
Abstract
The world today is battling to being free from the shackles of Covid-19. The unexpected health emergency has left many nations halted and continues to pose a major challenge with newer strains of the coronavirus disease. The international community is coming forward for cooperative strategies in managing the epidemic, sharing innovations and vaccine development. In India, the government had been quick and responsive in controlling the spread of deadly Covid-19 since the first case was detected in late January 2020. The governments took many initiatives at all levels—Union, state and local. There is enough evidence to prove that the states have done fairly well by institutionalising responses to manage the spread of the virus. Rajasthan, Kerala and Madhya Pradesh are examples of the states that have devised and articulated policies to get hold of the crisis.
This article deals with the institutional arrangements adopted by the Government of Rajasthan and its widely appreciated Bhilwara and Ramganj models. The article also discusses the enactment of various legislations intended at seizing the spread of the virus.
Understanding the Covid-19 Pandemic in Rajasthan
The governments across the world have the task of developing, regulating and providing public goods and services. Today, the world is confronting grave challenges caused by the outbreak of Covid-19. The matter of contestation remains whether it is a human-made or a natural disaster, and debates on theories attributing the origin and virus spread have acquired spaces in international spheres. However, the crisis has provided the global community with greater cooperation and coordination for saving the mankind. There are instances where nations are working together to explore the causes, prevention and vaccines for the Covid-19. The government plays a pivotal role in managing epidemics as it is expected to be prepared and proactive in responding to any health hazard. The growing uncertainty of future and the increasing number of natural disasters have reoriented the government towards financing health, education and environment to ensure viability and sustainability. The government’s responsibility in any disease outbreak includes providing institutional arrangements, policies, infrastructures, contingent and resource planning and so on (Kauzya & Niland, 2020). During the epidemics, the governments perform activities in three crucial fields: leadership, health sector and non-health sector (WHO, 2009).
So far as leadership is concerned, the government acts as the natural leader tasked with identifying, appointing and leading the coordinating body responsible for pandemic preparedness, enacting new legislation and policies, or modifying the existing ones. It prioritises and guides the allocation of resources for achieving desired outcomes. The government provides for additional resources, both men and material, to mitigate the impact of the epidemic in the country and extends help to other countries. In the health sector, the government shoulders the responsibility to raise awareness among the citizens about the epidemic, associated risks, prevention and related positive initiatives. It needs to provide a strong containment strategy to prevent the spread, continue providing healthcare for the infected and those with co-morbidities. The protection of, and support to, healthcare workers becomes a priority of the government. Besides, there are non-health sectors where the government has to ensure uninterrupted delivery of public goods and services and implement policies for the citizens’ economic, social and psychological well-being (Pareek & Sole, 2020).
The initial cases of Covid-19 in India were reported by the end of January 2020. While, in Rajasthan, the first case was reported a month later on 2 March 2020. The state emerged as the region with many hotspots and the sudden reduction in the number of active cases reported and discharged. The state has reported around 3.12 lakh total Covid cases with 2,727 fatalities and a recovery index of around 97% until 8 January 2021. The state reported that the doubling time had increased to 214 days for active cases (PTI, 2020). It also occupied the first rank in the Covid-19 management index for ten states (Iqbal, 2020). The government’s prompt measures to contain the spread of the virus and some of the strategies adopted gained wide appraisal nationally and internationally.
Additionally, there were many executive orders by the state government to prevent the contagion. The guidelines issued by the National Disaster Management Authority (NDMA) mandated the constitution of district-level taskforces to coordinate administration and containment efforts during the Covid-imposed lockdown. It gave the authority to the district administration for handling the epidemic. The Government of Rajasthan has also planned and executed these relief measures at the district level to achieve the desired ends of preventing the spread of the virus. The article may serve as a foundation for future studies into how governments have responded to the Covid-19 pandemic and developed innovative, context-specific models to manage the impact of the crisis and develop strategies for managing any such outbreak in the future.
Methodology
The objective of the article is to highlight the institutional mechanisms developed by the Government of Rajasthan in response to the Covid-19 pandemic. The article discusses the Bhilwara model, the Ramganj model and other innovative measures put in place to control the situation in the places that became initial hotspots in the spread of the virus in the state. The article concludes with a critical appraisal of the existing measures and the suggestions that could be adopted as long-term strategies to contain the spread of the deadly virus.
This is a qualitative study where the available literature has been systematically analysed to find the results. The content analysis method has been used. As this is a review of literature article, secondary data sources such as books, journal articles and newspaper reports have been extensively used to collect data. The article would help understand the challenges before any government in general during a disease outbreak, measures to be taken in case of any virus outbreak, analysing the steps taken by the Government of Rajasthan and its administrative pro-activeness.
Glocal Perspective: Localised Response Strategy with Global Orientation
‘Glocal’ here refers to the localised planning with a global outlook. The strategies adopted in Rajasthan have been formulated and implemented at the local level, either district or area-specific. However, the orientation of strategies was global in outlook and scope. There are three ways of looking at any model developed so far: preparedness, response and success in achieving defined objectives. The administration at Central, state and local levels was least prepared as the virus outbreak was on such a massive scale that it was not anticipated. The local administration, being embedded in the local setting, had a better understanding of local problems and the local community’s needs and challenges of policy formulation and implementation (Munoz et al., 2017). The local administration, being aware of existing resources, is better at optimal utilisation, risk assessment and decision-making (Col, 2007). The local governments respond to public needs urgently and are perceived as immediate and legitimate authorities to carry out government functioning (Manor, 1999). The past experiences with epidemic management help the local administrators to formulate models meeting the local needs.
Planning at the local level can help achieve development objectives and mitigate the impact of epidemics (Rondinelli et al., 1983). There is evidence that district and local administration can effectively manage climate change and develop adaptation among the local community (Vogel & Henstra, 2015). Localised planning and implementation help build social capital and add value to society (Warner, 2001). The knowledge of socio-demographic structures, local culture, remotely available resources at the disposal and so on shape the modelled strategies for managing an epidemic in a local area. These models can be adopted in various places with similar environmental contexts as well as different contexts with modification and customisation based on the local needs and challenges, without the one-size-fits-all approach. The flexibility of these models helps adaptation even in other nations.
The models developed in Rajasthan and other states such as Kerala and Madhya Pradesh are formulated keeping in view the local factors and their success ensured adaptation in global contexts. These models’ success can only be assured when the stakeholders participate and facilitate by complying with established rules (Lakshminarayanan, 2011). Three Indian states—Rajasthan, Kerala and Odisha—with relatively low health infrastructure, poverty and moderate state capacity have done relatively well in controlling the Covid-19 epidemic with a rapid and vigorous response through localised planning (Dutta & Fischer, 2020). The reflections from these states suggest that the pursuit of making states and districts Covid-free enabled the development of widely appreciated models. The following section provides insights into the measures taken by the Government of Rajasthan and models developed like the Bhilwara model, the Ramganj model and other related responses. Chief Minister Ashok Gehlot has appreciated the role played by the civil society organisations during the pandemic. He asserted that, at the local level, the civil societies have created synergies with the state governments in the fight against coronavirus disease (Outlook, 2020).
The Bhilwara Model
Bhilwara emerged as one of the first hotspots for Covid-19 super spread in the state. The district became the epicentre of an outbreak as soon as the first case of a doctor in Brijesh Bangar Hospital was confirmed and was alone responsible for transmission to the patients and hospital staff therein. The possibility of an outbreak made Bhilwara referred to as Wuhan and Italy of Rajasthan (Bhatt, 2020). The district administration estimated that a significant population could have been infected with the virus and imposed strict curfew within an hour of detecting the first Covid-19 positive case (Hindustan Times, 2020a). For this, a ruthless containment strategy and testing had been devised to track the people who possibly came in contact with the doctor, hospital staff and the patients. The Bhilwara model had been appreciated by Prime Minister Narendra Modi and Cabinet Secretary Rajeev Gauba, suggesting its implementation in the entire nation. The Bhilwara model operated on six pillars of cluster containment (Figure 1) (Meghwal et al., 2020).
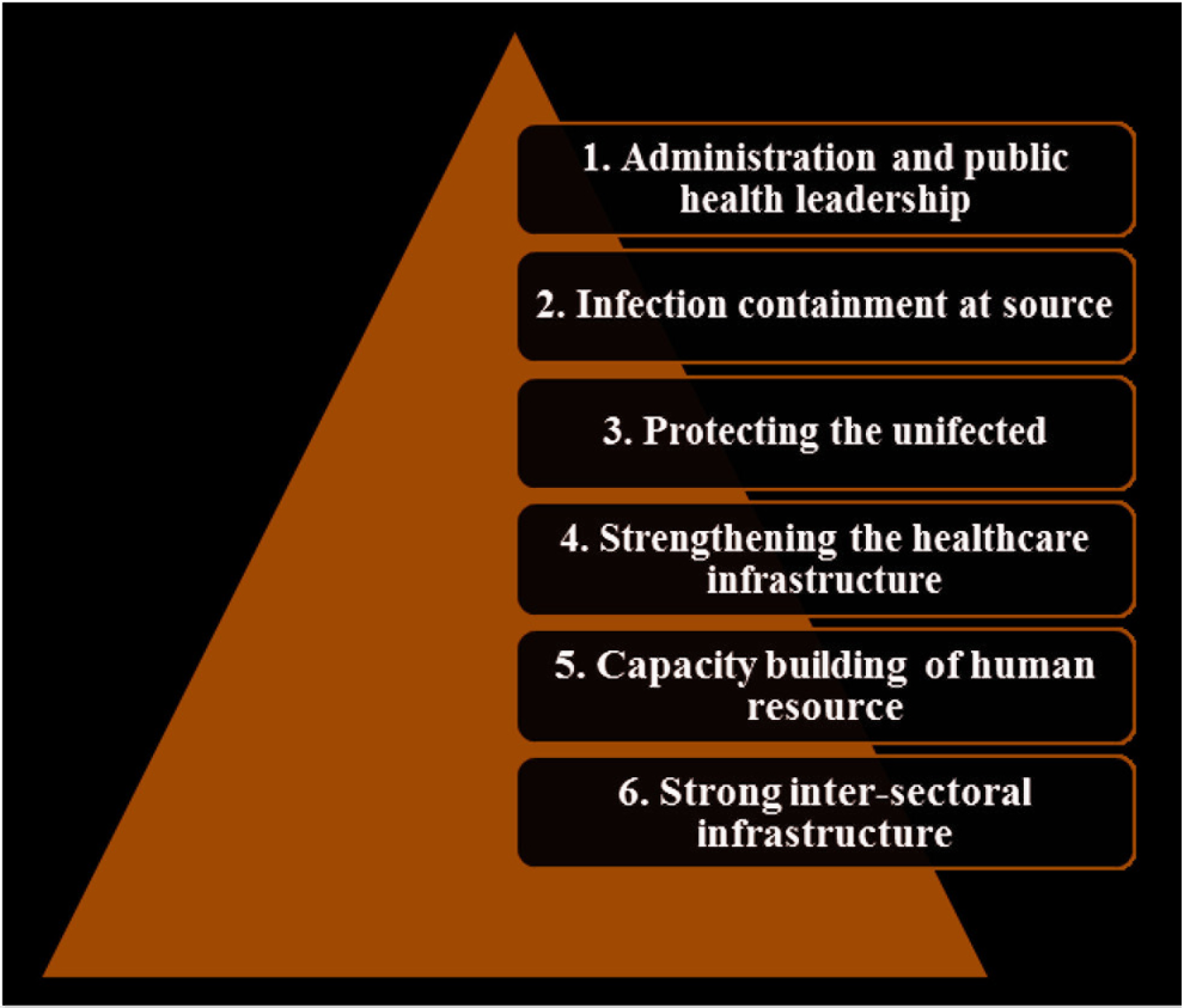
Administration and public health leadership is the first pillar of the cluster containment strategy adopted in Bhilwara. The measures taken under this pillar included leadership role of the office of district collector in mobilising health experts and rapid response teams. The objective of setting health teams was to conduct mapping of the entire district and provide inputs in designing the containment plan. The second pillar was infection containment at source which included sealing the Bangar Hospital, tracing, screening and isolating the people who were at the high risk of transmission. The third pillar was protecting the uninfected by active door-to-door surveillance, curfew in the city, sealing borders and movement through any public transportation and disinfection of the city. The fourth pillar was strengthening healthcare infrastructure, which included maintaining isolation and treatment facilities for mild patients in one group and moderate to severe patients in another. The district hospital was converted into a Covid Care Centre; the number of beds were increased with medical attendants and increased testing. The fifth pillar was capacity building of human resources, including training medical, paramedical staff and administrative personnel, establishing control room, regular monitoring and review by the district collector. The last pillar was strong inter-sectoral coordination, including sound and robust teamwork for administrative coordination and making compliance with the state plan mandatory. The various measures taken under these pillars are discussed below in detail.
As soon as the number of infected cases shot up, the district administration and the state’s health department became very active. A war-footing plan for ruthless-containment included isolating the district, mapping the hotspots within the disrict, massive door-to-door screening, aggressive contact tracing, home and institutional quarantine and isolation wards (Safoora, 2020). They constituted 3,000 teams for conducting a door-to-door survey in three phases at the city level and in two phases at the rural level. In the first phase, 850 teams surveyed around 56,025 households with 280,937 people (Mukherjee, 2020). The medical teams consisted of doctors, nurses, midwives, auxiliary nurses and nursing students to carry out the survey. About 7,000 people with influenza-like symptoms and travel history were asked to home quarantine. An intense contact tracing was conducted, and detailed charts of all those who came in contact with Covid-19-infected patients were prepared. In the last week of March, around 30 lakh households were intensely surveyed, and the district did not report any new case on 31 March 2020. The survey exercise was repeated after a few days to check new cases and symptomatic people if any. The sub-divisional magistrate of Bhilwara, associated with the formulation and implementation of Bhilwara model, the topper of the Union Public Service Commission exam and an Indian Administrative Service (IAS) officer of the 2016 Batch, Tina Dabi, said that the pandemic gave the best opportunity in her career to serve the citizens at large: ‘We just had one mission in mind, just one target that we just need to stop it, we were sitting on a timebomb, where it could spread and reach any number. It was actually a possibility of massive community spreading’ (Hindustan Times, 2020a).
A total and strict lockdown was imposed in the district, and the local police were given the responsibility to ensure strict compliance to its regulations. Additionally, the local police were also responsible for ensuring the supply of essential goods and services such as medicines, fruits, vegetables, groceries and milk to the citizens at their doorsteps. For the home quarantined people, a special mobile application was used for tracking their movement through Global Position System (GPS) and updates on their health conditions. The infected patients were treated with a trio consisting of Hydroxychloroquine, Tamiflu and HIV drugs, through which many patients recovered. The provision of free ration for poor households and cooked food for needy people were made available in the district for two months.
There were many challenges confronted by the District Administration as there was a sharp rise in the number of cases within a few days after the first few cases were reported. The district administration sensed the possibility of community transmission. The district collector imposed ‘maha [great] curfew’ to ensure stricter lockdown for 42 days (3 spells of 14-day cycles) (Bhatt, 2020). ‘The Covid crisis appeared as a shark in the sea and in the process of swimming, the swimmer had just one option, either to swim as fast as possible to save himself or let the shark finish him’, said the District Collector of Bhilwara, Mr Rajendra Bhatt (as quoted in Sawshilya, 2020, p. 4). The Administration sealed the district’s borders to curb the movement of private vehicles; the trains had no stoppage and buses were not allowed to operate in view of community-transmission in the nation’s textile-hub, Bhilwara. The practices adopted in the district proved successful due to prompt measures and policies of the administration and compliance on part of the citizens.
The Ramganj Model
Ramganj, a densely populated area in Jaipur, became the epicentre of virus spread just after Bhilwara recorded success in containing the spread of the disease. The district administration stated that the first case was confirmed on 26 March 2020 when a returnee from Oman had tested Covid-19 positive. The abrupt increase in the number of infected cases in Jaipur became a cause of concern, here 90% of the total cases reported accounted for Ramganj and pointed towards the the possibility of community transmission (Goswami, 2020). The district administration became active and was quick to adopt the Bhilwara model due to its success in containing the spread of coronavirus. Several factors made it difficult to adopt the Bhilwara model in Ramganj and necessitated carving out a new model based on the local needs with some modifications to the Bhilwara model (Mukherjee, 2020). The measures such as intense contact tracing, surveillance and managing quarantine remained common in both Bhilwara and Ramganj models. The District Collector of Jaipur, Joga Ram, said that the factors such as the demography of the area, people’s cooperation with the administration and availability of and access to resources are the major factors that necessitated a different strategy formulated for containing the virus’ spread in Ramganj (Goswami, 2020a). Demographically, Ramganj is one of the most populous places in the walled city area of Jaipur Heritage Municipal Corporation (TOI, 2020b). It is a ghettoised Muslim colony with low access to hygiene and sanitation facilities, lower level of education and income among the population, narrowly packed streets, lack of public trust on administration, less participation and cooperation by the people (Agrahari, 2020). The district administration soon realised that ‘one size does not fit all’ and formulated a new model commonly referred to as the ‘Ramganj model’. The government’s main focus was to reduce the number of deaths related to Covid-19. Mission ‘LiSa’ (Life-Saving) was launched to reduce the number of deaths related to Covid-19 with the target group that included the old age, pregnant women and people with co-morbidities. The model was adopted in four stages based on the number of active cases present in an area, and the measures were designed in a stage-wise manner. Table 1 provides an in-depth understanding of various measures adopted in the four-stage Ramganj model to contain the Covid-19 crisis (Ali, 2020).
Stages in Ramganj Model for Containing Covid-19
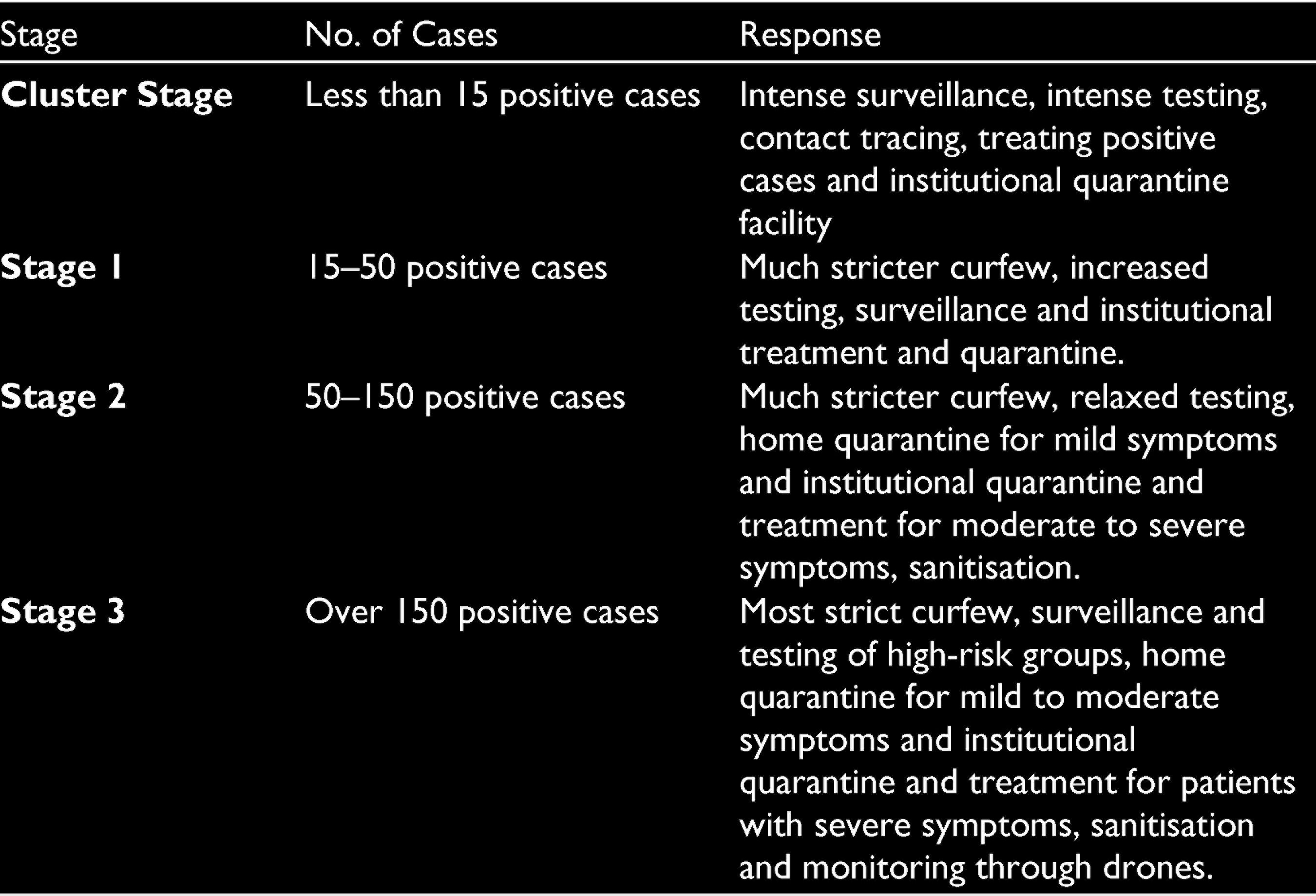
The first stage of the virus outbreak was termed as the cluster stage with less than 15 positive cases. The measures under cluster stage included intense contact tracing, increased testing, surveillance, treatment to the infected and providing isolation and institutional quarantine facilities. An increase in the number of active cases ranging from 15–50 is classified as Stage 1, where stricter measures are followed. The strategies adopted in this stage included a more stringent curfew, increased testing, surveillance, daily reporting and meetings by the administrators, institutional quarantine and treatment for infected ones. As the number of positive cases in an area exceeded from 50 to 150, it was classified in Stage 2 with much stricter curfew, slightly relaxed testing, home quarantine for patients with mild symptoms and institutional quarantine, treatment for moderate to severe symptomatic patients. It also included sanitisation of an area with sodium hypochlorite. Stage 3 was classified when the number of active cases surpassed 150. The measures in this stage included a stricter curfew, surveillance, testing of risk groups, home quarantine for patients with mild to moderate symptoms and institutional quarantine for moderate-to-severe symptomatic patients. This stage also had sanitisation work and use of drones to control people’s movement and their compliance with government guidelines for preventing the spread of the pandemic.
The political representatives and administrative officials paid regular visits to monitor the situation of Ramganj. All the essential services were provisioned at the doorsteps of the people and extending all help to the poor and needy. There was strict contact tracing, and testing was carried out as the people willingly did not report about their travel history or influenza-like symptoms. There were also cases where the medical officials were confronted with in the people who refused to cooperate. Although the administration adopted a milder path to persuade the citizens to cooperate with the administration, religious leaders, citizens’ representatives and volunteers were asked to spread awareness. These civil society elements also assisted the state government in the distribution of food, ration, PPE kits, shelter and movement of migrant workers and most importantly by following government rules and orders (Outlook, 2020).
The random sampling in the entire area was conducted several times to take account of the situation and plan the course of action accordingly. People with influenza-like symptoms were tested and asked to quarantine. Localised resources were apportioned to conduct randomised sampling. Teams consisted of nursing students, primary healthcare workers, ANM (Auxiliary Nurse Midwife) and ASHA (Accredited Social Health Activist) workers and school teachers. The objective behind random sampling was to collect data of the infected people, in contact with the infected person, any travel history or history of illness to track possible contagion and control its spread (TOI, 2020a).
The district administration ensured compliance with stricter lockdown and social distancing guidelines (Sharma, 2020). However, moving through narrow streets made it difficult for the administration to restrict their movements. People’s participation and their cooperation are crucial to the success of every public policy and programme. For this purpose, the local police used drones and mobile applications with GPS to monitor their movements (Wadhawan, 2020).
The Administration spread awareness among citizens with the help of citizens’ representatives to persuade citizens to cooperate with the officials. Some civil society organisations operating in the state also came forward to provide shelter to homeless, protective provisions like sanitisers, organising health camps, volunteering and care-giving to vulnerable groups and synchronising their efforts with the state government for care, quarantine and treatment to the migrant workers (NITI Aayog, 2020). The limited access to health services and limited hygiene practices compelled the administration to conduct drives for spreading awareness among the people. There were lots of rumours about the disease, its spread and medicine. There were many incidents where the infected patients were stigmatised and isolated from the society. Moreover, the first case identified in Ramganj was held responsible for the spread of the virus in the area (Bohra, 2020). Thus, it became very important to inform the citizens about the disease, its spread, impact on individual health and repercussions for the community at large and preventive measures. The district administration also carried out regular sanitisation work of the entire Jaipur Heritage Municipal Corporation with sodium hypochlorite to control the spread of the virus. Free masks were distributed to the residents, and a flag rally was organised as a part of awareness-generation drive Covid-19 (Wadhawan, 2020). The success of the Ramganj model was lauded and proposed to be applied in hotspots in Jodhpur (Sharma, 2020).
Other Measures of the State Government
There were series of other measures taken by the state government to contain the spread of the disease. These measures included enactment of the Rajasthan Epidemic Diseases Act (REDA), 2020, and an amendment to the Act for making the use of facemask compulsory for the people to measure prevention and ban on spitting in public places in view of possible spread of the virus. There were other measures put in place for managing the Covid-19 crisis and have been discussed below.
REDA 2020: It was introduced in the Rajasthan State Legislative Assembly on 21 August 2020 and got passed on 16 September 2020. 1 The Act provides powers to the state government to notify any disease as epidemic disease and take special measures and regulations to prevent such an epidemic. The Act provides that powers and duties of the district administration shall be exercised by the district collectors. The Act prohibits any gathering of any type. It also provides for medical screening of the people arriving in the state and arrange their isolation, seal state borders for a period that may be necessary, restrict public and private transport, prescribe social distancing or other measures, prohibit public places or congregation at religious institutions. The Act provided the state government to limit the operation of public and private educational institutions, shops and commercial establishments, restrict the duration of services in essential and emergency services and other measures that may be necessary to prevent an outbreak of an epidemic disease. The Act incorporates punishment provisions of two-year imprisonment or a fine of ₹10,000 or both for individuals and institutions who fail to comply with the provisions listed in the Act during an epidemic disease.
The Rajasthan Epidemic Disease (Amendment) Act, 2020: The amendment bill was proposed on 31 October 2020 and passed on 4 November 2020. 2 The amendment to the Act added the provision using a facemask or face cover compulsory for people at any public place, public or private transportation, workplace or social, political or general functions. This was the first initiative by any state government to make mandatory facemasks during an epidemic outbreak as a preventive measure. The state government on the opinion of health experts and researches by various institutions like the Duke University found the use of well-fitted N-95 masks, triple-layer surgical masks and double-layer pleated cotton masks effective in preventing the spread of coronavirus (Hindustan Times, 2020b). The newly elected US President Joe Biden has also made 100 days mandatory mask to fight Covid-19 in the USA. The Government of Rajasthan was quick in understanding its importance and made it compulsory before many developed nations did so (Hindustan Times, 2021).
Ban on spitting in public places: The state government of Rajasthan banned the spitting of betel leaf, any chewable tobacco or non-tobacco products or sputum in public places or institutions from 11 April 2020. The ban came as a response measure taken to control the spread of highly contagious Covid-19 pandemic. The ban was introduced under Section 2 of the REDA 1957. The violation of the ban would invite penalty under Section 188 of Indian Penal Code that deals with the matters relating to disobedience to order duly promulgated by a public servant (The Hindu, 2020). The state government’s decision was hailed by many activists who indicated the high risk of Covid infection to the tobacco-users and urged the government for a complete ban on sale, purchase and advertisement of tobacco products as a measure to control the spread of pandemics.
Besides, there were other measures like setting up of post-Covid care centres in Ayurveda hospitals, post-Covid clinics and post-Covid wards in every district to provide counselling and rehabilitation to Covid-recovered patients battling with post-Covid symptoms such as respiratory, cardiac, transitory disease, pancreas disease, kidney problem, body fatigue and mental trauma, stress and so on. 3
Critical Appraisal
Rajasthan was the first state to clamp a state-wide lockdown and gave many models and adopted measures to manage the Covid-19 pandemic. The menace caused by the pandemic affected all sectors, regions and all segments of the population. The government is the most legitimate functionary that exercises authority, makes rational use of resources, takes decisions and works to minimise the impact of and control the outbreak of any epidemic disease. Many exhaustive plans and effective strategies were developed globally to counter the effects of Covid-19 crisis. Some governments were proactive and citizen-centric, while others lost their battle against the unscrupulous enemy in the form of the virus, causing significant damage to the humankind. This article has highlighted the models developed and measures adopted by the state of Rajasthan and its promptness in handling the Covid-19 crisis in the state.
In terms of disaster preparedness, the state governments that had not anticipated a virus outbreak and was least prepared in handling the pandemic. The shortage of health infrastructure was worrying the state in the initial days of Covid-19 outbreak. Rajasthan has a ratio of 1:10,976 for doctor and population (DTE, 2018) and a ratio of 1:1,521 for the availability of hospital bed to population (SIHFW, 2019). The management of the pandemic in many developed countries with adequate health infrastructure was an utter failure, and states like Rajasthan with inadequate infrastructure were also perceived to be a failure. However, the management in Rajasthan with all adversities proved reasonably successful. The reason lies in the proactive, responsive, dedicated, competent and citzen-centric approaches of the state administration, political will and strategic decision-making for most rational use of resources.
The pandemic was viewed as an opportunity for a trial-and-error approach and learning from experience for managing the crisis. The state administration created district war rooms which gave full powers to the district magistrate and additional district magistrate for district-wise plan formulation. It enabled them to formulate district-specific plans, coordinate all departments working in the district and local government to mitigate the impact of the pandemic, dovetail responses and use of locally available human resources. The war rooms also had the responsibility to redress the grievances related to the Covid-19 management in the district and ensure the provision of essential services and overall monitoring. These attempts landed the state into becoming a role model nationally and internationally and presenting models to handle any epidemic in the future. The learnings from the Bhilwara model and the Ramganj model make it evident that well-knit and properly implemented plans are the key to successful management of epidemics.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article
Funding
The authors received no financial support for the research, authorship and/or publication of this article.