I can’t take my breaks anyway. I sit and eat here in the office, while I work. (Andrew, RN)
While RNs had an option to eat food at their desk if they were unable to take a meal break, CAs’ breaks were structured throughout the 12-hour shift and could be taken as either two 15-minute or one 30-minute break period. If they were able to take a break, getting to the staff room, preparing food, eating and drinking, and returning to the floor where they worked within the designated 15 minutes was difficult to achieve: Sometimes you don’t get a break at all and that is the truth. Even if you do take a break, you’re back up on your feet within minutes. You’re allowed half an hour during the 12 hour shift. Or you can take up to 15 minutes in the morning and 15 minutes in the afternoon. By the time you’ve got to the staff room and you’ve rushed your food down, you’re rushing back on the floor and running about. This is why I always have a drink up here. We are not supposed to but I do because it’s very hard work and it’s hot in the home, you need to drink all the time. But they said you’re not supposed to sit with the residents and have a drink. I don’t see there’s any harm in that because it also helps the residents to drink fluids too if you’re sat with them talking to them. (Claire, CA)
The cutbacks to staffing levels and reduction in skill mix, in combination with a custodial approach to care, such as structuring when workers took their formal break and not allowing informal breaks, limited the workers’ potential to develop work-arounds. Instead, frontline care was organized to meet management’s rather than the residents’ needs and preferences. In this context, the custodial approach to care, focusing on meeting only the basic physical needs of residents, inhibited the workers’ autonomy, which would have allowed them to decide (with the residents) how individual care might be provided.
The withdrawal of paid time for the handover meetings also had the effect of reducing the CAs’ autonomy. RNs continued to start work and remain on duty for 15 minutes before and after their shift (although now unpaid). But CAs were now absent from the handover meetings. Instead, RNs passed essential information about the care needs of residents individually to the CAs while they were working on the floor. This information was limited to “major” items: Handovers used to be quite brief and general but I think if there’s something major like a person’s not been well and you need to check on this person then it’s told to you. But the staffing level is wrong for residents because if you can’t see to them quickly it can cause incontinence. Sometimes you can’t get back to them because you have to deal with somebody else and other staff are dealing with somebody too. Dealing with that it’s horrible. The residents need to be looked after properly. You are having to turn residents every two hours but when you’re turning them they also need changing, you can’t just turn them and get away with it, they need more of your time. (Janice, CA)
Communicating residents’ care needs in this way was not sufficient to enable CAs to provide enough care. The CAs acknowledged that residents did not receive the care they needed, and in response, they tried to work faster when they could. This did not work, but neither did the alternative—meeting the essential needs of one resident at a time, leaving other residents in need. A double bind resulted, which CAs found distressing.
Financial cutbacks had eroded job quality to the extent that little flexibility remained and the effects were felt by residents and spilled over into impoverished care in the following ways. First, cutbacks in the catering budget depleted the quantity, timing, and availability of food: The lunch is good and it’s well cooked and plated. But then the teatime meal is at 4 o’clock in the afternoon. It’s the last food you have until next morning and all you have are sandwiches. How many sandwiches would you need to satisfy the hunger pangs when you go without food between half past four one afternoon and half past eight the next morning; its soul destroying. (Barbara, resident)
Next, understaffing affected interactions between the staff and residents: It’s recorded that sometimes they’re so understaffed they haven’t time to communicate with you, that’s one of the main things I have against the home they’re very understaffed. My Aunt, she’s paying the whole of the fee herself. So it’s a lot of money every week for quite a small service. (Annette, relative).
And understaffing affected the quality of personal care: I didn’t feel right, she [the CA] didn’t get me washed properly and I felt dirty, you know, its loss of dignity, love. (Lilly, resident).
Basic care routines were hurried and impoverished. A shift in the management of frontline care work toward the en masse treatment of residents (set times for meals, getting up and going to bed, toileting, and activities) highlighted the lack of control residents had over their schedules. Workers moved residents into the dining room as soon as they were up, washed, and dressed. As a result residents were seated up to 90 minutes before breakfast was served. In the evenings, CAs pressed residents to get into bed at times that suited the workload of staff: They expect you to go to bed early and stay asleep all through the night. The night shift starts at half past seven. When it gets to half past eight, the CAs they’ve been in to my room about ten times to ask “are you ready to go to bed?” I say “no”; they say “why not?” It’s because I don’t feel ready to go to bed. End of story. (Annie, resident)
The Tipping Point—How the Low Quality of Jobs Spills over into Poor Care
In the case of Hazel Tree Court, the negative effects of financial cutbacks on the quality of jobs was much more severe than in the first group of seven homes, allowing staff few resources or opportunities to develop workarounds and little motivation to do so as well. The company cut back workers’ pay to the minimum statutory levels (workers’ weekly take home pay was reduced when paid breaks were eliminated), reduced the allowed breaks of 30 minutes in a 12-hour period (under Working Regulations 1988, the minimum a worker is entitled to is an uninterrupted break of 20 minutes when the daily working time is more than six hours; Legislation.gov.uk. 1998), and reduced the staff to levels deemed unsafe by national regulators. Workloads increased, and the staff had little ability to effect change and little autonomy in making decisions about how to care for residents. Rather, the view shared among staff was that poor care was unavoidable.
In addition, the establishment of rules by management preventing staff from adapting care to meet the residents’ needs (e.g., staff were forbidden to drink fluids with residents, even though doing so would encourage residents to increase their fluid intake) reduced worker autonomy and disempowered both workers and residents from making decisions about care. Residents had to fit in with the extant care routines: to sit in the dining room 90 minutes before meals were served (to reduce the time spent handling and moving residents), to go to bed when staff said to (so staff could complete a long list of domestic tasks during the night), and to not complain if they were not washed properly or were hungry. The nursing home workers blamed the residents and relatives for expecting too much: I was talking to three CAs as they stood together in the corridor this afternoon. They were waiting for a resident who would need their assistance. We talked about the difficult aspects of their job. One CA (who has worked here for over 8 years) said “the hardest thing can be the relatives.”“They come in and pick holes in what you have done for the resident, their expectations are too high.” (field note observation)
At one point, one of the researchers informed a manager about poor care practices we had observed. Rather than dealing with the problem, the manager blamed the resident for expecting “hotel” care: I went into the office to let the manager know I had arrived. She brought the subject around to the resident I had spoken to her about in confidence. When I reported the poor care to the manager yesterday she said she was going to talk to the resident involved and not in a way that would make the resident feel uncomfortable. She said she would do one of her “walk rounds” where she speaks to each resident and asks how they are and if there are any things she should know about. But today the manager said that “Mrs Beecham expects too much, we can’t cater for the wants of every individual, we can’t provide special treatment.” The administrator joined in saying “she can’t have hotel-level care.” (field note observation)
Complaints about poor care were translated by management to mean that residents had unrealistic expectations about the level of care they might receive: I have made efforts to remind CAs they are here for the resident, you know, I remind them of what they are supposed to do and that they just have to do it. Some care staff I have spoken to, have gone to the manager and complained about what I have said to them. What I get back from the manager is “ah you’re getting like them [the residents and relatives who complain].” (Rachel, RN)
The erosion of job quality left scant resources and few opportunities for staff to develop work-arounds to provide better care—and the custodial approach discouraged them from doing so. Instead, care practices were instituted to deal with residents en masse rather than as individuals, and the resulting hurried treatment of residents did nothing to improve the diminishing quality of care. In contrast to the patient-centered approach, custodial approaches tolerated poor care by blaming the residents for being unrealistic and by dismissing worker concerns. The organization was unconcerned about the residents as individuals, and the workers could not protect them.
CAs were aware of the double bind they faced in their jobs as they attempted to meet both the specific individual needs of residents and expediently carry out care as encouraged by the custodial approach, but were unable to effect change. This resulted in a poor standard of care for residents, which led to residents and relatives voicing their concerns, which led to managements’ redefining these complaints as unrealistic expectations. Thus, poor care was tolerated and care standards were allowed to decline. In effect, the relation between job quality and care quality had reached a tipping point at which spiraling declines in care occurred.
This pattern of spillover from depleted resources and the declining job quality into poor care was evident at all five of these nursing homes (Table 3). Although staff initially tried to absorb the effects of the cutbacks, they were unable to develop work-arounds to protect the residents. For example, in Hyssop Place and Tulip Grange, staff worked unpaid hours to supplement the low staffing levels. Workers at Hyssop Place organized a fundraising drive to continue activities for residents when the owners removed this service. Despite these efforts, in all five homes workers were unable to prevent the fall in care quality following the cutbacks. In Tulip Grange, for example, CAs and managers wrestled unsuccessfully to turn around the decline in quality of care (rated “Poor” by inspectors in 2010) by working additional shifts and unpaid overtime to cover staff vacancies and staff absences. After three months, however, workers became highly task focused in their approach; they closed areas of the home previously used by residents and put residents in one communal sitting room, where they could watch them while also writing up care records. In effect, care became custodial. Similarly in Chives Court, staff often worked double shifts in an attempt to maintain staffing levels and quality of care; however, the results were high levels of fatigue among the staff, en masse treatment of residents, and immobile residents being isolated and unattended for long periods. Depleted job quality spilled over into care. The cutbacks eroded the job quality needed for quality of care and fundamentally changed the purpose of the job from care to task completion, resulting in impoverished care.
Conclusion
As we have demonstrated with these findings, all 12 homes experienced an external financial shock, which was severe in the first group of homes but far worse in the second group. All homes responded by cutting labor costs, and this led to a deterioration in job quality across the board, with job quality deteriorating more in the second set of homes than in the first. The dimensions of job quality that affected workers’ ability to protect residents from spillover effects were reductions in staffing, longer working hours, and work intensification. Although pay was important to workers, the indirect effects of the pay cuts—lower staffing and longer working hours—more directly affected their ability to maintain quality of care.
The two approaches to care, patient-centered and custodial, differentiated the care-quality outcomes. Management in the first set of homes had adopted a person-centered approach to care and encouraged workers to do the same. As a result, workers embraced the approach and developed workarounds to protect residents from the spillover effects of the cutbacks. In these homes, enough job quality remained to enable workers to develop shift and/or job-role swapping and ensure the usual staff-to-resident ratios remained unchanged. By forgoing breaks, workers were able to meet care needs. In addition, if staffing levels fell below the home’s own ratio, resources were available to bring in agency workers. As a result the quality of care was maintained.
Management in the second set of homes had adopted a custodial approach to care. Faced with financial strains, management reduced labor costs, which led to a deterioration in job quality. Cutbacks to lower labor costs (including resources that managers could use to hire agency workers) reduced staffing levels still further, pared down pay and working conditions to statutory minimum levels, and increased the level of work intensification. The effects of the cutbacks were so severe that workers did not have the time or resources to protect residents or maintain prior levels of care. As a result of this cost cutting, frontline care work was reorganized using predetermined schedules for meeting the hygiene, nutrition, and toileting needs of residents. The dearth of resources available and low job quality, combined with a custodial care approach, failed to provide workers with the dimensions of job quality they needed to determine how to provide care—leading to a spillover into impoverished care. In some of these homes, management also cut back on care services beyond the control of workers, such as food and repairs. The workers could not protect residents from the effects of these cutbacks, and the quality of care declined. Custodial approaches to care adopted by management and staff included blaming the residents, so that resident complaints were interpreted as resulting from residents’ own unreasonable expectations, not the deterioration in care quality.
Our findings go beyond previous research that linked care quality to job quality (e.g., Eaton 2000; Yallowitz and Hofland 2008; Avgar et al. 2011) to indicate that the dimensions of job quality that suffer most during times of financial cutbacks are the ones that matter most for quality of care. The spillover effects from the erosion of job quality into poor quality care resulted in nursing homes in which workers were unable to develop work-arounds. As shown here, lower job quality can be mitigated by employees’ workarounds and using resources to meet the demand for care. Initially, care quality can be maintained in the face of cutbacks to lower labor costs through a person-centered approach to care that allows workers more autonomy and flexibility in determining how to provide care.
Footnotes
Acknowledgements
We thank the editors of the special issue, Rosemary Batt, and our colleagues Dermot Breslin, Jason Heyes, Jonah Earl, Rachael Finn, and John Hassard for their helpful comments on earlier versions of this article. This research was funded through the Prevention of Abuse and Neglect in the Institutional Care of Older Adults (PANICOA) program by the Department of Health and Comic Relief UK. The views expressed in this article are those of the authors and do not necessarily reflect those of the Department of Health or of Comic Relief UK. We gratefully acknowledge the collaboration with Alison Bowes, Dawn Brooker, Jenny La Fontaine, Richard Gray, Fiona Kelly, Isabelle Latham, Martin O’Neill, Fiona Poland, and Mike Wilson and the advice of Bridget Penhale and thank the residents, relatives, and care home staff who took part in the projects.
1
In keeping with international terminology, in this article we use the term nursing home when referring to long-term residential care of the elderly, instead of the term care home, more commonly used in the United Kingdom.
2
Approval was gained from the appropriate ethical review committees.
3
All names of homes and people used here are pseudonyms.
4
The handover meeting is when information about residents’ needs is transferred from the workers about to end their shift to the incoming group of workers to allow immediate continuity of care.