
Abstract
During organizational entry, newcomers often draw upon internal resources like coworkers and supervisors to navigate their roles. Could external interactions with customers or patients hold the key to newcomer adjustment in certain job contexts? Our study, rooted in the conservation of resources theory, identifies a critical link between mistreatment from external parties and newcomer adjustment—a connection that is explained by rumination and work engagement. Through two studies involving new nurses in China (Study 1: four-wave cross-lagged panel design, N = 181; Study 2: four-wave time-lagged design, N = 198), we uncover that mistreatment from patients results in rumination among newcomers, leading to diminished task mastery and role clarity, as mediated by reduced work engagement. This ripple effect of external mistreatment persists even when accounting for internal mistreatment (abusive supervision and coworker incivility). Our results illustrate how negative interactions with external entities can hinder newcomer adjustment—a revelation with far-reaching implications for practitioners and future research.1
Every year, millions of newly graduated individuals enter job markets worldwide. For instance, in 2021, there were around 4.2 million college graduates in the United States (Melanie, 2023). In China, an expected 11.6 million college graduates (both undergraduates and postgraduates) are estimated to enter the job market in 2023 (Ministry of Education of the People’s Republic of China, 2022). Ongoing job transitions are also becoming more common. Individuals in the United States, for example, undergo an average of 12.3 job transitions between the ages of 18 and 52 (Bureau of Labor Statistics, 2019). Thus, increasing numbers of employees are newcomers to their work groups and organizations. As such, newcomer socialization, the interactive process by which new employees learn the knowledge, skills, and behaviors necessary to succeed in their new roles (Bauer et al., 2007), has become a research topic of increasing significance.
In the field of newcomer socialization literature, it is widely accepted that the interactions between newcomers and their supervisors/coworkers within organizations greatly impact their adjustment to new environments. Studies have shown that positive experiences, such as receiving social support (Kammeyer-Mueller et al., 2013), developmental feedback (Li et al., 2011), and empowerment (Chen and Klimoski, 2003; Harris et al., 2014), all contribute to the success of the newcomer’s transition. Conversely, negative experiences, such as social undermining (Kammeyer-Mueller et al., 2013) and interpersonal conflict (Nifadkar and Bauer, 2016), can have damaging effects on this process. While prior investigations have largely directed their attention toward exploring social interactions between organizational insiders and newcomers, there remains a notable dearth of studies delving into the effects of social interactions with organizational outsiders on newcomer adjustment (for a few notable exceptions, see Liu et al., 2015; Scott and Myers, 2005).
Organizational outsiders constitute a potentially valuable source of feedback on the services the organization provides. By definition, organizational outsiders are stakeholders external to the organization. Interacting with and serving organizational outsiders is part of many professionals’ core daily work activities (e.g. Baranik et al., 2017; Boukis et al., 2020; Karaeminogullari et al., 2018; Liu et al., 2015, 2020b) and meeting the expectations of outsiders is becoming an increasingly important goal for organizations and employees, including newcomers (Ehrhart et al., 2011; Grant and Parker, 2009). Through interacting with and serving organizational outsiders, newcomers learn to use job-related skills and knowledge. Thus, service encounters involving organizational outsiders and newcomers are likely to influence the process whereby newcomers learn to perform their new jobs. By the same token, negative interactions with organizational outsiders are likely to erode newcomers’ confidence, deplete psychological resources, and impair their adaptation to the new job. Given the predominant focus in previous research on exploring the social interactions between newcomers and organizational insiders (Fang et al., 2011), our current grasp of the potential consequences arising from unfavorable social interactions with organizational outsiders on newcomer adjustment is somewhat limited.
In this study, we draw upon the conservation of resources theory (COR; Hobfoll et al., 2018) to investigate the impact of negative service encounters on the process of newcomers adjusting to their new roles. We focus on the healthcare industry in China and examine patient mistreatment as a type of negative service encounters. We propose that beyond mistreatment from organizational insiders such as supervisors or coworkers, patient mistreatment triggers rumination, hindering a newcomer’s ability to maintain sufficient energy and attention required to perform their job duties (i.e. work engagement), thereby causing harm to their learning outcomes like task mastery and role clarity. The mistreatment of healthcare workers by patients is a prevalent issue (Karaeminogullari et al., 2018). Specific to our research context, a survey in China found that 66% of nurses had experienced conflicts with patients and 51% had experienced verbal aggression from patients (Cai et al., 2022). Conceptualizing patient mistreatment as a work stressor (depleting personal resources) and drawing upon COR theory (Hobfoll et al., 2018), we propose that patient mistreatment negatively relates to newcomer adjustment by triggering rumination and hindering work engagement. The research model is presented in Figure 1.

The conceptual model.
Our study aims to make the following contributions to the literature. First, we highlight the role of organizational outsiders as information sources that affect how well newcomers adjust to their new jobs. Specifically, our investigation makes a distinctive contribution to the existing literature by simultaneously examining the effects of social interactions with insiders and outsiders. By doing so, our research provides insights into whether the effects of external mistreatment go beyond that of internal mistreatment in shaping newcomer adjustment. We identify two learning outcomes (also called proximal adjustment indicators): role clarity and task mastery. For service employees, providing service to clients, customers, or patients is an essential part of their job. Therefore, it is crucial that newcomers understand their job responsibilities (role clarity) and master necessary job skills (task mastery) to perform their job efficiently (Bauer et al., 2007). Negative social interactions such as mistreatment can hinder newcomers’ learning process by causing them to be preoccupied with negative thoughts (e.g. “Maybe I should just give up now because I cannot handle difficult patients”) and become less engaged in service activities (e.g. “I am not motivated to learn to serve patients”). By developing and examining a sequential mediation model, our study provides a more nuanced understanding of how patient mistreatment influences newcomer adjustment through newcomer rumination and work engagement.
Second, our study responds to the call for integrating the literature on work stress and newcomer socialization (Ellis et al., 2015) and advances the understanding of the link between work stressors and newcomer adjustment. An explicit focus on newcomer adjustment in the context of mistreatment is important because the process of newcomer adjustment involves learning and uncertainty reduction. The key outcome of interest in newcomer socialization studies is the degree to which employees learn their jobs by achieving a sense of role clarity and task mastery (Bauer et al., 2007). In contrast, past research to date focusing on longer tenured employees tended to explore how such mistreatment of employees affected their mood (Wang et al., 2013), stress (Shih et al., 2023), well-being (Chi et al., 2018), and job performance (Baranik et al., 2017). While important, these studies do not speak to how such mistreatment affects the process of learning one’s job. For example, studies examining the role of mistreatment on veteran employees tends to treat our focal outcomes (role clarity and task mastery) as factors that buffer the effects of third-party aggression (e.g. Gilardi et al., 2020; Park and Kim, 2019). In other words, mastery of one’s job is assumed to be independent of the mistreatment experience, and instead it is treated as a resource helping employees cope with the stress arising from mistreatment. It is our contention that among newcomers, patient mistreatment affects the very process by which newcomers learn their roles.
Third, newcomer adjustment is a dynamic process characterized by change and evolution. Accordingly, newcomer adjustment must be examined from a temporal perspective (Allen et al., 2017). The research design of our study offers new insights into the focal relationships. In Study 1, we utilized a four-wave cross-lagged panel design, which explored the reverse relationships from newcomer adjustment to patient mistreatment. In Study 2, we utilized a four-wave time-lagged design with multiple sources of data to test the robustness of the mechanism linking patient mistreatment to newcomer adjustment. Study 2 provided evidence for the mechanism of rumination by controlling for alternative mechanisms and utilizing coworker-reported data on newcomer adjustment. Our research design allowed for a more comprehensive understanding of the mechanisms underlying the relationship between patient mistreatment and newcomer adjustment, ultimately enhancing the validity and reliability of our findings.
Our study’s findings have implications for service industries beyond healthcare. In industries such as healthcare, retail, hospitality, banking, and education, employees often have to engage in interactions with outsiders in the regular course of their jobs. These industries are also among those with high turnover (Bureau of Labor Statistics, 2023) and find it “mission critical” to bring newcomers on board quickly. Taking a broad perspective on how social contexts shape employees’ adjustment to work, especially newcomers, can improve organizational practices and employee well-being. Therefore, our work is a step forward in understanding the complexities of work environments, which can potentially impact service employees.
Theoretical background and hypotheses
Social context of newcomer adjustment
The socialization literature considers newcomer adjustment as a process of uncertainty reduction and learning (Bauer et al., 2007; Boulamatsi et al., 2021; Van Maanen and Schein, 1979), whereby newcomers use the social context of work to acquire knowledge and information and to learn appropriate behaviors. The social context of work refers to “interpersonal interactions and relationships that are embedded in and influenced by the jobs, roles, and tasks that employees perform and enact” (Grant and Parker, 2009: 322). In these interpersonal interactions and relationships, organizational insiders such as supervisors and coworkers play an important role in shaping newcomer work experience and behaviors. Numerous studies have shown that organizational insiders are key influencers of newcomer adjustment (e.g. Ellis et al., 2017; Gross et al., 2021; Morrison, 2002). The implications of such studies have been valuable in advancing our understanding of the social context of newcomer adjustment; however, the interactions between organizational outsiders and newcomers in newcomer adjustment have been overlooked even though they occur on a daily basis (Wang et al., 2015).
In service-oriented jobs like nursing, negative service interactions with outsiders of an organization, such as patients, can be viewed as work stressors that result in the loss of resources (Hobfoll, 1989; Hobfoll et al., 2018). The COR theory highlights the crucial need for recovery (Hobfoll, 1989), and insufficient recovery (i.e. rumination) can be considered the mechanism that links stressors to outcomes (Geurts and Sonnentag, 2006; Syrek and Antoni, 2014). In line with this perspective, Ellis et al. (2015) proposed that work stressors, especially hindrance stressors (e.g. patient mistreatment), lead to the depletion of personal resources, exacerbating negative reactions like rumination and negatively impacting newcomer adjustment. We build upon this premise and suggest that rumination acts as an explanatory mechanism that links patient mistreatment and new nurse adjustment.
Patient mistreatment and rumination
Patient mistreatment can be defined as intentionally or unintentionally hostile verbal and non-verbal behaviors (Baranik et al., 2022; Tepper, 2000), which are often directed at nurses in the healthcare industry. Dealing with patient mistreatment is highly stressful, which implies a threat to new nurses’ resources. We expect that patient mistreatment will trigger rumination among new nurses. In our study, we defined and operationalized rumination as negative work rumination, which refers to “the preoccupation with and repetitive thoughts about negative work experiences that may extend beyond the workday” (Frone, 2015: 150). Negative work rumination is an unpleasant and undesired cognitive process that commonly occurs after prolonged exposure to negative work experiences.
COR theory asserts that individuals strive to preserve their limited resources and minimize the loss of them. The theory also suggests that stress occurs when individuals perceive a threat to their resources, which triggers a defensive response aimed at protecting those resources (Hobfoll, 1989; Hobfoll et al., 2018). In the context of nursing, patient mistreatment can be perceived as a threat to a nurse’s resources. Patient mistreatment can cause emotional distress for the nurse, leading to feelings of guilt, anger, or disillusionment. This emotional distress can deplete a nurse’s emotional resources, causing an accumulation of stress that may lead to rumination or dwelling on negative experiences. As new nurses are still establishing their roles and developing their professional identities (Liu et al., 2020a), patient mistreatment can be particularly impactful. Negative experiences of mistreatment can lead to feelings of inadequacy or incompetence among new nurses, which can damage their self-esteem and reduce their motivation to continue in the profession (Michelle Rowe and Sherlock, 2005). Additionally, new nurses may already be experiencing higher levels of stress owing to the challenges of adapting to a new work environment and adjusting to a new role. Patient mistreatment can exacerbate this stress and impair their ability to cope effectively. Therefore, building on the above theoretical reasoning, we suggest that new nurses tend to ruminate after experiencing patient mistreatment.
We further propose that patient mistreatment has a positive relationship with rumination even after controlling for internal mistreatment. This is because patient mistreatment can have a unique impact on new nurses, beyond internal mistreatment from supervisors or coworkers. First, organizational outsiders, such as patients or their families, provide unique feedback and interaction that is distinct from that of insiders. Therefore, negative experiences with outsiders, such as patient mistreatment, could cause a distinct and possibly more severe form of newcomer rumination than negative interactions with insiders. Second, past research suggests that new nurses may ruminate in different ways caused by negative events (Baranik et al., 2017). Thus, negative interactions with outsiders and insiders can be different root causes of newcomer rumination. Therefore, while internal mistreatment from supervisor or coworkers may cause newcomer rumination (in a non-newcomer setting, Su et al., 2022), patient mistreatment can have a particularly detrimental effect on new nurses and may cause additional rumination beyond internal mistreatment. Accordingly, we propose the following hypothesis:
Hypothesis 1: Patient mistreatment has a positive relationship with later newcomer rumination above and beyond internal mistreatment.
Rumination and newcomer adjustment: The role of work engagement
Individuals who experience work engagement—an affective motivational state—will experience greater vigor, dedication, and absorption at work (Schaufeli et al., 2002). Rumination about patient mistreatment entails a continued focus on thoughts and feelings related to that negative experience and impedes one’s ability to recover and decreases work engagement.
Vigor refers to having high levels of energy and enthusiasm while performing work. When a new nurse engages in rumination, it can lead to the depletion of physical and mental resources (Syrek et al., 2017), resulting in reduced vigor. Rumination can increase stress and anxiety levels (Capobianco et al., 2018), draining a nurse’s energy and motivation. This can cause them to feel less enthusiastic and less passionate about their work. Dedication involves a strong sense of involvement in and commitment to one’s work. When a new nurse is stuck in rumination, they may have trouble disengaging from negative experiences (Syrek et al., 2017), which can lead to reduced dedication over time. The persistent focus on negative aspects of work can make a nurse feel disconnected from the purpose of their work and the positive impact they are having on patients (Sonnentag and Kruel, 2006), leading to decreased dedication. Absorption refers to being fully engaged in one’s work and losing track of time while performing tasks. Rumination can negatively impact absorption by causing distractions and interfering with the nurse’s ability to focus on their work. When ruminating on negative experiences, it can be difficult to fully engage in the present moment and remain absorbed in the task at hand, leading to decreased absorption over time. Together, newcomer work engagement deteriorates owing to rumination about patient mistreatment. We propose the following hypothesis:
Hypothesis 2: Newcomer rumination is negatively related to later work engagement.
Work engagement is an important predictor of newcomer learning because it reflects an active and positive motivational state. Engaged individuals are highly committed to their work, and they invest significant effort and attention into their tasks. Research has shown that work engagement is positively related to learning outcomes, such as increased performance (Bakker and Bal, 2010). Engaged employees are also more likely to be open to learning opportunities and to seek out feedback from others (Kleine et al., 2019; Lu et al., 2014). This motivation to learn is critical for effective newcomer adjustment, as it helps new employees acquire the knowledge, skills, and attitudes needed to perform well.
Task mastery and role clarity are two critical indicators of newcomer learning outcomes (Bauer et al., 2007). Highly engaged employees focus their physical, cognitive, and emotional efforts on goal attainment (Kahn, 1990). Investing physical energy into work contributes to newcomers’ adjustment because it helps them to learn organizationally valued behaviors as they increase their effort over time. Allocating cognitive energy into work roles promotes greater vigilance, attentiveness, and focus, which can help newcomers to adapt to their work roles by mastering the necessary job skills (Gwinner et al., 2005) and understanding their job duties and whether they are able to acquire sufficient information about their tasks (Newman et al., 2015). More engaged individuals also experience more positive emotions (e.g. happiness, joy, and enthusiasm) and can thus invest more emotional energy in their work, which is likely to facilitate their learning to perform the job (Bakker and Bal, 2010). Moreover, work engagement can potentially drive workplace behaviors, including learning behaviors (Bakker et al., 2012), which contribute to learning outcomes. Therefore, we postulate the following:
Hypothesis 3: Work engagement is positively related to later newcomer adjustment outcomes in terms of task mastery (H3a) and role clarity (H3b).
Together, we propose a sequential model of patient mistreatment, rumination, work engagement, and newcomer adjustment. Put differently, we suggest that experiencing patient mistreatment impairs new nurses’ adjustment to their new work roles by triggering rumination and reducing work engagement. Thus, the following hypothesis is proposed:
Hypothesis 4: The relationships between patient mistreatment and task mastery (H4a) and role clarity (H4b) are sequentially mediated by rumination and work engagement.
Are those who have lesser adjustment more susceptible to patient mistreatment?
While our hypothesis suggests that patient mistreatment has a negative impact on newcomer adjustment, it is essential to consider that how well newcomers perform their jobs may also affect their interactions with patients. It is possible that those who tend to ruminate or have lower job-related skills are more prone to being targets of mistreatment (Aquino and Thau, 2009). Furthermore, the resource loss corollary of the COR theory (Hobfoll et al., 2018) suggests that a lack of resources can result in further resource depletion in a loss cycle. As individuals face resource exhaustion, their focus shifts toward self-preservation, often resulting in irrational behavior (Hobfoll, 1989). Consequently, the adjustment outcomes of newcomers within an organization can significantly impact their interactions with individuals outside the organization.
In the context of healthcare, when newcomers lack proficiency in job skills, it can hinder their ability to deliver high-quality services to patients, consequently leading to unfavorable interactions between the newcomers and the patients. By the same token, when new nurses have a firm grasp on the required job skills and better understand their tasks and responsibilities, they can offer better patient care and social interactions. Studies indicate that task mastery (Xanthopoulou et al., 2008) and role clarity (Venz et al., 2018) positively relate to employee work engagement. In another study, Frögéli et al. (2019) found that new nurses who experienced higher levels of task mastery and role clarity also experienced lower levels of stress. These findings seem to suggest that better work adjustment can lead to increased work engagement, less negative rumination, and fewer incidents of patient mistreatment. Accordingly, we propose an alternative research question:
Research question: Does newcomer adjustment have reverse effects on patient mistreatment through work engagement and rumination?
Study 1
Method
Procedures and sample
Four waves of data were collected from a sample of newly hired nurses in China, based on a large research project on newcomer adjustment (Liu et al., 2020a). In collaboration with a nursing school at a university in central China, we sent emails to the nursing students in the final year of study and invited them to participate in our longitudinal survey. To ensure the selection of authentic newcomers, participants were asked if they were “about to start work or has been employed in a hospital for less than a month?”, and only those who responded with “yes” were included in our study. They were informed that participation was voluntary and that all of their responses were confidential and would only be used for research purposes. Participants were offered 100 RMB (approximately US$15) as an incentive if they completed all the surveys. Ultimately, 278 graduates agreed to participate. The first-wave survey was sent to the participants approximately two months after they graduated (Time 1). The second-, third-, and fourth-wave surveys were distributed in three months (Time 2, T2), four months (Time 3, T3), and five months post-graduation (Time 4, T4), respectively. We repeated the measurement of our focal variables in all four waves.
Online questionnaires were distributed to the participants via WeChat (a Chinese social networking app). The participants were asked to create a personal code to match their responses across survey waves. The sample sizes at Times 1–4 were 217, 204, 196, and 181, respectively. The four-wave matched sample included 181 new nurses, giving an overall response rate of 65%. The majority (94.5%) of our participants were women (n = 171), and their average age was 22.73 years (SD = 2.73). Participants were from 64 hospitals. Among these hospitals, 27 had only one participant, 20 had two participants (40 participants in total), and 17 had three or more participants (114 participants in total).
Measurement
All of the survey items were translated into Chinese following the standard back-translation procedures (Brislin, 1986). The reliability (Cronbach’s α) of our measures is reported in Table 1. Given our study involved monthly repeated measurements, we used “the last month” as the time frame to capture the potential changes in our focal variables.
Study 1: Means, standard deviations, reliabilities, and correlations among studied variables.
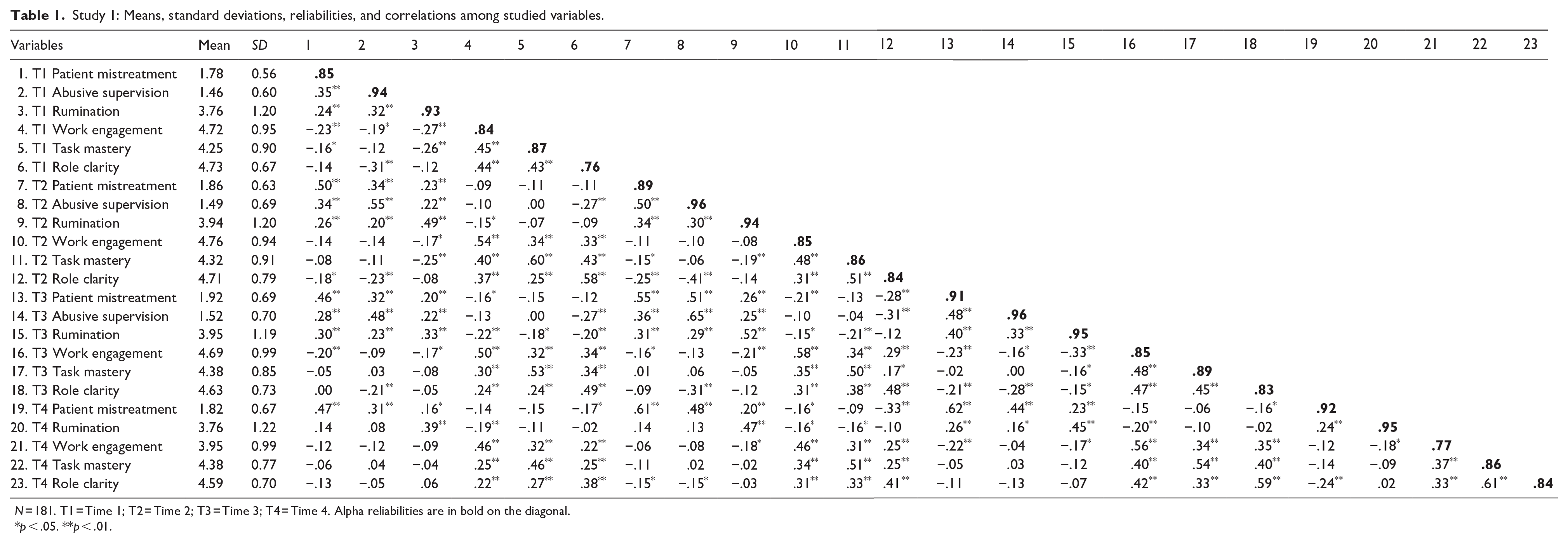
N = 181. T1 = Time 1; T2 = Time 2; T3 = Time 3; T4 = Time 4. Alpha reliabilities are in bold on the diagonal.
p < .05. **p < .01.
Patient mistreatment
We measured patient mistreatment using seven items from Cortina et al. (2001). A sample item is “Have you been in a situation where a patient put you down or was condescending to you?” Responses ranged from 1 (never) to 5 (always).
Rumination
Rumination was measured with four items developed by Frone (2015). A sample item is “How often do you replay negative work events in your mind even after you leave work?” Responses ranged from 1 (never) to 7 (always).
Work engagement
Work engagement was measured using the three-item version of the Utrecht Work Engagement Scale (Schaufeli et al., 2019). A sample item is “I am enthusiastic about my job.” Responses ranged from 1 (never) to 7 (always).
Task mastery
Newcomer task mastery was measured using three items from Spreitzer (1995). A sample item is “I have mastered the skills necessary for my job.” Responses ranged from 1 (strongly disagree) to 6 (strongly agree).
Role clarity
Newcomer role clarity was measured using a three-item scale, which was adapted from Jokisaari and Nurmi (2009). The three items are: “I know what my responsibilities are”; “I know exactly what is expected of me at work”; “Clear goals and objectives are defined for my job.” Responses ranged from 1 (strongly disagree) to 6 (strongly agree).
Internal mistreatment
We measured internal mistreatment in terms of abusive supervision. Abusive supervision refers to the sustained display of hostile verbal and non-verbal behaviors toward subordinates by their supervisors (Tepper, 2000). A 15-item scale developed by Tepper (2000) was used. A sample item is “My supervisor tells me my thoughts and feelings are stupid.” Responses ranged from 1 (never) to 5 (always).
Results
Table 1 reports the descriptive statistics, correlations, and reliability estimates of the focal variables. To confirm the construct validity of our measurements, we conducted a set of confirmatory factor analyses (CFAs). In particular, we conducted four separate CFAs, one at each of the four time points. In addition, as our variables were repeatedly measured, we conducted a series of analyses to test the measurement invariance. Following previous studies (Vandenberg and Lance, 2000), we examined configural and metric invariance. The results of CFAs in Table 2 show that the hypothesized measurement model provided adequate fit to the data at each time point. The results of the measurement invariance tests are also reported in Table 2. As shown, the model fit remained stable as additional constraints were imposed, supporting the measurement equivalence of our focal variables over time.
Study 1: Confirmatory factor analyses of the hypothesized model and longitudinal measurement invariance tests.
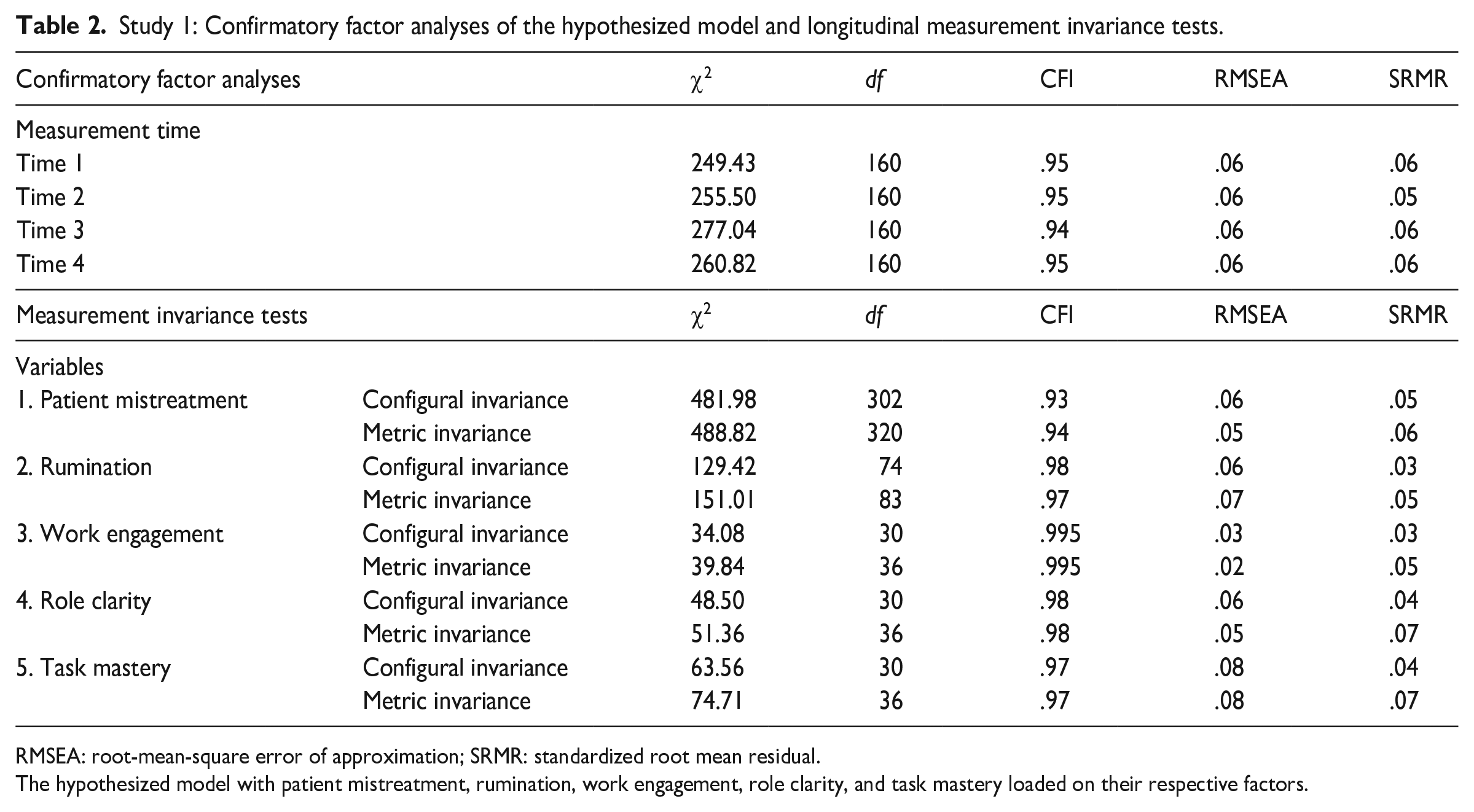
RMSEA: root-mean-square error of approximation; SRMR: standardized root mean residual.
The hypothesized model with patient mistreatment, rumination, work engagement, role clarity, and task mastery loaded on their respective factors.
Model comparisons
We conducted cross-lagged panel analyses in Mplus (Muthén and Muthén, 1998–2011). Following previous studies (e.g. Liang et al., 2018; Zablah et al., 2016), we tested a baseline model versus several competing models. In the baseline model (M1), we included temporal stabilities and synchronous effects (i.e. covariance among constructs measured at the same time) at each wave. For example, Time t patient mistreatment predicted Time t + 1 patient mistreatment. Next, we tested a causal model (M2), in which paths were added to M1 from Time t patient mistreatment to Time t + 1 rumination, from Time t rumination to Time t + 1 engagement, and from Time t engagement to Time t + 1 task mastery and role clarity. Third, we tested a reverse causality model (M3), in which paths were added to M1 from Time t rumination to Time t + 1 patient mistreatment, from Time t engagement to Time t + 1 rumination, and from Time t task mastery and role clarity to Time t + 1 engagement. Fourth, we tested a reciprocal model (M4) in which both the causal and the reverse paths were added to M1 (i.e. a combination of M2 and M3).
The fit indices for the competing models (M1–M4) are presented in Table 3. The hypothesized causal model (M2) fit the data better than the baseline model (M1) (Δχ²(12) = 56.77, p < .001). The reverse causality model (M3) fit the data better than M1 (Δχ²(12) = 21.37, p = .045). The reciprocal model (M4) did not fit the data better than M2 (Δχ²(12) = 18.23, p = .109). We acknowledge that the model fit of the causal model is lower than the conventional cutoff. This is mainly because we did not include all the possible lagged effects in our tested models, including the causal model. Specifically, we only included the autoregression effects generated from two consecutive time points (i.e. T1→T2, T2→T3, T3→T4, as illustrated in Figure 2). When including the autoregression effects generated from two non-consecutive time points (i.e. T1→T3, T1→T4, T2→T4), the causal model showed an acceptable fit (χ2 (108) = 146.94, CFI = .97, RMSEA = .05, SRMR = .06), and the results of the hypothesized relationships were comparable to those from the original causal model (see our online supplemental, Table S1). Nonetheless, we opted not to include these autoregression effects generated from two non-consecutive time points in our tested models owing to the principle of parsimony and in line with prior research (e.g. Hakanen et al., 2011; Kwok and Fang, 2021; Wang et al., 2023).
Study 1: Model fit indices for competing models and results of chi-square difference tests.
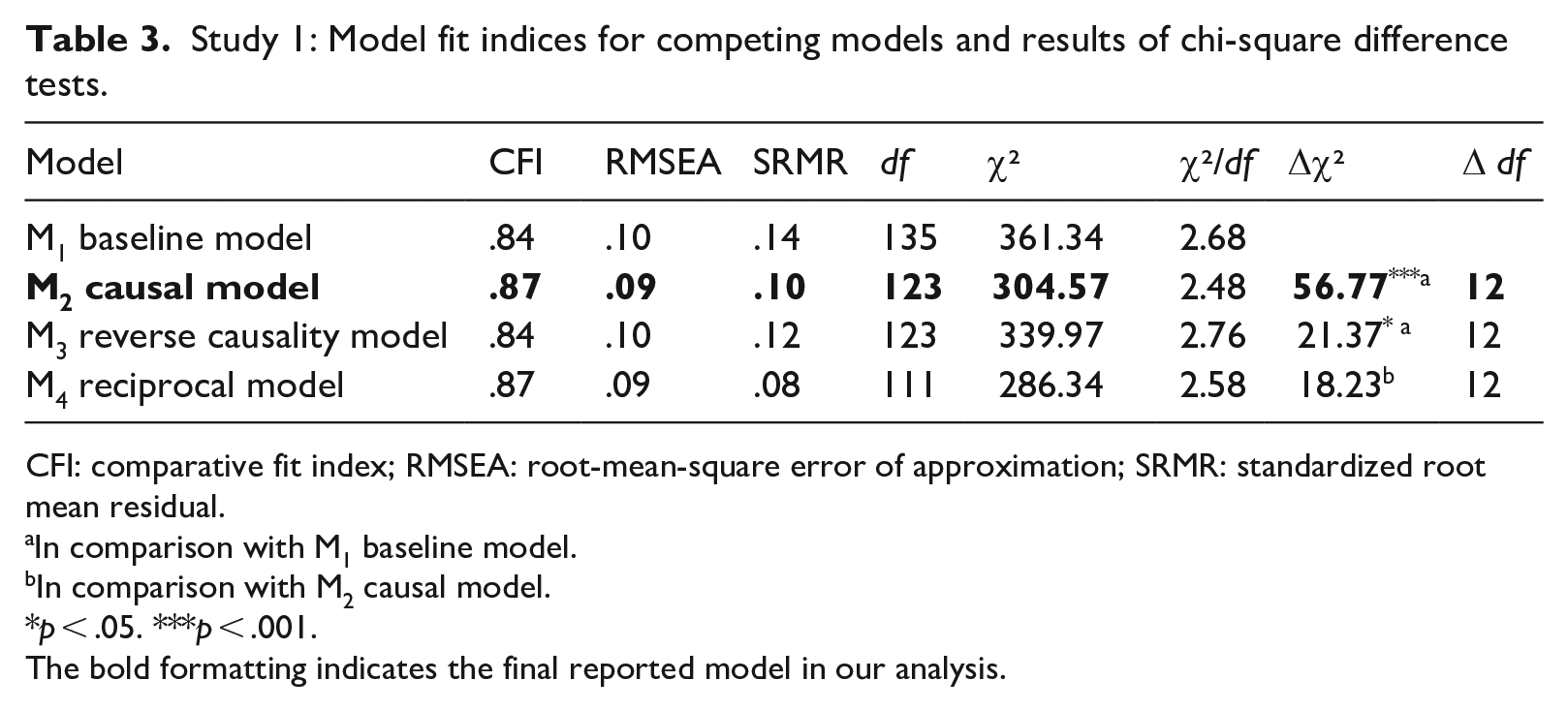
CFI: comparative fit index; RMSEA: root-mean-square error of approximation; SRMR: standardized root mean residual.
In comparison with M1 baseline model.
In comparison with M2 causal model.
p < .05. ***p < .001.
The bold formatting indicates the final reported model in our analysis.
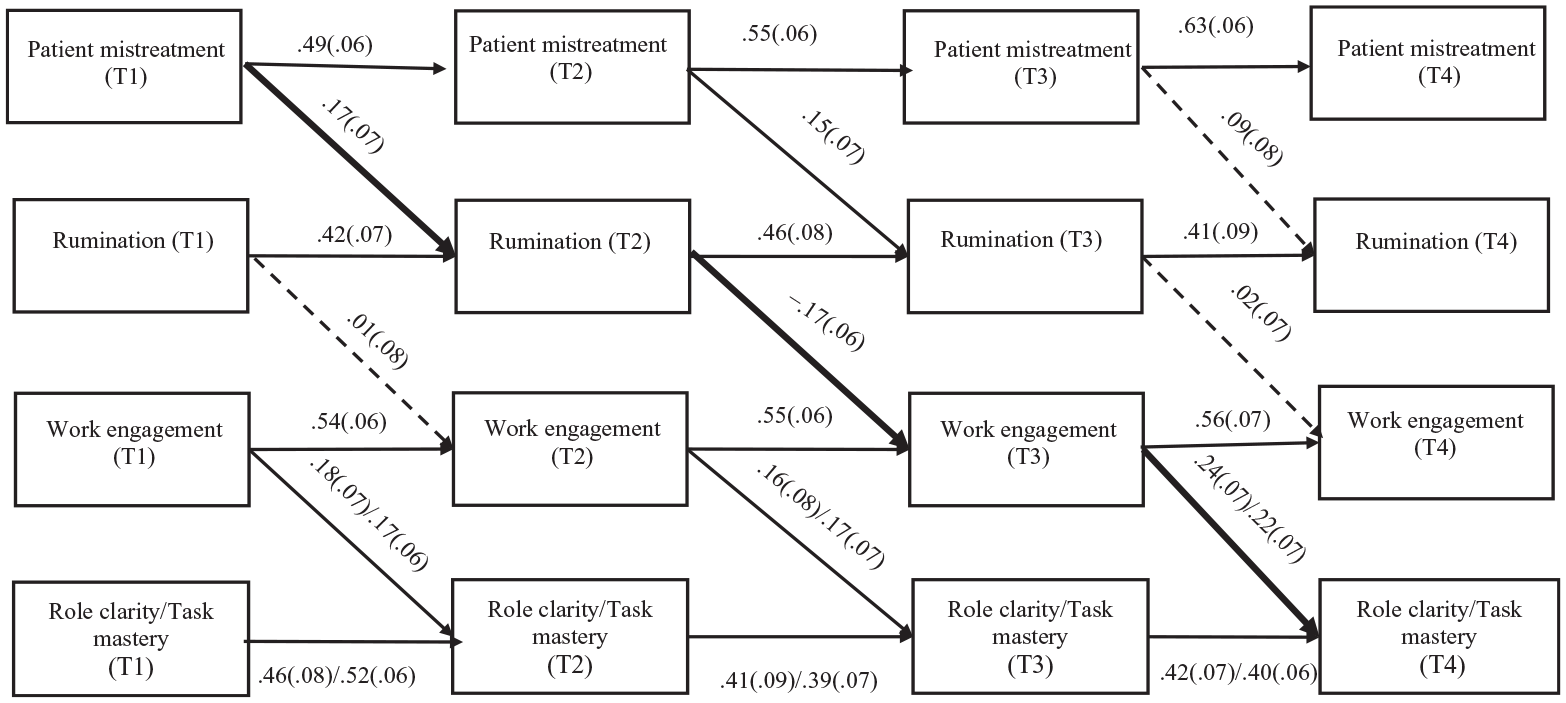
The results of the proposed model in Study 1.
Hypothesis testing
We present the standardized estimation results of the causal model in Figure 2. In the causal model, T1 patient mistreatment was positively related to T2 rumination (β = .17, SE = .07, p = .014); T2 rumination was negatively related to T3 work engagement (β = −.17, SE = .06, p = .003); and T3 work engagement was positively related to T4 task mastery (β = .22, SE = .07, p = .003) and T4 role clarity (β = .24, SE = .07, p = .001). To test the indirect effects, we used a Monte Carlo-based resampling approach with 20,000 replications in Mplus to calculate the 95% bias-corrected confidence intervals for the indirect effects. The bootstrapped results show that the indirect effects of T1 patient mistreatment on T4 task mastery (b = −.008, 95% CI [−.026, −.001]) and T4 role clarity (b = −.008, 95% CI [−.023, −.002]) via T2 rumination and T3 work engagement were negative and significant.
External verus internal mistreatment
We conducted further analyses by adding the effects of T1, T2, and T3 abusive supervision on T2, T3, and T4 rumination, respectively. The results, summarized in Table 4, show that after including abusive supervision, T1 patient mistreatment was positively related to T2 rumination (β = .14, SE = .07, p = .050), but T1 abusive supervision was not related to T2 rumination (β = −.02, SE = .07, p = .822). We compared the unstandardized coefficient of T1 patient mistreatment and T2 rumination with that of T1 abusive supervision and T2 rumination, and we found no significant difference (b = .32, 95% CI [−.11, .77]). The bootstrapped results show that after including abusive supervision, the indirect effects of T1 patient mistreatment on T4 task mastery (b = −.007, 95% CI [−.022, −.001]) and T4 role clarity (b = −.006, 95% CI [−.020, −.001]) via T2 rumination and T3 work engagement were still negative and significant. And the indirect effects of T1 abusive supervision on T4 task mastery (b = .001, 95% CI [−.005, .009]) and T4 role clarity (b = .001, 95% CI [−.005, .008]) via T2 rumination and T3 work engagement were not significant.
Study 1: The cross-lagged results controlling for abusive supervision.
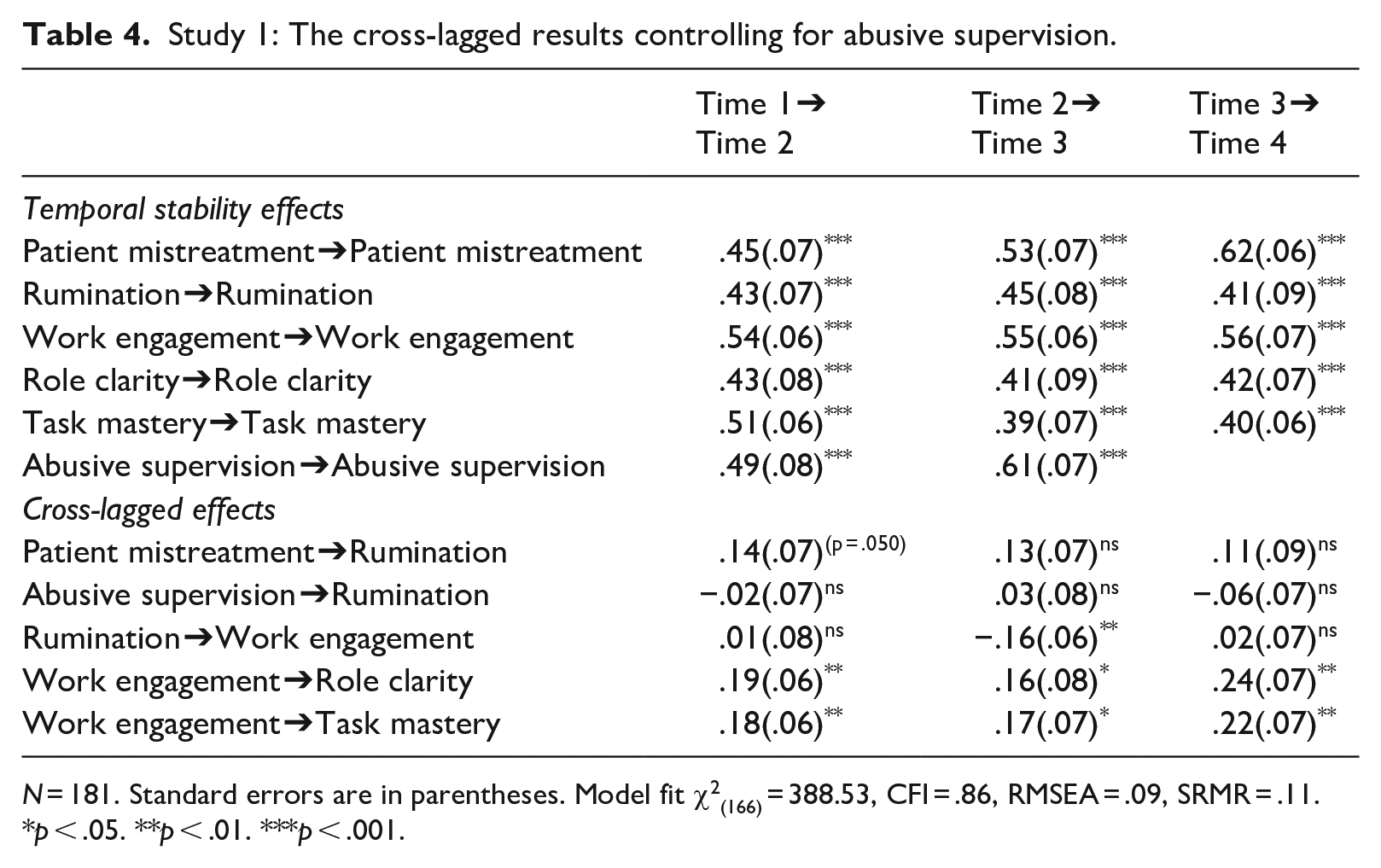
N = 181. Standard errors are in parentheses. Model fit χ2(166) = 388.53, CFI = .86, RMSEA = .09, SRMR = .11.
p < .05. **p < .01. ***p < .001.
Reverse effects
To test whether newcomer adjustment has reverse effects on patient mistreatment through work engagement and rumination (research question). Our model comparison results showed that the reverse effect model (Table 3, M3) fit the data better than our baseline model (Δχ²(12) = 21.37, p = .045). In M3, T1 task mastery (β = .13, SE = .07, p = .075) and T1 role clarity (β = .03, SE = .08, p = .707) were not related to T2 work engagement; T2 work engagement was not related to T3 rumination (β = −.06, SE = .07, p = .378); T3 rumination was not related to T4 patient mistreatment (β = −.03, SE = .07, p = .671). In addition, the indirect effect of T1 task mastery (b = .000, 95% CI [.000, .004]) and T1 role clarity (b = .000, 95% CI [.000, .002]) on T4 patient mistreatment via T2 work engagement and T3 rumination were not significant. Therefore, the reverse effects were not supported. The detailed results can be found in our online supplemental (Table S2).
Additional analysis
The consistency of the same relationship across time points
We tested a constrained model in which the hypothesized lagged relationships across time points were constrained to be equal (e.g. the paths from patient mistreatment to rumination were constrained to be equal). Our results showed that the constrained model (χ2 (131) = 312.57, CFI = .87, RMSEA = .09, SRMR = .10) did not become worse than our hypothesized causal model in which the paths were freely estimated (Δχ² = 8.00; Δ df = 8). The results indicated that our tested causal relationships (e.g. patient mistreatment predicting subsequent rumination) across time points were stable. Similarly, we tested a constrained model for the reverse causal relationships. Our results showed that the constrained model (χ2 (131) = 346.51, CFI = .84, RMSEA = .095, SRMR = .12) did not become worse than the freely estimated reverse causal model (Δχ² = 6.54; Δ df = 8). These results again indicated that our tested reverse causal relationships (e.g. rumination predicting subsequent patient mistreatment) were also stable across time.
Nestedness of observations
As some of our participants were from the same hospital, we addressed the issue of nested data. We first calculated the Intra-Class Correlation (ICC) values for our focal variables in Study 1. The ICC scores were found to be very small, ranging from .007 to .049. We then re-analyzed the data using the sandwich estimator (Type = complex) in Mplus to account for the nested data structure (Farh et al., 2017). The results of this analysis were consistent with the original analysis and we present the results in the online supplemental (Table S3).
Discussion of Study 1
The above results indicated that controlling for abusive supervision, T1 patient mistreatment was related to T4 newcomer adjustment (task mastery and role clarity), mediated by T2 rumination and T3 work engagement, providing support for our Hypotheses 1–4. In addition, we found that the reversed effects of newcomer adjustment on patient mistreatment were not significant. We must acknowledge several limitations of Study 1. First, we used self-report measures for all variables, which could lead to concerns regarding common method variance bias (Podsakoff et al., 2012). Second, the study’s focus on negative reactions to patient mistreatment overlooks the potential positive coping strategies that newcomers might adopt (e.g. Ashford and Black, 1996; Cheng et al., 2022). Third, our measures of rumination, which asked participants to report rumination related to negative work events, may not specifically capture rumination related to negative social interactions such as patient mistreatment. Finally, while supervisors were critical insiders in our study, the role of coworkers in shaping newcomer adjustment was not adequately addressed (e.g. Kammeyer-Mueller et al., 2013).
To overcome the limitations in Study 1, we conducted a second study among new nurses, wherein: (1) we gathered information on newcomer adjustment reported by coworkers; (2) we measured newcomer cognitive (positive framing) and behavioral (job crafting) strategies that can be used to positively cope with negative experiences at work; (3) we operationalized rumination specifically owing to negative social interactions; and (4) we included negative social interactions with both supervisors (abusive supervision) and coworkers (coworker incivility) to capture internal mistreatment.
Study 2
Method
Procedure and participants
In alignment with Study 1, we collaborated with the same nursing school located in central China to conduct a four-wave study. Our first step involved sending an email invitation to nursing students in their final year of study (different sample from Study 1), approximately two months after their graduation (Time 1). Subsequently, the second (Time 2), third (Time 3), and fourth (Time 4) surveys were sent out, each two weeks after the previous survey. Accordingly, we used “in the past two weeks” as our time frame. At Time 1, we measured patient mistreatment, abusive supervision, and coworker incivility. Time 2 focused on assessing rumination, positive framing, and job crafting. Work engagement was evaluated at Time 3, while at Time 4, new nurses were requested to invite one of their coworkers to report on their adjustment outcomes. New nurses were instructed to generate a unique personal code that would serve as an identifier for matching their responses across the different survey waves. This personal code was provided by the new nurses themselves. In turn, their coworkers were asked to enter this personal code in the survey, ensuring the alignment of their responses with the respective new nurse participant. It is important to note that new nurses were instructed to share their personal code with only one coworker, and each coworker reported on no more than one new nurse’s adjustment.
Initially, 410 new nurses agreed to participate in the study, and responses were obtained from 377, 303, 288, and 262 of them, at Time 1–4, respectively. Ultimately, 198 new nurses had matched responses, and 123 of them had adjustment data reported by their coworkers. The majority of new nurses held a bachelor’s degree or higher (71%), and 139 of them were women (70%), with a mean tenure of 45 days (with a range between three and 89 days). Participants were from 109 hospitals. Among these hospitals, 71 had only one participant, 16 had two participants (32 participants in total), and 22 had three or more participants (95 participants in total). We used the same approach as Study 1 to deal with the nestedness issue. The results of the analysis accounting for nested data structure (presented in the online supplemental, Table S4) were consistent with those of the following analysis.
Measurement
In Study 2, we utilized the same scales from Study 1 to assess patient mistreatment (α = .94), work engagement (α = .89), task mastery (coworker-rated) (α = .92), and role clarity (coworker-rated) (α = .94). To measure internal mistreatment, we included mistreatment from both supervisors (abusive supervision) and coworkers (coworker incivility). We used the same scale from Study 1 to measure abusive supervision (α = .98). To measure coworker incivility, we employed four items developed by Sliter et al. (2012) (e.g. “Colleagues ignore or exclude you at work”). Ratings ranged from 1 (“never”) to 5 (“often”), and Cronbach’s alpha was .96. In measuring rumination, we used the same scale as in Study 1. However, we modified the instructions to focus on negative social interactions in the workplace, instructing participants to think about the negative incidents they have encountered in their work interactions with people (e.g. patients/family members, supervisors, coworkers, etc.). Rating ranged from 1 (“never”) to 7 (“always”), and Cronbach’s alpha was .98.
Positive framing pertains to a cognitive appraisal wherein newcomers view ambiguous situations as opportunities and challenges rather than stress-inducing obstacles (Ashford and Black, 1996). We measured positive framing using three items developed by Ashford and Black (1996). Following the same procedure as specific rumination, participants were instructed to contemplate negative social interactions in the workplace and respond to questions on a seven-point scale. A sample item is “Tried to look on the bright side of things?” Cronbach’s alpha was .88.
Job crafting reflects employee proactive job redesign behaviors to modify job demands and resources (Tims et al., 2012). Studies show that newcomers use job crafting to adapt to a new work environment proactively (Cheng et al., 2022). We measured job crafting with a seven-item scale (Cheng et al., 2022). A sample item is “I seek feedback on my job performance from others” (1 = “strongly disagree” to 5 = “strongly agree”). Cronbach’s alpha was .89.
Results
Table 5 presents the means, standard deviations, and intercorrelations among Study 2 variables. Before testing our hypotheses, we first conducted CFAs to assess the discriminant validity of the study variables. The results showed that our hypothesized measure model demonstrated an acceptable fit to the data (χ2 = 2289.78, df = 1091, CFI = .89, RMSEA = .07, SRMR = .06).
Study 2: Means, standard deviations, and correlations among Study 2 variables.
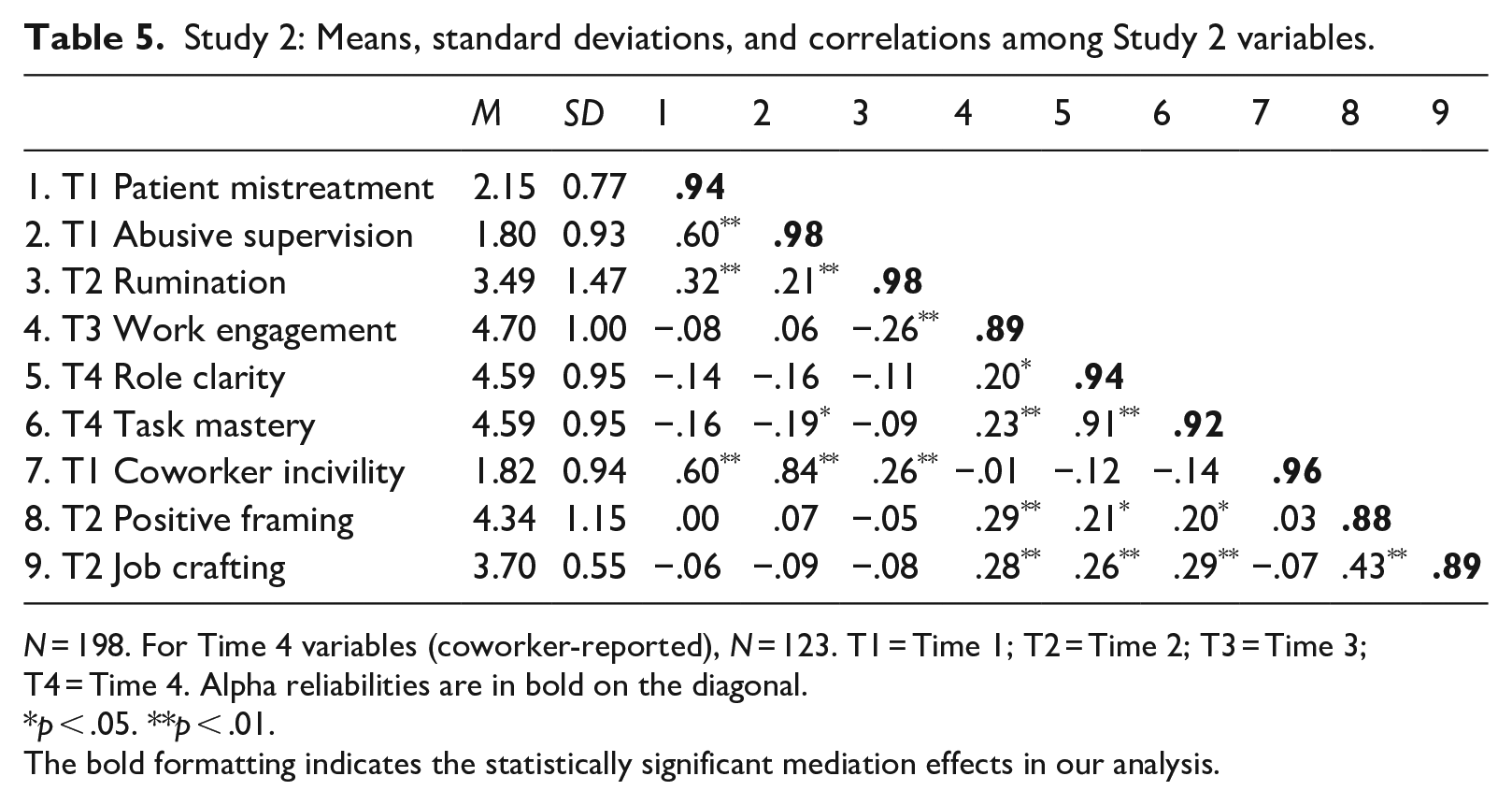
N = 198. For Time 4 variables (coworker-reported), N = 123. T1 = Time 1; T2 = Time 2; T3 = Time 3; T4 = Time 4. Alpha reliabilities are in bold on the diagonal.
p < .05. **p < .01.
The bold formatting indicates the statistically significant mediation effects in our analysis.
Path analysis results showed that after adding internal mistreatment, T1 patient mistreatment was positively related to T2 rumination (β = .27, SE = .09, p = .002). Furthermore, T2 rumination was negatively related to T3 work engagement (β = −.25, SE = .07, p = .001). In turn, T3 work engagement was positively related to T4 task mastery (β = .25, SE = .07, p = .001) and T4 role clarity (β = .21, SE = .07, p = .004). These results again supported Hypotheses 1−3. Additionally, we found no significant association of abusive supervision (β = −.13, SE = .16, p = .413) and coworker incivility (β = .21, SE = .15, p = .157) with rumination. Patient mistreatment showed no relationship with positive framing (β = −.004, SE = .07, p = .950) or job crafting (β = −.06, SE = .07, p = .379). We compared the unstandardized coefficient of T1 patient mistreatment and T2 rumination with that of T1 abusive supervision (coworker incivility) and T2 rumination. We found that compared with T1 abusive supervision (b = .71, 95% CI [0.06, 1.39]), T1 patient mistreatment had a more substantial impact on T2 rumination. For T1 patient mistreatment and T1 coworker incivility, no significant difference was observed (b = .19, 95% CI [−0.37, 0.81]).
The bootstrapped outcomes (see Table 6) indicated that controlling for abusive supervision, coworker incivility, positive framing, and job crafting, the indirect effects of T1 patient mistreatment on T4 role clarity (b=−.017, 95% CI [−.050, −.003]) and T4 task mastery (b= = −.020, 95% CI [−.055, −.004]) via T2 rumination and T3 work engagement were significantly negative. Thus, Hypothesis 4 was again supported. 2
Study 2: Mediation results.
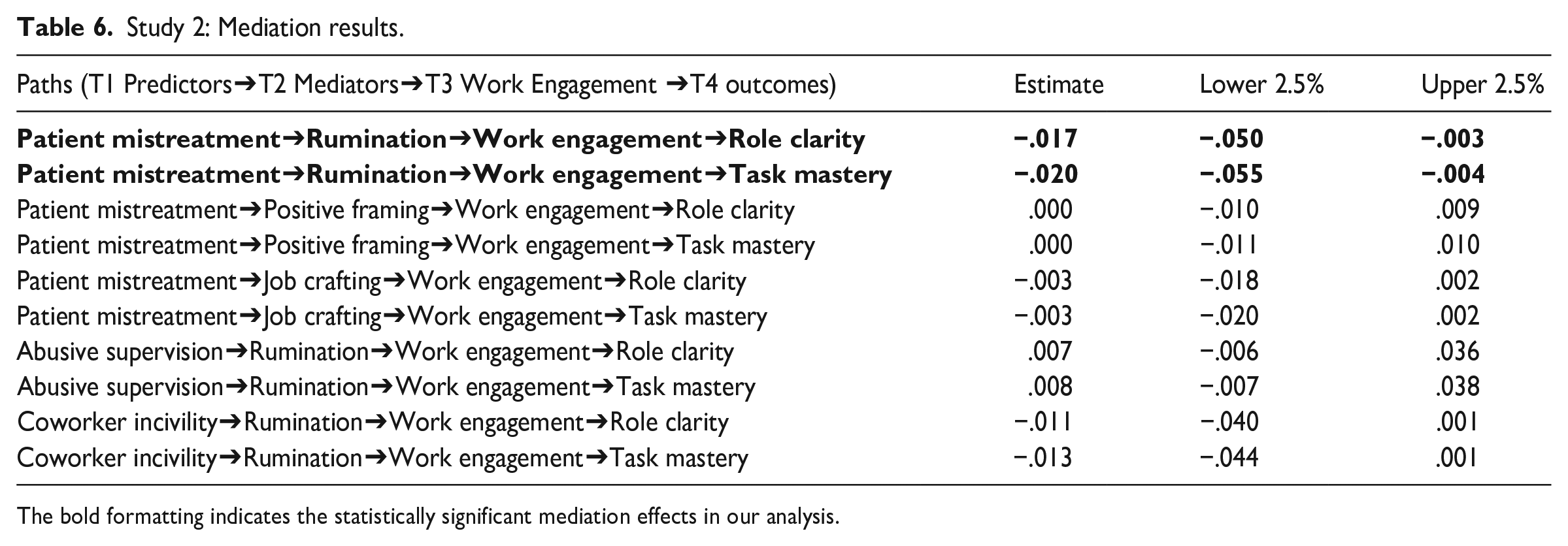
The bold formatting indicates the statistically significant mediation effects in our analysis.
Discussion of Study 2
In Study 2, we utilized a four-wave time-lagged design with multiple sources of data to test the robustness of the mechanism linking patient mistreatment to newcomer adjustment. Study 2 provided robust evidence for the mechanism of rumination by controlling for alternative mechanisms and utilizing coworker-reported data on newcomer adjustment. We found that patient mistreatment significantly predicted rumination and had a negative effect on newcomer adjustment, even after controlling for both abusive supervision and coworker incivility.
General discussion
Theoretical implications
Our research makes several contributions. First, we embedded newcomer adjustment in a broader social context and examined organizational outsiders (i.e. patients) as an important aspect of newcomer adjustment. As such, our study responds to the call by Wang et al. (2015) for research integrating organizational outsiders as an important social aspect of the newcomer adjustment process. Previous studies using the interactionist perspective have focused on how organizational or individual tactics (Bauer et al., 2007) or the characteristics and behaviors of organizational insiders (Boulamatsi et al., 2021; Li et al., 2011) influence newcomer adjustment. Yet, clients and customers, as organizational outsiders, are also important stakeholders through whom newcomers can learn to perform their work tasks and roles (Wang et al., 2015). Our findings provide initial evidence that external organizational stakeholders play a critical role in newcomer adjustment, expanding the interactionist perspective and identifying a broader range of social factors that shape newcomer adjustment.
We believe that our results can encourage future research to simultaneously consider the influence of both organizational insiders and outsiders on employee outcomes. Moreover, we investigated the effects of both insiders and outsiders and found that external mistreatment has unique associations with newcomer rumination and subsequent adjustment, beyond the effects of internal mistreatment. This result suggests that organizational socialization research may underestimate the influence of social context on newcomer adjustment when not considering organizational outsiders. Our study adds to the literature by showing that abuse from outsiders affects the process by which newcomers learn their new job (Grandey et al., 2007). This finding offers new insights beyond what we would expect for experienced nurses. In essence, it reveals that key indicators of work adjustment, such as task mastery and role clarity, may not remain independent of the mistreatment experience, as seen in situations involving experienced individuals (e.g. Gilardi et al., 2020; Park and Kim, 2019). Instead, they can emerge as direct consequences of mistreatment for newcomers.
Second, from a COR theory perspective we examined rumination in a newcomer context and illustrated the role of work engagement in linking rumination to newcomer proximal adjustment. Rumination is a cognitive process underlying the association between work stressors and employee outcomes (Syrek et al., 2017; Wang et al., 2013). However, the exact role that rumination plays in the newcomer adjustment process remains unclear, even though new employees encounter work stress when learning to perform their new jobs during onboarding (Ellis et al., 2015). On the one hand, we extend this line of research to a newcomer context. On the other hand, the organizational socialization literature also benefits by recognizing such a perspective because learning to address work stressors in itself is part of the aims of organizational socialization. Further, our results indicated that rumination as a result of work stressors is not directly related to newcomer adjustment, but indirectly through work engagement. This finding suggests that a motivational process explains why negative cognition is associated with behavioral outcomes (Mitchell et al., 2019), and thus provides a more nuanced understanding of the processes underlying the association between work stress and employee outcomes. Notably, in Study 2, we included rumination and positive coping mechanisms (positive framing and job crafting) and showed the unique influence of rumination.
Finally, we contribute to the newcomer literature by testing the hypothesized relationships over time. Although the newcomer literature suggests that newcomer adjustment is a dynamic process (Ashforth et al., 2007; Li et al., 2011), empirical examinations of newcomers’ dynamic relationships have been limited (Bauer et al., 2021). We provide empirical evidence for the direction of the relationships in the adjustment process. The results indicate that patient mistreatment is more likely to impair newcomer adjustment by inducing rumination and reducing work engagement than the other way around. In other words, the effective adjustment in terms of task mastery and role clarity does not help newcomers reduce mistreatment from patients. This finding provides implications for the antecedents of mistreatment at work. Previous research implies that employees’ own behaviors (e.g. poor performance) may lead to mistreatment from supervisors (Tepper et al., 2011) or customers (Groth and Grandey, 2012). Yet, in a newcomer context, workplace mistreatment seems not to be triggered by newcomers’ own adjustment levels. This informs the research that one needs to take into account employees’ organizational tenure when examining the reasons behind the mistreatment they encounter.
Practical implications
Our study has several practical implications. Managers should be aware that organizational outsiders can have significant effects on newcomer adjustment beyond organizational insiders, and that negative social interactions with them may hinder newcomers from learning their new roles. Organizational socialization programs should thus not only focus on the role of organizational insiders in helping newcomers to learn and grow but also on the influence of outsiders such as clients, customers, and patients. In such programs, newcomers could be taught to deal with organizational outsiders to mitigate the effects of negative service experiences. Customers are more likely to act aggressively when they encounter situational and physiological stressors in the service environment (DeCelles et al., 2019). By improving organizational conditions that have a tendency to upset patients, organizations may help with newcomer adjustment, in addition to improving customer service quality.
Newcomers who experience mistreatment must find ways to eliminate negative rumination. Despite some newcomers using positive appraisal or job crafting strategies to cope with undesirable situations, our research found that they are more likely to resort to negative coping behaviors. Therefore, it is especially important to offer targeted support mechanisms to new nurses. This can include providing them with resources and interventions aimed at promoting emotional well-being. Training programs focused on emotional intelligence may help new nurses develop self-awareness, emotional regulation, and empathy (Smith et al., 2009), enabling them to navigate mistreatment and negative experiences more effectively. In addition, pairing new nurses with experienced mentors or coaches within the organization can provide invaluable support and guidance (Chen and Lou, 2014). Mentors can share their experiences, provide advice, and help new nurses develop effective coping strategies. This support system can also facilitate a safe space for newcomers to discuss and address any negative rumination they may be experiencing.
Limitations and future research
Our study has several potential limitations. First, research with more measurement occasions can more accurately capture the nuances of the changes in organizational phenomena/variables. The optimal number of measurement occasions and their intervals in modeling change require both theoretical and practical justification. Although we employed a four-wave cross-lagged panel design in Study 1, this design may not capture the full range of the dynamics of newcomer socialization. Relatedly, although we tested the reciprocal relationships in Study 1, it does not allow us to make strong causal claims. We encourage future research to further use field experiments to test causal effects.
Second, our samples are from the healthcare industry, which raises concern regarding the generalizability of our findings. We recommend that future research extend our findings to non-nursing settings. In this study, we focused exclusively on new nurses who had just graduated from colleges/universities and who had little full-time working experience before their current jobs. However, work experience does affect newcomer adjustment (Bauer et al., 2007). Researchers could examine the present model among different types of newcomers, such as those who change to a different job. Future research could also seek to replicate our findings in different service industries (e.g. sales) and examine other types of mistreatment (e.g. customer mistreatment) and newcomer adjustment.
Third, while it is possible that the focal relationships could also emerge among long tenured employees, we would expect the relationship to be more acute for newcomers. This is owing to the fact that newcomers, such as new nurses, who lack experience in serving clients or patients, are particularly stressed by mistreatment from these individuals (e.g. patient mistreatment). We encourage future research to compare the focal relationships between newcomers and long tenured employees. Finally, we acknowledge the existence of alternative learning outcomes, such as organizational knowledge, and recommend that future research endeavors delve into these dimensions to further enrich our understanding.
Supplemental Material
sj-pdf-1-hum-10.1177_00187267231211847 – Supplemental material for Patient mistreatment and new nurse adjustment: The role of rumination and work engagement
Supplemental material, sj-pdf-1-hum-10.1177_00187267231211847 for Patient mistreatment and new nurse adjustment: The role of rumination and work engagement by Hai-Jiang Wang, Peikai Li, Talya N Bauer and Berrin Erdogan in Human Relations
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by National Natural Science Foundation of China (project no. 71701074; 72132001).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.